Assessment, diagnosis and management of leg ulcers. Sarah Gardner, Clinical lead, Tissue viability service
|
|
|
- Lester Richard
- 6 years ago
- Views:
Transcription
1 Assessment, diagnosis and management of leg ulcers Sarah Gardner, Clinical lead, Tissue viability service

2 What are the challenges of leg ulcer management?


3 How do you feel when a patient is referred with a leg ulcer?

4 How do you think your patient feels about their leg ulcer?
5 Aim of the session To develop a better understanding of the factors that contribute to the development of leg ulceration and how the application of proven treatments can improve clinical outcomes
6 Objectives - } To gain a better understanding of the anatomy & Physiology of the vascular system } To understand the function of the veins and how venous incompetence can lead to skin breakdown } Be able to carry out a full holistic leg ulcer assessment in order to correctly diagnose the aetiology. } On diagnosis, be able to put an appropriate plan of care in place in order to support timely wound healing } Be able to differentiate between normal and abnormal ulceration and recognise when referral is necessary.

7 Leg ulcer training? Why bother? } Hopefully you are here because you want to be } We have variable healing rates } LU assessment not always holistic } Bandaging challenges } Wounds that are constantly colonised and inflammatory } Wounds that are not progressing aren't always referred on in a timely way } Pain is difficult to manage } Co morbidities are sometimes seen in isolation to the wound

8 Exposed tendon

9 Chronic ulceration what is effective leg ulcer management?

10 Arterial or venous???

11 Skin condition or leg ulceration?

12 Multiple wound types

13 Stubborn ulcers over the malleoli

14 Severe local infection what do we do?

15 When does trauma become leg ulceration?

16 The tipping point. Today you will leave this training session and you will do things differently!
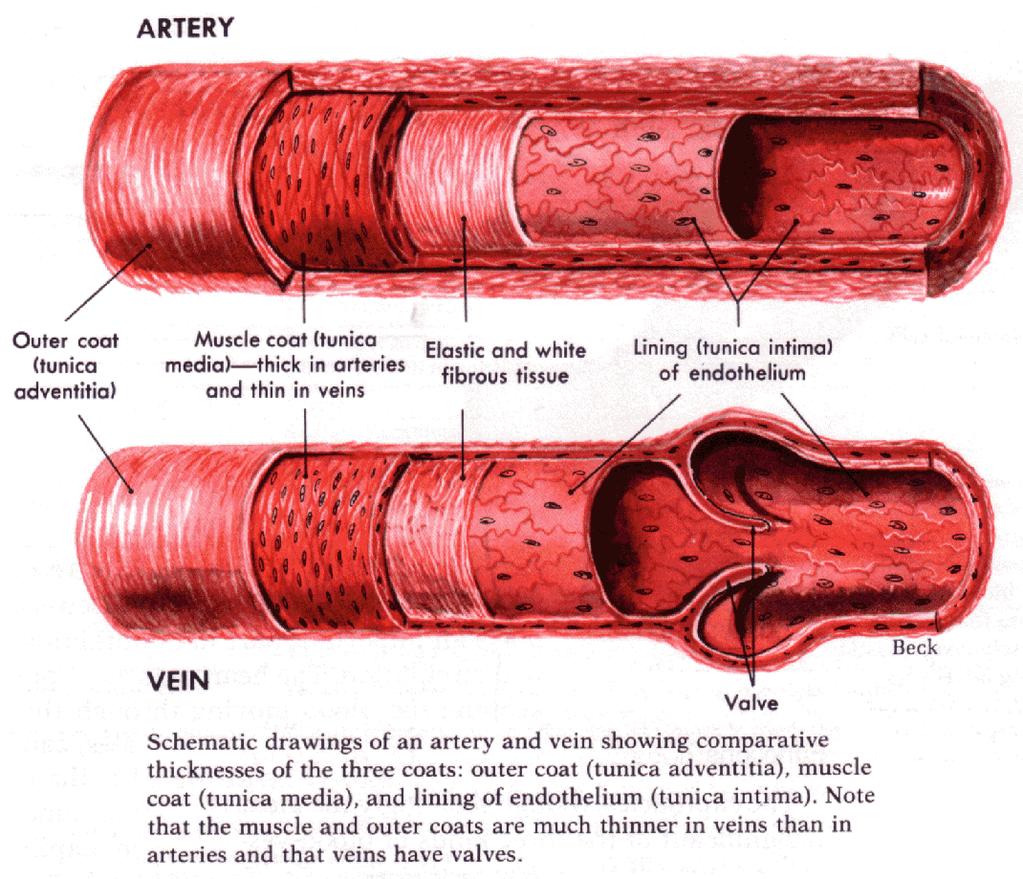
17

18 Patient experience film
19 What is a leg ulcer?
20 Definition A leg ulcer is a long-lasting (chronic) wound on your leg or foot that takes more than six weeks to heal. NHS choices, A Venous leg ulcer is an open lesion between the knee and the ankle that remains unhealed for 4 weeks and occurs in the presence of venous disease. (SIGN, 2010)
21 Epidemiology of leg ulcers } Point Prevalence } 0.1%-0.2% per 1000 } 4.5% per 1000 in older people (over 80) } Overall Prevalence } 1%-2% (Oxford is 0.8%) } Cost } million a year (Simon et al 2004).
22 Causes/ aetiology } Venous disease = 70% } Arterial = 10-15% } Mixed arterial & venous disease = %

23 The circulatory system Arteries carry oxygenated blood to your legs and the veins carry de-oxygenated blood away from your legs. The blood returns to the lungs to pick up more oxygen and returns to the heart to be pumped out again through the arteries.
24 Blood vessels Arteries Arteries take blood away from the heart and are the strongest blood vessels, as they have to withstand the pumping action of the heart. Arterial blood is charged with oxygen and nutrients for healthy tissues. Artery walls consist of three layers, the walls are more muscular and the lumen smaller enabling blood to travel at high pressure. Arteries branch into smaller vessels known as arterioles, which merge into capillaries. Capillaries Minute vessels, no wider than a hair, which connect arteries to veins. The exchange of gases (oxygen for carbon dioxide) occurs within the capillaries. A capillary wall is a semi permeable membrane and interstitial fluid moves continually between the blood capillary and the tissue. The rate of fluid leaking depends on several factors, including blood pressure in the blood capillaries and the concentration of plasma proteins in the tissue spaces.
25 Venules - When blood has left the tiny capillaries on its journey back to the heart, the vessels widen into venules and then into the larger vessels known as veins. Veins These take blood back to the heart. Their walls are weaker than arteries and take impure blood back to the heart as oxygen has now been exchanged for carbon dioxide in the capillaries. Veins can be classed as superficial or deep. 10% of blood travels through the superficial veins, which are situated just beneath the skin. The remaining 90% of blood travels through deep veins, which are found closer to the bones in the leg and are surrounded and protected by various muscles. These are the veins squeezed by the calf pump on contraction. Veins are also equipped with valves to assist the flow of blood back to the heart. The valves in the veins open in one direction, therefore helping to prevent backflow of blood. When valves are working as they should, healthy veins are divided into compartments and this helps to relieve strain on the vessel walls. Perforator -So called because they perforate the deep fascia of muscles, to connect the superficial veins to the deep veins where they drain. Their role is to maintain correct blood drainage. They have valves which prevent blood flowing back (reflux), from deep to superficial veins in muscular systole.

26 Lymphatic system This is a one-way drainage system that returns fluid to the vascular circulation via a network of lymphatic vessels and lymph nodes. Some lie deep within the body, others close to the skin. The lymphatic system has an important role to play in maintaining fluid balance, transporting fats and proteins and providing an immune response. The main function of the lymphatics is to help the re-absorption of interstitial fluid into the blood circulation. Normal balance is reached when fluid and waste products are removed from the tissues as quickly as they are produced. Increased capillary leakage can overwhelm the capacity of the lymphatics to drain the excess fluid, which can result in oedema.
27

28 HEALTHY VENOUS FUNCTION For blood to be effectively taken against gravity back to the heart the body needs valves in the veins to prevent the backflow of blood Leg Ulcers
 changes can start to occur within the legs which can result in leg ulceration.")
29 Faulty valves } When the deep system has faulty valves (the valves do not close tightly allowing the blood to leak back down) changes can start to occur within the legs which can result in leg ulceration. This is known as venous insufficiency.
30 ABNORMAL VENOUS FUNCTION - Damaged valves are a predisposing factor not a cause for developing a leg ulcer Leg Ulcers

31 Capillary exchange Fluids flow out of a capillary at the upstream end near an arteriole and re- enters a capillary downstream near a venule. The direction of fluid movement across the capillary wall at any point depends on the difference between two opposing forces: blood pressure and osmotic pressure. When the pressure in the venous system is high it will affect the movement.

32 How does this result in venous disease/ ulceration?
33 Progression of damage incompetent valves venous stasis (pooling) exacerbates high pressure venous dilation tissue flooding intoxication and local Ischaemia venous ulcer
34 CEAP Classification of chronic venous disease } Clinical classification C0: no visible or palpable signs of venous disease C1: telangiectasies or reticular veins C2: varicose veins C3: oedema C4a: pigmentation or eczema C4b: lipodermatosclerosis or athrophîe blanche C5: healed venous ulcer C6: active venous ulcer S: symptomatic, including ache, pain, tightness, skin irritation, heaviness, and muscle cramps, and other complaints attributable to venous dysfunction A: Asymptomatic
35 Risk factors for venous disease/ ulceration: } Hereditary } Age } Female sex } Obesity } Pregnancy } Prolonged standing } Greater height } Immobilisation } PMH DVT
36 Arterial ulcers } Arterial insufficiency refers to poor blood circulation to the lower leg and foot and is most often due to atherosclerosis. In atherosclerosis the arteries become narrowed from deposits of fatty substances in the arterial vessel walls, often due to high levels of circulating cholesterol and aggravated by smoking and high blood pressure (hypertension). The arteries fail to deliver oxygen and nutrients to the leg and foot resulting in tissue breakdown.

37 PATHOLOGY Progressive occlusion Increased oxygen demand Leg Ulcers
38 Risk factors for arterial disease } Smoking } Diabetes } Obesity } High BP } High cholesterol } Increasing age } Family history
39 Assessment } For every 1 mistake for not knowing, 10 are made for not looking!!

40 Assessment } Obtaining a diagnosis can only be achieved with a robust leg ulcer assessment } A leg ulcer assessment, including a doppler and/ or lower limb assessment should be carried out within 1-2 weeks of the patient presenting } Doppler is only an aid to diagnosis not the be all and end all. LOOK AT THE LIMB WHAT DOES IT TELL YOU?
41 Assessing patients with leg ulceration } 1 Patient assessment (Extrinsic factors) } 2 Patient assessment (Intrinsic factors) } 3 Lower limb assessment } 4 Wound assessment

42 Patient assessment } What information do you need to obtain when you carry out a patient assessment? } Why is this information important/ relevant? } From the case study you have in front of you, what information is relevant and why? } Is this information assisting your diagnosis? } Do you require more information at this point?
43 Feedback
44 PATIENT FACTORS (extrinsic & Intrinsic) } socio-economic factors } cultural and religious beliefs } hygiene / environment } mobility; activity levels } lifestyle choices smoking / drugs / alcohol } major life stressors } Occupation/ previous occupation } treatments (appropriateness) } isolation } health beliefs / belief in treatment } relationship with nurse } concordance levels } medicines, drug therapies } Full medical history } Anxiety & Depression score } Quality of Life assessment } Bloods } Medication } MUST/ BMI } BP } Co-morbidities e.g. diabetes, rheumatoid arthritis current status. } Pain assessment/ score
45 Clinical history indicators of possible venous involvement } DVT } Thrombophlebitis } Leg, Pelvis or foot Fractures } Vein surgery or Sclerotherapy } Obesity } Multiple pregnancies } H/O Pulmonary embolism
46 Clinical history indicators of possible arterial involvement } Intermittent Claudication } Ischemic rest pain } CVA } MI } TIA } Peripheral vascular disease } Smoker } Diabetes } Heart disease or surgery } Hypertension } Renal Disease

47 84 yr old diabetic, COPD, renal disease.

48 8 weeks after commencing insulin

49 Pain assessment & management

50 Pain Scale (Taken from the Wong-Baker Faces Scale)
51 Abbey Pain scale } For measurement of pain in people with dementia who cannot verbalise. } Focusses on: vocalisation (whimpering, groaning, crying) } Facial expression } Changes in body language } Behavioural change } Physiological change (Temp, pulse or BP) } Physical changes (Skin tears, pressure areas, contractures)
52 What type of pain- Use descriptors Neuropathic Pain } shooting } burning } tingling } stabbing } piercing } raw } pricking } throbbing } Pins and needles } dagger like Nociceptive Pain } dull } aching } tender } cramping } sore } twinge } hurt } uncomfortable } spasm } nagging } sickly
53 Hyperalgesia and allodynia } Patients can get Hyperalgesia (Excruciating pain in the wound bed } Allodynia (Pain in the surrounding skin) } Pain can follow a non-painful event such as wound exposure } Usual forms of analgesia are often not effective

54 Lower limb assessment } Signs and symptoms of leg ulceration
 } Hyperkeratosis } Lipodermatosclerosis } Oedema } Varicose veins } Skin colour pale/ red/ normal } Skin colour changes on elevation & dependence } Temperature } Capillary refil < 3 seconds")
55 Assessment of the limb } VASCULAR STATUS Doppler and/ or lower limb asessment } Limb shape & size } Haemosiderin staining } Atrophie blanche } Ankle flare } Eczema (& cause varicose, contact, irritant) } Hyperkeratosis } Lipodermatosclerosis } Oedema } Varicose veins } Skin colour pale/ red/ normal } Skin colour changes on elevation & dependence } Temperature } Capillary refil < 3 seconds } Site of ulceration
56 ARTERIAL ULCERS VENOUS ULCERS Cause Arterial disease Chronic venous hypertension Wound bed appearance Deep Cliff edge margins Shallow Irregular wound margins Evolution Rapid deterioration Slow evolution Skin aspect Localization Oedema Shiny Pale Cold to touch Hair loss At the extremity: foot and lower limb May have a localised oedema Pigmented Eczema Warm to touch Ankle flare Lateral or medial malleolus Generalized oedema Acute and chronic wound, Ruth A. Bryant lower extremity ulcers, chapter 12, 2000 Pain Painful: Ischaemic pain Painful if infected Leg Ulcers
57 Lymphovenous disease } Venous and lymphovenous disease is progressive } Symptoms manifest as skin changes } These deteriorate as the disease progresses } Following the mid term disease stage (atrophie blanche, haemosiderin staining etc) legs progress to the advanced stage. } This includes enhanced skin folds, papillomatosis (superficial lymphatic vessels protruding through the skin), lymphorrhoea (wet legs), cellulitis. } On reaching this stage your management plan would differ to that of a standard venous leg ulcer patient.
58 Vascular assessment
59 Why is Doppler Assessment Necessary? } All patients presenting with an ulcer or lower limb problems should be screened for arterial disease by Doppler measurement of ABPI. } To enable effective treatment options to be established. } To minimise the risk factors of compression therapy. } To support holistic assessment.
 Graduated Compression Therapy")
60 USING A DOPPLER ULTRASOUND v ABPI = Normal range vabpi = Venous disease v ABPI = = Mixed aetiology v ABPI < 0.6 = Severe arterial disease vabpi > 1.3 = Medial wall calcification (Nelson E.A., 1996) Graduated Compression Therapy

61 Wound assessment } Look at your case study and the wound } What are you looking at? } What information is required? } What does this mean/ is it important? } How is this information recorded?
62 Feedback
63 Wound assessment } Cause } Is it a reoccurrence? } Duration } Wound area in cm² as a baseline (Is it bigger/ smaller and in what timescale) } Tissue type (including hypergranulation) } Infection/ biofilm prescence } Wound edges } Odour } Type and level of exudate } Peri wound skin status } Photograph } Previous management regimes } History of healing rates

64 TIME slide } T = Tissue } I = Infection } M = Moisture } E = Edge

65 T = Tissue } What does it look like? } What type of tissue in the in wound bed? } Granulating } Epithelialising } Sloughy } Necrotic } Work out % s and document

66 Epithelialising

67 Granulating

68 Sloughy

69 Necrotic

70 I = Identifying wound bed infection } Wound bed contamination } Wound bed colonisation } Local wound bed infection } Systemic infection } Use the AMBL tool

71 M = Moisture. Exudate pathway } Follow the pathway to identify causes of exudate levels } Is wound too wet or too dry? } What does exudate look like? } How much is there? How do you measure it?

72 E = Wound edges and peri wound skin assessment } Rolled edges may indicate malignancy } Cliff edges/ punched out often indicative of arterial disease } Epithelialising edges will be fragile and vulnerable and must be protected. } Moisture balance is essential not too wet and not too dry! } Consider skin barriers

73 Wound measurement Working out surface area in cm²
74 Identifying abnormal or difficult to treat leg ulcers

75 Diabetic foot ulcer not a leg ulcer! } Caused by the combination of arterial blockage and nerve damage. Although diabetic ulcers may occur on other parts of the body they are more common on the foot.

76 Squamous cell carcinoma Squamous-cell carcinoma (SCC or SqCC) is a cancer of a kind of epithelial cell, the squamous cell. These cells are the main part of the epidermis of the skin, and this cancer is one of the major forms of skin cancer.

77 Pyoderma granulosum Though the aetiology is not well understood, the disease is thought to be due to immune system dysfunction, and particularly improper functioning of neutrophils. At least half of all pyoderma gangrenosum patients also suffer from illnesses that affect their systemic function. For instance, ulcerative colitis and rheumatoid arthritis.

78 Vasculitis Vasculitis is a group of disorders that destroy blood vessels by inflammation. Both arteries and veins are affected.

79 Marjolin's ulcer Refers to an aggressive ulcerating squamous cell carcinoma presenting in an area of previously traumatised, chronically inflamed, or scarred skin. They are commonly present in the context of chronic wounds including burn injuries, venous ulcers, ulcers from osteomyelitis, and post radiotherapy scars.

80 Bowens disease Bowen's disease is a very early form of squamous cell skin cancer, which is easily curable. The main sign is a red, scaly patch on the skin.

81 Leg ulcer management
82

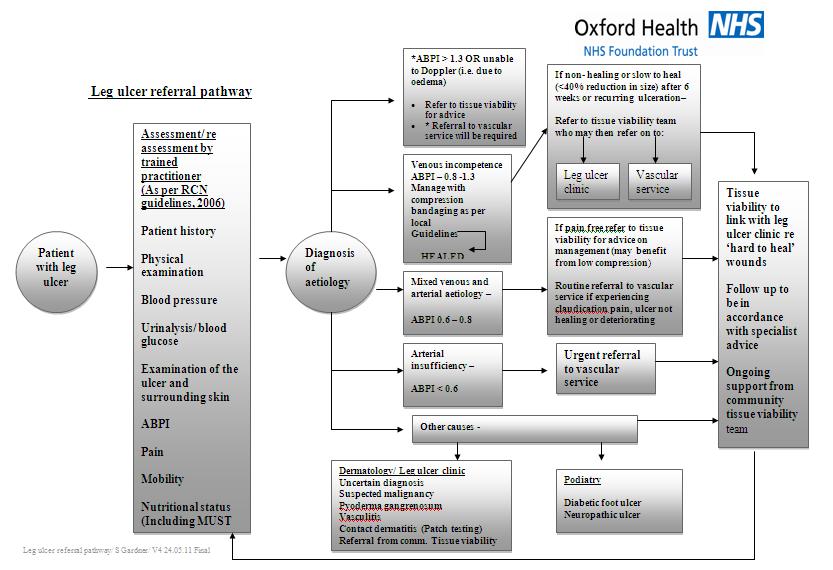
83 Venous leg ulcer management using the VLU pathway.

84 Set out your milestones
85 Milestones } Assessment } Diagnosis } Consider Do I need to refer at this stage? } If no. } Management } Leg ulcer pathway allocation (If venous) } Re-assessment (every 6 weeks) } Progressing? If no then refer to tissue viability. } Healed? } If yes. Prevention of recurrence care plan
86 Venous LU Pathways: Standard or complex? Standard criteria Complex criteria } First ulcer } Ulcer < 6 months old } Size < 100cm² } < 3 episodes of local infection Ulcer > 6 months old Recurrent ulcer (automatically allocated to complex pathway) Size > 100cm² > 3 episodes of local infection

87 Venous leg ulcer pathway Provides an evidence based approach to LU management with an aim to heal by 24 weeks.
88 Treatment pathways focus on: } Wound bed preparation } Eradication of infection } Pain management } Correct bandage selection and application } % Progression at 6 week intervals } Early referral to tissue viability
89 Patient Status at a Glance board } All DN teams should now be displaying a board } Mandatory requirement for OH staff now } All new patients with a leg wound greater than 4 weeks need adding and will remain on if assessed as venous. } All new patients and those removed in the past month get reported } Information gets passed to CCG re healing rates } 70% healing at 24 weeks is expected.
 } Emollient")
90 First - Washing and skin care } Legs should be washed at each dressing change } Emollient should be added to water } NO aqueous } Remove debris/ hyperkeratotic plaques } Use a cloth/ flannel for large areas of hyperkeratosis (get pt to wash it properly in between use) } Emollient therapy


91 } What is available to use? } How do you choose an emollient for your patient? } How do you apply the emollient
92 Feedback


93 Wound bed preparation Debridement required?


94 Primary dressing If healthy Based on pathway allocated } Atrauman if wound bed healthy } Absorbent pad based on exudate level. } Urgostart contact if complex


95 If debridement needed } Standard Urgoclean } Complex Topical antimicrobial

96 Locally Infected? Use Antimicrobial formulary to guide your clinical decision Honey = 1 st line Cadexomer iodine = 2 nd line NOT INADINE NOT SILVER 2 weeks

97 Managing the exudate } How do you make a decision re amount? } How do you choose absorbent pad? } How do you choose how often to change the dressings? } How does the padding affect the compression? } Use exudate pathway
 if more mobile and getting out of house walking } This applies to venous ulceration NOT chronic oedema/")
98 Compression } Based on level of mobility } K Two if immobile or limited mobility (Restricted to the house/ getting to loo or kitchen) } Actico (short stretch) if more mobile and getting out of house walking } This applies to venous ulceration NOT chronic oedema/ lymphoedema
99 Treatment requirements included Treatment objective Standard Complex Maintaining healthy wound bed Atrauman + Absorbent pad Urgostart contact + absorbent pad Debridement Urgoclean Honey or iodine (2 weeks) Management of local WB infection Honey or iodine (2 weeks) Honey or iodine (2 weeks) Ongoing WB maintenance Atrauman + absorbent pad Urgostart contact (for max of 12 weeks) then Atrauman + absorbent pad Failure to progress at 6 weeks Transfer to complex pathway Refer to tissue viability Exudate management Based on level: Zetuvit E, Zetuvit plus or Sorbion Based on level: Zetuvit E, Zetuvit plus or Sorbion Compression Based on level of mobility: Actico or K Two Based on level of mobility: Actico or K Two

100 Progression at 6 weeks If the wound is progressing in a normal way then there should be a 40% reduction in wound size at 6 weeks. If this is not achieved RE ASSESS, consider possible reasons and refer to tissue viability for advice.

101 Wound size progression % = Continue on pathway 20 30% = Consider: Is the wound sloughy or infected? Is the wound inflamed? Is the compression on properly? Has there been a change in Pts health? 0 20% = Refer to Tissue Viability for advice





102 Management plan should also include: } Care plan for pain management } Mobility/ exercises } Lifestyle/ QoL

103 Exercise/ leg elevation } In the case of an ulcer, it is not expedient to stand, especially if the ulcer be situated on the leg (Hippocrates, 400 yrs BC)
104 Topical steroids in wound care The evidence??? } Is known to work but why? } Not licensed to be used directly on wound beds so where do you stand re accountability? } How much should be used and for how long? } Full of allergens particularly the ones with antibiotics. } Possibly mask underlying problems } Can have similar long term effects as systemic steroids. } Should not routinely be used unless discussed with tissue viability first. NEW PROTOCOL AVAILABLE } Trimovate now YELLOW listed (For continuation following specialist recommendation only)and should be time specific.

105 Gallop through compression.

106 Bandaging - Compression therapy, the gold standard treatment for venous leg ulcers
107 Factors to be considered before applying compression } Skin condition delicate friable skin can be damaged by high levels of pressure } Shape of the limb the sub-bandage pressure and the pressure gradient will be altered by the limb shape in accordance with Laplace s Law. Skin overlying exposed bony prominences may be subject to pressure damage } Presence of neuropathy the absence of a protective response increases the risk of sub-bandage pressure damage } Presence of cardiac failure rapid fluid shifts can be dangerous as it increases the preload of the heart

108 How does compression work?

109 Feedback
110 FUNCTIONS OF COMPRESSION THERAPY } Reduces distension of the veins } Increases the function of the calf muscle pump } Restores valve function } Increases the velocity of venous blood flow } Reverses venous hypertension } Reduces oedema } Improves the microcirculation blood flow } Reduces inflammation } Improves symptoms of lipodermatosclerosis Graduated Compression Therapy
111 Why compression? The evidence 2 Systematic reviews of RCTs concluded that more people heal their ulcers under compression than without compression (Cullum et al, 2001) Taken from the RCN guidelines, 2006


 Graduated")
112 LAPLACE S LAW C T T N c (4630) P = CW P = sub bandage pressure T = bandage tension N = number of layers applied c = constant C = circumference of the limb W = bandage width W Clinical studies have focused on 40mmHg pressure at the ankle because this is the figure calculated to reverse venous hypertension (Blair et al, 1988) Graduated Compression Therapy
113 GRADUATED COMPRESSION Graduated compression is when the bandages are applied at the correct compression up the leg The pressures fall as the circumference of the leg increases 20 mmhg 30 mmhg 40 mmhg Providing the bandage is applied according to manufacturer instruction Graduated Compression Therapy

114 Bandages

115 Wool } How should it be applied?



116 Compression bandages } Short stretch } Elastic } Multi layered } 2 layer } 4 Layer } Reduced compression
117 What is the difference between long (elastic) and short stretch (inelastic) bandages?
118 Working and resting pressures Working Pressure When the muscle pump is active and expands it presses against the bandage The resistance of the bandage presses back against the muscle This creates a working pressure An inelastic bandage with no give donates a high working pressure Resting Pressure When the muscle pump relaxes it is not pressing against the bandages No resistance from the bandages This creates a low resting pressure Elastic bandages maintain a constant pressure by squeezing the muscle
119 Compression bandage choices for Oxfordshire } Ko Flex (Low compression) 20mmHg } K Two (Multilayer) Will give a constant 40mmHg. Will be more effective in patients who have limited or no mobility. } Actico (Short stretch) Will deliver high working pressure and low resting pressure. Possibly more suitable for mobile patients. ALL available on ONPOS
120 Applying compression } Establish ABPI (Full compression needs an ABPI of ) } Gain consent & supply verbal/ written information. } Assess shape of limb first (Photograph as baseline) } Measure ankle circumference and document } Apply dressings then shape limb to create a graduated shape. } Re - measure ankle circumference and choose bandage size/ number based on type. } Consider H&S issues risk assess } Offer advise post application things to look out for.


121 CAUTIONS WITH FULL COMPRESSION Heart failure Arterial ulcers Graduated Compression Therapy
until pain is")
122 Discontinue compression if patient has a systemic infection (Cellulitis)until pain is less acute.
123 Concordance } Assess why patient is not concording } Is pain managed effectively } Is patient anxious or depressed? (HADS score) } Do they need to be referred? } Consider your skills/ your approach to the care } Have you taken time to explain why they have leg ulceration and how compression works? } Have you issued a patient information leaflet?

124 Managing non healing, complex ulcers/ wounds When is a wound palliative?
125 Managing complex ulcers } Failure to progress } Exudate management } Pain } Odour } Infection } Dealing with pts anxiety re the problem } Feeling helpless never ending! } When to refer } When do we give up? } Palliative wounds
 } Reassess ABPI } Refer to TV if uncertain of")
126 Mixed aetiology } Correct diagnosis } Establish degree of arterial disease } Consider reduced compression (Ko flex) } Debride and treat local infection } Skin care } Monitor progress every 6 weeks (Unlikely to achieve 40%) } Reassess ABPI } Refer to TV if uncertain of plan
 } Evaluate effectiveness of actions } Refer to TV for advice/")
127 Arterial disease- may become palliative } Refer to vascular for an opinion } Reassess following intervention re healing potential } Careplan should be focussed on symptom management (Pain, infection, exudate, skin care etc) } Evaluate effectiveness of actions } Refer to TV for advice/ support

128 Dressings for mixed and arterial ulcers treat the symptom/ problem } Layering dressings will not necessarily improve the outcome } Most advanced dressings are effective on their own } Use the step up step down approach } Consider your rationale for choice } Measure whether its working } Give the dressing time to work } Is it a formulary dressing?

129 And now. Case studies As a group. Put together a plan of care for your patient
130 Thank you }You have been.
PRODIGY Quick Reference Guide
 PRODIGY Quick Venous leg ulcer infected How do I assess a venous leg ulcer? Chronic venous insufficiency and venous hypertension result from damage to the valves in the veins of the leg and inadequate
PRODIGY Quick Venous leg ulcer infected How do I assess a venous leg ulcer? Chronic venous insufficiency and venous hypertension result from damage to the valves in the veins of the leg and inadequate
Promoting best practice in leg ulcer management
 Promoting best practice in leg ulcer management Sylvie Hampton MA BSc (Hons) DpSN RGN Independent Tissue Viability Consultant Nurse Leg Ulcers - What are the causes? Chronic leg ulcers are defined as those
Promoting best practice in leg ulcer management Sylvie Hampton MA BSc (Hons) DpSN RGN Independent Tissue Viability Consultant Nurse Leg Ulcers - What are the causes? Chronic leg ulcers are defined as those
Reality TV Managing patients in the real world. Wounds UK Harrogate 2009
 Reality TV Managing patients in the real world Wounds UK Harrogate 2009 Reality TV Managing patients in the real world Brenda M King Nurse Consultant Tissue Viability Sheffield PCT Harrogate 2009 Familiar
Reality TV Managing patients in the real world Wounds UK Harrogate 2009 Reality TV Managing patients in the real world Brenda M King Nurse Consultant Tissue Viability Sheffield PCT Harrogate 2009 Familiar
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT
 VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
Leg ulcer assessment and management
 Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Appendix D: Leg Ulcer Assessment Form
 Nursing Best Practice Guideline Appendix D: Ulcer Assessment Form Person Completing Assessment: Date: Client Name: Caf # CM# VON ID #: District CCAC ID # Address Telephone Home: Work: Date of Birth Y/M/D:
Nursing Best Practice Guideline Appendix D: Ulcer Assessment Form Person Completing Assessment: Date: Client Name: Caf # CM# VON ID #: District CCAC ID # Address Telephone Home: Work: Date of Birth Y/M/D:
Identification and recommended management of leg ulcers Jill Robson RGN and Gerard Stansby MA, MChir, FRCS
 Identification and recommended management of leg ulcers Jill Robson RGN and Gerard Stansby MA, MChir, FRCS thickened skin, lipodermatosclerosis skin stained haemosiderin shallow ulcer irregular shape Our
Identification and recommended management of leg ulcers Jill Robson RGN and Gerard Stansby MA, MChir, FRCS thickened skin, lipodermatosclerosis skin stained haemosiderin shallow ulcer irregular shape Our
Venous Insufficiency Ulcers. Patient Assessment: Superficial varicosities. Evidence of healed ulcers. Dermatitis. Normal ABI.
 Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Managing Wounds. Esther White Tissue Viability Nurse
 Managing Wounds Esther White Tissue Viability Nurse First things first.. Assess, measure and photograph Know what you re dealing with, look at anatomical position and the bigger picture to look for extra
Managing Wounds Esther White Tissue Viability Nurse First things first.. Assess, measure and photograph Know what you re dealing with, look at anatomical position and the bigger picture to look for extra
The Management of Lower Limb Oedema. Catherine Hammond CNS/CNE 2018
 The Management of Lower Limb Oedema Catherine Hammond CNS/CNE 2018 Causes of oedema Venous stasis Lymphoedema Heart Failure Dependency Liver and kidney failure Medications Cellulitis Low protein Under
The Management of Lower Limb Oedema Catherine Hammond CNS/CNE 2018 Causes of oedema Venous stasis Lymphoedema Heart Failure Dependency Liver and kidney failure Medications Cellulitis Low protein Under
Jackie Stephen-Haynes. Compression therapies- Does. Jackie Stephen-Haynes 2011
 Jackie Stephen-Haynes Compression therapies- Does compression meet the patients needs? 2011 Aims For practitioner to be able to consider compression options and the impact for the patient Leg Ulcer Definition
Jackie Stephen-Haynes Compression therapies- Does compression meet the patients needs? 2011 Aims For practitioner to be able to consider compression options and the impact for the patient Leg Ulcer Definition
HOW TO APPLY EFFECTIVE MULTILAYER COMPRESSION BANDAGING
 HOW TO APPLY EFFECTIVE MULTILAYER COMPRESSION BANDAGING Alison Hopkins is Clinical Nurse Specialist, East London Wound Healing Centre, Tower Hamlets Primary Care Trust Compression therapy is essential
HOW TO APPLY EFFECTIVE MULTILAYER COMPRESSION BANDAGING Alison Hopkins is Clinical Nurse Specialist, East London Wound Healing Centre, Tower Hamlets Primary Care Trust Compression therapy is essential
Improving customer care in compression hosiery
 Improving customer care in compression hosiery Introduction Within the modern NHS, the Pharmacy Team provides the front line service that most patients have contact with. Compression hosiery has a key
Improving customer care in compression hosiery Introduction Within the modern NHS, the Pharmacy Team provides the front line service that most patients have contact with. Compression hosiery has a key
Chronic Venous Insufficiency Compression and Beyond
 Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
Venous leg ulcers: importance of early assessment and intervention for long-term success
 Venous leg ulcers: importance of early assessment and intervention for long-term success Introduction A venous leg ulcer (VLU) can be defined as: an open lesion between the knee and ankle joint that occurs
Venous leg ulcers: importance of early assessment and intervention for long-term success Introduction A venous leg ulcer (VLU) can be defined as: an open lesion between the knee and ankle joint that occurs
All WALES LYMPHOEDEMA GUIDANCE:
 All WALES LYMPHOEDEMA GUIDANCE: Lymphoedema Vascular Assessment Policy (Toe Brachial Pressure Index / TBPI) April 2013 Created by the All Wales Lymphoedema Service Leads 1 Background The presence of peripheral
All WALES LYMPHOEDEMA GUIDANCE: Lymphoedema Vascular Assessment Policy (Toe Brachial Pressure Index / TBPI) April 2013 Created by the All Wales Lymphoedema Service Leads 1 Background The presence of peripheral
Lower Extremity Venous Disease (LEVD)
") Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Treating your leg ulcer
 Page 1 of 7 Treating your leg ulcer Introduction The information in this leaflet will answer many questions you may have about your leg ulcer. If you have any further questions about your condition or
Page 1 of 7 Treating your leg ulcer Introduction The information in this leaflet will answer many questions you may have about your leg ulcer. If you have any further questions about your condition or
GUIDELINES FOR THE MEASUREMENT OF ANKLE BRACHIAL PRESSURE INDEX USING DOPPLER ULTRASOUND
 GUIDELINES FOR THE MEASUREMENT OF ANKLE BRACHIAL PRESSURE INDEX USING DOPPLER ULTRASOUND AIM To provide evidence based principles for the measurement of Ankle Brachial Pressure Index (ABPI) using a BACKGROUND/EVIDENCE
GUIDELINES FOR THE MEASUREMENT OF ANKLE BRACHIAL PRESSURE INDEX USING DOPPLER ULTRASOUND AIM To provide evidence based principles for the measurement of Ankle Brachial Pressure Index (ABPI) using a BACKGROUND/EVIDENCE
Housekeeping 15/03/2016 URGO MEDICAL, HEALING PEOPLE. Tissue Viability information. Tissue Viability Intranet page
 TO REPAIR TO HEAL TO REPAIR TO HEAL TO LOVE TO TOUCH TO LOVE TO TOUCH TO LIVE TO MOVE TO LIVE TO MOVE TO SHARE TO CURE TO SHARE TO CURE URGO MEDICAL, HEALING PEOPLE Leg Ulcer Assessment 2016 Tissue Viability
TO REPAIR TO HEAL TO REPAIR TO HEAL TO LOVE TO TOUCH TO LOVE TO TOUCH TO LIVE TO MOVE TO LIVE TO MOVE TO SHARE TO CURE TO SHARE TO CURE URGO MEDICAL, HEALING PEOPLE Leg Ulcer Assessment 2016 Tissue Viability
Prevention and Management of Leg Ulcers
 EWMA Educational Development Programme Curriculum Development Project Education Module: Prevention and Management of Leg Ulcers Latest revision: October 2015 ABOUT THE EWMA EDUCATIONAL DEVELOPMENT PROGRAMME
EWMA Educational Development Programme Curriculum Development Project Education Module: Prevention and Management of Leg Ulcers Latest revision: October 2015 ABOUT THE EWMA EDUCATIONAL DEVELOPMENT PROGRAMME
Wound Assessment Report
 Wound Assessment Report Single Assessment, Single Wound Mary Taylor Assessment Patient ID MT4367147 Date of Birth 1939-4-18 Left Foot, Sole: Wound A Image taken 16-45-43 Area 1.7cm2 Perimeter 48mm Maximum
Wound Assessment Report Single Assessment, Single Wound Mary Taylor Assessment Patient ID MT4367147 Date of Birth 1939-4-18 Left Foot, Sole: Wound A Image taken 16-45-43 Area 1.7cm2 Perimeter 48mm Maximum
WHY WOUNDS FAIL TO HEAL SIMPLIFIED
 WHY WOUNDS FAIL TO HEAL SIMPLIFIED 10 Some of the common signs of failure to heal with possible causes and some interventions WHY WOUNDS FAIL TO HEAL There must be adequate supplies of nutrients and oxygen
WHY WOUNDS FAIL TO HEAL SIMPLIFIED 10 Some of the common signs of failure to heal with possible causes and some interventions WHY WOUNDS FAIL TO HEAL There must be adequate supplies of nutrients and oxygen
Independent evaluation of BEMER physical vascular regulation therapy
 of BEMER Liezl Naudé Advanced nurse specialist: wound management Advanced lower limb and wound management centre, Pretoria Heart 4 the Wounded 5-7 July Pretoria Introduction Lower limb wounds have always
of BEMER Liezl Naudé Advanced nurse specialist: wound management Advanced lower limb and wound management centre, Pretoria Heart 4 the Wounded 5-7 July Pretoria Introduction Lower limb wounds have always
LEG ULCERATION. BY Helen Langthorne And Emma Rayner
 LEG ULCERATION BY Helen Langthorne And Emma Rayner Definition A leg ulcer is a loss of skin below the knee on the leg or foot which takes more than six weeks to heal (CKS 2012). Venous ulcer account for
LEG ULCERATION BY Helen Langthorne And Emma Rayner Definition A leg ulcer is a loss of skin below the knee on the leg or foot which takes more than six weeks to heal (CKS 2012). Venous ulcer account for
Case study: Young athlete suffering from PTS recovers from traumatic foot ulcer, following use of the geko TM device.
 Case study: Young athlete suffering from PTS recovers from traumatic foot ulcer, following use of the geko TM device.... Subject 34-year-old male, ex professional rugby player. Wound Type Lower left leg
Case study: Young athlete suffering from PTS recovers from traumatic foot ulcer, following use of the geko TM device.... Subject 34-year-old male, ex professional rugby player. Wound Type Lower left leg
AWMA MODULE ACCREDITATION. Module Three: Assessment and Management of Lower Leg Ulceration
 AWMA MODULE ACCREDITATION Module Three: Assessment and Management of Lower Leg Ulceration Introduction - The Australian Wound Management Association Education & Professional Development Sub Committee-(AWMA
AWMA MODULE ACCREDITATION Module Three: Assessment and Management of Lower Leg Ulceration Introduction - The Australian Wound Management Association Education & Professional Development Sub Committee-(AWMA
Latmedical, LLC is the exclusive Caribbean distributor
 No-Varix Graduated Compression Hosiery is manufactured by TEXPON S.A., the only Latin- American company certified with the norm ISO 9001:00 with scope of manufacture of graduate compression hosiery for
No-Varix Graduated Compression Hosiery is manufactured by TEXPON S.A., the only Latin- American company certified with the norm ISO 9001:00 with scope of manufacture of graduate compression hosiery for
Lower Leg Ulceration. Wendy McInnes Vascular Nurse Practitioner; Northern Adelaide Local Health Network;
 Lower Leg Ulceration Wendy McInnes Vascular Nurse Practitioner; Northern Adelaide Local Health Network; wendy.mcinnes@sa.gov.au 0447 051 036 1 Lower Leg Ulceration A manifestation of underlying pathology/disease
Lower Leg Ulceration Wendy McInnes Vascular Nurse Practitioner; Northern Adelaide Local Health Network; wendy.mcinnes@sa.gov.au 0447 051 036 1 Lower Leg Ulceration A manifestation of underlying pathology/disease
Wound Jeopardy: Name That Wound Session 142 Saturday, September 10 th 2011
 Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
4-layer compression bandaging system (includes microbe binding wound contact layer) Latex-free, 4-layer compression bandaging system
 Latex-free, 4-layer compression bandaging system") JOBST Comprifore JOBST Comprifore at a glance: provides effective levels of sustained graduated compression provides built in safety and ease of application Insures compliance and maximum healing for cost
JOBST Comprifore JOBST Comprifore at a glance: provides effective levels of sustained graduated compression provides built in safety and ease of application Insures compliance and maximum healing for cost
Assessment & Management of Wounds in primary practice.
 Assessment & Management of Wounds in primary practice. Nutrition Successful wound management depends on appropriate nutritional support. Poor nutrition is recognised as one of the major causes of poor
Assessment & Management of Wounds in primary practice. Nutrition Successful wound management depends on appropriate nutritional support. Poor nutrition is recognised as one of the major causes of poor
Leg ulcers. Causes and management. OBJECTIVE This article outlines the assessment and management of patients with leg ulceration.
 THEME Wounds Leg ulcers Causes and management BACKGROUND A leg ulcer is not a disease but the manifestation of an underlying problem that requires a clear diagnosis. Sandra Dean RN, is nurse consultant
THEME Wounds Leg ulcers Causes and management BACKGROUND A leg ulcer is not a disease but the manifestation of an underlying problem that requires a clear diagnosis. Sandra Dean RN, is nurse consultant
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
RADIOFREQUENCY ABLATION. Professor M Baguneid MB ChB MD FRCS
 RADIOFREQUENCY ABLATION This minimally invasive treatment involves closing the faulty veins using a keyhole approach thereby avoiding the larger cuts and avoiding stripping of the veins. Professor M Baguneid
RADIOFREQUENCY ABLATION This minimally invasive treatment involves closing the faulty veins using a keyhole approach thereby avoiding the larger cuts and avoiding stripping of the veins. Professor M Baguneid
ULCERS 1/12/ million diabetics in the US (2012) Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years
 Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years") Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Priorities Forum Statement
 Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
How varicose veins occur
 Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
Varicose veins are a very common problem, generally appearing as twisting, bulging rope-like cords on the legs, anywhere from groin to ankle. Spider veins are smaller, flatter, red or purple veins closer
DRESSING SELECTION. Rebecca Aburn MN NP Candidate
 DRESSING SELECTION Rebecca Aburn MN NP Candidate Should be individually tailored in conjunction with the patient to meet their individual needs. WOUND MANAGEMENT: Comprehensive health assessment Wound
DRESSING SELECTION Rebecca Aburn MN NP Candidate Should be individually tailored in conjunction with the patient to meet their individual needs. WOUND MANAGEMENT: Comprehensive health assessment Wound
Sores That Will Not Heal
 Sores That Will Not Heal Introduction Some sores have trouble healing on their own. Sores that will not heal are a common problem. Open sores that will not heal are also known as wounds or skin ulcers.
Sores That Will Not Heal Introduction Some sores have trouble healing on their own. Sores that will not heal are a common problem. Open sores that will not heal are also known as wounds or skin ulcers.
How to manage leg ulcers in the elderly
 How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
Case study: A targeted approach to healing complex wounds using the geko device.
 Case study: A targeted approach to healing complex wounds using the geko device. Authors: Mr Sameh Dimitri Consultant Vascular and Endovascular Surgeon MSc FRCS (Eng Edin) Nikki Pavey Physiotherapist at
Case study: A targeted approach to healing complex wounds using the geko device. Authors: Mr Sameh Dimitri Consultant Vascular and Endovascular Surgeon MSc FRCS (Eng Edin) Nikki Pavey Physiotherapist at
Healthy Legs For Life! Prevention is better then cure
 Healthy Legs For Life! Prevention is better then cure Ellie Lindsay Independent Specialist Practitioner Associate Lecturer, CRICP, London Visiting Fellow, Queensland University of Technology Occurrence
Healthy Legs For Life! Prevention is better then cure Ellie Lindsay Independent Specialist Practitioner Associate Lecturer, CRICP, London Visiting Fellow, Queensland University of Technology Occurrence
Wound Classification. Overview
 Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Take 5 - Imagine these legs are yours.
 HOLISTIC ASSESSMENT Take 5 - Imagine these legs are yours. Take a minute to imagine how they would impact on; - Your life at home - Your relationships partner, children - Your job - How you feel about
HOLISTIC ASSESSMENT Take 5 - Imagine these legs are yours. Take a minute to imagine how they would impact on; - Your life at home - Your relationships partner, children - Your job - How you feel about
Deep Vein Thrombosis
 Deep Vein Thrombosis Introduction Deep vein thrombosis (DVT) is a blood clot in a vein. This condition can affect men and women of any age and race. DVT is a potentially serious condition. If not treated,
Deep Vein Thrombosis Introduction Deep vein thrombosis (DVT) is a blood clot in a vein. This condition can affect men and women of any age and race. DVT is a potentially serious condition. If not treated,
Venous Leg Ulcers. Care for Patients in All Settings
 Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Additional Information S-55
 Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Venous. Arterial. Neuropathic (e.g. diabetic foot ulcer) Describe Wound Types & Stages of. Pressure Ulcers. Identify Phases of Healing & Wound Care
 Describe Wound Types & Stages of. Pressure Ulcers. Identify Phases of Healing & Wound Care") A dressing the situation at hand Describe Wound Types & Stages of Pressure Ulcers Identify Phases of Healing & Wound Care Goals Clarify Referral Protocol Lacerations- The goal is nearest to complete approximation
A dressing the situation at hand Describe Wound Types & Stages of Pressure Ulcers Identify Phases of Healing & Wound Care Goals Clarify Referral Protocol Lacerations- The goal is nearest to complete approximation
Wound Healing Community Outreach Service
 Wound Healing Community Outreach Service Wound Management Education Plan January 2011 December 2011 Author: Michelle Gibb Nurse Practitioner Wound Management Wound Healing Community Outreach Service Institute
Wound Healing Community Outreach Service Wound Management Education Plan January 2011 December 2011 Author: Michelle Gibb Nurse Practitioner Wound Management Wound Healing Community Outreach Service Institute
Arterial & Venous Ulcers. A Comprehensive Review Assessment & Management
 Arterial & Venous Ulcers A Comprehensive Review Assessment & Management 1 Objectives Understand Arterial & Venous disease Understand the etiology of lower extremities ulcers Understand assessment of lower
Arterial & Venous Ulcers A Comprehensive Review Assessment & Management 1 Objectives Understand Arterial & Venous disease Understand the etiology of lower extremities ulcers Understand assessment of lower
Determine the patients relative risk of thrombosis. Be confident that you have had a meaningful discussion with the patient.
 Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
AN INTRODUCTION TO DOPPLER. Sarah Gardner, Clinical lead, Tissue viability service. Oxford Health NHS Foundation Trust.
 AN INTRODUCTION TO DOPPLER Sarah Gardner, Clinical lead, Tissue viability service. Oxford Health NHS Foundation Trust. THE DOPPLER EFFECT The Doppler Principle was described by Physicist and mathematician
AN INTRODUCTION TO DOPPLER Sarah Gardner, Clinical lead, Tissue viability service. Oxford Health NHS Foundation Trust. THE DOPPLER EFFECT The Doppler Principle was described by Physicist and mathematician
Leg Ulcer Case Study
 Leg Ulcer Case Study Wound Healing Community Outreach Service Mrs Ivy Hurtzalot, a 71-year-old lady, presents to her general practitioner with an ulcer on her right medial malleolus. Ivy reveals that the
Leg Ulcer Case Study Wound Healing Community Outreach Service Mrs Ivy Hurtzalot, a 71-year-old lady, presents to her general practitioner with an ulcer on her right medial malleolus. Ivy reveals that the
Dr Peter Chapman-Smith
 Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Managing venous leg ulcers and oedema using compression hosiery
 Managing venous leg ulcers and oedema using compression hosiery Tickle J (2015) Managing venous leg ulcers and oedema using compression hosiery. Nursing Standard. 30, 8, 57-63. Date of submission: July
Managing venous leg ulcers and oedema using compression hosiery Tickle J (2015) Managing venous leg ulcers and oedema using compression hosiery. Nursing Standard. 30, 8, 57-63. Date of submission: July
Blood flows away from the heart in arteries, to the capillaries and back to the heart in the veins
 Cardiovascular System Summary Notes The cardiovascular system includes: The heart, a muscular pump The blood, a fluid connective tissue The blood vessels, arteries, veins and capillaries Blood flows away
Cardiovascular System Summary Notes The cardiovascular system includes: The heart, a muscular pump The blood, a fluid connective tissue The blood vessels, arteries, veins and capillaries Blood flows away
Your guide to wound debridement and assessment. Michelle Greenwood. Lorraine Grothier. Lead Nurse, Tissue Viability, Walsall Healthcare NHS Trust
 Your guide to wound debridement and assessment Michelle Greenwood Lead Nurse, Tissue Viability, Walsall Healthcare NHS Trust Lorraine Grothier Clinical Nurse Specialist, Tissue Viability, Central Essex
Your guide to wound debridement and assessment Michelle Greenwood Lead Nurse, Tissue Viability, Walsall Healthcare NHS Trust Lorraine Grothier Clinical Nurse Specialist, Tissue Viability, Central Essex
Ch. 12 The Circulatory System. The heart. The heart is a double pump. A quick note on arteries vs. veins. = the muscular pump of the CV system
 Ch. 12 The Circulatory System The heart A.k.a. the cardiovascular system Blood was discussed in Ch. 11 Focus of Ch. 12: heart and blood vessels = the muscular pump of the CV system ~ 100,000 heartbeats/day!
Ch. 12 The Circulatory System The heart A.k.a. the cardiovascular system Blood was discussed in Ch. 11 Focus of Ch. 12: heart and blood vessels = the muscular pump of the CV system ~ 100,000 heartbeats/day!
lipodermatosclerosis standards of medical practitioners and the quality of patient care related to the treatment of venous disorders.
 Chattanooga s premiere VEIN CENTER Update on Venous Insufficiency, Varicose and Spider Veins 2016 Vincent W. Gardner, MD, FACS, RPVI Fellow, American College of Surgeons Board Certified, American Board
Chattanooga s premiere VEIN CENTER Update on Venous Insufficiency, Varicose and Spider Veins 2016 Vincent W. Gardner, MD, FACS, RPVI Fellow, American College of Surgeons Board Certified, American Board
CLINICAL PROTOCOL - VENOUS LEG ULCER MANAGEMENT. SCOPE: Western Australia. Clinical Protocol for Venous Leg Ulcer Management
 CLINICAL PROTOCOL - VENOUS LEG ULCER MANAGEMENT SCOPE: Western Australia Clinical Protocol for Venous Leg Ulcer The following protocol outlines the sequence of events in the assessment and management of
CLINICAL PROTOCOL - VENOUS LEG ULCER MANAGEMENT SCOPE: Western Australia Clinical Protocol for Venous Leg Ulcer The following protocol outlines the sequence of events in the assessment and management of
Supporting Information Leaflet (11): Managing Oedema and Circulatory Problems in Neuromuscular Disorders
: Managing Oedema and Circulatory Problems in Neuromuscular Disorders") Supporting Information Leaflet (11): Managing Oedema and Circulatory Problems in Neuromuscular Disorders Oedema, sometimes known as Lymphoedema or fluid retention is the build up of fluid and other elements
Supporting Information Leaflet (11): Managing Oedema and Circulatory Problems in Neuromuscular Disorders Oedema, sometimes known as Lymphoedema or fluid retention is the build up of fluid and other elements
Dr Paul Thibault. Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology
 Australasian College of Phlebology") Dr Paul Thibault Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology Prescribing Effective Compression and PTS Dr Paul Thibault Phlebologist, Newcastle,
Dr Paul Thibault Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology Prescribing Effective Compression and PTS Dr Paul Thibault Phlebologist, Newcastle,
New Guideline in venous ulcer treatment: dressing, medication, intervention
 New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
GP Practice Woundcare Formulary
 Agreed jointly by Ipswich and East Suffolk and West Suffolk Clinical Commissioning Groups GP Practice Woundcare Formulary Version 28 October 2017 Formulary items should be prescribed wherever possible.
Agreed jointly by Ipswich and East Suffolk and West Suffolk Clinical Commissioning Groups GP Practice Woundcare Formulary Version 28 October 2017 Formulary items should be prescribed wherever possible.
Unit 1: Human Systems. The Circulatory System
 Unit 1: Human Systems The Circulatory System nourish all cells with oxygen, glucose, amino acids and other nutrients and carry away carbon dioxide, urea and other wastes Purposes Transport chemical messengers
Unit 1: Human Systems The Circulatory System nourish all cells with oxygen, glucose, amino acids and other nutrients and carry away carbon dioxide, urea and other wastes Purposes Transport chemical messengers
Advazorb. Hydrophilic foam dressing range
 Advazorb Hydrophilic foam dressing range Advazorb A comprehensive range of patient friendly, absorbent foam dressings Non-adhesive and atraumatic silicone adhesive options Designed to manage exudate whilst
Advazorb Hydrophilic foam dressing range Advazorb A comprehensive range of patient friendly, absorbent foam dressings Non-adhesive and atraumatic silicone adhesive options Designed to manage exudate whilst
Wound debridement: guidelines and practice to remove barriers to healing
 Wound debridement: guidelines and practice to remove barriers to healing Learning objectives 1. The burden of wounds and the impact to the NHS 2. Understand what debridement is and why it is needed 3.
Wound debridement: guidelines and practice to remove barriers to healing Learning objectives 1. The burden of wounds and the impact to the NHS 2. Understand what debridement is and why it is needed 3.
Recurrent varicose veins. Information for patients Sheffield Vascular Institute
 Recurrent varicose veins Information for patients Sheffield Vascular Institute You have been diagnosed as having varicose veins that have recurred (come back). This leaflet explains more about recurrent
Recurrent varicose veins Information for patients Sheffield Vascular Institute You have been diagnosed as having varicose veins that have recurred (come back). This leaflet explains more about recurrent
DRESSING SELECTION SIMPLIFIED
 10 DRESSING SELECTION SIMPLIFIED It must be recognised that no one dressing provides the optimum environment for the healing of all wounds (Mahoney, 2015) DRESSING SELECTION SIMPLIFIED Selecting the correct
10 DRESSING SELECTION SIMPLIFIED It must be recognised that no one dressing provides the optimum environment for the healing of all wounds (Mahoney, 2015) DRESSING SELECTION SIMPLIFIED Selecting the correct
Velcro Compression Devices
 Velcro Compression Devices Joseph A. Caprini, MD, MS, FACS, RVT, FACCWS Louis W. Biegler Chair of Surgery NorthShore University HealthSystem, Evanston, IL Clinical Professor of Surgery University of Chicago
Velcro Compression Devices Joseph A. Caprini, MD, MS, FACS, RVT, FACCWS Louis W. Biegler Chair of Surgery NorthShore University HealthSystem, Evanston, IL Clinical Professor of Surgery University of Chicago
VeinOPlus Vascular Peripheral Vascular & Wound Therapy Device
 VeinOPlus Vascular Peripheral Vascular & Wound Therapy Device Calf Muscle Pump Dysfunction Therapy Increases blood flow, accelerates wound healing, and improves CVD and PAD symptoms Tomorrow s Technology
VeinOPlus Vascular Peripheral Vascular & Wound Therapy Device Calf Muscle Pump Dysfunction Therapy Increases blood flow, accelerates wound healing, and improves CVD and PAD symptoms Tomorrow s Technology
West Gloucestershire Primary Care Trust Community Nursing Service. Leg Ulcer Audit. Gloucestershire Primary & Community Care Audit Group
 West Gloucestershire Primary Care Trust Community Nursing Service Leg Ulcer Audit 2006 Gloucestershire Primary & Community Care Audit Group Contents Page number Background 3 Audit Aims 4 Methodology 4
West Gloucestershire Primary Care Trust Community Nursing Service Leg Ulcer Audit 2006 Gloucestershire Primary & Community Care Audit Group Contents Page number Background 3 Audit Aims 4 Methodology 4
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
Welcome to Allied Health Telehealth
 Welcome to Allied Health Telehealth Paediatric lymphoedema A challenge for clinicians and families To receive an attendance certificate please complete your online evaluation at: https://www.surveymonkey.com/s/paedlymphoedema
Welcome to Allied Health Telehealth Paediatric lymphoedema A challenge for clinicians and families To receive an attendance certificate please complete your online evaluation at: https://www.surveymonkey.com/s/paedlymphoedema
End Diastolic Pneumatic Compression Boot as a Treatment of Peripheral Vascular Disease or Lymphedema. Original Policy Date
 MP 2.02.12 End Diastolic Pneumatic Compression Boot as a Treatment of Peripheral Vascular Disease or Lymphedema Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
MP 2.02.12 End Diastolic Pneumatic Compression Boot as a Treatment of Peripheral Vascular Disease or Lymphedema Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
JoyTickle, Tissue Viability Nurse Specialist, Shropshire Community Health NHS Trust
 Lower limb Ulceration Pathway: Leanne Atkin, Lecturer practitioner/vascular Nurse Specialist, School of Human and Health Sciences, University of Huddersfield and Mid Yorkshire NHS Trust, E mail: l.atkin@hud.ac.uk
Lower limb Ulceration Pathway: Leanne Atkin, Lecturer practitioner/vascular Nurse Specialist, School of Human and Health Sciences, University of Huddersfield and Mid Yorkshire NHS Trust, E mail: l.atkin@hud.ac.uk
Types of circulatory systems
 Types of circulatory systems Open system Mostly invertebrates Low pressure Haemocoel Suitable for small organisms Closed system Vertebrates High pressure Blood remains in blood vessels Separate tissue
Types of circulatory systems Open system Mostly invertebrates Low pressure Haemocoel Suitable for small organisms Closed system Vertebrates High pressure Blood remains in blood vessels Separate tissue
Wound Management Capital Health Network Practice Nurses 20 Feb 2018
 Wound Management Capital Health Network Practice Nurses 20 Feb 2018 ) MNP Judith Barker RN; NP; STN; B Hlth Sc (Nurs); MN (NP) Nurse Practitioner Wound Management Rehabilitation, Aged & Community Care
Wound Management Capital Health Network Practice Nurses 20 Feb 2018 ) MNP Judith Barker RN; NP; STN; B Hlth Sc (Nurs); MN (NP) Nurse Practitioner Wound Management Rehabilitation, Aged & Community Care
Varicose Vein Cyanoacrylate Glue treatment
 The South West s premier independent healthcare and cosmetic clinic Varicose Vein Cyanoacrylate Glue treatment Varicose veins are a sign of underlying venous insufficiency and affect 20 30% of adults.
The South West s premier independent healthcare and cosmetic clinic Varicose Vein Cyanoacrylate Glue treatment Varicose veins are a sign of underlying venous insufficiency and affect 20 30% of adults.
Compression Bandaging Formulary 2017
 Area Drugs Therapeutics Committee Compression Bandaging Formulary 2017 Compression Bandaging Formulary 2017 Developed by the NHS Fife Wound and Skin Care Forum (WSCF) Group Approved: October 2017 Review:
Area Drugs Therapeutics Committee Compression Bandaging Formulary 2017 Compression Bandaging Formulary 2017 Developed by the NHS Fife Wound and Skin Care Forum (WSCF) Group Approved: October 2017 Review:
EDUCATION. Peripheral Artery Disease
 EDUCATION Peripheral Artery Disease Peripheral Artery Disease You may have circulation problems that have to do with your blood vessels. You may feel aches, pains, cramps, numbness or muscle fatigue when
EDUCATION Peripheral Artery Disease Peripheral Artery Disease You may have circulation problems that have to do with your blood vessels. You may feel aches, pains, cramps, numbness or muscle fatigue when
Interactive Learning Session
 Chronic Venous Disease - Part I Interactive Learning Session 2011 Ali Sabbour Prof of Vascular Surgery http://mic.shams.edu.eg/moodle6 Login as a guest Surgery 2 Ali Sabbour - Chronic Venous Disease Intended
Chronic Venous Disease - Part I Interactive Learning Session 2011 Ali Sabbour Prof of Vascular Surgery http://mic.shams.edu.eg/moodle6 Login as a guest Surgery 2 Ali Sabbour - Chronic Venous Disease Intended
VENOUS LEG ULCERS (VLU)
") VENOUS LEG ULERS (VLU) REOMMENDTION S Evidence-based gradings Excellent evidence ody of evidence can be trusted to guide practice. Good evidence ody of evidence can be trusted to guide practice in most
VENOUS LEG ULERS (VLU) REOMMENDTION S Evidence-based gradings Excellent evidence ody of evidence can be trusted to guide practice. Good evidence ody of evidence can be trusted to guide practice in most
The Triangle of Wound Assessment
 The Triangle of Wound Assessment A simple and holistic framework for wound management CPWSC_TOWA_Brochure_210x210_2018.indd 1 10/01/2018 15.13 ? We asked healthcare professionals around the world about
The Triangle of Wound Assessment A simple and holistic framework for wound management CPWSC_TOWA_Brochure_210x210_2018.indd 1 10/01/2018 15.13 ? We asked healthcare professionals around the world about
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) GUIDELINES FOR THE USE OF COMPRESSION HOSIERY
 GUIDELINES FOR THE USE OF COMPRESSION HOSIERY") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) GUIDELINES FOR THE USE OF COMPRESSION HOSIERY Do not include made to measure on the prescription; the community pharmacy/dispensing practice will endorse
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) GUIDELINES FOR THE USE OF COMPRESSION HOSIERY Do not include made to measure on the prescription; the community pharmacy/dispensing practice will endorse
Topic 6: Human Physiology
 Topic 6: Human Physiology 6.2 The Blood System D.4 The Heart Essential Questions: 6.2 The blood system continuously transports substances to cells and simultaneously collects waste products. D.3 The chemical
Topic 6: Human Physiology 6.2 The Blood System D.4 The Heart Essential Questions: 6.2 The blood system continuously transports substances to cells and simultaneously collects waste products. D.3 The chemical
Ligation with Stripping
 Ligation with Stripping Understanding Problem Leg Veins Do your legs feel tired and achy at the end of the day? Have you stopped wearing shorts because you don t like the way your legs look? Vein problems
Ligation with Stripping Understanding Problem Leg Veins Do your legs feel tired and achy at the end of the day? Have you stopped wearing shorts because you don t like the way your legs look? Vein problems
Compression therapy can
 What are the benefits of using cohesive inelastic compression bandages in the community? Compression therapy can play a vital role in improving the quality of life for those with chronic venous insufficiency,
What are the benefits of using cohesive inelastic compression bandages in the community? Compression therapy can play a vital role in improving the quality of life for those with chronic venous insufficiency,
Ch 9 Transport of substances in humans
 Ch 9 Transport of substances in humans Think about (Ch 9, p.2) 1. Blood transports various substances and distributes heat around the body. It also plays a role in body defence. 2. Blood is a liquid tissue
Ch 9 Transport of substances in humans Think about (Ch 9, p.2) 1. Blood transports various substances and distributes heat around the body. It also plays a role in body defence. 2. Blood is a liquid tissue
Varicose Veins: A guide for patients
 Varicose Veins: A guide for patients Varicose Veins: A guide for patients What are varicose veins? Varicose veins are swollen, twisted and unsightly veins (usually on the legs) that look lumpy and bluish
Varicose Veins: A guide for patients Varicose Veins: A guide for patients What are varicose veins? Varicose veins are swollen, twisted and unsightly veins (usually on the legs) that look lumpy and bluish
Address: Left Leg. other: Nails: thick yellow brittle fungus abnormal thick yellow brittle fungus abnormal
 South West Regional Wound Care Toolkit: Interdisciplinary Lower Leg Assessment Form Instructions for use: Competent/ Proficient/ Expert level HCP to complete if lower leg ulcer present or risk of ulcer
South West Regional Wound Care Toolkit: Interdisciplinary Lower Leg Assessment Form Instructions for use: Competent/ Proficient/ Expert level HCP to complete if lower leg ulcer present or risk of ulcer
Venous Insufficiency Ulcer
 Disclosure NOTHING Venous Insufficiency Ulcer Venous Insufficiency Ulcer Also know as Venous Stasis Ulcer Ulcerative Venous Reflux Disease Statistics / Clinical Frequency Affects 2-5 % of the population
Disclosure NOTHING Venous Insufficiency Ulcer Venous Insufficiency Ulcer Also know as Venous Stasis Ulcer Ulcerative Venous Reflux Disease Statistics / Clinical Frequency Affects 2-5 % of the population
KINESIOLOGY TAPING GUIDE
 KINESIOLOGY TAPING GUIDE What is Kinesiology tape and how does Kinesiology tape work? How to apply Kinesiology tape Examples of application of UP Kinesiology tape for common injuries and conditions Introduction
KINESIOLOGY TAPING GUIDE What is Kinesiology tape and how does Kinesiology tape work? How to apply Kinesiology tape Examples of application of UP Kinesiology tape for common injuries and conditions Introduction
COMMISSIONING POLICY
 Ref No. 1a7.5 COMMISSIONING POLICY Surgery for venous disease of the leg (Varicosities of the Long Saphenous Vein) April 2011 CONTENTS Section Page Summary 2 1. Background 2 2. Criteria for eligibility
Ref No. 1a7.5 COMMISSIONING POLICY Surgery for venous disease of the leg (Varicosities of the Long Saphenous Vein) April 2011 CONTENTS Section Page Summary 2 1. Background 2 2. Criteria for eligibility
Blood Flow and Blood Pressure Regulation *
 OpenStax-CNX module: m44806 1 Blood Flow and Blood Pressure Regulation * OpenStax This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 By the end of this
OpenStax-CNX module: m44806 1 Blood Flow and Blood Pressure Regulation * OpenStax This work is produced by OpenStax-CNX and licensed under the Creative Commons Attribution License 4.0 By the end of this
Outcomes: By the end of this session the student will be able to:
 Outcomes: By the end of this session the student will be able to: Discuss the cardiovascular system Identify the normal changes that occur with ageing Explain the nurses role in the care of residents with
Outcomes: By the end of this session the student will be able to: Discuss the cardiovascular system Identify the normal changes that occur with ageing Explain the nurses role in the care of residents with
Occasional pain or other discomfort (ie, not restricting regular daily activity)
") Revised Venous Clinical Severity Score Pain : 0 Mild: 1 or other discomfort (ie, aching, heaviness, fatigue, soreness, burning) Occasional pain or other discomfort (ie, not restricting regular daily activity)
Revised Venous Clinical Severity Score Pain : 0 Mild: 1 or other discomfort (ie, aching, heaviness, fatigue, soreness, burning) Occasional pain or other discomfort (ie, not restricting regular daily activity)
UNDERSTANDING VEIN PROBLEMS
 UNDERSTANDING VEIN PROBLEMS Varicose Veins, Chronic Venous Insufficiency, and DVT Do You Have a Vein Problem? Have you noticed pain or swelling in your legs? Do your symptoms worsen when you re sitting
UNDERSTANDING VEIN PROBLEMS Varicose Veins, Chronic Venous Insufficiency, and DVT Do You Have a Vein Problem? Have you noticed pain or swelling in your legs? Do your symptoms worsen when you re sitting
Circulatory System 10.1
 1 Circulatory System 10.1 2 ARTERIES Arteries-blood vessels that carry blood away from the heart Thick walls Inner & Outer layers: connective tissue Middle layers are muscle and elastic connective tissue
1 Circulatory System 10.1 2 ARTERIES Arteries-blood vessels that carry blood away from the heart Thick walls Inner & Outer layers: connective tissue Middle layers are muscle and elastic connective tissue