Damage Control in Abdominal and Pelvic Injuries
|
|
|
- Phillip Bryan
- 6 years ago
- Views:
Transcription
1 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department of Surgery Chief, Division of Trauma, Surgical Critical Care, Burns. And Acute Care Surgery University of California San Diego School of Medicine
2 Damage Control the ability to sustain, control and repair combat damage and allow a warship to return to offensive action U.S. Navy
3 Damage Control a concept of temporary measures that can be applied as a part of a staged approach to a complex problem Hirshberg and Mattox Surg Clin North America 1997
4 Historical Perspective The traditional approach to penetrating trauma of the abdomen has been exploratory laparotomy for control of hemorrhage and contamination If physiological stability is maintained definitive repair of injuries should be accomplished Rotondo MF, et al J Trauma 1993
5 Historical Perspective Feliciano and co-workers in 1988 evaluated 300 consecutive abdominal gunshot wounds: Tried and true approach Definitive repair achieved in majority of cases Overall survival ~ 88% GSW with major vascular injury ~ 60% Multiple visceral injuries survival plummeted Concluded that acidosis, hypothermia and coagulopathy contributed to ~ 85% of deaths
6 The Cycle of Death You do not need to do everything at the initial operation..
7 Potential Solutions H. Harlan Stone, in 1983, described the use of a rapidly terminated laparotomy after abdominal packing was undertaken at the onset of clinically apparent coagulopathy followed by SICU stabilization and delayed operative correction of major injuries Stone HH, et al Ann Surg 1983
8 Potential Solutions The term Damage control was coined at the University of Pennsylvania in 1993 by Rotondo and Schwab Described three separate and distinctive phases Control of hemorrhage and contamination with temporary abdominal closure Core rewarming, correction of coagulopathy, ventilatory support, identification of associated injuries and maximization of hemodynamic values Re-exploration and definitive surgical repair
9 Potential Solutions Retrospective study evaluating 46 patients with penetrating abdominal trauma requiring laparotomy and massive transfusion (> 10u PRBC s) No significant difference between definitive repair and damage control surgery Subset analysis of 22 patients with major vascular injury, however, revealed a statistically significant difference in survival: Damage control 10/13 = 77% (p <.02) Definitive repair 1/9 = 11%

10 Damage Control Strategy
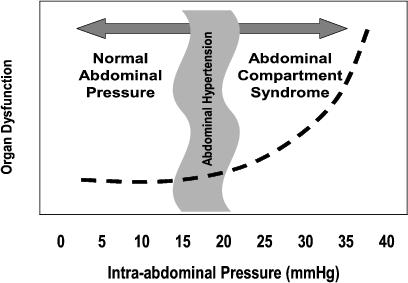
11 Damage Control When? Patient too sick Altered Physiology Hemorrhage induced- lethal triad Bowel too edematous Aggressive resuscitation too much crystalloid Risk of IAH / ACS Second Look for diseases other than trauma Mesenteric Ischemia, Severe Pancreatitis, Peritonitis
12 Patient Selection
13



14 WHAT IS PRIMARY ACS? Primary ACS is a condition associated with injury or disease in the abdominopelvic region that frequently requires early surgical or interventional radiological intervention. Traumatic Injury Ascites / Fluid Abdominal Tumor



15 WHAT IS SECONDARY ACS? Secondary ACS refers to conditions that do not originate from the abdominopelvic region. Sepsis / Burns Massive Capillary Leak Resuscitation


16 Damage Control - Abdomen Spillage Control Staple off bowel Packing for solid organ bleeding Ligation or shunt for vascular injury Temporary closure of abdomen.




17 Temporary Abdominal Closure vacuum pack/ Ioban closure
18 Postoperative Management Resuscitation Adequate oxygen delivery is the goal and is achieved with continue transfusion Response monitored by observing HR, SBP, UOP, ph, serum lactate levels and correction of coagulopathy Inotropic support may be necessary for those who do not respond to volume
19 Postoperative Management Pulmonary function Goal is to achieve SaO2 > 92% with FiO2 < 0.6 Conventional volume ventilation may require high PEEP with the resulting decline in cardiac filling pressures and barotrauma Pressure control ventilation can achieve oxygenation and ventilation goals with significantly reduced airway pressures
20 Postoperative Management Hemostasis PBRC:FFP:Platelets = 1:1:1 Judicious use of fresh frozen plasma and platelets is warranted Most common cause of persistent coagulopathy is surgical bleeding. Reevaluate the need ot go back to the OR for bleeding comtrol Normalizing temperature Tertiary survey

21 J Trauma 2010: 69:46-52
22 The Take Back Phase 3 Timing Definitive surgical care for intra-abdominal injuries Many will remain with open abdomen and will require multiple take backs
23 Postoperative Complications Missed injuries Abdominal wound Suture temporary prosthetic material to the skin vice the fascia Never close under tension Fistula Infection Multiple procedures results in a 12-67% intraabdominal infection rate
24 Postoperative Complications Nutrition Enteral nutrition preferred route of administration Thromboembolism prophylaxis Skin complications
25 Damage Control - Pelvic
26 Hemorrhage in Pelvic Fractures Retroperitoneal bleeding Up to 4 L of blood Tamponade Direct surgical control usually not indicated Early stabilization Decrease volume of pelvis Reopposes bleeding surfaces Clot formation
27 Control of Pelvic Bleeding Fracture reduction techniques Angiography Operative control Reserved for large vessel bleeding Retroperitoneal packing Open Fractures Packing, packing, packing

28 Fracture Reduction Pneumatic Antishock Garment Bed sheet, taping knees together External fixation 15 minutes Anterior frame, two pins in each iliac crest Decreases pelvic volume, confers bony stability Interference with abdominal exam, CT scan, and surgical exposure Improved outcomes, decreased mortality? No prospective data

29 Fracture Reduction Pelvic clamps Posterior fixation Greater compression posteriorly Little data
30 Angiography Arterial bleeding, embolization: 10% APC II or III Criteria: no clear consensus Contrast extravasation on CT Continued blood loss (4U in 24 hrs, 6U in 48 hrs) Hemodynamically unstable Large, expanding retroperitoneal hematoma Prior placement of external fixator?


31 Embolization as part of Damage Control


32 Pelvis Fractures with Hemorrhage


33 Angio Embolization

34 Pelvic Packing

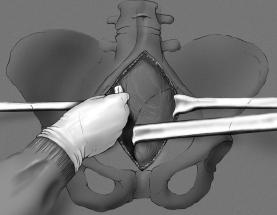
35 Pelvic Packing

36 Pelvic Packing


37 Pelvic Packing



38 Open Pelvis: Pack First, Angio After



39 Open Pelvis: Pack First, Angio After
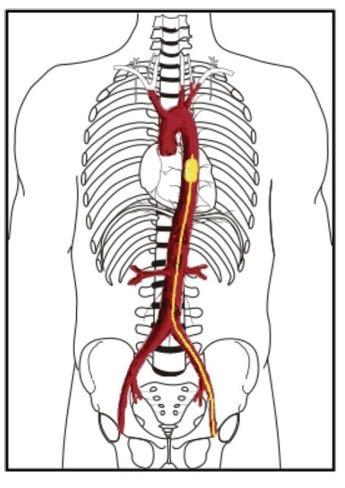
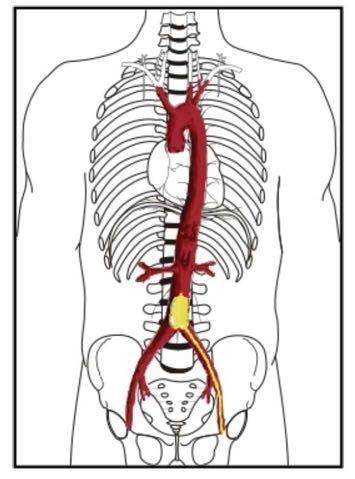
40 The new kid on the block REBOA
41
42
43 AORTIC ZONES 4
44
45 Biffl et al.: J Trauma Acute Care Surg. 78, 5:
46 Conclusions Paradigm shift in the care of critically injured trauma patients within the last 15 years Elimination of acidosis, coagulopathy and hypothermia paramount to patient survival Multiple intensive and expensive resources required along with dedicated surgeons, nurses and ancillary personnel
47 Visit us at:

48
Management of the Open Abdomen
 Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Thicker than Water. Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago
 Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
Thicker than Water Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago I have no relevant financial relationships to disclose. Who is bleeding? How much and what kind
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
Adult Trauma Advances in Pediatrics. (sometimes they are little adults) FAST examination. Who is bleeding? How much and what kind of TXA volume?
 FAST examination. Who is bleeding? How much and what kind of TXA volume?") Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Adult Trauma Advances in Pediatrics (sometimes they are little adults) Alisa McQueen MD, FAAP, FACEP Associate Professor of Pediatrics The University of Chicago Alisa McQueen MD, FAAP, FACEP Associate
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
The Abdominal Compartment Syndrome
 The Abdominal Compartment Syndrome Andre R. Campbell, MD, FACS, FACP, FCCM Professor of Surgery, UCSF Endowed Chair of Surgical Education San Francisco General Hospital Outline Case presentations Review
The Abdominal Compartment Syndrome Andre R. Campbell, MD, FACS, FACP, FCCM Professor of Surgery, UCSF Endowed Chair of Surgical Education San Francisco General Hospital Outline Case presentations Review
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Emergency Laparotomy. Open vs Closed Abdomen
 Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
Emergency Laparotomy Open vs Closed Abdomen Disclosure Dr. McLean is a site primary investigator for XenMatrix AB Tissue Insert for Ventral Hernia repair. Sponsor: Bard Davol Learning Objectives: 1. The
The Acute Management of Pelvic Ring Injuries
 The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
Chapter 2 Damage Control
 Chapter 2 Damage Control Rona E. Altaras, Firas G. Madbak and Dale A. Dangleben History Originally a naval term, damage control (DC) is a simple and useful idea referring to the ability of a battleship
Chapter 2 Damage Control Rona E. Altaras, Firas G. Madbak and Dale A. Dangleben History Originally a naval term, damage control (DC) is a simple and useful idea referring to the ability of a battleship
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Civilian versus Military Trauma Management
 Western University From the SelectedWorks of Vivian C. McAlister November, 2010 Civilian versus Military Trauma Management Vivian C. McAlister Available at: https://works.bepress.com/vivianmcalister/151/
Western University From the SelectedWorks of Vivian C. McAlister November, 2010 Civilian versus Military Trauma Management Vivian C. McAlister Available at: https://works.bepress.com/vivianmcalister/151/
LIVER TRAUMA. Jonathan R. Hiatt, MD
 Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Jonathan R. Hiatt, MD HISTORY 1880 1900 1908 MORTALITY OF LIVER INJURY MODERN CONCEPTS PACKS, RESECTION PRINGLE WW II 27% KOREA 14% VIETNAM 8.5% URBAN TRAUMA CTRS. EPIDEMIOLOGY CLASSIFICATION THERAPEUTIC
Abdominal V.A.C. Therapy in Trauma
 Abdominal V.A.C. Therapy in Trauma Stefaan Nijs, M.D., Ph.D. Mathieu D Hondt, M.D. Dept Abdominal Surgery UZ Leuven 1 2 Damage control = naval technique Damage Control in Trauma 3 USS Nevada 4 In extremis
Abdominal V.A.C. Therapy in Trauma Stefaan Nijs, M.D., Ph.D. Mathieu D Hondt, M.D. Dept Abdominal Surgery UZ Leuven 1 2 Damage control = naval technique Damage Control in Trauma 3 USS Nevada 4 In extremis
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
2 Blunt Abdominal Trauma
 2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
2 Blunt Abdominal Trauma Ricardo Ferrada, Diego Rivera, and Paula Ferrada Pearls and Pitfalls Patients suffering a high-energy trauma have solid viscera rupture in the abdomen and/or aortic rupture in
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Presented at 2015 TQIP conference. Developed by a panel of experts. Evidence based with expert opinion as needed
 Presented at 2015 TQIP conference Developed by a panel of experts Evidence based with expert opinion as needed Orthopaedic Trauma Best Practice Guidelines (BPG) Goals Offer guidance on what is practical
Presented at 2015 TQIP conference Developed by a panel of experts Evidence based with expert opinion as needed Orthopaedic Trauma Best Practice Guidelines (BPG) Goals Offer guidance on what is practical
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
ICU treatment of the trauma patient. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
ICU treatment of the trauma patient Intensive Care Training Program Radboud University Medical Centre Nijmegen Christian Kleber Surgical Intensive Care Unit - The trauma surgery Perspective Langenbecks
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Selective Nonoperative Management of Penetrating Abdominal Trauma. Kings County Hospital Center Verena Liu, MD 10/13/2011
 Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Selective Nonoperative Management of Penetrating Abdominal Trauma Kings County Hospital Center Verena Liu, MD 10/13/2011 Case Presentation 28M admitted on 8/27/2011 s/p GSW to right upper quadrant and
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
DAMAGE CONTROL. Outline. Definition 5/29/2014. No Disclosures
 DAMAGE CONTROL No Disclosures Rochelle A. Dicker, MD Associate Professor of Surgery and Anesthesia University of California, San Francisco Definition Term used in the Merchant Marines and in Navies for
DAMAGE CONTROL No Disclosures Rochelle A. Dicker, MD Associate Professor of Surgery and Anesthesia University of California, San Francisco Definition Term used in the Merchant Marines and in Navies for
5/30/2013. I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow. Trauma = #1 cause of death persons <40 yo 1
 I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
I have no conflicts of interest to disclose. Alicia Privette, MD Trauma & Critical Care Fellow Trauma = #1 cause of death persons
Difficult Abdominal Closure. Mark A. Carlson, MD
 Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Difficult Abdominal Closure Mark A. Carlson, MD Illustrative case 14 yo boy with delayed diagnosis of appendicitis POD9 Appendectomy 2 wk after onset of symptoms POD4: return to OR for midline laparotomy
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Ballistic Trauma. L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016
 Ballistic Trauma L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016 Case Presentation Most cases at Kings County Hospital Case Presentation HPI: 22yo male presented as Level I Trauma
Ballistic Trauma L Yuko Shimotake, MD Kings County Hospital Center September 22, 2016 Case Presentation Most cases at Kings County Hospital Case Presentation HPI: 22yo male presented as Level I Trauma
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Epidemiology. Case. Pre-Hospital SI and Massive Transfusion
 Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Epidemiology Preston Maxim, MD Assoc. Professor of Emergency Medicine San Francisco General Hospital ~180,000 deaths 2007 due to trauma 25% trauma patients require 1 unit of PRBC and only 25% of those
Case Presentation Conference Ravi Dhanisetty, M.D. Kings County Hospital Center
 Case Presentation Morbidity and Mortality Conference Ravi Dhanisetty, M.D. Kings County Hospital Center 1 May 2009 Case Presentation 53 year old male bus driver had a syncopal episode and found down unresponsive.
Case Presentation Morbidity and Mortality Conference Ravi Dhanisetty, M.D. Kings County Hospital Center 1 May 2009 Case Presentation 53 year old male bus driver had a syncopal episode and found down unresponsive.
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
Unrestricted. Dr ppooransari fellowship of perenatalogy
 Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Unrestricted Dr ppooransari fellowship of perenatalogy Assessment of severity of hemorrhage Significant drops in blood pressure are generally not manifested until substantial bleeding has occurred, and
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
the bleeding won t stop? Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital
 Royal Alexandra Hospital") What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
What do you do when the bleeding won t stop? Teddie Tanguay RN, MN, NP, CNCC(c) Teddie Tanguay RN, MN, NP, CNCC(c) Liane Manz RN, BScN, CNCC(c) Royal Alexandra Hospital Outline Case study Normal coagulation
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
TRAUMA RESUSCITATION. Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital
 TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
TRAUMA RESUSCITATION Dr. Carlos Palisi Dr. Nicholas Smith Liverpool Hospital First Principles.ATLS/EMST A- Airway and C-spine B- Breathing C- Circulation and Access D- Neurological deficit E- adequate
Damage Control Resuscitation
 Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Damage Control Resuscitation H M Cassimjee Critical Care Specialist Department of Critical Care & Level 1 Trauma Unit Inkosi Albert Luthuli Central Hospital Damage Control Resuscitation only for DAMAGED
Northern Trauma Network. Management of Haemodynamically Unstable Patients with Pelvic Injury
 Management of Haemodynamically Unstable Patients with Pelvic Injury Northern Trauma Network This guideline focuses on the assessment of haemodynamic instability related to haemorrhage associated with a
Management of Haemodynamically Unstable Patients with Pelvic Injury Northern Trauma Network This guideline focuses on the assessment of haemodynamic instability related to haemorrhage associated with a
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Hemostatic Resuscitation in Trauma. Joanna Davidson, MD 6/6/2012
 Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Hemostatic Resuscitation in Trauma { Joanna Davidson, MD 6/6/2012 Case of HM 28 yo M arrives CCH trauma bay 5/27/12 at 241 AM Restrained driver in low speed MVC after getting shot in the chest Arrived
Amputations. Chapter 23
 Amputations Chapter 23 Amputations Introduction Battle casualties who sustain amputations have the most severe extremity injuries. Historically, 1 in 3 patients with a major amputation (proximal to the
Amputations Chapter 23 Amputations Introduction Battle casualties who sustain amputations have the most severe extremity injuries. Historically, 1 in 3 patients with a major amputation (proximal to the
Endovascular Trauma Management. Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden
 Endovascular Trauma Management Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden Medtronic Symposium, LINC 2016 Disclosures I have the following potential
Endovascular Trauma Management Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden Medtronic Symposium, LINC 2016 Disclosures I have the following potential
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC
 Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to
Bleeding and Shock *** CME Version *** Aaron J. Katz, AEMT-P, CIC www.es26medic.net Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Masatoku Arai 1*, Shiei Kim 1, Hiromoto Ishii 1, Jun Hagiwara 1, Shigeki Kushimoto 2 and Hiroyuki Yokota 1
 Arai et al. World Journal of Emergency Surgery (2018) 1:9 https://doi.org/10.118/s1017-018-0200-7 RESEARCH ARTICLE Open Access The long-term outcomes of early abdominal wall reconstruction by bilateral
Arai et al. World Journal of Emergency Surgery (2018) 1:9 https://doi.org/10.118/s1017-018-0200-7 RESEARCH ARTICLE Open Access The long-term outcomes of early abdominal wall reconstruction by bilateral
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Pediatric Trauma Practice. Guideline for Management of the Child in Shock. Background
 Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Bleeding and Shock. Circulatory System
 Bleeding and Shock Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to body tissues Delivers
Bleeding and Shock Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Circulatory System Composed of heart, blood vessels and blood A closed system Pumps oxygenated blood and nutrients to body tissues Delivers
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
IS POLYTETRAFLUOROETHYLENE (PTFE) THE CORRECT CHOICE TO TREAT CONTAMINATED TRAUMATIC VASCULAR INJURIES?
 THE CORRECT CHOICE TO TREAT CONTAMINATED TRAUMATIC VASCULAR INJURIES?") IS POLYTETRAFLUOROETHYLENE (PTFE) THE CORRECT CHOICE TO TREAT CONTAMINATED TRAUMATIC VASCULAR INJURIES? Nigel Denis MD Class of 2016 University of Miami Miller School of Medicine Miami, Florida, USA Disclosures
IS POLYTETRAFLUOROETHYLENE (PTFE) THE CORRECT CHOICE TO TREAT CONTAMINATED TRAUMATIC VASCULAR INJURIES? Nigel Denis MD Class of 2016 University of Miami Miller School of Medicine Miami, Florida, USA Disclosures
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
World Journal of Colorectal Surgery
 World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
World Journal of Colorectal Surgery Volume 3, Issue 1 2013 Article 9 ISSUE 1 Perforation Of The Caecum Owing To Benign Rectal Obstruction: A Paradigm Of Damage Control In Emergency Colorectal Surgery DIMITRIOS
REBOA - Real World. Lena M. Napolitano, MD
 REBOA - Real World Lena M. Napolitano, MD Lena M. Napolitano MD, FACS Massey Foundation Professor of Surgery Acute Care Surgery [Trauma, Burn, Critical Care, Emergency Surgery] University of Michigan Ann
REBOA - Real World Lena M. Napolitano, MD Lena M. Napolitano MD, FACS Massey Foundation Professor of Surgery Acute Care Surgery [Trauma, Burn, Critical Care, Emergency Surgery] University of Michigan Ann
Javier Marquez Graciani, MD Attending Dr F. Joglar
 Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Modern Management of the Open Abdomen A Cautionary Tale. Grand Rounds December 16, 2010 SUNY, Downstate
 Modern Management of the Open Abdomen A Cautionary Tale Grand Rounds December 16, 2010 SUNY, Downstate Case HPI: 41 yo M BIBA; stabbed in left back while walking out of a shopping center. PMH/PSH: GSW
Modern Management of the Open Abdomen A Cautionary Tale Grand Rounds December 16, 2010 SUNY, Downstate Case HPI: 41 yo M BIBA; stabbed in left back while walking out of a shopping center. PMH/PSH: GSW
Recombinant Activated Factor VII: Useful. Department of Surgery Grand Rounds 11/8/10 David Mauchley MD
 Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Recombinant Activated Factor VII: Useful Department of Surgery Grand Rounds 11/8/10 David Mauchley MD Hemostasis and Coagulation Traditional cascade model Two convergent pathways Series of proteolytic
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Management of the Mangled Extremity Clinical Practice Policy
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Management of the Mangled Extremity Clinical Practice Policy Original Date: 03/2015 Purpose: To coordinate multi-disciplinary
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Management of the Mangled Extremity Clinical Practice Policy Original Date: 03/2015 Purpose: To coordinate multi-disciplinary
T-PODResponder Pelvic Stabilization Device
 T-PODResponder Pelvic Stabilization Device Training Session Pyng Medical Corp. 1-604-303-7964 2014 Pyng Medical Corp. August 2014 PM-176a Why T-PODResponder? Pelvic fractures have a mortality rate of 5%
T-PODResponder Pelvic Stabilization Device Training Session Pyng Medical Corp. 1-604-303-7964 2014 Pyng Medical Corp. August 2014 PM-176a Why T-PODResponder? Pelvic fractures have a mortality rate of 5%
Review. A. abrasion B. contusion C. hematoma D. avulsion
 Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Chapter 24 Review Review 1. A young male was struck in the forearm with a baseball and complains of pain to the area. Slight swelling and ecchymosis are present, but no external bleeding. What type of
Trauma Resuscitation: more than just blood products
 Trauma Resuscitation: more than just blood products Benjamin T. Houseman, MD, PhD Assistant Professor in Residence Department of Anesthesia University of California San Francisco Traumatic injury Leading
Trauma Resuscitation: more than just blood products Benjamin T. Houseman, MD, PhD Assistant Professor in Residence Department of Anesthesia University of California San Francisco Traumatic injury Leading
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Pelvic fractures. Dr Raymond Yean, MBBS Surgical SRMO
 Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
Cover Page The handle http://hdl.handle.net/1887/39153 holds various files of this Leiden University dissertation. Author: Hommes, M. Title: The injured liver : management and hepatic injuries in the traumapatient
A Review on the Role of Laparoscopy in Abdominal Trauma
 10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
10.5005/jp-journals-10007-1109 ORIGINAL ARTICLE WJOLS A Review on the Role of Laparoscopy in Abdominal Trauma Aryan Ahmed Specialist General Surgeon, ATLS Instructor, Department of General Surgery, Hamad
Prehospital Hemorrhage Control
 Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
Prehospital Hemorrhage Control LCOL Edward Tan, MD PhD Military Traumasurgeon Radboud University Medical center, LCOL Edward C.T.H. Tan, MD PhD Nijmegen, The Netherlands Military traumasurgeon Radboud
Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for External Hemorrhage Control
 Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
Eileen M. Bulger, MD Professor of Surgery, Chief of Trauma Harborview Medical Center University of Washington Disclosure Chair of ACS COT EMS Committee Authored Evidence Based Prehospital Guideline for
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Management of traumatic liver injuries, Mafraq hospital experience, UAE
 International Surgery Journal Alkatary MM et al. Int Surg J. 2017 Aug;4(8):2413-2418 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20173163
International Surgery Journal Alkatary MM et al. Int Surg J. 2017 Aug;4(8):2413-2418 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20173163
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
Clinical Questions. Clinical Questions. Clinical Questions. Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen
 Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
ATLS 10th ed. Course Structure and Content Changes. Current Update on ATLS For Trauma Patients
 ATLS 10th ed. Course Structure and Content Changes Current Update on ATLS For Trauma Patients ATLS 10th ed. Course Structure and Content Changes International ATLS 86 countries > 1 million trained > 50%
ATLS 10th ed. Course Structure and Content Changes Current Update on ATLS For Trauma Patients ATLS 10th ed. Course Structure and Content Changes International ATLS 86 countries > 1 million trained > 50%