Investigator Meeting. Monday, September 12, 2016
|
|
|
- Ursula Katrina Ball
- 6 years ago
- Views:
Transcription



1 Investigator Meeting Monday, September 12, 2016

2 Principal Investigators Milan Gupta, MD, FRCPC, FACC Associate Clinical Professor of Medicine, McMaster University Brampton, ON Steering Committee David Bewick, MD, FRCP, FACP, FACC Associate Professor, Dalhousie University Saint John, NB Daniel Gaudet, MD, PhD Lipid Unit Director, Community Genomic Medicine Center Associate Professor, Université de Montréal Montréal, QC Jacques Genest, MD, CM, FRCPC, FACC, FAHA Professor, Faculty of Medicine, McGill University Montréal, QC Narendra Singh, MD, FRCPC, FACC, FAHA Clinical Assistant Professor, Medical College of Georgia at Augusta University Atlanta, GA Rob Hegele, MD, FRCPC, FACP, FAHA, FCAHS Department of Medicine, Schulich School of Medicine and Dentistry, Western University London, ON Eva Lonn, MD, MSc (HRM, McMaster), FRCPC, FACC Professor, Division of Cardiology, Department of Medicine McMaster University Hamilton, ON Daniel Ngui, MD, BSc (P.T), MD, CFPC, FCFP Vancouver, BC
3 Agenda 12:00 Introduction Dr. Milan Gupta 12:05 Practical Management, PCSK9i/Ezetimibe Dr. Milan Gupta 12:15 Lipid Guidelines Update Dr. Jacques Genest 12:25 Question and Answer Dr. Narendra Singh 12:35 REACT Protocol Review Michelle Tsigoulis 12:42 Case Report Form Review Mahesh Kajil 12:49 Good Clinical Practice Guidelines Stephanie Effendi 12:54 Question and Answer Michelle and Dr. Gupta 1:00 Closing remarks Dr. Milan Gupta

, silent MI, or resuscitated cardiac arrest.")
4 Scandinavian Simvastatin Survival Study (1994) Primary End Point: Total Mortality Secondary End Point: Major Coronary Events Proportion alive Placebo Simvastatin 30% Total mortality P=.0003 Proportion without major coronary event Placebo Simvastatin 34% Major coronary events P= Years since randomization 4S=Scandinavian Simvastatin Survival Study Group. Primary end point of trial was total mortality. Secondary end point was first major coronary event defined as coronary death, nonfatal definite or probable myocardial infarction (MI), silent MI, or resuscitated cardiac arrest. Scandinavian Simvastatin Survival Study Group. Lancet. 1994;344: Years since randomization
5 Lessons from the CTTC meta-analysis Statins lower risk to the same relative degree independent of baseline risk and baseline LDL-C The absolute risk benefit with statins is greatest in the highest risk patients High intensity vs. lower intensity statin therapy further lowers risk No RCT has tested a specific strategy of dosing statin to achieve a pre-specified LDL-C target However, evidence suggests that treatment at lower and lower levels, leading to lower and lower achieved LDL-C levels, supports a "lower is better" philosophy 1. Cholesterol Treatment Trialists (CTT) Collaboration. Lancet. 2010;376: Cholesterol Treatment Trialists (CTT) Collaborators. Lancet. 2005;366:
6 6
7 26,846 High-Risk Patients Worldwide Mean LDL = 2.6 mmol/l
8 Barriers to LDL-C Management Over reliance on diet Use of insufficient starting doses Inability to reach more aggressive targets even with high dose statin Lack of followup for uptitration Complacency with sub-optimal cholesterol values achieved Confusion around recommended lipid targets Fear of sideeffects of statins Inertia Patient Non- Adherence Media / Dr. Google 8
9 Why REACT? The benefits of LDL-C lowering in high risk patients are irrefutable. We have new evidence demonstrating that risk can be lowered with non-statin drugs (ezetimibe / IMPROVE-IT). New non-statin drugs, PCSK9 inhibitors, have been introduced into the Canadian marketplace. Updated recommendations for the diagnosis and management of statin intolerance have recently been published. We have new, evidence-based lipid guidelines in Canada. Incorporating new guidelines and drugs into clinical practice should result in better outcomes for high risk patients.
10

11 Lipid Guidelines Update Jacques Genest MD, CM, FRCPC, FACC, FAHA



12 DYSLIPIDEMIA GUIDELINES DYSLIPIDEMIA Canadian Cardiovascular Society Guidelines for the Diagnosis and Treatment of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult DYSLIPIDEMIA GUIDELINES

13 Canadian Journal of Cardiology DOI: ( /j.cjca ) Copyright 2016 Terms and Conditions

14 Canadian Journal of Cardiology DOI: ( /j.cjca ) Copyright 2016 Terms and Conditions

15 Framingham Risk Score Estimation of 10-year CVD Risk

16 Primary and Secondary Lipoprotein Determinants Recommendations We recommend that non-hdl-c and apo B should continue to be considered alternate targets to LDL-C to evaluate risk in adults Strong Recommendation, High Quality Evidence Values and preferences As clinicians are most familiar with LDL-C we continue to recommend its use as the primary target, but anticipate a shift to preferential use of non-hdl-c or apo B in the future.

17 Canadian Journal of Cardiology DOI: ( /j.cjca ) Copyright 2016 Terms and Conditions

18 Figure 2 Strong Recommendation, Moderate-Quality Evidence


19 Figure 3 Conditional Recommendation, Moderate-Quality Evidence Strong Recommendation, Moderate-Quality Evidence

20 Figure 4 Strong Recommendation, High-Quality Evidence

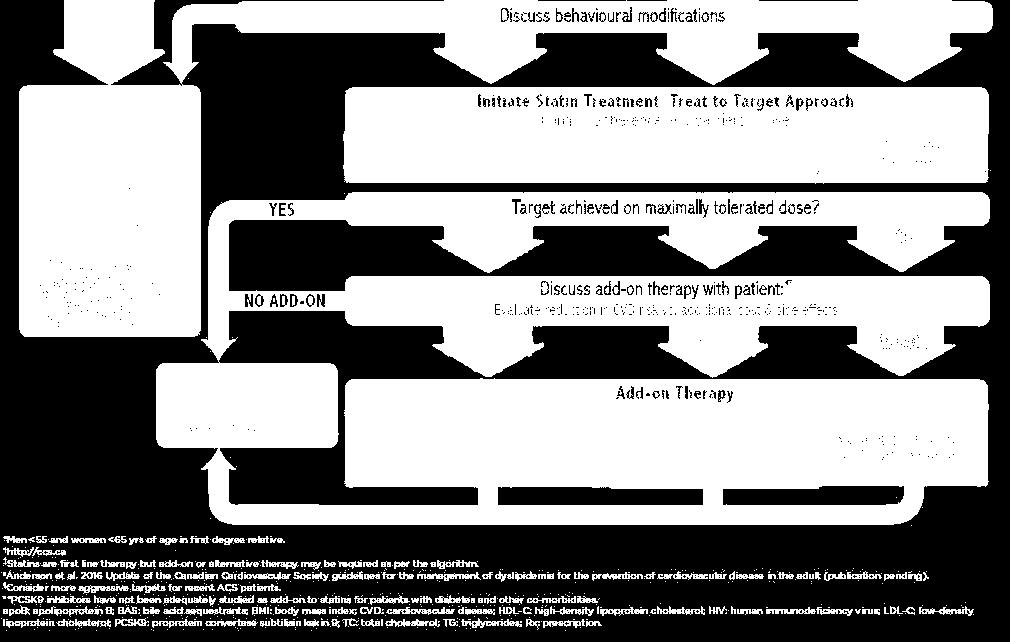
21 Approach to Risk Management
22 Figure 5 Risk Level Initiate therapy if Primary Target LDL-C High FRS 20% Intermediate FRS 10-19% Consider treatment in all (Strong, High) LDL-C 3.5 mmol/l (Strong, Moderate) For LDL-C < 3.5 consider if: Apo B 1.2 g/l or Non-HDL-C 4.3 mmol/l TARGETS 2 mmol/l or 50% decrease in LDL-C (Strong, High) 2 mmol/l or 50% decrease in LDL-C (Strong, Moderate) Alternate Target Apo B 0.8 g/l Non HDL-C 2.6 mmol/l (Strong, High) Apo B 0.8 mg/l Non HDL-C 2.6 mmol/l Low FRS <10% LDL-C 5.0 mmol/l Familial hypercholesterolemia (Strong, Moderate) 50% reduction in LDL- C (Strong, Moderate)
23
24 Practical Management, PCSK9i/Ezetimibe Milan Gupta MD, FRCPC, FACC
25 Practical Management Issues High potency statins (atorvastatin mg, rosuvastatin mg) should be used to achieve LDL-C targets. Statin intolerance Ezetimibe PCSK9 inhibitors



26 The Elephant in the Room: Goal-inhibiting Statin Intolerance (GISI) Mancini GBJ et al. Can J Cardiol 2016; 10:1016
27 Trials of Atorvastatin mg daily/intermittently Trials of Rosuvastatin 5-40 mg daily/intermittently Partial or complete intolerance Partial or complete intolerance Trials of Rosuvastatin 5-40 mg daily/intermittently Trials of Atorvastatin mg daily/intermittently Partial or complete intolerance to Atorvastatin and/or Rosuvastatin* *Other statins (Simva 40 mg, Lova 80 mg, Prava 40 mg, Fluva 80 mg) may be the only tolerated statins but due to lower potency and ineffectiveness of intermittent dosing schedules, failure to achieve goals solely through trials of these statins would not normally be considered adequate for establishing GISI. Mancini et al, DOI:
28 Practical Management Issues High potency statins (atorvastatin mg, rosuvastatin mg) should be used to achieve LDL-C targets. Statin intolerance Ezetimibe PCSK9 inhibitors
29 IMPROVE-IT Cardiovascular death, MI, documented unstable angina requiring rehospitalization, coronary revascularization ( 30 days), or stroke Hazard Ratio, (95% CI, ) p=0.016 Simvastatin: 34.7% events Mean LDL-C = 1.8 mmol/l NNT*= 50 Event Rate (%) Simvastatin/Ezetimibe: 32.7% events Mean LDL-C = 1.4 mmol/l Time since randomization (years) * NNT = Number Needed to Treat Cannon CP et al. N Engl J Med 2015;372:




30 IMPROVE-IT vs. CTT: Ezetimibe vs. Statin Benefit IMPROVE-IT CTT Collaboration. Lancet 2005; 366: ; Lancet 2010;376:

31 Non-Statin Therapy 31 Recommendations We recommend ezetimibe as second-line therapy to lower LDL- C in patients with clinical cardiovascular disease if targets are not reached on maximally tolerated statin therapy. Strong Recommendation, High Quality Evidence 31
32 Practical Management Issues High potency statins (atorvastatin mg, rosuvastatin mg) should be used to achieve LDL-C targets. Statin intolerance Ezetimibe PCSK9 inhibitors






33 In the Presence of PCSK9, the LDL-R Is Degraded and Does Not Cycle Back to Cell Surface LDL Plasma PCSK9 LDL LDL-R LDL-R Endocytosis Hepatocyte Endocytosis Endosom e PCSK9 Self-procession LDL-R Recycling Endosome LDL Degradation LDL, LDL-R and PCSK9 Degradation Nucleu s Golgi Apparatus Endoplasmic Reticulum (ER) 2013 Amgen Canada Inc. All rights reserved. Qian YW, et al. J Lipid Res. 2007;48: ; Horton JD, et al. J Lipid Res. 2009;50(suppl):S172-S177.

:S172-S177.")
34 Blocking PCSK9 Activity Inhibits Intracellular Degradation of LDL-R PCSK9 MAb Plasma LDL LDL-R Recycling LDL-R Endocytosis Hepatocyte Endosom e PCSK9 Self-procession LDL Degradation Lyosome Nucleu s Golgi Apparatus Endoplasmic Reticulum (ER) 2013 Amgen Canada Inc. All rights reserved. Qian YW, et al. J Lipid Res. 2007;48: ; Horton JD, et al. J Lipid Res. 2009;50(suppl):S172-S177.




35 PCSK9 Inhibitors Alirocumab Administration 1 injection SC q2wk, Doses: 75 mg or 150 mg Auto-injector ALIROCUMAB ALIROCUMAB Evolocumab Administration 1 injection SC q2wk, Dose: 140 mg 3 injections SC q4wk Total Dose: 420 mg Auto-injector 35
36 Evolocumab: Phase III LDL-C Lowering Summary % Change from Baseline In Reflexive LDL-C % 56.9% MENDEL-2* (Monotherapy) Q2W 0.4% 1.4% 1.3% 17.5% Q2W 57% QM GAUSS-2* (Statin Intolerance) 19.2% 56.1% 56.1% 17.8% 18.1% 19.1% 58.8% 56.1% QM 16.6% 55.3% 52.6% % % LAPLACE-2 (Combo with Statin) Q2W QM +6.8% +8.1% +3.2%+4.6% 62% 63% 64% 58% 1% 1% RUTHERFORD-2 (FH, Combo with Statin) Q2W QM 61% 61% +2% +5% 64% 56% Placebo wk10&12 Placebo wk12 EvoMab wk10&12 EvoMab wk12 Ezetimibe wk10&12 Ezetimibe wk12 *Ezetimibe comparator Koren MJ, et al. J Am Coll Cardiol. 2014;63(23): (MENDEL-2); Stroes E, et al. JACC 2014: /j.jacc (GAUSS-2); Robinson JG, et al. JAMA. 2014;311(18): doi: /jama (LAPLACE-2); Raal F, et al. Lancet Published Online October 2,
37 Alirocumab: Phase III LDL-C Lowering Summary % change from baseline in calculated LDL-C Monotherapy Q2W n=52 EZE n=51-16% -47% (26.9% had dose increase at W12) FH I 20.7% Alirocumab 75 mg with potential to 150 mg Q2W SC at week 12 LDL-C >1.8mmol/L Unable to tolerate at least 2 different statins, including one at lowest dose, due to muscle-related symptoms. Alternative Kastelein JJP, et al. Presented at ESC Sept 2014 (FH I & FH II); Roth EM, et al. Int J Cardiol Sep;176(1):55-61 (MONOTHERAPY); Cannon CP, et al. Presented at ESC Sept 2014 (COMBO II): Moriarity PM, et al. Presented at AHA Nov 2014 (Alternative). FH II COMBO II (HeFH, Combo with Statin) (Combo with Statin) (Statin intolerant ) Q2W EZE 9.1% Q2W EZE Q2W EZE 2.8% N=163 N=322 N=81 N= % 48.7% (43.4% had dose increase at W12) (38.6% had dose increase at W12) N= % (18.4% had dose increase at W12) N=240 N= % N=122 (49.5% had dose increase at W12) 14.6% Placebo Alirocumab Ezetimibe
38 Evolocumab: Adverse Event Profile at Week 52 (OSLER 1 and 2) Evolocumab + stnd of care (N=2976) Standard of care alone (N=1489) Adverse Events (%) Any 69.2% 64.8% Serious 7.5% 7.5% Leading to discontinuation of evolocumab 2.4% n/a Injection-site reactions 4.3% n/a Muscle-related 6.4% 6.0% Neurocognitive 0.9% 0.3% Laboratory results (%) ALT or AST >3 ULN 1.0% 1.2% Creatine kinase >5 ULN 0.6% 1.1% Pooled analysis from extension studies (OSLER 1 and 2) Sabatine MS, et al. N Engl J Med. 2015;372(16):
39 Alirocumab: Adverse Event Profile at Week 70 (ODYSSEY Long Term study) Alirocumab (n=1550) Placebo (N=788) Adverse Events (%) Any 81% 82.5% Serious 18.7% 19.5% Leading to discontinuation of alirocumab 7.2% 5.8% Injection-site reactions 5.9% 4.2% Muscle-related 5.4% 2.9% Neurocognitive 4.2% 4.4% Laboratory results (%) ALT & AST >3 ULN 1.8% & 1.4% 2.1% & 2.3% Creatine kinase >3 ULN 3.7% 4.9% Adverse events were defined as those that developed, worsened, or became serious after the first injection and up to 10 weeks after the last injection Adapted from Robinson J, et al. N Engl J Med. 2015;372(16):
40 Outcome Trials with PCSK9 Inhibitors Study FOURIER ODYSSEY OUTCOMES SPIRE-1/ SPIRE-2 Treatment Evolocumab: 420 mg QM or 140 mg Q2W Background: optimal lipid lowering therapy Alirocumab: 75 mg Q2W (up titrated to 150 mg Q2W if LDL >1.3 mmol/l; down titrated if LDL <0.65 mmol/l) Background: optimized lipid lowering therapy Bococizumab: 150 mg Q2W Background: lipid lowering therapy Population MI or stroke ( last 4 weeks) OR PAD (plus Risk factors for CVD) Patients hospitalized for ACS (<12 months before randomization) Patients at high risk of a CV event # patients 27,500 18,000 SPIRE-1: 17,000 SPIRE-2: 9,000 LDL-C for eligibility LDL-C 1.8 mmol/l (or non- HDL-C 2.6 mmol/l) after 4 week stabilization with optimal lipid lowering therapy 1.8 mol/l or non-hdl-c 2.6 mmol/l SPIRE-1: LDL-C 1.8 and <2.6 mmol/l SPIRE-2: LDL-C 2.6 mmol/l or non-hdl-c 3.4 mmol/l Estimated study completion 2017 December 2017 SPIRE-1:June 2018 SPIRE-2: March 2018 ACS: acute coronary syndrome; CAD: coronary artery disease; CHD: coronary heart disease; CVD: coronary vascular disease; EZE: ezetimibe; FH:Familial Hypercholesterolemia; HeFH: Heterozygous Familial Hypercholesterolemia; PAD: peripheral-artery disease; T2DM: type 2 diabetes mellitus. clinicaltrials.gov accessed August 25, 2015.
41 Non-Statin Therapy 41 Recommendations We suggest the use of PCSK9 inhibitors (evolocumab, alirocumab) to lower LDL-C for patients with heterozygous familial hypercholesterolemia whose LDL-C remains above target despite maximally tolerated statin therapy (Conditional Recommendation, Moderate Quality Evidence). We suggest that Evolocumab be added to background therapy in patients with homozygous familial hypercholesterolemia and continued if LDL-C lowering is documented (Conditional Recommendation, Moderate Quality Evidence). We suggest that PCSK9 inhibitors be considered to lower LDL-C for patients with atherosclerotic cardiovascular disease in those not at LDL-C goal despite maximally tolerated statin +/- ezetimibe therapy. Conditional Recommendation, Moderate Quality Evidence Values and preferences: Definitive outcome trials with PCSK9 inhibitors are underway but have not yet been completed. However, phase 3 efficacy trials show consistent reduction in LDL-C and reassuring trends towards reduced CV events, even though not powered for such. Given the very high lifetime risk faced by patients with FH or ASCVD, clinicians should balance the anticipated benefits of robust LDL C lowering with PCSK9 inhibitors against the lack of definitive outcomes data. 41


42 Questions and Answers Narendra Singh MD, FRCPC, FACC, FAHA
43 REACT Protocol Review Michelle Tsigoulis CCRN Executive Director
44 Protocol Review: REACT Title: Relating Evidence to Achieve Cholesterol Targets Description: An observational practice assessment. Design: A prospective, non-interventional, multicentre, practice assessment of Canadian adults with ASCVD and FH.
45 Protocol Review: REACT Primary Objective To facilitate the identification and management of patients with high residual CV risk attributable to LDL-C
46 Secondary Objectives To characterize the clinical profile, lipid levels, and treatment strategies of patients at high risk for CV events (those with ASCVD and those with FH) To provide a contemporary assessment of patients with LDL-C above target, and the potential reasons for this To enable clinicians to use evidence-based guidelines and treatments to close care gaps, resulting in more patients achieving LDL-C target levels
47 Patient Eligibility Inclusion Criteria: Consecutive subjects over 18 years of age with documented atherosclerotic cardiovascular disease (ASCVD) or familial hypercholesterolemia (FH) LDL-C level within past 3 months >3.0 mmol/l despite maximally tolerated statin treatment Willingness to give informed consent
48 Patient Eligibility Exclusion Criteria: Current use of a PCSK9 inhibitor Active participation in a randomized clinical trial involving a lipid-modifying agent Co-morbidities with anticipated life expectancy < 12 months Pregnancy or nursing mothers
49 Visit Outline Baseline - Week 0 Site follow-up Week 12 (± 4 weeks) Site follow-up Week 24 (± 4 weeks)
50 Visit 1 Patient consent Demographics Medical history and CV risk factors Vital signs and anthropometric measurements Laboratory collection (-12 to +1 wk) Concomitant therapies Investigator assessment of patient LDL-C target and goal Investigator decision regarding LDL-C/Lipidlowering therapy
51 Protocol Review: REACT Visit 2 - wk 12 and Visit 3 - wk 24 (+/- 4wks) Vital signs and anthropometric measurements Laboratory collection (+/-2wks) Concomitant therapies Investigator assessment of patient LDL-C target and goal Investigator decision regarding LDL-C/Lipidlowering therapy Assessment for adverse events/suspected adverse drug reactions since last visit Assessment for ASCVD events and/or death since last visit
52 Collection of ASCVD Events/Death Death any cause Myocardial Infarction or Acute Coronary Syndrome PCI or CABG Angiogram confirming at least 70% stenosis of a major epicardial coronary artery or at least 50% stenosis of the left main coronary artery Ischemic stroke not-attributable to atrial fibrillation Carotid revascularization by endarterectomy or stenting Peripheral arterial disease with either symptomatic with ABI < 0.9 or requiring revascularization or amputation Atherosclerosis felt to be clinically relevant by physician
53 Collection of Events The coordinating centre office will collect source documents for reported medical events occurring after the baseline visit. The site will complete the event report and fax supporting documentation to CCRN on a shuttle form.
54 Adverse Events and Suspected Adverse Drug Reactions AE s will be collected at visit 2 and 3 on the Adverse Event form. AE s suspected to be an adverse drug reaction related to any of the patient s current drug therapies will require further reporting on the Suspected Adverse Drug Reaction report form. The SADR form will capture all Events that in the investigator s opinion is believed to be potentially related to a current medical therapy. SADR form to be submitted to CCRN within 24 hours of becoming aware of the suspected adverse drug reaction.

55 Case Report Form Review Mahesh Kajil Project Manager
56 REACT Visit Schedule Visit 1 (Baseline): Week 0 Visit 2: Week 12 (+/- 4 weeks) Visit 3: Week 24 (+/- 4 weeks) All three visits are clinic visits
57 Visit 1 Baseline Inclusion Criteria PAGE #1

58 Pt ID will be prefilled. The first 3 digits corresponds to your site # and the last 2 digits will be the patient number. Visit 1-Baseline, PAGE #1 Electronic Data Capture form EDC training to be provided
59 Visit 1 Baseline PAGE #2

60 Pt ID will be auto filled Visit 1 Baseline PAGE #2 EDC
61 Visit 1 Baseline PAGE #3
62 Visit 1 Baseline PAGE #4 Question A is optional. Required only if the patient is not currently receiving a potent statin therapy Question B is required only if the patient is statin intolerant
63 Visit 1 Baseline PAGE #5
64 Visit 1 Baseline PAGE # 6 **The LDL-C target goal must be indicated by the investigator
65 Visit 1 Baseline PAGE #7 OPTIONAL
66 Visit 2/3
67 Visit 2/3
68 Visit 2/3
69 Visit 2/3 OPTIONAL
70 ASCVD or Death Event Report Form Visit 2/3
71 Adverse Event Report Form Visit 2/3

72 Suspect Adverse Drug Reaction Form Visit 2/3 Paper-based form to be faxed to CCRN within 24hrs of becoming aware of the event.

73 Good Clinical Practice Stephanie Effendi Project Coordinator
74 Definition and Goals What is GCP? GCP is defined as a standard for the design, conduct, performance, monitoring, auditing, recording, analysis, and reporting of clinical trials What are the goals of GCP? 1. To protect the rights, safety and welfare of humans participating in research 2. To assure the quality, reliability and integrity of the data collected 3. To provide standards and guidelines for the conduct of clinical research
75 3 Key Principles of GCP 1. Research is conducted by a qualified investigator 2. Informed consent 3. Ethics
76 Qualified Investigator Responsibilities Be qualified by education, training and experience Holds the overall responsibility for the conduct of the study as well as the safety and medical care of the participants. Communication with the Research Ethics Board Compliance with the protocol Maintenance of study records and reports Oversight of research staff
77 What is the Research Ethics Board? (REB) An institution that reviews the ethical acceptability of all research involving humans The review committee consists of a body of researchers, community members, and others with specific expertise (e.g. in ethics, in relevant research disciplines)
78 REB Approval Before an investigator can begin a study at his/her site, REB approval must first be obtained. The REB will review the following: Study protocol Informed consent form Any documents being provided to or to be viewed by the study subjects The REB will conduct continuing review of each ongoing trial at least once a year.
79 Informed Consent Informed consent must be obtained from all study participants prior to engaging in any study related activities.
80 How to Obtain Informed Consent Ensure the study subject meets all inclusion and exclusion criteria Provide the subject time to read the consent form and to ask questions Ensure questions are answered to the subjects satisfaction Allow the subject time to discuss participation with others Have the subject sign and date the consent form The PI or delegated study staff obtaining consent must also sign and date the consent form Provide the subject a copy of the signed consent
81 What constitutes GCP in research? Research conducted by a qualified investigator Research ethics board (REB) approval of protocol Valid informed consent Proper documentation and record keeping Accurate reporting Data verification and monitoring plan



82 Questions and Answers Milan Gupta MD, FRCPC, FACC Michelle Tsigoulis CCRN Executive Director
83 Close
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Challenges in lipid management
 Challenges in lipid management Milan Gupta MD, FRCPC, FACC State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University of Toronto
Challenges in lipid management Milan Gupta MD, FRCPC, FACC State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University of Toronto
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine
 Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine The new england journal of medicine Original Article Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes
Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine The new england journal of medicine Original Article Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
New Horizons in Dyslipidemia Management in Primary Care
 New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
PCSK9 Inhibitors: Promise or Pitfall?
 PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
PCSK9 Inhibitors: Promise or Pitfall? Tracy Harlan, PharmD PGY2 Ambulatory Care Resident University of Iowa Hospitals and Clinics tracy harlan@uiowa.edu Tracy Harlan does not have any actual or potential
Whats new in lipid management, and Can your high CV risk patients benefit from a PCSK9i?
 Whats new in lipid management, and Can your high CV risk patients benefit from a PCSK9i? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Whats new in lipid management, and Can your high CV risk patients benefit from a PCSK9i? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
New Strategies for Lowering LDL - Are They Really Worth It?
 New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
New Strategies for Lowering LDL - Are They Really Worth It? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of CV Medicine and Science Director, Ahmanson-UCLA Cardiomyopathy Center Co-Director,
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis?
 Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Does IMPROVE-IT & FOURIER Confirm or Refute the LDL Hypothesis? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Cholesterol, guidelines, targets and new medications
 Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Cholesterol, guidelines, targets and new medications Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers Grants/Research
Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges
 ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
EVIDENCE TO DATE EVOLOCUMAB (REPATHA)
") and Clinical Outcomes in Patients with Cardiovascular Disease, March 2017 1 CLINICAL QUESTION In patients with atherosclerotic cardiovascular disease and LDL >1.8mmol/L or non-hdl > 2.6mmol/L, how does
and Clinical Outcomes in Patients with Cardiovascular Disease, March 2017 1 CLINICAL QUESTION In patients with atherosclerotic cardiovascular disease and LDL >1.8mmol/L or non-hdl > 2.6mmol/L, how does
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH
 PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
PCSK9 Inhibitors Are They Worth The Money? Michael J. Blaha MD MPH Presented by: Michael J. Blaha November 16, 2017 1 Financial Disclosures Grants: Amgen Foundation, Aetna Foundation Advisory Boards: Amgen,
Statins and PCSK9 inhibitors for stroke prevention
 Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Drug Class Monograph
 Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
Drug Class Monograph Class: Proprotein Convertase Subtilisin/Kexin Type 9 (PCSK9) Inhibitor Drugs: Praluent (alirocumab), Repatha (evolocumab) Line of Business: Medi-Cal Effective Date: February 17, 2016
PCSK9 Inhibitors Current Status
 PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Fall Conference 2015 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Fall Conference 2015 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
New Approaches to Lower LDL-C
 New Approaches to Lower LDL-C CSIM 27 October 2016 Jacques Genest MD Cardiovascular Health Across the Lifespan Program McGill University Health Center Disclosure J. Genest MD 2016 Advisory Board, Speaker
New Approaches to Lower LDL-C CSIM 27 October 2016 Jacques Genest MD Cardiovascular Health Across the Lifespan Program McGill University Health Center Disclosure J. Genest MD 2016 Advisory Board, Speaker
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial
 Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
MS Sabatine, RP Giugliano, AC Keech, PS Sever, SA Murphy and TR Pedersen, for the FOURIER Steering Committee & Investigators
 Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Evolocumab Reduces Cardiovascular Events in Patients with Baseline LDL-C
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
PCSK9 Inhibitors Current Status
 PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Spring Conference 2016 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
PCSK9 Inhibitors Current Status Ryan T. Whitney, MD FACC Bryan Heart Spring Conference 2016 Disclosures, Conflicts, and Nefarious Connections I own no stock in the companies mentioned in this talk. I am
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
PCSK9 inhibition across a wide spectrum of patients: One size fits all?
 PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
PCSK9 inhibition across a wide spectrum of patients: One size fits all? PACE ESC Barcelona 2017 G.K. Hovingh MD PhD MBA dept of vascular medicine Academic Medical Center the Netherlands g.k.hovingh@amc.uva.nl
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP
 Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Cost-effectiveness of evolocumab (Repatha ) for primary hypercholesterolemia and mixed dyslipidemia.
 for primary hypercholesterolemia and mixed dyslipidemia.") Cost-effectiveness of evolocumab (Repatha ) for primary hypercholesterolemia and mixed dyslipidemia. The NCPE has issued a recommendation regarding the cost-effectiveness of evolocumab (Repatha ) Following
Cost-effectiveness of evolocumab (Repatha ) for primary hypercholesterolemia and mixed dyslipidemia. The NCPE has issued a recommendation regarding the cost-effectiveness of evolocumab (Repatha ) Following
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Workshop. Todd Anderson MD / Jacques Genest MD
 Workshop Todd Anderson MD / Jacques Genest MD Game-Changing Trials 2017 FOURIER Evolocumab n=27,564 HR 0.80 CANTOS Canakinumab n=10,061 HR 0.85 COMPASS Rivaroxaban + ASA n=27,395 HR 0.76 Key Secondary
Workshop Todd Anderson MD / Jacques Genest MD Game-Changing Trials 2017 FOURIER Evolocumab n=27,564 HR 0.80 CANTOS Canakinumab n=10,061 HR 0.85 COMPASS Rivaroxaban + ASA n=27,395 HR 0.76 Key Secondary
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
S3-13: Lipids: Looking forward to
 S3-13: Lipids: Looking forward to 2018 Heart and Stroke Clinical Update 1010-1140 9 Dec 2017 Robert Hegele MD, FRCPC, FACP Distinguished University Professor Endocrinologist, University Hospital Western
S3-13: Lipids: Looking forward to 2018 Heart and Stroke Clinical Update 1010-1140 9 Dec 2017 Robert Hegele MD, FRCPC, FACP Distinguished University Professor Endocrinologist, University Hospital Western
Drug Class Review Proprotein Convertase Subtilisin Kexin type 9 (PCSK9) Inhibitors
 Inhibitors") Drug Class Review Proprotein Convertase Subtilisin Kexin type 9 (PCSK9) Inhibitors Final Original Report July 2015 The purpose of reports is to make available information regarding the comparative clinical
Drug Class Review Proprotein Convertase Subtilisin Kexin type 9 (PCSK9) Inhibitors Final Original Report July 2015 The purpose of reports is to make available information regarding the comparative clinical
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Drug Prior Authorization Guideline PCSK9 Inhibitors -
 Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Guidelines on Lowering LDL-C Levels
 Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Scientific Insights Into LDL-C, PCSK9, and CV Risks High circulating LDL-C levels are associated with increased risk for ASCVD 1,2 Statin drugs interfere with cholesterol production, lowering serum LDL-C
Problem patients in primary care Patient 4: Peripheral artery disease
 Problem patients in primary care Patient 4: Peripheral artery disease Dr Terry McCormack Hambleton Richmond Whitby Clinical Commissioning Group Research Lead 01/05/2014 Delivering clinical research to
Problem patients in primary care Patient 4: Peripheral artery disease Dr Terry McCormack Hambleton Richmond Whitby Clinical Commissioning Group Research Lead 01/05/2014 Delivering clinical research to
PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia
 : 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
: 262-267, 2017 Περίληψη Διάλεξης PCSK9 antibodies: A new therapeutic option for the treatment of hypercholesterolemia I. Gouni-Bethold Polyclinic for Endocrinology, Diabetes, and Preventive Medicine University
CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update. November 17 th, 2018
 CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update November 17 th, 2018 Faculty/Presenter Disclosure Faculty: Rick Ward Relationships with commercial interests: Grants/Research Support:
CCC Dyslipidemia Lipid lowering/atherosclerosis clinical trials update November 17 th, 2018 Faculty/Presenter Disclosure Faculty: Rick Ward Relationships with commercial interests: Grants/Research Support:
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Clinical Policy: Evolocumab (Repatha) Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial
 Reference Number: CP.CPA.269 Effective Date: Last Review Date: Line of Business: Commercial") Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Repatha) Reference Number: CP.CPA.269 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Cost-effectiveness of evolocumab (Repatha ) for hypercholesterolemia
 for hypercholesterolemia") Cost-effectiveness of evolocumab (Repatha ) for hypercholesterolemia The NCPE has issued a recommendation regarding the cost-effectiveness of evolocumab (Repatha ). Following NCPE assessment of the applicant
Cost-effectiveness of evolocumab (Repatha ) for hypercholesterolemia The NCPE has issued a recommendation regarding the cost-effectiveness of evolocumab (Repatha ). Following NCPE assessment of the applicant
Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia. Prof. Alberto Corsini University of Milan, Italy
 Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia Prof. Alberto Corsini University of Milan, Italy Outline of the presentation State of the art on statin therapy Explore unmet
Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia Prof. Alberto Corsini University of Milan, Italy Outline of the presentation State of the art on statin therapy Explore unmet
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials?
 PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials? Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis
PCSK9 for LDL Cholesterol Reduction: What have we learned from clinical trials? Slide deck kindly supplied as an educational resource by Dr Evan A Stein MD PhD Director Emeritus Metabolic & Atherosclerosis
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
PCSK9 Inhibitors: A View of Clinical Studies
 PCSK9 Inhibitors: A View of Clinical Studies Slide deck kindly donated for website use by Professor Raul D. Santos Lipid Clinic InCor-HCFMUSP Sao Paulo, Brazil PCSK9 Inhibitors : A View of Clinical Studies
PCSK9 Inhibitors: A View of Clinical Studies Slide deck kindly donated for website use by Professor Raul D. Santos Lipid Clinic InCor-HCFMUSP Sao Paulo, Brazil PCSK9 Inhibitors : A View of Clinical Studies
EVOLOCUMAB Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378
 Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
Generic Brand HICL GCN Exception/Other EVOLOCUMAB REPATHA 42378 This drug requires a written request for prior authorization. All requests for Repatha (evolocumab) require review by a pharmacist prior
PCSK9 Inhibitors DRUG POLICY BENEFIT APPLICATION
 DRUG POLICY BENEFIT APPLICATION PCSK9 Inhibitors Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
DRUG POLICY BENEFIT APPLICATION PCSK9 Inhibitors Benefit determinations are based on the applicable contract language in effect at the time the services were rendered. Exclusions, limitations or exceptions
Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
 2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
2017 Focused Update of the 2016 ACC Expert Consensus Decision Pathway on the Role of Non-statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA
REPATHA (PCSK9 INHIBITORS)
") REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia
 and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia") PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Objectives. Hypercholesterolemia and Coronary Heart Disease. LDL Cholesterol. Hypercholesterolemia Is a Global Public Health Epidemic
 12:3 1:45 pm Dyslipidemia in Primary Care: New Guideline Recommendations and Treatment Options SPEAKERS Carl E. Orringer, MD, FACC, FNLA James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA Presenter Disclosure
12:3 1:45 pm Dyslipidemia in Primary Care: New Guideline Recommendations and Treatment Options SPEAKERS Carl E. Orringer, MD, FACC, FNLA James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA Presenter Disclosure
2/26/19. Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care. Disclosures. Faculty
 Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care Faculty v Karol E. Watson, MD, PhD Professor of Medicine/Cardiology Co-director, UCLA Program in Preventive Cardiology
Secondary Cardiovascular Risk Reduction: Incorporating Evolving Data to Individualize Care Faculty v Karol E. Watson, MD, PhD Professor of Medicine/Cardiology Co-director, UCLA Program in Preventive Cardiology
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Educational Objectives. Disease Trajectories and CVD Risk Reduction. Hypercholesterolemia Support for LDL-C Causality
 Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Simvastatin With or Without Ezetimibe in Familial Hypercholesterolemia
 Simvastatin With or Without Ezetimibe in Familial Hypercholesterolemia The trial ClinicalTrials.gov number: NCT00552097 John J.P. Kastelein, MD, PhD* Department of Vascular Medicine Academic Medical Center
Simvastatin With or Without Ezetimibe in Familial Hypercholesterolemia The trial ClinicalTrials.gov number: NCT00552097 John J.P. Kastelein, MD, PhD* Department of Vascular Medicine Academic Medical Center
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Proprotein Convertase Subtilisin/kexin type 9 Page 1 of 24 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Proprotein Convertase Subtilisin/kexin type 9 (PCSK9)
Drug Class Prior Authorization Criteria PCSK9 Inhibitors
 Drug Class Prior Authorization Criteria PCSK9 Inhibitors Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Drug Class Prior Authorization Criteria PCSK9 Inhibitors Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Management of Dyslipidaemias: PCSK9 Inhibition. Alberico L. Catapano Professor President EAS University of Milano Italy
 Management of Dyslipidaemias: PCSK9 Inhibition Alberico L. Catapano Professor President EAS University of Milano Italy Conflict of interest Grants, consulting fees and/or honoraria and delivering lectures
Management of Dyslipidaemias: PCSK9 Inhibition Alberico L. Catapano Professor President EAS University of Milano Italy Conflict of interest Grants, consulting fees and/or honoraria and delivering lectures
Dyslipidemia Treatment in 2016 Novel Agents Combination Therapies Statin Intolerance
 Dyslipidemia Treatment in 2016 Novel Agents Combination Therapies Statin Intolerance Hani Sabbour MD FACC FHRS Clinical Assistant Professor of Cardiology Brown University Rhode Island USA Consultant Cardiology
Dyslipidemia Treatment in 2016 Novel Agents Combination Therapies Statin Intolerance Hani Sabbour MD FACC FHRS Clinical Assistant Professor of Cardiology Brown University Rhode Island USA Consultant Cardiology
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Managing Lipids and Cardiovascular Risk: Using the Data to Optimize Care
 Clinical Updates for Nurse Practitioners and Physician Assistants: 2018 Managing Lipids and Cardiovascular Risk: Using the Data to Optimize Care Faculty Robert L. Gillespie, MD, FACC, FASE, FASNC Immediate
Clinical Updates for Nurse Practitioners and Physician Assistants: 2018 Managing Lipids and Cardiovascular Risk: Using the Data to Optimize Care Faculty Robert L. Gillespie, MD, FACC, FASE, FASNC Immediate
PCSK9 Inhibitors for Lowering Cholesterol: Ready for Prime Time?
 Original Article Thomas Knickelbine, MD, FACC, FSCCT, FSCAI From: Minneapolis Heart Institute at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Thomas Knickelbine, MD, FACC,
Original Article Thomas Knickelbine, MD, FACC, FSCCT, FSCAI From: Minneapolis Heart Institute at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Thomas Knickelbine, MD, FACC,
Best Lipid Treatments
 Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy
 PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for