Bile Duct Injuries. Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India
|
|
|
- Betty Lambert
- 5 years ago
- Views:
Transcription
1 Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India
2 Introduction Bile duct injury (BDI) rare but potentially devastating condition biliary peritonitis & sepsis, cholangitis, portal hypertension & secondary biliary cirrhosis significant morbidity & mortality Iatrogenic BDI Increased financial burden (patient or hospital) Malpractice litigation
3 56 yrs, male Heavy smoker, COPD History Lap.cholecystectomy elsewhere on 16 th May 09 Acute cholecystitis Post-extubation bronchospasm hydrocortisone, nebulisers, antibiotics 6 th POD Referred to Cardiologist, Dr. A. M for further management of sepsis & respiratory distress CCU
4 On Examination Afebrile, no icterus, extensive wheeze P/A Slight distention, diffuse tenderness & guarding Inj. Cefoperazone-Sulbactum & Metronidazole Hydrocortisone stopped U/S abdomen (7 th POD): Moderate ascites, aspiration 700ml thick yellowish fluid. Ofloxacin added Post cholecystectomy bile leak Rpt. U/S (9 th POD): More than 1.5 litres ascites
5 Management CT scan guided drainage (9 th POD): Subphrenic Malecot catheter 850ml bile drained. 300ml aspirated from pelvis 9 th POD 1175ml 10 th POD 700ml (? ERCP) 11 th POD 900ml, Fluid culture: Klebsiella oxytoca antibiotics changed to Piptaz & Cifran 12 th POD 500ml, MRCP planned 13 th POD 450ml, Malecot catheter fell out. CT guided repositioning done 18 th POD MRCP

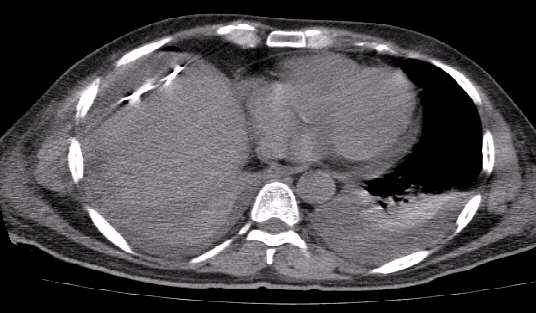
6 CT scan abdomen

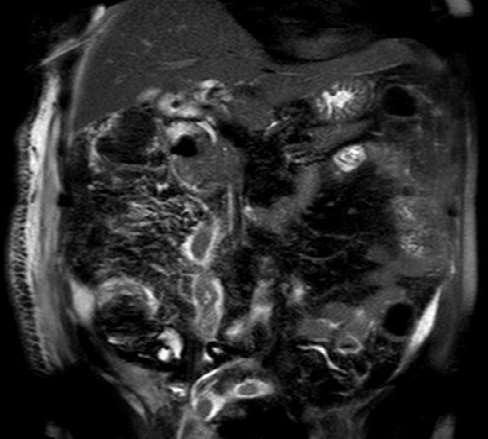
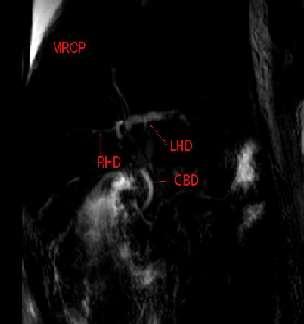
7 MRCP
8 Bile Drainage POD Amount POD Amount ml ml ml ml ml 26 50ml, Bilirubin 0.9mg% ml, MRCP 27,28 & 29 Minimal, rpt. Ultrasound ml 30 15ml ml 31 3ml Drain removed ml 32 no fever or jaundice ml 33 Discharged 28 days
9 Discussion
10 Anatomy Calot s triangle between inferior surface of liver, Cystic duct & CHD Contents Cystic artery, RHA, Cystic lymph node
11 Bile Duct Injuries (BDI) Iatrogenic injury Cholecystectomy Gastrectomy Pancreatectomy ERCP Trauma Duodenal ulcer
12 Laparoscopic cholecystectomy (LC) Late 1980s Gold standard for management of benign gallbladder disease Compared with laparotomy Less post-op pain Shorter hospital stay Earlier return to normal activity Better cosmesis Iatrogenic bile duct injury rate 0.1% to 0.2% (open) vs 0.4% to 0.6% (lap)
13 LC & Bile duct injury (BDI) LC most common cause of BDI More severe than those seen with Open chole Learning curve phenomenon? BDI after LC stable around 0.6 to 0.7%, 4 times that of open chole high for a benign condition
14 Classification location of injury mechanism & type of injury effect on biliary continuity timing of identification Each plays significant role in determining appropriate management & operative repair
15 Classification of BDI Bismuth classification (1982) era of Open Chole location of biliary strictures with respect to hepatic bifurcation based on most distal level at which healthy biliary mucosa available for anastomosis helps surgeon choose appropriate site for repair degree of injury correlates with surgical outcomes
16 Classification of BDI McMahon system Bile duct laceration Transection Excision Stricture Strasberg classification (1995) Type A to E, with type E subdivided into E1 to E5 like Bismuth classification
17 Strasberg classification Type A B C D E1 E2 E3 E4 E5 Criteria Leak from Cystic duct or small ducts in liver bed Occlusion of an aberrant RHD Transection without ligation of an aberrant RHD Lateral injury to a major bile duct Transection >2 cm from the hilum Transection <2 cm from the hilum Transection in the hilum Separation of major ducts in the hilum Type C injury plus injury in the hilum
18 Strasberg classification
19 Timing of Identification Intra-op Post-op unexpected ductal structures seen bile leak into field from lacerated or transected duct depends on continuity of bile duct & presence or absence of bile leak
20 Obstruction Bile Leak Clinical Presentation (post-op) Clip ligation or resection of CBD obstructive jaundice, cholangitis Bile from intra-op drain or More commonly, localized biloma or free bile ascites / peritonitis, if no drain Diffuse abdominal pain & persistent ileus several days post-op high index of suspicion possible unrecognized BDI
21 Classical laparoscopic injury CBD mistaken for cystic duct CBD clipped & resected Proximal dissection & division injury to RHA loss of length & occlusion of proximal biliary tree with possible concomitant right hepatic ischemia

22 Classical LC BDI
23 Intra-op diagnosis About 30% BDI recognized at time of initial surgery If injury recognized, two options, depending on expertise Drain OR Primary repair at time of LC Primary end-to-end CBD repair or Roux-en-Y hepaticojejunostomy Primary repair high incidence of failure percutaneous or endoscopic balloon dilatation later
24 Post-op diagnosis Diffuse abdominal pain & persistent ileus several days post-op high index of suspicion possible unrecognized BDI Ultrasound & CT scan HIDA scan intraabdominal collections or ascites, if bile leak dilatation of biliary tree, if bile duct obstruction If doubt exists, HIDA scan can confirm leak but not the specific leak site
25 Management CT or U/S guided (or surgical) drainage Sepsis control Broad-spectrum antibiotics & percutaneous biliary drainage to control any bile leak most fistulas will be controlled or even close 1.5% mortality rate due to uncontrolled sepsis No rush to proceed with definitive management of BDI Delay of several weeks allows local inflammation to resolve & almost certainly improves final outcome

26 ERCP multiple stents Lateral duct wall injury or cystic duct leak transampullary stent controls leak & provides definitive treatment Distal CBD must be intact to augment internal drainage with endoscopic stent
 necessary")
27 ERC clips across CBD CBD transection normal-sized distal CBD upto site of transection Percutaneous transhepatic cholangiography (PTC) necessary Surgery
28 Cholangiography (ERCP + PTC) Percutaneous transhepatic cholangiography (PTC) defines proximal anatomy allows placement of percutaneous transhepatic biliary catheters to decompress biliary tree treats or prevents cholangitis & controls bile leak
29 Noninvasive MRCP / CT cholangiography May avoid invasive procedures like ERCP or PTC CT cholangiography not adequate for evaluation of bile duct Do not allow intervention Interpretatation in presence of bile collection difficult Potentially delays treatment
30 Definitive management Goal reestablishment of bile flow into proximal GIT in a manner that prevents cholangitis, sludge or stone formation, restricturing & progressive liver injury Bile duct intact & simply narrowed percutaneous or endoscopic dilatation
31 Biliary enteric anastomosis Most laparoscopic BDI complete discontinuity of biliary tree Surgical reconstruction, Roux-en-Y hepaticojejunostomy tension-free, mucosa-tomucosa anastomosis with healthy, nonischemic bile duct
32 Treatment summary Strasberg Type A ERCP + sphincterotomy + stent Type B & C traditional surgical hepaticojejunostomy Type D primary repair over an adjacently placed T-tube (if no evidence of significant ischemia or cautery damage at site of injury) More extensive type D & E injuries Roux an-y hepaticojejunostomy over a 5-F pediatric feeding tube to serve as a biliary stent
33 Risk Factors for BDI Acute inflammation at Calot s triangle Atypical anatomy aberrant RHD (most common) complex cystic duct insertion Conditons that impair Critical view of safety Obesity & periportal fat Complex biliary disease choledocholithiasis, gallstone pancreatitis, cholangitis Intra-op bleeding
34 Reasons Misidentification CBD or aberrant RHD mistaken for cystic duct Risk factors inexperience, inflammation or aberrant anatomy Infundibular technique flaring of cystic duct as it becomes infundibulum misleading in inflammation Technical errors Cautery induced injury
35 Prevention 30 laparoscope, high quality imaging equipment Firm cephalic traction on fundus & lateral traction on infundibulum, so cystic duct perpendicular to CBD Dissect infundibulo-cystic junction Expose Critical view of safety before dividing cystic duct Convert to open, if unable to mobilise infundibulum or bleeding or inflammation in Calot s triangle Routine intra-op cholangiogram Fundus-first dissection

36 Critical view of safety Calot s triangle dissected free of all tissue except cystic duct & artery Base of liver bed exposed When this view is achieved, the two structures entering GB can only be cystic duct & artery Not necessary to see CBD
37 Cystic duct or CBD? Cystic duct CBD Caution 2 3mm wide 5mm wide CD > 5mm Is it CBD? Even with low cystic duct insertion, CD rarely goes behind duodenum Double cystic duct very rare No vessels on surface CBD goes behind duodenum Vessels on surface Duct behind duodenum must be CBD -- 2 ducts seem to go towards inflammed Gallbladder one must be CBD --
38 Routine intra-op cholangiogram (IOC) Done via presumed cystic duct If this happens to be CBD, injury has already occurred!! IOC does not identify all aberrant ducts Arterial anatomy not identified IOC does not prevent BDI but may reduce its severity ( if correctly performed & interpreted, IOC can prevent complete CBD transection) IOC higher rate of intra-op identification of BDI decreased cost of treatment & shorter hospital stay
39 Anatomic illusion? Misperception (97%) rather than technical error (3%) Everyone is susceptible experience, knowledge & technical skill alone may not be adequate Current BDI rate may be near upper limits of human performance (1% mortality accepted for CABG) All BDI may not represent substandard practice Improvements may have to depend on technology
40 The Future No need to dissect cystic duct unlike IOC Lap. Ultrasound & Doppler Tactile sensor probes Intra-op fluorescent cholangiography using IV Indocyanine green Injection of a dye into gallbladder to visualise biliary tree Intraoperative bile duct visualization using near-infrared hyperspectral video imaging Light cholangiography fibreoptic cable via ampulla of Vater
41 The reality Technology largely unavailable Not validated Costly For now, no alternative to planned meticulous dissection with precise identification of structures before division
42 Outcome Hospital expenses Rs. 2,30,000/ - Plus loss of income for at least 2 months Plus loss of income for attenders Hopefully, successful conservative management? All is well that ends well OR Will he develop a bile duct stricture? ( & then jaundice, cholangitis, portal HT or secondary biliary cirrhosis etc)

43 Summary Multidisciplinary management of BDI expertise of surgeons, radiologists & gastroenterologists From benign gallstone disease bile duct injury Mismanagement lifelong disability & chronic liver disease biliary cripple BDI with lap. Chole results of operative repair, excellent in Specialist Centres
44 Acknowledgement Dept. of Radiology for significant contributions in the management of this patient Thank You
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Complication of Laparoscopic Cholecystectomy
 Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Study of post cholecystectomy biliary leakage and its management
 Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Original Research Article Study of post cholecystectomy biliary leakage and its management P. Krishna Kishore 1*, B. Manju Sruthi 2, G. Obulesu 3 1 Assistant Professor, Departmentment of General Surgery,
Common Bile Duct Injury: Recognition and Management
 Common Bile Duct Injury: Recognition and Management Jaime A Pineda, MD Division of Transplantation Department of Surgery University of Vermont Medical Center No disclosure Is This Going to Happen to Me
Common Bile Duct Injury: Recognition and Management Jaime A Pineda, MD Division of Transplantation Department of Surgery University of Vermont Medical Center No disclosure Is This Going to Happen to Me
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Cholangiocarcinoma: Radiologic evaluation and interventions
 November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
Lutheran Medical Center. Daniel H. Hunt, M.D. June 10 th, 2005
 Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
SUNY Downstate Medical Center Kings County Hospital
 Management of Choledocholithiasis SUNY Downstate Medical Center Kings County Hospital Department of Surgery Grand Rounds Kiyanda Baldwin October 22, 2009 Case Presentation 43 y/o F c/o jaundice x 3 days
Management of Choledocholithiasis SUNY Downstate Medical Center Kings County Hospital Department of Surgery Grand Rounds Kiyanda Baldwin October 22, 2009 Case Presentation 43 y/o F c/o jaundice x 3 days
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Rokitansky-Aschoff sinuses are epithelial invaginations in the gallbladder wall that from as a result of increased gallbladder pressures.
 Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
Biliary MRI w Eovist
 Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Biliary Anatomy in Living-related Liver Transplantation
 The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE
 ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE Dr. Sohan kumar sah *, Dr. Liu Sibin, Dr. sumendra raj pandey, Dr. Prakashmaan shah, Dr. Gaurishankar pandit, Dr. Suraj kurmi and Dr. Sanjay kumar jaiswal
ROLE OF RADIOLOGY IN INVESTIGATION OF JAUNDICE Dr. Sohan kumar sah *, Dr. Liu Sibin, Dr. sumendra raj pandey, Dr. Prakashmaan shah, Dr. Gaurishankar pandit, Dr. Suraj kurmi and Dr. Sanjay kumar jaiswal
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Early View Article: Online published version of an accepted article before publication in the final form.
 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD) Type of Article:
Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD) Type of Article:
MAKING CONNECTIONS. Los Angeles Medical Center
 MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Early management of complicated gallstones and acute pancreatitis
 Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Early management of complicated gallstones and acute pancreatitis A/Prof Richard Cade George Kalogeropoulos ( Fellow) HPB/Upper GI Unit Eastern Health, Melbourne biliary colic/acute cholecystitis common
Biliary tract injuries after lap cholecystectomy types, surgical intervention and timing
 Focus on Surgical Techniques from Bench to Bedside Page 1 of 9 Biliary tract injuries after lap cholecystectomy types, surgical intervention and timing Michail Karanikas 1, Ferdi Bozali 1, Vasileia Vamvakerou
Focus on Surgical Techniques from Bench to Bedside Page 1 of 9 Biliary tract injuries after lap cholecystectomy types, surgical intervention and timing Michail Karanikas 1, Ferdi Bozali 1, Vasileia Vamvakerou
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Post Laparoscopic Cholecystectomy Biloma in a Child Managed by Endoscopic Retrograde Cholangio-Pancreatography and Stenting: A Case Report
 pissn: 2234-8646 eissn: 2234-8840 https://doi.org/10.5223/pghn.2016.19.4.281 Pediatr Gastroenterol Hepatol Nutr 2016 December 19(4):281-285 Case Report PGHN Post Laparoscopic Cholecystectomy Biloma in
pissn: 2234-8646 eissn: 2234-8840 https://doi.org/10.5223/pghn.2016.19.4.281 Pediatr Gastroenterol Hepatol Nutr 2016 December 19(4):281-285 Case Report PGHN Post Laparoscopic Cholecystectomy Biloma in
THE INTERVENTIONAL RADIOLOGIST CHRISTIAAN VAN DER LEIJ, MD. EBIR. INTERVENTIONAL RADIOLOGY MAASTRICHT UMC+
 THE INTERVENTIONAL RADIOLOGIST CHRISTIAAN, MD. EBIR. INTERVENTIONAL RADIOLOGY MAASTRICHT UMC+ DISCLOSURES None 78 Y/O FEMALE Painful RUQ Fever Lab: Raised Leukocytes/CRP CHOLECYSTITIS 3-9% patients ER
THE INTERVENTIONAL RADIOLOGIST CHRISTIAAN, MD. EBIR. INTERVENTIONAL RADIOLOGY MAASTRICHT UMC+ DISCLOSURES None 78 Y/O FEMALE Painful RUQ Fever Lab: Raised Leukocytes/CRP CHOLECYSTITIS 3-9% patients ER
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Guidelines for Laparoscopic CBD Exploration
 Guidelines for Laparoscopic CBD Exploration INDICATIONS Since the 1992 National Institutes of Health Consensus Development Conference Statement on Gallstones and Laparoscopic Cholecystectomy the indications
Guidelines for Laparoscopic CBD Exploration INDICATIONS Since the 1992 National Institutes of Health Consensus Development Conference Statement on Gallstones and Laparoscopic Cholecystectomy the indications
Classification of choledochal cyst with MR cholangiopancreatography in children and infants: special reference to type Ic and type IVa cyst
 Classification of choledochal cyst with MR cholangiopancreatography in children and infants: special reference to type Ic and type IVa cyst Poster No.: C-1333 Congress: ECR 2011 Type: Educational Exhibit
Classification of choledochal cyst with MR cholangiopancreatography in children and infants: special reference to type Ic and type IVa cyst Poster No.: C-1333 Congress: ECR 2011 Type: Educational Exhibit
LAPAROSCOPIC GALLBLADDER SURGERY
 LAPAROSCOPIC GALLBLADDER SURGERY Treating Gallbladder Problems with Laparoscopy A Common Problem If you ve had an attack of painful gallbladder symptoms, you re not alone. Gallbladder disease is very common.
LAPAROSCOPIC GALLBLADDER SURGERY Treating Gallbladder Problems with Laparoscopy A Common Problem If you ve had an attack of painful gallbladder symptoms, you re not alone. Gallbladder disease is very common.
Bile duct injuries related to misplacement of T tubes
 Annals of Hepatology 2006; 5(1): January-March: 44-48 Original Article Annals of Hepatology Bile duct injuries related to misplacement of T tubes Miguel Ángel Mercado;* Carlos Chan; Héctor Orozco;* Alexandra
Annals of Hepatology 2006; 5(1): January-March: 44-48 Original Article Annals of Hepatology Bile duct injuries related to misplacement of T tubes Miguel Ángel Mercado;* Carlos Chan; Héctor Orozco;* Alexandra
Imaging of Biliary Tract Emergencies in Jorge A. Soto, MD Professor of Radiology Boston University Medical Center.
 Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Imaging of Biliary Tract Emergencies in 2011 Jorge A. Soto, MD Professor of Radiology Boston University Medical Center Introduction Biliary emergencies are: Common Come in many flavors Deceiving: frequent
Cholelithiasis & cholecystitis
 1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
1 Cholelithiasis & cholecystitis Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
The role of cholangiography with t-tube in the liver transplantation
 The role of cholangiography with t-tube in the liver transplantation Poster No.: C-0362 Congress: ECR 2012 Type: Educational Exhibit Authors: S. Magalhães, I. Ferreira, A. B. Ramos, F. Reis, M. Ribeiro
The role of cholangiography with t-tube in the liver transplantation Poster No.: C-0362 Congress: ECR 2012 Type: Educational Exhibit Authors: S. Magalhães, I. Ferreira, A. B. Ramos, F. Reis, M. Ribeiro
Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study
 Study title Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study Primary Investigator: Kazuhide Matsushima, MD Co-Primary investigator: Zachary Warriner,
Study title Subtotal cholecystectomy for complicated acute cholecystitis: a multicenter prospective observational study Primary Investigator: Kazuhide Matsushima, MD Co-Primary investigator: Zachary Warriner,
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
ERCP in altered anatomy. Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway
 ERCP in altered anatomy Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway CO2 as insufflation gas Reduces post-procedure pain Reduces in-procedure bowel distension Improves the intubation
ERCP in altered anatomy Lars Aabakken Oslo University Hospital - Rikshospitalet Oslo, Norway CO2 as insufflation gas Reduces post-procedure pain Reduces in-procedure bowel distension Improves the intubation
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
MANAGEMENT OF COMPLICATED GALLSTONE DISEASE
 gastrointestinal tract and abdomen MANAGEMENT OF COMPLICATED GALLSTONE DISEASE Carmen L. Mueller, BSc(H), MD, FRCSC, Amy A. Neville, MD, FRCSC, MSc, and Gerald M. Fried, MD, FRCSC, FACS, FCAHS Gallstones
gastrointestinal tract and abdomen MANAGEMENT OF COMPLICATED GALLSTONE DISEASE Carmen L. Mueller, BSc(H), MD, FRCSC, Amy A. Neville, MD, FRCSC, MSc, and Gerald M. Fried, MD, FRCSC, FACS, FCAHS Gallstones
Tata Memorial Centre s opinion is summarized as follows: 1. Given the type 1 stricture (as mentioned in the structured summary), assessment
, assessment") March 5 th 2016 Dear Ms. Malti Sinha, Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online
March 5 th 2016 Dear Ms. Malti Sinha, Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online
Original article: SURGICAL TREATMENT FOR BENIGN BILIARY STRICTURES: SINGLE-CENTER EXPERIENCE ON 64 CASES
 Original article: SURGICAL TREATMENT FOR BENIGN BILIARY STRICTURES: SINGLE-CENTER EXPERIENCE ON 64 CASES Yunfeng Cui, Hongtao Zhang, Naiqiang Cui, Zhonglian Li* Department of Surgery, Tianjin Nankai Hospital,
Original article: SURGICAL TREATMENT FOR BENIGN BILIARY STRICTURES: SINGLE-CENTER EXPERIENCE ON 64 CASES Yunfeng Cui, Hongtao Zhang, Naiqiang Cui, Zhonglian Li* Department of Surgery, Tianjin Nankai Hospital,
The Present Scenario of Cholecystectomy
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 5 Ver. III (May. 2016), PP 71-75 www.iosrjournals.org The Present Scenario of Cholecystectomy
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 5 Ver. III (May. 2016), PP 71-75 www.iosrjournals.org The Present Scenario of Cholecystectomy
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Postoperative Bile Duct Strictures: Management and Outcome in the 1990s
 ANNALS OF SURGERY Vol. 232, No. 3, 430 441 2000 Lippincott Williams & Wilkins, Inc. Postoperative Bile Duct Strictures: Management and Outcome in the 1990s Keith D. Lillemoe, MD, Genevieve B. Melton, MD,
ANNALS OF SURGERY Vol. 232, No. 3, 430 441 2000 Lippincott Williams & Wilkins, Inc. Postoperative Bile Duct Strictures: Management and Outcome in the 1990s Keith D. Lillemoe, MD, Genevieve B. Melton, MD,
SAGES GUIDELINES FOR THE CLINICAL APPLICATION OF LAPAROSCOPIC BILIARY TRACT SURGERY
 Practice/Clinical Guidelines published on: 01/2010 by the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) SAGES GUIDELINES FOR THE CLINICAL APPLICATION OF LAPAROSCOPIC BILIARY TRACT
Practice/Clinical Guidelines published on: 01/2010 by the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) SAGES GUIDELINES FOR THE CLINICAL APPLICATION OF LAPAROSCOPIC BILIARY TRACT
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Case Report Simultaneous Non-Traumatic Perforation of Right Hepatic Duct and Gallbladder: An Atypical Occurrence
 Case Report Simultaneous Non-Traumatic Perforation of Right Hepatic Duct and Gallbladder: An Atypical Occurrence Pankaj Kumar GARG1, Bhupendra Kumar JAIN1, Satya Deo PANDEY1, Vinita RATHI2, Amarendra Singh
Case Report Simultaneous Non-Traumatic Perforation of Right Hepatic Duct and Gallbladder: An Atypical Occurrence Pankaj Kumar GARG1, Bhupendra Kumar JAIN1, Satya Deo PANDEY1, Vinita RATHI2, Amarendra Singh
cholangiopancreatography
 1250 Hepatopancreatic-Biliary Unit, Academic Medical Centre, University of Amsterdam, The Netherlands P H P Davids J Ringers E A J Rauws L Th de Wit K Huibregtse M N van der Heyde G N J Tytgat Correspondence
1250 Hepatopancreatic-Biliary Unit, Academic Medical Centre, University of Amsterdam, The Netherlands P H P Davids J Ringers E A J Rauws L Th de Wit K Huibregtse M N van der Heyde G N J Tytgat Correspondence
CBD stones & strictures (Obstructive jaundice)
") 1 CBD stones & strictures (Obstructive jaundice) Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz
1 CBD stones & strictures (Obstructive jaundice) Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz
Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis
 Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Original Article Presence of choledocholithiasis in patients undergoing cholecystectomy for mild biliary pancreatitis Pradhan S 1, Shah S 2, Maharjan S 2, Shah JN 3 1 2 2 3 Professor, Patan hospital Correspondence:
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno. Objectives. Why?
 Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
Hepatobiliary Ultrasound Rimon Bengiamin, MD, RDMS Assistant Clinical Professor Director of Emergency Ultrasound UCSF Fresno Objectives Discuss the goals of point-of-care biliary ultrasound Review the
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous.
 Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Repair 0ptions Following Iatrogenic Bile Duct Injuries
 Journal of Surgery 2015; 3(5): 50-55 Published online October 23, 2015 (http://www.sciencepublishinggroup.com/j/js) doi: 10.11648/j.js.20150305.12 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Repair
Journal of Surgery 2015; 3(5): 50-55 Published online October 23, 2015 (http://www.sciencepublishinggroup.com/j/js) doi: 10.11648/j.js.20150305.12 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Repair
Endoscopic management of postoperative bile duct injuries: a single center experience.
 1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
Risk Factors for Development of Biliary Stricture in Patients Presenting with Bile Leak after Cholecystectomy
 Gut and Liver, Vol. 7, No. 3, May 2013, pp. 352-356 ORiginal Article Risk Factors for Development of Biliary Stricture in Patients Presenting with Bile Leak after Cholecystectomy Hosur Mayanna Lokesh,
Gut and Liver, Vol. 7, No. 3, May 2013, pp. 352-356 ORiginal Article Risk Factors for Development of Biliary Stricture in Patients Presenting with Bile Leak after Cholecystectomy Hosur Mayanna Lokesh,
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
ISSN X (Print) Research Article. *Corresponding author Bikramjit Pal
 Research Article. *Corresponding author Bikramjit Pal") Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2014; 2(5F):1900-1905 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2014; 2(5F):1900-1905 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
PERCUTANEOUS BILIARY DRAINAGE
 PERCUTANEOUS BILIARY DRAINAGE MEDICAL IMAGING INFORMATION FOR PATIENTS Introduction This booklet tells you about the procedure known as percutaneous biliary drainage, explains what is involved and what
PERCUTANEOUS BILIARY DRAINAGE MEDICAL IMAGING INFORMATION FOR PATIENTS Introduction This booklet tells you about the procedure known as percutaneous biliary drainage, explains what is involved and what
Long-term Results of a Primary End-to-end Anastomosis in Peroperative Detected Bile Duct Injury
 J Gastrointest Surg (2007) 11:296 302 DOI 10.1007/s11605-007-0087-1 Long-term Results of a Primary End-to-end Anastomosis in Peroperative Detected Bile Duct Injury P. R. de Reuver & O. R. C. Busch & E.
J Gastrointest Surg (2007) 11:296 302 DOI 10.1007/s11605-007-0087-1 Long-term Results of a Primary End-to-end Anastomosis in Peroperative Detected Bile Duct Injury P. R. de Reuver & O. R. C. Busch & E.
What Are Gallstones? GALLSTONES. Gallstones are pieces of hard, solid matter that form over time in. the gallbladder of some people.
 What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Malignant Obstructive Jaundice has dismal
 Proceeding S.Z.P.G.M.L vol: 22(2}: pp. 79-83, 2008. Anatomic Level of Biliary Obstruction and Outcome of Pre-Operative Biliary Stenting in Malignant Obstructive Jaundice -A Shaikh Zayed Hospital Experience
Proceeding S.Z.P.G.M.L vol: 22(2}: pp. 79-83, 2008. Anatomic Level of Biliary Obstruction and Outcome of Pre-Operative Biliary Stenting in Malignant Obstructive Jaundice -A Shaikh Zayed Hospital Experience
Biliary Tract Disease. Emmet Andrews Cork University Hospital 6 th September 2010
 Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
CHOLECYSTECTOMY CONSENT FORM
 1 of 6 Patient Name: I, have been asked to carefully read all of the (name of patient or substitute decision-maker) information contained in this consent form and to consent to the procedure described
1 of 6 Patient Name: I, have been asked to carefully read all of the (name of patient or substitute decision-maker) information contained in this consent form and to consent to the procedure described
Ruptured choledochal cyst: a rare presentation and unique approach to management
 Case Report Ruptured choledochal cyst: a rare presentation and unique approach to management Michael Meschino, Carlos García-Ochoa, Roberto Hernandez-Alejandro London Health Sciences Centre, Western University,
Case Report Ruptured choledochal cyst: a rare presentation and unique approach to management Michael Meschino, Carlos García-Ochoa, Roberto Hernandez-Alejandro London Health Sciences Centre, Western University,
Surface Anatomy. Location Shape Weight Role of Five Surfaces Borders Fissures Lobes Peritoneal Lig
 The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Appendix A: Summary of evidence from surveillance
 Appendix A: Summary of evidence from surveillance 2018 surveillance of Gallstone disease: diagnosis and management (2014) NICE guideline CG188 Summary of evidence from surveillance Studies identified in
Appendix A: Summary of evidence from surveillance 2018 surveillance of Gallstone disease: diagnosis and management (2014) NICE guideline CG188 Summary of evidence from surveillance Studies identified in
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
ERCP complications and challenges in their diagnosis and management.
 ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
NEW CLASSIFICATION OF MAJOR BILE DUCT INJURIES ASSOCIATED WITH LAPAROSCOPIC CHOLECYSTECTOMY
 SCRIPTA MEDICA (BRNO) 75 (6): 283 290, December 2002 NEW CLASSIFICATION OF MAJOR BILE DUCT INJURIES ASSOCIATED WITH LAPAROSCOPIC CHOLECYSTECTOMY MICHEK J., ZELNÍâEK P., OCHMANN J., SVOBODA P., VRASTYÁK
SCRIPTA MEDICA (BRNO) 75 (6): 283 290, December 2002 NEW CLASSIFICATION OF MAJOR BILE DUCT INJURIES ASSOCIATED WITH LAPAROSCOPIC CHOLECYSTECTOMY MICHEK J., ZELNÍâEK P., OCHMANN J., SVOBODA P., VRASTYÁK
In any operation. Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications.
 In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
In any operation Indications. Anaesthesia. Position of the patient. Incision. Steps of the operation. Complications. Abdominal operation I position for operation Supine Abdominal operation I position for
Percutaneous transhepatic cholangiogram (PTC) and biliary drainage. An information guide
 and biliary drainage. An information guide") TO PROVIDE THE VERY BEST CARE FOR EACH PATIENT ON EVERY OCCASION Percutaneous transhepatic cholangiogram (PTC) and biliary drainage An information guide Percutaneous transhepatic cholangiogram (PTC) and
TO PROVIDE THE VERY BEST CARE FOR EACH PATIENT ON EVERY OCCASION Percutaneous transhepatic cholangiogram (PTC) and biliary drainage An information guide Percutaneous transhepatic cholangiogram (PTC) and
DISCLAIMER. No Conflict of Interest
 DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
DISCLAIMER No Conflict of Interest EXCLAIMER No Interest in Conflict GALLSTONES FAQs and FACTS John Dunn, FRACS Laparoscopy Auckland YOU GOTTA KNOW THIS STUFF HOW DO THEY FORM? Gallbladder Lithogenic
Gallstones. Classification
 Gallstones Nariman Karanjia Tahir Ali Abstract Gallstones are extremely common in the UK and have a major effect on healthcare resources. Presentation depends on whether the stones occlude the cystic duct
Gallstones Nariman Karanjia Tahir Ali Abstract Gallstones are extremely common in the UK and have a major effect on healthcare resources. Presentation depends on whether the stones occlude the cystic duct
JAUNDICE. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
 JAUNDICE Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Definition of Jaundice Icterus A yellowish staining of the skin, sclerae and deeper
JAUNDICE Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Definition of Jaundice Icterus A yellowish staining of the skin, sclerae and deeper
Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study
 Original article: Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study Sudhir Tyagi 1, Sanjeev Kumar 2* 1 Assistant Professor, 2* Associate
Original article: Evaluation of Complications Occurring in Patients Undergoing Laparoscopic Cholecystectomy: An Institutional Based Study Sudhir Tyagi 1, Sanjeev Kumar 2* 1 Assistant Professor, 2* Associate
Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento
 Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento https://www.google.com/search?sa=g&hl=en&q=public+disclosure&tbm=isch&tbs=simg:caqsigeahwelekju2aqaaawlelcmpwgaygpgcamskpib_1qnza7ai
Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento https://www.google.com/search?sa=g&hl=en&q=public+disclosure&tbm=isch&tbs=simg:caqsigeahwelekju2aqaaawlelcmpwgaygpgcamskpib_1qnza7ai
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Gallstones & Other Biliary Disorders
 Gallstones & Other Biliary Disorders Jason Smith MD DMI FRCS(Gen.Surg) Consultant General & Colorectal Surgeon Introduction Gallstones are found in 12% men and 24% women Prevalence increases with advancing
Gallstones & Other Biliary Disorders Jason Smith MD DMI FRCS(Gen.Surg) Consultant General & Colorectal Surgeon Introduction Gallstones are found in 12% men and 24% women Prevalence increases with advancing