Management of the Open Abdomen
|
|
|
- Alfred Peters
- 6 years ago
- Views:
Transcription
1 Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen How did we get here? abdominal compartment syndrome damage control surgery staged laparotomy for general surgery Temporary closure ICU considerations Attaining fascial closure Complications Abdominal Compartment Syndrome 1 ACS - due to abdominal injury/condition major solid organ injury perforated viscus ruptured AAA bowel obstruction postoperative hemorrhage Burch et al. Surg Clin North Am 1996 Ivatury et al. J Trauma 1998 Meldrum et al. Am J Surg 1997 Raeburn et al. Am J Surg 2001 Balogh et al. Am J Surg 2002 Balogh et al. Arch Surg 2003

2 Abdominal Compartment Syndrome 2 ACS - develops during resuscitation aggressive fluid resuscitation - iatrogenic massive transfusion sepsis and capillary leak pancreatitis Burch et al. Surg Clin North Am 1996 Ivatury et al. J Trauma 1998 Meldrum et al. Am J Surg 1997 Raeburn et al. Am J Surg 2001 Balogh et al. Am J Surg 2002 Balogh et al. Arch Surg 2003 ACS: Physiology INCREASED ABDOMINAL PRESSURE ICP compression of kidneys venous return intrathoracic pressure renal blood flow UOP extremity ischemia SV CO SVR splanchnic ischemia hypoxemia airway pressures compliance PA pressures CVP readings PITFALL Physical exam is NOT reliable!
3 ACS: Diagnosis Bladder pressure: 3-way foley installation of 50cc of saline into the bladder manometer at level of pubic symphysis measure pressure in cm of H 2 0 Kron et al. Ann Surg 1984 PITFALL bladder pressure intraabdominal pressure - pelvic packing - bladder rupture - neurogenic bladder - adhesions -? unparalyzed patient KEY POINT ACS = bladder pressure AND deranged physiology urine output cardiac output airway pressures ICP If the patient has ACS DECOMPRESS!!







4 ACS: Decompression Options Formal Operative Decompression ACS: Decompression Options Bedside Decompression in the ICU Bringing the OR to the SICU Even the MICU ACS: Decompression Options Decompression via drainage of ascites bedside ultrasound perc drain placement Reed et al. J Trauma 2006 Parra et al. J Trauma 2006


5 PITFALL Just because the abdomen is open doesn t mean they don t have ACS! Damage Control Surgery Abbreviated operation: control hemorrhage limit contamination Indications: hypothermia (T < 35 ) acidosis (ph < 7.2, base def > 15) coagulopathy (PT/PTT > 50% nl) Stone et al. J Trauma 1983 Rotondo et al. J Trauma 1993 Damage Control General Surgery Similar principles: control hemorrhage limit contamination Shorten operation and resuscitate patient in the SICU
6 KEY POINT If in doubt, leave the abdomen open. KEY POINT Open abdomens are temporary*. * in the vast majority of cases. Now What?




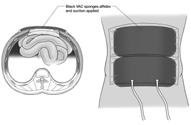
7 Temporary Option #1 Towel clip closure rapid technique skin only limits angiography may develop ACS Trial closure minutes in OR empty urimeter measure output blood products check for surgical bleeding Temporary Option #2 Bogotá bag closure temporary silo 3L sterile GU irrigation bag sewn to skin contains the edematous bowel no issues with angiography suturing - time consuming Temporary Option # drape & ioban closure temporary covering no issues with angiography less time consuming

8 ICU Management General principles: goal directed resuscitation transfusion therapy lung protective ventilation limit hyperglycemia Abdomen specific principles: fluid balance nutrition support management of bowel injuries ICU Management: Fluid Management Correction of acidosis/lactate vs flooding with fluid Crystalloid vs colloid Do not create a hyperchloremic metabolic acidosis Target O 2 delivery = 500 ml/min/m 2 Consider lasix drip once resuscitated Moore et al. J Trauma 2006 McKinley et al. J Trauma 2002 ICU Management: Nutrition Support Benefit of enteral nutrition septic complications Understandable hesitation edematous bowel associated injuries Enteral access possible Moore et al. J Trauma 1986 Cothren et al. Am J Surg 2005
9 ICU Management: Nutrition Support Enteral nutrition is feasible May decrease time to fascial closure Decreased rate of pneumonia Increase the protein given?? Collier et al. JPEN 2007 Dissanaike et al. JACS 2008 Cheatham et al. Crit Care Med 2007 Cothren et al. Am J Surg 2005 Management of Bowel Injuries WTA multicenter study 10 institutions 204 patients Overall Leak Rate Small Bowel (n = 62) Right Colon (n = 38) Transverse Colon (n = 5) Left Colon (n = 22) 2/62 (3%) 1/38 (3%) 1/5 (20%) 10/22 (45%) Burlew et al. J Trauma 2011 Management of Bowel Injuries % with leak Incidence of leak by closure day R 2 = Closure Day % with leak Incidence of leak by closure day Chi-sq p= <5 days >=5 days Closure Day Higher incidence of leak with closure day Fascia closure day 5 had a 4 times higher likelihood of developing leak

10 ICU Management: Other Considerations Peritoneal resuscitation: dialysis solution flushed directly into abdomen increased blood flow, decreased bowel edema increased fascial closure rates Neuromuscular blockade: increased primary fascial closure Garrison et al. JACS 2010 Abouassaly et al. J Trauma 2010 Open Abdomen Management How do we go from: To: The Goal: Fascial Closure Early primary closure Prosthetic fascia (foreign vs biologic) Skin grafting and delayed repair Sequential fascial closure


11 Closure Options Early fascial closure able to close primarily at repeat exploration Mesh options prosthetic mesh foreign body infection/fistula risk biologic mesh incorporated by fibroblasts longterm similar to native fascia resistant to infection eventration fascial closure biologic mesh closure Skin Grafting temporary coverage granulation tissue over bowel STSG covers bowel 9 months later loose covering PITFALL Don t screw up the fascia think twice about feeding tubes Place stomas FAR lateral No exposed suture lines Warn the patient it takes a year








12 Sequential Fascial Closure Sequential Fascial Closure Sequential Fascial Closure



13 Sequential Fascial Closure CLOSED!! Rejoicing residents Abdominal Complications Intraabdominal abscess Enterocutaneous fistula Enteroatmospheric fistula abscess EA fistula split open STSG The Open Abdomen: Summary Open abdomens do save lives - abdominal compartment syndrome - damage control surgery ICU principles continue to evolve Temporary closure should be: - fast, covering, angio compatible Autologous tissue is the ideal closure
14 The Open Abdomen?
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Difficult Abdominal Closure. Mark A. Carlson, MD
 Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Emergency Laparotomy. Open vs Closed Abdomen
 Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
The Abdominal Compartment Syndrome
 The Abdominal Compartment Syndrome Andre R. Campbell, MD, FACS, FACP, FCCM Professor of Surgery, UCSF Endowed Chair of Surgical Education San Francisco General Hospital Outline Case presentations Review
The Abdominal Compartment Syndrome Andre R. Campbell, MD, FACS, FACP, FCCM Professor of Surgery, UCSF Endowed Chair of Surgical Education San Francisco General Hospital Outline Case presentations Review
One hundred percent fascial approximation with sequential abdominal closure of the open abdomen
 The American Journal of Surgery 192 (2006) 238 242 HowIdoit One hundred percent fascial approximation with sequential abdominal closure of the open abdomen C. Clay Cothren, M.D. a,b, *, Ernest E. Moore,
The American Journal of Surgery 192 (2006) 238 242 HowIdoit One hundred percent fascial approximation with sequential abdominal closure of the open abdomen C. Clay Cothren, M.D. a,b, *, Ernest E. Moore,
Open abdomen in trauma. Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland
 Open abdomen in trauma Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland Frequency and causes of open abdomen - in 23% (344/1531) after trauma laparotomies - damage control
Open abdomen in trauma Ari Leppäniemi Abdominal Center Meilahti hospital University of Helsinki Finland Frequency and causes of open abdomen - in 23% (344/1531) after trauma laparotomies - damage control
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Chapter 2 Damage Control
 Chapter 2 Damage Control Rona E. Altaras, Firas G. Madbak and Dale A. Dangleben History Originally a naval term, damage control (DC) is a simple and useful idea referring to the ability of a battleship
Chapter 2 Damage Control Rona E. Altaras, Firas G. Madbak and Dale A. Dangleben History Originally a naval term, damage control (DC) is a simple and useful idea referring to the ability of a battleship
DAMAGE CONTROL. Outline. Definition 5/29/2014. No Disclosures
 DAMAGE CONTROL No Disclosures Rochelle A. Dicker, MD Associate Professor of Surgery and Anesthesia University of California, San Francisco Definition Term used in the Merchant Marines and in Navies for
DAMAGE CONTROL No Disclosures Rochelle A. Dicker, MD Associate Professor of Surgery and Anesthesia University of California, San Francisco Definition Term used in the Merchant Marines and in Navies for
Abdominal V.A.C. Therapy in Trauma
 Abdominal V.A.C. Therapy in Trauma Stefaan Nijs, M.D., Ph.D. Mathieu D Hondt, M.D. Dept Abdominal Surgery UZ Leuven 1 2 Damage control = naval technique Damage Control in Trauma 3 USS Nevada 4 In extremis
Abdominal V.A.C. Therapy in Trauma Stefaan Nijs, M.D., Ph.D. Mathieu D Hondt, M.D. Dept Abdominal Surgery UZ Leuven 1 2 Damage control = naval technique Damage Control in Trauma 3 USS Nevada 4 In extremis
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Bogota-VAC A Newly Modified Temporary Abdominal Closure Technique
 Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2008 Bogota-VAC A Newly Modified Temporary Abdominal Closure Technique von
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2008 Bogota-VAC A Newly Modified Temporary Abdominal Closure Technique von
Is the evolving management of intra-abdominal hypertension and abdominal compartment syndrome improving survival?*
 Continuing Medical Education Article Is the evolving management of intra-abdominal hypertension and abdominal compartment syndrome improving survival?* Michael L. Cheatham, MD, FCCM; Karen Safcsak, RN
Continuing Medical Education Article Is the evolving management of intra-abdominal hypertension and abdominal compartment syndrome improving survival?* Michael L. Cheatham, MD, FCCM; Karen Safcsak, RN
INTRA-ABDOMINAL HYPERTENSION AND SECONDARY ABDOMINAL COMPARTMENT SYNDROME IN MEDICAL PATIENTS COMPLICATION WITH A HIGH MORTALITY
 Trakia Journal of Sciences, Vol. 12, Suppl. 1, pp 202-207, 2014 Copyright 2014 Trakia University Available online at: http://www.uni-sz.bg ISSN 1313-7050 (print) ISSN 1313-3551 (online) INTRA-ABDOMINAL
Trakia Journal of Sciences, Vol. 12, Suppl. 1, pp 202-207, 2014 Copyright 2014 Trakia University Available online at: http://www.uni-sz.bg ISSN 1313-7050 (print) ISSN 1313-3551 (online) INTRA-ABDOMINAL
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
In the early 1980s, Kron et al. 1 showed in an. Surgical management of abdominal compartment syndrome
 This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this
This document is protected by international copyright laws. No additional reproduction is authorized. It is permitted for personal use to download and save only one file and print only one copy of this
Oncology case of the week:
 Oncology case of the week: The Abdomen That Won t Close Anton Sharapov, R4 July 14, 2004 Case 56 yof in ER resident on call asked to assess stoma looks infected has been on antibiotics not settling PMH
Oncology case of the week: The Abdomen That Won t Close Anton Sharapov, R4 July 14, 2004 Case 56 yof in ER resident on call asked to assess stoma looks infected has been on antibiotics not settling PMH
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Trauma Scenario. Abdominal Compartment Syndrome. Disclosure Statement of Financial Interest 8/17/2015
 Abdominal Compartment Syndrome Diane Cobble M.D., FACS Professor, ETSU Dept. of Surgery 7 th Annual Rural Trauma Symposium August 27, 2015 Disclosure Statement of Financial Interest I DO NOT have a financial
Abdominal Compartment Syndrome Diane Cobble M.D., FACS Professor, ETSU Dept. of Surgery 7 th Annual Rural Trauma Symposium August 27, 2015 Disclosure Statement of Financial Interest I DO NOT have a financial
Clinical Questions. Clinical Questions. Clinical Questions. Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen
 Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
General Review: The open abdomen: Management with temporary abdomincal closure. The open abdomen
 The open abdomen Part 2: Management of the open abdomen using temporary abdominal closure Abstract Pretorius JP, MBChB, MMed (Surg), FCS (SA); Liebenberg C, MBChB; Piek D, MBChB; Smith M, MBChB Correspondence
The open abdomen Part 2: Management of the open abdomen using temporary abdominal closure Abstract Pretorius JP, MBChB, MMed (Surg), FCS (SA); Liebenberg C, MBChB; Piek D, MBChB; Smith M, MBChB Correspondence
Comparison of open abdomens in non-trauma and trauma patients: A retrospective study
 Comparison of open abdomens in non-trauma and trauma patients: A retrospective study S. Peter Stawicki, MD 1, James Cipolla, MD 2, Corinne Bria, MD 3 1 Principal Scientist, OPUS 12 Foundation, King of
Comparison of open abdomens in non-trauma and trauma patients: A retrospective study S. Peter Stawicki, MD 1, James Cipolla, MD 2, Corinne Bria, MD 3 1 Principal Scientist, OPUS 12 Foundation, King of
Intra-abdominal Hypertension and Abdominal Compartment Syndrome: A Potentially Fatal Mix. Daria C. Ruffolo
 Intra-abdominal Hypertension and Abdominal Compartment Syndrome: A Potentially Fatal Mix Daria C. Ruffolo No Conflict of Interest druffol@lumc.edu 708.216.4541 Objectives Differentiate between intra-abdominal
Intra-abdominal Hypertension and Abdominal Compartment Syndrome: A Potentially Fatal Mix Daria C. Ruffolo No Conflict of Interest druffol@lumc.edu 708.216.4541 Objectives Differentiate between intra-abdominal
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
MESH REPAIR VERSUS PLANNED VENTRAL HERNIA STAGED REPAIR IN THE MANAGEMENT OF TRAUMA PATIENTS WITH ACUTE ABDOMINAL COMPARTMENT SYNDROME
 TOFIQ Journal of Medical Sciences, TJMS, Vol. 1, Issue 1, (2014), 47-61 ISSN: 2377-2808 MESH REPAIR VERSUS PLANNED VENTRAL HERNIA STAGED REPAIR IN THE MANAGEMENT OF TRAUMA PATIENTS WITH ACUTE ABDOMINAL
TOFIQ Journal of Medical Sciences, TJMS, Vol. 1, Issue 1, (2014), 47-61 ISSN: 2377-2808 MESH REPAIR VERSUS PLANNED VENTRAL HERNIA STAGED REPAIR IN THE MANAGEMENT OF TRAUMA PATIENTS WITH ACUTE ABDOMINAL
Colostomy & Ileostomy
 Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
Colostomy & Ileostomy Indications, problems and preference By Waleed Omar Professor of Colorectal surgery, Mansoura University. Disclosure I have no disclosures. Presentation outline Stoma: Definition
MIST. Minimally invasive Infusion & Suction Therapy Device. Effective treatment for deadly abdominal trauma and sepsis
 MIST Minimally invasive Infusion & Suction Therapy Device Effective treatment for deadly abdominal trauma and sepsis Summary Medical device for treating condition that annually kills ~156k intensive care
MIST Minimally invasive Infusion & Suction Therapy Device Effective treatment for deadly abdominal trauma and sepsis Summary Medical device for treating condition that annually kills ~156k intensive care
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Case Presentation. Joseph M Brandel, MD Kings County Hospital Center Department of Surgery Friday, November 12, 2004
 Case Presentation Joseph M Brandel, MD Kings County Hospital Center Department of Surgery Friday, November 12, 2004 The Abdominal Compartment Syndrome Definition A syndrome of intra-abdominal hypertension
Case Presentation Joseph M Brandel, MD Kings County Hospital Center Department of Surgery Friday, November 12, 2004 The Abdominal Compartment Syndrome Definition A syndrome of intra-abdominal hypertension
Abdominal Ultrasonography
 Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Abdominal Ultrasonography David A. Masneri, DO, FACEP, FAAEM Assistant Professor of Emergency Medicine Assistant Director, Emergency Medicine Residency Medical Director, Operational Medicine Division Center
Management of the Open Abdomen Usefulness of the bilateral anterior rectus abdominis sheath turnover flap method for early fascial closure
 From the Japanese ssociation of Medical Sciences Japanese ssociation for cute Medicine Management of the Open bdomen Usefulness of the bilateral anterior rectus abdominis sheath turnover flap method for
From the Japanese ssociation of Medical Sciences Japanese ssociation for cute Medicine Management of the Open bdomen Usefulness of the bilateral anterior rectus abdominis sheath turnover flap method for
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Clinical Evidence Summary ACCURYN ADVANCED CRITICAL CARE MONITORING
 Clinical Evidence Summary ACCURYN ADVANCED CRITICAL CARE MONITORING Table of Contents Introduction: Urine Output 3 Intensive monitoring of urine output is associated with increased detection 4 of acute
Clinical Evidence Summary ACCURYN ADVANCED CRITICAL CARE MONITORING Table of Contents Introduction: Urine Output 3 Intensive monitoring of urine output is associated with increased detection 4 of acute
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER
 SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
Discussion of Complex Clinical Scenarios and Variable Review ACS NSQIP Clinical Support Team
 Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
Discussion of Complex Clinical Scenarios and Variable Review CS NSQIP Clinical Support Team SCR Open Q& Calls The CS NSQIP Clinical Team is trialing Open format Q& calls for NSQIP SCRs Participation in
IVC. Fig. ACS. 84/60mmHg. CT Fig. 2 AAA. 30 declamp. declamp. Tel:
 12 633 637 2003 IVC 3 4 5 3 12 633 637 2003 1 ACS ACS 1 6 3 ACS 3 Tel: 0566-75-2111 446-8602 28 2003 7 18 2003 10 15 Fig. 1 4 5 1 71 12 5 COPD 14 10 30 60 CT AAA 84/60mmHg 8.2g/dl6.6g/dl2.5mg/dl CT Fig.
12 633 637 2003 IVC 3 4 5 3 12 633 637 2003 1 ACS ACS 1 6 3 ACS 3 Tel: 0566-75-2111 446-8602 28 2003 7 18 2003 10 15 Fig. 1 4 5 1 71 12 5 COPD 14 10 30 60 CT AAA 84/60mmHg 8.2g/dl6.6g/dl2.5mg/dl CT Fig.
Masatoku Arai 1*, Shiei Kim 1, Hiromoto Ishii 1, Jun Hagiwara 1, Shigeki Kushimoto 2 and Hiroyuki Yokota 1
 Arai et al. World Journal of Emergency Surgery (2018) 1:9 https://doi.org/10.118/s1017-018-0200-7 RESEARCH ARTICLE Open Access The long-term outcomes of early abdominal wall reconstruction by bilateral
Arai et al. World Journal of Emergency Surgery (2018) 1:9 https://doi.org/10.118/s1017-018-0200-7 RESEARCH ARTICLE Open Access The long-term outcomes of early abdominal wall reconstruction by bilateral
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair BACKGROUND EPIDEMIOLOGY 9/11/2018
 Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
Pancreatico-Duodenal Trauma: Drain, Debride, Divert, Despair Rochelle A. Dicker, M.D. Professor of Surgery and Anesthesia UCLA BACKGROUND Lancet 1827: Travers, B Rupture of the Pancreas British Journal
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
General'Surgery'Service'
 General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
General'Surgery'Service' Patient Care Goals and Objectives 1)! Stomach/Duodenum and Bariatric 2)! Interpret the results of clinical evaluations (history, physical examination) performed on patients being
Pelvic Prolapse. A Patient Guide to Pelvic Floor Reconstruction
 Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Pelvic Prolapse A Patient Guide to Pelvic Floor Reconstruction Pelvic Prolapse When an organ becomes displaced, or slips down in the body, it is referred to as a prolapse. Your physician has diagnosed
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Abdominal compartment syndrome
 Review Article Abdominal compartment syndrome Biswajit Mohapatra As per definition Abdominal Compartment Syndrome (ACS) is the sudden increase in the Intra-Abdominal pressure resulting in alteration in
Review Article Abdominal compartment syndrome Biswajit Mohapatra As per definition Abdominal Compartment Syndrome (ACS) is the sudden increase in the Intra-Abdominal pressure resulting in alteration in
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
Index Note: Page numbers of article titles are in boldface type. A Abdominal compartment syndrome, as complication of fluid resuscitation, 331 338 abdominal perfusion pressure, 332 fluid restriction practice
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
The Focused Assessment with Sonography for Trauma, (FAST) procedure.
 procedure.") The Focused Assessment with Sonography for Trauma, (FAST) procedure. ROBERT H. WRIGLEY Professor Veterinary Diagnostic Imaging University of Sydney Veterinary Teaching Hospital Professor Emeritus Colorado
The Focused Assessment with Sonography for Trauma, (FAST) procedure. ROBERT H. WRIGLEY Professor Veterinary Diagnostic Imaging University of Sydney Veterinary Teaching Hospital Professor Emeritus Colorado
Colorectal non-inflammatory emergencies
 Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
Colorectal non-inflammatory emergencies Prof. Hesham Amer Professor of general surgery, Kasr Alainy hospital, Cairo university Dr. Doaa Mansour Dr. Ahmed Nabil Dr. Ahmed Abdel-Salam Lecturers of general
DESCRIPTIONS FOR MED 3 ROTATIONS Critical Care A2 ICU
 Critical Care A2 ICU A. Neurological 1. Delirium Discuss the differential diagnosis and appropriate investigation for delirium. Provide non-pharmological and pharmological treatment options for delirium.
Critical Care A2 ICU A. Neurological 1. Delirium Discuss the differential diagnosis and appropriate investigation for delirium. Provide non-pharmological and pharmological treatment options for delirium.
Volume 16 - Issue 3, Cover Story
 Volume 16 - Issue 3, 2016 - Cover Story Update on Intra-Abdominal Hypertension Prof. Manu Malbrain, MD, PhD ******@***uzbrussel.be ICU Director - Intensive Care Unit, University Hospital Brussels (UZB)
Volume 16 - Issue 3, 2016 - Cover Story Update on Intra-Abdominal Hypertension Prof. Manu Malbrain, MD, PhD ******@***uzbrussel.be ICU Director - Intensive Care Unit, University Hospital Brussels (UZB)
Abdo Pain rules & regulations. Mark Hartnell 2010
 Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
Abdo Pain rules & regulations Mark Hartnell 2010 Aims Simple rules which might help in patients with abdominal pain Talk about some myths and realities Discuss some practical how to s in day to day treatment
This information is intended as an overview only
 This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
This information is intended as an overview only Please refer to the INSTRUCTIONS FOR USE included with this device for indications, contraindications, warnings, precautions and other important information
Review Abdominal compartment syndrome Jeffrey Bailey and Marc J Shapiro
 http://ccforum.com/content/4/1/023 Review Abdominal compartment syndrome Jeffrey Bailey and Marc J Shapiro Saint Louis University, St Louis, Missouri, USA Received: 4 January 2000 Accepted: 5 January 2000
http://ccforum.com/content/4/1/023 Review Abdominal compartment syndrome Jeffrey Bailey and Marc J Shapiro Saint Louis University, St Louis, Missouri, USA Received: 4 January 2000 Accepted: 5 January 2000
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
General surgery. Thyroid surgery. Physiological response to pneumoperitoneum. Bowel resection
 General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
General surgery Thyroid surgery Physiological response to pneumoperitoneum Bowel resection General surgery 3.D.9.1 James Mitchell (December 24, 2003) Thyroid surgery Preoperative Assessment Routine, plus
Understanding Intra-Abdominal Pressures
 Understanding Intra-Abdominal Pressures 1 Contact Hour Course Expires: May 31, 2018 Course Updated: October 14, 2014 First Published: October 14, 2011 Copyright 2011 by RN.com All Rights Reserved Reproduction
Understanding Intra-Abdominal Pressures 1 Contact Hour Course Expires: May 31, 2018 Course Updated: October 14, 2014 First Published: October 14, 2011 Copyright 2011 by RN.com All Rights Reserved Reproduction
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Parenteral Nutrition in IBD: Any indication?
 Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
Parenteral Nutrition in IBD: Any indication? Name: Institution: Marianna Arvanitakis Erasme University Hospital, Brussels, Belgium Clinical case 42 year old male Crohn s disease since he was 16 years old
Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs.
 Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern
Understanding the benefits of early enteral nutrition in the major trauma patient requiring intensive care: From clinical trials to costs. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH)
") EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH) Note: For the answers, refer to the SCDH Manual. The pages listed below each question will contain the answers,
EVALUATION OF SELF LEARNING BASED ON WHO MANUAL SURGICAL CARE AT THE DISTRICT HOSPITAL (SCDH) Note: For the answers, refer to the SCDH Manual. The pages listed below each question will contain the answers,
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Gastro-intestinal failure. ICU Fellowship Training Radboudumc
 Gastro-intestinal failure ICU Fellowship Training Radboudumc Case history (1) Male, 47 No previous medical history Mechanical ventilation for severe CAP Stable HD on NE 0.04 μg/kg/min Early enteral nutrition
Gastro-intestinal failure ICU Fellowship Training Radboudumc Case history (1) Male, 47 No previous medical history Mechanical ventilation for severe CAP Stable HD on NE 0.04 μg/kg/min Early enteral nutrition
Severe and Tertiary Peritonitis
 Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
Severe and Tertiary Peritonitis Addison K. May, MD FACS Professor of Surgery and Anesthesiology Division of Trauma and Surgical Critical Care Vanderbilt University Medical Center PS204: The Bad Infections:
Urologic Surgical Complications In Renal Transplantation
 Urologic Surgical Complications In Renal Transplantation Chris Freise, MD Professor of Surgery UCSF Transplant Division Urologic Complications Review of Bladder Anastomosis Complications and Management
Urologic Surgical Complications In Renal Transplantation Chris Freise, MD Professor of Surgery UCSF Transplant Division Urologic Complications Review of Bladder Anastomosis Complications and Management
Bronchoscopy SICU Protocol
 Bronchoscopy SICU Protocol Updated January 2013 Outline Clinical indications Considerations Preparation Bronchoscopy technique Bronchoalveolar Lavage (BAL) Post-procedure Purpose Bronchoscopy is a procedure
Bronchoscopy SICU Protocol Updated January 2013 Outline Clinical indications Considerations Preparation Bronchoscopy technique Bronchoalveolar Lavage (BAL) Post-procedure Purpose Bronchoscopy is a procedure
Transplant Surgery. Patient Education Guide to Your Kidney/Pancreas Transplant Page 9-1. For a kidney/pancreas transplant. Before Your Surgery
 Patient Education Page 9-1 Transplant Surgery For a kidney/pancreas transplant By the time you have your transplant surgery, you may have been waiting for some time. Reading this chapter before surgery
Patient Education Page 9-1 Transplant Surgery For a kidney/pancreas transplant By the time you have your transplant surgery, you may have been waiting for some time. Reading this chapter before surgery
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Piotr W. Trzeciak, Joanna Porzeżyńska, Karolina Ptasińska,
 POLSKI PRZEGLĄD CHIRURGICZNY 2015, 87, 11, 592 597 10.1515/pjs-2016-0008 Abdominal cavity eventration treated by means of the open abdomen technique using the negative pressure therapy system case report
POLSKI PRZEGLĄD CHIRURGICZNY 2015, 87, 11, 592 597 10.1515/pjs-2016-0008 Abdominal cavity eventration treated by means of the open abdomen technique using the negative pressure therapy system case report
Objectives. ER & ICU Pot Pourri. Why is this important? Brady et al: Objective. Discuss published information. Take away new information
 ER & ICU Pot Pourri Karl E. Jandrey, DVM, DACVECC Asst. Professor of Clinical Emergency and Critical Care Veterinary Medical Teaching Hospital University of California-Davis Objectives Discuss published
ER & ICU Pot Pourri Karl E. Jandrey, DVM, DACVECC Asst. Professor of Clinical Emergency and Critical Care Veterinary Medical Teaching Hospital University of California-Davis Objectives Discuss published
Reinterventions belong to complications
 Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Emergency Medicine Scope of Practice
 Emergency Medicine Scope of Practice All Physician Assistants working in Emergency Medicine will encounter a wide variety of non acute, urgent and emergent patient complaints and conditions. Given the
Emergency Medicine Scope of Practice All Physician Assistants working in Emergency Medicine will encounter a wide variety of non acute, urgent and emergent patient complaints and conditions. Given the
Complicated Diverticulitis. Evidence Based Recommendations
 Complicated Diverticulitis Evidence Based Recommendations Frederick A Moore MD September 10, 2014 Complicated Diverticulitis Evidence Based Recommendations I have no financial disclosures A Management
Complicated Diverticulitis Evidence Based Recommendations Frederick A Moore MD September 10, 2014 Complicated Diverticulitis Evidence Based Recommendations I have no financial disclosures A Management
Post-Cardiac Surgery Evaluation
 Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Post-Cardiac Surgery Evaluation 20th Annual Heart Conference October 15, 2016 Gary A Mayman PROFESSOR PEDIATRICS UNIVERSITY OF NEVADA Look Touch Listen Temperature, pulse, respiratory rate, & blood pressure
Early enteral nutrition in the major trauma patient requiring intensive care: An overview of the evidence.
 Early enteral nutrition in the major trauma patient requiring intensive care: An overview of the evidence. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern Clinical School Intensive Care
Early enteral nutrition in the major trauma patient requiring intensive care: An overview of the evidence. Dr. Gordon S. Doig Associate Professor in Intensive Care Northern Clinical School Intensive Care
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS
 GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
GENERAL SURGERY FOR SMART PEOPLE JOE NOLD MD, FACS WICHITA SURGICAL SPECIALISTS CONFLICTS/DECLARATIONS I have no financial conflicts or declarations I AM always willing to see a consult for you TEXT TOPICS
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Shock. William Schecter, MD
 Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Shock William Schecter, MD The Cell as a furnace O 2 1 mole Glucose Cell C0 2 ATP 38 moles H 2 0 Shock = Inadequate Delivery of 02 and Glucose to the Cell 0 2 Cell ATP 2 moles Lactic Acid Treatment of
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM
 Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM") ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
ANZ Emergency Laparotomy Audit Quality Improvement (ANZELA-QI) Pilot Collaboration between RACS, ANZCA, GSA, NZAGS, ASA, NZSA, ACEM, CICM DATA COLLECTION FORM Most Australian hospitals contribute data
Current concepts in Critical Care Nutrition
 Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
Current concepts in Critical Care Nutrition Dr.N.Ramakrishnan AB (Int Med), AB (Crit Care), MMM, FACP, FCCP, FCCM Director, Critical Care Services Apollo Hospitals, Chennai Objectives Why? Enteral or Parenteral
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
An Experience in the Management of the Open Abdomen in Severely Injured Burn Patients
 An Experience in the Management of the Open Abdomen in Severely Injured Burn Patients Mark O. Hardin, MD, James E. Mace, MD, John D. Ritchie, MD, Kevin K. Chung, MD, Katharine W. Markell, MD, Evan M. Renz,
An Experience in the Management of the Open Abdomen in Severely Injured Burn Patients Mark O. Hardin, MD, James E. Mace, MD, John D. Ritchie, MD, Kevin K. Chung, MD, Katharine W. Markell, MD, Evan M. Renz,
Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine
 Running on Empty Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine Nationwide id Children s Hospital Associate Professor, Department of Pediatrics The Ohio State
Running on Empty Kathryn Nuss, MD Associate Trauma Medical Director Associate Director, Emergency Medicine Nationwide id Children s Hospital Associate Professor, Department of Pediatrics The Ohio State
Modified Opsite sandwich for temporary abdominal closure: a non-traumatic experience
 The Royal College of Surgeons of England GASTROINTESTINAL doi 10.1308/003588407X155446 Modified Opsite sandwich for temporary abdominal closure: a non-traumatic experience JM WILDE, MA LOUDON Department
The Royal College of Surgeons of England GASTROINTESTINAL doi 10.1308/003588407X155446 Modified Opsite sandwich for temporary abdominal closure: a non-traumatic experience JM WILDE, MA LOUDON Department
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Surgery and Crohn s. Crohn s Disease 70 % Why Operate? Complications of Disease. The Gastrointestinal Tract. Surgery for Inflammatory Bowel Disease
 The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
The Gastrointestinal Tract Surgery for Inflammatory Bowel Disease Jonathan Chun, MD The regon Clinic Gastrointestinal and Minimally Invasive Surgery Crohn s Disease Can affect anywhere in the GI tract,
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Inadvertent Enterotomy in Minimally Invasive Abdominal Surgery
 SCIENTIFIC PAPER Inadvertent Enterotomy in Minimally Invasive Abdominal Surgery Steven J. Binenbaum, MD, Michael A. Goldfarb, MD ABSTRACT Background: Inadvertent enterotomy (IE) in laparoscopic abdominal
SCIENTIFIC PAPER Inadvertent Enterotomy in Minimally Invasive Abdominal Surgery Steven J. Binenbaum, MD, Michael A. Goldfarb, MD ABSTRACT Background: Inadvertent enterotomy (IE) in laparoscopic abdominal
Proximal Loop Ileostomy-A Life Saving Approach in ComplicatedEnterocutaneous Fistulas
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 8 Ver. III (Aug. 2014), PP 58-67 Proximal Loop Ileostomy-A Life Saving Approach in ComplicatedEnterocutaneous
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 8 Ver. III (Aug. 2014), PP 58-67 Proximal Loop Ileostomy-A Life Saving Approach in ComplicatedEnterocutaneous
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Procedure: Chest Tube Placement (Tube Thoracostomy)
") Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct