Introduction Hyperlipidemia hyperlipoproteinemia Primary hyperlipidemia (Familial) Secondary hyperlipidemia (Acquired)
|
|
|
- Daniela Lawrence
- 6 years ago
- Views:
Transcription
1
2 Introduction Hyperlipidemia, or hyperlipoproteinemia, is the condition of abnormally elevated levels of any or all lipids and/or lipoproteins in the blood. Hyperlipidemias are divided in primary and secondary subtypes. Primary hyperlipidemia (Familial) is usually due to genetic causes (such as a mutation in a receptor protein), while Secondary hyperlipidemia (Acquired) arises due to other underlying causes such as diabetes mellitus, alcoholism, nephrotic syndrome, chronic renal failure, administration of drug. Also, hyperlipidemia may be idiopathic, that is, without known cause. Lipid and lipoprotein abnormalities are common in the general population, and are regarded as a modifiable risk factor for cardiovascular disease due to their influence on atherosclerosis. In addition, some forms may predispose to acute pancreatitis.
3 Classification Hyperlipidemias may also be classified directly into which types of lipids are elevated, that is hypercholesterolemia, hypertriglyceridemia or both in combined hyperlipidemia. Elevated levels of lipoproteins may also be classified as a form of hyperlipidemia.
4
5 Lipoprotein Metabolism Lipids originate from two sources: Exogenous lipids, ingested and processed in the intestine. Endogenous lipids, synthesized in the liver. Over 93% of the fat that is consumed in the diet is in the form of triglycerides (TG). Dietary cholesterol and triglycerides are packaged into chylomicrons in the intestine, before passing into the blood stream via lymphatics. The liver synthesizes triglycerides and cholesterol, and packages them as VLDLs before releasing them into the blood.


6 Excess dietary carbohydrates are converted into triglycerides and also stored in adipose tissue.

7 Dietary intake supplies only about 20 25% of the cholesterol needed everyday to build cell membranes,

8 The other 75 80% of our daily need for cholesterol is synthesized in the liver. Saturated fats raise LDL cholesterol by decreasing the synthesis of LDL receptors.

9 The overall results are about the same, no matter which defect you consider, cholesterol is not removed from the circulation
10 Lipoprotein Metabolism LIPIDS, including LESTEROL () and TRIGLYCERIDES (TG), are transported in the plasma as lipoproteins, of which there are four classes: Chylomicrons transport TG and from the GIT to the tissues, where they are split by lipoprotein lipase (LPL), releasing free fatty acids. There are taken up in capillary of muscles and adipose tissue. Chylomicron remnants are taken up in the liver for disposal. Very low density lipoproteins (VLDL), which transport and newly synthetised TG to the tissues. Low density lipoproteins (LDL) with a large component of, some of which is taken up by the tissues and some by the liver, by endocytosis via specific LDL receptors High density lipoproteins (HDL): are also secreted from the liver and intestine, have the task of preventing lipid accumulation, absorb derived from cell breakdown in tissues and transfer it to VLDL and LDL
11 Lipoprotein Metabolism There are two different pathways for exogenous and endogenous lipids: THE EXOGENOUS PATHWAY: + TG absorbed from the GIT are transported in the lymph and than in the plasma as CHYLOMICRONS to capillaries in muscle and adipose tissues. Here, the core TG are hydrolysed by lipoprotein lipase, and the tissues take up the resulting FREE FATTY ACIDS is liberated within the liver cells and may be stored, oxidised to bile acids or secreted in the bile unaltered Alternatively it may enter the endogenous pathway of lipid transport in VLDL
12 Lipoprotein Metabolism EXOGENOUS PATHWAY ENDOGENOUS PATHWAY may be stored oxidised to bile acids secreted in the bile unaltered
13 ENDOGENOUS PATHWAY for lipids EXOGENOUS PATHWAY for lipids Fig.1a HEPATOCYTE GIT bile acids Bile duct bile acids Fat + + fatty acids ENDOGENOUS PARTHWAY chylomicr remn TG chylomicr TG Peripheral tissues Fatty acids (According to Rang, Dale 1999)

14 Lipoprotein Metabolism THE ENDOGENOUS PATHWAY: 1. and newly synthetised TG are transported from the liver as VLDL to muscle and adipose tissue, there TG are hydrolysed and the resulting FATTY ACIDS enter the tissues 2. The lipoprotein particles become smaller and progressively more dense and ultimetaly turn into LDL, which provides the source of for incorporation into cell membranes, for synthesis of steroids, and bile acids 3. While most of the resulting LDLs are taken up by the liver cells by endocytosis via LDL receptors that recognise LDL apolipoproteins for disposal, some circulate and distribute cholesterol to the rest of the body tissues. 4. can return to plasma from the tissues in HDL particles and the resulting cholesteryl esters are subsequently transferred to VLDL or LDL
15 ENDOGENOUS PATHWAY for lipids EXOGENOUS PATHWAY for lipids Fig.1b HEPATOCYTE GIT ACoA MVA bile acids Bile duct bile acids 3 LDL receptors 4 HDL LDL VLDL TG 2 1 lipase from cells Uptake of Fatty acids Peripheral tissues (According to Rang, Dale 1999)
16 Dyslipidemia The normal range of plasma total concentration < 6.5 mmol/l. There are smooth gradations of increased risk with elevated LDL-C conc, and with reduced HDL-C conc. Elevated concentrations of lipid (hyperlipidemia) can lead to the development of atherosclerosis and CAD. VLDLs and LDLs are atherogenic lipoproteins, whereas HDL concentrations are inversely related to the incidence of CAD. Hence, treatments for hyperlipidemia aim to reduce LDL levels and raise HDL levels.
17 Lipid-lowering drugs Drug therapy to lower plasma lipids is only one approach to treatment and is used in addition to dietary management and correction of other modifiable cardiovascular risk factors Several drugs are used to decrease plasma LDL-C
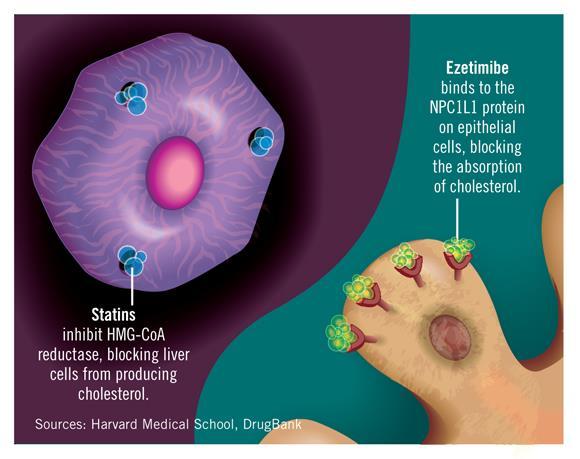
18 Pharmacotherapeutic options in hyperlipidemia I-Agents Targeting Endogenous Cholesterol: A. Statins B. Fibrates C. Nicotinic acid II-Agents Targeting Exogenous Cholesterol A. Cholesterol Uptake Inhibitors, e.g. ezetemibe B. Bile acid binding resins, e.g. colestipol & cholestyramine
19 ENDOGENOUS PATHWAY for lipids EXOGENOUS PATHWAY for lipids GIT Fig.1c HEPATOCYTE GIT STATINS ACoA STATINS FIBRATES MVA bile acids Bile duct bile acids FIBRATES LDL receptors VLDL TG FIBRATES Chylomikr remn TG v.portae Chylomikr RESINS fat + + fatty acids HDL LDL lipase TG from cells Uptake of Fatty acids Fatty acids Peripheral tissues (According to Rang, Dale 1999)
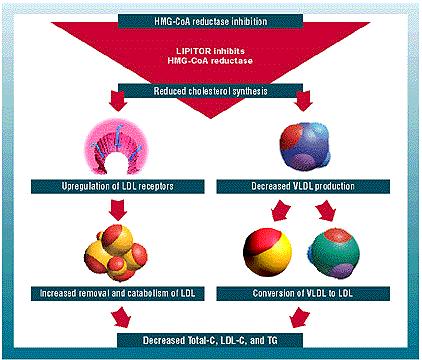
20 Statins Drugs: Simvastatin, atorvastatin, mevastatin, lovastatin, pravastatin and their derivatives Pharmacological effects: Apparently decrease plasma TC and LDL-C HMG-CoA (3-hydroxy-3-methylglutaryl-coenzyme A) reductase inhibitors. The reductase catalyses the conversion of HMG-CoA to mevalonic acid Several studies demonstrated positive effects on morbidity and mortality
21
22
23 Statins Pharmacokinetics: well absorbed when given orally They are subjected to extensive first-pass metabolism by the liver. More than 95% of most of these drugs are bound to plasma proteins. All statins are taken orally at bedtime because of diurnal rhythm of cholesterol synthesis, except atorvastatin taken at any time because of its long half-life (14 hours). At the peak of the rhythm (between midnight and 3 a.m.) MVA concentrations were 3-5 times greater than (between 9 a.m. and noon).
24 Adverse effects: Statins - Nearly 10% patients suffer from mild gastrointestinal disturbances, insomnia, headache and rash - More serious adverse effects are rare but include Hepatotoxicity (increased serum transaminase), myositis (rhabdomyolysis) and angio-oedema - Myopathy (increased creatine kinase) especially when combined with: other lipid lowering drugs: i) Fibrates. ii) Niacin. other drugs that are metabolized by 3A4 isoform of cytochrome P450 e.g.: erythromycin, cyclosporine, verapamil, ketoconazole. Note: liver transaminases and CK must be regularly measured during therapy with statins
; swollen, tender muscles of the thighs, calves, and")
25 The most common symptoms of rhabdomyolysis include: dark urine (typically brown); swollen, tender muscles of the thighs, calves, and lower back.
26 Statins Contraindications 1. Pregnancy & lactation (Cholesterol is important for normal development, and it is possible that statins could cause serious problems). The effects of high cholesterol do not cause problems for many years or even decades. Therefore, if a woman does not take her statin or other cholesterol medications during breastfeeding, it will likely have only a minimal impact on her long-term risks. Therefore, it is best to wait until you have weaned your child before starting or resuming a statin medication 2. Active liver diseases.
27 Statins Drug interactions Potentiate the action of oral anticoagulant and antidiabetic drugs (displacement from plasma protein binding sites). Clinical uses Secondary prevention of myocardial infarction and stroke Primary prevention of arterial disease
28 Fibric Acid Derivatives [Fibrates] Drugs: Clofibrate, gemfibrozil, bezafibrate, fenofibrate, ciprofibrate Pharmacological effects and mechanisms: to decrease TG, VLDL and to increase HDL Stimulate the beta-oxidative degradation of fatty acids Liberate free fatty acids for storage in fat or for metabolism in striated muscle Increase the activity of lipoprotein lipase, hence increasing hydrolysis of triglyceride in chylomicrons and VLDL particles reduce hepatic VLDL production and increase hepatic LDL uptake
29 Fibric Acid Derivatives [Fibrates] Adverse effects: Mild GIT symptoms, skin rashes, decrease in white blood count, hepatic dysfunction In patients with renal impairment myositis (rhabdomyolysis) myoglobulinuria, acute renal failure [Fibrates should be avoided in such patients and also in alcoholics]
30 Fibric Acid Derivatives [Fibrates] Drug interactions: 1. Increased risk of myopathy when combined with statins. 2. Displace drugs from plasma proteins (e.g. oral anticoagulants and oral hypoglycemic drugs). Contraindications: 1- Patients with impaired renal functions. 2- Pregnant or nursing women. 3-Preexisting gall bladder disease.
31 Fibric Acid Derivatives [Fibrates] Clinical uses: Mixed dyslipidemia (i.e. raised serum TG and ) Patients with low HDL and high risk of atheromatous disease (often type 2 diabetic patients) Patients with severe treatment- resistant dyslipidemia (combination with other lipidlowering drugs)

32 NICOTINIC ACID (NIACIN) Mechanism of action: 1. In adipose tissue: it binds to adipose nicotinic acid receptors, this will lead to decrease in free fatty acids mobilization from adipocytes to the liver resulting in TG and thus VLDL synthesis. 2. In liver: niacin inhibits hepatocyte diacylglycerol acyltransferase-2, a key enzyme for TG synthesis. Thus, it decreases VLDL production. 3. In plasma: it increases LPL activity that increases clearance of VLDL & chylomicron.
33 Nicotinic acid (Niacin) Adverse effects: Pruritus, rashes, flush acanthosis: The niacin flush results from the stimulation of prostaglandins D(2) and E(2). This flush is avoided by low dose aspirin 325 mg ½ h before niacin. Reactivation of peptic ulcer (because it stimulates histamine release resulting in increased gastric motility and acid production. Hepatic dysfunction Hyperglycemia which is believed to be caused by an increase in insulin resistance. Palpitations, Nausea and abdominal discomfort Hyperuricaemia
34 Nicotinic acid (Niacin) Contraindications 1. Gout. 2. Peptic ulcer. 3. Hepatotoxicity. 4. Diabetes mellitus. Therapeutic Uses Niacin is the most effective medication for increasing HDL cholesterol levels and it has positive effects on the complete lipid profile. Mixed dyslipidemias.
35 Ezetimibe Mechanism of action: Impairs dietary and biliary cholesterol absorption at the brush border of the intestines without affecting fat-soluble vitamins. Reducing the pool of cholesterol absorbed from the diet results in a reduced pool of cholesterol available to the liver. The liver in turn will upregulate the LDL receptor, trapping more LDL particles from the blood and result in a fall in measured LDL cholesterol. Pharmacokinetics Elimination half-life of ezetimibe approx. 22 h Long half-life: 1. Permits once-daily dosing 2. May improve compliance
36
37 Bile acid binding resins Anion exchange resins Drugs : Cholestyramine, Colestipol Pharmacological effects: TC/LDL-C HDL MOA: When resins are given orally, they are not absorbed, they sequester bile acids in the GIT, prevent their reabsorption and enterohepatic recirculation. The r e s u l t is: decreased absorption of exogenous and increased metabolism of endogenous into bile acids in the liver increased expression of LDL receptors on liver cells increased removal of LDL from the blood reduced concentration of LDL-C in plasma
38 Bile acid binding resins Adverse effects: GIT symptoms: nausea, constipation or diarrhea abdominal bloating, Interfere with the absorption of fat-soluble vitamins and drugs (chlorothiazide, digoxin, warfarin) : These drugs should be given at least 1 hour before or 4-6 hours after a resin Use of these agents has declined since the introduction of the statins. They require very large doses and need to be taken with lots of water. C l i n i c a l u s e s: Heterozygous familial hypercholesterolemia: Hypercholesterolemia when a statin is contraindicated Uses unrelated to atherosclerosis, including: pruritus
39 Others Fish oil (rich in highly unsaturated fatty acids) to decrease TG, VLDL, LDL-C and to increase HDL-C Reduce plasma TG but increase ( is more strongly associated wih coronary artery disease) The effects on cardiac morbidity or mortality is unproven (although there is epidemiological evidence that eating fish regularly does reduce ischemic heart disease)

40
Antihyperlipidemic Drugs
 Antihyperlipidemic Drugs Lipid disorders: Disorders of lipid metabolism are manifest by elevation of the plasma concentrations of the various lipid and lipoprotein fractions (total and LDL cholesterol,
Antihyperlipidemic Drugs Lipid disorders: Disorders of lipid metabolism are manifest by elevation of the plasma concentrations of the various lipid and lipoprotein fractions (total and LDL cholesterol,
Anti Hyperlipidemic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anti Hyperlipidemic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Lipoproteins Macromolecular complexes in the blood that transport lipids Apolipoproteins
Anti Hyperlipidemic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Lipoproteins Macromolecular complexes in the blood that transport lipids Apolipoproteins
ANTIHYPERLIPIDEMIA. Darmawan,dr.,M.Kes,Sp.PD
 ANTIHYPERLIPIDEMIA Darmawan,dr.,M.Kes,Sp.PD Plasma lipids consist mostly of lipoproteins Spherical complexes of lipids and specific proteins (apolipoproteins). The clinically important lipoproteins, listed
ANTIHYPERLIPIDEMIA Darmawan,dr.,M.Kes,Sp.PD Plasma lipids consist mostly of lipoproteins Spherical complexes of lipids and specific proteins (apolipoproteins). The clinically important lipoproteins, listed
Antihyperlipidemic drugs
 Antihyperlipidemic drugs The clinically important lipoproteins are LDL low density lipoprotein, VLDL very low density lipoprotein, HDL high density lipoprotein. Hyperlipidemia may caused 1. by individual
Antihyperlipidemic drugs The clinically important lipoproteins are LDL low density lipoprotein, VLDL very low density lipoprotein, HDL high density lipoprotein. Hyperlipidemia may caused 1. by individual
DYSLIPIDEMIA PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
Antihyperlipidemic Drugs
 Antihyperlipidemic Drugs Hyperlipidemias. Hyperlipoproteinemias. Hyperlipemia. Hypercholestrolemia. Direct relationship with acute pancreatitis and atherosclerosis Structure Lipoprotein Particles Types
Antihyperlipidemic Drugs Hyperlipidemias. Hyperlipoproteinemias. Hyperlipemia. Hypercholestrolemia. Direct relationship with acute pancreatitis and atherosclerosis Structure Lipoprotein Particles Types
Lipid Lowering Drugs. Dr. Alia Shatanawi
 Lipid Lowering Drugs Dr. Alia Shatanawi Atherosclerosis A form of arteriosclerosis characterized by the deposition of atheromatous plaques containing cholesterol and lipids on the innermost layer of the
Lipid Lowering Drugs Dr. Alia Shatanawi Atherosclerosis A form of arteriosclerosis characterized by the deposition of atheromatous plaques containing cholesterol and lipids on the innermost layer of the
Hyperlipidemia. Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi
 Hyperlipidemia Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi Outline The story of lipids Definition of hyperlipidemia Classification of hyperlipidemia Causes of hyperlipidemia
Hyperlipidemia Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi Outline The story of lipids Definition of hyperlipidemia Classification of hyperlipidemia Causes of hyperlipidemia
Podcast (Video Recorded Lecture Series): Lipoprotein Metabolism and Lipid Therapy for the USMLE Step One Exam
: Lipoprotein Metabolism and Lipid Therapy for the USMLE Step One Exam") Podcast (Video Recorded Lecture Series): Lipoprotein Metabolism and Lipid Therapy for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com Podcast (Video Recorded
Podcast (Video Recorded Lecture Series): Lipoprotein Metabolism and Lipid Therapy for the USMLE Step One Exam Howard J. Sachs, MD www.12daysinmarch.com Email: Howard@12daysinmarch.com Podcast (Video Recorded
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Drug regulation of serum lipids
 Drug regulation of serum lipids Foundations of Biomedical Science MEDS90001 Dr Michelle Hansen Pharmacology & Therapeutics mjhansen@unimelb.edu.au References Katzung, Basic & Clinical Pharmacology Ch 35
Drug regulation of serum lipids Foundations of Biomedical Science MEDS90001 Dr Michelle Hansen Pharmacology & Therapeutics mjhansen@unimelb.edu.au References Katzung, Basic & Clinical Pharmacology Ch 35
CLINICAL IMPORTANCE OF LIPOPROTEINS
 25 Hyperlipidemias CLINICAL IMPORTANCE OF LIPOPROTEINS Raised levels of low-density lipoprotein (LDL) cholesterol and low levels of high density lipoprotein (HDL) cholesterol are independent risk factor
25 Hyperlipidemias CLINICAL IMPORTANCE OF LIPOPROTEINS Raised levels of low-density lipoprotein (LDL) cholesterol and low levels of high density lipoprotein (HDL) cholesterol are independent risk factor
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
A Review: Atherosclerosis & its treatment
 73 Review Article A Review: Atherosclerosis & its treatment Yogesh K. Patil* Department of Pharmacology, Shree Mahavir Institute of Pharmacy, Nashik, Maharashtra, India *yogesh_kpatil85@yahoo.co.in ABSTRACT
73 Review Article A Review: Atherosclerosis & its treatment Yogesh K. Patil* Department of Pharmacology, Shree Mahavir Institute of Pharmacy, Nashik, Maharashtra, India *yogesh_kpatil85@yahoo.co.in ABSTRACT
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Imbalances in lipid components
 Drugs for Dyslipidemia Vivien Gam, Pharm.D. 1 Dyslipidemia Imbalances in lipid components High total cholesterol High LDL cholesterol Low HDL cholesterol High triglycerides Significant risk factor for
Drugs for Dyslipidemia Vivien Gam, Pharm.D. 1 Dyslipidemia Imbalances in lipid components High total cholesterol High LDL cholesterol Low HDL cholesterol High triglycerides Significant risk factor for
Lipids digestion and absorption, Biochemistry II
 Lipids digestion and absorption, blood plasma lipids, lipoproteins Biochemistry II Lecture 1 2008 (J.S.) Triacylglycerols (as well as free fatty acids and both free and esterified cholesterol) are very
Lipids digestion and absorption, blood plasma lipids, lipoproteins Biochemistry II Lecture 1 2008 (J.S.) Triacylglycerols (as well as free fatty acids and both free and esterified cholesterol) are very
Unit IV Problem 3 Biochemistry: Cholesterol Metabolism and Lipoproteins
 Unit IV Problem 3 Biochemistry: Cholesterol Metabolism and Lipoproteins - Cholesterol: It is a sterol which is found in all eukaryotic cells and contains an oxygen (as a hydroxyl group OH) on Carbon number
Unit IV Problem 3 Biochemistry: Cholesterol Metabolism and Lipoproteins - Cholesterol: It is a sterol which is found in all eukaryotic cells and contains an oxygen (as a hydroxyl group OH) on Carbon number
In May 2001, the National Cholesterol. Effective Management of Patients With Dyslipidemia REPORT. Robert J. Lipsy, PharmD
 REPORT Effective Management of Patients With Dyslipidemia Robert J. Lipsy, PharmD Abstract Coronary heart disease (CHD) is the leading cause of morbidity and mortality in the United States. A direct relationship
REPORT Effective Management of Patients With Dyslipidemia Robert J. Lipsy, PharmD Abstract Coronary heart disease (CHD) is the leading cause of morbidity and mortality in the United States. A direct relationship
Hypertriglyceridemia. Ara Metjian, M.D. Resident s Report 20 December 2002
 Hypertriglyceridemia Ara Metjian, M.D. Resident s Report 20 December 2002 Review of Lipids Chylomicrons (CM): Dietary lipids absorbed through the GI tract are assembled intracellularly into CM. Very Low
Hypertriglyceridemia Ara Metjian, M.D. Resident s Report 20 December 2002 Review of Lipids Chylomicrons (CM): Dietary lipids absorbed through the GI tract are assembled intracellularly into CM. Very Low
Antihyperlipidemic Drugs Munir Gharaibeh, MD, PhD, MHPE
 Antihyperlipidemic Drgs Mnir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan November, 2017 Antihyperlipidemic Drgs Hyperlipidemias. Hyperlipoproteinemias. Hyperlipemia. Dyslipidemias
Antihyperlipidemic Drgs Mnir Gharaibeh, MD, PhD, MHPE School of Medicine, The University of Jordan November, 2017 Antihyperlipidemic Drgs Hyperlipidemias. Hyperlipoproteinemias. Hyperlipemia. Dyslipidemias
Rosuvastatin 5 mg, 10 mg and 20 mg Tablet
 Rosuvastatin 5 mg, 10 mg and 20 mg Tablet Description is a preparation of Rosuvastatin. Rosuvastatin is a member of the drug class of statins, used in combination with exercise, diet, and weight-loss to
Rosuvastatin 5 mg, 10 mg and 20 mg Tablet Description is a preparation of Rosuvastatin. Rosuvastatin is a member of the drug class of statins, used in combination with exercise, diet, and weight-loss to
Copy right protected Page 1
 CHOLESTEROL and TGs LOWERING DRUGS Introduction: Fat (lipids) are combinations (esters) of fatty acids plus an alcohol. The two main fats in the body are triglycerides (TGs) and cholesterol Triglycerides
CHOLESTEROL and TGs LOWERING DRUGS Introduction: Fat (lipids) are combinations (esters) of fatty acids plus an alcohol. The two main fats in the body are triglycerides (TGs) and cholesterol Triglycerides
ANTI-HYPERLIPIDEMIC AGENTS AND NSAIDS LECTURE 6
 ANTI-HYPERLIPIDEMIC AGENTS AND NSAIDS LECTURE 6 HYPERLIPIDEMIA Cholesterol Total cholesterol LDL cholesterol HDL cholesterol men women Triglycerides
ANTI-HYPERLIPIDEMIC AGENTS AND NSAIDS LECTURE 6 HYPERLIPIDEMIA Cholesterol Total cholesterol LDL cholesterol HDL cholesterol men women Triglycerides
Cholesterol metabolism. Function Biosynthesis Transport in the organism Hypercholesterolemia
 Cholesterol metabolism Function Biosynthesis Transport in the organism Hypercholesterolemia - component of all cell membranes - precursor of bile acids steroid hormones vitamin D Cholesterol Sources: dietary
Cholesterol metabolism Function Biosynthesis Transport in the organism Hypercholesterolemia - component of all cell membranes - precursor of bile acids steroid hormones vitamin D Cholesterol Sources: dietary
Dyslipidemia. (Med-341)
") Dyslipidemia (Med-341) Anwar A Jammah, MD, FRCPC, FACP, CCD, ECNU. Associate Professor of Medicine Consultant Medicine, Endocrinology, Thyroid Oncology Department of Medicine, King Saud University The
Dyslipidemia (Med-341) Anwar A Jammah, MD, FRCPC, FACP, CCD, ECNU. Associate Professor of Medicine Consultant Medicine, Endocrinology, Thyroid Oncology Department of Medicine, King Saud University The
Plasma lipoproteins & atherosclerosis by. Prof.Dr. Maha M. Sallam
 Biochemistry Department Plasma lipoproteins & atherosclerosis by Prof.Dr. Maha M. Sallam 1 1. Recognize structures,types and role of lipoproteins in blood (Chylomicrons, VLDL, LDL and HDL). 2. Explain
Biochemistry Department Plasma lipoproteins & atherosclerosis by Prof.Dr. Maha M. Sallam 1 1. Recognize structures,types and role of lipoproteins in blood (Chylomicrons, VLDL, LDL and HDL). 2. Explain
CHOLESTAGEL 625 mg Genzyme
 CHOLESTAGEL 625 mg Genzyme 1. NAME OF THE MEDICINAL PRODUCT Cholestagel 625 mg film-coated tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains 625 mg colesevelam hydrochloride (hereafter
CHOLESTAGEL 625 mg Genzyme 1. NAME OF THE MEDICINAL PRODUCT Cholestagel 625 mg film-coated tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains 625 mg colesevelam hydrochloride (hereafter
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
VI.2 Elements for a public summary. VI.2.1 Overview of disease epidemiology
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology This medicine is used to lower levels of total cholesterol, LDL cholesterol ( bad cholesterol), and fatty substances called triglycerides
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology This medicine is used to lower levels of total cholesterol, LDL cholesterol ( bad cholesterol), and fatty substances called triglycerides
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Cholesterol. Medicines To Help You
 Medicines To Help You Cholesterol Use this guide to help you talk to your doctor, pharmacist, or nurse about your cholesterol medicines. The guide lists all of the FDA-approved products now available to
Medicines To Help You Cholesterol Use this guide to help you talk to your doctor, pharmacist, or nurse about your cholesterol medicines. The guide lists all of the FDA-approved products now available to
Drugs for Dyslipidemias
 Drugs for Dyslipidemias HMG CoA reductase inhibitors (statins): atorvastatin, lovastatin, pravastatin, simvastatin Bile acid-binding resins: cholestyramine, colestipol, colesevelam Fibric acid derivatives
Drugs for Dyslipidemias HMG CoA reductase inhibitors (statins): atorvastatin, lovastatin, pravastatin, simvastatin Bile acid-binding resins: cholestyramine, colestipol, colesevelam Fibric acid derivatives
Topic 11. Coronary Artery Disease
 Topic 11 Coronary Artery Disease Lipid metabolism http://news.bbc.co.uk/2/hi/health/7372495.stm Sterol Metabolism and Coronary Artery Disease Big Picture: Exogenous Cholesterol and Fat Metabolism Fats-Triglycerides
Topic 11 Coronary Artery Disease Lipid metabolism http://news.bbc.co.uk/2/hi/health/7372495.stm Sterol Metabolism and Coronary Artery Disease Big Picture: Exogenous Cholesterol and Fat Metabolism Fats-Triglycerides
ANSC/NUTR 618 LIPIDS & LIPID METABOLISM Lipoprotein Metabolism
 ANSC/NUTR 618 LIPIDS & LIPID METABOLISM Lipoprotein Metabolism I. Chylomicrons (exogenous pathway) A. 83% triacylglycerol, 2% protein, 8% cholesterol plus cholesterol esters, 7% phospholipid (esp. phosphatidylcholine)
ANSC/NUTR 618 LIPIDS & LIPID METABOLISM Lipoprotein Metabolism I. Chylomicrons (exogenous pathway) A. 83% triacylglycerol, 2% protein, 8% cholesterol plus cholesterol esters, 7% phospholipid (esp. phosphatidylcholine)
ANSC/NUTR 618 LIPIDS & LIPID METABOLISM The LDL Receptor, LDL Uptake, and the Free Cholesterol Pool
 ANSC/NUTR 618 LIPIDS & LIPID METABOLISM The, LDL Uptake, and the Free Cholesterol Pool I. Michael Brown and Joseph Goldstein A. Studied families with familial hypercholesterolemia. B. Defined the relationship
ANSC/NUTR 618 LIPIDS & LIPID METABOLISM The, LDL Uptake, and the Free Cholesterol Pool I. Michael Brown and Joseph Goldstein A. Studied families with familial hypercholesterolemia. B. Defined the relationship
PATIENT INFORMATION. Medicine To Treat: C ardiac Diseases. Lipid-Lowering Medicines. Statins Fibrates Fat Binding Agents Nicotinic Acid Group
 PATIENT INFORMATION Medicine To Treat: C ardiac Diseases Lipid-Lowering Medicines Statins Fibrates Fat Binding Agents Nicotinic Acid Group ABOUT YOUR MEDICINE Your doctor has just prescribed for you: Medicine
PATIENT INFORMATION Medicine To Treat: C ardiac Diseases Lipid-Lowering Medicines Statins Fibrates Fat Binding Agents Nicotinic Acid Group ABOUT YOUR MEDICINE Your doctor has just prescribed for you: Medicine
1Why lipids cannot be transported in blood alone? 2How we transport Fatty acids and steroid hormones?
 1Why lipids cannot be transported in blood alone? 2How we transport Fatty acids and steroid hormones? 3How are dietary lipids transported? 4How lipids synthesized in the liver are transported? 5 Lipoprotien
1Why lipids cannot be transported in blood alone? 2How we transport Fatty acids and steroid hormones? 3How are dietary lipids transported? 4How lipids synthesized in the liver are transported? 5 Lipoprotien
The new guidelines issued in PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice
 ... PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice Based on a presentation by Daniel J. Rader, MD Presentation Summary The guidelines recently released by the National Cholesterol
... PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice Based on a presentation by Daniel J. Rader, MD Presentation Summary The guidelines recently released by the National Cholesterol
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipids Board Review. Ira Goldberg, MD New York University School of Medicine. Which of the following is the best initial therapy choice?
 Lipids Board Review Ira Goldberg, MD New York University School of Medicine 1. A 22 year old male college student is referred for severe hypertriglyceridemia ( 1500 mg/dl [ 17.0 mmol/l]). He has a history
Lipids Board Review Ira Goldberg, MD New York University School of Medicine 1. A 22 year old male college student is referred for severe hypertriglyceridemia ( 1500 mg/dl [ 17.0 mmol/l]). He has a history
Lipoproteins Metabolism Reference: Campbell Biochemistry and Lippincott s Biochemistry
 Lipoproteins Metabolism Reference: Campbell Biochemistry and Lippincott s Biochemistry Learning Objectives 1. Define lipoproteins and explain the rationale of their formation in blood. 2. List different
Lipoproteins Metabolism Reference: Campbell Biochemistry and Lippincott s Biochemistry Learning Objectives 1. Define lipoproteins and explain the rationale of their formation in blood. 2. List different
Lipoproteins Metabolism
 Lipoproteins Metabolism LEARNING OBJECTIVES By the end of this Lecture, the student should be able to describe: What are Lipoproteins? Describe Lipoprotein Particles. Composition of Lipoproteins. The chemical
Lipoproteins Metabolism LEARNING OBJECTIVES By the end of this Lecture, the student should be able to describe: What are Lipoproteins? Describe Lipoprotein Particles. Composition of Lipoproteins. The chemical
Chapter VIII: Dr. Sameh Sarray Hlaoui
 Chapter VIII: Dr. Sameh Sarray Hlaoui Lipoproteins a Lipids are insoluble in plasma. In order to be transported they are combined with specific proteins to form lipoproteins: Clusters of proteins and lipids.
Chapter VIII: Dr. Sameh Sarray Hlaoui Lipoproteins a Lipids are insoluble in plasma. In order to be transported they are combined with specific proteins to form lipoproteins: Clusters of proteins and lipids.
Financial Disclosures
 1 Lipids in Type 2 Diabetes July 20, 2013 Abhimanyu Garg, M.D. Professor of Internal Medicine Chief, Division of Nutrition and Metabolic Diseases Distinguished Chair in Human Nutrition Research UT Southwestern
1 Lipids in Type 2 Diabetes July 20, 2013 Abhimanyu Garg, M.D. Professor of Internal Medicine Chief, Division of Nutrition and Metabolic Diseases Distinguished Chair in Human Nutrition Research UT Southwestern
Pathophysiology of Lipid Disorders
 Pathophysiology of Lipid Disorders Henry Ginsberg, M.D. Division of Preventive Medicine and Nutrition CHD in the United States CHD is the single largest killer of men and women 12 million have history
Pathophysiology of Lipid Disorders Henry Ginsberg, M.D. Division of Preventive Medicine and Nutrition CHD in the United States CHD is the single largest killer of men and women 12 million have history
CHM333 LECTURE 34: 11/30 12/2/09 FALL 2009 Professor Christine Hrycyna
 Lipid Metabolism β-oxidation FA Acetyl-CoA Triacylglycerols (TAGs) and glycogen are the two major forms of stored energy in vertebrates Glycogen can supply ATP for muscle contraction for less than an hour
Lipid Metabolism β-oxidation FA Acetyl-CoA Triacylglycerols (TAGs) and glycogen are the two major forms of stored energy in vertebrates Glycogen can supply ATP for muscle contraction for less than an hour
Dyslipidemia. Team Members: Laila Mathkour, Khalid Aleedan, Bayan Al-Mugheerha, Fatima AlTassan
 Dyslipidemia Objectives: Not given. Team Members: Laila Mathkour, Khalid Aleedan, Bayan Al-Mugheerha, Fatima AlTassan Team Leader: Amal Alshaibi Revised By: Yara Aldigi and Basel almeflh Resources: 435
Dyslipidemia Objectives: Not given. Team Members: Laila Mathkour, Khalid Aleedan, Bayan Al-Mugheerha, Fatima AlTassan Team Leader: Amal Alshaibi Revised By: Yara Aldigi and Basel almeflh Resources: 435
Classification. Etiology
 Dyslipidemia Dyslipidemia is the elevation of plasma cholesterol, triglycerides (TGs), or both, or a low high-density lipoprotein level that contributes to the development of atherosclerosis. Causes may
Dyslipidemia Dyslipidemia is the elevation of plasma cholesterol, triglycerides (TGs), or both, or a low high-density lipoprotein level that contributes to the development of atherosclerosis. Causes may
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Cholesterol and its transport. Alice Skoumalová
 Cholesterol and its transport Alice Skoumalová 27 carbons Cholesterol - structure Cholesterol importance A stabilizing component of cell membranes A precursor of bile salts A precursor of steroid hormones
Cholesterol and its transport Alice Skoumalová 27 carbons Cholesterol - structure Cholesterol importance A stabilizing component of cell membranes A precursor of bile salts A precursor of steroid hormones
FORTH VALLEY. LIPID LOWERING GUIDELINE v5 2016
 FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
International Journal of Research and Development in Pharmacy and Life Sciences. Research Article
 International Journal of Research and Development in Pharmacy and Life Sciences Available online at http//www.ijrdpl.com February - March, 214, Vol. 3, No.2, pp 943-948 ISSN: 2278-238 Research Article
International Journal of Research and Development in Pharmacy and Life Sciences Available online at http//www.ijrdpl.com February - March, 214, Vol. 3, No.2, pp 943-948 ISSN: 2278-238 Research Article
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Diseases & Conditions
 http://my.clevelandclinic.org Diseases & Conditions About Cholesterol-Lowering Drugs Some people have a genetic predisposition to high blood cholesterol levels. These people may need drug therapy in addition
http://my.clevelandclinic.org Diseases & Conditions About Cholesterol-Lowering Drugs Some people have a genetic predisposition to high blood cholesterol levels. These people may need drug therapy in addition
High density lipoprotein metabolism
 High density lipoprotein metabolism Lipoprotein classes and atherosclerosis Chylomicrons, VLDL, and their catabolic remnants Pro-atherogenic LDL HDL Anti-atherogenic Plasma lipid transport Liver VLDL FC
High density lipoprotein metabolism Lipoprotein classes and atherosclerosis Chylomicrons, VLDL, and their catabolic remnants Pro-atherogenic LDL HDL Anti-atherogenic Plasma lipid transport Liver VLDL FC
Fibrate and cardiovascular disease: Evident from meta-analysis. Thongchai Pratipanawatr
 Fibrate and cardiovascular disease: Evident from meta-analysis Thongchai Pratipanawatr ??? ย คห นใหม ย คห นกลาง ย คห นเก า ?? Statin era? ย คห นใหม ย คห นกลาง ย คห นเก า CURRENT ROLE OF FIBRATE What are
Fibrate and cardiovascular disease: Evident from meta-analysis Thongchai Pratipanawatr ??? ย คห นใหม ย คห นกลาง ย คห นเก า ?? Statin era? ย คห นใหม ย คห นกลาง ย คห นเก า CURRENT ROLE OF FIBRATE What are
Fibrates. Spotlight on. Fibric acid derivatives (fibrates) have been used. When should I prescribe fibrates? In this article: Andrew s visit
 have been used. When should I prescribe fibrates? In this article: Andrew s visit") Focus on CME at the University of Alberta Spotlight on By T. K. Lee, MSc (Exp. Medicine), MB, BS, MRCP(UK), ABIM, FRCPC As presented at the Drug Update & Practical Therapeutics Course, November 8, 2002.
Focus on CME at the University of Alberta Spotlight on By T. K. Lee, MSc (Exp. Medicine), MB, BS, MRCP(UK), ABIM, FRCPC As presented at the Drug Update & Practical Therapeutics Course, November 8, 2002.
Elements for a Public Summary
 Rosuvastatin Stada 5 mg film-coated tablets Rosuvastatin Stada 10 mg film-coated tablets Rosuvastatin Stada 20 mg film-coated tablets Rosuvastatin Stada 40 mg film-coated tablets 25.8.2014, V1.1 PUBLIC
Rosuvastatin Stada 5 mg film-coated tablets Rosuvastatin Stada 10 mg film-coated tablets Rosuvastatin Stada 20 mg film-coated tablets Rosuvastatin Stada 40 mg film-coated tablets 25.8.2014, V1.1 PUBLIC
Hypertriglyceridemia: Why, When, and How to Treat. Gregory Cohn, MD, FNLA, FASPC
 Hypertriglyceridemia: Why, When, and How to Treat Gregory Cohn, MD, FNLA, FASPC DISCLOSURES Consultant to Akcea Therapeutics (in the past 12 months). OUTLINE I. Lipoproteins II. Non-HDL-C III. Causes and
Hypertriglyceridemia: Why, When, and How to Treat Gregory Cohn, MD, FNLA, FASPC DISCLOSURES Consultant to Akcea Therapeutics (in the past 12 months). OUTLINE I. Lipoproteins II. Non-HDL-C III. Causes and
Coronary heart disease is the leading cause of death in
 PHARMACOLOGY NOTES Ezetimibe (Zetia): a new type of lipid-lowering agent JIGNA PATEL, PHARMD CANDIDATE, VALERIE SHEEHAN, PHARMD, AND CHERYLE GURK-TURNER, RPH Coronary heart disease is the leading cause
PHARMACOLOGY NOTES Ezetimibe (Zetia): a new type of lipid-lowering agent JIGNA PATEL, PHARMD CANDIDATE, VALERIE SHEEHAN, PHARMD, AND CHERYLE GURK-TURNER, RPH Coronary heart disease is the leading cause
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
CHOLESTEROL REDUCING MEDICATIONS. Five Main Categories. 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor
 Page 1 of 5 PHA-GEN-002-2004 CHOLESTEROL REDUCING MEDICATIONS Five Main Categories 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor Statins Also called HMG-CoA reductase inhibitors
Page 1 of 5 PHA-GEN-002-2004 CHOLESTEROL REDUCING MEDICATIONS Five Main Categories 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor Statins Also called HMG-CoA reductase inhibitors
Niacin Metabolism: Effects on Cholesterol
 Niacin Metabolism: Effects on Cholesterol By Julianne R. Edwards For Dr. William R. Proulx, PhD, RD Associate Professor of Nutrition and Dietetics In partial fulfillments for the requirements of NUTR342
Niacin Metabolism: Effects on Cholesterol By Julianne R. Edwards For Dr. William R. Proulx, PhD, RD Associate Professor of Nutrition and Dietetics In partial fulfillments for the requirements of NUTR342
Elements for a public summary
 VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Cardiovascular disease (CVD) is responsible for one-third of global deaths and is a leading and increasing contributor to the
VI.2 Elements for a public summary VI.2.1 Overview of disease epidemiology Cardiovascular disease (CVD) is responsible for one-third of global deaths and is a leading and increasing contributor to the
Lipid/Lipoprotein Structure and Metabolism (Overview)
") Lipid/Lipoprotein Structure and Metabolism (Overview) Philip Barter President, International Atherosclerosis Society Centre for Vascular Research University of New South Wales Sydney, Australia Disclosures
Lipid/Lipoprotein Structure and Metabolism (Overview) Philip Barter President, International Atherosclerosis Society Centre for Vascular Research University of New South Wales Sydney, Australia Disclosures
Arteriosclerosis & Atherosclerosis
 Arteriosclerosis & Atherosclerosis Arteriosclerosis = hardening of arteries = arterial wall thickening + loss of elasticity 3 types: -Arteriolosclerosis -Monckeberg medial sclerosis -Atherosclerosis Arteriosclerosis,
Arteriosclerosis & Atherosclerosis Arteriosclerosis = hardening of arteries = arterial wall thickening + loss of elasticity 3 types: -Arteriolosclerosis -Monckeberg medial sclerosis -Atherosclerosis Arteriosclerosis,
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Zetia (Ezetimibe) Drug Monograph. Clinical clerkship Students (Week 1)
 Drug Monograph. Clinical clerkship Students (Week 1)") Zetia (Ezetimibe) Drug Monograph Clinical clerkship Students (Week 1) Fan Sheung Yin Chan Wai Lok Lau Man Pong Li Kwan Lam Chau Chung Yan Wong Yi Man Law Wing Yan Tsang Chun Man Li Wing Suen Cynthia Ho
Zetia (Ezetimibe) Drug Monograph Clinical clerkship Students (Week 1) Fan Sheung Yin Chan Wai Lok Lau Man Pong Li Kwan Lam Chau Chung Yan Wong Yi Man Law Wing Yan Tsang Chun Man Li Wing Suen Cynthia Ho
 Glossary For TheFatNurse s For All Ages Series Adipocytes, also known as lipocytes and fat cells, are the cells that primarily compose adipose tissue, specialized in storing energy as fat. Apolipoprotein
Glossary For TheFatNurse s For All Ages Series Adipocytes, also known as lipocytes and fat cells, are the cells that primarily compose adipose tissue, specialized in storing energy as fat. Apolipoprotein
ROSULIP. Composition Rosulip 10 mg Each tablet contains 10 mg Rosuvastatin (as calcium).
.") ROSULIP Composition Rosulip 10 mg Each tablet contains 10 mg Rosuvastatin (as calcium). Tablets Rosulip 20 mg Each tablet contains 20 mg Rosuvastatin (as calcium). Action Rosuvastatin is a selective and
ROSULIP Composition Rosulip 10 mg Each tablet contains 10 mg Rosuvastatin (as calcium). Tablets Rosulip 20 mg Each tablet contains 20 mg Rosuvastatin (as calcium). Action Rosuvastatin is a selective and
Pediatric Dyslipidemia: Angela Gooden MSN, RN, CPNP- AC/PC, Texas Children s Hospital, Pediatric Cardiology
 Pediatric Dyslipidemia: Angela Gooden MSN, RN, CPNPAC/PC, Texas Children s Hospital, Pediatric Cardiology Objectives Define pediatric dyslipidemia Describe the association between pediatric dyslipidemia
Pediatric Dyslipidemia: Angela Gooden MSN, RN, CPNPAC/PC, Texas Children s Hospital, Pediatric Cardiology Objectives Define pediatric dyslipidemia Describe the association between pediatric dyslipidemia
International Journal of Chemistry and Pharmaceutical Sciences
 Available online at www.pharmaresearchlibrary.com Pharma Research Library International Journal of Chemistry and Pharmaceutical Sciences 2013, Vol.1 (2): 180-186 ISSN 2321-3132 Pharma Research Library
Available online at www.pharmaresearchlibrary.com Pharma Research Library International Journal of Chemistry and Pharmaceutical Sciences 2013, Vol.1 (2): 180-186 ISSN 2321-3132 Pharma Research Library
Behind LDL: The Metabolism of ApoB, the Essential Apolipoprotein in LDL and VLDL
 Behind LDL: The Metabolism of ApoB, the Essential Apolipoprotein in LDL and VLDL Sung-Joon Lee, PhD Division of Food Science Institute of Biomedical Science and Safety Korea University Composition of Lipoproteins:
Behind LDL: The Metabolism of ApoB, the Essential Apolipoprotein in LDL and VLDL Sung-Joon Lee, PhD Division of Food Science Institute of Biomedical Science and Safety Korea University Composition of Lipoproteins:
Physiology Unit 4 DIGESTIVE PHYSIOLOGY
 Physiology Unit 4 DIGESTIVE PHYSIOLOGY In Physiology Today Functions Motility Ingestion Mastication Deglutition Peristalsis Secretion 7 liters/day! Exocrine/endocrine Digestion Absorption Digestion of
Physiology Unit 4 DIGESTIVE PHYSIOLOGY In Physiology Today Functions Motility Ingestion Mastication Deglutition Peristalsis Secretion 7 liters/day! Exocrine/endocrine Digestion Absorption Digestion of
 Acetyl CoA HMG CoA Mevalonate (C6) Dimethylallyl Pyrophosphate isopentenyl Pyrophosphate (C5) Geranyl Pyrophosphate (C10) FarnesylPyrophosphate (C15) Squalene (C30) Lanosterol (C30) 7 Dehydrocholesterol
Acetyl CoA HMG CoA Mevalonate (C6) Dimethylallyl Pyrophosphate isopentenyl Pyrophosphate (C5) Geranyl Pyrophosphate (C10) FarnesylPyrophosphate (C15) Squalene (C30) Lanosterol (C30) 7 Dehydrocholesterol
ATP III (Adult Treatment Panel III) CLASSIFICATION C IN ADULTS
 CLASSIFICATION C IN ADULTS") LABORATORY AND RISK FACTORS OF ATHEROSCLEROSIS S R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty RISK FACTORS FOR CHD Clinical Risk Factors Laboratory Risk Factors MAJOR CLINICAL RISK
LABORATORY AND RISK FACTORS OF ATHEROSCLEROSIS S R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty RISK FACTORS FOR CHD Clinical Risk Factors Laboratory Risk Factors MAJOR CLINICAL RISK
Altered concentrations of blood plasma
 C O N S E N S U S S T A T E M E N T Detection and Management of Lipid Disorders in Diabetes Altered concentrations of blood plasma lipoproteins are powerful predictors of coronary heart disease (CHD) and
C O N S E N S U S S T A T E M E N T Detection and Management of Lipid Disorders in Diabetes Altered concentrations of blood plasma lipoproteins are powerful predictors of coronary heart disease (CHD) and
Eveness Rosuvastatin. Each tablet contains 5mg, 10mg, 20mg, or 40 mg of rosuvastatin (as calcium salt)
") Eveness Rosuvastatin Composition Each tablet contains 5mg, 10mg, 20mg, or 40 mg of rosuvastatin (as calcium salt) Pharmacological properties Pharmacotherapeutic gruoup: HMG CoA reductase inhibitors Pharmacodynamic
Eveness Rosuvastatin Composition Each tablet contains 5mg, 10mg, 20mg, or 40 mg of rosuvastatin (as calcium salt) Pharmacological properties Pharmacotherapeutic gruoup: HMG CoA reductase inhibitors Pharmacodynamic
Cellular control of cholesterol. Peter Takizawa Department of Cell Biology
 Cellular control of cholesterol Peter Takizawa Department of Cell Biology Brief overview of cholesterol s biological role Regulation of cholesterol synthesis Dietary and cellular uptake of cholesterol
Cellular control of cholesterol Peter Takizawa Department of Cell Biology Brief overview of cholesterol s biological role Regulation of cholesterol synthesis Dietary and cellular uptake of cholesterol
13/09/2012. Dietary fatty acids. Triglyceride. Phospholipids:
 CARDIOVASCULAR DISEASES (CVD) and NUTRITION Major cause of morbidity & mortality in Canada & other developed countries e.g., majority of approved health claims on food labels relate to lowering CVD Relation
CARDIOVASCULAR DISEASES (CVD) and NUTRITION Major cause of morbidity & mortality in Canada & other developed countries e.g., majority of approved health claims on food labels relate to lowering CVD Relation
hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER
 Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD),
Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD),
March 2005 Current Trends in Treating Elevated Cholesterol H01
 W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 March 2005 Current Trends in Treating Elevated Cholesterol 707-000-05-003-H01 IT S ALWAYS A GOOD IDEA TO
W-F Professional Associates, Inc. 400 Lake Cook Rd., Suite 207 Deerfield, IL 60015 847-945-8050 March 2005 Current Trends in Treating Elevated Cholesterol 707-000-05-003-H01 IT S ALWAYS A GOOD IDEA TO
STATIN UTILIZATION MANAGEMENT CRITERIA
 STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Lipoprotein Formation, Structure and Metabolism: Cholesterol Balance and the Regulation of Plasma Lipid Levels
 Lipoprotein Formation, Structure and Metabolism: Balance and the Regulation of Plasma Lipid Levels David E. Cohen, MD, PhD Director of Hepatology, Gastroenterology Division, Brigham and Women s Hospital
Lipoprotein Formation, Structure and Metabolism: Balance and the Regulation of Plasma Lipid Levels David E. Cohen, MD, PhD Director of Hepatology, Gastroenterology Division, Brigham and Women s Hospital
Nicotinic Acid Nicotinic Acid
 Nicotinic Acid Nicotinic Acid PRODUCT INFORMATION NAME OF THE MEDICINE Active ingredient: Nicotinic acid BP 250 mg. Structural formula: Molecular weight: 123.1 CAS Registry no.: 59-67-6 DESCRIPTION Inactive
Nicotinic Acid Nicotinic Acid PRODUCT INFORMATION NAME OF THE MEDICINE Active ingredient: Nicotinic acid BP 250 mg. Structural formula: Molecular weight: 123.1 CAS Registry no.: 59-67-6 DESCRIPTION Inactive
In the Know: Canadian Guidelines for Dyslipidemia, 2003
 In the Know: Canadian Guidelines for Dyslipidemia, 2003 In his reviews of Canadian dyslipidemia guidelines, Dr. Curnew explores the impact of major trials, the assessment and categories of risk, and both
In the Know: Canadian Guidelines for Dyslipidemia, 2003 In his reviews of Canadian dyslipidemia guidelines, Dr. Curnew explores the impact of major trials, the assessment and categories of risk, and both
PART III: CONSUMER INFORMATION
 PART III: CONSUMER INFORMATION Pr SIMVASTATIN 5 Pr SIMVASTATIN 10 Pr SIMVASTATIN 20 Pr SIMVASTATIN 40 Pr SIMVASTATIN 80 Simvastatin Tablets, USP This leaflet is part III of a three-part Product Monograph
PART III: CONSUMER INFORMATION Pr SIMVASTATIN 5 Pr SIMVASTATIN 10 Pr SIMVASTATIN 20 Pr SIMVASTATIN 40 Pr SIMVASTATIN 80 Simvastatin Tablets, USP This leaflet is part III of a three-part Product Monograph
BIOL2171 ANU TCA CYCLE
 TCA CYCLE IMPORTANCE: Oxidation of 2C Acetyl Co-A 2CO 2 + 3NADH + FADH 2 (8e-s donated to O 2 in the ETC) + GTP (energy) + Heat OVERVIEW: Occurs In the mitochondrion matrix. 1. the acetyl portion of acetyl-coa
TCA CYCLE IMPORTANCE: Oxidation of 2C Acetyl Co-A 2CO 2 + 3NADH + FADH 2 (8e-s donated to O 2 in the ETC) + GTP (energy) + Heat OVERVIEW: Occurs In the mitochondrion matrix. 1. the acetyl portion of acetyl-coa
If yes, continue to #2. If no, do not approve. DENIAL TEXT: See the initial denial text at the end of the guideline.
 Generic Brand HICL GCN Exception/Other LOMITAPIDE JUXTAPID 39883 This drug requires a written request for prior authorization. All requests for Juxtapid (lomitapide) require review by a pharmacist prior
Generic Brand HICL GCN Exception/Other LOMITAPIDE JUXTAPID 39883 This drug requires a written request for prior authorization. All requests for Juxtapid (lomitapide) require review by a pharmacist prior
Cholesterol Metabolism
 Cholesterol Metabolism Lippincott s Illustrated Review Chapter 18 Steroid Nucleus 1 2 Cholesterol was isolated from gall bladder stones in 1774 3 Sources and Elimination of Cholesterol Synthesis: 1000
Cholesterol Metabolism Lippincott s Illustrated Review Chapter 18 Steroid Nucleus 1 2 Cholesterol was isolated from gall bladder stones in 1774 3 Sources and Elimination of Cholesterol Synthesis: 1000
PLASMA LIPOPROTEINS AND LIPIDS DETERMINATION OF PLASMA CHOLESTEROL AND TRIGLICERIDE LEVEL
 PLASMA LIPOPROTEINS AND LIPIDS DETERMINATION OF PLASMA CHOLESTEROL AND TRIGLICERIDE LEVEL Lipids are characterized by low polarity and limited solubility in water. Their plasma concentration is about 500-600
PLASMA LIPOPROTEINS AND LIPIDS DETERMINATION OF PLASMA CHOLESTEROL AND TRIGLICERIDE LEVEL Lipids are characterized by low polarity and limited solubility in water. Their plasma concentration is about 500-600
CE Prn. Pharmacy Continuing Education from WF Professional Associates ABOUT WFPA LESSONS TOPICS ORDER CONTACT MCA EXAM REVIEWS
 CE Prn Pharmacy Continuing Education from WF Professional Associates ABOUT WFPA LESSONS TOPICS ORDER CONTACT MCA EXAM REVIEWS Hyperlipidemia---Update & Review The objectives of this lesson are such that
CE Prn Pharmacy Continuing Education from WF Professional Associates ABOUT WFPA LESSONS TOPICS ORDER CONTACT MCA EXAM REVIEWS Hyperlipidemia---Update & Review The objectives of this lesson are such that
DISLIPIDEMIA. Dharma Lindarto. Div: Endokrinologi-Metabolik. Departemen Ilmu Penyakit Dalam FK USU/RSUP. H Adam Malik Medan
 DISLIPIDEMIA Dharma Lindarto Div: Endokrinologi-Metabolik. Departemen Ilmu Penyakit Dalam FK USU/RSUP. H Adam Malik Medan Introduction Dyslipidemia is a general term associated with high cholesterol and/or
DISLIPIDEMIA Dharma Lindarto Div: Endokrinologi-Metabolik. Departemen Ilmu Penyakit Dalam FK USU/RSUP. H Adam Malik Medan Introduction Dyslipidemia is a general term associated with high cholesterol and/or
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Moh Tarek + Suhayb. Tamara Al-Azzeh + Asmaa Aljeelani ... Faisal
 28 Moh Tarek + Suhayb Tamara Al-Azzeh + Asmaa Aljeelani... Faisal Digestion of dietary lipids Lipid digestion and absorption are complex processes. They involve soluble enzymes, substrates with different
28 Moh Tarek + Suhayb Tamara Al-Azzeh + Asmaa Aljeelani... Faisal Digestion of dietary lipids Lipid digestion and absorption are complex processes. They involve soluble enzymes, substrates with different
srmp Atorvastatin Medical Valley
 srmp Atorvastatin Medical Valley VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology This product is indicated for the lowering of cholesterol blood levels and the prevention of
srmp Atorvastatin Medical Valley VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology This product is indicated for the lowering of cholesterol blood levels and the prevention of
MMBS, MMED (Path),MAACB, MACTM, MACRRM
,MAACB, MACTM, MACRRM") Dr Mere Kende MMBS, MMED (Path),MAACB, MACTM, MACRRM Lecturer- SMSH Brief Overview of Lipids What is dyslipidemia? Classification of hyperlipidemia Primary vs secondary hyperlipidemia Hypercholesterolaemia
Dr Mere Kende MMBS, MMED (Path),MAACB, MACTM, MACRRM Lecturer- SMSH Brief Overview of Lipids What is dyslipidemia? Classification of hyperlipidemia Primary vs secondary hyperlipidemia Hypercholesterolaemia
Dyslipidemia and HIV NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Dyslipidemia and HIV Heidi Crane, MD, MPH Madison Metabolic Clinic Associate Professor UW Department of Medicine Presentation prepared by: Heidi Crane, MD,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Dyslipidemia and HIV Heidi Crane, MD, MPH Madison Metabolic Clinic Associate Professor UW Department of Medicine Presentation prepared by: Heidi Crane, MD,