Difficult Polypectomy 2015 Tool of the Trade
|
|
|
- John Charles
- 6 years ago
- Views:
Transcription
1 Difficult Polypectomy 2015 Tool of the Trade Jonathan Cohen, MD FACG FASGE Clinical Professor of Medicine NYU Langone School of Medicine Improving Therapeutics in the Colon Improved detection of polyp and polyp margins Improved resection techniques Improved closure of iatrogenic mucosal defects Copyright 2015 American College of Gastroenterology 1




2 Know Where to Look! Cecal Retroflexion & Effort to Confirm all Polyp Borders Visualized Copyright 2015 American College of Gastroenterology 2
3 Therapeutic Tips & Considerations Generous use of saline lift Epi injection to thick bases and stalks Suction to reduce diameter Recognize non-lifting and signs of invasive i cancer Fulgurate the base of sessile polyps Therapeutic Tips & Considerations Carefully image the margins to ensure complete resection Insist on comfortable short scope positions with torque to get lesion in ideal location Creation of leading edges for piecemeal polypectomy Suction to small flat lesions to facilitate t removal Consideration of clips to close larger defects Copyright 2015 American College of Gastroenterology 3
 for advanced colonic mucosal")

4 Polypectomy Piece by Piece EMR Effective if Done Right Moss, A., Williams, S.J., Hourigan, L.F. et al. Longterm adenoma recurrence following wide-field endoscopic mucosal resection (WF-EMR) for advanced colonic mucosal neoplasia is infrequent: results and risk factors in 1000 cases from the Australian Colonic EMR (ACE) study. Gut. 2015; 64: Care to excise normal mucosa around lateral margin 97% success rates in <2 sessions Copyright 2015 American College of Gastroenterology 4
![Efficacy of wemr ACE [Australian Colonic EMR] Study](/docs-images/76/74253648/images/5-0.jpg "Prospective study of flst >20 mm with f/u exams at 4 and")



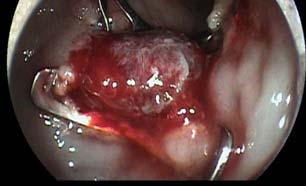
5 Efficacy of wemr ACE [Australian Colonic EMR] Study Prospective study of flst >20 mm with f/u exams at 4 and 12 months 940 cases, successful excision in 91% 81% no recurrence at 4 months; 0.6% at 12 mo. 19% diminutive i and generally easy to remove recurrence; only 3 persisted at 12 mo. Only 1 patient required surgery 120 mm sized laterally spreading tumor of the proximal transverse colon from ACE study Copyright 2015 American College of Gastroenterology 5


6 Should we clip large resection sites together? Video Rationale for Closure Clips cost effective only for polyps >10 mm in anticoagulated patients: Parikh, N.D., Zanocco, K., Keswani, R.N. et al. Acost- efficacy decision analysis of prophylactic clip placement after endoscopic removal of large polyps. Clin Gastroenterol Hepatol. 2013; 11: Prophylactic clip closure reduced the risk of delayed ed postpolypectomypectom hemorrhage: experience in 277 clipped large sessile or flat colorectal lesions and 247 control lesions: Hammad Liaquat, Elizabeth Rohn, Douglas K. Rex Gastrointestinal Endoscopy, Vol. 77, Issue 3, p Copyright 2015 American College of Gastroenterology 6
7 Obstacles to Successful Large EMR Fibrosis [suggested by non-lifting] Prior biopsy or partial polypectomy Tatooing close to the lesion Imaging evidence suggestive of cancer Location right colon; multiple folds, flexures Approaches to Non-Lifting, Fibrosis, and Residual Tissue Water jet assisted lifting Avulsion technique to remove non-lifting mucosal bridges Endocut via HBF Underwater polypectomy Cap assisted gentle suction with great care! Hybrid ESD techniques combined with piecemeal EMR Copyright 2015 American College of Gastroenterology 7

![laterally spreading tumors [LST s] Saito Y et al. Surg Endosc 2010; 24:343-52 2% vs.](/docs-images/76/74253648/images/8-1.jpg "14% recurrence rate Improved histologic assessments when 1 micron of sm1 might suffice without surgery")
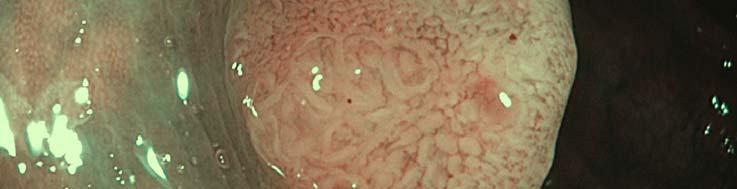
8 Extreme Polypectomy: ESD Colon ESD Considerations High perforation rates: 2.7% in Japanese series Dependent on available local expertise Potential reduced recurrence of large laterally spreading tumors [LST s] Saito Y et al. Surg Endosc 2010; 24: % vs. 14% recurrence rate Improved histologic assessments when 1 micron of sm1 might suffice without surgery Copyright 2015 American College of Gastroenterology 8

9 When to consider ESD Large LST granular type >30 mm Large LST non granular >20 mm Non lifting sign Imaging suggestion of advance histology or submucosal invasion: Kudo V Sano 3 Image of ESD small defects Copyright 2015 American College of Gastroenterology 9




10 Wider opening possible following EMR OOPS! What do I do now? Preparing for Effective Perforation Management Copyright 2015 American College of Gastroenterology 10

11 Damage Control Bowel prep ensure a clean field before embarking on colon EMR C02 insufflation reduces pneumoperitoneum Immediate recognition target target sign If you think it might be a perforation assume it is and close it! Target sign accentuated by use of dye in submucosal injection Copyright 2015 American College of Gastroenterology 11

12 Acute perforation management Tools and options: Standard clip closure OTSC technique and limitations Overstitch technique and limitations Copyright 2015 American College of Gastroenterology 12
13 TIPS FOR CLIPS Keep the clip close to the end of the endoscope with the clip-endoscope acting as a single unit. Position the wide-open clip across the defect at 90 degrees to the defect. Gently push the clip-endoscope unit as one unit while applying gentle suction to collapse the lumen so that as much tissue away from the edge of perforation as possible could be grasped while slowly closing the clip. More Tips for Clips Confirm satisfactory clip closure of the perforation with approximation of the edges before deployment of the clip. Be patient while applying a clip because a misplaced clip to one edge of the perforation could lead to difficulty in applying additional clips for satisfactory closure. Copyright 2015 American College of Gastroenterology 13
14 Tips for Clips 3 Place additional clips from top-todown in linear perforations or left-to- to right in circular perforations after satisfactory application of the first clip, which is the most critical component of closure. Consider pinch just lateral l to edge of defect to bring sides closer together Copyright 2015 American College of Gastroenterology 14





15 Clipping of Post-op Sigmoid Anastamotic Fistula Lots of clips may be needed Early recognition and prompt management Copyright 2015 American College of Gastroenterology 15
16 Clip Caveats I. Avoid panic. Be calm and steady for proper use of the equipment by you and your assistant. Keep the endoscope close to the site of perforation Distance will interfere with proper clip control Minimize i i air insufflation Clip Caveats II. Avoid stretching the tissue by pushing the clip against the wall as this limits successful approximation of the edges together. Avoid hasting deployment of the first clip without checking that both the edges were successfully approximated as this will result in a wasted deployment to one edge of the perforation without complete tissue apposition of both edges of perforation. Copyright 2015 American College of Gastroenterology 16





17 OTSC Closure OTSC Closure Copyright 2015 American College of Gastroenterology 17


18 Overstitch closure Special Imaging Considerations for Colon EMR Recognizing lesions containing high grade dysplasia that t will require good submucosal lift Detection serrated lesions Detecting margins for complete polypectomy Copyright 2015 American College of Gastroenterology 18




19 Copyright 2015 American College of Gastroenterology 19





20 What about SSA detection? Beyond Polyp Recognition-Complete Resection Potential ti future key quality targett Advanced imaging may lead to improvement Copyright 2015 American College of Gastroenterology 20
21 Delineation of Margins: Can OCE Help us Leave Less Behind? Optical contrast appears to facilitate recognition of borders. Data confirming that optical contrast assisted resection reduces incomplete polypectomy rates has yet to be obtained. Demarcation of Margins: Duodenal Adenoma Copyright 2015 American College of Gastroenterology 21


22 Poor Margin Assessment Leads to Poor Outcome: Incomplete polypectomy U of Minnesota: 27% of interval cancers Sawhney Gastro 2006;131: Pink Rim Accentuates Polyp Margins Copyright 2015 American College of Gastroenterology 22




23 Imaging Critical to Improve Complete Resection 1. Type 3 mucosal and vessel pattern requires saline EMR or ESD to ensure deep margin 2. Lateral margin delineation assistance Low Tech Margins Assessment Small amounts of contrast dye indigo carmine added to saline cushion may separate pits and facilitate examination of margins post-polyp resection Copyright 2015 American College of Gastroenterology 23




24 The Iceberg Effect NBI Reveals Flat Adenomatous Projections of Polyp Visible on White Light Polypectomy of Tubular Adenoma Post-polypectomy inspection of polyp border: normal pit pattern confirms complete resection Copyright 2015 American College of Gastroenterology 24


25 Accentuation of Normal Pit Pattern to Confirm Clear Margins Putting All the Tools Together: 69-year-old male presented with depression, mild weight loss and chronic constipation without blood No prior colorectal screening Normal CBC, iron studies, metabolic panel No family history of GI cancer Copyright 2015 American College of Gastroenterology 25





26 Index Colonoscopy Findings Proximal right colon 3 cm on fold Copyright 2015 American College of Gastroenterology 26





27 Copyright 2015 American College of Gastroenterology 27





28 Hmmmm! Splenic flexure giant polypoid soft mass CT scan Copyright 2015 American College of Gastroenterology 28




29 Cap Fitted Colonoscopy Kondo S. et al Am J Gastro 2007;102: Increased overall polyp detection 49.3% vs 39.1% p< 0.05 Decreased cecal intubation time NBI Characterization Anterograde Copyright 2015 American College of Gastroenterology 29



30 Retrograde View Post Injection with Capped Gastroscope Piecemeal resection of edges including normal mucosa Copyright 2015 American College of Gastroenterology 30



31 Coagrasper hemostasis of prominent exposed vessels Post-retrieval-all TV adenoma Copyright 2015 American College of Gastroenterology 31


32 A Long Time Later... Copyright 2015 American College of Gastroenterology 32
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Do any benign polyps require an operation?
 Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Finding and Removing Difficult Polyps (safely)
") Finding and Removing Difficult Polyps (safely) David Lieberman MD Chief, Division of Gastroenterology and Hepatology Oregon Health and Science University Colonoscopy Clouds Interval Cancers Interval Cancer:
Finding and Removing Difficult Polyps (safely) David Lieberman MD Chief, Division of Gastroenterology and Hepatology Oregon Health and Science University Colonoscopy Clouds Interval Cancers Interval Cancer:
Rectal EMR: Techniques and Tips
 Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Benchmarking For Colonoscopy. Technology and Technique to Improve Adenoma Detection
 Benchmarking For Colonoscopy Technology and Technique to Improve Adenoma Detection Objectives 1. Review the latest data on performance characteristics and efficacy for colon cancer prevention 2. Highlight
Benchmarking For Colonoscopy Technology and Technique to Improve Adenoma Detection Objectives 1. Review the latest data on performance characteristics and efficacy for colon cancer prevention 2. Highlight
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Improving you ADR. Robert Enns Colonoscopy Education Day October 2018
 Improving you ADR Robert Enns Colonoscopy Education Day October 2018 ADR Applying to CSP Assume 50% ADR in FIT positive patients Out of 40 patients only 20 will have polyps Out of 20 likely 15 will be
Improving you ADR Robert Enns Colonoscopy Education Day October 2018 ADR Applying to CSP Assume 50% ADR in FIT positive patients Out of 40 patients only 20 will have polyps Out of 20 likely 15 will be
(Hot Snare) Polypectomy : Best Practice
 Polypectomy : Best Practice") (Hot Snare) Polypectomy : Best Practice Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Tuesday October 2 nd 1440-1515 X X X
(Hot Snare) Polypectomy : Best Practice Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Tuesday October 2 nd 1440-1515 X X X
Shou Jiang Tang, MD, FASGE. Director of Endoscopic Research Professor in Medicine
 Shou Jiang Tang, MD, FASGE Director of Endoscopic Research Professor in Medicine Through-the-scope clipping devices Over-the-scope clipping devices First reported clipping device Hayshi T, Yonezawa M,
Shou Jiang Tang, MD, FASGE Director of Endoscopic Research Professor in Medicine Through-the-scope clipping devices Over-the-scope clipping devices First reported clipping device Hayshi T, Yonezawa M,
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working Group chair: Michal F. Kaminski, Poland
 Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
COLON: Innovations 3 steps, 3 parts..
 COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
Introduction. Piecemeal EMR (EPMR) Symposium
 Symposium") Symposium Symposium II - Lower GI : Colonoscopy Issues in 2015 Resection of Large Polyps Using Techniques other than Endoscopic Submucosal Dissection: Piecemeal Resection, Underwater Endoscopic Mucosal
Symposium Symposium II - Lower GI : Colonoscopy Issues in 2015 Resection of Large Polyps Using Techniques other than Endoscopic Submucosal Dissection: Piecemeal Resection, Underwater Endoscopic Mucosal
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Improving Your Adenoma Detection Rate
 Improving Your Adenoma Detection Rate JILL TINMOUTH, ASSOCIATE PROFESSOR, UNIVERSITY OF TORONTO JERRY MCGRATH, ASSOCIATE PROFESSOR, MEMORIAL UNIVERSITY OF NEWFOUNDLAND FEB. 11 2017 X CanMEDS Roles Covered
Improving Your Adenoma Detection Rate JILL TINMOUTH, ASSOCIATE PROFESSOR, UNIVERSITY OF TORONTO JERRY MCGRATH, ASSOCIATE PROFESSOR, MEMORIAL UNIVERSITY OF NEWFOUNDLAND FEB. 11 2017 X CanMEDS Roles Covered
Research Article Endoscopic Management of Nonlifting Colon Polyps
 Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
Factors for Endoscopic Submucosal Dissection in Early Colorectal Neoplasms: A Single Center Clinical Experience in China
 ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Title Description Type / Priority
 Merit-based Incentive Payment system (MIPS) 2019 Qualified Clinical Data Registry (QCDR) Measure Specifications Summary Listing of QCDR measures supported by the NHCR Measure # NHCR4 NHCR5 GIQIC12 GIQIC15
Merit-based Incentive Payment system (MIPS) 2019 Qualified Clinical Data Registry (QCDR) Measure Specifications Summary Listing of QCDR measures supported by the NHCR Measure # NHCR4 NHCR5 GIQIC12 GIQIC15
Feasibility of endoscopic mucosa-submucosa clip closure method (with video)
") Feasibility of endoscopic mucosa-submucosa clip closure method (with video) Authors Toshihiro Nishizawa 1, Shigeo Banno 2, Satoshi Kinoshita 1,HidekiMori 2, Yoshihiro Nakazato 3,YuichiroHirai 2,Yoko Kubosawa
Feasibility of endoscopic mucosa-submucosa clip closure method (with video) Authors Toshihiro Nishizawa 1, Shigeo Banno 2, Satoshi Kinoshita 1,HidekiMori 2, Yoshihiro Nakazato 3,YuichiroHirai 2,Yoko Kubosawa
Carol A. Burke, MD, FACG
 Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Aberrant crypt foci, chromocolonoscopy for, 539 540 Absorptive stains, for chromocolonoscopy, 522 524 Accessories, for colonoscopy, 680 684
Note: Page numbers of article titles are in boldface type. A Aberrant crypt foci, chromocolonoscopy for, 539 540 Absorptive stains, for chromocolonoscopy, 522 524 Accessories, for colonoscopy, 680 684
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
GIQIC18 Appropriate follow-up interval of not less than 5 years for colonoscopies with findings of 1-2 tubular adenomas < 10 mm
 GI Quality Improvement Consortium, Ltd. (GIQuIC) 1 Following is an overview of the clinical quality measures in GIQuIC that can be reported to CMS for the Quality performance category of the Merit-Based
GI Quality Improvement Consortium, Ltd. (GIQuIC) 1 Following is an overview of the clinical quality measures in GIQuIC that can be reported to CMS for the Quality performance category of the Merit-Based
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
The Importance of Complete Colonoscopy and Exploration of the Cecal Region
 The Importance of Complete Colonoscopy and Exploration of the Cecal Region Kuangi Fu, Takahiro Fujii, Takahisa Matsuda, and Yutaka Saito 2 2.1 The Importance of a Complete Colonoscopy Ever since case-control
The Importance of Complete Colonoscopy and Exploration of the Cecal Region Kuangi Fu, Takahiro Fujii, Takahisa Matsuda, and Yutaka Saito 2 2.1 The Importance of a Complete Colonoscopy Ever since case-control
Spartan Medical Research Journal
 Spartan Medical Research Journal Research at Michigan State University College of Osteopathic Medicine Volume 2 Number 2 Winter, 2017 Pages 14-21 Title: Endoscopic Combined Snare-Forceps Technique for
Spartan Medical Research Journal Research at Michigan State University College of Osteopathic Medicine Volume 2 Number 2 Winter, 2017 Pages 14-21 Title: Endoscopic Combined Snare-Forceps Technique for
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom
 Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Quality in Endoscopy: Can We Do Better?
 Quality in Endoscopy: Can We Do Better? Erik Rahimi, MD Assistant Professor Division of Gastroenterology, Hepatology, and Nutrition UT Health Science Center at Houston McGovern Medical School Ertan Digestive
Quality in Endoscopy: Can We Do Better? Erik Rahimi, MD Assistant Professor Division of Gastroenterology, Hepatology, and Nutrition UT Health Science Center at Houston McGovern Medical School Ertan Digestive
The utility of a novel colonoscope with retroflexion for colorectal endoscopic submucosal dissection
 Original article The utility of a novel colonoscope with retroflexion for colorectal endoscopic submucosal dissection Authors Hidenori Tanaka 1,ShiroOka 2, Shinji Tanaka 1, Katsuaki Inagaki 2,YukiOkamoto
Original article The utility of a novel colonoscope with retroflexion for colorectal endoscopic submucosal dissection Authors Hidenori Tanaka 1,ShiroOka 2, Shinji Tanaka 1, Katsuaki Inagaki 2,YukiOkamoto
Colorectal Cancer Screening: Colonoscopy, Potential and Pitfalls. Disclosures: None. CRC: still a major public health problem
 Colorectal Cancer Screening: Colonoscopy, Potential and Pitfalls Disclosures: None Jonathan P. Terdiman, M.D. Professor of Clinical Medicine University of California, San Francisco CRC: still a major public
Colorectal Cancer Screening: Colonoscopy, Potential and Pitfalls Disclosures: None Jonathan P. Terdiman, M.D. Professor of Clinical Medicine University of California, San Francisco CRC: still a major public
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD)
 & Endoscopic Submucosal Dissection (ESD)") Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Retroflexion and prevention of right-sided colon cancer following colonoscopy: How I approach it
 Retroflexion and prevention of right-sided colon cancer following colonoscopy: How I approach it Douglas K Rex 1 MD, MACG 1. Indiana University School of Medicine Division of Gastroenterology/Hepatology
Retroflexion and prevention of right-sided colon cancer following colonoscopy: How I approach it Douglas K Rex 1 MD, MACG 1. Indiana University School of Medicine Division of Gastroenterology/Hepatology
Endoscopic Management of Perforations
 Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Prof Rupert Leong, Director of Endoscopy, Head of IBD Professor of Medicine UNSW, University of Sydney, Concord Hospital Australia IBDSydney
 10:30-10:50 25 Sept 2017 Monday A-PSDE / WEO Colorectal Cancer Screening Committee (CRCSC) Meeting Room S228 (2/F) Prof Rupert Leong, Director of Endoscopy, Head of IBD Professor of Medicine UNSW, University
10:30-10:50 25 Sept 2017 Monday A-PSDE / WEO Colorectal Cancer Screening Committee (CRCSC) Meeting Room S228 (2/F) Prof Rupert Leong, Director of Endoscopy, Head of IBD Professor of Medicine UNSW, University
The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions
 Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Extreme Endo Toolbox. Slide 1. Slide 2. Slide 3. Outline. Endo Toolbox - Requisites
 Slide 1 Extreme Endo Toolbox Pramod Malik, MD, FACG, FASGE, AGAF, CPI Gastroenterology Associates of Tidewater Slide 2 Outline New Tools - Confocal endomicroscopy (Cellvizio) - HD/ NBI/ FICE - Ovesco clip
Slide 1 Extreme Endo Toolbox Pramod Malik, MD, FACG, FASGE, AGAF, CPI Gastroenterology Associates of Tidewater Slide 2 Outline New Tools - Confocal endomicroscopy (Cellvizio) - HD/ NBI/ FICE - Ovesco clip
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
GI Coding Updates. Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC
 GI Coding Updates Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC Copyright/Disclaimer 2014 AAPC text CPT copyright 2016 American Medical Association. All rights reserved.
GI Coding Updates Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC Copyright/Disclaimer 2014 AAPC text CPT copyright 2016 American Medical Association. All rights reserved.
Colorectal Cancer Screening
 Recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer Colorectal Cancer Screening Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D, Robertson
Recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer Colorectal Cancer Screening Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D, Robertson
How to remove BE cancer: EMR or ESD? Expected outcome
 How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
Local recurrence after endoscopic resection of colorectal tumors
 Int J Colorectal Dis (2009) 24:225 230 DOI 10.1007/s00384-008-0596-8 ORIGINAL ARTICLE Local recurrence after endoscopic resection of colorectal tumors Kinichi Hotta & Takahiro Fujii & Yutaka Saito & Takahisa
Int J Colorectal Dis (2009) 24:225 230 DOI 10.1007/s00384-008-0596-8 ORIGINAL ARTICLE Local recurrence after endoscopic resection of colorectal tumors Kinichi Hotta & Takahiro Fujii & Yutaka Saito & Takahisa
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Quality in Endoscopy and Cost Effective Practice
 Quality in Endoscopy and Cost Effective Practice Sunanda Kane, MD MSPH FACG Director, ACG Quality Council 1 What is Quality and/or Cost Effectiveness in an Endoscopic Practice? Value Equation Quality (Outcomes,
Quality in Endoscopy and Cost Effective Practice Sunanda Kane, MD MSPH FACG Director, ACG Quality Council 1 What is Quality and/or Cost Effectiveness in an Endoscopic Practice? Value Equation Quality (Outcomes,
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy
 Gut and Liver, Vol. 9, No. 1, January 2015, pp. 66-72 ORiginal Article Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy Sang Pyo Lee, In-Kyung Sung, Jeong Hwan Kim, Sun-Young
Gut and Liver, Vol. 9, No. 1, January 2015, pp. 66-72 ORiginal Article Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy Sang Pyo Lee, In-Kyung Sung, Jeong Hwan Kim, Sun-Young
The Natural History of Right-Sided Lesions
 The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
Merit-based Incentive Payment system (MIPS) 2018 Qualified Clinical Data Registry (QCDR) Measure Specifications
 2018 Qualified Clinical Data Registry (QCDR) Measure Specifications") Merit-based Incentive Payment system (MIPS) 2018 Qualified Clinical Data Registry (QCDR) Measure Specifications This document contains a listing of the clinical quality measures which the New Hampshire
Merit-based Incentive Payment system (MIPS) 2018 Qualified Clinical Data Registry (QCDR) Measure Specifications This document contains a listing of the clinical quality measures which the New Hampshire
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
Predict, Resect and discard : Yes we can! (at least in some hands)
") Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
T. Shono, 1 K. Ishikawa, 1 Y. Ochiai, 1 M. Nakao, 1 O. Togawa, 1 M. Nishimura, 1 S. Arai, 1 K. Nonaka, 2 Y. Sasaki, 2 and H. Kita 1. 1.
 International Surgical Oncology Volume 2011, Article ID 948293, 6 pages doi:10.1155/2011/948293 Clinical Study Feasibility of Endoscopic Submucosal Dissection: A New Technique for En Bloc Resection of
International Surgical Oncology Volume 2011, Article ID 948293, 6 pages doi:10.1155/2011/948293 Clinical Study Feasibility of Endoscopic Submucosal Dissection: A New Technique for En Bloc Resection of
2015 Winter School 대장종양성병변의진단과치료. Dong Kyung Chang. Sungkyunkwan University, School of Medicine Samsung Medical Center
 2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
Size of colorectal polyps determines time taken to remove them endoscopically
 Original article Size of colorectal polyps determines time taken to remove them endoscopically Authors Heechan Kang 1, Mo Hameed Thoufeeq 2 Institutions 1 Department of Medicine, Peterborough Hospitals
Original article Size of colorectal polyps determines time taken to remove them endoscopically Authors Heechan Kang 1, Mo Hameed Thoufeeq 2 Institutions 1 Department of Medicine, Peterborough Hospitals
Romanian Journal of Morphology and Embryology 2006, 47(3):
:") Romanian Journal of Morphology and Embryology 26, 7(3):239 23 ORIGINAL PAPER Predictive parameters for advanced neoplastic adenomas and colorectal cancer in patients with colonic polyps a study in a tertiary
Romanian Journal of Morphology and Embryology 26, 7(3):239 23 ORIGINAL PAPER Predictive parameters for advanced neoplastic adenomas and colorectal cancer in patients with colonic polyps a study in a tertiary
Quality indicators for colonoscopy and colonoscopist. Mirjana Kalauz Clinical Hospital Center Zagreb
 Quality indicators for colonoscopy and colonoscopist Mirjana Kalauz Clinical Hospital Center Zagreb Why is quality monitoring important in CRC screening programme? Quality adjustment in all endoscopic
Quality indicators for colonoscopy and colonoscopist Mirjana Kalauz Clinical Hospital Center Zagreb Why is quality monitoring important in CRC screening programme? Quality adjustment in all endoscopic
Traction-assisted colonic endoscopic submucosal dissection using clip and line: a feasibility study
 E51 Traction-assisted colonic endoscopic submucosal dissection using clip and line: a feasibility study Authors Institution Yasushi Yamasaki, Yoji Takeuchi, Noriya Uedo, Minoru Kato, Kenta Hamada, Kenji
E51 Traction-assisted colonic endoscopic submucosal dissection using clip and line: a feasibility study Authors Institution Yasushi Yamasaki, Yoji Takeuchi, Noriya Uedo, Minoru Kato, Kenta Hamada, Kenji
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
Technology and Interventions to Improve ADR
 Technology and Interventions to Improve ADR Aasma Shaukat, MD MPH, FACG GI Section Chief, Minneapolis VAMC Associate Professor, University of Minnesota Outline Why is quality important? Fundamentals of
Technology and Interventions to Improve ADR Aasma Shaukat, MD MPH, FACG GI Section Chief, Minneapolis VAMC Associate Professor, University of Minnesota Outline Why is quality important? Fundamentals of
Devices To Improve Colon Polyp Detection
 Devices To Improve Colon Polyp Detection ACG/VGS Regional Postgraduate Course Sep 10-11, 2016 Williamsburg, VA VIVEK KAUL, MD, FACG Segal-Watson Professor of Medicine Chief, Division of Gastroenterology
Devices To Improve Colon Polyp Detection ACG/VGS Regional Postgraduate Course Sep 10-11, 2016 Williamsburg, VA VIVEK KAUL, MD, FACG Segal-Watson Professor of Medicine Chief, Division of Gastroenterology
Colon Cancer Screening. Layth Al-Jashaami, MD GI Fellow, PGY 4
 Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate
 Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions
 Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Bowel Screening Colonoscopy in Glasgow How well are we doing? How well should we be doing? How can we evidence and improve performance?
 Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Cold snare piecemeal resection of colonic and duodenal polyps 1cm
 E508 THIEME Cold snare piecemeal resection of colonic and duodenal polyps 1cm Authors Neel Choksi 1, B. Joseph Elmunzer 2, Ryan W. Stidham 1, Dmitry Shuster 1, Cyrus Piraka 3 Institutions 1 Division of
E508 THIEME Cold snare piecemeal resection of colonic and duodenal polyps 1cm Authors Neel Choksi 1, B. Joseph Elmunzer 2, Ryan W. Stidham 1, Dmitry Shuster 1, Cyrus Piraka 3 Institutions 1 Division of
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
SAGES 2019 Flexible Endoscopy Course for Fellows
 Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease
 An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease Roy Soetikno, MD a, *, Silvia Sanduleanu, MD, PhD b, Tonya Kaltenbach, MD a KEYWORDS Inflammatory bowel disease Nonpolypoid
An Atlas of the Nonpolypoid Colorectal Neoplasms in Inflammatory Bowel Disease Roy Soetikno, MD a, *, Silvia Sanduleanu, MD, PhD b, Tonya Kaltenbach, MD a KEYWORDS Inflammatory bowel disease Nonpolypoid
Accepted Manuscript. En bloc resection for mm polyps to reduce post-colonoscopy cancer and surveillance. C. Hassan, M. Rutter, A.
 Accepted Manuscript En bloc resection for 10-20 mm polyps to reduce post-colonoscopy cancer and surveillance C. Hassan, M. Rutter, A. Repici PII: S1542-3565(19)30412-4 DOI: https://doi.org/10.1016/j.cgh.2019.04.022
Accepted Manuscript En bloc resection for 10-20 mm polyps to reduce post-colonoscopy cancer and surveillance C. Hassan, M. Rutter, A. Repici PII: S1542-3565(19)30412-4 DOI: https://doi.org/10.1016/j.cgh.2019.04.022
Endoscopic full-thickness resection in the colorectum with a novel over-the-scope device: first experience
 Original article 719 Endoscopic full-thickness resection in the colorectum with a novel over-the-scope device: first experience Authors Arthur Schmidt 1, *, Peter Bauerfeind 2, *, Christoph Gubler 2, Michael
Original article 719 Endoscopic full-thickness resection in the colorectum with a novel over-the-scope device: first experience Authors Arthur Schmidt 1, *, Peter Bauerfeind 2, *, Christoph Gubler 2, Michael
THE INS & OUTS OF COLONOSCOPY
 THE INS & OUTS OF COLONOSCOPY INSERTION TIPS & FEATURES OF HIGH-QUALITY WITHDRAWAL C A M E R O N B E L L R O Y A L N O R T H S H O R E H O S P I T A L C H A I R, N E T I N A T I O N A L T C T L E A D WHY
THE INS & OUTS OF COLONOSCOPY INSERTION TIPS & FEATURES OF HIGH-QUALITY WITHDRAWAL C A M E R O N B E L L R O Y A L N O R T H S H O R E H O S P I T A L C H A I R, N E T I N A T I O N A L T C T L E A D WHY
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions
 Showa Univ J Med Sci 12(3), 253-258, September 2000 Original Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions Masaaki MATSUKAWA, Mototsugu FUJIMORI, Takahiko KOUDA,
Showa Univ J Med Sci 12(3), 253-258, September 2000 Original Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions Masaaki MATSUKAWA, Mototsugu FUJIMORI, Takahiko KOUDA,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Tips to Improve ADRs during Colonoscopy
 Tips to Improve ADRs during Colonoscopy Aasma Shaukat, MD, MPH, FACG GI Section Chief, Minneapolis VAMC Associate Professor, University of Minnesota Outline Why is quality important? Fundamentals of high-quality
Tips to Improve ADRs during Colonoscopy Aasma Shaukat, MD, MPH, FACG GI Section Chief, Minneapolis VAMC Associate Professor, University of Minnesota Outline Why is quality important? Fundamentals of high-quality
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Colorectal cancer will soon surpass lung cancer as the
 GASTROENTEROLOGY 2011;140:1909 1918 CLINICAL Endoscopic Mucosal Resection Outcomes and Prediction of Submucosal Cancer From Advanced Colonic Mucosal Neoplasia ALAN MOSS,* MICHAEL J. BOURKE,* STEPHEN J.
GASTROENTEROLOGY 2011;140:1909 1918 CLINICAL Endoscopic Mucosal Resection Outcomes and Prediction of Submucosal Cancer From Advanced Colonic Mucosal Neoplasia ALAN MOSS,* MICHAEL J. BOURKE,* STEPHEN J.
EXPERT WORKING GROUP Surveillance after neoplasia removal. Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum
 EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
Short and longterm outcomes after endoscopic resection of malignant polyps.
 Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Digestive Health Southwest Endoscopy 2016 Quality Report
 Digestive Health 2016 Quality Report Our 2016 our quality and value management program focused on one primary area of interest: Performing high quality colonoscopy High quality Colonoscopy We selected
Digestive Health 2016 Quality Report Our 2016 our quality and value management program focused on one primary area of interest: Performing high quality colonoscopy High quality Colonoscopy We selected
How to treat early gastric cancer? Endoscopy
 How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
Colorectal Cancer Screening: A Clinical Update
 11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
Felix W. Leung 1,2,3. Editorial
 Editorial Incomplete resection after macroscopic radical endoscopic resection of T1 colorectal cancer should a paradigm-changing approach to address the risk be considered? Felix W. Leung 1,2,3 1 Sepulveda
Editorial Incomplete resection after macroscopic radical endoscopic resection of T1 colorectal cancer should a paradigm-changing approach to address the risk be considered? Felix W. Leung 1,2,3 1 Sepulveda