Perianal Fistula of Crohn s Disease
|
|
|
- Simon Shields
- 5 years ago
- Views:
Transcription
1 Case 3
2 Perianal Fistula of Crohn s Disease
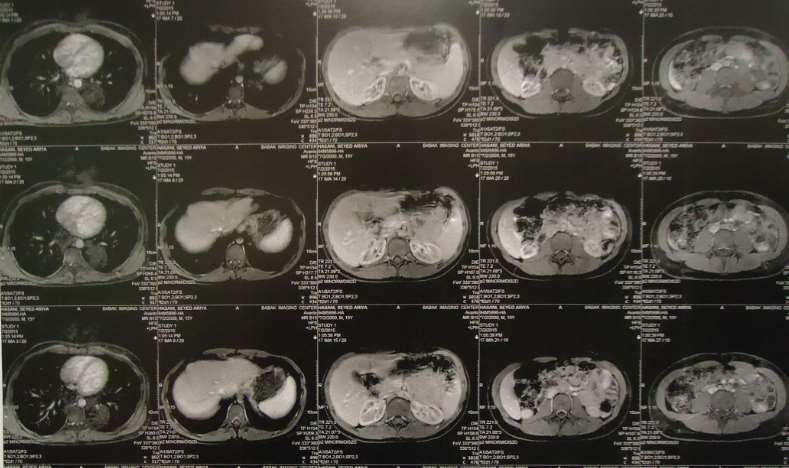
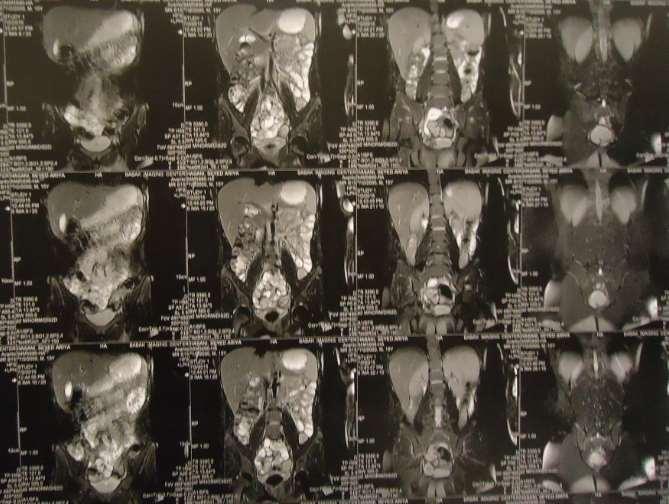
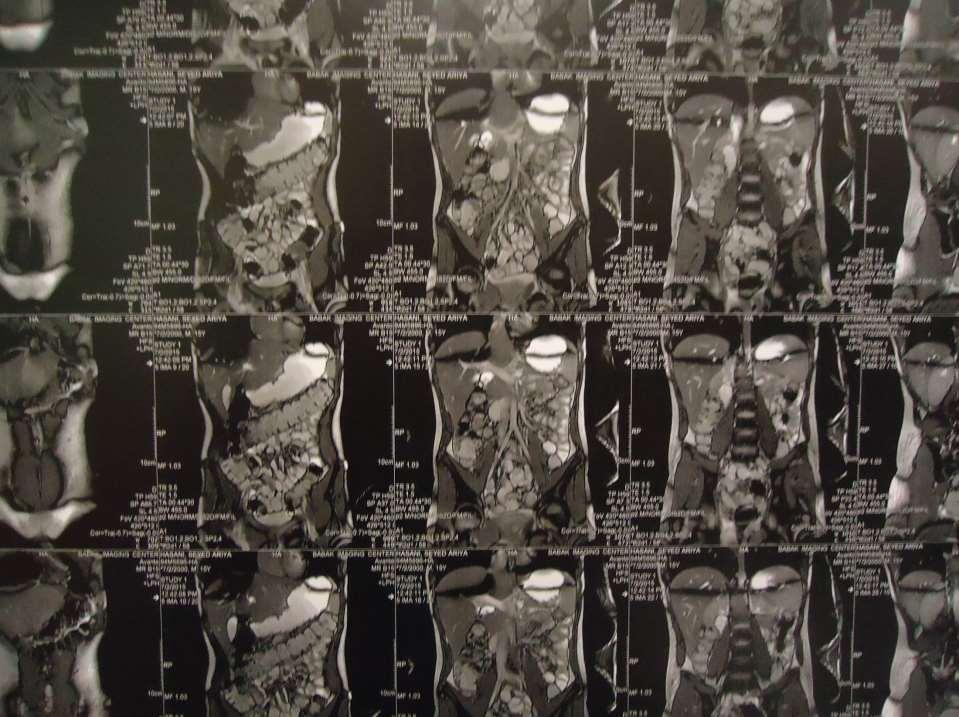
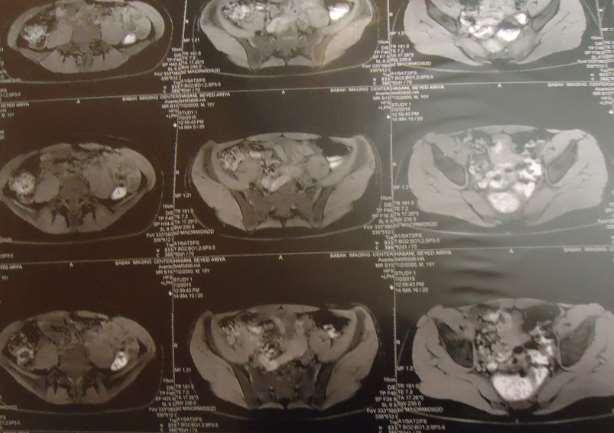
3 A 16 year-old boy referred by surgeon due to perianal fistula since 6mo ago CC=perianal pain History of intermittent non-bloody diarrhea and mild abdominal pain and 2-3kg weight loss and without history of fever or chills Ph/E=normal RE=8x3cm perianal lesion
4
5
6

7

8
9
10
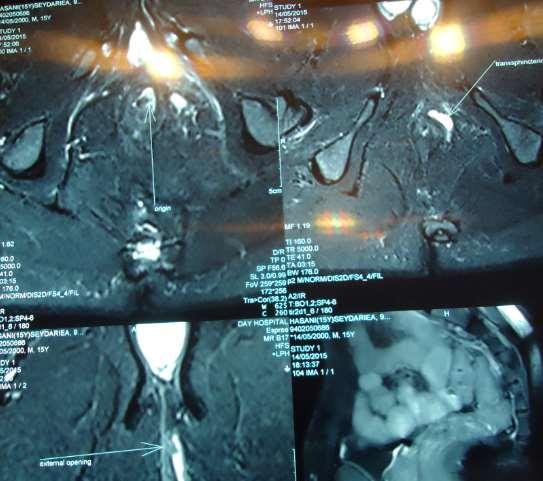
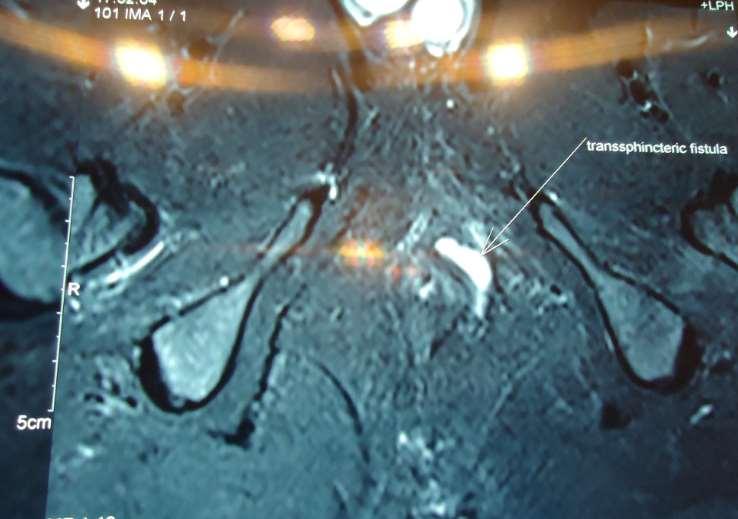
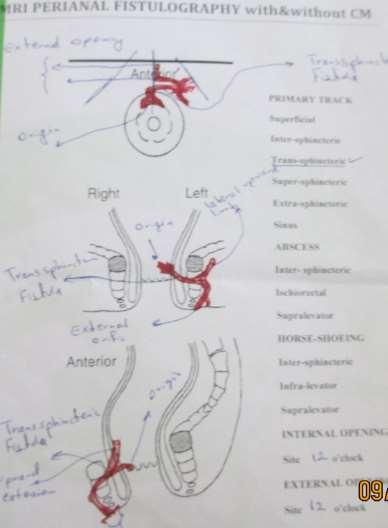
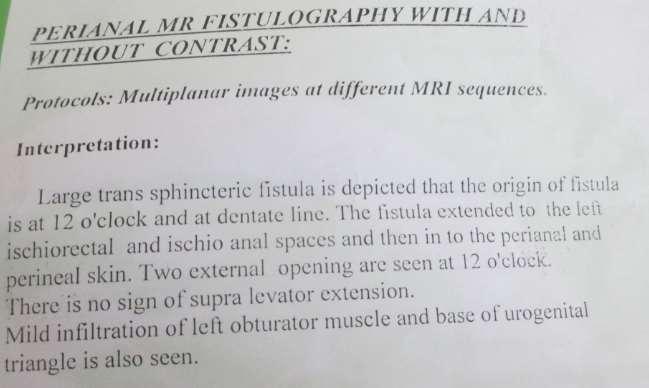
11 Transsphincteric Fistula
12
13 Lab data Hb=13.5, MCV=76, plt=345000, ESR=45 CRP=60 LFT=Nl, FBS, Cr, TG, Chol=nl S/E *3=Nl Stool calprotectin=565
14
15
16

17
18
19
20 What is your plan?

21
22
23

24
25

26 What is your plan?
27
 3. Identify or exclude local sepsis (abscess) 4.")
28 The main aspects in planning a strategy for the management of CD fistulae are 1. Locate the origin of the fistula and its anatomy 2. Evaluate the originating intestinal loop (inflammation or stenosis) 3. Identify or exclude local sepsis (abscess) 4. Determine which organs are affected and their contribution to systemic symptoms or impairment of the quality of life 5. Assess the nutritional status of the patient.
29 Initial diagnostic approach Pelvic MRI should be the initial procedure because it is accurate and non-invasive, although it is not needed routinely in simple fistulae

30 Evaluation - Imaging Fistulography CT U/S MRI <25% accuracy abscess assess sphincters 86% concordance with operative findings for presence of 1o track, 2o extensions and abscess, 97% for horseshoeing

31 Initial diagnostic approach Examination under anaesthetic is considered the gold standard only in the hands of an experienced surgeon. It may allow concomitant surgery obtain appropriate Informed consent of the patient, since unexpected findings may preclude this
32

33 Initial diagnostic approach Anorectal ultrasound requires expertise, but can be equivalent to pelvic MRI in completing examination under anaesthesia if rectal stenosis has been excluded. Fistulography is not recommended
34 . A prospective, blinded study found high accuracy in diagnosis individually for MRI, EUS and examination under anesthesia. When either of the imaging modalities was combined with examination under anesthesia, the accuracy was 100% and was the most cost effective approach.
35

36 Initial diagnostic approach Concomitant rectosigmoid inflammation has prognostic and therapeutic relevance therefor: proctosigmoidoscopy should be used routinely in the initial evaluation
37 About 20% of patients with Crohn s disease will develop perianal fistulas within 10 years of diagnosis..
38

39

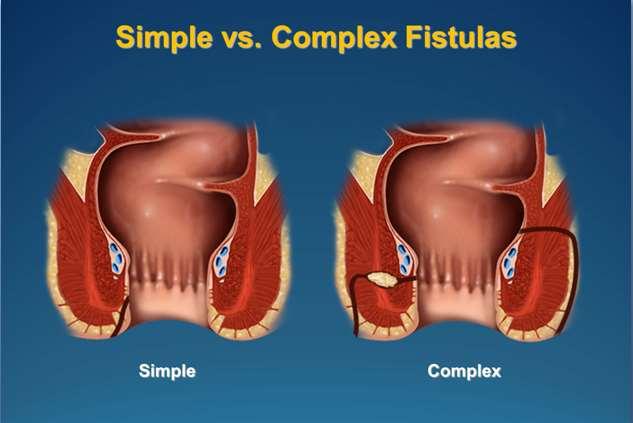
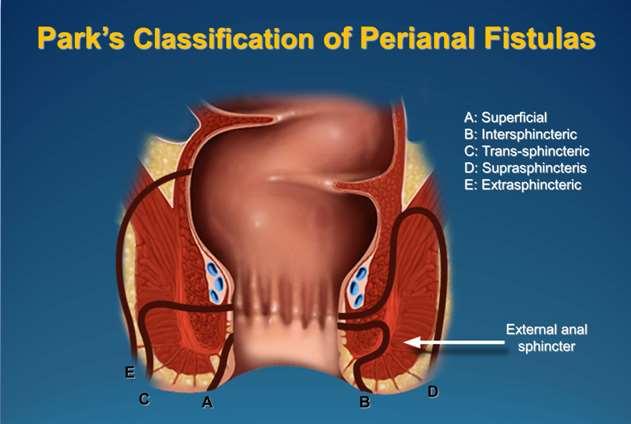
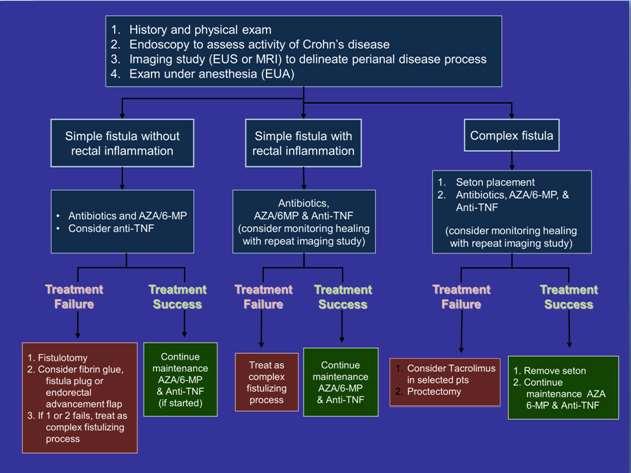
40 Classification of perianal fistulae There is no consensus for classifying perianal fistulae in CD. In clinical practice most experts use a classification of simple or complex. From the surgical point of view Parks' classification is more descriptive and can influence surgical decisions, but it is complicated to use in routine practice
41 A simple fistula is superficial or begins low in the rectal canal, has a single opening on the skin, is not associated with an abscess, and does not communicate with other organs
42 In contrast, a complex fistula begins high in the anal canal, is associated with an abscess, has multiple skin openings, connects with adjacent structures or is associated with inflammation of the colonic mucosa.
43
44
45
46 . A prospective, blinded study found high accuracy in diagnosis individually for MRI, EUS and examination under anesthesia. When either of the imaging modalities was combined with examination under anesthesia, the accuracy was 100% and was the most cost effective approach.
47
48
49
50
51
52
53

54
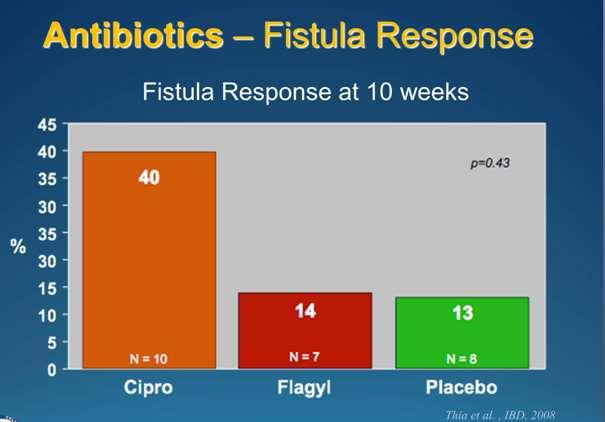
55 WCOG Statement on Medical Treatment Aminosalicylates, corticosteroids, antibiotics There is no demonstrable role for corticosteroids or aminosalicylates in perianal Crohn s disease Grade of Recommendation: 1C Antibiotics, namely metronidazole and ciprofloxacin improve symptoms and may contribute to healing. Therefore, antibiotics are only recommended as adjunctive treatments for fistulas. Grade of Recommendation: 1C and 2C. Gecse et al., Gut 2014
56
57
58
59
60
61
62
63
64
65 Vedolizumab for Crohn s Disease Fistulae Characteristic VDZ/PBO (n=153) VDZ Q8W (n=154) VDZ Q4W (n=154) With concomitant glucocorticoids, n (%) 56 (37) 59 (38) 58 (38) With concomitant immunosuppressants, n (%) 23 (15) 27 (18) 31 (20) With glucocorticoid and immunosuppressive, n (%) 26 (17) 23 (15) 22 (14) No glucocorticoid or immunosuppressive, n (%) 48 (31) 45 (29) 43 (28) Median prednisone equivalent dose, mg (interquartile range) 20.0 (12.5,30.0) 20.0 (15.0,30.0) 20 (15.0,30.0) With prior anti-tnfα use, n (%) 82 (54) 88 (57) 83 (54) With prior anti-tnfα failure, n (%) 1 TNFα antagonist 78 (51) 82 (55) 77 (50) Inadequate response 35 (45) 37 (45) 31 (40) Loss of response 29 (37) 35 (43) 33 (43) Intolerance 14 (18) 10 (12) 13 (17) 2 TNFα antagonists 53 (35) 46 (30) 49 (32) Prior surgery for CD, n (%) 57 (37) 57 (37) 61 (40) History of fistulizing disease, n (%) 57 (37) 47 (31) 49 (32) Draining fistulae at baseline, n (%) 18 (12) 17 (11) 22 (14) GEMINI 35 II MAINTENANCE Sandborn WJ et al. N Engl J Med. 2013
66
67
68
69
70
71
72 REMAINING QUESTIONS - When to remove the Seton? - When to repeat imaging? - When to stop concomitant antibiotics? - When to consider definitive surgery? - When can you stop medical therapy
73
74
75 Parks Anal Fistula Classification Intersphincteric 45%-70% Transsphincteric 23-30% Suprasphincteric 5-20% Extrasphincteric 2-5% Horseshoe extension 8.8%
76
77
78
79
80 Intersphincteric Fistula
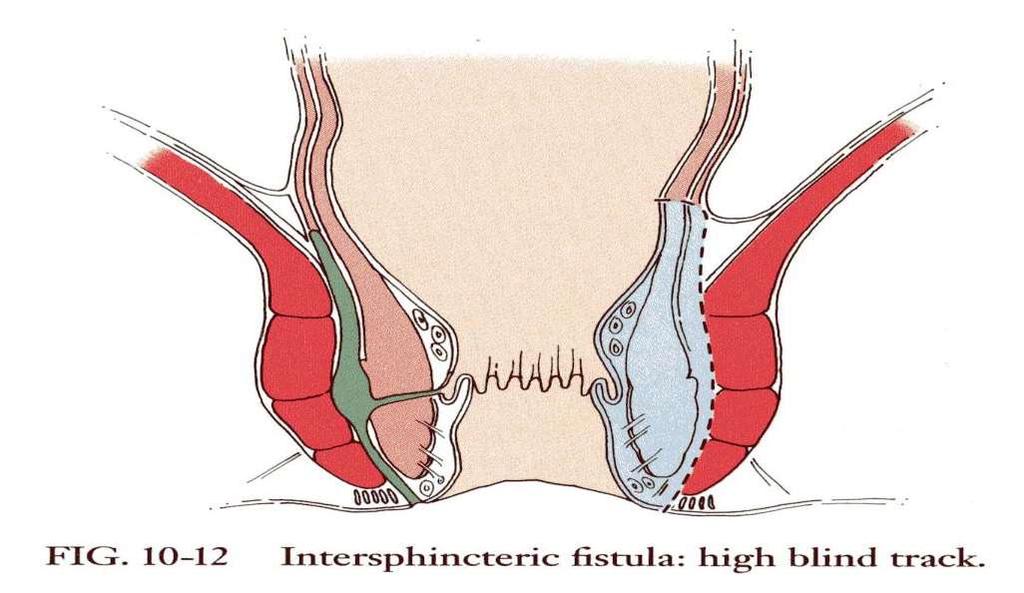
81 Intersphincteric Fistula
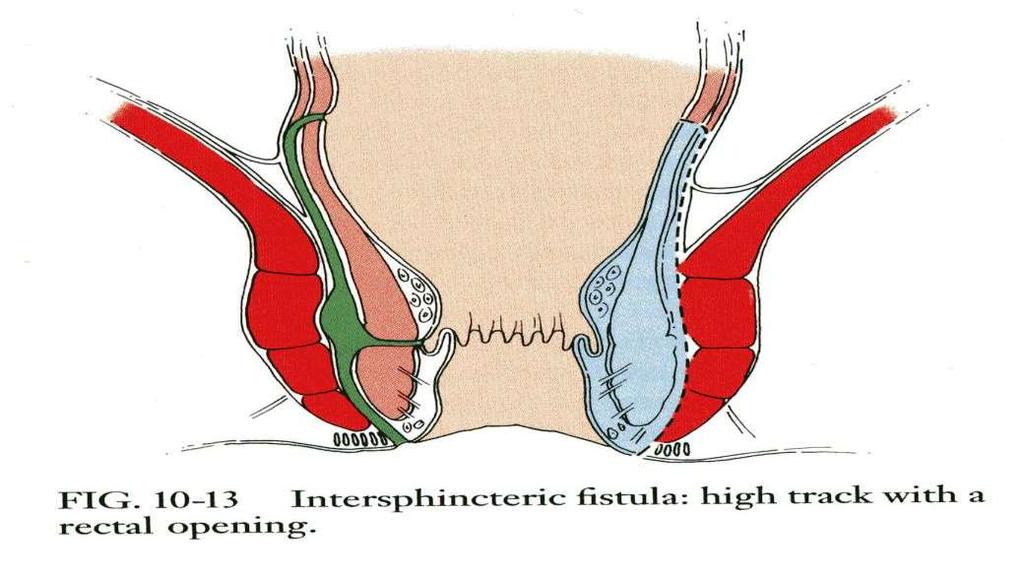
82 Intersphincteric Fistula
83 Intersphincteric Fistula
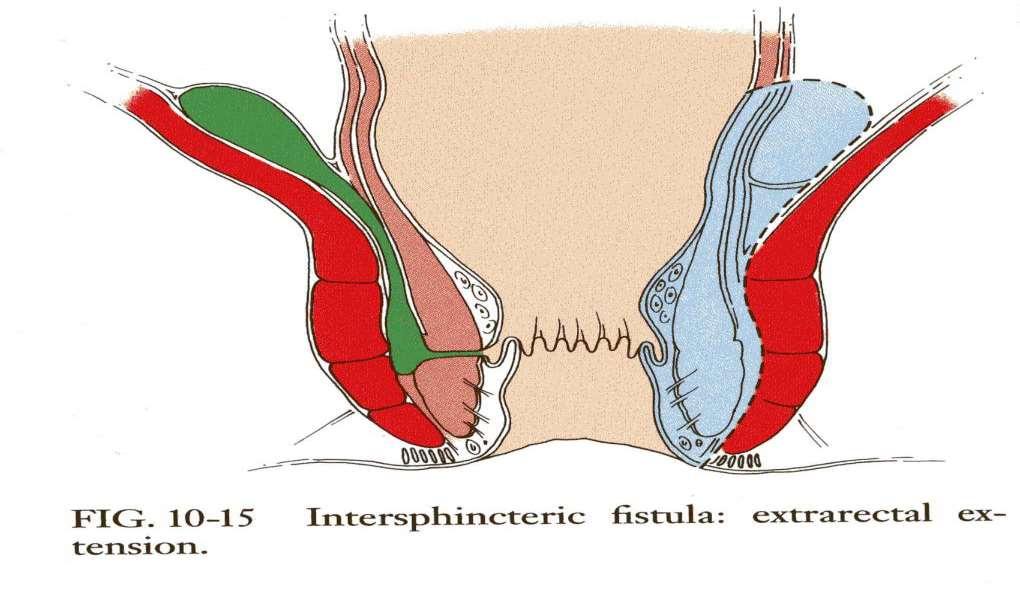
84 Intersphincteric Fistula
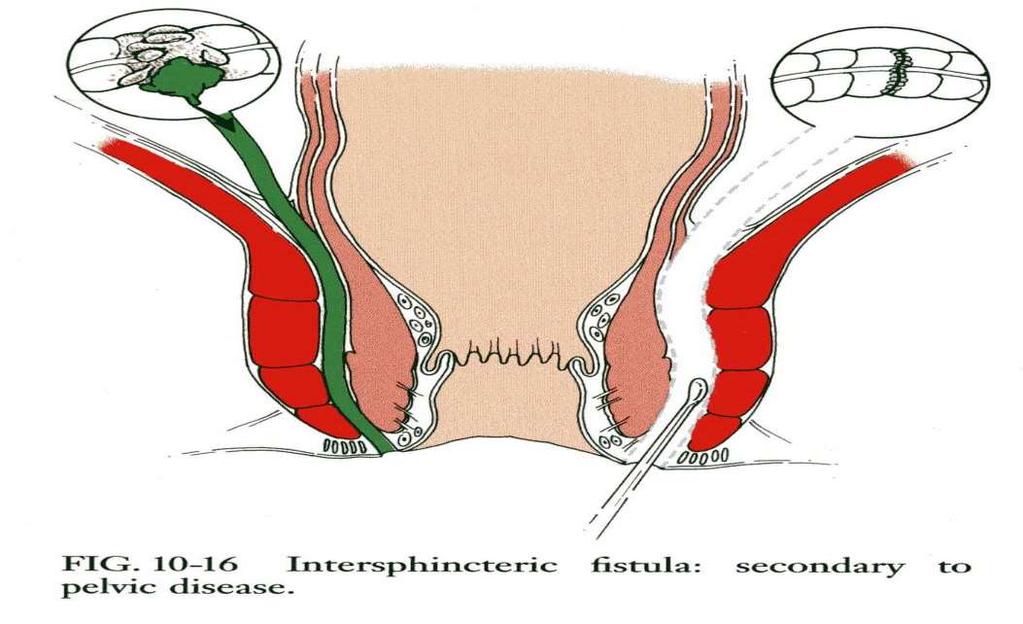
85 Intersphincteric Fistula
86 Extrasphincteric Fistula
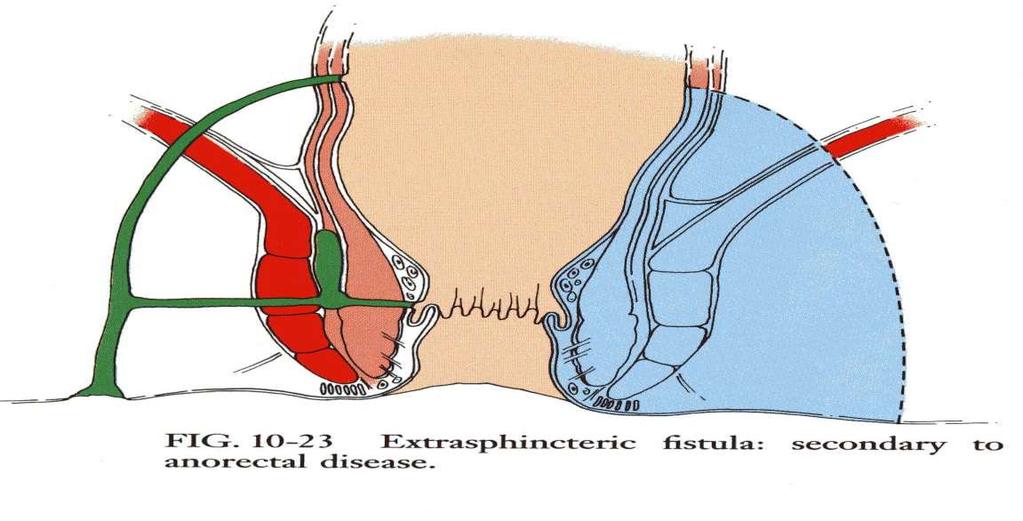
87 Extrasphincteric Fistula
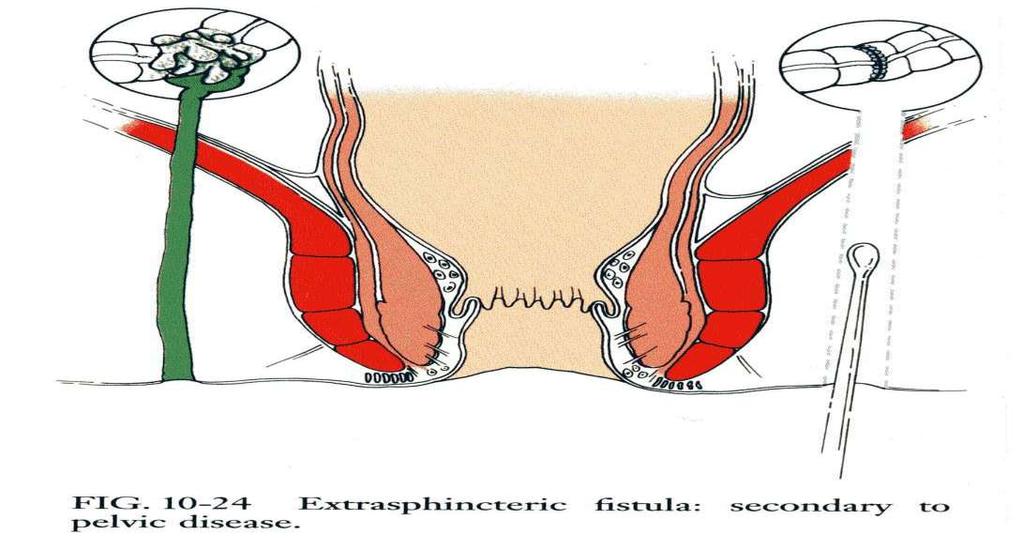
88 Extrasphincteric Fistula

89 Extrasphincteric Fistula
90 Suprasphincteric Fistula
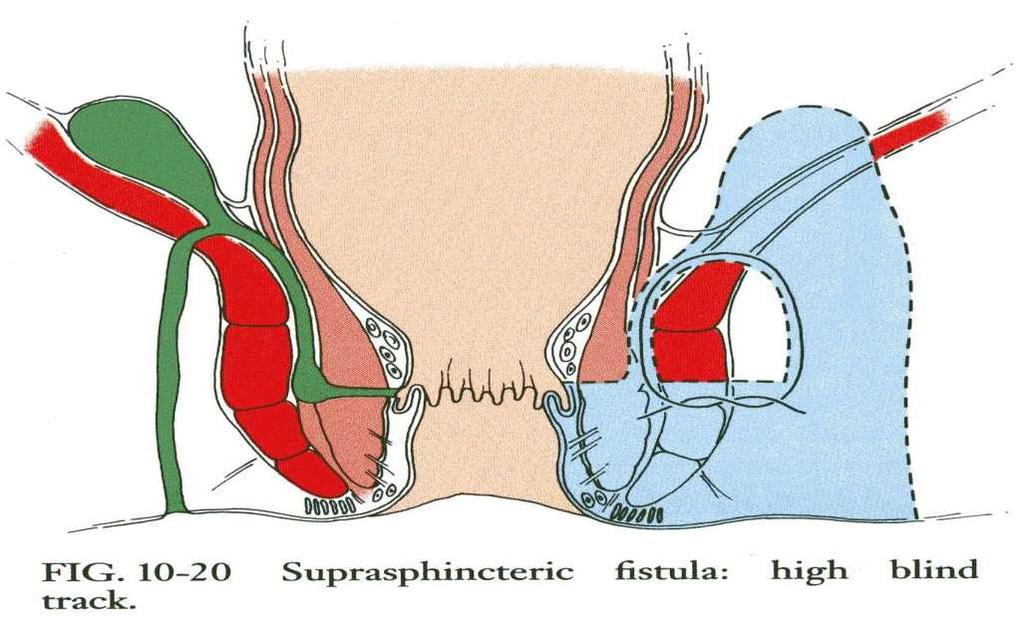
91 Suprasphincteric Fistula
92 Transsphincteric Fistula
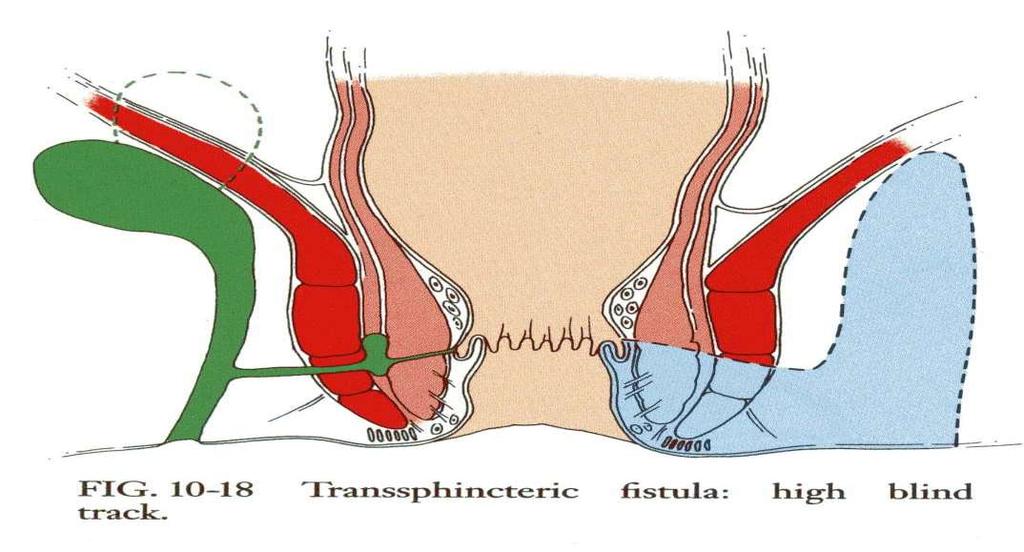
93 Transsphincteric Fistula
94 Evaluation Digital assessment (<85% accurate) H2O2 (97% accuracy) Dyes Goodsall s rule (59% accuracy) Anterior external opening radial track Posterior external opening posterior midline Exception long anterior
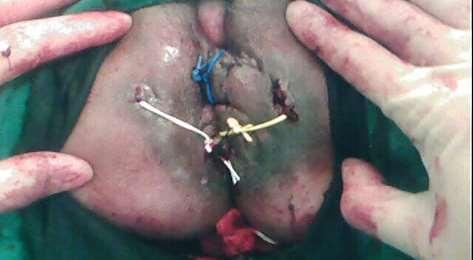
95 Anal Fistula - Management Fistulotomy +/- marsupialisation Fistulectomy open vs core Seton insertion Loose/Draining seton Tight/Cutting seton Chemical seton Rectal Advancement Flap Fibrin Glue

96

97

98

99

100

101

102

103

104
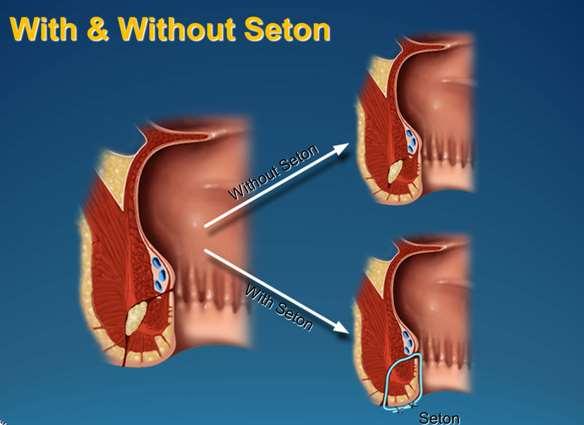
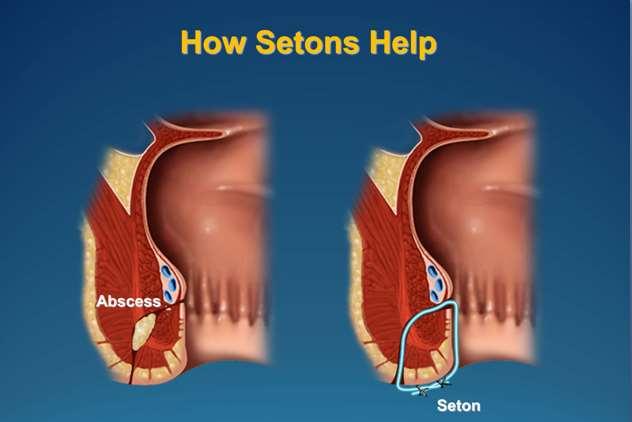
105 Setons Potential actions of the seton Act as a drain for acute sepsis To allow resolution of inflammation prior to definitive fistula surgery Role in staged fistulotomy Delineation of the amount of muscle caudal to the fistulous track Cutting & Chemical setons: Controlled division of the enclosed sphincter mechanism with minimal separation of the transected ends.
106 Benefits: Fibrin Glue Sphincter apparatus not disturbed No significant scarring from the treatment Technique EUA; identification of primary and any secondary tract openings. Fistula tract then curetted Fibrin adhesive injected into the secondary tract opening until seen coming from the primary opening. Vaseline gauze applied over the openings
107 Study Results: Fibrin Glue Lindsay I; Dis Colon & Rectum % healed at in the short term (8/12 follow up) Probably little advantage over conventional Rx but may be useful first line treatment for higher fistulas Cintron JR; Dis Colon & Rectum Jul % fistula closure at 12 months with autologous fibrin 64% fistula closure at 12 months with commercial fibrin sealant. Most treatment failures occurred within 3 months

108 Surgical procedures for perianal Crohn's disease Fistulectomy and fistulotomy should be performed very selectively, because of the risk of incontinence. A diverting stoma or proctectomy may be necessary for severe disease refractory to medical therapy

109 Uncontrolled evidence suggests that local injection of infliximab close to the fistula track may be beneficial in patients not responding to or intolerant of intravenous infliximab
110 Summary for Successful Management of Anal Fistula 1. Definition of the anatomy. 2. Surgical drainage of abscess and tracks. 3. Eradication of anal gland origin. 4. Preservation of sphincter function.
 during IFX therapy may improve long-term healing rates")
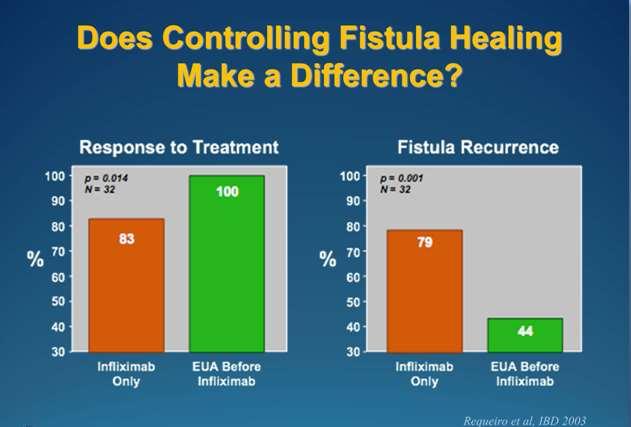
111 combination of seton placement and IFX is superior to either strategy alone, probably because of better drainage of abscesses and fistulae. This combination gives better response,longer effect duration and lower recurrence rate. Moreover, reparative surgery (e.g. mucosal flap or fistula plug) during IFX therapy may improve long-term healing rates
 should be used.")
112 Monitoring the therapeutic response Clinical assessment (decreased drainage) is usually sufficient. To quantify treatment efficacy the Perianal Crohn's Disease Activity Index (PCDAI) should be used. In the setting of clinical trials,mri in combination with clinical assessment is now considered mandatory

113 Continuing therapy for perianal Crohn's disease Azathioprine/6-mercaptopurine,infliximab or adalimumab or seton drainage, or a combination of drainage and medical therapy should be used as maintenance therapy. All mainte-nance therapies should be used for at least one year

114 There are no data on the effect of AZA/MP as maintenance therapy for fistulae after induction with IFX, or during IFX maintenance therapy

115 Therapeutic approach in the event of infliximab failure In the event of anti-tnf failure, the use of azathioprine/mercaptopurine or methotrexate,with antibiotics as adjunctive treatment, is the first therapeutic choice Depending on the severity of the disease, a diverting ostomy can be performed and can rapidly restore quality of life, proctectomy is the last resort
 with rectovaginal fistulae in the ACCENT II trial, IFX was only modestly effective (45% closure at week 14).")
116 Enterocutaneous fistulae There are no randomised-controlled trials on the effect of medical treatment for non-perianal fistulating CD. For the 25 patients (out of 282) with rectovaginal fistulae in the ACCENT II trial, IFX was only modestly effective (45% closure at week 14). The management is a complex,multidisciplinary challenge, and referral to a specialist centre is recommended. Early re-operation to close a fistulous track, is often associated with recurrence or further complications. the nutritional state should be optimised.

117

118

119

120

121
122

123

124
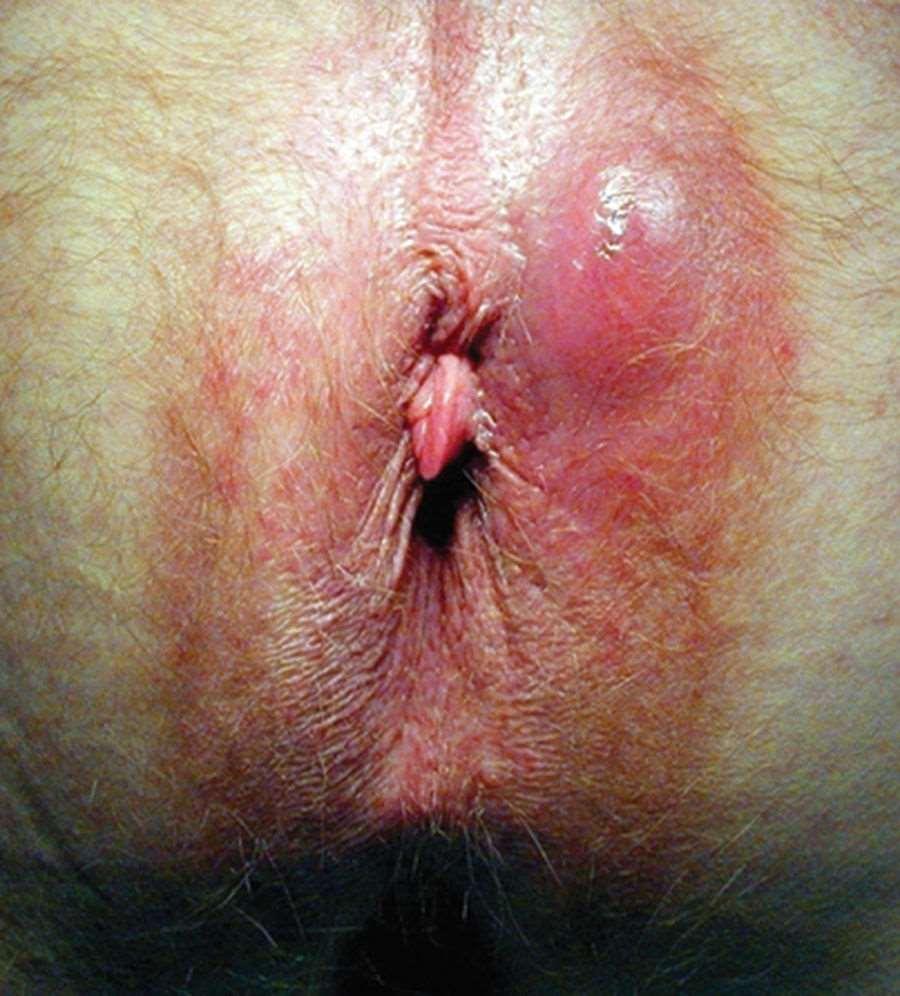
125 question A 30-year-old female with a 5 year history of Crohn s disease comes to you for evaluation of a 3 week history of perianal pain and drainage. On physical exam you find the following [see figure].

126
127 Which one of the following is an appropriate treatment option for this patient? A Prednisone B Oral 5-ASA treatment C Infliximab D Budesonide
128 C is correct Explanation The only agent that has been shown to have activity for Crohn s perianal fistulae is infliximab. In particular, prednisone in this setting has been associated with increased chances of abscess formation and complications associated with treatment.
129 question Which one of the following is an effective treatment option for a patient with Crohn's disease who has active proctitis and a draining perianal fistula? A EUA with fistulotomy B Prednisone C EUA with placement of a cutting seton D EUA with placement of a draining /non-cutting seton
130 D is correct Explanation Patients with active proctitis are at increased risk of poor outcomes with aggressive surgical intervention. EUA with fistulotomy and EUA with cutting seton placement are both associated with non-healing wounds and incontinence in the setting of active proctitis.
131 Prednisone is not effective for fistulizing disease and may increase the risk of abscess. The placement of a draining or non-cutting seton helps control healing and reduces the risk of sphincter injury in this setting.
132 QUESTION A 19-year-old man presents with 2 months of gradually worsening diarrhea, urgency, fatigue, and right lower quadrant abdominal pain. He has perirectal discomfort. He has lost 15 pounds. Examination reveals mild abdominal tenderness and a simple perianal fistula draining a small amount of purulent material.
133 He has moderate microcytic anemic, and his serum C-reactive protein concentration is elevated at 25 mg/l (normal < 8 mg/l). Colonoscopy reveals the following findings in the terminal ileum as far as intubated (15 cm) [FIGURE].

134
135 Biopsies reveal moderately active chronic ileitis. The colon is endoscopically normal. He is interested in pursuing the therapy with the highest chance of achieving success (steroid-free remission without surgery).
136 Which of the following do you recommend? A Controlled ileal release budesonide 9 mg by mouth daily, with a taper over 3-4 months B Azathioprine 2.5 mg/kg body weight by mouth daily C Prednisone 60 mg by mouth daily, with a taper over 2-3 months D Mesalamine 2,000 mg by mouth twice daily E Infliximab 5 mg/kg body weight infusions (induction and maintenance dose) along with azathioprine, mg/kg body weight daily
137 Answer: E Explanation This patient is at high risk for progression to intestinal complications or surgery. He has young age at diagnosis, male gender, small bowel involvement (as opposed to pure colonic involvement which has a milder clinical course) and perianal disease at diagnosis.
138 All of these factors have been implicated in various natural history models of Crohn s disease as being associated with progression to disabling Crohn s disease, stricturing and/or penetrating complications, or bowel resection. While budesonide and prednisone are reasonable drugs for induction of remission, they are not indicated as maintenance therapy.
139 Mesalamine is not effective for induction or maintenance therapy in Crohn s disease. The SONIC trial showed that the combination of infliximab and azathioprine resulted in higher rates of steroid-free remission than infliximab monotherapy or azathioprine monotherapy.
140 QUESTION A 60-year-old man with a 6-year history of Crohn's disease involving the ileum and left colon presents with new onset of perianal pain for the last week. He has previously been well-controlled on 1.5 mg/kg/day of 6-mercaptopurine, and denies any increase in stool or abdominal pain recently.
141 On physical exam, he is afebrile and his abdomen is soft and non-tender. His rectal exam is significant for extreme tenderness and a large fluctuant mass [FIGURE].
142
143 What is the appropriate next step in his management? A Begin prednisone 40 mg a day B Refer him immediately to a colorectal surgeon for an incision and drainage procedure C Start anti-tnf antibody treatment D Image perianal process with pelvic MRI or rectal EUS
144 Answer: D Explanation is recommended that patients with either a suspected abscess, failing medical therapy, or who are being referred to surgery, undergo imaging with EUS or MRI.
145 Similarly, the ECCO guidelines for the management of Crohn's disease recommended imaging with MRI or EUS for all patients with fistulas. This patient has a large fluctuant mass suggestive of an abscess so should have either an MRI or EUS performed according to both guidelines.

146
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions. Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic
 Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Perianal and Fistulizing Crohn s Disease: Tough Management Decisions Jean-Paul Achkar, M.D. Kenneth Rainin Chair for IBD Research Cleveland Clinic Talk Overview Background Assessment and Classification
Fistulizing Crohn s Disease: The Aggressive Approach
 Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Fistulizing Crohn s Disease: The Aggressive Approach Bruce E. Sands, MD, MS MGH Crohn s and Colitis Center and Gastrointestinal Unit Massachusetts General Hospital Boston, USA Case Presentation: Summary
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions
: Future Directions") Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Modern Management of Perianal Fistulas in Crohn s Disease (PFCD): Future Directions Rami Ismail, Pharm.D., BCPS, BCCCP, CACP Lead Clinical staff Pharmacist, Cleveland Clinic Abu Dhabi Disclosure Information
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Sunanda Kane, MD, FACG Professor of Medicine Department of Gastroenterology and Hepatology Mayo Clinic Rochester, MN In my lecture today, I will be
Crohn's Disease The What, When, and Why of Treatment Sunanda Kane, MD, FACG Professor of Medicine Department of Gastroenterology and Hepatology Mayo Clinic Rochester, MN In my lecture today, I will be
Percent Cumulative. Probability. Penetrating. Inflammatory. Stricturing. Months Patients at risk N =
 Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Fistulizing Crohn s Disease Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology & Hepatology Mayo Clinic Rochester, Minnesota, USA Outline Fistulizing Crohn s Etiology Incidence
Epidemiology / Morbidity
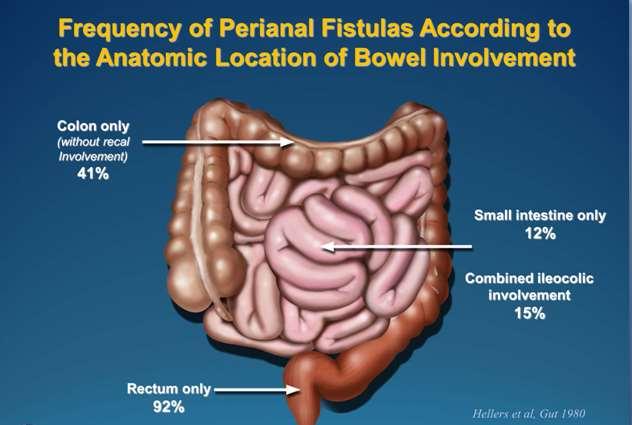
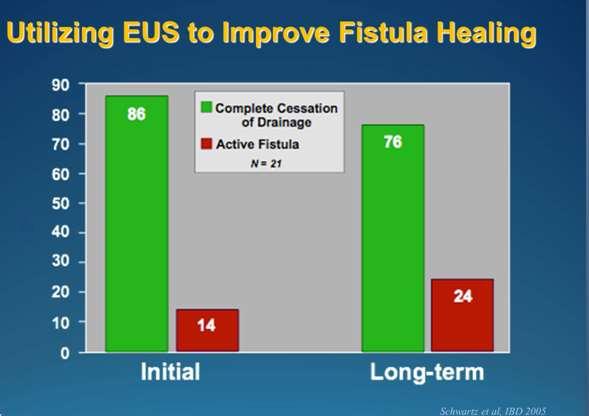
 Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Perianal Crohn s Disease: Current Treatment Approach David A Schwartz, MD Director, Inflammatory Bowel Disease Center Vanderbilt University Medical Center Epidemiology / Morbidity Hellers et al, Gut 1980
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Treatment of Inflammatory Bowel Disease. Michael Weiss MD, FACG
 Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Treatment of Inflammatory Bowel Disease Michael Weiss MD, FACG What is IBD? IBD is an immune-mediated chronic intestinal disorder, characterized by chronic or relapsing inflammation within the GI tract.
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy
 Dipartimento di Scienze Mediche e Chirurgiche Istituto di Clinica Chirurgica Prof. Aroldo Fianchini Ancona INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy Cristina Marmorale PERIANAL
Dipartimento di Scienze Mediche e Chirurgiche Istituto di Clinica Chirurgica Prof. Aroldo Fianchini Ancona INNOVATIONS IN TREATMENT OF PERIANAL CROHN DISEASE combined therapy Cristina Marmorale PERIANAL
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Surgical Management of IBD in the Age of Biologics
 Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Surgical Management of IBD in the Age of Biologics Lisa S. Poritz, M.D Associate Professor of Surgery Division of Colon and Rectal Surgery Objectives Discuss surgical management of IBD When to operate
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Crohn's disease CAUSES COURSE OF CROHN'S DISEASE TREATMENT. Sulfasalazine
 Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
Crohn's disease Crohn's disease is an inflammatory condition of the digestive tract that affects children and adults. Common features of Crohn's disease include mouth sores, diarrhea, abdominal pain, weight
, may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely,
 ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
ANORECTAL ABSCESSES , may spread caudally to present as a perianal abscess, laterally across the external sphincter to form an ischiorectal abscess or, rarely, superiorly above the anorectal junction
INFLAMMATORY BOWEL DISEASE
 1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
1. Medical Condition INFLAMMATORY BOWEL DISEASE (IBD) specifically includes Crohn s disease (CD) and ulcerative colitis (UC) but also includes IBD unclassified (IBDu), seen in about 10% of cases. These
What is Crohn's disease?
 What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
What is Crohn's disease? Crohn's disease is a chronic inflammatory disorder that causes inflammation of the digestive tract. It can affect any area of the GI tract, from the mouth to the anus, but it most
The Best of IBD at UEGW (Crohn s)
") The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
The Best of IBD at UEGW (Crohn s) Iyad Issa MD Head of Gastroenterology, Rafik Hariri Univ Hosp Adjunct Faculty, School of Medicine, Leb Univ Founding Faculty, School Of Medicine, Leb Am Univ 1 The Best
PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc. Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Konservative Behandlungsmöglichkeiten?
 PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Fisteln bei M. Crohn : Konservative Behandlungsmöglichkeiten? INTERDISZIPLINÄRE VISZERALE CHIRURGIE
PD Dr. med. R. Wiest / Dr. med. P. Juillerat, MSc Donnerstag 18 ten Oktober 2012 UPDATE PROKTOLOGIE: Fisteln bei M. Crohn : Konservative Behandlungsmöglichkeiten? INTERDISZIPLINÄRE VISZERALE CHIRURGIE
Special Authorization Drug Products with
 Effective August 1, 2008 Summary Special Authorization Drug Products with Changes to Criteria Special Authorization Drug Products with Changes to Criteria Alberta Blue Cross has been advised by Alberta
Effective August 1, 2008 Summary Special Authorization Drug Products with Changes to Criteria Special Authorization Drug Products with Changes to Criteria Alberta Blue Cross has been advised by Alberta
Surgical Management of IBD. Val Jefford Grand Rounds October 14, 2003
 Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Surgical Management of IBD Val Jefford Grand Rounds October 14, 2003 Introduction Important Features Clinical Presentation Evaluation Medical Treatment Surgical Treatment Cases Overview Introduction Two
Homayoon Akbari, MD, PhD
 Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Recent Advances in IBD Surgery Homayoon M. Akbari, MD, PhD, FRCS(C), FACS Associate Professor of Surgery Virginia Commonwealth University Crohn s disease first described as a surgical condition, with the
Surgery in Inflammatory Bowel Disease. Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh
 Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized
Surgery in Inflammatory Bowel Disease Rajesh Gupta MS, MCh Surgical Gastroenterology Division Dept of General Surgery PGIMER, Chandigarh 1 Ulcerative colitis (UC) Ulcerative colitis (UC) characterized
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: Feb. 14, 2018 Last Revised: April 1, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: Feb. 14, 2018 Last Revised: April 1, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Crohn s Disease. Resident Lecture 1/17/19
 Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Crohn s Disease Resident Lecture 1/17/19 Objectives Features/Classification of Crohn s Disease Medical Treatment Surgical Indications Surgical Considerations 2 Case 25 yo F presents to your office with
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Predicting the natural history of IBD. Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium
 Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
Predicting the natural history of IBD Séverine Vermeire, MD, PhD Department of Gastroenterology University Hospital Leuven Belgium Patient 1 Patient 2 Age 22 Frequent cramps and diarrhea for 6 months Weight
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
The second European evidence-based Consensus on the diagnosis and management of Crohn's disease: Special situations
 Journal of Crohn's and Colitis (2010) 4, 63 101 available at www.sciencedirect.com SPECIAL ARTICLE The second European evidence-based Consensus on the diagnosis and management of Crohn's disease: Special
Journal of Crohn's and Colitis (2010) 4, 63 101 available at www.sciencedirect.com SPECIAL ARTICLE The second European evidence-based Consensus on the diagnosis and management of Crohn's disease: Special
Corporate Presentation
 Corporate Presentation The treatment of perianal December fistula 2015in Crohn s disease patients Key Opinion Leader Event 8 th May 2017 Forward-Looking Statements This document does not constitute or
Corporate Presentation The treatment of perianal December fistula 2015in Crohn s disease patients Key Opinion Leader Event 8 th May 2017 Forward-Looking Statements This document does not constitute or
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: June 9, 2019* Last Revised: Feb. 12, 2019 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: June 9, 2019* Last Revised: Feb. 12, 2019 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Dr David Epstein Vincent Pallotti Hospital and University of Cape Town
 Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
Inflammatory Bowel Disease Management in South Africa in 2016 Pharmaceutical Care Management Association Dr David Epstein Vincent Pallotti Hospital and University of Cape Town Inflammatory Bowel Disease
New treatment options in UC. Rob Bryant IBD Consultant Royal Adelaide Hospital
 New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Research Article Temporary Fecal Diversion in the Management of Colorectal and Perianal Crohn s Disease
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 286315, 5 pages http://dx.doi.org/10.1155/2015/286315 Research Article Temporary Fecal Diversion in the Management
Pouchitis and Cuffitis A bloody mess. Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board
 Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Pouchitis and Cuffitis A bloody mess Sze-Lin Peng Colorectal Surgeon Counties Manukau District Health Board Ileal-pouch anal anastomosis https://www.pennmedicine.org/for-health-care-professionals/for-physicians/physician-education-and-resources/clinicalbriefings/2018/february/total-proctocolectomy-with-jpouch-reconstruction-for-ulcerative-colitis
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball
 Looking for the Crystal Ball") Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
I B D. etter than this. isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES
 I B D m etter than this isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES What types of people have learned how to manage their IBD? Athletes Musicians Firefighters DOCTORS HEROES Artists Presidents Actors
I B D m etter than this isease UNDERSTANDING INFLAMMATORY BOWEL DISEASES What types of people have learned how to manage their IBD? Athletes Musicians Firefighters DOCTORS HEROES Artists Presidents Actors
Index. Surg Clin N Am 87 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Surg Clin N Am 87 (2007) 787 796 Index Note: Page numbers of article titles are in boldface type. A Abscesses in anorectal Crohn s disease, 622 intra-abdominal, in Crohn s disease, 590 591 perirectal,
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Crohn's Disease. What causes Crohn s disease? What are the symptoms?
 Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Crohn's Disease Crohn s disease is an ongoing disorder that causes inflammation of the digestive tract, also referred to as the gastrointestinal (GI) tract. Crohn s disease can affect any area of the GI
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP)
") European Medicines Agency London, 22 February 2007 Doc. Ref. CPMP/EWP/2284/99 Rev. 1 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT GUIDELINE ON THE DEVELOPMENT OF NEW MEDICINAL PRODUCTS FOR
European Medicines Agency London, 22 February 2007 Doc. Ref. CPMP/EWP/2284/99 Rev. 1 COMMITTEE FOR MEDICINAL PRODUCTS FOR HUMAN USE (CHMP) DRAFT GUIDELINE ON THE DEVELOPMENT OF NEW MEDICINAL PRODUCTS FOR
Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152
 Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Crohn's disease: management Clinical guideline Published: 10 October 2012 nice.org.uk/guidance/cg152 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
A Comparitive Study of Laying Open of Wound Vs Primary Closure In Fistula in Ano
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 13, Issue 9 Ver. III (Sep. 214), PP 39-45 A Comparitive Study of Laying Open of Wound Vs Primary Closure
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 13, Issue 9 Ver. III (Sep. 214), PP 39-45 A Comparitive Study of Laying Open of Wound Vs Primary Closure
An Unusual Complication of Crohn s Disease. Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008
 An Unusual Complication of Crohn s Disease Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008 Case Presentation 70 year old lady k/c of Crohns disease h/o of Hartmann s procedure
An Unusual Complication of Crohn s Disease Dr Gerald Busuttil Mr Debono s Firm Surgical Grand Round 25 th November 2008 Case Presentation 70 year old lady k/c of Crohns disease h/o of Hartmann s procedure
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children
 Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Ileal Pouch Anal Anastomosis: The Preferred Method of Reconstruction after Proctocolectomy in Children Stephanie Jones, D.O. Surgical Fellow March 21, 2011 Ulcerative Colitis Spectrum of inflammatory bowel
Inflammatory Bowel Disease and Surgery: What You Should Know
 Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Inflammatory Bowel Disease and Surgery: What You Should Know Ask the Experts March 9, 2019 Kristen Blaker, MD Colon and Rectal Surgery MetroHealth Medical Center Disclosures None Outline Who undergoes
Inflammatory Bowel Disease RTC 10/30/09
 Inflammatory Bowel Disease RTC 10/30/09 October 30, 1735 2nd President of the United States, John Adams, was born. Prior to becoming president he served 2 terms as Vice President under George Washington.
Inflammatory Bowel Disease RTC 10/30/09 October 30, 1735 2nd President of the United States, John Adams, was born. Prior to becoming president he served 2 terms as Vice President under George Washington.
CROHN S DISEASE. The term "inflammatory bowel disease" includes Crohn's disease and the other related condition called ulcerative colitis.
 CROHN S DISEASE What does it consist of? Crohn s disease is an inflammatory process that affects mostly to the intestinal tract, although it can affect any other part of the digestive apparatus from the
CROHN S DISEASE What does it consist of? Crohn s disease is an inflammatory process that affects mostly to the intestinal tract, although it can affect any other part of the digestive apparatus from the
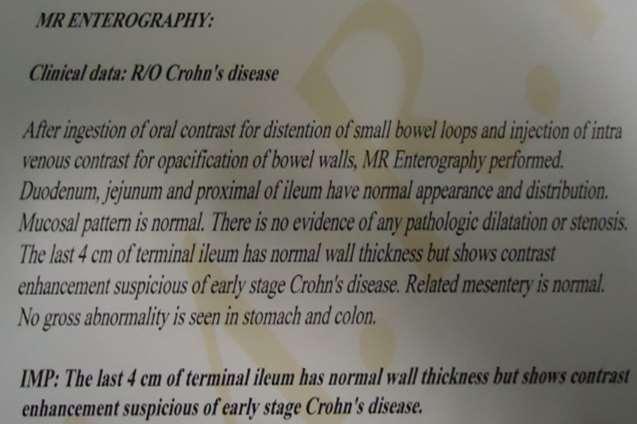
children Crohn s disease in MR enterography for GI Complications Microscopy Characterization Primary sclerosing cholangitis Anorectal fistulae
 MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
MR enterography for Crohn s disease in children BOAZ KARMAZYN, MD PEDIATRIC RADIOLOGY ASSOCIATE PROFESSOR Characterization Crohn disease Idiopathic chronic transmural IBD Increasing incidence Age 7/100,000
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Biologic Therapy for Inflammatory. Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida
 Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
1. Background: Infliximab is administered parenterally; therefore, it is not covered under retail pharmacy benefits.
 Subject: Infliximab (Remicade ) Original Original Committee Approval: October 13, 2006 Revised Last Committee Approval: December 3, 2008 Last Review: October 19, 2007 1. Background: Infliximab is a genetically
Subject: Infliximab (Remicade ) Original Original Committee Approval: October 13, 2006 Revised Last Committee Approval: December 3, 2008 Last Review: October 19, 2007 1. Background: Infliximab is a genetically
Case Discussion. Nutrition in IBD. Rémy Meier MD. Ulcerative colitis. Crohn s disease
 26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
26.08.2017 Case Discussion Nutrition in IBD Crohn s disease Ulcerative colitis Rémy Meier MD Case Presentation 30 years old female, with diarrhea for 3 months Shool frequency 3-4 loose stools/day with
Treating Crohn s and Colitis in the ASC
 Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
Treating Crohn s and Colitis in the ASC Kimberly M Persley, MD Texas Digestive Disease consultants TASC Meeting Outline IBD 101 Diagnosis Treatment Burden of Disease Role of ASC Inflammatory Bowel Disease
The Role of Surgery in Inflammatory Bowel Disease. Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health
 The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
The Role of Surgery in Inflammatory Bowel Disease Cory D Barrat, MD Colon and Rectal Surgeon Mercy Health THANKS FOR INVITING ME! I have no financial disclosures Outline - Who am I and what do I do? -
Cx601 ADMIRE-CD Top-Line Results Webcast. 24 August 2015
 Cx601 ADMIRE-CD Top-Line Results Webcast 24 August 2015 1 Cx601 ADMIRE-CD Top-Line Results Webcast Speakers Mr Eduardo Bravo, Chief Executive Officer Dr Julián Panés, Head of Gastroenterology Department,
Cx601 ADMIRE-CD Top-Line Results Webcast 24 August 2015 1 Cx601 ADMIRE-CD Top-Line Results Webcast Speakers Mr Eduardo Bravo, Chief Executive Officer Dr Julián Panés, Head of Gastroenterology Department,
Use of Seton in Management of High Variety of Anal Fistula
 ORIGINAL ARTICLE Use of Seton in Management of High Variety of Anal Fistula *M or, S Abbasi Background: Anal fistula is an abnormal communicative small channel that has an internal opening and an external
ORIGINAL ARTICLE Use of Seton in Management of High Variety of Anal Fistula *M or, S Abbasi Background: Anal fistula is an abnormal communicative small channel that has an internal opening and an external
Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula
 Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
Hindawi Case Reports in Surgery Volume 2017, Article ID 1929182, 4 pages https://doi.org/10.1155/2017/1929182 Case Report Squamous Cell Carcinoma Originating from a Crohn s Enterocutaneous Fistula Bogdan
Management of complex perianal Crohn s disease
 REVIEW ARTICLE Annals of Gastroenterology (2017) 30, 1-12 Management of complex perianal Crohn s disease Lara Aguilera-Castro, Carlos Ferre-Aracil, Ana Garcia-Garcia-de-Paredes, Enrique Rodriguez-de-Santiago,
REVIEW ARTICLE Annals of Gastroenterology (2017) 30, 1-12 Management of complex perianal Crohn s disease Lara Aguilera-Castro, Carlos Ferre-Aracil, Ana Garcia-Garcia-de-Paredes, Enrique Rodriguez-de-Santiago,
Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series
 CASE REPORT Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series Kaori Fujiwara, Takuya Inoue, Naoki Yorifuji, Munetaka Iguchi, Taisuke Sakanaka, Ken Narabayashi,
CASE REPORT Effect of Adalimumab on an Enterocutaneous Fistula in Patients with Crohn s Disease: A Case Series Kaori Fujiwara, Takuya Inoue, Naoki Yorifuji, Munetaka Iguchi, Taisuke Sakanaka, Ken Narabayashi,
Case Presentations #2 Saturday November 13, Case #1 HPI 11/14/10. Uma Mahadevan-Velayos MD. Complicated Crohn s Pregnancy
 Case Presentations #2 Saturday November 13, 2010 Uma Mahadevan-Velayos MD Case #1 Complicated Crohn s Pregnancy HPI 34 yo F with Crohn s disease presents to office 18 weeks pregnant, moved back to SF from
Case Presentations #2 Saturday November 13, 2010 Uma Mahadevan-Velayos MD Case #1 Complicated Crohn s Pregnancy HPI 34 yo F with Crohn s disease presents to office 18 weeks pregnant, moved back to SF from
Proctitis Workshop. PD Dr Michel H. Maillard, MD-PhD 1,2. Crohn s and Colitis Center, Gastroentérologie Beaulieu SA.
 Proctitis Workshop PD Dr Michel H. Maillard, MD-PhD 1,2 1 Crohn s and Colitis Center, Gastroentérologie Beaulieu SA 2 CHUV, Lausanne PD Dr Lukas Brügger, Universitätsklinik für Viszerale Chirurgie und
Proctitis Workshop PD Dr Michel H. Maillard, MD-PhD 1,2 1 Crohn s and Colitis Center, Gastroentérologie Beaulieu SA 2 CHUV, Lausanne PD Dr Lukas Brügger, Universitätsklinik für Viszerale Chirurgie und
Pharmacotherapy of Inflammatory Bowel Disorder
 PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: May 1, 2018 Last Revised: April 18, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
PHARMACY / MEDICAL POLICY 5.01.563 Pharmacotherapy of Inflammatory Bowel Disorder Effective Date: May 1, 2018 Last Revised: April 18, 2018 Replaces: Extracted from 5.01.550 RELATED MEDICAL POLICIES: 11.01.523
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation?
 Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
Crohn s Disease: Should We Treat Based on Symptoms or Based on Objective Markers of Inflammation? Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών. Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων
 Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab.
 Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab. Dr Peter Irving Guy s and St Thomas Hospital, London King s College London Response to vedolizumab
Predicting response to anti - integrin therapy: long term efficacy and roles for optimisation with vedolizumab. Dr Peter Irving Guy s and St Thomas Hospital, London King s College London Response to vedolizumab
Clinical Policy: Vedolizumab (Entyvio) Reference Number: CP.PHAR.265 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.265 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Entyvio) Reference Number: CP.PHAR.265 Effective Date: 07.16 Last Review Date: 11.18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this
Clinical Policy: (Entyvio) Reference Number: CP.PHAR.265 Effective Date: 07.16 Last Review Date: 11.18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Cover Page The handle http://hdl.handle.net/1887/38545 holds various files of this Leiden University dissertation. Author: Molendijk, Ilse Title: Mesenchymal stromal cell therapy for Crohn's disease :
Doncaster & Bassetlaw Medicines Formulary
 Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Doncaster & Bassetlaw Medicines Formulary Section 1.5 Chronic Bowel Disorders (including IBD) Aminosalicylates: Mesalazine 400mg and 800mg MR Tablets (Octasa) Mesalazine 1.2g MR Tablets (Mezavant XL) Mesalazine
Identifying and Managing Patients with IBD at Risk for Progressive Disease
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Practice Parameters for the management of perianal abscess and fistula-in-ano(1)
") New frontiers in Crohn s perianal fistulae disease Dr Nadine Harran Colorectal surgeon, WDGMC 1. Introduction 2. Seton 3. The OVESCO Proctology Clip 4. Collagen fistula plugs 5. Sealents 6. Mucosal advancement
New frontiers in Crohn s perianal fistulae disease Dr Nadine Harran Colorectal surgeon, WDGMC 1. Introduction 2. Seton 3. The OVESCO Proctology Clip 4. Collagen fistula plugs 5. Sealents 6. Mucosal advancement
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication
 Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication") UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
UvA-DARE (Digital Academic Repository) Surgical treatment of perianal and rectal fistula van Koperen, P.J. Link to publication Citation for published version (APA): van Koperen, P. J. (2010). Surgical
Outcome of hybrid seton placement for the treatment of high complex anal fistulas with and without tube drainage: A prospective comparative study
 715581EJI0010.1177/1721727X17715581European Journal of InflammationWushouer et al. letter2017 Letter to the Editor Outcome of hybrid seton placement for the treatment of high complex anal fistulas with
715581EJI0010.1177/1721727X17715581European Journal of InflammationWushouer et al. letter2017 Letter to the Editor Outcome of hybrid seton placement for the treatment of high complex anal fistulas with
Inflectra Frequently Asked Questions
 Inflectra Frequently Asked Questions 1. What is the funding status of Inflectra (infliximab)? Earlier in 2016, Inflectra (infliximab) was added to the Ontario Drug Benefit (ODB) Formulary as a Limited
Inflectra Frequently Asked Questions 1. What is the funding status of Inflectra (infliximab)? Earlier in 2016, Inflectra (infliximab) was added to the Ontario Drug Benefit (ODB) Formulary as a Limited
Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma: a pilot study
 Tech Coloproctol (2015) 19:455 459 DOI 10.1007/s10151-015-1311-8 ORIGINAL ARTICLE Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma:
Tech Coloproctol (2015) 19:455 459 DOI 10.1007/s10151-015-1311-8 ORIGINAL ARTICLE Treatment of Crohn s disease-related high perianal fistulas combining the mucosa advancement flap with platelet-rich plasma:
IBD 101. Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition
 IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
IBD 101 Ronen Stein, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Objectives Identify factors involved in the development of inflammatory bowel
Disclosure of Affiliations. The Way We Hope It Goes. Medicines and Surgery for IBD. None. Cases: Sweet and Not So Sweet
 Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
Immunomodulators and Complications of Surgery for Inflammatory Bowel Disease Disclosure of Affiliations None Thomas E. Read, MD, FACS, FASCRS Professor of Surgery Tufts University School of Medicine Senior
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL
 INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
INFLIXIMAB FOR PREVENTION OF POST-OPERATIVE CROHN S DISEASE RECURRENCE: THE PREVENT TRIAL A. Hillary Steinhart, MD MSc FRCP(C) Medical Lead, Mount Sinai Hospital IBD Centre Professor of Medicine University
Implementation of disease and safety predictors during disease management in UC
 Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male
Implementation of disease and safety predictors during disease management in UC DR ARIELLA SHITRIT DIGESTIVE DISEASES INSTITUTE SHAARE ZEDEK MEDICAL CENTER JERUSALEM Case presentation A 52 year old male