Managing Complex Lipid Patients
|
|
|
- Alexandrina Sparks
- 6 years ago
- Views:
Transcription
1 September 10, th Cardiology for the Primary Care Provider Conference, Salishan, OR Cezary Wójcik MD, PhD, FNLA Department of Family Medicine Diplomate, American Board of Clinical Lipidology Managing Complex Lipid Patients
2 National Cholesterol Education Program ATP National Heart, Lung, and Blood Institute (NHLBI) ATP I 1988 patients with and without CAD who had 2 or more risk factors for CAD have an LDL-C target of <130 mg/dl ATP II lowered the goal LDL-C to 100 mg/dl in patients with known CAD ATP III 2001 introduced risk stratification, LDL-C goal for high-risk patients is <100 mg/dl ATP III 2004 update - optional goal of <70 mg/dl for very high-risk patients ATP IV - aborted in 2013
3 2013 ACC/AHA Guidelines Original ATP IV panel appointed by NHLBI, transitioned to ACC/AHA Expert Panel in mid 2013
4 Cholesterol goals of therapy have been eliminated Advises initiation and maintenance of maximal statin dose (no wasting time to titrate therapy) Evidence limited to RCTs with ASCVD outcomes and systematic reviews and meta-analyses of RCTs with ASCVD outcomes
5 2013 ACC/AHA Guidelines Four Major Statin Benefit Groups Patients with: Clinical ASCVD Primary elevations of LDL C 190 mg/dl DM yo with LDL C mg/dl and without clinical ASCVD Without clinical ASCVD or diabetes with LDL C mg/dl and estimated 10-year ASCVD risk 7.5% using pooled cohort equations

6 Different statin dosages Doses not tested in RCTs are italicized
7 Case 1 63 yom w/ ASCVD 63 yo male, former smoker with established CAD: STEMI at age 55, CABGx4 at age 60, no anginal symptoms currently. Normal BMI, eating healthy, active. Taking all medications. No muscle pain. Had muscle pain on higher rosuvastatin dose, had muscle pain with any atorvastatin dose. Positive family history of heart disease, BP 130/65 Medications: ASA 81 mg daily Carvedilol 12.5 mg BID Lisinopril 20 mg daily Rosuvastatin 20 mg daily
8 Case 1-63 yom w/ ASCVD Labs normal CMP, A1C, TSH, CBC, NT-BNP Total cholesterol 200 HDL-C 35 LDL-C 129 Non-HDL-C 165 TG 180
9 Case 1-63 yom w/ ASCVD Labs normal CMP, A1C, TSH, CBC, NT-BNP Total cholesterol 200 HDL-C 35 LDL-C 129 Non-HDL-C 165 TG 180 Are we done? Does patient need other lipid lowering therapy?
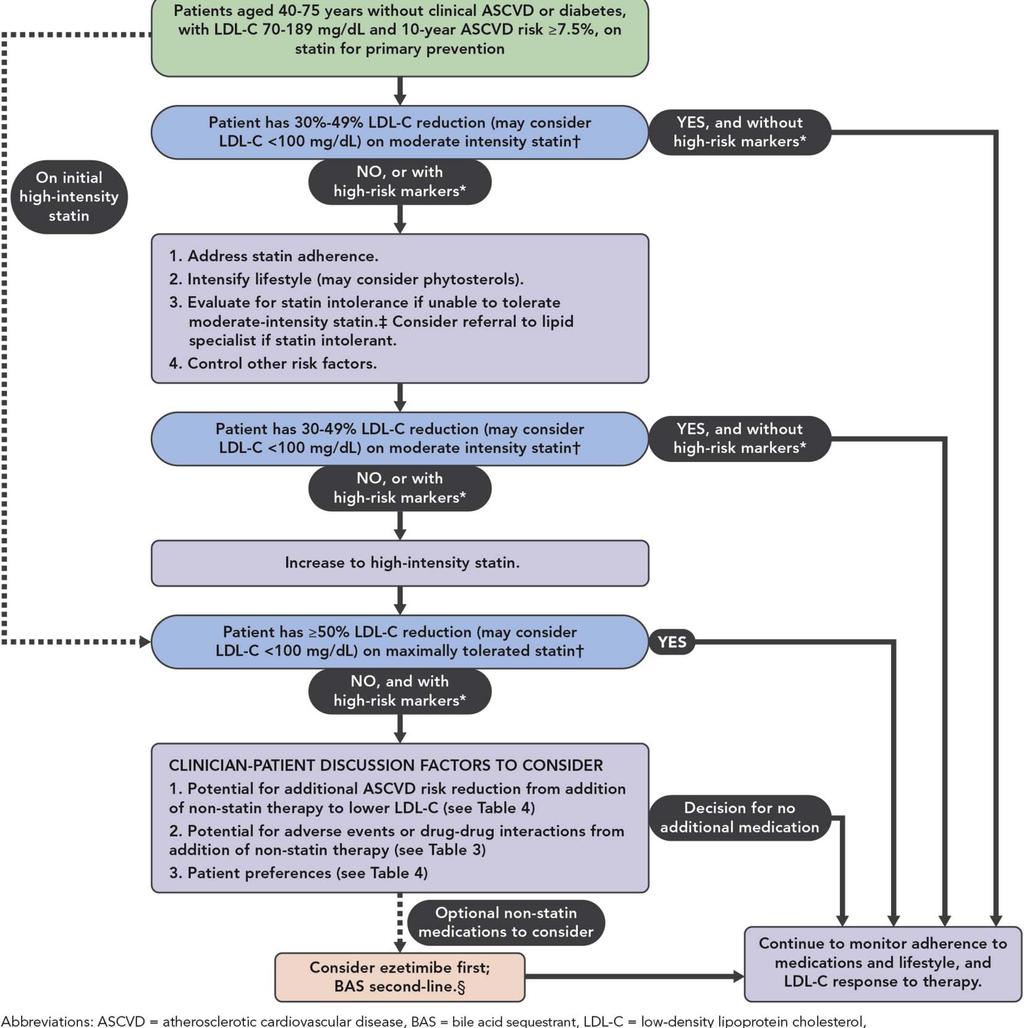
10 2013 ACC/AHA Guidelines Non-Statins Clinicians treating high-risk patients who have a less-than-anticipated response to statins, who are unable to tolerate a less-thanrecommended intensity of a statin, or who are completely statin intolerant may consider the addition of a nonstatin cholesterol-lowering therapy. His untreated LDL-C was 188 mg/dl at time of NSTEMI
11 2013 ACC/AHA Guidelines Non-Statins High-risk individuals include those with ASCVD, those with LDL C 190 mg/dl and individuals with diabetes. In this situation, this guideline recommends clinicians preferentially prescribe drugs that have been shown in RCTs to provide ASCVD risk-reduction benefits that outweigh the potential for adverse effects drug-drug interaction, and patient preferences. The patient is certainly high risk
12 Currently Available Non-Statin Lipid Lowering Drugs Niacin (vitamin B3) Fibrates (PPARα agonists) Bile acid binding resins Ezetimibe (cholesterol absorption inhibitor) Omega3-PUFAs PCSK9 inhibitors
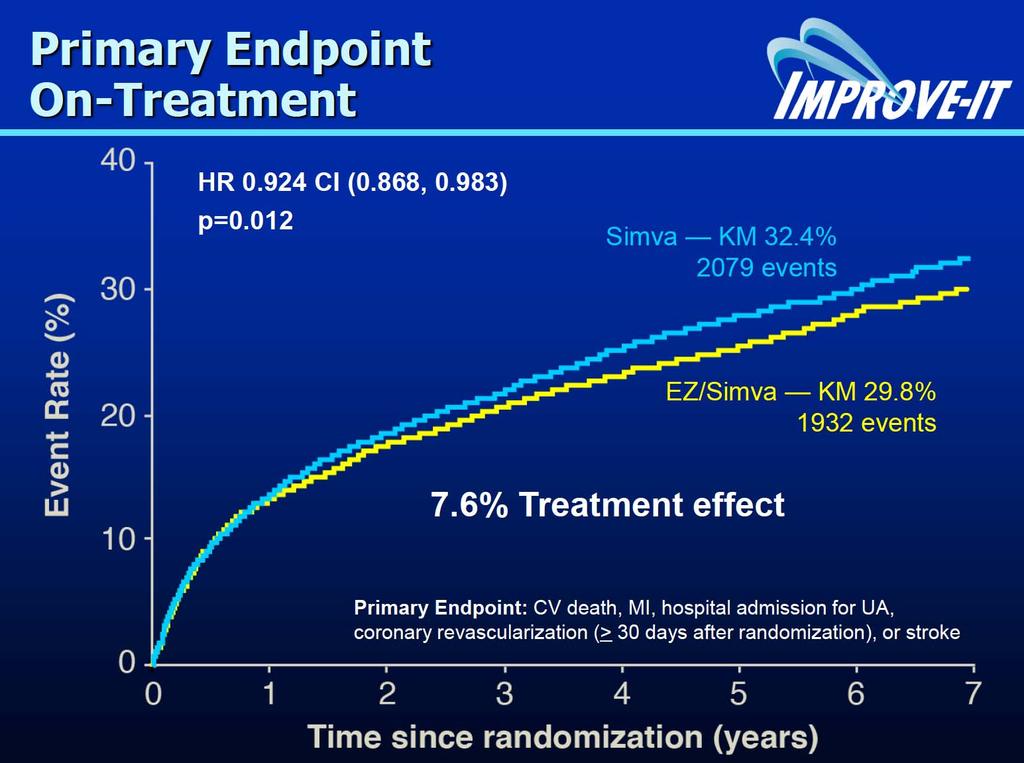
13 New Evidence Since 2013 ACC/AHA Guidelines IMPROVE-IT trial: CV benefits of ezetimibe AIM-HIGH and HPS2-THRIVE trials: Lack of CV benefits of niacin Many trials with PCSK9 inhibitors: Potent LDL-C lowering Secondary analysis show CV benefit ~48-53% Major CV outcome trials under way

14

15 AIM-HIGH Results Primary Outcome 1 o Endpoint: CHD Death, nonfatal MI, ischemic stroke, high-risk ACS, hospitalization for coronary or cerebrovascular revascularization Boden WE. N Engl J Med. epub 15 Nov 2011; doi /NEJMoa
 15 10 5 Risk ratio 0.96 (95% CI 0.90 1.")

16 HPS2 THRIVE 20 Patients suffering events (%) Risk ratio 0.96 (95% CI ) Logrank P=0.29 Placebo ERN/LRPT 15.0% 14.5% 0 NEJM Years of follow up
17 PCSK9 Inhibitors PCSK9 inhibitors available Alirocumab (Praluent) Evolocumab (Repatha) Bococizumab - in phase 3 trials Lower LDL-C 50-80% on top or without statins Post hoc analysis shows ~48-53% decrease in MACE
18 Dramatic LDL-C Lowering by PCSK9 inhibitors LDL-C Mean (±SE) % Change from Baseline Baseline Week 2 Week 4 Week 6 Week 8 Week 10 Week % -62.9% -5.1% Placebo -72.4% Alirocumab LOCF = last observation carried forward. McKenney JM. A Randomized, Double-blind, Placebo-controlled Trial of the Safety and Efficacy of a Monoclonal Antibody to Proprotein Convertase Subtilisin/Kexin Type 9 Serine Protease, REGN727/SAR236553, in Patients with Primary Hypercholesterolemia (NCT: ). American Cardiology Conference 2012, Chicago, IL.
19 Post Hoc Analysis of OSLER Trial: Effect of Evolocumab on Cardiovascular Outcomes 3 Composite Endpoint: Death, MI, UA hosp, coronary revasc, stroke, TIA, or CHF hosp Cumulative Incidence (%) 2 1 HR % CI P=0.003 Standard of care alone (n=1489) 2.18% 0.95% Evolocumab plus standard of care (n=2976) Days Since Randomization TIA = transient ischemic attack; CHF = congestive heart failure; MI = myocardial infarction; UA = unstable angina. Sabatine MS, et al. N Engl J Med. 2015;372:
20 Cardiovascular Outcomes Trials of PCSK9 Inhibitors Alirocumab Evolocumab Bococizumab Sponsor Sanofi/Regeneron Amgen Pfizer Trial ODYSSEY Outcomes FOURIER SPIRE I SPIRE II Sample Size 18,000 22,500 12, Patients 4-16 weeks post-acs MI, stroke, or PAD High risk of CV event Atorvastatin 20 mg or Statin Evidence-based Rx Lipid-lowering Rx equivalent LDL-C 70 mg/dl 70 mg/dl mg/dl 100 mg/dl PCSK9i Dosing Endpoint Every 2 weeks Every 2 or Every 4 weeks Every 2 weeks CHD death, MI, ischemic stroke, or UA hospitalization Primary: CV death, MI, stroke, UA hospitalization or coronary revascularization Key Secondary: CV death, MI, or stroke CV death, MI, stroke, or urgent revascularization Completion March 2018 December 2017 August 2017
21 Biology of PCSK9
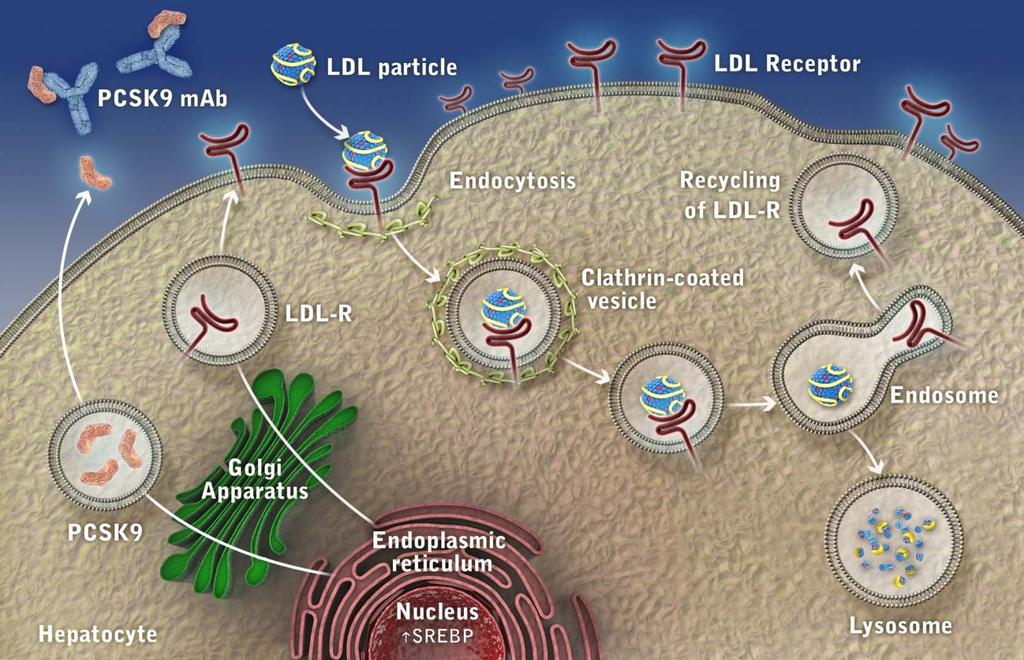
22 Inhibition of PCSK9
23




24
25
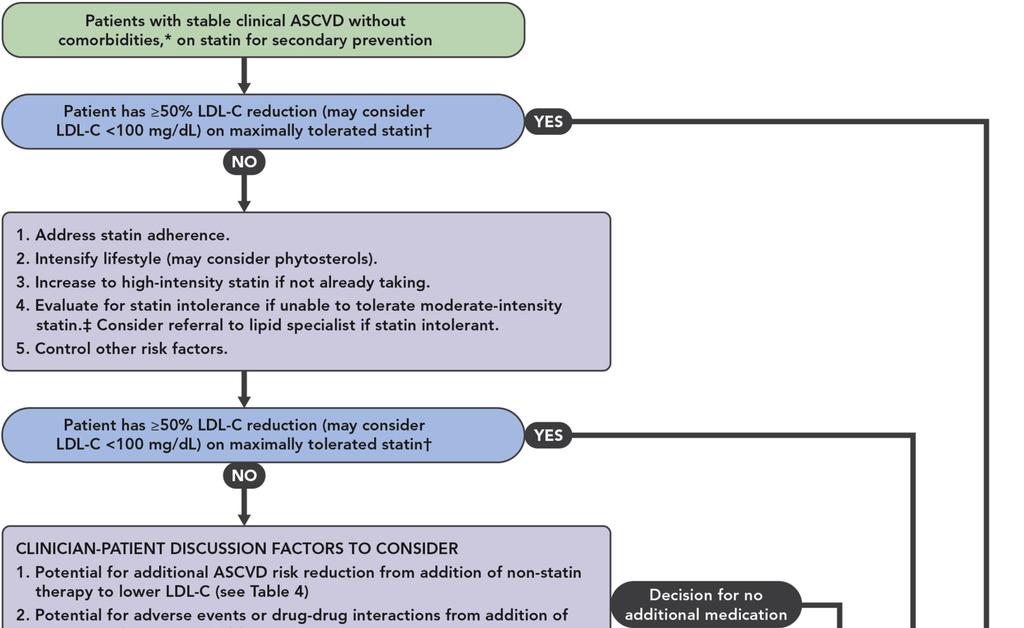
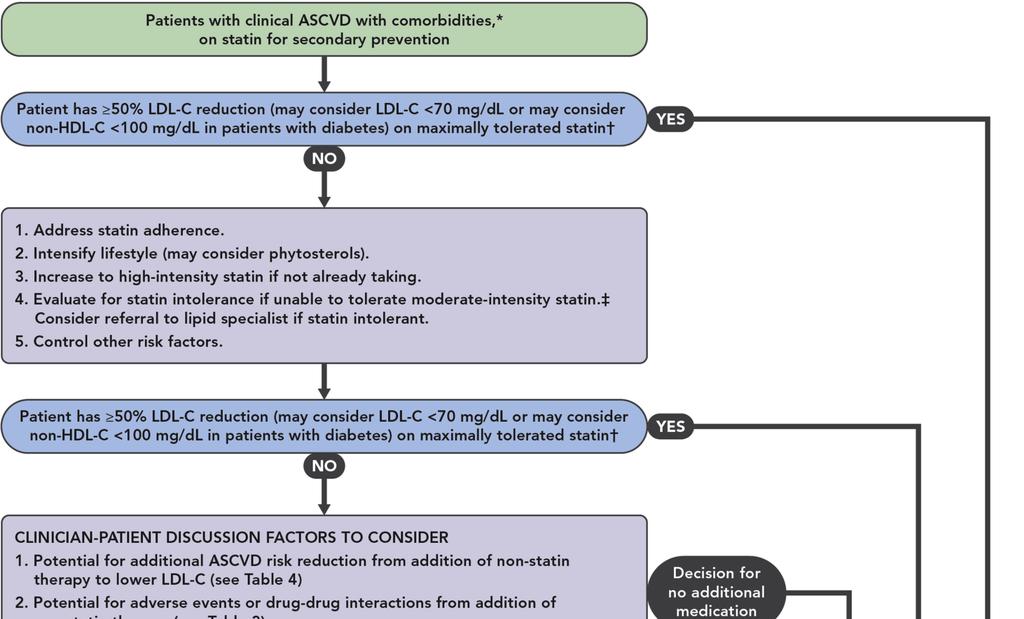
26 Definition of comorbidities Diabetes mellitus Recent (<3 months) ASCVD event ASCVD event while on statin therapy Baseline LDL-C 190 mg/dl not due to secondary causes Poorly controlled other major ASCVD risk factors Elevated lipoprotein (a) Chronic kidney disease
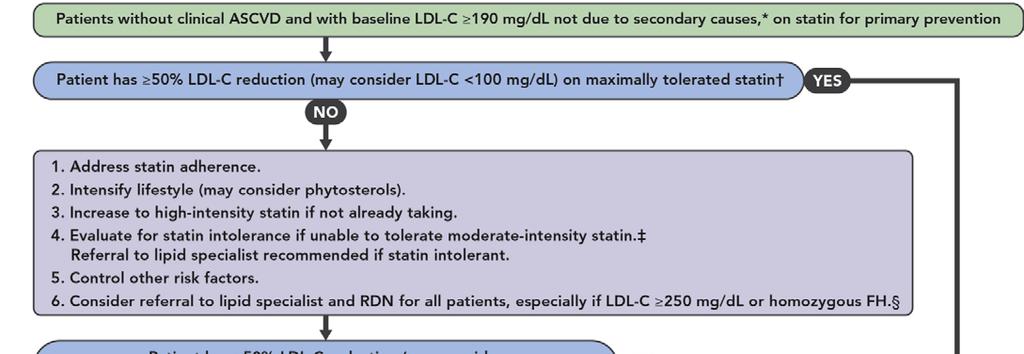
27 Case 1-63 yom w/ ASCVD Labs normal CMP, A1C, TSH, CBC, NT-BNP Total cholesterol 200 HDL-C 35 LDL-C 129 Non-HDL-C 165 TG 180 LDL-C 188 mg/dl before rosuvastatin 20 mg Not 50% reduction, above LDL-C goal < 100 mg/dl
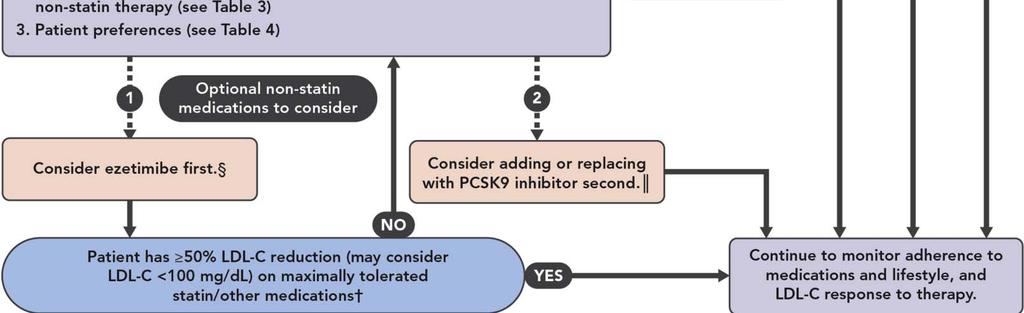
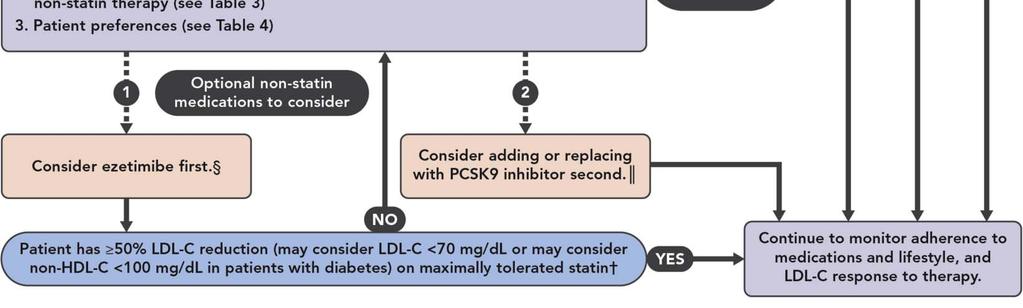
28 Case 1-63 yom w/ ASCVD Ezetimibe 10 mg prescribed
29 Case 1-63 yom w/ ASCVD Ezetimibe 10 mg prescribed Insurance denies ezetimibe stating must try niacin or fenofibrate first
30 Case 1-63 yom w/ ASCVD You write a lengthy PA letter arguing that according to 2016 ACC EDCP: On the basis of currently available evidence of nonefficacy and potential harms, the committee judged that there are no clear indications for the routine use of niacin preparations as additional non-statin therapies, and niacin is therefore not recommended for use in any of the clinical situations addressed below.
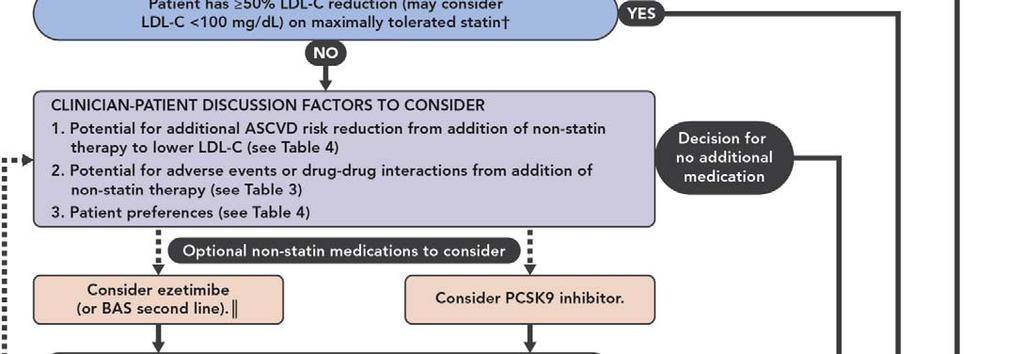
31 Case 1-63 yom w/ ASCVD After 6 weeks on ezetimibe 10 mg plus rosuvastatin 20 mg Total cholesterol 173 HDL-C 35 LDL-C 103 Non-HDL-C 138 TG 175 LDL-C 188 mg/dl before therapy Still not 50% reduction, still >100 mg/dl What next?
32 Case 1-63 yom w/ ASCVD PCSK9 inhibitor prescribed
33 Case 1-63 yom w/ ASCVD PCSK9 inhibitor prescribed Insurance sends back a denial letter arguing that those are experimental drugs for the treatment of high blood fats
34 Case 1-63 yom w/ ASCVD While you are involved in letter exchange with insurance, patient gets to the ER with chest pain, diagnosed with ACS, followed by cath and placement of 2 drug eluting stents Now what?
35
36 Case 1-63 yom w/ ASCVD PCSK9 inhibitor prescribed again, this time arguing that patient had an ASCVD event and needs additional LDL-C lowering (new LDL-C goal < 70 mg/dl) -Alirocumab (Praluent - Sanofi Regeneron) - 75 or 150 mg subcutaneous injection with prefilled pen q2 weeks -Evolocumab (Repatha - Amgen) mg subcutaneously with Pushtronex system monthly mg subcutaneously with prefilled pen q2 weeks
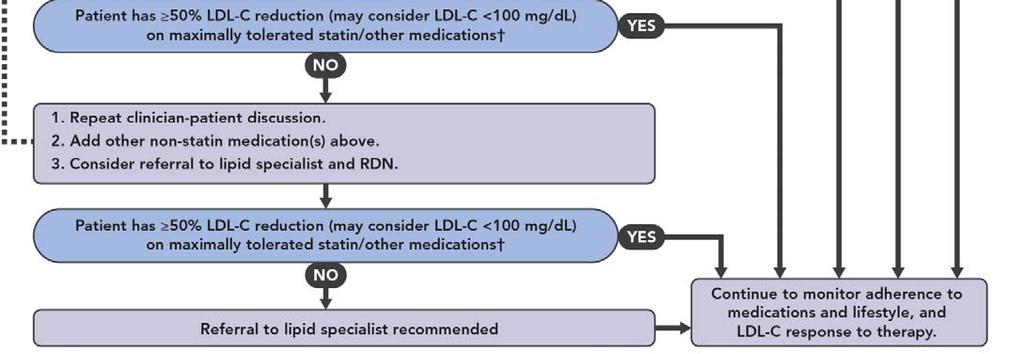
37 Case 1-63 yom w/ ASCVD PCSK9 inhibitor got approved. After 6 weeks on ezetimibe 10 mg plus rosuvastatin 20 mg plus PCSK9 inhibitor injection: Total cholesterol 80 HDL-C 36 LDL-C 25 Non-HDL-C 44 TG 170 LDL-C 188 mg/dl before therapy Now 50% reduction, <70 mg/dl What next?
38 Case 1-63 yom w/ ASCVD Patient is seen by cardiologist who told patient your LDL cholesterol is too low and suggested to stop ezetimibe. What do you tell the patient? Was the cardiologist right?
39 Case 1-63 yom w/ ASCVD
40 Lower is better
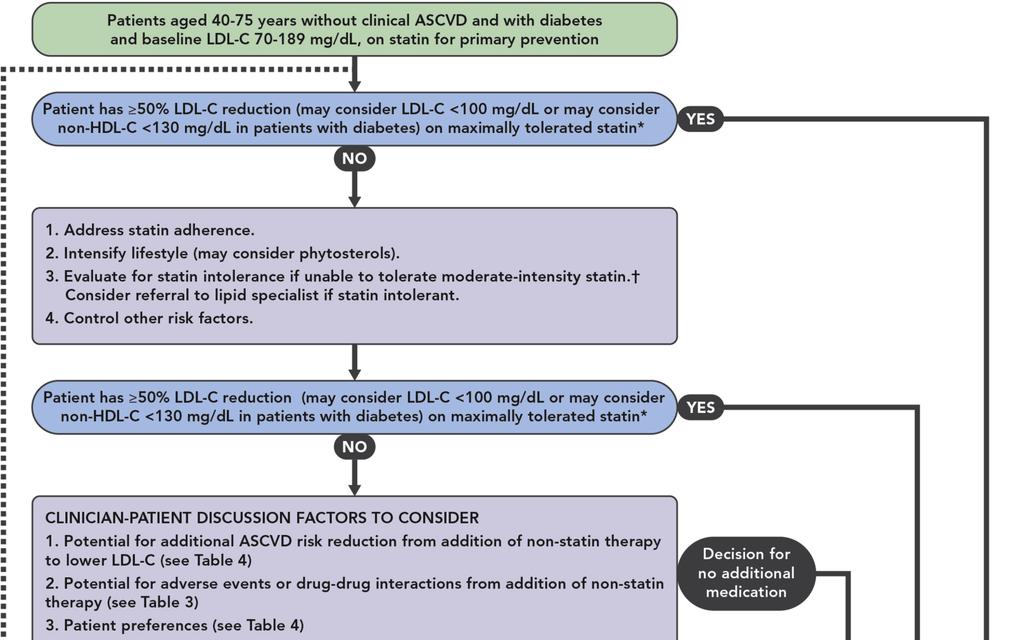
41 Case 2 52 yof w/ T2DM 52 yo female with type 2 DM, HTN, depression and chronic lower back pain. BMI of 32, not eating healthy, mostly sedentary. VS: 138/82 PE: obese female, trace BP edema, otherwise WNL Medications: ASA 81 mg daily Metformin 500 mg BID Lisinopril 20 mg daily Citalopram 20 mg daily Ibuprofen 600 mg q6h prn Hydrocodone/acetaminophen 5mg /325 mg q8h prn
42 Case 2 52 yof w/ T2DM CBC, TSH normal, A1C 6.7, CMP normal except mild AST elevation of 55 and egfr of 58. Total cholesterol 220 HDL-C 35 LDL-C 123 Non-HDL-C 185 TG 310 Based on 2013 ACC/AHA guidelines you advise starting patient on atorvastatin 80 mg (ASCVD risk 8.2%)
43 Case 2 52 yof w/ T2DM Patient calls your office in a week, reports severe muscle cramps in legs, she is attributing to statin. You advise to stop atorvastatin, wait 2 weeks for the pain to go away and try rosuvastatin 20 mg instead. Pt starts rosuvastatin and after a week calls your office that she has her leg cramps back. She tells you she never wants to be on any statin again.
44 Case 2 52 yof w/ T2DM What to do next? For statin intolerant patients consider referral to a lipid specialist according to the 2016 ACC ECDP
45 Case 2 52 yof w/ T2DM 3 mo follow up You use your magic skills convince the patient to try pravastatin 10 mg and she tolerates it. When you try to increase dose to 20 mg she develops muscle cramps. She goes back to 10 mg and is able to take it without problems. Total cholesterol 179 HDL-C 33 LDL-C 90 Non-HDL-C 146 TG 280 What next?
46
47 Case 2 52 yof w/ T2DM - 3 mo follow up On pravastatin 10 mg Total cholesterol 179 HDL-C 33 LDL-C 90 Non-HDL-C 146 TG 280 What next? LDL-C not reduced by 50%, LDL-C < 100 mg/dl Non-HDL-C above goal of < 130 mg/dl
48 Case 2 52 yof w/ T2DM - 3 mo follow up You convince patient to start ezetimibe in addition to her statin. Patient is tolerating it well, has no side effects. Total cholesterol 140 HDL-C 34 LDL-C 51 Non-HDL-C 106 TG 275 Success! LDL-C reduced by 50%, LDL-C < 100 mg/dl Non-HDL-C < 130 mg/dl Other options per ECDP: Bile acid
49 Case 2 52 yof w/ T2DM - 3 mo follow up Could we have used bile acid binding resins?
50 Case 2 52 yof w/ T2DM - 3 mo follow up Could we have used bile acid binding resins? Contraindicated if triglycerides > 300 mg/dl as paradoxically it may increase TG and cholesterol concentrations
51 Case 2 52 yof w/ T2DM - 3 mo follow up How about PCSK9 inhibitors?
52 Case 2 52 yof w/ T2DM - 3 mo follow up How about PCSK9 inhibitors? They will certainly work and lower LDL-C, they will very likely also lower ASCVD risk, but there is no clinical trial data of benefit in this group of patients at the moment, therefore there is no indication for its use.
53 Case 3-22 yof 22 year old college student presents to your office for a physical. No complaints. Not taking any meds. She has been playing basketball since HS, very active, eats healthy. Non smoker, drinks socially 1-2 x per month. IUD for birth control since 2 years. Both parents alive and healthy. HR: 56 RR: 12 BP 115/65 BMI 24.5 PE: athletic female, PE findings WNL Any labs you are willing to do?
54 Case 3-22 yof Detailed Family History: Both parents well and alive. Father age 42, Mother 43. Paternal grandfather died in Vietnam at young age Paternal grandmother alive, no mayor issues. Maternal grandfather was obese and alcoholic, died in his 50s, Maternal grandmother alive, has type 2 diabetes
55 Case 2-22 yof Will you check her lipids?

56 Case 2-22 yof

57 Case 2-22 yof What is meant by increased risk? Diabetes Previous personal history of CHD or non-coronary atherosclerosis Family history of cardiovascular disease before age 50 in male relatives or age 60 in female relatives. Tobacco use Hypertension Obesity (BMI 30)
58 American Heart Association Position (2014) If you are age 20 or older and have not been diagnosed with cardiovascular disease, the American Heart Association recommends having your cholesterol levels checked every four to six years as part of a cardiovascular risk assessment
59 Case 2-22 yof Should her pediatrician/family doctor check her lipids before age 21?
60 USPSTF 2016 Statement The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents 20 years or younger (Grade I statement)
61 American Academy of Pediatrics 2016 Recommendations for Preventive Pediatric Health Care Universal lipid screening between ages 9 and 11 following 2011 guidelines from the National Heart Lung and Blood Institute
62 National Lipid Association Recommendations (2016) Universal screening is recommended beginning at 10 years of age (range 9 to 11). If lipid levels are acceptable, then screening should be repeated every 5 years throughout life, with earlier screening prompted by change in ASCVD risk factors
63 Case 3-22 yof w/hefh Total cholesterol 378 HDL-C 65 LDL-C 295 Non-HDL-C 313 TG 90
64 Rule out 4Ds: Secondary Causes of Hypercholesterolemia Diet : Saturated or trans fats, weight gain, anorexia Drugs: Diuretics, cyclosporine, glucocorticoids, amiodarone Diseases: Biliary obstruction, nephrotic syndrome Disorders and altered states of metabolism: Hypothyroidism, obesity, pregnancy
65 Case 3-22 yof w/hefh Total cholesterol 378 HDL-C 65 LDL-C 295 Non-HDL-C 313 TG 90 Patient does not want to take a statin. She wants to become vegan and is willing to take any natural supplements you recommend.
66 Supplements able to lower LDL-C Red Rice Yeast Plant Sterols/Stanols Berberine Soluble fiber others
67 Case 3-22 yof w/hefh back in 3 months Total cholesterol 350 HDL-C 75 LDL-C 275 Non-HDL-C 313 TG 75 Patient frustrated being vegan and taking three expensive supplements. Decides to take atorvastatin 80 mg.
68 Case 3-22 yof w/hefh back in 3 months Total cholesterol 250 HDL-C 80 LDL-C 156 Non-HDL-C 170 TG 70 Taking atorvastatin 80 mg without any problems. Are we done?
69
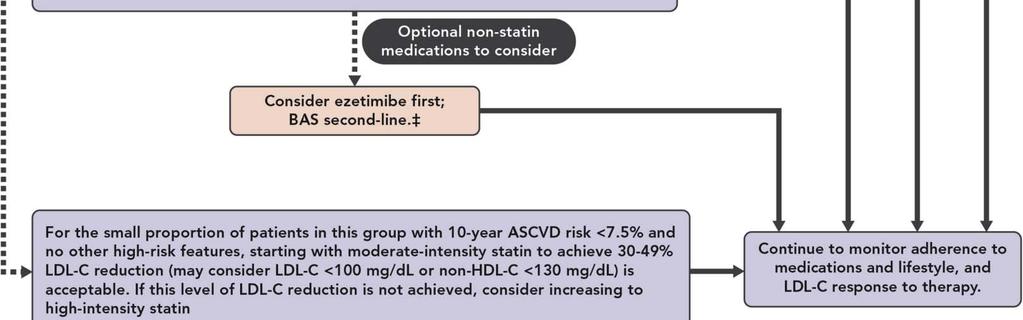
70 Case 3-22 yof w/hefh back in 3 months Total cholesterol 250 HDL-C 80 LDL-C 156 Non-HDL-C 170 TG 70 Taking atorvastatin 80 mg without any problems. Not achieving 50% LDL-C reduction, above goal of 100 mg/dl Rx of ezetimibe
71 Case 3-22 yof w/hefh back in another 3 months Total cholesterol 210 HDL-C 77 LDL-C 117 Non-HDL-C 133 TG 80 Taking atorvastatin 80 mg and ezetimibe 10 mg without any problems. Achieving 50% LDL-C reduction, but above goal of 100 mg/dl Are we done?
72 Case 3-22 yof w/hefh The committee also notes that for patients with baseline LDL-C 190 mg/dl and without other high-risk features or comorbidities, achievement of 50% reduction in LDL-C and LDL-C <130 mg/dl is a reasonable therapeutic outcome that may not require further intensification of therapy. Does she have other high risk features or comorbidities?
73 Case 3-22 yof w/hefh EKG and treadmill EKG normal (insurance did not authorize stress ECHO) Coronary calcium score 0.2 (above 99 th percentile for age/gender) Lipoprotein(a) 150 mg/dl HS-CRP 5.0
74 Case 3-22 yof w/hefh Rx of Welchol patient called in 2 weeks that she just cann not take it: too bulky and causing severe constipation. Taking atorvastatin 80 mg and ezetimibe 10 mg without any problems. Rx for PCSK9 inhibitors Finally approved
75 Case 3-22 yof w/hefh back in another 3 months Total cholesterol 145 HDL-C 75 LDL-C 52 Non-HDL-C 133 TG 90 Taking atorvastatin 80 mg, ezetimibe 10 mg and biweekly injections of PCSK9 inhibitors without any problems. Achieving 50% LDL-C reduction, at LDL-C goal of <100 mg/dl
76 Case 4 55 yom 65 yo male, smokes ½ PPD, not eating very healthy, msotly sedentary. Taking all medications. Negative family history of heart disease, BP 115/65 Medications: ASA 81 mg daily Losartan 25 mg
77 Case 4 55 yom Labs normal CMP, A1C, TSH, CBC, NT-BNP Total cholesterol 210 HDL-C 35 LDL-C 139 Non-HDL-C 175 TG 180 You advise smoking cessation, healthy lifestyle and starting atorvastatin 40 mg based on ASCVD risk of 14.3%
78 Case 4 55 yom In 1 week patient reports muscle pain with this dose. You rechallenge him with rosuvastatin 20 mg. Also muscle pain. Muscle pain with pravastatin 10 mg. You try atorvastatin 10 mg weekly, patient able to tolerate this dose. Total cholesterol 200 HDL-C 36 LDL-C 130 Non-HDL-C 164 TG 170 What next?
79
80 Case 4 55 yom Not achieving 50% LDL-C reduction, not achieving LDL-C < 100 mg/dl Rx of ezetimibe: too expensive Rx of colesevalam: too expensive Rx of cholestyramine: too bulky, patient unable to tolerate it. Anything else that can be done?
81 Cost- Effectiveness of PCSK9 Inhibitors Current price for 1 year of PCSK9 inhibitor therapy ~$14,000 Simulation model of US adults yo Adding PCSK9 inhibitor therapy to current statin regimens $423,000 per QALY pained compared with adding ezetimibe $565 billions increase of US health care costs over 5 years Price reduction needed to $4536 to reach the $100,000 QALY threshold JAMA 2016;316(7):
82
83
84
85
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy
 PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
 2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors
 Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Drug Prior Authorization Guideline PCSK9 Inhibitors -
 Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
HYPERCHOLESTEROLEMIA
 UPDATES ON HYPERCHOLESTEROLEMIA WITH EMPHASIS ON PCSK9 INHIBITORS July, 2018 Chicago by Ernesto L. Chua, MD, FACC, FACP, FPCP Board Certified in Internal Medicine Board Certified in Cardiology COL, USAF,
UPDATES ON HYPERCHOLESTEROLEMIA WITH EMPHASIS ON PCSK9 INHIBITORS July, 2018 Chicago by Ernesto L. Chua, MD, FACC, FACP, FPCP Board Certified in Internal Medicine Board Certified in Cardiology COL, USAF,
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
2017 Update in Internal Medicine: Clinical Dyslipidemia Update
 2017 Update in Internal Medicine: Clinical Dyslipidemia Update Erin E. Kershaw, M.D. Chief, Division of Endocrinology Associate Professor of Medicine Certified in Endocrinology, Diabetes, and Metabolism
2017 Update in Internal Medicine: Clinical Dyslipidemia Update Erin E. Kershaw, M.D. Chief, Division of Endocrinology Associate Professor of Medicine Certified in Endocrinology, Diabetes, and Metabolism
Reducing Cardiovascular Risk Through Non-Statins. Kim K. Birtcher, PharmD Joseph Saseen, PharmD
 Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Deep Dive into Contemporary Cholesterol Management. Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City
 Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Joshua Shepherd PA-C, MMS, MT (ASCP)
") Joshua Shepherd PA-C, MMS, MT (ASCP) None What is Cholesterol? Why cholesterol is it important? Review the National Cholesterol Education Programs guidelines (NCEP-ATPIII) Discuss New guidelines from the
Joshua Shepherd PA-C, MMS, MT (ASCP) None What is Cholesterol? Why cholesterol is it important? Review the National Cholesterol Education Programs guidelines (NCEP-ATPIII) Discuss New guidelines from the
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Clinical Policy: Evolocumab (Repatha) Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis?
 Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Patient Lists. Epic ABOUT THIS GUIDE INDICATIONS AND USAGE IMPORTANT SAFETY INFORMATION. Please see accompanying full Prescribing Information
 ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Lists in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Lists in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Controversies in Cardiac Pharmacology
 Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Controversies in Cardiac Pharmacology Thomas D. Conley, MD FACC FSCAI Disclosures I have no relevant relationships with commercial interests to disclose. 1 Doc, do I really need to take all these medicines?
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus
 Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
Isn't Xstatin 10mg good enough for the control of lipids for my patient? Do we need more?
 Isn't Xstatin 10mg good enough for the control of lipids for my patient? Do we need more? Singhealth GP CME Symposium 2018 ~ Keep Well, Age Well Pan Pacific Hotel, Singapore 12 May 2018 Dr Farhad Fakhrudin
Isn't Xstatin 10mg good enough for the control of lipids for my patient? Do we need more? Singhealth GP CME Symposium 2018 ~ Keep Well, Age Well Pan Pacific Hotel, Singapore 12 May 2018 Dr Farhad Fakhrudin
Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary
 Inhibitors Prior Authorization with Quantity Limit Program Summary") Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization
Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization with Quantity Limit Program Summary Proprotein Convertase Subtilisin/Kexin type 9(PCSK9) Inhibitors Prior Authorization
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
ADMINISTRATIVE POLICY AND PROCEDURE
 ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
Patient Lists. Allscripts Professional ABOUT THIS GUIDE INDICATIONS AND USAGE IMPORTANT SAFETY INFORMATION
 ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Lists in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
ABOUT THIS GUIDE This Guide provides a high-level overview of Patient Lists in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for PRALUENT
PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia
 : 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
: 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
Pharmacy Management Drug Policy
 SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Patient List Inquiries
 ABOUT THIS GUIDE This Guide provides a high-level overview of Patient List Inquiries in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for
ABOUT THIS GUIDE This Guide provides a high-level overview of Patient List Inquiries in and how they can be used to help identify clinically appropriate and approvable patients who may be candidates for
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
REPATHA (PCSK9 INHIBITORS)
") REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as