|
|
|
- Anabel Scott
- 5 years ago
- Views:
Transcription
1 PUBLISHED VERSION Fairhurst, Katherine; Strickland, Andrew David; Bridgewater, Franklin Herbert G.; Maddern, Guy John Painless obstructive jaundice secondary to a common bile duct abscess: A delayed sequela of cholecystectomy, HPB Surgery, 2009; 2009:Article ID Copyright 2009 Katherine Fairhurst et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. PERMISSIONS /journals/hpb/guidelines/ Open Access authors retain the copyrights of their papers, and all open access articles are distributed under the terms of the Creative Commons Attribution license, which permits unrestricted use, distribution and reproduction in any medium, provided that the original work is properly cited. 13 th August
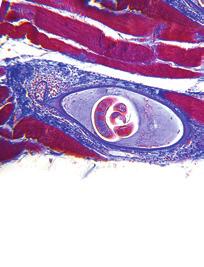
2 HPB Surgery Volume 2009, Article ID , 3 pages doi: /2009/ Case Report Painless Obstructive Jaundice Secondary to a Common Bile Duct Abscess: A Delayed Sequela of Cholecystectomy Katherine Fairhurst, Andrew Strickland, Franklin H. G. Bridgewater, and Guy J. Maddern The Queen Elizabeth Hospital, University of Adelaide Discipline of Surgery, Woodville, South Australia, SA 5011, Australia Correspondence should be addressed to Guy J. Maddern, guy.maddern@adelaide.edu.au Received 14 September 2009; Revised 20 October 2009; Accepted 16 November 2009 Recommended by Guntars Pupelis Complications related to cholecystectomy are well described. Most occur in the early postoperative period and are recognised either at the time of, or shortly after surgery. Clinical sequelae occurring years following cholecystectomy are rare and infrequently reported. In addition, most delayed complications are related to the continuing presence or new formation of gallstones. In this paper we present a unique case of an abscess of the common bile duct wall, presenting with painless obstructive jaundice more than 30 years following an open cholecystectomy, without the presence of gallstones. The clinical presentation, investigations, and treatment are discussed with a review of other relevant reported cases in the literature. Copyright 2009 Katherine Fairhurst et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 1. Introduction Commonly reported complications of cholecystectomy include damage to the common bile duct [1], bile leaks from the gallbladder bed or cystic duct stump [2], dropped gallstones [3], and damage to other structures such as the small bowel, liver, or diaphragm [4]. The complications of laparoscopic surgery have lessened with growing technical expertise, and laparoscopic cholecystectomy is now considered the gold standard [5]. However, the essential steps of a cholecystectomy remain the same. These steps include adequate visualisation of the structures to obtain the critical view, secure occlusion of the cystic duct and artery, good haemostasis, and the treatment of any bile leaks from the gallbladder bed, or bile or stone spillages from an iatrogenically perforated gallbladder. Inadequate performance of any of these steps can lead to complications many years following the initial operation, as presented in this paper, and as such attention to operative detail is of paramount importance. 2. Case Report A 70-year-old female presented to a rural hospital with painless jaundice. She had undergone a routine open cholecystectomy 30 years earlier at the same hospital. Biochemical markers showed an obstructive pattern: Bilirubin 155 μmol/l (6 24), ALP 262 U/L (30 110), ALT 272 U/L (0 55), AST 161 U/L (0 45). The white cell count was within the normal range at /L (4 11), and the CRP was mildly elevated at 11 mg/l (<8.0). In the 30-year interval, she had experienced no other episodes of jaundice, abdominal pain, or unexplained fever and had undergone no other abdominal surgery. Unfortunately the hospital records (on microfilm) were incomplete so no operation note from the cholecystectomy 30 years previously was available. The anaesthetic chart and drug chart were retrieved and revealed that no antibiotics were given and no specific intraoperative difficulty or postoperative complications were recorded in the clinical records. The patient also confirmed an uneventful recovery. She was referred to the gastroenterologists at a tertiary centre for endoscopic retrograde cholangiopancreatography (ERCP). The images at ERCP demonstrated a round filling defect approximately 2 cm in diameter associated with a smooth stricture consistent with extrinsic compression in the proximal bile duct (Figure 1). The common bile duct was cannulated without difficulty and measured 8mm in diameter. A guidewire was easily placed past the area of compression and insertion of a 10 French; 12 cm Cotton Leung biliary stent was performed. The jaundice resolved within 72 hours of the procedure. No antibiotics were given
 with the common bile duct stent seen more medially. Figure 1: Stricture of the proximal bile duct at ERCP.")


3 2 HPB Surgery 12 LAO 0 CRAN 0 MAG 1.67 SID 106 cm Zoom 100% 87 kv 10.1mAs40.5ms Figure 2: CT demonstrating lesion arising from common bile duct (arrow) with the common bile duct stent seen more medially. Figure 1: Stricture of the proximal bile duct at ERCP. at the time of the ERCP. No malignant cells were identified from the aspirated bile sent for histology. The patient was discharged the day following the ERCP and referral to the hepatopancreaticobiliary surgical team was made for further investigation into the cause of the jaundice. CT imaging demonstrated mild intrahepatic dilatation. No lesions other than a rounded soft tissue mass immediately lateral to the stent and below the porta hepatis were identified (Figure 2). This was consistent with the ERCP findings. The mass measured slightly smaller on the CT images at approximately 1.5 cm in diameter. The mass had varying density but seemed complex in nature and as such the possibility of a choledochal cyst was raised. Diagnostic laparoscopy was performed one month following the ERCP. The view was obscured by adhesions from the previous open cholecystectomy completed via a right paramedian incision. No antibiotics were given at the time of the laparoscopy. An esophagogastroduodenoscopy and colonoscopy excluded primary malignant lesions in those areas. Following extensive discussion at the hepatopancreaticobiliary multidisciplinary meeting and with the patient, it was decided that due to the diagnostic uncertainty of the obstructing tumour in the hepatic duct, laparotomy and attempted excision of the lesion should be performed. At operation, the common bile duct was identified and the lesion located within the proximal bile duct at the usual position of the insertion of the cystic duct, though the cystic duct stump itself could not be identified. The dimensions of the lesion were similar to those measured on the CT images and the common bile duct again measured 8 mm in diameter. During dissection pus started exuding from the duct wall. A sample was sent for microbiological analysis. No bile was seen in the purulent discharge and probing of the underlying cavity did not reveal a communication with the common bile duct. Because of the possibility of malignancy, the common Figure 3: T-tube cholangiogram demonstrating resolution of the stricture. bile duct was opened and choledochoscopy showed normal primary and secondary bifurcations of the common bile duct, a normal duct distally and no apparent communication with the abscess cavity. The lateral wall of the abscess cavity was resected and sent for histology. This confirmed mild, chronic nonspecific inflammation and fibrosis only. The stent placed at ERCP three months previously was removed and the tip sent for culture. Because the medial wall of the common bile duct was found to be thinned and delicate due to the abscess formation and consequent resection, a T-tube was inserted and sutured into position. Intravenous cephazolin and metronidazole were given intraoperatively as part of the hospital microbiology guidelines for antibiotic prophylaxis of biliary tract surgery. These antibiotics were given for 4 days postoperatively with the addition of gentamycin, whilst culture results were awaited. Klebsiella ornithinolytica and Enterococcus casseliflavus were subsequently identified and were sensitive to the prescribed antibiotic regime. The postoperative recovery was uneventful with no episodes of sepsis. A T-tube cholangiogram thirteen days postoperatively showed no abnormalities (Figure 3). The tube was clamped following the cholangiogram and removed without incident two weeks later.
4 HPB Surgery 3 3. Discussion Complications relating to cholecystectomy have been extensively documented throughout the literature. The diagnostic difficulties associated with nonmalignant, biliary strictures such as those caused by autoimmune processes, have also been discussed [6]. This case of an abscess forming within the wall of the common bile duct presenting as obstructive painless jaundice more than 30 years following this procedure and without the presence of gallstones, appears to be unique in the literature to date. The most logical explanation for this outcome is that of a small leak from the cystic duct stump with the formation of a chronic abscess. The possibility of iatrogenic injury at the time of ERCP is unlikely because the procedure was technically simple and the images at the time of the ERCP demonstrate the presence of the obstructing lesion clearly. Additionally, the procedure was not followed by any episodes of pain or sepsis during the interval between the ERCP and laparotomy; a period of 3 months in total. The abscess became clinically evident only when it finally obstructed the common bile duct resulting in jaundice. Our patient had remained entirely well with no symptoms of sepsis or pain until her presentation with jaundice. It is unclear why she suddenly became jaundiced or what factors may have been involved in reactivating the abscess. Other cases of abscesses around the common bile duct causing jaundice have been reported previously. Stevens et al. reported a case of obstructive jaundice 12 months following laparoscopic cholecystectomy [7]. ERCP and stenting were performed but the stent rapidly occluded necessitating laparotomy. An abscess cavity containing multiple small gallstones, presumed to have been spilt during the original operation, was found surrounding the common bile duct causing compression and fibrosis. Plehwe and Glenn in 1978 recounted a case of obstructive jaundice on a background of recurrent abdominal pain for one year [8]. Spontaneous perforation of the common bile duct by a one centimetre gallstone causing abscess formation just below the cystic duct and consequent obstructive jaundice was found at open cholecystectomy. Xing et al. described a 73-year-old male presenting with an abscess in the gallbladder fossa 6 years following laparoscopic cholecystectomy [9]. The abscess resolved following CT-guided aspiration but 4 years later ERCP performed for ascending chlolangitis secondary to common duct stones, revealed the presence of a phantom gallbladder image. The authors postulate that the cystic stump was communicating with the gallbladder fossa in some way, presumably relating to the previous abscess as a result of fistula formation into the cystic duct. The alternative theory was that increased pressure in the cystic duct stump associated with choledocholithiasis caused rupture into the gallbladder fossa. However, all of these reports are associated with complications from the presence of gallstones specifically. This is in contrast to this particular case. Enterococcus casseliflavus is rarely isolated from clinical specimens but is of specific interest because of its low level resistance to vancomycin and its low virulence exhibited clinically [10]. Klebsiella ornithinolytica is one of the least common species of Klebsiella and is occasionally isolated from wounds and abscesses but often represents colonisation only. These isolates are of interest in this case as they represent unusual pathogens which may not have been treated at the time of the original surgery and may consequently have contributed to chronic abscess formation. 4. Conclusion The importance of precise identification and adequate occlusion of the cystic duct stump and the prevention of bile leaks at cholecystectomy is demonstrated. The classical teaching of painless obstructive jaundice; malignant until proven otherwise is also reiterated. Modern imaging with ERCP and CT and less invasive tests such as diagnostic laparoscopy used here could not prove entirely the nonmalignant nature of this lesion and as such exploratory laparotomy was warranted. This case demonstrates a rare cause of painless obstructive jaundice, and a uniquely reported complication of cholecystectomy in the literature to date. References [1] S. B. Archer, D. W. Brown, C. D. Smith, G. D. Branum, and J. G. Hunter, Bile duct injury during laparoscopic cholecystectomy: results of a national survey, Annals of Surgery, vol. 234, no. 4, pp , [2] S. Eisenstein, A. J. Greenstein, U. Kim, and C. M. Divino, Cystic duct stump leaks: after the learning curve, Archives of Surgery, vol. 143, no. 12, pp , [3] A.R.Tumer,Y.N.Yüksek, A. C. Yasti, U. Gözalan, and N. A. Kama, Dropped gallstones during laparoscopic cholesystectomy: the consequences, World Surgery, vol. 29, no. 4, pp , [4] G. N. Marakis, T. E. Pavlidis, K. Ballas, et al., Major complications during laparoscopic cholecystectomy, International Surgery, vol. 92, no. 3, pp , [5]F.Keus,J.A.F.deJong,H.G.Gooszen,andC.J.H.M. van Laarhoven, Laparoscopic versus open cholecystectomy for patients with symptomatic cholecystolithiasis, Cochrane Database of Systematic Reviews, vol. 18, no. 4, Article ID CD006231, [6] J.J.BennettandR.H.Green, Malignantmasquerade:dilemmas in diagnosing biliary obstruction, Surgical Oncology Clinics of North America, vol. 18, no. 2, pp , [7] S.Stevens,H.Rivas,R.N.Cacchione,N.A.O Rouke,andJ.W. Allen, Jaundice due to extrabiliary gallstones, the Society of Laparoendoscopic Surgeons, vol. 7, no. 3, pp , [8] W. E. Plehwe and D. C. Glenn, Spontaneous perforation of the common bile duct: report of a case, Australian and New Zealand Surgery, vol. 48, no. 5, pp , [9]J.Xing,J.Rochester,C.K.Messer,B.P.Reiter,andM.A. Korsten, A phantom gallbladder on endoscopic retrograde cholangiopancreatography, World Gastroenterology, vol. 13, no. 46, pp , [10] G.Pappas,E.Liberopoulos,E.Tsianos,andM.Elisaf, Enterococcus casseliflavus bacteremia. Case report and literature review, Infection, vol. 48, no. 2, pp , 2004.










5 International Endocrinology Gastroenterology Research and Practice The Scientific World Journal Diabetes Research Mediators Clinical & Developmental Immunology of inflammation Evidence-Based Complementary and Alternative Medicine BioMed Research International Submit your manuscripts at Ophthalmology PPAR Obesity Oncology Research Computational and Mathematical Methods in Medicine Oxidative Medicine and Cellular Longevity AIDS Biomarkers Addiction Anesthesiology Allergy
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder in an Elderly Patient
 Case Reports in Surgery Volume 2015, Article ID 767196, 4 pages http://dx.doi.org/10.1155/2015/767196 Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder
Case Reports in Surgery Volume 2015, Article ID 767196, 4 pages http://dx.doi.org/10.1155/2015/767196 Case Report Overlap of Acute Cholecystitis with Gallstones and Squamous Cell Carcinoma of the Gallbladder
Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience
 Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Study of post cholecystectomy biliary leakage and its management
 Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary Mucinous Neoplasm
 Case Reports in Surgery Volume 2015, Article ID 816960, 4 pages http://dx.doi.org/10.1155/2015/816960 Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary
Case Reports in Surgery Volume 2015, Article ID 816960, 4 pages http://dx.doi.org/10.1155/2015/816960 Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary
ABDOMINAL WALL HAEMATOMA COMPLICATING LAPAROSCOPIC CHOLECYSTECTOMY
 HPB Surgery, 1994, Vol. 7, pp. 291-296 Reprints available directly from the publisher Photocopying permitted by license only (C) 1994 Harwood Academic Publishers GmbH Printed in the United States of America
HPB Surgery, 1994, Vol. 7, pp. 291-296 Reprints available directly from the publisher Photocopying permitted by license only (C) 1994 Harwood Academic Publishers GmbH Printed in the United States of America
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Complication of Laparoscopic Cholecystectomy
 Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis
 Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
SURGERY? COMMON BILE DUCT STONES ERCP OR. Room 759. Maryland
 HPB INTERNATIONAL 277 alter the natural history of the disease, and delay or prevent the development or cirrhosis. Data from our unit as well as others suggests that to be the case. The current series,
HPB INTERNATIONAL 277 alter the natural history of the disease, and delay or prevent the development or cirrhosis. Data from our unit as well as others suggests that to be the case. The current series,
Recurring abdominal wall wounds and cutaneous sinus tract formations secondary to spilled gallstones
 ISPUB.COM The Internet Journal of Surgery Volume 21 Number 1 Recurring abdominal wall wounds and cutaneous sinus tract formations secondary to spilled gallstones D Brown, A Wagner, M Aronis, A Isenberg
ISPUB.COM The Internet Journal of Surgery Volume 21 Number 1 Recurring abdominal wall wounds and cutaneous sinus tract formations secondary to spilled gallstones D Brown, A Wagner, M Aronis, A Isenberg
Laparoscopic cholecystectomyy
 Laparoscopic cholecystectomyy What is the gall bladder? The gallbladder is a small pear sized organ that stores bile. Bile is necessary for the digestion of fatty food. The bile duct is a tube that carries
Laparoscopic cholecystectomyy What is the gall bladder? The gallbladder is a small pear sized organ that stores bile. Bile is necessary for the digestion of fatty food. The bile duct is a tube that carries
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit
 Minimally Invasive Surgery, Article ID 562785, 4 pages http://dx.doi.org/10.1155/2014/562785 Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit Ritu Khatuja, 1 Geetika Jain, 1 Sumita
Minimally Invasive Surgery, Article ID 562785, 4 pages http://dx.doi.org/10.1155/2014/562785 Clinical Study Changing Trends in Use of Laparoscopy: A Clinical Audit Ritu Khatuja, 1 Geetika Jain, 1 Sumita
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
SPHINCTER OF ODDI DYSFUNCTION (SOD)
") SPHINCTER OF ODDI DYSFUNCTION (SOD) Sphincter of Oddi dysfunction refers to structural or functional disorders involving the biliary sphincter that may result in impedance of bile and pancreatic juice
SPHINCTER OF ODDI DYSFUNCTION (SOD) Sphincter of Oddi dysfunction refers to structural or functional disorders involving the biliary sphincter that may result in impedance of bile and pancreatic juice
CME Article Clinics in diagnostic imaging (115) Wai C T, Seto K Y, Sutedja D S
 Wai C T, Seto K Y, Sutedja D S") Medical Education Singapore Med.1 2007, 48 (4) : 361 CME Article Clinics in diagnostic imaging (115) Wai C T, Seto K Y, Sutedja D S fit. B CD - -0 o -5 r t -10 Fig. I US images of the upper right abdomen
Medical Education Singapore Med.1 2007, 48 (4) : 361 CME Article Clinics in diagnostic imaging (115) Wai C T, Seto K Y, Sutedja D S fit. B CD - -0 o -5 r t -10 Fig. I US images of the upper right abdomen
Synchronous Hepatic Cryotherapy and Resection
 HPB Surgery, 2000, Vol. 11, pp. 379-382 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
HPB Surgery, 2000, Vol. 11, pp. 379-382 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
PUBLISHED VERSION.
 PUBLISHED VERSION Shay Keren, Gad Dotan, Leah Leibovitch, Dinesh Selva, and Igal Leibovitch Indocyanine green assisted removal of orbital lacrimal duct cysts in children Ophthalmology, 2015; 2015:130215-1-130215-5
PUBLISHED VERSION Shay Keren, Gad Dotan, Leah Leibovitch, Dinesh Selva, and Igal Leibovitch Indocyanine green assisted removal of orbital lacrimal duct cysts in children Ophthalmology, 2015; 2015:130215-1-130215-5
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Gall bladder cancer. Information for patients Hepatobiliary
 Gall bladder cancer Information for patients Hepatobiliary page 2 of 12 Who will provide my care? You will be cared for by a number of professionals who work together. These professionals will be specialist
Gall bladder cancer Information for patients Hepatobiliary page 2 of 12 Who will provide my care? You will be cared for by a number of professionals who work together. These professionals will be specialist
Clinical Study Adhesive Intestinal Obstruction in Infants and Children: The Place of Conservative Treatment
 International Scholarly Research Network ISRN Surgery Volume 2011, Article ID 645104, 4 pages doi:10.5402/2011/645104 Clinical Study Adhesive Intestinal Obstruction in Infants and Children: The Place of
International Scholarly Research Network ISRN Surgery Volume 2011, Article ID 645104, 4 pages doi:10.5402/2011/645104 Clinical Study Adhesive Intestinal Obstruction in Infants and Children: The Place of
Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 )
 膽囊切除術 ( 腹腔鏡 / 開放性 )") Version 1.0 Page 1 of 3 Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 ) Introduction Gallbladder is a sac connected to the biliary tree. It serves the function of concentration
Version 1.0 Page 1 of 3 Information for Consent Cholecystectomy (Laparoscopic/Open) 膽囊切除術 ( 腹腔鏡 / 開放性 ) Introduction Gallbladder is a sac connected to the biliary tree. It serves the function of concentration
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
The campaign on laboratory: focus on Gallstone Disease and ERCP
 The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital
 in a District General Hospital") Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper Intestinal Obstruction
 Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
Case Reports in Surgery Volume 2016, Article ID 5321081, 4 pages http://dx.doi.org/10.1155/2016/5321081 Case Report Spontaneous Intramural Duodenal Hematoma: Pancreatitis, Obstructive Jaundice, and Upper
laparoscopic cholecystectomy
 Combined percutaneous and endoscopic approach in management of dropped gallstones following laparoscopic cholecystectomy John S.F. Shum 1*, K.H. Fung 1, George P.C. Yang 2, Chung Ngai Tang 2, Michael K.W.
Combined percutaneous and endoscopic approach in management of dropped gallstones following laparoscopic cholecystectomy John S.F. Shum 1*, K.H. Fung 1, George P.C. Yang 2, Chung Ngai Tang 2, Michael K.W.
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
CHOLECYSTECTOMY CONSENT FORM
 1 of 6 Patient Name: I, have been asked to carefully read all of the (name of patient or substitute decision-maker) information contained in this consent form and to consent to the procedure described
1 of 6 Patient Name: I, have been asked to carefully read all of the (name of patient or substitute decision-maker) information contained in this consent form and to consent to the procedure described
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Arpit Amin, Yuriy Zhurov, George Ibrahim, Anthony Maffei, Jonathan Giannone, Thomas Cerabona, and Ashutosh Kaul
 Case Reports in Surgery Volume 2016, Article ID 1896368, 9 pages http://dx.doi.org/10.1155/2016/1896368 Case Report Combined Endoscopic and Management of Postcholecystectomy Mirizzi Syndrome from a Remnant
Case Reports in Surgery Volume 2016, Article ID 1896368, 9 pages http://dx.doi.org/10.1155/2016/1896368 Case Report Combined Endoscopic and Management of Postcholecystectomy Mirizzi Syndrome from a Remnant
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous.
 Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Case Rep Gastroenterol 2010;4:71 78 DOI: /
 71 Gallstone Ileus, Bouveret s Syndrome and Choledocholithiasis in a Patient with Billroth II Gastrectomy A Case Report of Combined Endoscopic and Surgical Therapy R. Fejes G. Kurucsai A. Székely F. Luka
71 Gallstone Ileus, Bouveret s Syndrome and Choledocholithiasis in a Patient with Billroth II Gastrectomy A Case Report of Combined Endoscopic and Surgical Therapy R. Fejes G. Kurucsai A. Székely F. Luka
Case Report Postoperative Megarectum in an Adult Patient with Imperforate Anus and Rectourethral Fistula
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 613926, 4 pages http://dx.doi.org/10.1155/2015/613926 Case Report Postoperative Megarectum in an Adult Patient with Imperforate Anus and
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 613926, 4 pages http://dx.doi.org/10.1155/2015/613926 Case Report Postoperative Megarectum in an Adult Patient with Imperforate Anus and
Case Report Formation of a Tunnel under the Major Hepatic Vein Mouths during Removal of IVC Tumor Thrombus
 Case Reports in Urology Volume 2013, Article ID 129632, 4 pages http://dx.doi.org/10.1155/2013/129632 Case Report Formation of a Tunnel under the Major Hepatic Vein Mouths during Removal of IVC Tumor Thrombus
Case Reports in Urology Volume 2013, Article ID 129632, 4 pages http://dx.doi.org/10.1155/2013/129632 Case Report Formation of a Tunnel under the Major Hepatic Vein Mouths during Removal of IVC Tumor Thrombus
담낭절제술후발생한미리찌증후군의내시경적치료 1 예
 Case Report The Korean Journal of Pancreas and Biliary Tract 2014;19:199-203 http://dx.doi.org/10.15279/kpba.2014.19.4.199 pissn 1976-3573 eissn 2288-0941 담낭절제술후발생한미리찌증후군의내시경적치료 1 예 인하대학교의학전문대학원내과학교실 이정민
Case Report The Korean Journal of Pancreas and Biliary Tract 2014;19:199-203 http://dx.doi.org/10.15279/kpba.2014.19.4.199 pissn 1976-3573 eissn 2288-0941 담낭절제술후발생한미리찌증후군의내시경적치료 1 예 인하대학교의학전문대학원내과학교실 이정민
Obstructive jaundice due to a blood clot after ERCP: a case report and review of the literature
 Zhu et al. BMC Gastroenterology (2018) 18:163 https://doi.org/10.1186/s12876-018-0898-4 CASE REPORT Open Access Obstructive jaundice due to a blood clot after ERCP: a case report and review of the literature
Zhu et al. BMC Gastroenterology (2018) 18:163 https://doi.org/10.1186/s12876-018-0898-4 CASE REPORT Open Access Obstructive jaundice due to a blood clot after ERCP: a case report and review of the literature
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Case Reports. Intraductal Papillary Cholangiocarcinoma: Case Report and Review of the Literature INTRODUCTION CASE REPORT
 Case Reports Kongkam K, Rerknimitr R 45 Case Report and Review of the Literature Pradermchai Kongkam, M.D. Rungsun Rerknimitr, M.D. ABSTRACT A case of papillary cholangiocarcinoma is presented. A 64-year-old
Case Reports Kongkam K, Rerknimitr R 45 Case Report and Review of the Literature Pradermchai Kongkam, M.D. Rungsun Rerknimitr, M.D. ABSTRACT A case of papillary cholangiocarcinoma is presented. A 64-year-old
A Guide for Patients Living with a Biliary Metal Stent
 A Guide for Patients Living with a Biliary Metal Stent What is a biliary metal stent? A biliary metal stent (also known as a bile duct stent ) is a flexible metallic tube specially designed to hold your
A Guide for Patients Living with a Biliary Metal Stent What is a biliary metal stent? A biliary metal stent (also known as a bile duct stent ) is a flexible metallic tube specially designed to hold your
Early management of complicated gallstones and acute pancreatitis
 Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
What Are Gallstones? GALLSTONES. Gallstones are pieces of hard, solid matter that form over time in. the gallbladder of some people.
 What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study
 Original article: Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study Sudhir Tyagi 1, Sanjeev Kumar 2* 1 Assistant Professor, 2* Associate
Original article: Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study Sudhir Tyagi 1, Sanjeev Kumar 2* 1 Assistant Professor, 2* Associate
ENDOSCOPIC TREATMENT OF A BILE DUCT
 HPB Surgery, 1990, Vol. 3, pp. 67-71 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORT
HPB Surgery, 1990, Vol. 3, pp. 67-71 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORT
CHOLANGIOCARCINOMA (CCA)
") CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
Case Report Transvaginal Hybrid NOTES Procedure for Treatment of Gallstone Ileus
 Case Reports in Surgery Volume 2016, Article ID 9513874, 4 pages http://dx.doi.org/10.1155/2016/9513874 Case Report Transvaginal Hybrid NOTES Procedure for Treatment of Gallstone Ileus Takuya Shiraishi,
Case Reports in Surgery Volume 2016, Article ID 9513874, 4 pages http://dx.doi.org/10.1155/2016/9513874 Case Report Transvaginal Hybrid NOTES Procedure for Treatment of Gallstone Ileus Takuya Shiraishi,
What can you expect after your ERCP?
 ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
ERCP Explained and respond to bed rest, pain relief and fasting to rest the gut with the patient needing to stay in hospital for only a few days. Some patients develop severe pancreatitis and may require
Bile Duct Injuries. Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India
, MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India") Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India Introduction Bile duct injury (BDI) rare but potentially
Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India Introduction Bile duct injury (BDI) rare but potentially
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 Appendix B: Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE Post publication note: The title of this guideline changed during development. This scope was published before the guideline
Appendix B: Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE Post publication note: The title of this guideline changed during development. This scope was published before the guideline
Vascular complications in percutaneous biliary interventions: A series of 111 procedures
 Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Case Report Perforated Closed-Loop Obstruction Secondary to Gallstone Ileus of the Transverse Colon: A Rare Entity
 Case Reports in Surgery Volume 2015, Article ID 691713, 4 pages http://dx.doi.org/10.1155/2015/691713 Case Report Perforated Closed-Loop Obstruction Secondary to Gallstone Ileus of the Transverse Colon:
Case Reports in Surgery Volume 2015, Article ID 691713, 4 pages http://dx.doi.org/10.1155/2015/691713 Case Report Perforated Closed-Loop Obstruction Secondary to Gallstone Ileus of the Transverse Colon:
Takuya SAKODA* ), Yoshiaki MURAKAMI, Naru KONDO, Kenichiro UEMURA, Yasushi HASHIMOTO, Naoya NAKAGAWA and Taijiro SUEDA ABSTRACT
, Yoshiaki MURAKAMI, Naru KONDO, Kenichiro UEMURA, Yasushi HASHIMOTO, Naoya NAKAGAWA and Taijiro SUEDA ABSTRACT") Hiroshima J. Med. Sci. Vol. 64, No. 3, 45~49, September, 2015 HIJM 64 8 45 Takuya SAKODA* ), Yoshiaki MURAKAMI, Naru KONDO, Kenichiro UEMURA, Yasushi HASHIMOTO, Naoya NAKAGAWA and Taijiro SUEDA Department
Hiroshima J. Med. Sci. Vol. 64, No. 3, 45~49, September, 2015 HIJM 64 8 45 Takuya SAKODA* ), Yoshiaki MURAKAMI, Naru KONDO, Kenichiro UEMURA, Yasushi HASHIMOTO, Naoya NAKAGAWA and Taijiro SUEDA Department
A RARE EXTRAHEPATIC BILIARY ANOMALY
 HPB Surgery 1989, Vol. 1, pp. 353-358 Reprints available directly from the publisher Photocopying permitted by license only 1989 Harwood Academic Publishers GmbH Printed in Great Britain CASE REPORT A
HPB Surgery 1989, Vol. 1, pp. 353-358 Reprints available directly from the publisher Photocopying permitted by license only 1989 Harwood Academic Publishers GmbH Printed in Great Britain CASE REPORT A
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Case Report Acute Obstructive Suppurative Pancreatic Ductitis in an Asymptomatic Patient
 Case Reports in Medicine Volume 2015, Article ID 919452, 4 pages http://dx.doi.org/10.1155/2015/919452 Case Report Acute Obstructive Suppurative Pancreatic Ductitis in an Asymptomatic Patient Eisha Wali,
Case Reports in Medicine Volume 2015, Article ID 919452, 4 pages http://dx.doi.org/10.1155/2015/919452 Case Report Acute Obstructive Suppurative Pancreatic Ductitis in an Asymptomatic Patient Eisha Wali,
Department of General Surgery, Al Khor Hospital, Hamad Medical Corporation, Qatar 2
 International Scholarly Research Network ISRN Minimally Invasive Surgery Volume 2012, Article ID 469013, 5 pages doi:10.5402/2012/469013 Clinical Study Laparoscopic Intraoperative Cholangiography Interpretation
International Scholarly Research Network ISRN Minimally Invasive Surgery Volume 2012, Article ID 469013, 5 pages doi:10.5402/2012/469013 Clinical Study Laparoscopic Intraoperative Cholangiography Interpretation
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Routine Testing of Liver Function Before and After Elective Laparoscopic Cholecystectomy: Is It Necessary?
 Routine Testing of Liver Function Before and After Elective Laparoscopic Cholecystectomy: Is It Necessary? Nasir Zaheer Ahmad, FRCSI SCIENTIFIC PAPER ABSTRACT Background and Objectives: Liver function
Routine Testing of Liver Function Before and After Elective Laparoscopic Cholecystectomy: Is It Necessary? Nasir Zaheer Ahmad, FRCSI SCIENTIFIC PAPER ABSTRACT Background and Objectives: Liver function
Clinical Study Laparoscopic Surgery in Elderly Patients Aged 65 Years and Older with Gynecologic Disease
 International Scholarly Research Network ISRN Obstetrics and Gynecology Volume 2012, Article ID 678201, 4 pages doi:10.5402/2012/678201 Clinical Study Laparoscopic Surgery in Elderly Patients Aged 65 Years
International Scholarly Research Network ISRN Obstetrics and Gynecology Volume 2012, Article ID 678201, 4 pages doi:10.5402/2012/678201 Clinical Study Laparoscopic Surgery in Elderly Patients Aged 65 Years
Endoscopic management of postoperative bile duct injuries: a single center experience.
 1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
Setting The study setting was hospital. The economic analysis was carried out in California, USA.
 Preoperative versus postoperative endoscopic retrograde cholangiopancreatography in mild to moderate gallstone pancreatitis: a prospective randomized trial Chang L, Lo S, Stabile B E, Lewis R J, Toosie
Preoperative versus postoperative endoscopic retrograde cholangiopancreatography in mild to moderate gallstone pancreatitis: a prospective randomized trial Chang L, Lo S, Stabile B E, Lewis R J, Toosie
Downloaded from jssu.ssu.ac.ir at 13:10 IRST on Saturday October 28th 2017
 Journal of Shahid Sadoughi University of Medical Sciences Vol. 21, No. 5, Nov-Dec 2013 Pages: 675-681 1392 5 21 675-681 : 3 2* 1 1392/8/ : -1-2 -3 1391/8/24 : (). :. 1390 200 :.. SPSS (%0/5) 200 (8%) (%9/5)19
Journal of Shahid Sadoughi University of Medical Sciences Vol. 21, No. 5, Nov-Dec 2013 Pages: 675-681 1392 5 21 675-681 : 3 2* 1 1392/8/ : -1-2 -3 1391/8/24 : (). :. 1390 200 :.. SPSS (%0/5) 200 (8%) (%9/5)19
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT
 GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
GASTRO-INTESTINAL TRACT INFECTIONS - ANTIMICROBIAL MANAGEMENT Name & Title Of Author: Dr Linda Jewes, Consultant Microbiologist Date Amended: December 2016 Approved by Committee/Group: Drugs & Therapeutics
Cystic Biliary Atresia: Why Is It Important to Distinguish this from Congenital Choledochal Cyst?
 Bahrain Medical Bulletin, Vol. 36, No. 2, June 2014 Cystic Biliary Atresia: Why Is It Important to Distinguish this from Congenital Choledochal Cyst? Hussein Ahmed Mohammed Hamdy, MRCSEd, FEBPS* Hind Mustafa
Bahrain Medical Bulletin, Vol. 36, No. 2, June 2014 Cystic Biliary Atresia: Why Is It Important to Distinguish this from Congenital Choledochal Cyst? Hussein Ahmed Mohammed Hamdy, MRCSEd, FEBPS* Hind Mustafa
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Comparative Study between Laparoscopic and Open Cholecystectomy for Dr. B. Hemasankararao 1,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Comparative Study between Laparoscopic and Open Cholecystectomy for Dr. B. Hemasankararao 1,
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
REFERRAL GUIDELINES: GALLSTONES
 REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Mirizzi syndrome with an unusual type of biliobiliary fistula a case report
 Kawaguchi et al. Surgical Case Reports (2015) 1:51 DOI 10.1186/s40792-015-0052-2 CASE REPORT Mirizzi syndrome with an unusual type of biliobiliary fistula a case report Tsutomu Kawaguchi 1,2*, Tadao Itoh
Kawaguchi et al. Surgical Case Reports (2015) 1:51 DOI 10.1186/s40792-015-0052-2 CASE REPORT Mirizzi syndrome with an unusual type of biliobiliary fistula a case report Tsutomu Kawaguchi 1,2*, Tadao Itoh
Gallstones and Cholecystectomy Information Sheet
 Gallstones and Cholecystectomy Information Sheet Gallstones & Cholecystectomy This information sheet desrcibes what they are, the treatment options, and what to expect following a operation. The following
Gallstones and Cholecystectomy Information Sheet Gallstones & Cholecystectomy This information sheet desrcibes what they are, the treatment options, and what to expect following a operation. The following
Biliary Tract Disease. Emmet Andrews Cork University Hospital 6 th September 2010
 Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria
 ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-6 Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria Ankit Chhoda
ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-6 Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria Ankit Chhoda
MAKING CONNECTIONS. Los Angeles Medical Center
 MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
Having a Stent Placed at ERCP
 Having a Stent Placed at ERCP Information for patients, relatives and carers This information leaflet should be read in conjunction with the ERCP information booklet (ref PIL 78) Endoscopy Unit For more
Having a Stent Placed at ERCP Information for patients, relatives and carers This information leaflet should be read in conjunction with the ERCP information booklet (ref PIL 78) Endoscopy Unit For more
Naoyuki Toyota, Tadahiro Takada, Hodaka Amano, Masahiro Yoshida, Fumihiko Miura, and Keita Wada
 J Hepatobiliary Pancreat Surg (2006) 13:80 85 DOI 10.1007/s00534-005-1062-4 Endoscopic naso-gallbladder drainage in the treatment of acute cholecystitis: alleviates inflammation and fixes operator s aim
J Hepatobiliary Pancreat Surg (2006) 13:80 85 DOI 10.1007/s00534-005-1062-4 Endoscopic naso-gallbladder drainage in the treatment of acute cholecystitis: alleviates inflammation and fixes operator s aim
Portal Vein in a Patient Undergoing Hepatic Resection
 HPB Surgery, 1997, Vol. 10, pp. 323-327 Reprints available directly from the publisher Photocopying permitted by license only (C) 1997 OPA (Overseas Publishers Association) Amsterdam B.V. Published in
HPB Surgery, 1997, Vol. 10, pp. 323-327 Reprints available directly from the publisher Photocopying permitted by license only (C) 1997 OPA (Overseas Publishers Association) Amsterdam B.V. Published in
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
THE CURRENT PLACE OF SHOCK-WAVE LITHOTRIPSY FOR BILE DUCT STONES. Department of Surgery AUSTRALIA
 HPB INTERNATIONAL 217 assessment of a predictive scoring system, both in patients treated by modern techniques and in a less highly selected group of patients, and the authors indicate that such studies
HPB INTERNATIONAL 217 assessment of a predictive scoring system, both in patients treated by modern techniques and in a less highly selected group of patients, and the authors indicate that such studies
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Abdominal Imaging. Gallbladder perforation: color Doppler findings
 Abdom Imaging 27:47 50 (2002) DOI: 10.1007/s00261-001-0048-1 Abdominal Imaging Springer-Verlag New York Inc. 2002 Gallbladder perforation: color Doppler findings K. Konno, 1 H. Ishida, 1 M. Sato, 1 H.
Abdom Imaging 27:47 50 (2002) DOI: 10.1007/s00261-001-0048-1 Abdominal Imaging Springer-Verlag New York Inc. 2002 Gallbladder perforation: color Doppler findings K. Konno, 1 H. Ishida, 1 M. Sato, 1 H.
Case Report Reresection of Colorectal Liver Metastasis with Vena Cava Resection
 Case Reports in Surgery Volume 2016, Article ID 8173048, 4 pages http://dx.doi.org/10.1155/2016/8173048 Case Report Reresection of Colorectal Liver Metastasis with Vena Cava Resection Ali Tardu, Cuneyt
Case Reports in Surgery Volume 2016, Article ID 8173048, 4 pages http://dx.doi.org/10.1155/2016/8173048 Case Report Reresection of Colorectal Liver Metastasis with Vena Cava Resection Ali Tardu, Cuneyt
ACUTE CHOLANGITIS AS a result of an occluded
 Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct