et al.. Long-term outcome of perianal fistulizing Crohn s disease treated with infliximab..
|
|
|
- Roy Shaw
- 5 years ago
- Views:
Transcription



1 Long-term outcome of perianal fistulizing Crohn s disease treated with infliximab. Guillaume Bouguen, Laurent Siproudhis, Emmanuel Gizard, Timothée Wallenhorst, Vincent Billioud, Jean-François Bretagne, Marc-André Bigard, Laurent Peyrin-Biroulet To cite this version: Guillaume Bouguen, Laurent Siproudhis, Emmanuel Gizard, Timothée Wallenhorst, Vincent Billioud, et al.. Long-term outcome of perianal fistulizing Crohn s disease treated with infliximab.. Clinical Gastroenterology and Hepatology, WB Saunders, 2013, 11 (8), pp e1-4. < /j.cgh >. <inserm > HAL Id: inserm Submitted on 23 Sep 2013 HAL is a multi-disciplinary open access archive for the deposit and dissemination of scientific research documents, whether they are published or not. The documents may come from teaching and research institutions in France or abroad, or from public or private research centers. L archive ouverte pluridisciplinaire HAL, est destinée au dépôt et à la diffusion de documents scientifiques de niveau recherche, publiés ou non, émanant des établissements d enseignement et de recherche français ou étrangers, des laboratoires publics ou privés.
2 Long-term outcome of perianal fistulizing Crohn s disease treated with infliximab Short title: Infliximab for perianal Crohn s fistula Guillaume Bouguen 1, Laurent Siproudhis 1, Emmanuel Gizard 2, Timothée Wallenhorst 1, Vincent Billioud 2, Jean-François Bretagne 1, Marc-André Bigard 2, Laurent Peyrin-Biroulet 2 1 Department of Hepato-Gastroenterology, University Hospital of Rennes, Pontchaillou, Inserm U991 university of Rennes 1, Rennes, France 2 Inserm, U954 and Department of Hepato-Gastroenterology, University Hospital of Nancy, Vandoeuvre-les-Nancy, France Grant support: This work did not receive any financial support. Abbreviations used in this paper: Tumor necrosis factor, TNF; Standard deviation, SD; Receiver operating characteristic, ROC; Inter Quartile Range, I.Q.R., perianal fistula of Crohn s disease, PCD; infliximab, IFX; Crohn s disease, CD. Correspondence to: Prof. Laurent Peyrin-Biroulet, MD, PhD Inserm U954, and Department of Hepato-Gastroenterology, University Hospital of Nancy, Allée du Morvan, Vandœuvre-lès-Nancy, FRANCE Phone: / Fax: address: peyrinbiroulet@gmail.com Disclosures G.B., has received lecture fees from Abbott Laboratories, Ferring and MSD Pharma 1
3 L.PB. has received consulting and/or lecture fees from Merck, Abbott Laboratories and UCB Pharma L.S. has received lecture fees from Abbott Laboratories and MSD Pharma J-F.B has received lecture fees from Abbott Laboratories V.B., E.G., M.A.B. declare no conflict of interest. Writing Assistance: none Author contributions: LPB and GB: study design, interpretation and analysis of data, editing of the manuscript; LS, EG, TW, VB, JFB and MAB collected data. All authors reviewed the paper and approved the final submitted draft. 2
4 ABSTRACT Background and aims: Long-term efficacy of infliximab in fistulizing perianal Crohn s disease is unknown. Outcomes and predictors of outcomes were evaluated in these patients. Methods: The medical records of 156 patients treated with infliximab for fistulizing perianal Crohn s disease in two referral centers between 1999 and 2010 were reviewed through September Cumulative probabilities of fistula closure and recurrence were estimated using the Kaplan- Meier method. Predictors of outcomes were identified using a Cox proportional hazards model. Results: At infliximab initiation, only 17.9% of patients had a simple fistula and seton drainage was performed for 97 (62%) patients. Concomitant immunosuppressants were used for 90 (56%) patients. After a median follow-up of 250 weeks, 108 (69%) patients experienced at least one fistula closure. Cumulative probabilities of first fistula closure were 40% and 65% at 1 and 5 years, respectively. Predictors of fistula closure were ileocolonic disease (HR=1.88), concomitant immunosuppressants (HR=2.58), duration of seton drainage < 34 weeks (HR=2.31) and a long duration of infliximab treatment (HR=1.76). Of the 108 patients, cumulative probabilities of first fistula recurrence were 16.6%, and 40.1% at 1 and 5 years, respectively. Forty-four (28.9%) patients developed an abscess during follow-up. A number of infliximab infusions beyond 19 was associated with less abscess recurrence (HR=0.33). At maximal follow-up, 55% of patients had fistula closure. Conclusions: About two thirds of patients experienced fistula closure and one third of patients had fistula recurrence after infliximab initiation. Combination therapy, duration of seton drainage under 34 weeks and long-term infliximab treatment were associated with better outcomes. Keywords: fistula, perianal disease, Crohn s disease, infliximab 3
5 INTRODUCTION Perianal fistulas are one of the more dreaded manifestations of Crohn's disease (CD). 1 Perianal disease generally denotes a more aggressive and disabling CD phenotype. 2,3 Patients with perianal CD (PCD) experience anal pain, discharge, dyschezia and fecal incontinence in addition to emotional symptoms and impairment of social and sexual functioning that significantly alter quality of life. 4 In population-based studies, perianal or rectal fistulas occur either before or after the diagnosis of CD in 13.7% to 37% of cases. 3,5-8 The treatment of PCD remains a challenge in clinical practice. Before the era of biologics, 40% of patients with PCD underwent proctocolectomy. 9 Over the last decade, tumor necrosis factor (TNF) antagonists have changed the way of treating both luminal and fistulizing CD refractory to standard medications. 10 Two large placebo-controlled, randomized trials demonstrated that infliximab (IFX) is effective in inducing and maintaining fistula closure in CD. 11,12 Adalimumab was also significantly more effective than placebo for inducing fistula closure in a subgroup analysis of the CHARM study. 13 Hence, anti-tnf therapy is recommended for the treatment of complex perianal fistulas in CD. 14,15 Surprisingly, data regarding the long-term outcome of perianal fistulas in patients with CD treated with IFX are scarce Due to small sample size and the relatively short follow-up of these studies, these results remain difficult to interpret. The aim of this study was therefore to evaluate the long-term outcome of fistulizing PCD beyond one year, in a large cohort of patients treated with IFX in two French referral centers. 4
6 METHODS Study population All hospital records of consecutive adult (age > 18 years) patients treated with IFX for CD in two French referral centers (University Hospitals of Rennes and Nancy, France) between January 1998 and September 2011, were reviewed. A centralized diagnostic index was used to identify all patients with diagnosis of CD. The database of these patients with CD was then compared to the pharmacy records of all patients treated with IFX at these two hospitals. All adult patients with documented PCD at first IFX infusion and an established diagnosis of CD based on clinical, biological, radiological, endoscopic and/or histological evidence were included. The following data were recorded: sex, birth date, age at diagnosis, CD phenotype according to the Montreal classification 24 at diagnosis, previous medications and history of surgery. Regarding IFX treatment, the date of first and last infusions, the number of infusions, and drug regimen for both induction and maintenance therapy were collected. IFX was administered initially at a dose of 5 mg/kg as a 2-h i.v. infusion in all patients included in this study; patients received one to three doses of IFX at weeks 0, 2 and 6 as induction therapy according to study period. Before 2003, maintenance treatment was individually tailored by the treating physician because of a lack of published data and regulatory approval defining the optimal maintenance treatment regimen. Maintenance treatment was defined as episodic (on demand) if IFX was given only upon relapse of symptoms and it was defined as scheduled if IFX was intentionally planned every 8 weeks as previously described. 25 Episodic treatment was also part of treatment discontinuation if patients had stopped IFX treatment for at least 4 months at maximal follow-up. Concomitant immunosuppressive medications were included in the analysis only if the total drug exposure lasted at least 3 months after IFX treatment initiation. Regarding concomitant therapy, two groups were analyzed: patients naïve to immunosuppressants (medication started after first IFX 5
7 infusion) and those with failure to immunosuppressants which were continued after IFX treatment initiation. All patients had clinical examination under general anesthesia, associated with MRI after 2002, before starting IFX therapy according to international guidelines. Perianal fistulas were classified according to the American Gastroenterological Association (AGA) classification as either simple or complex, 26 and abscesses were only defined as present or absent. All patients benefited from a standardized follow-up within first year. The patients were seen by their proctologist at week 6 at third IFX infusion and then at 6 months-1 year. All proctologic reports mentioning the evolution of fistulizing perianal lesions after first IFX infusion were reviewed until last news. All perianal surgeries after IFX initiation were collected, including the presence of seton drainage. All patients treated at University Hospitals of Rennes and Nancy for PCD benefit from a standardized follow-up by two experienced proctologists (L.S. and M.A.B.). Statistical analysis Quantitative variables were described as median and percentile (I.Q.R. for Inter Quartile Range: 25% and 75%). Categorical variables were presented as counts and percent of the cohort. Four events were defined: (1) fistula closure was defined as the absence of any draining by fistula openings at one visit, (2) recurrence of PCD defined by the presence of fistula openings among patient who experienced fistula closure, (3) recurrence of abscess after IFX initiation, and (4) sustained fistula closure for patients without any recurrence during the follow-up after PCD healing. The events were analyzed using survival analysis. The cumulative probabilities of fistula closure, recurrence of PCD or abscess were estimated using the Kaplan Meier method. For fistula closure and recurrence of abscess, the time to healing or to recurrence was considered to begin at 6
8 the date of first IFX infusion and end at the date of complete fistula closure/recurrence of abscess or last known follow-up. For fistula, the time to recurrence was considered to begin at the date of first fistula closure and the end at the date of event or last known follow-up. To identify factors predictive of each event, we performed a univariate analysis using the log-rank test. When considering the continuous variables for dichotomous analysis, cut-off values were determined using receiver operating characteristic (ROC) analysis to reduce the risk of bias related to arbitrarily defined cut-off and identify the optimal cut-off using each outcome as a classification variable. To identify independent predictors of surgery using a multivariate analysis, all significant variables with p values of <0.05 in the log-rank test were retained in the model and integrated into a Cox proportional hazards regression model. The results are shown as HRs with 95% CIs. Statistical analyses were performed using JMP Pro software. RESULTS Characteristics of the population at IFX initiation A total of 156 CD patients were included. The baseline characteristics at first IFX infusion are listed in Table 1. Of these patients, 61 (39%) were male (Table 1). The median age at CD diagnosis was 24 years (IQR 13-84) and the median duration of CD before IFX was 3.8 years (IQR 1-8). According to the Montreal classification, patients (15%) were diagnosed with a penetrating complication (B3) and 45% of the patients had ileo-colitis involvement (L3) at the time of diagnosis. Baseline clinical assessment revealed complex PCD for 128 patients (82%; 95% CI 75-87), including 90 patients (58%; 95% CI 50-65) with at least one abscess. A total of 98 patients (63%; 95% CI 55-70) underwent surgery for perianal fistula. Except one patient surgically treated with fistulotomy, all surgical procedures consisted of the placement of non-cutting draining seton(s). 7
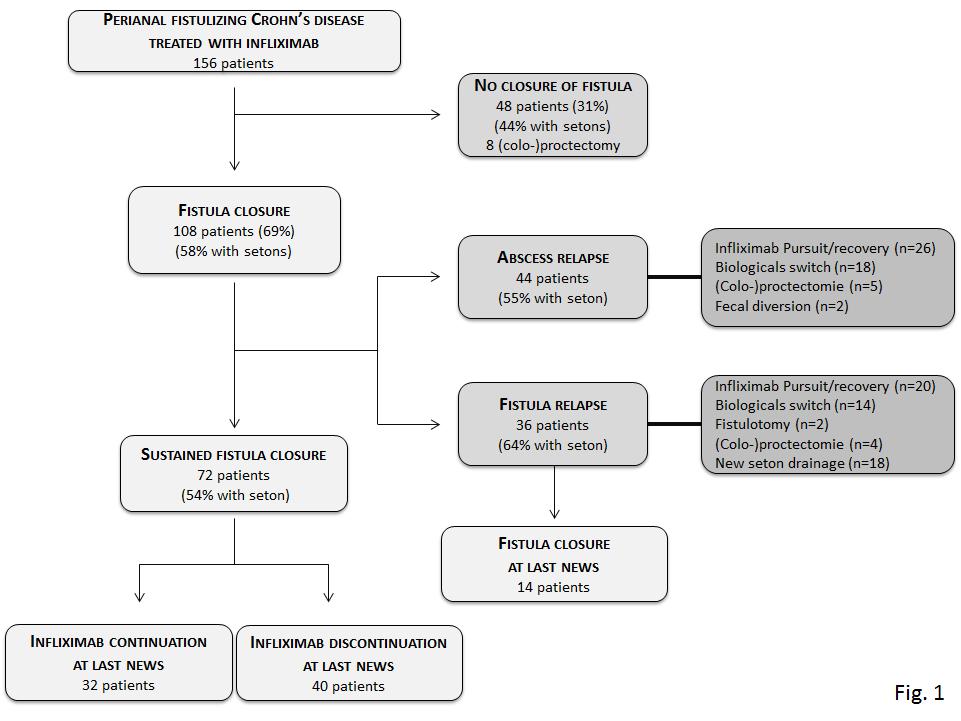
9 Fifty-one patients (36%) received immunosuppressant therapy before IFX therapy initiation and 3 patients had prior adalimumab treatment. Concomitant medications are listed in Table 1. Among the 90 patients receiving antibiotics, 27 patients had at least one abscess. A total of 105 patients were naïve to immunosuppressant. A combination therapy (IFX in association with an immunosuppressant) was started for 26 patients of these 105 patients, including 25 patients treated with thiopurine and one patient receiving methotrexate. Management of perianal lesions during follow-up (Figure 1) After a median duration follow-up of 250 weeks (IQR ), a total of 2536 IFX infusions were administered to the 156 included patients, corresponding to a median number of IFX infusions per patient of 11.5 (IQR 5-23). Induction regimen with 3 IFX infusions at week 0, 2 and 6 were performed for 151 patients. One patient had only one infusion and the 4 remaining patients had to stop IFX after the second infusion because of side effects. Regarding maintenance IFX treatment, 42 patients (27%; 95% CI 21-34) had only episodic IFX regimen, 90 patients (58%; 95% CI 50-65) had scheduled IFX treatment with infusions every 8 weeks, and 24 patients (15%; 95% CI 11-22) had first episodic treatment before receiving scheduled IFX maintenance treatment (Table 1). For patients undergoing a seton drainage, IFX was started after a median time of 4 weeks after surgery (IQR ). Removal of seton was performed for 95 of 97 patients after a median duration of 33 weeks (~1.2 years; IQR 14-64). Additional surgical procedures were performed for 37 patients (24%;95CI 17-31), consisting of fistulotomy for 17 patients, rectal advancement flap for one patient, fibrin glue for 15 patients and anal fistula plug for 4 patients. Anti-TNF treatment was still ongoing for 90 of the 156 patients (57%) at last news: 67 patients were still on IFX, 21 patients switched from IFX to adalimumab and 2 patients were receiving cerolizumab pegol as a third-line anti-tnf therapy. IFX treatment was discontinued after a 8
10 median duration of 86 weeks (IQR ) for the following reasons: 40 patients (22%) achieved sustained clinical benefit, 21 patients (14%) were primary or secondary non-responders leading to switch to adalimumab for 20 patients, 17 patients (11%) experienced adverse events leading to switch TNFα antagonist for 10 patients, and 10 patients (6%) for other reasons. Finally, 72 (46%) patients achieved sustained fistula closure with IFX treatment without requiring switching to another biological agent. Fistula closure Of the 156 patients, 108 (69%; 95% CI 61-75) had at least one complete closure of fistulas during follow-up. The median time to first fistula closure from IFX initiation was 53 weeks (~1 year; IQR ). The cumulative probabilities of first clinical fistula closure at 1, 3, 5 and 10 years from the time of IFX initiation were 33%, 59%, 73% and 88%, respectively (Figure 2). At maximal follow-up, 86 (55%; 95% CI 47-63) patients had complete fistula closure. Importantly, 72 (46%) of the 156 patients had sustained complete fistula closure throughout follow-up, including maximal follow-up. The cumulative probabilities of sustained complete fistula closure were 22%, 43%, and 57% at 1, 3, and 5 years from the time of IFX initiation, respectively. Factors associated with fistula closure In the ROC analysis, optimal cut-off values associated with fistula closure were over 118 weeks for duration of IFX treatment, less than 34 weeks for duration of seton drainage, and less than 6 weeks between surgery and IFX initiation. All baseline factors were evaluated in the univariate analysis using the log-rank test (See Supplementary Table 1 online). Ileocolonic disease, simple fistula, absence of draining seton, 9
11 treatment with IFX for >118 weeks as defined by ROC analysis and combination therapy were associated with fistula closure. Conversely, ileal disease, draining seton(s), long duration of inserted seton(s) over 34 weeks and long duration between surgery and IFX initiation over 6 weeks were negatively associated with fistula closure. Overall, additional surgeries (including fistulotomy, flap advancement, fibrin glue and plug) were not associated with an increased rate of fistula closure. When considering the type of additional surgery, fistulotomy but not fibrin glue was significantly associated with an increased rate of fistula closure. The other surgical procedures (flap advancement and plug) were not taking into account because of the low number of patients. Using multivariate analysis, patients with ileocolonic disease, long-term IFX treatment over 118 weeks (2.2 years), combination therapy for patient naïve to immunosuppressant, and short draining seton(s) under 34 weeks duration were associated with first fistula closure (Table 2 and Figure 3). Concerning sustained fistula closure, all baseline factors and treatment characteristics were first evaluated in the univariate analysis using the log-rank test (See Supplementary Table 2 online). Simple fistula, prior major abdominal surgery, absence of seton and short seton drainage duration were associated with an increased probabilities of achieving sustained fistula closure. Conversely, IFX discontinuation and a long interval period over 6 weeks between the placement of seton and the start of IFX was negatively associated with sustained fistula closure. Using multivariate analysis, sustained fistula closure was associated with a drainage seton duration <34 weeks (HR=2.6; CI% p=0.0085) and negatively associated with IFX therapy discontinuation (HR=0.18; 95% CI ) (See Supplementary Table 3). Recurrence of fistula and abscess 10
12 Of the 108 patients who experienced at least one complete fistula closure, 36 (33.3%, 95% CI 25-42) had recurrence of fistula, including 24 patients with concomitant abscess. A non-cutting seton was inserted for half of patients (n=18) in case of fistula recurrence. The cumulative probabilities of first fistula recurrence were 16.6%, 31.3%, 40.1% at 1, 3 and 5 years, respectively.(see Supplementary Figure 1). When considering only the subgroup of patients treated with maintenance IFX treatment, the cumulative probabilities of first fistula recurrence were broadly similar: 12% and 36.6% at 1 and 5 years, respectively. A total of 13 patients (9%, 95% CI 5-14) underwent proctectomy or coloproctectomy for disease refractory to IFX therapy and a stomy was performed for 2 additional patients. Of the 156 patients 44 (29%, 95% CI 22-36) had abscess recurrence. Among them, 26 patients developed an abscess while ongoing IFX treatment and 26 patients required a new seton drainage. Of note, among the 90 patients with an abscess at time of IFX initiation, 26 patients (28.9%) had abscess recurrence. Factors associated with fistula and abscess recurrence Using log rang test, only ileal disease was associated with fistula recurrence (See Supplementary Table 4 online). None of the baseline characteristics, including concomitant medications, were associated with fistula recurrence using multivariate analysis. When considering abscess recurrence, IFX discontinuation and a low number of infusions (under 19 using ROC curve analysis) were associated with recurrence in univariate analysis (See Supplementary Table 5 online). Using the Cox proportional hazards regression model, only a number of IFX infusions over 19 was negatively associated with abscess recurrence (HR=0.33; 95% CI 0.13 to 0.77, p=0.0096) (Figure 4). 11
13 DISCUSSION This is the largest study specifically investigating the long-term outcome of perianal fistulizing CD treated with IFX, with a median follow-up of 5 years. All patients were managed by two experienced proctologists (L.S. and M.A.B.) according to international guidelines. 14,15 We found that the cumulative probability of first fistula closure was 33% at one year. These results are in line with those of the ACCENT II trial that evaluated maintenance IFX treatment until at one year in fistulizing CD. 12 In this trial enrolling a total of 282 patients, 271 (96%) patients had perianal fistulas. Over the 54-week study, 36% of the patients had a complete absence of draining fistula, which was significantly superior to the placebo. 12 Data on long-term outcome beyond one year of fistulizing PCD treated with IFX were scarce. Retrospective studies of small sample size reported that 29%, 18%, 75% and 42% of patients treated with IFX achieved sustained complete fistula closure after a median follow-up ranging from 20 to 60 months. 16,18,19,22 Only the group of Leuven has evaluated the long-term efficacy of IFX in fistulizing CD on a large cohort treated with IFX, but the authors did not formally analyze the outcome of perinal fistulas/abscess. 25 Some studies reported a same efficacy for surgery alone and an approach combining surgery and IFX treatment. 17,19,23 However, these studies were of small sample size and patients were only receiving IFX induction therapy. We showed that the cumulative probability of fistula closure was 73% at 5 years and 88% at 10 years. Interestingly, after a median follow-up of 5 years, 72 (46%) of the 156 patients had sustained fistula closure. These findings underscore the beneficial effect of IFX in these patients in the long term. Predictors of long-term outcomes in patients treated with infliximab for perianal fistulizing Crohn s disease had never been formally investigated. As observed in the population-based study from Stockholm county conducted in the pre-biologic era, we found that ileocolonic disease was 12
14 associated with a better outcome. 9 Available data were conflicting in PCD concerning the efficacy of concomitant immunosuppressant use. Subgroup analysis of the ACCENT II trial found that concomitant immunosuppressants did not improve response rates to IFX at one year. 27 By contrast, the recent SONIC trial has clearly shown therapeutic gain when IFX therapy is used in combination with azathioprine in luminal CD in immunosuppressants naïve patients. 28 About 12% of patients had perianal fistulas but no separate analysis was performed in this group to determine the relative benefits of single or dual therapy In a prospective study enrolling 18 patients treated with IFX, combination therapy was not associated with better outcomes, but this finding remains difficult to interpret due to small sample size. 29 Importantly, we could demonstrate that combination therapy was associated with higher fistula closure rates. We also found that duration of seton drainage under 34 weeks was associated with better outcomes. In our study, removal of seton was performed for 95 of 97 patients after a median duration of 33 weeks. Little is known about the ideal removal time of seton after starting anti- TNF therapy; it is ranging from 3 weeks to 3 months in available reports. 19,21,29,31,32 Present et al found that closure of draining fistulae by IFX treatment was characterized by rapid onset (usually within 2 weeks) and a lasting benefit of action, with a median duration of closure of 12 weeks. 12,33 Our results are likely explained by the fact that a longer duration of seton drainage may be required in partial responders or non-responders to IFX. Short duration of seton drainage might reflect less severe disease (either less fistula tracks or less complex anatomy of the tracks), thus leading to a quicker removal of the setons. Moreover, except fistulotomy restricted to low and simple fistula, none of additional surgical procedure, including plug, fibrin glue or advancement flap was associated to clinical remission underlying the low efficacy of associated surgery for the treatment of PCD. 13
15 Recurrence of PCD after initial fistula closure was high in our study, occurring in about one third of patients during follow-up. In the ACCENT II trial, 42% of randomized patients treated with IFX as maintenance therapy experienced loss of response, including 16% of patients with recrudescence of fistulas. A prospective trial reported a 16% rate of loss of response at 18 months after IFX induction therapy followed by methotrexate maintenance therapy. 21 In the pre-biologic era nearly half of patients experienced fistula recurrence after first treatment of perianal fistula with only anal surgery. 9 Regarding perianal abscess, the ACCENT II trial showed that maintenance IFX did not result in increased abscess development in fistulizing CD (12% in the IFX group versus 17% in the placebo group). 12 Our data are consistent with these results as 26 patients (16.6%) developed an anal abscess after IFX therapy initiation. We found that long-term IFX treatment was associated with less abscess recurrence, further highlighting the long-term efficacy of IFX treatment in PCD. A limitation of our study, in addition to its retrospective study design, is the absence of MRI data, as it was not routinely performed during study period. The main strengths are the duration of follow-up (about 5 years), the management of patients by experienced proctologists with a standardized monitoring on the largest cohort specifically investigating the long-term outcome of perianal fistulizing CD treated with IFX. In conclusion, our results indicate that about two thirds of patients experienced fistula closure and one third of patients had fistula recurrence after infliximab initiation. At last follow-up, 46% of patients had sustained fistula closure. Combination therapy, duration of seton drainage < 34 weeks and long-term infliximab treatment were associated with better outcomes. 14
16 REFERENCES 1. Schwartz DA. Editorial: Imaging and the treatment of Crohn's perianal fistulas: to see is to believe. Am J Gastroenterol 2009;104: Ingle SB, Loftus EV, Jr. The natural history of perianal Crohn's disease. Dig Liver Dis 2007;39: Schwartz DA, Loftus EV, Jr., Tremaine WJ, et al. The natural history of fistulizing Crohn's disease in Olmsted County, Minnesota. Gastroenterology 2002;122: Mahadev S, Young JM, Selby W, et al. Quality of life in perianal Crohn's disease: what do patients consider important? Dis Colon Rectum 2011;54: Lapidus A. Crohn's disease in Stockholm County during : an epidemiological update. World J Gastroenterol 2006;12: Lapidus A, Bernell O, Hellers G, et al. Clinical course of colorectal Crohn's disease: a 35-year follow-up study of 507 patients. Gastroenterology 1998;114: Peyrin-Biroulet L, Loftus EV, Jr., Colombel JF, et al. The natural history of adult Crohn's disease in population-based cohorts. Am J Gastroenterol 2010;105: Tang LY, Rawsthorne P, Bernstein CN. Are perineal and luminal fistulas associated in Crohn's disease? A population-based study. Clin Gastroenterol Hepatol 2006;4: Hellers G, Bergstrand O, Ewerth S, et al. Occurrence and outcome after primary treatment of anal fistulae in Crohn's disease. Gut 1980;21: Peyrin-Biroulet L, Deltenre P, de Suray N, et al. Efficacy and safety of tumor necrosis factor antagonists in Crohn's disease: meta-analysis of placebo-controlled trials. Clin Gastroenterol Hepatol 2008;6:
17 11. Present DH, Rutgeerts P, Targan S, et al. Infliximab for the treatment of fistulas in patients with Crohn's disease. N Engl J Med 1999;340: Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance therapy for fistulizing Crohn's disease. N Engl J Med 2004;350: Colombel JF, Schwartz DA, Sandborn WJ, et al. Adalimumab for the treatment of fistulas in patients with Crohn's disease. Gut 2009;58: Lichtenstein GR, Hanauer SB, Sandborn WJ. Management of Crohn's disease in adults. Am J Gastroenterol 2009;104:465-83; quiz 64, Van Assche G, Dignass A, Reinisch W, et al. The second European evidence-based Consensus on the diagnosis and management of Crohn's disease: Special situations. J Crohns Colitis 2010;4: Antakia R, Shorthouse AJ, Robinson K, et al. Combined modality treatment for Complex Fistulating Perianal Crohn's Disease. Colorectal Dis in press 17. Gaertner WB, Decanini A, Mellgren A, et al. Does infliximab infusion impact results of operative treatment for Crohn's perianal fistulas? Dis Colon Rectum 2007;50: Hotokezaka M, Ikeda T, Uchiyama S, et al. Results of seton drainage and infliximab infusion for complex anal Crohn's disease. Hepatogastroenterology 2011;58: Hyder SA, Travis SP, Jewell DP, et al. Fistulating anal Crohn's disease: results of combined surgical and infliximab treatment. Dis Colon Rectum 2006;49: Karmiris K, Bielen D, Vanbeckevoort D, et al. Long-term monitoring of infliximab therapy for perianal fistulizing Crohn's disease by using magnetic resonance imaging. Clin Gastroenterol Hepatol 2011;9:
18 21. Roumeguere P, Bouchard D, Pigot F, et al. Combined approach with infliximab, surgery, and methotrexate in severe fistulizing anoperineal Crohn's disease: results from a prospective study. Inflamm Bowel Dis 2011;17: Tougeron D, Savoye G, Savoye-Collet C, et al. Predicting factors of fistula healing and clinical remission after infliximab-based combined therapy for perianal fistulizing Crohn's disease. Dig Dis Sci 2009;54: Uchino M, Ikeuchi H, Bando T, et al. Long-term efficacy of infliximab maintenance therapy for perianal Crohn's disease. World J Gastroenterol 2011;17: Satsangi J, Silverberg MS, Vermeire S, et al. The Montreal classification of inflammatory bowel disease: controversies, consensus, and implications. Gut 2006;55: Schnitzler F, Fidder H, Ferrante M, et al. Long-term outcome of treatment with infliximab in 614 patients with Crohn's disease: results from a single-centre cohort. Gut 2009;58: Sandborn WJ, Fazio VW, Feagan BG, et al. AGA technical review on perianal Crohn's disease. Gastroenterology 2003;125: Lichtenstein GR, Diamond RH, Wagner CL, et al. Clinical trial: benefits and risks of immunomodulators and maintenance infliximab for IBD-subgroup analyses across four randomized trials. Aliment Pharmacol Ther 2009;30: Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn's disease. N Engl J Med 2010;362: Ng SC, Plamondon S, Gupta A, et al. Prospective evaluation of anti-tumor necrosis factor therapy guided by magnetic resonance imaging for Crohn's perineal fistulas. Am J Gastroenterol 2009;104:
19 30. Tozer P, Ng SC, Siddiqui MR, et al. Long-term MRI-guided combined anti-tnf-alpha and thiopurine therapy for crohn's perianal fistulas. Inflamm Bowel Dis 2012., in press 31. Topstad DR, Panaccione R, Heine JA, et al. Combined seton placement, infliximab infusion, and maintenance immunosuppressives improve healing rate in fistulizing anorectal Crohn's disease: a single center experience. Dis Colon Rectum 2003;46: van der Hagen SJ, Baeten CG, Soeters PB, et al. Anti-TNF-alpha (infliximab) used as induction treatment in case of active proctitis in a multistep strategy followed by definitive surgery of complex anal fistulas in Crohn's disease: a preliminary report. Dis Colon Rectum 2005;48: Rutgeerts P. Review article: treatment of perianal fistulizing Crohn's disease. Aliment Pharmacol Ther 2004;20:
20 Table 1: Baseline characteristics Variable Gender (M:F) Median age at first IFX infusion years (min-max) Median disease duration years (min-max) Montreal classification at first infliximab infusion n (%; 95% CI) Disease location L1 ileal L2 colonic L3 ileo-colonic L4 upper digestive tract Disease behavior B1 non-penetrating non-stricturing B2 stricturing B3 penetrating Prior treatment n (%; 95% CI ) Purine analog (Azathioprine/6-mercaptopurine) Methotrexate Adalimumab Major abdominal surgery Infliximab treatment Regiment n (%; 95% CI ) Episodic Episodic then scheduled Scheduled Median duration of seton drainage before IFX weeks (IQR75) Concomitant medications n (%; 95% CI ) Steroids Purine analog (azathioprine/6-mercaptopurine) Methotrexate Antibiotics Perianal disease n (%; 95% CI ) Perianal Fistula according to the AGA classification Simple Complex Associated abscess Placement of seton IFX, Infliximab; CI, confidence interval; M, male; F, female Patients (n=156) 61: (13-84) 3.8 (0-30) 19 (12.2 ; ) 63 (40 ; 33-48) 70 (45 ; 37-53) 8 (5.8 ; ) 113 (72.5 ; ) 19 (12.1 ; ) 24 (15.4 ; ) 51 (32.7 ; ) 6 (3.8 ; ) 3 (2 ; ) 44 (28 ; ) 57 (36 ; ,3) 9 (5,7 ; 3-10,6) 90 (57,7 ; ,2) 4 ( ) 45 (28.8 ; ) 82 (82.5 ; ) 8 (5.1 ; ) 90 (57.7 ; ) 28 (17.9 ; ) 128 (82 ; ) 90 (58.1 ; ) 98 (63.22 ; ) 19
21 Table 2: Factors associated with first perianal fistula closure, as determined by multivariate analysis Covariates HR 95% CI of HR p-value L1 (isolated ileal disease) behavior L3 (ileocolonic disease) behavior Seton drain duration < 34 weeks IFX duration > 118 weeks Combination therapy immunosuppressant/ifx Combination therapy immunosuppressant/ifx for naïve patients Simple vs Complex perianal fistula* Interval between seton drainage and IFX initiation less than 6 weeks HR, Hazard Ratio; IFX, infliximab;*according to the AGA classification 26 ;CI, confidence interval; M, male; F, female 20
22 Figure legends Figure 1: Flow chart of the 156 patients. Figure 2: Cumulative probability of first fistula closure Figure 3: Kaplan-Meier analysis of first fistula closure after infliximab therapy initiation according to predictors identified by multivariate analysis (A) Ileocolonic disease (L3) (B) Seton drainage duration (C) Long-term treatment with infliximab over 118 months (D) Combination therapy for immunosuppressants naïve patients. Figure 4: Cumulative probability of fistula recurrence among the 108 patients who experienced fistula closure. 21
23 22
24 23
25 24
26 25
Crohn s disease: is there any link between anal and luminal phenotypes?
 Crohn s disease: is there any link between anal and luminal phenotypes? Timothée Wallenhorst, Charlène Brochard, Jean-François Bretagne, Guillaume Bouguen, Laurent Siproudhis To cite this version: Timothée
Crohn s disease: is there any link between anal and luminal phenotypes? Timothée Wallenhorst, Charlène Brochard, Jean-François Bretagne, Guillaume Bouguen, Laurent Siproudhis To cite this version: Timothée
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Percent Cumulative. Probability. Penetrating. Inflammatory. Stricturing. Months Patients at risk N =
 Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Sunanda Kane, MD, FACG Professor of Medicine Department of Gastroenterology and Hepatology Mayo Clinic Rochester, MN In my lecture today, I will be
Crohn's Disease The What, When, and Why of Treatment Sunanda Kane, MD, FACG Professor of Medicine Department of Gastroenterology and Hepatology Mayo Clinic Rochester, MN In my lecture today, I will be
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc. Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Konservative Behandlungsmöglichkeiten?
 PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Fisteln bei M. Crohn : Konservative Behandlungsmöglichkeiten? INTERDISZIPLINÄRE VISZERALE CHIRURGIE
PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Fisteln bei M. Crohn : Konservative Behandlungsmöglichkeiten? INTERDISZIPLINÄRE VISZERALE CHIRURGIE
EXPERIMENTAL AND THERAPEUTIC MEDICINE 12: , 2016
 EXPERIMENTAL AND THERAPEUTIC MEDICINE 12: 1939-1945, 2016 Similar outcomes for anti-tumor necrosis factor-α antibody and immunosuppressant following seton drainage in patients with Crohn's disease-related
EXPERIMENTAL AND THERAPEUTIC MEDICINE 12: 1939-1945, 2016 Similar outcomes for anti-tumor necrosis factor-α antibody and immunosuppressant following seton drainage in patients with Crohn's disease-related
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Epidemiology / Morbidity
 Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort
 Alimentary Pharmacology and Therapeutics Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort N. Gies, K. I. Kroeker, K. Wong & R. N. Fedorak Division
Alimentary Pharmacology and Therapeutics Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort N. Gies, K. I. Kroeker, K. Wong & R. N. Fedorak Division
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Long-term outcome after infliximab for refractory ulcerative colitis
 Journal of Crohn's and Colitis (2008) 2, 219 225 available at www.sciencedirect.com Long-term outcome after infliximab for refractory ulcerative colitis Marc Ferrante a, Séverine Vermeire a, Herma Fidder
Journal of Crohn's and Colitis (2008) 2, 219 225 available at www.sciencedirect.com Long-term outcome after infliximab for refractory ulcerative colitis Marc Ferrante a, Séverine Vermeire a, Herma Fidder
Perianal fistulizing Crohn s disease (pfcd) comprises a wide
 comprises a wide") CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:130 136 Long-Term Monitoring of Infliximab Therapy for Perianal Fistulizing Crohn s Disease by Using Magnetic Resonance Imaging KONSTANTINOS KARMIRIS,* DIDIER
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:130 136 Long-Term Monitoring of Infliximab Therapy for Perianal Fistulizing Crohn s Disease by Using Magnetic Resonance Imaging KONSTANTINOS KARMIRIS,* DIDIER
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Levels of C-reactive Protein Are Associated With Response to Infliximab Therapy in Patients With Crohn s Disease
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:421 427 Levels of C-reactive Protein Are Associated With Response to Infliximab Therapy in Patients With Crohn s Disease MATTHIAS JÜRGENS,* JESTINAH M. MAHACHIE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:421 427 Levels of C-reactive Protein Are Associated With Response to Infliximab Therapy in Patients With Crohn s Disease MATTHIAS JÜRGENS,* JESTINAH M. MAHACHIE
healing with methotrexate in Crohn s disease: a prospective comparative study with azathioprine infliximab
 Mucosal healing with methotrexate in Crohn s disease: a prospective comparative study with azathioprine and infliximab David Laharie, Armel Reffet, Genevieve Belleannée, Edouard Chabrun, Clement Subtil,
Mucosal healing with methotrexate in Crohn s disease: a prospective comparative study with azathioprine and infliximab David Laharie, Armel Reffet, Genevieve Belleannée, Edouard Chabrun, Clement Subtil,
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy of Adalimumab in Korean Patients with Crohn s Disease
 Gut and Liver, Vol. 10, No. 2, March 2016, pp. 255-261 ORiginal Article Efficacy of Adalimumab in Korean Patients with Crohn s Disease Il Woong Sohn, Sung Tae Kim, Bun Kim, Hyun Jung Lee, Soo Jung Park,
Gut and Liver, Vol. 10, No. 2, March 2016, pp. 255-261 ORiginal Article Efficacy of Adalimumab in Korean Patients with Crohn s Disease Il Woong Sohn, Sung Tae Kim, Bun Kim, Hyun Jung Lee, Soo Jung Park,
Perianal Fistula of Crohn s Disease
 Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
Case 3 Perianal Fistula of Crohn s Disease A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain
The Best of IBD at UEGW (Crohn s)
") The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Mono or Combination Therapy with. Individualized Approach
 Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review)
") Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Tumor necrosis factor-alpha antibody for maintenace of remission in Crohn s disease (Review) Behm BW, Bickston SJ This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease
 Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions
: Future Directions") Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Title: Treatment persistence during therapeutic sequences with adalimumab and. and infliximab in the treatment of Crohn s. disease
 Title: Treatment persistence during therapeutic sequences with adalimumab and infliximab in the treatment of Crohn s disease Authors: Carlos Taxonera, Pilar Robledo, Antonio Rodriguez DOI: 10.17235/reed.2017.4931/2017
Title: Treatment persistence during therapeutic sequences with adalimumab and infliximab in the treatment of Crohn s disease Authors: Carlos Taxonera, Pilar Robledo, Antonio Rodriguez DOI: 10.17235/reed.2017.4931/2017
Severe IBD: What to Do When Anti- TNFs Don t Work?
 Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Infliximab as rescue medication for patients with severe ulcerative/indeterminate colitis refractory to tacrolimus
 Infliximab as rescue medication for patients with severe ulcerative/indeterminate colitis refractory to tacrolimus Klaus R. Herrlinger, Daniel N Barthel, Klaus Jürgen Schmidt, Juergen Buening, Christiane
Infliximab as rescue medication for patients with severe ulcerative/indeterminate colitis refractory to tacrolimus Klaus R. Herrlinger, Daniel N Barthel, Klaus Jürgen Schmidt, Juergen Buening, Christiane
Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger
 ORIGINAL ARTICLE: GASTROENTEROLOGY Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger Judith R. Kelsen, Andrew B. Grossman, Helen Pauly-Hubbard, Kernika Gupta, Robert N. Baldassano, and
ORIGINAL ARTICLE: GASTROENTEROLOGY Infliximab Therapy in Pediatric Patients 7 Years of Age and Younger Judith R. Kelsen, Andrew B. Grossman, Helen Pauly-Hubbard, Kernika Gupta, Robert N. Baldassano, and
Corporate Presentation
 Corporate Presentation The treatment of perianal December fistula 2015in Crohn s disease patients Key Opinion Leader Event 8 th May 2017 Forward-Looking Statements This document does not constitute or
Corporate Presentation The treatment of perianal December fistula 2015in Crohn s disease patients Key Opinion Leader Event 8 th May 2017 Forward-Looking Statements This document does not constitute or
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball
 Looking for the Crystal Ball") Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study
 ORIGINAL ARTICLE The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study Norimitsu Uza, Hiroshi Nakase, Satoru Ueno, Satoko Inoue, Sakae Mikami, Hiroyuki Tamaki,
ORIGINAL ARTICLE The Effect of Medical Treatment on Patients with Fistulizing Crohn s Disease: A Retrospective Study Norimitsu Uza, Hiroshi Nakase, Satoru Ueno, Satoko Inoue, Sakae Mikami, Hiroyuki Tamaki,
Trends in Biologic Therapy for Crohn s Disease: Where Are We and Where Are We Going? CME
 Trends in Biologic Therapy for Crohn s Disease: Where Are We and Where Are We Going? CME Uma Mahadevan-Velayos, MD Supported by independent educational grants from View this activity online at: medscape.org/column/crohns
Trends in Biologic Therapy for Crohn s Disease: Where Are We and Where Are We Going? CME Uma Mahadevan-Velayos, MD Supported by independent educational grants from View this activity online at: medscape.org/column/crohns
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
T he treatment strategy for Crohn s disease (CD) is
 is") 237 INFLAMMATORY BOWEL DISEASE Impact of the increasing use of immunosuppressants in Crohn s disease on the need for intestinal surgery J Cosnes, I Nion-Larmurier, L Beaugerie, P Afchain, E Tiret, J-P
237 INFLAMMATORY BOWEL DISEASE Impact of the increasing use of immunosuppressants in Crohn s disease on the need for intestinal surgery J Cosnes, I Nion-Larmurier, L Beaugerie, P Afchain, E Tiret, J-P
Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma: a pilot study
 Tech Coloproctol (2015) 19:455 459 DOI 10.1007/s10151-015-1311-8 ORIGINAL ARTICLE Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma:
Tech Coloproctol (2015) 19:455 459 DOI 10.1007/s10151-015-1311-8 ORIGINAL ARTICLE Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma:
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
Available online at ScienceDirect
 Journal of Crohn's and Colitis (2014) 8, 1454 1463 Available online at www.sciencedirect.com ScienceDirect Crohn's disease outpatients treated with adalimumab have an earlier secondary loss of response
Journal of Crohn's and Colitis (2014) 8, 1454 1463 Available online at www.sciencedirect.com ScienceDirect Crohn's disease outpatients treated with adalimumab have an earlier secondary loss of response
Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series
 CASE REPORT Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series Kaori Fujiwara, Takuya Inoue, Naoki Yorifuji, Munetaka Iguchi, Taisuke Sakanaka, Ken Narabayashi,
CASE REPORT Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series Kaori Fujiwara, Takuya Inoue, Naoki Yorifuji, Munetaka Iguchi, Taisuke Sakanaka, Ken Narabayashi,
Anus,Rectum and Colon
 JOURNAL OF THE Anus,Rectum and Colon http://journal-arc.jp ORIGINAL RESEARCH ARTICLE Risk factors for recurrence of Crohn s disease requiring surgery in patients receiving post-operative anti-tumor necrosis
JOURNAL OF THE Anus,Rectum and Colon http://journal-arc.jp ORIGINAL RESEARCH ARTICLE Risk factors for recurrence of Crohn s disease requiring surgery in patients receiving post-operative anti-tumor necrosis
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Withdrawal of drug therapy in patients with quiescent Crohn s disease
 Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Scottish Medicines Consortium
 Scottish Medicines Consortium infliximab 100mg powder for intravenous infusion (Remicade ) No. (364/07) Schering-Plough UK Ltd 6 April 2007 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium infliximab 100mg powder for intravenous infusion (Remicade ) No. (364/07) Schering-Plough UK Ltd 6 April 2007 The Scottish Medicines Consortium (SMC) has completed its assessment
Anti-tumour necrosis factor treatment of inflammatory bowel disease in liver transplant recipients
 Alimentary Pharmacology and Therapeutics Anti-tumour necrosis factor treatment of inflammatory bowel disease in liver transplant recipients A. B. Mohabbat*, W. J. Sandborn, E. V. Loftus Jr, R. H. Wiesner
Alimentary Pharmacology and Therapeutics Anti-tumour necrosis factor treatment of inflammatory bowel disease in liver transplant recipients A. B. Mohabbat*, W. J. Sandborn, E. V. Loftus Jr, R. H. Wiesner
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Crohn disease is a chronic inflammatory bowel disease
 GASTROENTEROLOGY 2010;139:1147 1155 Risk Factors Associated With Progression to Intestinal Complications of Crohn s Disease in a Population-Based Cohort KELVIN T. THIA,*, WILLIAM J. SANDBORN,* WILLIAM
GASTROENTEROLOGY 2010;139:1147 1155 Risk Factors Associated With Progression to Intestinal Complications of Crohn s Disease in a Population-Based Cohort KELVIN T. THIA,*, WILLIAM J. SANDBORN,* WILLIAM
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy
 Dipartimento di Scienze Mediche e Chirurgiche Istituto di Clinica Chirurgica Prof. Aroldo Fianchini Ancona INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy Cristina Marmorale PERIANAL
Dipartimento di Scienze Mediche e Chirurgiche Istituto di Clinica Chirurgica Prof. Aroldo Fianchini Ancona INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy Cristina Marmorale PERIANAL
Immunogenicity of Biologic Agents and How to Prevent Sensitization
 Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Effectiveness of Concomitant Enteral Nutrition Therapy and Infliximab for Maintenance Treatment of Crohn s Disease in Adults
 Dig Dis Sci (2013) 58:1329 1334 DOI 10.1007/s10620-012-2374-2 ORIGINAL ARTICLE Effectiveness of Concomitant Enteral Nutrition Therapy and Infliximab for Maintenance Treatment of Crohn s Disease in Adults
Dig Dis Sci (2013) 58:1329 1334 DOI 10.1007/s10620-012-2374-2 ORIGINAL ARTICLE Effectiveness of Concomitant Enteral Nutrition Therapy and Infliximab for Maintenance Treatment of Crohn s Disease in Adults
Review article: remission rates achievable by current therapies for inflammatory bowel disease
 Alimentary Pharmacology and Therapeutics Review article: remission rates achievable by current therapies for inflammatory bowel disease L. Peyrin-Biroulet* & M. Lémann,1 *Inserm U954 and Department of
Alimentary Pharmacology and Therapeutics Review article: remission rates achievable by current therapies for inflammatory bowel disease L. Peyrin-Biroulet* & M. Lémann,1 *Inserm U954 and Department of
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
Evaluation of adalimumab therapy in multidisciplinary strategy for perianal Crohn's disease patients with infliximab failure
 Journal of Crohn's and Colitis (2010) 4, 654 660 available at www.sciencedirect.com Evaluation of adalimumab therapy in multidisciplinary strategy for perianal Crohn's disease patients with infliximab
Journal of Crohn's and Colitis (2010) 4, 654 660 available at www.sciencedirect.com Evaluation of adalimumab therapy in multidisciplinary strategy for perianal Crohn's disease patients with infliximab
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Ulcerative colitis (UC) and Crohn s disease (CD) are
 and Crohn s disease (CD) are") Original Article Changing Infliximab Prescription Patterns in Inflammatory Bowel Disease: A Population-Based Cohort Study, 1999 2014 Lone Larsen, MD,* Asbjørn Mohr Drewes, MD, PhD, DMSc,*, Marie Christine
Original Article Changing Infliximab Prescription Patterns in Inflammatory Bowel Disease: A Population-Based Cohort Study, 1999 2014 Lone Larsen, MD,* Asbjørn Mohr Drewes, MD, PhD, DMSc,*, Marie Christine
The Natural History of Fistulizing Crohn s Disease in Olmsted County, Minnesota
 GASTROENTEROLOGY 2002;122:875 880 CLINICAL RESEARCH The Natural History of Fistulizing Crohn s Disease in Olmsted County, Minnesota DAVID A. SCHWARTZ,* EDWARD V. LOFTUS, JR.,* WILLIAM J. TREMAINE,* REMO
GASTROENTEROLOGY 2002;122:875 880 CLINICAL RESEARCH The Natural History of Fistulizing Crohn s Disease in Olmsted County, Minnesota DAVID A. SCHWARTZ,* EDWARD V. LOFTUS, JR.,* WILLIAM J. TREMAINE,* REMO
Virtual imaging for teaching cardiac embryology.
 Virtual imaging for teaching cardiac embryology. Jean-Marc Schleich, Jean-Louis Dillenseger To cite this version: Jean-Marc Schleich, Jean-Louis Dillenseger. Virtual imaging for teaching cardiac embryology..
Virtual imaging for teaching cardiac embryology. Jean-Marc Schleich, Jean-Louis Dillenseger To cite this version: Jean-Marc Schleich, Jean-Louis Dillenseger. Virtual imaging for teaching cardiac embryology..
Guide to Gastroenterology Biological Therapeutic Drug Monitoring Pathway (TDM)
") Guide to Gastroenterology Biological Therapeutic Drug Monitoring Pathway (TDM) Author: Responsible Lead Consultants: Endorsing Body: Implementation Date: 01/08/2018 Version Number: 1.0 Review Date: 01/08/2020
Guide to Gastroenterology Biological Therapeutic Drug Monitoring Pathway (TDM) Author: Responsible Lead Consultants: Endorsing Body: Implementation Date: 01/08/2018 Version Number: 1.0 Review Date: 01/08/2020
DENOMINATOR: All patients aged 18 and older with a diagnosis of inflammatory bowel disease
 Measure #270: Inflammatory Bowel Disease (IBD): Preventive Care: Corticosteroid Sparing Therapy National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Measure #270: Inflammatory Bowel Disease (IBD): Preventive Care: Corticosteroid Sparing Therapy National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Cx601 ADMIRE-CD Top-Line Results Webcast. 24 August 2015
 Cx601 ADMIRE-CD Top-Line Results Webcast 24 August 2015 1 Cx601 ADMIRE-CD Top-Line Results Webcast Speakers Mr Eduardo Bravo, Chief Executive Officer Dr Julián Panés, Head of Gastroenterology Department,
Cx601 ADMIRE-CD Top-Line Results Webcast 24 August 2015 1 Cx601 ADMIRE-CD Top-Line Results Webcast Speakers Mr Eduardo Bravo, Chief Executive Officer Dr Julián Panés, Head of Gastroenterology Department,
Clinical Policy: Natalizumab (Tysabri) Reference Number: ERX.SPA.162 Effective Date:
 Reference Number: ERX.SPA.162 Effective Date:") Clinical Policy: (Tysabri) Reference Number: ERX.SPA.162 Effective Date: 10.01.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Tysabri) Reference Number: ERX.SPA.162 Effective Date: 10.01.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
11/13/11. Biologics for CD and CUC: The Impact on Surgical Outcomes. Principles of Successful Intestinal Surgery
 Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Biologics for CD and CUC: The Impact on Surgical Outcomes Robert R. Cima, M.D., M.A. Associate Professor of Surgery Division of Colon and Rectal Surgery Overview Antibody based medications (biologics)
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab.
 Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab. Dr Peter Irving Guy s and St Thomas Hospital, London King s College London Response to vedolizumab
Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab. Dr Peter Irving Guy s and St Thomas Hospital, London King s College London Response to vedolizumab
The evaluation and treatment of patients with Crohn s
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:395 399 PERSPECTIVE Do Not Assume Symptoms Indicate Failure of Anti Tumor Necrosis Factor Therapy in Crohn s Disease DAVID H. BRUINING* and WILLIAM J. SANDBORN
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:395 399 PERSPECTIVE Do Not Assume Symptoms Indicate Failure of Anti Tumor Necrosis Factor Therapy in Crohn s Disease DAVID H. BRUINING* and WILLIAM J. SANDBORN
Preventing post-operative recurrence
 Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
Oxford Inflammatory Bowel Disease MasterClass Preventing post-operative recurrence Dr Oliver Brain Oxford Disclosures Presented at IEE, Oxford 2013 AbbVie sponsored meeting Talk Outline Risk factors for
ORIGINAL ARTICLE. Abstract. Introduction
 ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 1-5 Effectiveness of adalimumab for ambulatory ulcerative colitis patients after failure of infliximab treatment: a first real-life experience in
ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 1-5 Effectiveness of adalimumab for ambulatory ulcerative colitis patients after failure of infliximab treatment: a first real-life experience in
How to use infliximab?
 How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD
 Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Practice Parameters for the management of perianal abscess and fistula-in-ano(1)
") New frontiers in Crohn s perianal fistulae disease Dr Nadine Harran Colorectal surgeon, WDGMC 1. Introduction 2. Seton 3. The OVESCO Proctology Clip 4. Collagen fistula plugs 5. Sealents 6. Mucosal advancement
New frontiers in Crohn s perianal fistulae disease Dr Nadine Harran Colorectal surgeon, WDGMC 1. Introduction 2. Seton 3. The OVESCO Proctology Clip 4. Collagen fistula plugs 5. Sealents 6. Mucosal advancement
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Clinical Policy: Vedolizumab (Entyvio) Reference Number: CP.PHAR.265
 Reference Number: CP.PHAR.265") Clinical Policy: (Entyvio) Reference Number: CP.PHAR.265 Effective Date: 07/16 Last Review Date: 07/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: (Entyvio) Reference Number: CP.PHAR.265 Effective Date: 07/16 Last Review Date: 07/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Impact of endoscopic monitoring in postoperative Crohn s disease patients already receiving pharmacological prevention of recurrence
 1130-0108/2015/107/10/586-590 Revista Española de Enfermedades Digestivas Copyright 2015 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 107, N.º 10, pp. 586-590, 2015 ORIGINAL PAPERS Impact of endoscopic
1130-0108/2015/107/10/586-590 Revista Española de Enfermedades Digestivas Copyright 2015 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 107, N.º 10, pp. 586-590, 2015 ORIGINAL PAPERS Impact of endoscopic
5/2/2018 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD
 5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
5/2/218 SHOULD DEEP REMISSION BE A TREATMENT GOAL? YES! Disclosures: R. Balfour Sartor, MD Grant support for preclinical studies: Janssen, Gusto Global, Vedanta, Artizan BALFOUR SARTOR, MD DISTINGUISHED
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Bowel Damage as Assessed by the Lémann Index is Reversible on Anti-TNF Therapy for Crohn s Disease
 Journal of Crohn's and Colitis, 215, 633 639 doi:1.193/ecco-jcc/jjv8 Advanced Access publication May 9, 215 Original Article Original Article Bowel Damage as Assessed by the Lémann Index is Reversible
Journal of Crohn's and Colitis, 215, 633 639 doi:1.193/ecco-jcc/jjv8 Advanced Access publication May 9, 215 Original Article Original Article Bowel Damage as Assessed by the Lémann Index is Reversible
IBD Biologicals and Novel therapeutic regimes. Dr S K Sinha Additional Professor Department of Gastroenterology PGIMER, Chandigarh
 IBD Biologicals and Novel therapeutic regimes Dr S K Sinha Additional Professor Department of Gastroenterology PGIMER, Chandigarh 1 Treatment aims in IBD Traditional treatment goals of IBD Control of symptoms?improvement
IBD Biologicals and Novel therapeutic regimes Dr S K Sinha Additional Professor Department of Gastroenterology PGIMER, Chandigarh 1 Treatment aims in IBD Traditional treatment goals of IBD Control of symptoms?improvement
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY?
 WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Submitted by xxxxxxxxxxxxxxxxx, xxxxxxxxx RCP and co-ordinated by xxxxxxxxxxxx, xxxxxxxxxxxxxxxxxxxxxxxxxxxxx, Royal Liverpool University Hospital.
 Royal College of Physicians statement on the appraisal of use of tumour necrosis factor alpha (TNF-α) inhibitors (adalimumab, certolizumab pegol and infliximab) and natalizumab for Crohn's disease Submitted
Royal College of Physicians statement on the appraisal of use of tumour necrosis factor alpha (TNF-α) inhibitors (adalimumab, certolizumab pegol and infliximab) and natalizumab for Crohn's disease Submitted
Clinical Policy: Vedolizumab (Entyvio) Reference Number: CP.PHAR.265 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.265 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Entyvio) Reference Number: CP.PHAR.265 Effective Date: 07.16 Last Review Date: 11.18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this
Clinical Policy: (Entyvio) Reference Number: CP.PHAR.265 Effective Date: 07.16 Last Review Date: 11.18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D.
 Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Crohn s disease is a chronic, progressive, destructive
 Mini-Reviews and Perspectives Current Directions in IBD Therapy: What Goals Are Feasible With Biological Modifiers? WILLIAM J. SANDBORN Inflammatory Bowel Disease Clinic, Division of Gastroenterology and
Mini-Reviews and Perspectives Current Directions in IBD Therapy: What Goals Are Feasible With Biological Modifiers? WILLIAM J. SANDBORN Inflammatory Bowel Disease Clinic, Division of Gastroenterology and
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
From universal postoperative pain recommendations to procedure-specific pain management
 From universal postoperative pain recommendations to procedure-specific pain management Hélène Beloeil, Francis Bonnet To cite this version: Hélène Beloeil, Francis Bonnet. From universal postoperative
From universal postoperative pain recommendations to procedure-specific pain management Hélène Beloeil, Francis Bonnet To cite this version: Hélène Beloeil, Francis Bonnet. From universal postoperative