Whats new in lipid management, and Can your high CV risk patients benefit from a PCSK9i?
|
|
|
- Juniper Alan Dennis
- 6 years ago
- Views:
Transcription

1 Whats new in lipid management, and Can your high CV risk patients benefit from a PCSK9i?
2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.

3 Who to Screen
. We suggest that for individuals with a history of triglyceride levels >4.")
4 How to Screen RECOMMENDATIONS We recommend non-fasting lipid and lipoprotein testing which can be performed in adults in whom screening is indicated as part of a comprehensive risk assessment to reduce CVD events (Strong Recommendation, High Quality Evidence). We suggest that for individuals with a history of triglyceride levels >4.5 mmol/l that lipid and lipoprotein levels be measured fasting (Conditional Recommendation, Low Quality Evidence). Practical tip: Compared to fasting lipid values, there will be minimal change with non-hdl-c, a slight decrease in LDL-C and small increase in triglyceride concentrations when individuals do not fast.
5 Changes in Postprandial Lipids in Normal Populations Langsted A et al., Circulation Fasting and nonfasting lipid levels influence of normal food intake on lipoids, lipoproteins, apolipoproteins and cardiovascular risk prediction Cross-sectional study of fasting versus nonfasting lipid levels in Copenhagen General Population Study and Copenhagen City Heart Study Siddhu D and Naugler C. Arch Int Med Fasting time and lipid levels in a community-based population Cross-sectional study of individuals tested from 1 to 16 hours postprandially In both studies, non-hdl-c, and apo B varied little between fasting and nonfasting TG levels increased up to 20% ( mm) and LDL-C was lower by up to 10% ( mm)
6 Benefits of Non-fasting Lipids Patient convenience no need to go to lab early in the morning and fasting; no need for retesting if not fasting Reduced wait times and reduced early morning patient burden in clinical laboratories Safety prevention of hypoglycemic episodes in diabetics Enhances compliance and avoids delay in lipid screening and follow up tests Enhanced predictive value for CVD and mortality of nonfasting lipids Identification of high remnants/insulin resistance Removal of need to perform fasting blood work generally HbA1c is accepted as a diagnostic test and follow up test by CDA and ADA that does NOT have to be accompanied by a fasting glucose High fasting glucose usually results in HbA1c test

7 2016 CCS Lipid Guidelines Recommend: Targeting Lower LDL-C to Lower the Risk for CV Events TREATMENT TARGETS: LDL-C consistently <2.0 mmol/l or >50% reduction Consider <1.8 mmol/l in patients with clinical atherosclerosis Apo B 0.80 g/l or non-hdl-c 2.6 mmol/l can be considered as alternative treatment targets STATIN INDICATED CONDITIONS (those who will benefit the most): Clinical atherosclerosis* Abdominal aortic aneurysm Most diabetes mellitus CKD (age >50 years) LDL-C 5.0 mmol/l *Clinical atherosclerosis, i.e., previous MI, or coronary revascularization by PCI or CABG surgery, other arterial revascularization procedures, angina pectoris, cerebrovascular disease including TIA, or peripheral arterial disease (claudication and/or ABI <0.9) ABI, ankle brachial index; Apo B, apolipoprotein B; CABG, coronary artery bypass graft surgery; CCS, Canadian Cardiovascular Society; CKD, chronic kidney disease; CV, cardivoascular; HDL-C, high-density lipoprotein cholestero; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarction; PCI, percutaneous coronary intervention; TIA, transient ischemic attack. Anderson TJ et al. 2016;32:
.")
8 When to Consider Pharmacological Treatment in Risk Management Statin Indicated Conditions a.we recommend a target LDL-C consistently <2.0 mmol/l or >50% reduction of LDLC for individuals for whom treatment is initiated to lower the risk of CVD events and mortality (Strong Recommendation, Moderate-Quality Evidence). Alternative target variables are apob <0.8 g/l or non-hdl-c <2.6 mmol/l (Strong Recommendation, Moderate Quality Evidence). b. We recommend a >50% reduction of LDL-C for patients with LDL-C > 5.0 mmol/l in individuals for whom treatment is initiated to decrease the risk of CVD events and mortality (Strong Recommendation, Moderate Quality Evidence).
9 Pharmacological Treatment Indications & Targets Category Consider Initiating pharmacotherapy if: Target NNT Primary Prevention High (FRS 20%) Intermediate (FRS 10-19%) LDL-C <2.0 mmol/l or >50% LDL-C 3.5 mmol/l or Non-HDL-C 4.3 mmol/l or Apo B 1.2 g/l or Men 50 & women 60 yrs and 1 CV risk factor Or Apo B <0.8 g/l Statin Indicated Conditions** Clinical atherosclerosis* (CAD, CVD, PAD) Abdominal aortic aneurysm Or 20 Diabetes mellitus: 40 yrs, or >15 yrs duration & age 30 yrs (DM 1), or microvascular disease non-hdl-c <2.6 mmol/l CKD (age 50 yrs): egfr < 60 ml/min/1.73 m 2, or ACR >3 mg/mmol LDL-C 5.0 mmol/l >50% in LDL-C * consider LDL-C < 1.8 mmol/l for subjects with ACS within last 3 months;** statins indicated as initial therapy
10 Beyond Statin Drugs for ASCVD Prevention 1. We recommend ezetimibe as second-line therapy to lower LDL-C in patients with clinical cardiovascular disease if targets are not reached on maximally tolerated statin therapy. (Strong Recommendation, High Quality evidence) 2. We recommend that niacin not be added to statin therapy for CVD prevention in patients who have achieved LDL-C targets. (Strong Recommendation, High Quality Evidence) 3. We do not recommend the addition of fibrates to statin therapy for CVD event prevention in patients who have achieved LDL-C targets. (Strong recommendation, High Quality evidence). Values and preferences: In sub-group analysis, patients with elevated triglycerides and low HDL-C may benefit from fibrate therapy. Anderson et al Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult Canadian Journal of Cardiology 2016;32:


 to lower LDL-C for patients with heterozygous familial hypercholesterolemia whose LDL-C remains above")
11 Beyond Statin Drugs for ASCVD Prevention and FH 4. We suggest that bile acid sequestrants be considered for LDL-C lowering in high risk patients who remain above target despite statin +/- ezetimibe therapy (Conditional Recommendation, Low Quality Evidence). 5. We suggest that PCSK9 inhibitors be considered to lower LDL-C for patients with atherosclerotic cardiovascular disease in those not at LDL-C goal despite maximally tolerated statin +/- ezetimibe therapy (Conditional Recommendation, Moderate Quality Evidence). 6. We suggest the use of PCSK9 inhibitors (evolocumab, alirocumab) to lower LDL-C for patients with heterozygous familial hypercholesterolemia whose LDL-C remains above target despite maximally tolerated statin therapy (Conditional Recommendation, Moderate Quality Evidence). Anderson et al Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult Canadian Journal of Cardiology 2016;32:
12 Major Changes Since the 2012 Update Provide better guidance to clinicians for the assessment of risk, screening and appropriate treatment of dyslipidemia for the prevention of cardiovascular disease Lipid screening for both men and women 40 years of age and inclusion of screening for women with a history of hypertensive diseases of pregnancy Use of non-fasting lipid determinations for initial screening and follow-up Expansion of CKD definition for high risk and harmonization with K-DIGO guidelines
13 Major Changes Since the 2012 Update Broader treatment recommendations for those in the intermediate risk category More explicit recommendations for health behaviour changes Greater emphasis about discussion with patients about their preferences (shared decision making) New recommendations about non-statin drug use
 OR")
14 CCS Position Statement on Familial Hypercholesterolemia (FH): Diagnostic and Treatment Flow when FH is Suspected LDL Cholesterol > 5 mmol/l + Rule out secondary causes - Obstructive liver disease Hypothyroidism Nephrotic syndrome Anorexia Positive Family History First degree relative with LDL cholesterol > 5 mmol/l OR Early coronary heart disease (<65 years in women, <55 years in men) OR Physical findings in patient + Genest J et al. Canadian Journal of Cardiology , DOI: ( /j.cjca )
15 CCS Position Statement on Familial Hypercholesterolemia (FH): Diagnostic and Treatment Flow when FH is Suspected Clinical diagnosis of FH Genetic diagnosis of FH Mutation in: LDLR (major gene) APOB, PCSK9 (secondary genes) Other minor genes Dietary pattern, Lifestyle, Pharmacological therapy to reduce LDL-C Cascade screening of family members Genest J et al. Canadian Journal of Cardiology , DOI: ( /j.cjca )
16 Recommendation Category Statin indicated conditions Consider Initiating pharmacotherapy if LDL > 5.0 mmol/l Target LDL-C > 50%
17 Optimal control of dyslipidemia in patients with CVD LDL-C target: guidelines and real world insights The need for LDL-C lowering beyond statin therapy PCSK9 inhibition and the data from clinical trials Case-based discussion Discussion Points

18 THE PATIENT WITH ASCVD
 non-hdl-c: 3.")
19 Identifying the High Risk Patient John: Age 56 Hypertension, BP 130/75 mm/hg (controlled for 5 years) Previous MI with PCI at age 48 Family history of CHD Had some issues with statin tolerance, currently trying different statin and low dose Non-smoker BMI 29 kg/m 2 History TC: 4.7 mmol/l TG:1.4 mmol/l HDL-C: 1.3 mmol/l LDL-C: 2.7 mmol/l (current) non-hdl-c: 3.5 mmol/l Lipid Profile Current Medication Lifestyle Has made recommended lifestyle changes Has attended healthy heart classes Completed dietitian consult Attempts to exercise 100 mins per week Cardiovascular Risk ASA 80 mg once daily Atorvastatin 20 mg Bisoprolol 5 mg once daily Ramipril 10 mg once daily High risk, pre-treatment Framingham risk score >20%
20 Despite Guideline Targets Many High-risk Canadian Patients Treated with Statins Are Not at LDL-C Goal 45% Canadian high-risk patients are NOT at LDL-C target 1* ( 2 mmol/l) 88% of patients received a potent statin with suboptimal dose 14% of patients received additional lipid-lowering agent 43% Canadian patients with diabetes are NOT at LDL-C target 2 ( 2 mmol/l) 82% of patients were on a lipid-lowering agent *High risk = coronary artery disease, peripheral arterial disease, cerebrovascular disease, diabetes mellitus or Framingham 10-year risk score 20%. DYSIS Study 2,436 patients, 1913 high risk patients. N = 5, Goodman SG, et al. on behalf of the DYSIS Canadian Investigators. Can J Cardiol. 2010;26(9):e330-e Leiter LD, et al. Can J Diabetes. 2013;37:82-89.
21 Even Maximal Statin Therapy May Not Be Sufficient In Achieving LDL-C Target 0% 10% 20% 30% 40% 50% 60% Rosuvastatin 10 5 mg 20 mg 10 mg 20 mg 40 mg Atorvastatin 10 mg 20 mg 40 mg 80 mg Simvastatin 10 mg 20 mg 40 mg Pravastatin 10 mg 20 mg 40 mg Doubling the statin dose results in only 6% LDL-C reduction Lovastatin 20 mg 40 mg 80 mg Fluvastatin 20 mg 40 mg *As per Canadian Product Monographs 1. Crestor (rosuvastatin) Product Monograph. AstraZeneca. April 21, Zocor (simvastatin) Product Monograph. Merck. Dec 10, Lescol (fluvastatin) Product Monograph. Novartis. Aug. 26, Adapted from CURVES Investigators. Am J Cardiol. 1998;81: Lipitor (atorvastatin) Product Monograph. Pfizer. Feb 18, 2016.
22 CHD Event Rate,% Getting to Goal: Statin Clinical Trials in Primary and Secondary Prevention Have Driven LDL-C Targets These trials have demonstrated that LDL-C lowering is associated with greater reduction of CHD events 4S-P Secondary Prevention JUP-T DIABETES 1 O PREVENTION HPS-T TNT-80 CARDS-T Ascot-T Care-T TNT-10 PROS-T JUP-P Lipid-T AFCAPS-T 4S-T HPS-P Care-P AFCAPS-P Ascot-P Lipid-P PROS-P WPS-T WPS-P Primary Prevention LDL-C mmol/l *Event rates for HPS, CARE, and LIPID are for death from CHD and nonfatal MI. Event rates for 4S and the TNT Study also include resuscitation after cardiac arrest. Cholesterol Treatment Trialists (CTT) Collaboration. Lancet. 2010;376: ; Cannon CP, et al. J Am Coll Cardiol. 2006;48(3):438-45; Anderson TJ, Grégoire J, et al. Can J Cardiol. 2014;30(4):377-80; Adapted from Gotto A Jr, Opie LH. Drugs for the Heart. 7th ed. Philadelphia: Elsevier Saunders. 2009:353.
23 Proportional reduction in event rate (% SE) Proportional reduction in event rate (% SE) Reduction in CV events is proportional to LDL-C reduction at 1 year A prospective meta-analysis of data from 90,056 individuals from 14 trials of statins 50 A 1 mmol/l (39 mg/dl) reduction in LDL-C was associated with a 23% reduction in major coronary events 50 21% reduction in major vascular events (19) 1.0 (38) 1.5 (58) Reduction in LDL-C mmol/l (mg/dl) 2.0 (77) (19) 1.0 (38) 1.5 (58) Reduction in LDL-C mmol/l (mg/dl) 2.0 (77) Adapted from Baigent C, et al, Cholesterol Treatment Trialists (CTT) Collaborators. Lancet 2005;366:
24 Event Rate (%) Statin trials have also shown that very low (vs moderately low) LDL-C is associated with significantly lower risk for major cv events Major coronary events (fatal or nonfatal MI, fatal other CHD, and hospitalization for UA) Major CV events (fatal or nonfatal MI, fatal other CHD, hospitalization for UA, or fatal or nonfatal stroke 25.2% 34.4% % 16.7% 18.2% % 10.9% 0 < >4.9 LDL-C (mmol/l) CHD, coronary heart disease; CV, cardiovascular; CVD, cardiovascular disease; HR, hazard ratio; LDL-C, low-density lipoprotein cholesterol; MI, myocardial infarction; UA, unstable angina. Boekholdt SM et al. J Am Coll Cardiol. 2014;64:
25 2 Year Event* Rate (%) 5 Year Event Rate (%) Substantial residual risk remains in many patients with high CV risk despite intense statin therapy 30 Acute Coronary Syndrome PROVE-IT TIMI Stable Coronary Heart Disease TNT % risk reduction Residual Risk % risk reduction 5 0 Median achieved LDL 2.5 mmol/l Less Intense LDL-C Management (40 mg pravastatin) (n = 2,063) Median achieved LDL 1.6 mmol/l More Intense LDL-C Management (80 mg atorvastatin) (n = 2,099) CV, cardiovascular. *Death, myocardial infarction, unstable angina requiring hospitalization, revascularization (>30 days), stroke Coronary heart disease death, non-procedure-related MI, resuscitation after cardiac arrest, stroke 1. Adapted from Cannon CP et al. N Engl J Med. 2004;350: Adapted from LaRosa JC et al. N Engl J Med. 2005;352: Median achieved LDL 2.5 mmol/l Less Intense LDL-C Management (10 mg atorvastatin) (n = 5,006) Median achieved LDL 1.6 mmol/l More Intense LDL-C Management (80 mg atorvastatin) (n = 4,995) Residual Risk TNT NNT 45 PROVE-IT NNT 26
26 Proportion of patients experiencing major CV event The TNT Study Shows that Residual Risk Remains Despite LDL Lowering in Post MI Patients HR = 0.78 (95% CI 0.69, 0.89) RRR=22% P= atorvastatin 10 mg mean LDL-C 2.6 mmol/l atorvastatin 80 mg mean LDL-C 2.0 mmol/l Residual Risk 0.02 LaRosa JC, et al. N Engl J Med. 2005;352: Years
27 Niacin BAS Statins 1 st Gen Statins 2 nd Gen* Ezetimibe Fibrates IMPROVE-IT Most non-statins have limited efficacy at lowering LDL-C and ASCVD events (beyond maximal statin therapy) LDL-C Lowering (%) 1970 s 1980 s 1990 s 2000 s 2010 s -20% -20% -10% -20% -40% -60% -20% reduction on top of statin ASCVD, atherosclerotic cardiovascular disease; BAS, bile acid sequestrants; Gen, generation; IMPROVE-IT, IMProved Reduction of Outcomes: Vytorin Efficacy International Trial; LDL-C, low-density lipoprotein cholesterol. *Impacted clinical practice guidelines. The Coronary Drug Project Research Group. JAMA. 1975;231: ; The Lipid Research Clinics Programs. JAMA 1984;251:351-64; Frick MH et al. N Engl J Med. 1987; 317: ; Vaughan CJ, Gotto AM Jr. Circulation. 2004;110:886-92; Cannon CP et al. N Engl J Med. 2015;372: ; National Clinical Guideline Centre (UK). NICE Clinical Guidelines, No. 181; July 2014.
28 CV Event Rate (%)* IMPROVE-IT reported that ezetimibe add-on to simvastatin incrementally lowered LDL-C and reduced CV event rates Hazard Ratio, 0936 (95% CI, ) P=0.016 Simvastatin monotherapy LDL: 2.4>1.8 (34.7%; 2,742 events) Simvastatin+ezetimibe LDL: 2.4>1.36 (32.7%; 2,572 events) NNT: 50 (at 6 years) Years since Randomization CV, cardiovascular; LDL-C, low-density lipoprotein cholesterol. *, CV death, myocadial infarction, documented unstable angina requiring re-hospitalization, coronary revascularization (30 or more days), or stroke Adapted from Cannon CP et al. N Engl J Med. 2015;372:
29 PCSK9i Niacin BAS Statins 1 st Gen Statins 2 nd Gen* Ezetimibe Fibrates IMPROVE-IT PCSK9I BACKGROUND LLT PCSK9i can produce a further 60% reduction in LDL-C levels LDL-C Lowering (%) 1970 s 1980 s 1990 s 2000 s 2010 s % -20% -10% -20% -40% -20% -57% -60% reduction on top of statin Additional -60% BAS, bile acid sequestrants; Gen, generation; IMPROVE-IT, IMProved Reduction of Outcomes: Vytorin Efficacy International Trial; LDL-C, low-density lipoprotein cholesterol; LLT, lipid lowering therapies. *Impacted clinical practice guidelines. The Coronary Drug Project Research Group. JAMA. 1975;231: ; The Lipid Research Clinics Programs. JAMA 1984;251:351-64; Frick MH et al. N Engl J Med. 1987; 317: ; Vaughan CJ, Gotto AM Jr. Circulation. 2004;110:886-92; Cannon CP et al. N Engl J Med. 2015;372: ; Sabatine MS et al. N Engl J Med. 2015;372:1500-9; Robinson J et al. N Engl J Med. 2015;372: ; National Clinical Guideline Centre (UK). NICE Clinical Guidelines, No. 181; July 2014.
30 Can Residual Risk be Further Reduced? Many patients experience cardiovascular events despite LDL-C reduction with statins 1. Anderson TJ, Grégoire J, et al Update of CCS Dyslipidemia Guidelines. Can J Cardiol. 2013;29: Cannon CP, IMPROVE-IT Investigators. N Engl J Med Jun Mancini GB, et al. Can J Cardiol. 2013;29:
31 Identifying True Statin Intolerance Statin intolerance is a clinical syndrome that is: I. characterized by inability to use statins long-term due to significant symptoms and/or biomarker abnormalities II. III. either complete (intolerant to any statin at any dose) or partial (intolerant to some statins at some doses) not attributable to established predispositions such as drug-drug interactions, untreated hypothyroidism, febrile illness, etc. Prevalence of statin intolerance is difficult to define Some patients can be successfully re-challenged Patient preference plays a role Mancini GB, et al. Can J Cardiol. 2013;29:
32 Options for Managing Statin Intolerance Patients should always be counselled regarding CV risk reduction benefit and potential side effects of statins Management options for patients who demonstrate actual intolerance to statin therapy Enhanced lifestyle Statin-based strategies* Nonstatin alternatives as adjuncts Dietary and health behaviour Reduction in dietary fat (especially saturated fat) Increased intake of plant sterols Increased physical activity and weight loss Rechallenge (after resolution of symptoms) with: Same, lower or intermittent dose of the same statin OR alternative statin Ezetimibe Niacin Fibrates Bile acid sequestrants LDL apheresis *Expert recommendation is to rechallenge with statin therapy after symptom resolution using the same statin at lower or intermittent dosing or an alternate statin Mancini GB, et al. Can J Cardiol. 2013;29:

33 Can Residual Risk be Further Reduced? Challenges with statin therapy limit effectiveness and CV risk remains: Optimizing statin therapy and managing possible side effects could lead to further decreases in LDLC and CV risk High risk patients not at goal may need adjunct therapy to help patients further decrease their LDL-C and CV risk Anderson TJ, Grégoire J, et al Update of CCS Dyslipidemia Guidelines. Can J Cardiol. 2013;29: Cannon CP, IMPROVE-IT Investigators. N Engl J Med. 2015;372(25): Mancini GB, et al. Can J Cardiol. 2013;29:

34 Challenges with lowering LDL-C in the high risk patient John: Age 56 Clinical Challenge: LDL-C above 2.0 mmol/l LDL-C 2.7 mmol/l, currently on atorvastatin 20 mg once daily Had some issues with statin tolerance, currently trying different statin and lower dose Clinical Challenge: High CV risk Previous MI with PCI at age 48 Family history of CHD Has made recommended lifestyle changes and attempts to exercise 100 mins per week








35 Statin Influence on LDL-C Metabolism plus LDL-R and PCSK9 Acetyl-CoA + acetoacetyl-coa HMG-CoA reductase STATIN PCSK9 Secretion Plasma HMG-CoA LDL Intracellular Cholesterol Biosynthesis LDL-R LDL Protein at Cell Surface PCSK9 Protein Hepatocyte Cholesterol Content Hepatocyte LDL-R Expression PCSK9 Expression SREBP Activation Nucleus Endoplasmic Reticulum (ER)
 * P < 0.05 versus baseline and placebo baseline and endpoint 1. Amgen, data on file. 2. Careskey HE, Davis RA, et al.")
36 PCSK9 (mg/ml) LDL-R and PCSK9 Expression Are Upregulated When Intracellular Cholesterol Levels Are Low Upregulation of PCSK9 increases degradation of LDL-R, serving as a counter-regulatory molecular brake on LDL-C lowering 75 * Baseline Placebo Endpoint Baseline Endpoint Atorvastatin (40 mg) * P < 0.05 versus baseline and placebo baseline and endpoint 1. Amgen, data on file. 2. Careskey HE, Davis RA, et al. J Lipid Res. 2008;49: This mechanism may explain the limitation in LDL lowering by statins and why doubling the dose, only results in 6% further LDL reduction
37 PCSK9 Inhibitors Developed to Target a Key Process in Lipid Metabolism: an Evolution in LDL-C Lowering Targeting and inhibiting PCSK9 activity leads to an increase in LDL receptor levels, which increases removal of LDL-C PCSK9 inhibitors (PCSK9i) Evolocumab Alirocumab PCSK9 = Proprotein Convertase Subtilisin Kexin Type 9



 Golgi")

38 PCSK9 Inhibitors: Targeted Therapy In Serum the Presence LDL-Cholesterol of PCSK9, Binds the to LDL-Receptors. Is Degraded Following and Does Internalization, Not Cycle Back LDL to is Cell Degraded Surface and the Receptor Recycled LDL Plasma PCSK9 LDL LDL-R LDL-R Endocytosis Hepatocyte Endocytosis Endosome PCSK9 Self-procession LDL-R Recycling Endosome LDL Degradation LDL, LDL-R and PCSK9 Degradation Nucleus Endoplasmic Reticulum (ER) Golgi Apparatus 2013 Amgen Canada Inc. All rights reserved. Qian YW, et al. J Lipid Res. 2007;48: ; Horton JD, et al. J Lipid Res. 2009;50(suppl):S172-S177.

:S172-S177.")
39 PCSK9 Inhibitors: Targeted Therapy Blocking PCSK9 Activity Inhibits Intracellular Monoclonal Antibody Degradation binds of to LDL-R PCSK9 and inhibits Binding to the LDL-Receptor PCSK9 mab Plasma LDL LDL-R Recycling LDL-R Endocytosis Hepatocyte Endosome PCSK9 Self-procession Lysosome LDL Degradation Nucleus Endoplasmic Reticulum (ER) Golgi Apparatus 2013 Amgen Canada Inc. All rights reserved. Qian YW, et al. J Lipid Res. 2007;48: ; Horton JD, et al. J Lipid Res. 2009;50(suppl):S172-S177.




40 MOA of PSCK9i differs from statins STATINS Statins inhibit HMG-CoA reductase Cholesterol synthesis falls and LDL-receptor production rises leading to increased LDL-C clearance PCSK9 Inhibitors PCSK9 inhibitors uncouple PCSK9 from LDL-receptors LDL-receptor degradation declines while LDL-receptor recycling increases, both promoting LDL-C clearance
41 PCSK9 Inhibitors: Opportunities for Further LDL-C Reduction Targeted therapy to lower LDL-C New MOA enables LDL receptor recycling Further reduction of LDL-C Certain high risk patients do not achieve optimal lipid lowering with statins Further reduction of LDL-C may reduce CV risk Challenges with optimizing statins Many high-risk Canadians are not at LDL-C goal due to challenges with statin dose, tolerance and adherence PCSK9 LDL-R LDL-C 1. Goodman SG, et al, on behalf of the DYSIS Canadian Investigators. Can J Cardiol. 2010;26(9):e330-e Steinberg D, Witztum JL. Proc Natl Acad Sci USA. 2009;106(24):
42 Mean LDL-C Level (mmol/l) Coronary Heart Disease (%) Patients with Less PCSK9 due to Loss-of-function Mutations have Lower Serum LDL-C and Significantly Lower Incidence of CHD 5 LDL-C Levels 15 Rate of Cardiovascular Disease P < % P = for the reduction HR, % CI, 0.02 to 0.81 P = No PCSK9 Mutation N=3278 PCSK9 142X or PCSK9 679X PCSK9 -ve Mutation N=85 0 No PCSK9 Mutation 1.2% PCSK9 ve Mutation PCSK9 142X or PCSK9 679X Lifetime exposure to lower LDL results in dramatic reduction in CV rates Cohen JC, et al. N Engl J Med. 2006;354:
43 PCSK9 Inhibitors and Their Indications Alirocumab 1 Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with HeFH Clinical ASCVD Evolocumab 2 Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with HeFH Clinical ASCVD Adjunct to diet and other LDL-C lowering therapies in persons 12 years with HoFH who require additional LDL-C lowering ASCVD, atherosclerotic cardiovascular disease; HeFH, heterozygous familial hypercholesterolemia; HoFH, homozygous familial hypercholesterolemia; LDL-C, low density lipoprotein cholesterol; PCSK9, proprotein convertase subtilisin kexin type Praluent Canadian Product Monograph, April 11, 2016; 2. IRepatha Canadian Product Monograph, June ;
44 Overview of PCSK9 Inhibitor Clinical Trial Populations Hypercholesterolemia Population Moderate-high risk patients with LDL above guidelines targets ( 1.9 mmol/l) while on optimal statin/lipid lowering therapy* * Dependent of study, baseline statin and risk HeFH Population HeFH patients meeting guidelines definition* (i.e. Simon Broom, Dutch Lipid Network Criteria) LDL-C 1.8 or 2.6 mmol/l while on statin therapy* * Study dependent Statin Intolerant Population Unable to tolerate 2 statins at any dose or above the minimum dose LDL above target levels (very high risk >1.8 mmol/l or moderate high risk 2.6 mmol/l) PCSK9i Phase III Clinical Studies in Each Population LAPLACE-2 (N=1700) (Evolocumab) ODYSSEY Combo II (N=660) (Alirocumab) RUTHERFORD-2 (N=300) ODYSSEY FH (N=471) ODYSSEY HIGH FH (N=105) GAUSS-2 (N=300) ODYSSEY Alternative (N=250) intolerant to 2 statins (evolocumab) or unable to tolerate at least 2 different statins, including one at lowest dose, due to muscle-related symptoms (alirocumab) HeFH: Heterozygous Familial Hypercholesterolemia Clinicaltrials.gov accessed Aug 25, 2015.
45 Safety of PCSK9i and Achieving Very Low LDL-C Levels Safety profile for alirocumab and evolocumab is similar to comparators (placebo and ezetimibe) across a range of patient types No major increase in AEs was observed in patients who reached low or very low LDL-C including muscle-related, neurocognitive dysfunction, liver enzymes or diabetes Joseph L, Robinson JG. Prog Cardiovasc Dis. 2015;58(1):19-31; Sabatine MS, et al. N Engl J Med. 2015;372(16):
46 FOURIER, ODYSSEY and OSLER: Key entry criteria FH ASCVD ODYSSEY OSLER FOURIER HeFH established CHD/CVD or CHD risk equivalents HeFH, ASCVD ASCVD Risk Factors Non-FH individuals with hypercholesterolemia and established CHD/CVD or CHD risk equivalents Hypertension, Diabetes Mellitus, Metabolic Syndrome, CAD, MI, PAD History of MI, nonhemorrhagic stroke or PAD LDL-C Levels LDL-C 1.8 mmol/l or non-hdl-c 2.6 mmol/l or ApoB 0.8 g/l LDL-C 1.9 mmol/l LDL-C 1.8 mmol/l or non-hdl-c 2.6 mmol/l Baseline Therapies On maximally tolerated statin other LLT On statin other LLT* On at least moderate intensity statin (atorvastatin 20 mg OD or equivalent) other LLT *MENDEL participants had no background statin therapy since evolocumab was investigated as monotherapy. ASCVD, a atherosclerotic cardiovascular disease; CAD, coronary artery disease; CHD, coronary heart disease; CVD, cardiovascular disease; HDL-C, high-density lipoprotein cholesterol; HeFH, heterozygous familial hypercholesterolemia; hscrp, high sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; LLT, lipid lowering therapy; MI, myocardial infarction; PAD, peripheral arterial disease. Adapted from Sabatine MS et al. Am Heart J. 2016;173:94-101; Sabatine MS et al. N Engl J Med. 2015;372:1500-9; Schwartz GG et al. Am Heart J. 2014;168:682-9; clinicaltrials.org, accessed Jan 20, 2017.

47 % Difference from placebo Short-term PCSK9i treatments significantly reduced LDL-C in statin-treated individuals with HeFH or ASCVD 0% Alirocumab 75 mg Q2W Alirocumab 75/150 mg Q2W Alirocumab 150 mg Q2W Evolocumab 140 mg Q2W Evolocumab 420 mg QM -10% -20% -30% -40% -36% -50% -48% -46% -43% -60% -70% -80% -54% -59% HeFH* Clinical ASCVD -61% -60% -74% -63% ASCVD, atherosclerotic cardiovascular disease; HeFH, heterozygous familial hypercholesterolemia. *Participants in the alirocumab groups were on a maximally tolerated dose of statin, those in the evolocumab groups were on statin therapy; Participants in the alirocumab groups were on a maximally tolerated dose of statin, those in the evolocumab groups were on maximum dose statin therapy. Praluent (alirocumab) Canadian Product Monograph. April 11, 2016; Repatha (evolocumab) Canadian Product Monograph. December
48 Patients on Statin Therapy who Require Additional LDL-C Reduction LDL-C Lowering Efficacy of PCSK9 Inhibitors on Background Statin Therapy 0% Alirocumab 75 mg Q2W Alirocumab 75/150 mg Q2W Alirocumab 150 mg Q2W Evolocumab 140 mg Q2W Evolocumab 420 mg QM -10% -20% -30% -40% -36% -50% -48% -46% -43% -60% -70% -80% -54% -59% -61% -60% -74% -63% Heterozygous Familial Hypercholesterolemia Praluent (alirocumab) Canadian Product Monograph. April 11, Repatha (evolocumab) Canadian Product Monograph. June Clinical ASCVD

49 % meeting LDL-C <1.8 mmol/l target % meeting LDL-C <1.8 mmol/l target PCSK9i therapy significantly increases LDL-C <1.8 mmol/l achievement among statintreated individuals with uncontrolled hypercholesterolemia Placebo Alirocumab (75 mg Q2W; increased to 150 mg Q2W at week 12 if week 8 LDL-C 1.8 mmol/l) Evolocumab (140 mg Q2W or 420 mg QM) Weeks Weeks 80 # * Baseline LDL-C (mmol/l) ODYSSEY Combo I Study ODYSSEY Long Term Study * P<0.001; # P<0.0001; P<0.05 Kereiakes DJ et al. Am Heart J. 2015;169: ; Robinson JG et al. JAMA. 2014;311: LAPLACE-2 Study
50 Evolocumab with background Statins Significant LDL-C Lowering with Monthly or Bi-weekly Fixed Dosing Q2W LAPLACE % QM Placebo wk10&12 EvomAb wk10& % Combo with Statin Study (n = 1,899) % Change from Baseline in LDL-C % Q2W 62% RUTHERFORD-2 +2% QM 64% 1º hypercholesterolemia/mixed dyslipidemia LDL-C criteria 2.1 to 3.9 mmol/l depending on baseline statin use Combination with statin: Atorva 10mg, 80mg, Rosuva 5mg, 40mg or Simva 40mg Placebo or EZE (not shown) controlled LDL lowering consistent regardless if added to high or moderate intensity statin HeFH Study (N = 331) % 64% HeFH patients unable to achieve an LDL-C < 2.6 mmol/l despite statin therapy with or without ezetimibe ~ 60% LDL lowering in this difficult patient group Reflexive LDL-C measurements; Co-primary Endpoints: Mean % change from baseline in LDL at week 10/12 Adapted from Robinson JG, et al. JAMA. 2014;311(18): (LAPLACE-2); Raal F, et al. Lancet. 2015;385(9965): (RUTHERFORD-2). HeFH: Heterozygous Familial Hypercholesterolemia
51 % change from baseline in calculated LDL-C at 24 weeks Alirocumab: Phase III LDL-C Lowering Summary with statin background (Combo with Statin) Q2W N=467 COMBO II EZE N= % N=163 FH I FH II (HeFH, Combo with Statin) N=322 Q2W 2.8% N=81 N=166 Combo with Statin Study (n = 707) High CV risk LDL-C <1.8 mmol/l+ CVD history; < 2.6 mmol/l no CVD history Combination with statin: Atorva, Rosuva or Simva stable dose; Comparator EZE -20 ~30% more LDL reduction vs ezetimibe % ODYSSEY FH (n = 732) HeFH patients 1.8 mmol/l with a history of documented CVD or HeFH patients with 2,6 mmol/l with no CVD history Combination with statin: Atorva, Rosuva or Simva stable dose Comparator placebo % (18.4% had dose increase at W12) 48.8% 48.7% (43.4% had dose increase at W12) (38.6% had dose increase at W12) ~ 50% LDL lowering in this difficult patient group Placebo Alirocumab Ezetimibe FH: Familial Hypercholesterolemia; HeFH: Heterozygous Familial Hypercholesterolemia Kastelein JJP, et al. Presented at ESC Sept 2014 (FH I & FH II);Cannon CP, et al. Presented at ESC Sept 2014 (COMBO II).
52 Evolocumab: Significant LDL-C Lowering with Monthly or Biweekly Dosing in Statin Intolerant Patients 10 GAUSS-2 Q2W QM 0 Statin-Intolerant Study (N = 307) % Change from Baseline in LDL-C % -16.6% Patients intolerant to 2 statins LDL-C >1.8 mmol/l Placebo and EZE comparator Robust efficacy combined with favourable tolerability at 12 weeks Mean LDL-C reduction of 2.7mmol/L at week % Ezetimibe wk10& % EvoMab wk10&12 Reflexive LDL-C measurements; Co-primary Endpoints: Mean % change from baseline in LDL at week 10/12 and at Week 12 Adapted from Stroes E, et al. J Am Coll Cardiol. 2014;63(23): (GAUSS-2).
53 Mean Calculated LDL-C (mmol/l) ODYSSEY Long-Term showed sustained LDL-C reduction with alirocumab + statin therapy in individuals with HeFH or ASCVD mmol/l 3.17 mmol/l 0.8% 3.6% % reduction, P<0.001 Absolute reduction: 1.2 mmol/l 1.25 mmol/l -61.0% 1.50 mmol/l -52.4% No. of patients with data available Placebo Alirocumab Alirocumab + maximally tolerated statin ± other LLT Placebo + maximally tolerated statin ± other LLT Week CHD, coronary heart disease; HeFH, heterozygous familial hypercholesterolemia; LDL-C, low-density lipoprotein cholesterol; LLT, lipid lowering therapy. Robinson J et al. N Engl J Med. 2015;372:


54 OSLER- Long Term demonstrated sustained LDL-C reduction with evolocumab + standard therapy in individuals with HeFH, hypercholesterolemia or statin intolerance mmol/l Evolocumab plus standard of care Standard of care alone 61% reduction (95%CI 59-63%), P< Absolute reduction: 1.9 mmol/l 1.2 mmol/l 0 (Parent study) (OSLER) N=4465 N=1258 N=4259 N=4204 N=1243 N=3727 HeFH, heterozygous familial hypercholesterolemia, Sabatine MS et al. N Engl J Med. 2015;372:
55 Proportional reduction in event rate (SE) Results from ODYSSEY Long-Term, OSLER-1 and OSLER-2 align with the LDL Hypothesis 60% 50% 40% ODYSSEY Long-Term* OSLER* 30% 20% 10% 0% -10% Reduction in LDL-cholesterol (mmol/l) * Based on exploratory endpoints from Phase 3 trials Waters DD. Hsue PY. Circ Res. 2015;16:
56 Cumulative probability of event ODYSSEY Long-Term, post-hoc analysis, revealed lower CV event rates in the alirocumab arm 0.06 Alirocumab [150 mg q2w] + maximally tolerated statin ± other LLT (27 events*; N=1550) Placebo + maximally tolerated statin ± other LLT (26 events*; N=788) HR = 0.52 (95% C.I 0.31 to 0.90) Nominal P value = 0.02 Mean treatment duration: 70 weeks 48% RRR Time (weeks) Placebo Alirocumab *, adjudicated major adverse cardiovascular events in post hoc analysis CV, cardiovascular; LLT, lipid-lowering therapy. Robinson JG et al. N Engl J Med ;372:
57 % change from baseline in calculated LDL-C at week 24 Alirocumab: Phase III LDL-C Lowering Summary in Statin Intolerant Patients 10 0 Alternative (Statin intolerant ) Q2W EZE N=126 N=122 Statin-Intolerant Study (n = 248) % Intolerant to 2 statins Very high CV risk with LDL-C 1.8 mmol/l or moderate high risk with LDL-C 2.6 mmol/l EZE comparator % of patients achieved LDL-C goals at week % -60 Alirocumab Ezetimibe Alirocumab 75 mg with potential to 150 mg Q2W SC at week 12 LDL-C >1.8mmol/L Unable to tolerate at least 2 different statins, including one at lowest dose, due to muscle-related symptoms. Moriarty PM, Thompson PD, Cannon CP, et al J Cin Lipidology Published online August 29, 2015
: up to 94% 1 ODYSSEY Combo I Study (Alirocumab): 75% 2 ODYSSEY Long Term Study (Alirocumab): 80% 3 *LDL-C goal = 1.8 mmol/l 1. Robinson JG, et al. JAMA.")
58 With PCSK9i More Patients Achieve LDL-C Goals * High Risk Patients on background statin therapy achieved an LDL-C target of <1.8 mmol/l LAPLACE-2 Study (Evolocumab): up to 94% 1 ODYSSEY Combo I Study (Alirocumab): 75% 2 ODYSSEY Long Term Study (Alirocumab): 80% 3 *LDL-C goal = 1.8 mmol/l 1. Robinson JG, et al. JAMA. 2014;311(18): Kereiakes DJ, et al. Am Heart J 2015;169: e Robinson J, et al. N Engl J Med. 2015;372(16):
59 Median Change in PAV (%) Intensive LDL-C Lowering Promotes Plaque Regression LDL-C Levels and Atherosclerosis Progression in IVUS Studies 1, ASTEROID Rosuvastatin REVERSAL Atorvastatin SATURN Rosuvastatin STRADIVARIUS Placebo CAMELOT Placebo ILLUSTRATE Atorvastatin PRECISE-IVUS (ACS) Atorvastatin SATURN Atorvastatin PRECISE-IVUS (ACS) Atorvastatin+Ezetimibe REVERSAL Pravastatin Average On-Treatment LDL-C (mmol/l) On treatment duration ranged from 10 to 24 months 1. Puri R et al. Am Heart J. 176:83-92; 2. Kenichi T et al J Am Coll Cardiol. 2015: 66:
60 Randomization 1:1 to study drug GLAGOV: Effect of Evolocumab on Coronary Plaque Area Volume (PAV) Clinically indicated coronary angiogram + IVUS LDL-C 2.07 mmol/l +/- additional risk factors, or 1.55 but < 2.07 mmol/l plus 1 major or 3 minor risk factors Up to 4-week lipid stabilization period Assigned to background statin therapy Placebo SC every month Evolocumab 420 mg SC every month Primary endpoint: Nominal change* in PAV from baseline to week 78 per IVUS 2 4 weeks Maximum 6 weeks Study visits: D1 W4 W12 W24 W36 W52 W64 W76 W78 W80 EOS Study drug was administered monthly at home or in the clinic Last Last dose of IVUS study procedure drug GLAGOV: Global Assessment of Plaque ReGression with a PCSK9 AntibOdy as Measured by IntraVascular Ultrasound IVUS, intravascular ultrasound; PAV, percentage atheroma volume; SC, subcutaneously; TAV, total atheroma volume. Nicholls SJ et al. JAMA. 2016;316:
61 GLAGOV: Baseline Characteristics and Statin Usage Parameter Placebo (N = 484) Evolocumab (N = 484) Age, years* 59.8 (8.8) 59.8 (9.6) Men 72.3% 72.1% Previous PCI 38.8% 39.0% Previous MI 35.3% 34.9% Diabetes 21.5% 20.2% LDL-C (mmol/l) 2.39 (2.33 to 2.46) 2.40 (2.33 to 2.46) Baseline statin use 98.3% 98.8% High intensity 59.9% 57.9% Moderate intensity 38.2% 40.5% Low intensity 0.2% 0.4% *, data expressed as mean (SD);, data expressed as mean (95% CI);, treated with statin at the end of the lipid stabilization period at randomization; as defined by the America College of Cardiology/American Heart Association criteria.
62 Absolute LDL-C Change From Baseline (mmol/l) GLAGOV: Change in LDL-C and PAV Change in % atheroma volume (%) Evolocumab Add-on to Optimized Statin Therapy Significantly Lowered LDL-C With Appreciable Reduction in Atheroma Mean LDL-C 2.41 mmol/l* Change from baseline 3.9% % (-0.32 to 0.42) 0.5 Placebo Evolocumab 0.5 P = NS* No. of patients Placebo 484 Evolocumab Mean LDL-C 0.95 mmol/l* Change from baseline -59.8% Study Week % (-1.33 to -0.58) P < 0.001* PAV Regression 17% more LDL-C patients* (64.3% vs. 47.3%) mmol/l* (2.4 vs mmol/l) PAV -1.0 %* (+0.5 vs %) *Time-weighted LDL-C. Nicholls SJ et al. JAMA. 2016;316:


63 Evolocumab Cardiovascular Outcomes Trial: Study Population FOURIER: Further cardiovascular OUtcomes Research with PCSK9 Inhibition in subjects with Elevated Risk Background lipid-lowering therapy Patients must be on an optimized lipid-lowering regimen (moderate to high intensity statin +/- ezetimibe) In general, patients are not to change open-label background lipid-lowering therapies after randomization Sabatine MS, et al. NEJM. [published online ahead of print March 17, 2017]. doi: /NEJMoa
64 FOURIER: Median LDL-C Levels Over Time: All Patients LDL Cholesterol (mmol/l) No. at risk Placebo Evolocumab 13,779 13, % mean reduction (95% CI 58-60), P < Absolute reduction: 1.45 mmol/l (95% CI ) Placebo Median 2.38 mmol/l Evolocumab Median 0.78 mmol/l Weeks 13,251 13,151 12,954 12,596 12,311 10,812 6,926 3, ,288 13,144 12,964 12,645 12,359 10,902 6,958 3, LDL-C was significantly reduced in the evolocumab group (median: 0.78 mmol/l) including 42% who achieved levels 0.65 mmol/l vs < 0.1% in the placebo group Data shown are median values with 95% confidence intervals in the two arms; ITT. Sabatine MS, et al. NEJM. [published online ahead of print March 17, 2017]. doi: /NEJMoa
65 Cumulative Incidence (%) FOURIER: Composite of CV Death, MI, Stroke, Hospitalization for UA, or Coronary Revascularization Primary Endpoint Placebo + SOC Evolocumab + SOC Months No. at Risk Placebo Evolocumab 13,780 13,784 13,278 13,351 12,825 12,939 11,871 12,070 7,610 7,771 3,690 3, HR 0.85 (95% CI 0.79 to 0.92); P < CV = Cardiovascular; MI = Myocardial infarction; UA = Unstable angina; HR = Hazard ratio Sabatine MS, et al. NEJM. [published online ahead of print March 17, 2017]. doi: /NEJMoa
66 FOURIER: Composite of CV Death, MI, or Stroke Cumulative Incidence (%) No. at Risk Placebo Evolocumab Key Secondary Endpoint Placebo + SOC Evolocumab + SOC Months 13,780 13,449 13,142 12,288 7,944 3, ,784 13,501 13,241 12,456 8,094 3, HR 0.80 (95% CI 0.73 to 0.88); P < CV = Cardiovascular; MI = Myocardial infarction; HR = Hazard ratio Sabatine MS, et al. NEJM. [published online ahead of print March 17, 2017]. doi: /NEJMoa

67 FOURIER RRR 20% ARR 2% NNT YEARS TNT RRR 22% ARR 2.2% NNT YEARS
68 FOURIER: Primary, Key Secondary, and Other Endpoints Outcome Evolocumab (n = 13,784) n (%) Placebo (n = 13,780) n (%) HR (95% CI) P- value Primary endpoint* 1344 (9.8) 1563 (11.3) 0.85 ( ) <0.001 Key secondary endpoint 816 (5.9) 1013 (7.4) 0.80 ( ) <0.001 Other endpoints CV death 251 (1.8) 240 (1.7) 1.05 ( ) 0.62 Due to acute MI 25 (0.18) 30 (0.22) 0.84 ( ) Due to stroke 31 (0.22) 33 (0.24) 0.94 ( ) Other CV death 195 (1.4) 177 (1.3) 1.10 ( ) Death from any cause 444 (3.2) 426 (3.1) 1.04 ( ) 0.54 MI 468 (3.4) 639 (4.6) 0.73 ( ) <0.001 Hospitalization for UA 236 (1.7) 239 (1.7) 0.99 ( ) 0.89 Stroke 207 (1.5) 262 (1.9) 0.79 ( ) 0.01 Ischemic 171 (1.2) 226 (1.6) 0.75 ( ) Hemorrhagic 29 (0.21) 25 (0.18) 1.16 ( ) Unknown 13 (0.09) 14 (0.10) 0.93 ( ) *CV death, myocardial infarction, stroke, hospitalization for unstable angina, or coronary revascularization CV death, myocardial infarction, or stroke. Given the hierarchical nature of the statistical testing, the P values for the primary and key secondary endpoint should be considered statistically significant whereas all other P values should be considered nominal. MI = Myocardial infarction; UA = Unstable angina Sabatine MS, et al. NEJM. [published online ahead of print March 17, 2017]. doi: /NEJMoa


69 More Intensive LDL-C Lowering and CV Mortality 1. Cannon CP, et al. N Engl J Med. 2004;350: de Lemos JA, JAMA 2004;292: LaRosa JC, et al. N Engl J Med. 2005;352: Pederson TR, et al. JAMA. 2005; 294: Search Collaborative Group. Lancet 2010; 376: Cannon CP, et al. N Engl J Med. 2015;372: Sabatine MS, et al. American College of Cardiology 66th Annual Scientific Session Late-Breaking Clinical Trial. Washington, D.C. March 17, 2017.
70 FOURIER: Adverse Events and Laboratory Measures in the Safety Population* Adverse Events, n (%) Evolocumab (N = 13,769) Placebo (N = 13,756) Injection-site reaction** 296 (2.1) 219 (1.6) Allergic reactions 420 (3.1) 393 (2.9) Muscle-related event 682 (5.0) 656 (4.8) Rhabdomyolysis 8 (0.1) 11 (0.1) Cataract 228 (1.7) 242 (1.8) Adjudicated case of new-onset diabetes 677 (8.1) 644 (7.7) Neurocognitive event 217 (1.6) 202 (1.5) Laboratory results - n/total n (%) Aminotransferase >3x ULN 240/13,543 (1.8) 242/13,523 (1.8) Creatinine kinase >5x ULN 95/13,543 (0.7) 99/13,523 (0.7) *Safety evaluations included all randomized patients who received at least one dose of study treatment and for whom post-dose data are available. **The between-group difference was nominally significant (P<0.001). HR 1.05 (95% CI ); denominators of 8337 (evolocumab) and 8339 (placebo) because patients with prevalent diabetes at the start of the trial were excluded. Incidence of neurocognitive events, cataracts, and new-onset diabetes were similar between the two arms Post-baseline anti-evolocumab antibodies were detected in 0.3%, with no neutralizing antibodies detected ULN = Upper Limit of Normal Sabatine MS, et al. NEJM. [published online ahead of print March 17, 2017]. doi: /NEJMoa
71

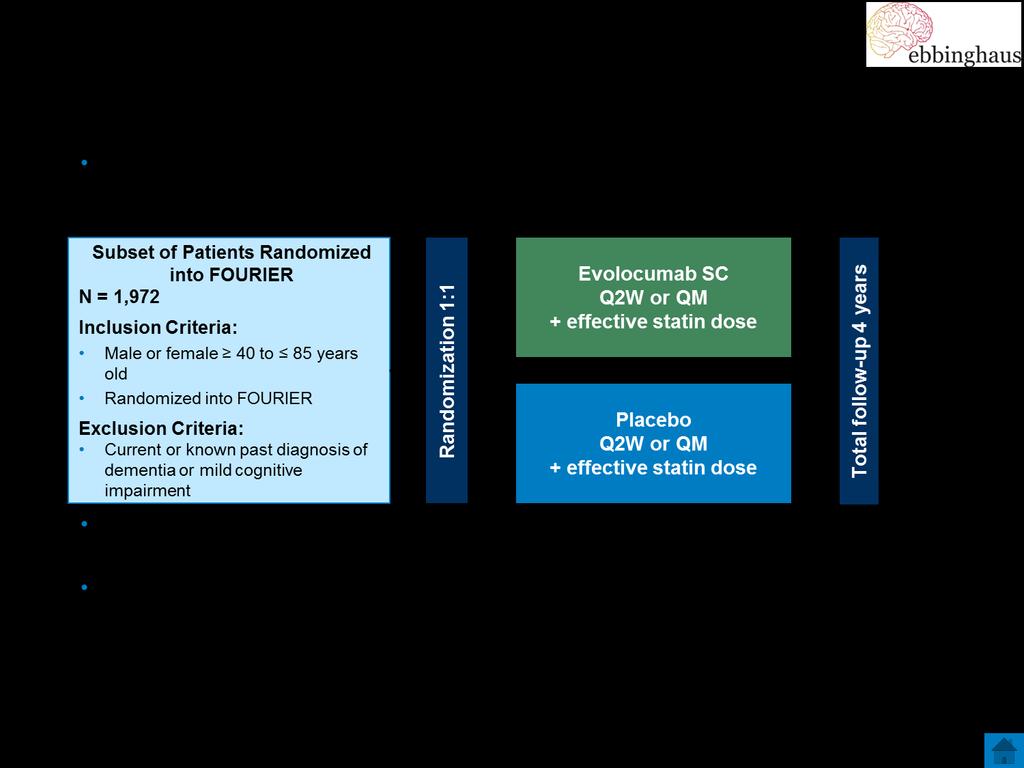
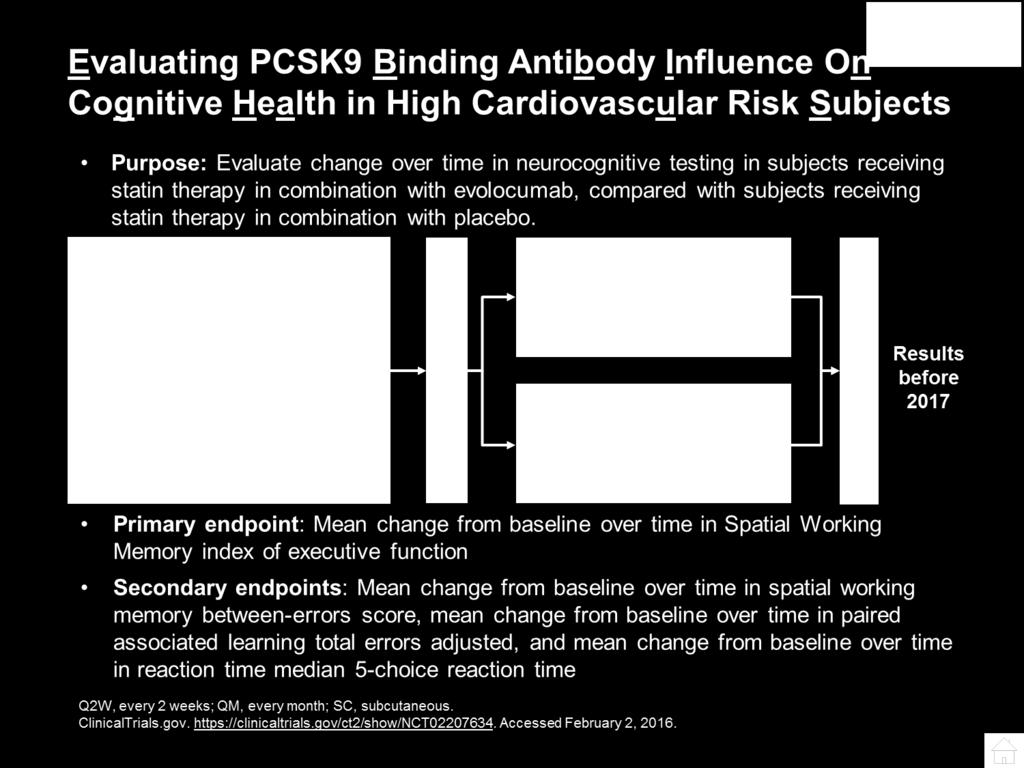
72 Results and Conclusions In patients with known cardiovascular disease on background statin followed for 20 months 1. No differences between evolocumab vs placebo A. A battery of cognitive tests B. Patient-reported everyday cognition C. Adverse cognitive events reported by MD 2. No evidence of differences in cognitive tests by achieved nadir LDL-C, even <25 mg/dl
73 PCSK9i are Demonstrating a Further Reduction in LDL-C and an Impact on CV Events LDL-C Reduction: PCSK9i achieve a 50-60% further reduction in LDL-C when added to statin therapy Safety of PCKS9i: no safety signals to date Safety of very low LDL-C: Little to no evidence to show that very low LDL-C has cause for concern (genetic, statin data, PCSK9i data) CV risk: Initial outcome data with PCSK9i to date have suggested CV event reduction Stein EA, Raal FJ. Best Pract Res Clin Endocrinol Metab. 2014;28(3):

74 HOW TO SCREEN AND IDENTIFY THE PCSK9I PATIENT?
75 Who is the high risk patient appropriate for PCSK9i Anderson TJ1, Grégoire J, et al. Can J Cardiol. 2016;32(11): ; Genest J et al. Can J Cardiol. 2014;30:
76 2016 CCS Lipid Guidelines Recommend: PCSK9 inhibitors for ASCVD and FH PCSK9 INHIBITORS ASCVD with sub-optimal LDL-C despite taking maximally tolerated statin ± ezetimibe PCSK9 INHIBITORS Heterozygous FH with sub-optimal LDL-C despite taking maximally tolerated statin ASCVD, atherosclerotic cardiovascular disease; CCS, Canadian Cardiovascular Society, FH, familial hypercholesterolemia, PCSK9, proprotein convertase subtilisin/kexin type 9 Anderson TJ1, Grégoire J, et al. Can J Cardiol. 2016;32(11):
 APOB,")
 or Physical findings in patient Management: Diet, lifestyle Drugs to reduce LDL-C by > 50% If CVD, LDL-C target should be <2 mmol/l Cascade screening of")

77 2014 CCS Guidance: FH Screening in Adults Early identification is the cornerstone of CVD prevention All adults with FH should be considered high risk due to lifelong exposure to high LDL-C LDL cholesterol > 5 mmol/l + Rule out secondary causes: - + Clinical diagnosis of FH Genetic diagnosis of FH Mutation in LDLR (major gene) APOB, PSCK9 (secondary genes) other minor genes Positive family history First degree relative with LDL-C > 5 mmol/l or Early coronary heart disease (<65 years in women, 55 years in men) or Physical findings in patient Management: Diet, lifestyle Drugs to reduce LDL-C by > 50% If CVD, LDL-C target should be <2 mmol/l Cascade screening of family members CVD, cardiovascular disease; FH, familial hypercholesterolemia; LDL-C, low-density lipoprotein cholesterol; LDLR, LDL receptor. *patients with severe HeFH or HoFH will likely require aggressive and complex therapy to reach this target. CCS, Canadian Cardiovascular Society. Genest J et al. Can J Cardiol. 2014;30:


78 FH is an autosomal genetic disease FH Heterozygotes (1/200-1/500) FH Homozygote (1/1000,000) LDL-C > mmol/l >10-13 mmol/l LDL-C receptors ½ the number None to few functional Cardiovascular presentation ~20-fold increased risk of CHD in untreated patients 5% of all heart attacks in persons <60 years old Widespread severe atherosclerosis Heart attacks in childhood CHD, coronary heart disease; LDL-C, low-density lipoprotein cholesterol. Goldstein JL, Brown MS. Arterioscler Thromb Vasc Biol. 2009;29: ; Moorjani S, et al. Arteriosclerosis.1989;9:211-6; Al-Sarraf A, et al. Can J Cardiol. 2013;29:6-9; Nordestgaard BG, et al. Eur Heart J. 2013;34: ; Cuchel M, et al. Eur Heart J. 2014;35:
79 PCSK9 Inhibitors and Their Indications Alirocumab 1 Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with HeFH Clinical ASCVD Evolocumab 2 Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with HeFH Clinical ASCVD Adjunct to diet and other LDL-C lowering therapies in persons 12 years with HoFH who require additional LDL-C lowering ASCVD, atherosclerotic cardiovascular disease; HeFH, heterozygous familial hypercholesterolemia; HoFH, homozygous familial hypercholesterolemia; LDL-C, low density lipoprotein cholesterol; PCSK9, proprotein convertase subtilisin kexin type Praluent Canadian Product Monograph, April 11, 2016; 2. IRepatha Canadian Product Monograph, June ;

 140 mg Q2W 420 mg QM ASCVD, atherosclerotic cardiovascular disease; HeFH, heterozygous familial hypercholesterolemia; HoFH, homozygous familial hypercholesterolemia; LDL-C, low")
80 PCSK9 inhibitors: Indications and dosings Alirocumab 1 Evolocumab 2 INDICATIONS AUTOINJECTOR DOSES DOSING Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with HeFH Clinical ASCVD 75 mg/ml in 1 ml 150 mg/ml in 1 ml Starting: 75 mg Q2W Maximum: 150 mg Q2W Adjunct to diet and maximally tolerated statin therapy where additional LDL-C lowering is needed in adults with HeFH Clinical ASCVD Adjunct to diet and other LDL-C lowering therapies in persons 12 years with HoFH who require additional LDL-C lowering 140 mg in 1 ml 420 mg in 3.5 ml (120mg/mL) 140 mg Q2W 420 mg QM ASCVD, atherosclerotic cardiovascular disease; HeFH, heterozygous familial hypercholesterolemia; HoFH, homozygous familial hypercholesterolemia; LDL-C, low density lipoprotein cholesterol; PCSK9, proprotein convertase subtilisin kexin type Praluent Canadian Product Monograph, April 11, 2016; 2. Repatha Canadian Product Monograph, December
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
New Horizons in Dyslipidemia Management in Primary Care
 New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Cholesterol, guidelines, targets and new medications
 Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Challenges in lipid management
 Challenges in lipid management Milan Gupta MD, FRCPC, FACC State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University of Toronto
Challenges in lipid management Milan Gupta MD, FRCPC, FACC State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University of Toronto
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine
 Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine The new england journal of medicine Original Article Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes
Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine The new england journal of medicine Original Article Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP
 Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update. November 17 th, 2018
 CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update November 17 th, 2018 Faculty/Presenter Disclosure Faculty: Rick Ward Relationships with commercial interests: Grants/Research Support:
CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update November 17 th, 2018 Faculty/Presenter Disclosure Faculty: Rick Ward Relationships with commercial interests: Grants/Research Support:
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: September 15, 2017 Repatha Description Repatha
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 9 Last Review Date: November 30, 2018 Repatha Description Repatha (evolocumab)
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia
 : 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
: 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
Investigator Meeting. Monday, September 12, 2016
 Investigator Meeting Monday, September 12, 2016 Principal Investigators Milan Gupta, MD, FRCPC, FACC Associate Clinical Professor of Medicine, McMaster University Brampton, ON Steering Committee David
Investigator Meeting Monday, September 12, 2016 Principal Investigators Milan Gupta, MD, FRCPC, FACC Associate Clinical Professor of Medicine, McMaster University Brampton, ON Steering Committee David
Praluent. Praluent (alirocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Clinical Policy: Evolocumab (Repatha) Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Educational Objectives. Disease Trajectories and CVD Risk Reduction. Hypercholesterolemia Support for LDL-C Causality
 Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia
 and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia") PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
PCSK9 Inhibitors DRUG POLICY BENEFIT APPLICATION
 DRUG POLICY BENEFIT APPLICATION PCSK9 Inhibitors Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
DRUG POLICY BENEFIT APPLICATION PCSK9 Inhibitors Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Statins and PCSK9 inhibitors for stroke prevention
 Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
New Approaches to Lower LDL-C
 New Approaches to Lower LDL-C CSIM 27 October 2016 Jacques Genest MD Cardiovascular Health Across the Lifespan Program McGill University Health Center Disclosure J. Genest MD 2016 Advisory Board, Speaker
New Approaches to Lower LDL-C CSIM 27 October 2016 Jacques Genest MD Cardiovascular Health Across the Lifespan Program McGill University Health Center Disclosure J. Genest MD 2016 Advisory Board, Speaker
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
EVIDENCE TO DATE EVOLOCUMAB (REPATHA)
") and Clinical Outcomes in Patients with Cardiovascular Disease, March 2017 1 CLINICAL QUESTION In patients with atherosclerotic cardiovascular disease and LDL >1.8mmol/L or non-hdl > 2.6mmol/L, how does
and Clinical Outcomes in Patients with Cardiovascular Disease, March 2017 1 CLINICAL QUESTION In patients with atherosclerotic cardiovascular disease and LDL >1.8mmol/L or non-hdl > 2.6mmol/L, how does
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Clinical Policy: Evolocumab (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017
 Reference Number: ERX.SPMN.184 Effective Date: 01/2017") Clinical Policy: (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017 Last Review Date: Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Clinical Policy: (Repatha) Reference Number: ERX.SPMN.184 Effective Date: 01/2017 Last Review Date: Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
PCSK9 inhibition across a wide spectrum of patients: One size fits all?
 PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2
 Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Established CVD Common Repatha Documentation Requirements for Patients With Primary Hyperlipidemia and Established CVD 1,2 Primary and Secondary Diagnosis Codes Primary Diagnosis: Primary hyperlipidemia
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
2/26/19. Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care. Disclosures. Faculty
 Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care Faculty v Karol E. Watson, MD, PhD Professor of Medicine/Cardiology Co-director, UCLA Program in Preventive Cardiology
Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care Faculty v Karol E. Watson, MD, PhD Professor of Medicine/Cardiology Co-director, UCLA Program in Preventive Cardiology
Clinical Policy: Lomitapide (Juxtapid) Reference Number: ERX.SPA.170 Effective Date:
 Reference Number: ERX.SPA.170 Effective Date:") Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Supplementary Online Content
 Supplementary Online Content Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and
Supplementary Online Content Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and
DYSLIPIDEMIA. Michael Brändle, Stefan Bilz
 DYSLIPIDEMIA Michael Brändle, Stefan Bilz Cardiovascular risk in patients with DM Current guidelines with emphasis on patients with DM Familial Hypercholesterolemia PCSK9-inhibitors Primary Prevention
DYSLIPIDEMIA Michael Brändle, Stefan Bilz Cardiovascular risk in patients with DM Current guidelines with emphasis on patients with DM Familial Hypercholesterolemia PCSK9-inhibitors Primary Prevention
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial
 Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Pharmacy Management Drug Policy
 SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
SUBJECT: ; Praluent (alirocumab), Repatha (evolocumab) POLICY NUMBER: Pharmacy-61 EFFECTIVE DATE: 8/15 LAST REVIEW DATE: 9/22/2017 If the member s subscriber contract excludes coverage for a specific service
Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges
 ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Clinical Policy: Evolocumab (Repatha) Reference Number: ERX.SPA.169 Effective Date:
 Reference Number: ERX.SPA.169 Effective Date:") Clinical Policy: (Repatha) Reference Number: ERX.SPA.169 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Repatha) Reference Number: ERX.SPA.169 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
THE CRUCIAL PROBLEM OF ASCVD Can New Therapeutic Options Resolve It? THE CRUCIAL PROBLEM OF ASCVD Can New Therapeutic Options Resolve It?
 James A. Underberg, MD, MS, FACPM, FACP, FNYAM, FASPC, FNLA Lipidology and Cardiovascular Disease Prevention Clinical Assistant Professor of Medicine NYU Medical School and NYU Center for CV Prevention
James A. Underberg, MD, MS, FACPM, FACP, FNYAM, FASPC, FNLA Lipidology and Cardiovascular Disease Prevention Clinical Assistant Professor of Medicine NYU Medical School and NYU Center for CV Prevention
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Problem patients in primary care Patient 4: Peripheral artery disease
 Problem patients in primary care Patient 4: Peripheral artery disease Dr Terry McCormack Hambleton Richmond Whitby Clinical Commissioning Group Research Lead 01/05/2014 Delivering clinical research to
Problem patients in primary care Patient 4: Peripheral artery disease Dr Terry McCormack Hambleton Richmond Whitby Clinical Commissioning Group Research Lead 01/05/2014 Delivering clinical research to
PCSK9 Inhibitors Current Status
 PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Fall Conference 2015 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Fall Conference 2015 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
Best Lipid Treatments
 Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Clinical Policy: Mipomersen (Kynamro) Reference Number: ERX.SPA.171 Effective Date:
 Reference Number: ERX.SPA.171 Effective Date:") Clinical Policy: (Kynamro) Reference Number: ERX.SPA.171 Effective Date: 01.11.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Kynamro) Reference Number: ERX.SPA.171 Effective Date: 01.11.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
MS Sabatine, RP Giugliano, AC Keech, PS Sever, SA Murphy and TR Pedersen, for the FOURIER Steering Committee & Investigators
 Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
LDL How Low can (should) you Go and be Safe
 you Go and be Safe") LDL How Low can (should) you Go and be Safe Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Definition of Low LDL National Health and
LDL How Low can (should) you Go and be Safe Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Definition of Low LDL National Health and
Reducing Cardiovascular Risk Through Non-Statins. Kim K. Birtcher, PharmD Joseph Saseen, PharmD
 Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Reducing Cardiovascular Risk Through Non-Statins Kim K. Birtcher, PharmD Joseph Saseen, PharmD Target Audience: Pharmacists ACPE#: 0202-0000-18-049-L01-P Activity Type: Application-based This activity
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
THIERS CHAGAS BAHIA FOURIER- ESTUDO DE INIBIÇÃO DA PCSK9 EM PACIENTES DE ALTO RISCO CARDIOVASCULAR
 FOURIER- ESTUDO DE INIBIÇÃO DA PCSK9 EM PACIENTES DE ALTO RISCO CARDIOVASCULAR THIERS CHAGAS BAHIA Global Core Content: Do not copy or distribute. Placeholder for Regional/Local Disclaimer. CONFLITO DE
FOURIER- ESTUDO DE INIBIÇÃO DA PCSK9 EM PACIENTES DE ALTO RISCO CARDIOVASCULAR THIERS CHAGAS BAHIA Global Core Content: Do not copy or distribute. Placeholder for Regional/Local Disclaimer. CONFLITO DE
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy
 PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
Guidelines on Lowering LDL-C Levels
 Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
HYPERCHOLESTEROLEMIA
 UPDATES ON HYPERCHOLESTEROLEMIA WITH EMPHASIS ON PCSK9 INHIBITORS July, 2018 Chicago by Ernesto L. Chua, MD, FACC, FACP, FPCP Board Certified in Internal Medicine Board Certified in Cardiology COL, USAF,
UPDATES ON HYPERCHOLESTEROLEMIA WITH EMPHASIS ON PCSK9 INHIBITORS July, 2018 Chicago by Ernesto L. Chua, MD, FACC, FACP, FPCP Board Certified in Internal Medicine Board Certified in Cardiology COL, USAF,
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Clinical Policy: (Repatha) Reference Number: HIM.PA.SP46 Effective Date: 01.01.18 Last Review Date: Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this
Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015. Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17
 Original Effective Date: 09/28/2015. Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17") Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015 Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17 Review Date(s): 5/4/2016, 4/17/2017, 7/10/2018 DISCLAIMER This Medical Policy
Subject: Repatha (evolocumab) Original Effective Date: 09/28/2015 Policy Number: MCP-258 Revision Date(s): 5/4/16; 4/17/17 Review Date(s): 5/4/2016, 4/17/2017, 7/10/2018 DISCLAIMER This Medical Policy
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
Nephrologisches Zentrum Göttingen GbR Priv. Doz. Dr. med. V. Schettler
 Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
Therapeutic algorithm for Patients with severe Hypercholesterolemia or isolated Lipoprotein(a)-Hyperlipoproteinemia with progressive cardiovascular disease: PCSK9- Inhibitors, Lipoprotein Apheresis or
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
Study 2 ( ) Pivotal Phase 3 Study Top-Line Results. October 29, 2018
 Pivotal Phase 3 Study Top-Line Results. October 29, 2018") Study 2 (1002-047) Pivotal Phase 3 Study Top-Line Results October 29, 2018 Safe Harbor Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements
Study 2 (1002-047) Pivotal Phase 3 Study Top-Line Results October 29, 2018 Safe Harbor Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements
EVOLOCUMAB Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378
 Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior