original article Turki AlAmeel MD FRCPC, Vincent Bain MD FRCPC, Gurpal Sandha MBBS FRCPC
|
|
|
- Melvyn Hopkins
- 6 years ago
- Views:
Transcription
1 original article Clinical application of a single-operator direct visualization system improves the diagnostic and therapeutic yield of endoscopic retrograde cholangiopancreatography Turki AlAmeel MD FRCPC, Vincent Bain MD FRCPC, Gurpal Sandha MBBS FRCPC T AlAmeel, V Bain, G Sandha. Clinical application of a single-operator direct visualization system improves the diagnostic and therapeutic yield of endoscopic retrograde cholangiopancreatography. Can J Gastroenterol 2013;27(1): l application clinique d un système de visualisation directe par un seul opérateur améliore le rendement diagnostique et thérapeutique de la cholangiopancréatographie endoscopique rétrograde BACkGround: Single-operator cholangioscopy enables direct diagnostic visualization and therapeutic intervention in the biliary tree. There is increasing evidence of its clinical utility in the assessment of biliary strictures and treatment of difficult stones. objective: To describe the first reported Canadian experience with managing biliary disease using single-operator cholangioscopy. MeThodS: The present study was a retrospective analysis of data collected from all sequential patients undergoing single-operator cholangioscopy for assessment of biliary strictures and treatment of biliary stones. The main outcome measures were the ability to make an overall diagnosis of stricture (based on visual appearances and tissue histology), and to fragment and extract biliary stones. results: Thirty patients (17 women), mean age 66 years (range 41 to 89 years) underwent single-operator cholangioscopy. In biliary strictures (20 patients), overall accuracy for visual and tissue diagnosis was 84% and 81%, respectively. Successful electrohydraulic lithotripsy with stone clearance was achieved in 90% of the 10 patients who failed previous conventional therapy. The mean (± SD) procedure time was 61±21 min (range 20 min to 119 min). One patient developed mild postendoscopic retrograde cholangioscopy pancreatitis. ConCluSion: The results of this experience reaffirms the clinical utility and safety of single-operator cholangioscopy for the management of biliary pathology. Further improvements can be achieved with increasing operator experience and refinements in optical technology. key Words: Biopsy; Cholangioscopy; Lithotripsy; SpyGlass; Stone; Stricture The assessment of biliary strictures remains a significant challenge. Malignant strictures (cholangiocarcinoma) often grow longitudinally rather than in a radial fashion and, thus, large tumour masses are often absent on modalities such as abdominal ultrasound, computed tomography and magnetic resonance imaging (1). Inflammatory strictures (eg, primary sclerosing cholangitis [PSC]), especially with their potential for developing malignancy, are also equally difficult to accurately diagnose and follow. Current clinical practices, such as biliary brush cytology and endoscopic retrograde cholangiopancreatography (ERCP)-directed biopsy acquisition, have a less than optimal sensitivity of 33% to 58% (2-4). False-negative results can delay life-saving interventions (5). On the other hand, false positives can result in unnecessary surgical intervention, thereby increasing morbidity and health care costs. The need for improved efforts to obtain accurate and directed tissue diagnosis cannot be overemphasized. To enable direct visualization and have the ability to perform biopsies of lesions within the bile duct, flexible cholangioscopes were developed in the 1990s and have been used in a procedure often historique : La cholangioscopie par un seul opérateur permet une visualisation diagnostique immédiate et une intervention thérapeutique directement dans l arbre biliaire. Les données probantes s accumulent pour en étayer l utilité clinique dans l évaluation des rétrécissements biliaires et le traitement des calculs complexes. objectif : Décrire la première expérience canadienne déclarée sur la prise en charge d une maladie biliaire à l aide d une cholangioscopie par un seul opérateur. MÉThodoloGie : La présente étude était une analyse rétrospective des données colligées auprès de tous les patients séquentiels qui avaient subi une cholangioscopie par un seul opérateur pour évaluer les rétrécissements biliaires et le traitement des calculs biliaires. Les principales mesures d issue étaient la capacité de poser un diagnostic global de rétrécissement (d après l apparence visuelle et l histologie tissulaire) et de fragmenter et extraire les calculs biliaires. résultats : Trente patients (17 femmes), d un âge moyen de 66 ans (plage de 41 à 89 ans) ont subi une cholangioscopie par un seul opérateur. En cas de rétrécissement biliaire (20 patients), la précision globale du diagnostic visuel et tissulaire s élevait à 84 % et à 81 %, respectivement. On a observé une lithotripsie électrohydraulique avec clairance des calculs chez 90 % des dix patients dont la thérapie classique avait échoué auparavant. L intervention avait une durée moyenne (±ÉT) de 61±21 min (plage de 20 minutes à 119 minutes). Un patient a présenté une pancréatite cholangioscopique rétrograde bénigne après l endoscopie. ConCluSion : Les résultats de cette expérience réitèrent l utilité et l innocuité cliniques d une cholangioscopie par un seul opérateur pour prendre en charge une pathologie biliaire. Les améliorations peuvent être directement proportionnelles à l expérience de l opérateur et au perfectionnement de la technologie optique. referred to as mother-baby cholangioscopy (6). The procedure requires two experienced endoscopists, one to work the mother duodenoscope and the other to operate the baby cholangioscope. The latter is introduced through the working channel of the mother scope. This has proven to be a cumbersome procedure and has not achieved widespread use. In addition, the baby cholangioscope only has two-way tip deflection capability, limiting its manoeuvreability, and is subject to increased repair costs because of its fragility. The SpyGlass (Boston Scientific, USA) cholangioscopy system is a relatively recent advance that enables one endoscopist to manoeuvre both the duodenoscope and the cholangioscope, enabling direct visualization of the bile duct. Studies have recently documented its clinical usefulness not only for the diagnosis of strictures (with biopsy) but also for therapeutic (with electrohydraulic lithotripsy [EHL] or laser lithotripsy) intervention of biliary stones refractory to conventional treatment (7-11). The objective of the present study was to describe our experience with SpyGlass cholangioscopy in managing biliary disease. Division of Gastroenterology, University of Alberta Hospital, Edmonton, Alberta Correspondence: Dr Gurpal Sandha, Division of Gastroenterology, University of Alberta Hospital, Zeidler Ledcor Centre, 130 University Campus, Edmonton, Alberta T6G 2X8. Telephone , fax , gurpal.sandha@ualberta.ca Received for publication May 23, Accepted June 4, 2012 Can J Gastroenterol Vol 27 No 1 January Pulsus Group Inc. All rights reserved 15


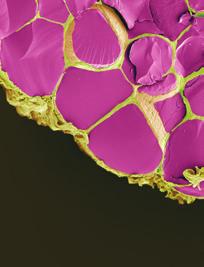
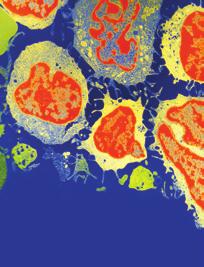
2 AlAmeel et al Figure 1) Common bile duct stricture in a patient with primary sclerosing cholangitis exhibiting smooth cicatrization without the presence of any mass lesion MeThodS The present analysis was an observational study evaluating data from all patients who underwent diagnostic and/or therapeutic SpyGlass cholangioscopy at the University of Alberta Hospital in Edmonton, Alberta. All procedures were performed by two experienced biliary endoscopists (VB and GS), with individual ERCP experience of >12 years, having performed >2000 procedures each. The SpyGlass cholangioscopy system is a single-operator, direct visualization system that is introduced via the working channel of a standard duodenoscope (Olympus TJF180 therapeutic duodenoscope, Olympus America Inc, USA). The SpyGlass system consists of a disposable SpyScope access and delivery catheter, a 10 Fr catheter with four-way tip deflection capability, channels for accommodating optical and accessory devices and two channels for saline irrigation, the reusable SpyGlass direct visualization optical probe for visual examination of the pancreaticobiliary ducts and the disposable SpyBite biopsy forceps for tissue acquisition (7). The generator and probes for EHL and laser lithotripsy are additional accessories acquired separately (see below). outcomes and procedure The data were analyzed using an intent-to-diagnose approach for the assessment of biliary strictures and an intent-to-treat approach for biliary stones. Biliary strictures: Using the intent-to-diagnose approach for biliary strictures, the ability of SpyGlass to aid in making a visual diagnosis and then to biopsy any mucosal abnormality identified using the SpyBite forceps was assessed. The inability to make a visual diagnosis or to obtain biopsies, where indicated, was considered a failure of the procedure. The visual diagnosis was categorized as a malignant stricture (ie, cholangiocarcinoma) or a stricture resulting either from a benign, inflammatory process (ie, PSC) or from extrinsic compression (eg, carcinoma of the gallbladder, pancreatic adenocarcinoma or autoimmune pancreatitis). The visual diagnosis with SpyBite tissue histology was individually correlated with surgical histology or clinical follow-up and SpyBite biopsy diagnosis with either surgical histology, where available, or clinical follow-up. The accuracy of both the visual ability of SpyGlass cholangioscopy to establish a diagnosis as well as the ability of SpyBite biopsies to confirm histology has been reported by previous investigators (7-9). 16 Figure 2) A series of images from a patient with primary sclerosing cholangitis with a mass lesion. A Normal distal bile duct. B The beginning of a mural-based mass. C and d The mass is clearly visible and was biopsied with SpyBite forceps (Boston Scientific, USA) An attempt was made to make an overall SpyGlass diagnosis in all patients. This was the final impression of the endoscopist and was based on information obtained from both the visual and tissue diagnosis. This overall diagnosis was made based on the most concerning interpretation. For example, if a stricture was considered to be malignant by visual diagnosis and the biopsy was reported benign and/or inflammatory, a diagnosis of a malignant stricture was entertained as the overall SpyGlass diagnosis. Because the present study was observational in nature and reports the institution s early experience with SpyGlass cholangioscopy, a follow-up time period was not defined a priori but simply reported at the time of preparing the manuscript. Figure 1 is an example of PSC in which only a visual diagnosis was made. The mass lesion shown in Figure 2 was found in a patient with PSC who underwent SpyBite biopsy. Figure 3 is an example of an apple-core lesion that appeared malignant on visual inspection and then underwent SpyBite biopsy. Biliary stones: For biliary stone lithotripsy, an EHL pulse generator (Northgate Technologies Inc, USA) was used. The intent-to-treat approach involved an attempt to visualize and fracture the targeted biliary stone(s) and eventually extract all fragments with the aim of bile duct clearance. The settings used on the pulse generator were as follows: power 30 W to 50 W, with a maximum of up to 100 W, if needed; and frequency 10 pulses/s to 30 pulses/s for 2 s. EHL is performed most effectively while irrigating with normal saline. After stone fragmentation, the need for additional intervention to aid in stone extraction (eg, balloon dilation of the sphincter and/or the use of balloon and/or basket extraction catheters) was left to the discretion of the endoscopist. If repeat ERCP was needed for EHL, this was considered in the analysis as a separate procedure, but if the repeat ERCP was simply to extract stones without the need for SpyGlass and/or EHL, these repeat procedures were not included in the final analysis. Inability to fracture the stone(s) with EHL was considered a failure of SpyGlass cholangioscopy. Figure 4 presents the various steps in the process of EHL with stone fracture and extraction of fragments from the bile duct. Can J Gastroenterol Vol 27 No 1 January 2013
 66 (41 89) Sex, male/female, n/n 13/17 biliary stricture (n=20) Anatomical location, n Distal")
 Achieved, n 20 Sensitivity, % 86 Specificity, % 85 biliary stones (n=10) Indication, n")
3 SpyGlass cholangioscopy improves diagnostic and therapeutic ERCP Figure 3) Cholangioscopic view of a malignant-appearing stricture exhibiting an apple-core lesion TAblE 1 baseline patient demographics with clinical characteristics and procedure outcome Patients, n 30 Age, years, mean (range) 66 (41 89) Sex, male/female, n/n 13/17 biliary stricture (n=20) Anatomical location, n Distal one-third of bile duct 5 Proximal two-thirds of bile duct 15 SpyGlass* visual diagnosis (see Table 2) Achieved, n 19 Sensitivity, % 83 Specificity, % 84 SpyBite* tissue diagnosis (see Table 3) Achieved, n 16 Sensitivity, % 40 Specificity, % 100 Overall SpyGlass diagnosis (see Table 4) Achieved, n 20 Sensitivity, % 86 Specificity, % 85 biliary stones (n=10) Indication, n Multiple/large/faceted stone(s) 3 Impacted stone(s) 3 Stone(s) above stricture 2 Electrohydraulic lithotripsy 8 Stone extraction, n (>1 may apply) Balloon extraction 8 Basket extraction 2 Dilation assisted stone extraction 2 Duration of procedure, min, mean ± SD (range) 61±20 (20 119) *Boston Scientific, USA; Visualization could not be achieved in one patient; No lesion identified in four patients; therefore, no biopsy attempted; One patient had no stone identified and, in another patient, there was difficulty visualizing the stone. Electrohydraulic lithotripsy was not performed in these two patients There was no funding available for the present study and it was approved by the local institutional health research ethics board. Figure 4) These images reveal the steps during electrohydraulic lithotripsy (EHL) of a large biliary stone. A Cholangioscopic view of the stone with EHL probe visible. B Initial fracture site in the stone. C Fragmentation of the stone with sequential EHL applications. d Extraction of fragments with balloon-extraction catheter All patients who underwent SpyGlass cholangioscopy underwent at least one previous ERCP with sphincterotomy and/or stent placement, either by one of the two study endoscopists or by the referring endoscopist. The SpyGlass procedures were planned electively and not performed on an ad hoc basis, in part, because the infection control policy at the institution requires cleansing and disinfection of the reusable SpyGlass fibreoptic probe at least 24 h before the procedure. All cholangioscopy procedures were performed under general anesthesia because prolonged procedures were anticipated and operators preferred not to have suboptimal sedation become a potential explanation for inadequate procedure performance. Statistical analysis Descriptive statistics included mean, SD and range. Statistical analysis of the data with calculation of sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) was performed using two-way contingency table analysis. results In the first 12 months (starting April 2011), 30 patients (17 women) with a mean age of 66 years (range 41 to 89 years) underwent ERCP with SpyGlass cholangioscopy. The mean (± SD) procedure time for the entire cohort was 61±20 min (range 20 min to 119 min). Table 1 summarizes the patient demographics and procedure indications, along with outcomes of intervention and corroborating information where available. The data were analyzed on an intention-to-diagnose and/or intent-to-treat basis. The two main indications for SpyGlass cholangioscopy were assessment of undiagnosed biliary strictures and EHL of biliary stones that were refractory to previous attempts with conventional modalities. The analysis of the results for these indications will be discussed separately. Can J Gastroenterol Vol 27 No 1 January
4 AlAmeel et al TAblE table describing the relationship between a visual diagnosis made during SpyGlass* cholangioscopy and verified against tissue diagnosis (Spybite* and/or surgical histology, where available) and clinical follow-up Tissue diagnosis (Spybite and/or surgical histology) and clinical follow-up Malignant benign/extrinsic Total SpyGlass visual diagnosis Malignant Benign/extrinsic Total *Boston Scientific, USA TAblE table describing the relationship between Spybite* tissue diagnosis verified against surgical histology, where available, and clinical follow-up Surgical histology and clinical follow-up Malignant benign/extrinsic Total SpyBite tissue diagnosis Malignant Benign/extrinsic Total *Boston Scientific, USA Biliary stricture assessment Of the 30 patients, 20 (67%) with a mean age of 64 years (range 41 to 82 years) were referred for assessment of biliary strictures. There were 12 women (60%). The location of stricture was in the distal one-third of the bile duct in five patients and in the proximal two-thirds in the remaining 15 patients. The mean procedure time was 55±16 min (range 20 min to 87 min). The mean follow-up period was five months (range two to 12 months). Only four patients had corroborating surgical histology available. Three other patients died within the follow-up period, presumably of malignant disease, although confirmation by autopsy was not available. SpyGlass visual diagnosis: The overall success of SpyGlass cholangioscopy in identifying the biliary stricture and making a visual diagnosis with respect to location, length and surface characteristics was 95% (19 of 20 patients). A distal stricture could not be visualized in one patient. The sensitivity (83%), specificity (84%), PPV (71%), NPV (91%) and overall accuracy (84%) of the ability of SpyGlass to make a visual diagnosis are shown in Table 2. SpyBite tissue diagnosis: Of the 20 patients, SpyBite biopsies were attempted and obtained in 16 patients. Biopsies were not performed in four patients in whom no obvious mucosal abnormality was apparent. The sensitivity (40%), specificity (100%), PPV (100%), NPV (78%) and overall accuracy (81%) of SpyBite biopsies to confirm the visual diagnosis are shown in Table 3. overall SpyGlass diagnosis: All 20 patients who underwent SpyGlass cholangioscopy for biliary strictures were included. The sensitivity (86%), specificity (85%), PPV (75%), NPV (92%) and overall accuracy (85%) of the ability of SpyGlass cholangioscopy to make an overall diagnosis are shown in Table 4. Biliary stone management Ten patients were referred for EHL for difficult stones. These patients were generally older (mean age 72 years, range 52 to 89 years) and sex was more evenly distributed (five females [50%]) than the biliary stricture cohort. Furthermore, the mean procedure time was longer for this group (72±25 min, range 36 min to 119 min). The indications for EHL in these patients were impacted stones, multiple large and faceted stones, and stones situated above a biliary stricture. The overall success with an intent-to-treat approach was 90% (nine of 10 patients). EHL was attempted and successful in eight of 18 TAblE table describing the overall SpyGlass* impression (SpyGlass visual diagnosis and Spybite* tissue diagnosis) verified against surgical histology, where available, and/or clinical follow-up Surgical histology and/or clinical follow-up Malignant benign/extrinsic Total Overall SpyGlass diagnosis Malignant Benign/extrinsic Total *Boston Scientific, USA nine patients (89%), and eventual clearance of the duct was achieved in all patients. No patient required more than one SpyGlass or EHL session, although one patient with multiple large stones underwent a repeat ERCP for extraction of stone fragments and duct clearance. In one patient referred for a reportedly large stone, a stone could not be visualized despite cholangiography and cholangioscopy. No subsequent intervention has been performed in this patient in 11 months of follow-up. One patient had a 1 cm stone situated distally in a dilated bile duct. Adequate visualization was never achieved and, because EHL could not be performed, this was considered to be a failure in the intent-to-treat analysis. The stone was removed during the same procedure after balloon dilation of the sphincter and may not have initially been a good indication for SpyGlass. Complications There has been no major complication associated with SpyGlass cholangioscopy in our experience. One patient developed post-ercp pancreatitis and recovered well with conservative treatment. One patient with cholangiocarcinoma developed an altered level of consciousness and acute urinary retention 24 h after the procedure and died three days later. An autopsy was not performed and it remains unclear whether the events were related to the SpyGlass procedure. discussion Evaluation of undetermined biliary strictures remains one of the most challenging tasks in pancreaticobiliary endoscopy. Conventional methods of investigation, including cross-sectional abdominal imaging, are poor at accurately defining benign and/or malignant lesions of the bile duct. Attempts at obtaining tissue for diagnosis by ERCP with brush cytology and/or ERCP-directed forceps biopsies within the bile duct have not yielded consistent and widely applicable results (2-4). Even the initial promise of endoscopic ultrasound-guided fine-needle aspiration has not translated into widespread use despite favourable results with respect to sensitivity and specificity (12-14). Direct intraductal visualization of biliary pathology has long been recognized as the best way to evaluate strictures. Mother-baby (also known as mother-daughter ) biliary endoscopy has been in clinical use for many years (6). However, this procedure also has not seen widespread acceptance, in part, because of the need for two endoscopists. To overcome this particular disadvantage, the SpyGlass single-operator direct visualization system was devised and first clinically tested in 2007 by Chen and Pleskow (7). Since then, various groups have reported their initial experience and success, although only a handful of these studies have collected data in a prospective manner (8,10). In these initial years of investigation with SpyGlass, several outcome measures have been evaluated. One of these is procedural success, which has been reported by most investigators to be significantly greater than 90% (7-11). The criteria to diagnose strictures have focused not only on the ability of SpyGlass cholangioscopy to identify the stricture and make a visual diagnosis (sensitivity and specificity ranging between 71% and 95%, and 79% and 100%, respectively) but also on the ability of SpyBite forceps biopsies to confirm the initial visual diagnosis (sensitivity and specificity ranging between 49% and 82%, and 82% and 98%, respectively) (7-11). Our results are also Can J Gastroenterol Vol 27 No 1 January 2013
5 SpyGlass cholangioscopy improves diagnostic and therapeutic ERCP consistent with these published data. Furthermore, the accuracy of SpyGlass in being able to make an overall diagnosis is 85%. This is certainly a significant improvement from the existing standard of care, which includes bile duct brushings and, less often, attempts with ERCP-guided biopsy. One of the limitations with analyses relating to biliary strictures with SpyGlass cholangioscopy is the consistent lack of a corroborating gold standard for verification of the diagnosis. It is easy to compare SpyGlass intervention (visual and/or biopsy results) against surgical histology, where available; however, as is more common, a vast majority of these patients are deemed inoperable candidates. This leaves investigators to assume the presence of malignancy based on patient survival rather than actual histology. The sensitivity of SpyBite tissue diagnosis in our study (40%) was less than optimal, and may be explained by the relatively low number of cases and also by the fact that these data are the result of our initial experience with SpyGlass cholangioscopy. We believe that this is likely to improve with increasing experience. Our initial results are comparable with the early experience of other investigators who have had a similarly low sensitivity of SpyBite tissue diagnosis as reported in a recent multicentre registry (9). Moreover, in benign strictures of the bile duct, such as PSC, similar corroborating histology is usually unavailable. Prolonged survival, usually >6 months, is assumed to indicate benign disease. This lack of a comparative gold standard is one of the limitations of our study, as it has been for previous investigators. The published results of intention-to-treat analyses of stone fragmentation and extraction using SpyGlass cholangioscopy are even better, with reported success rates of 92% to 100% (9,10). This is significant given that these particular stones had previously failed conventional attempts at extraction and could have undergone more invasive interventions, including open bile duct exploration, for extraction. Our 90% success rate with EHL for stone fragmentation and subsequent extraction is also consistent with data reported in the literature. SpyGlass cholangioscopy has certainly proven to be effective in the investigation of biliary strictures and treatment of biliary stones. However, there are certain technical limitations that warrant mention. This is a fibreoptic technology and image quality has been one of the major drawbacks, especially when compared with imaging using mother-baby video cholangioscopes. However, the development of high-definition video technology in the near future is inevitable and will certainly enhance image quality. Nonetheless, given the current constraints with this technology, and that these procedures are time consuming, visualization can be optimized by adequate irrigation and proper drainage and suctioning through a generous sphincterotomy. This, however, can sometimes be difficult proximal to a stricture. In our experience, free irrigation can be performed provided suctioning is performed by the assisting nurse with a syringe attached to the operating channel of the SpyScope access catheter. This can eliminate debris and improve image quality. We also believe that the distal bile duct is the most technically challenging area to visualize. This likely occurs because the tip of the SpyScope access catheter and, hence, the SpyGlass probe, abuts the wall of the bile duct as it straightens coming through the distal bile duct. Some investigators recommend examining the distal bile duct in a long ERCP position so as to align the access catheter with the long axis of the bile duct and position it in the middle of the lumen. Our study was not a prospective controlled analysis but rather an observational study in which we assessed data from each consecutive patient who underwent SpyGlass cholangioscopy. This design is bound to introduce potential bias in making a visual diagnosis if the clinical history and investigations are known to the endoscopist. This bias could be excluded if the endoscopist performing the procedure is blinded to clinical information. However, because this was an observational study involving a new technical procedure, we believed that the endoscopist should have as much clinical information available as possible to maximize the diagnostic and therapeuitc yield of SpyGlass cholangioscopy. ConCluSion SpyGlass cholangioscopy is a significant advance in the direct evaluation of the biliary tree and allows for a single endoscopist to directly visualize and biopsy strictures for tissue diagnosis, and perform EHL fragmentation of stones that are otherwise refractory to conventional modalities of extraction such as balloon/basket extraction, mechanical lithotripsy and dilation-assisted balloon extraction. It is a time-consuming albeit safe procedure and efficacy is bound to improve with increases in operator experience and improvements in technology, especially those targeting optical optimization. disclosures: Dr Gurpal Sandha is a consultant for Boston Scientific. The other authors have no finacial disclosures or conflict of interest relevant to this article. This study was presented, in part, as an abstract at Canadian Digestive Diseases Week, February 23 to 27, 2012, Montreal, Quebec. references 1. Weber A, Schmid RM, Prinz C. Diagnostic approaches for cholangiocarcinoma. World J Gastroenterol 2008;14: Ponchon T, Gagnon P, Berger F, et al. Value of endobiliary brush cytology and biopsies for the diagnosis of malignant bile duct stenosis: Results of a prospective study. Gastrointest Endosc 1995;42: Howell DA, Parsons WG, Jones MA, Bosco JJ, Hanson BL. Complete tissue sampling of biliary strictures at ERCP using a new device. Gastrointest Endosc 1996;43: Glasbrenner B, Ardan M, Boeck W, et al. Prospective evaluation of brush cytology of biliary strictures during endoscopic retrograde cholangiopancreatography. Endoscopy 1999;31: Siddiqui AA, Mehendiratta V, Jackson W et al. Identification of cholangiocarcinoma by using the Spyglass Spyscope system for peroral cholangioscopy and biopsy collection. Clin Gastroenterol Hepatol 2012;10: Kozarek R, Kodama T, Tatsumi Y. Direct cholangioscopy and pancreatoscopy. Gastrointest Endosc Clin N Am 2003;13: Chen YK, Pleskow DK. SpyGlass single-operator peroral cholangiopancreatoscopy system for the diagnosis and therapy of bile-duct disorders: A clinical feasibility study (with video). Gastrointest Endosc 2007;65: Ramchandani M, Reddy DN, Gupta R, et al. Role of single-operator peroral cholangioscopy in the diagnosis of indeterminate biliary lesions: A single-center, prospective study. Gastrointest Endosc 2011;74: Chen YK, Parsi MA, Binmoeller KF, et al. Single-operator cholangioscopy in patients requiring evaluation of bile duct disease or therapy of biliary stones (with videos). Gastrointest Endosc 2011;74: Draganov PV, Lin T, Chauhan S, et al. Prospective evaluation of the clinical utility of ERCP-guided cholangiopancreatoscopy with a new direct visualization system. Gastrointest Endosc 2011;73: Kalaitzakis E, Webster GJ, Oppong KW, et al. Diagnostic and therapeutic utility of single-operator peroral cholangioscopy for indeterminate biliary lesions and bile duct stones. Eur J Gastroenterol Hepatol 2012;24: Röcsh T, Hofrichter K, Frimberger E, et al. ERCP or EUS for tissue diagnosis of biliary strictures? A prospective comparative study. Gastrointest Endosc 2004;60: Byrne MF, Gerke H, Mitchell RM, et al. Yield of endoscopic ultrasound-guided fine-needle aspiration of bile duct lesions. Endoscopy 2004;36: Fritscher-Ravens A, Broering DC, Knoefel WT, et al. EUS-guided fine-needle aspiration of suspected hilar cholangiocarcinoma in potentially operable patients with negative brush cytology. Am J Gastroenterol 2004;99: Can J Gastroenterol Vol 27 No 1 January















6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Single-operator cholangioscopy is useful for visual assessment of bile duct pathology
 Single-operator cholangioscopy is useful for visual assessment of bile duct pathology Finnur Mellemgaard, Rune B. Strandby, Julie Blockmann, Steen C. Kofoed, Lars B. Svendsen & Michael P. Achiam SUMMARY
Single-operator cholangioscopy is useful for visual assessment of bile duct pathology Finnur Mellemgaard, Rune B. Strandby, Julie Blockmann, Steen C. Kofoed, Lars B. Svendsen & Michael P. Achiam SUMMARY
The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
Endoscopic Management of Biliary Strictures. Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center
 Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Identification of Cholangiocarcinoma by Using the Spyglass Spyscope System for Peroral Cholangioscopy and Biopsy Collection
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:466 471 ENDOSCOPY CORNER Identification of Cholangiocarcinoma by Using the Spyglass Spyscope System for Peroral Cholangioscopy and Biopsy Collection ALI
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2012;10:466 471 ENDOSCOPY CORNER Identification of Cholangiocarcinoma by Using the Spyglass Spyscope System for Peroral Cholangioscopy and Biopsy Collection ALI
Making ERCP Easy: Tips From A Master
 Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
SMJ Singapore Medical Journal
 SMJ Singapore Medical Journal ONLINE FIRST PUBLICATION Online first papers have undergone full scientific review and copyediting, but have not been typeset or proofread. To cite this article, use the DOIs
SMJ Singapore Medical Journal ONLINE FIRST PUBLICATION Online first papers have undergone full scientific review and copyediting, but have not been typeset or proofread. To cite this article, use the DOIs
Comparison of digital versus fiberoptic cholangioscopy in patients requiring evaluation of bile duct disease or treatment of biliary stones
 ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Comparison of digital versus fiberoptic cholangioscopy in patients requiring evaluation of bile duct disease or treatment of biliary stones Ioannis
ORIGINAL ARTICLE Annals of Gastroenterology (2019) 32, 1-6 Comparison of digital versus fiberoptic cholangioscopy in patients requiring evaluation of bile duct disease or treatment of biliary stones Ioannis
Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful
 Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful Chronic Pancreatitis Using SpyGlass Short title: EHL for Pancreatic Ductal Stones Noor LH Bekkali 1, MD, PhD;
Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful Chronic Pancreatitis Using SpyGlass Short title: EHL for Pancreatic Ductal Stones Noor LH Bekkali 1, MD, PhD;
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Approach to the Biliary Stricture
 Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Biliary and Pancreatic Endoscopy Stones, Strictures, and IPMN
 WE MAKE LIVES BETTER UTHSC SAN ANTONIO Memorial Hermann Gastroentrology & Hepatology Symposium February 10, 2018 Biliary and Pancreatic Endoscopy Stones, Strictures, and IPMN Sandeep N. Patel, DO Director,
WE MAKE LIVES BETTER UTHSC SAN ANTONIO Memorial Hermann Gastroentrology & Hepatology Symposium February 10, 2018 Biliary and Pancreatic Endoscopy Stones, Strictures, and IPMN Sandeep N. Patel, DO Director,
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
SpyGlass Direct Visualization System
 SpyGlass Direct Visualization System Final Results from Largest Prospective Investigation of Peroral Cholangioscopy Published in Gastrointestinal Endoscopy (GIE) October 2011 Lead Authors Yang K. Chen,
SpyGlass Direct Visualization System Final Results from Largest Prospective Investigation of Peroral Cholangioscopy Published in Gastrointestinal Endoscopy (GIE) October 2011 Lead Authors Yang K. Chen,
Evaluation and Management of Refractory Biliary Stricture. J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc.
 Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Diagnosis of tumor extension in biliary carcinoma has. Differential Diagnosis and Treatment of Biliary Strictures
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:S79 S83 Differential Diagnosis and Treatment of Biliary Strictures KAZUO INUI, JUNJI YOSHINO, and HIRONAO MIYOSHI Department of Internal Medicine, Second
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:S79 S83 Differential Diagnosis and Treatment of Biliary Strictures KAZUO INUI, JUNJI YOSHINO, and HIRONAO MIYOSHI Department of Internal Medicine, Second
6/17/2016. ERCP in June 26, Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates
 ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
Ken Ito, Yoshinori Igarashi, Naoki Okano, Takahiko Mimura, Yui Kishimoto, Seiichi Hara, and Kensuke Takuma
 Hindawi Publishing Corporation BioMed Research International Volume 2014, Article ID 732781, 8 pages http://dx.doi.org/10.1155/2014/732781 Clinical Study Efficacy of Combined Endoscopic Lithotomy and Extracorporeal
Hindawi Publishing Corporation BioMed Research International Volume 2014, Article ID 732781, 8 pages http://dx.doi.org/10.1155/2014/732781 Clinical Study Efficacy of Combined Endoscopic Lithotomy and Extracorporeal
Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico
 Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques Associate Professor
Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques Associate Professor
E ndoscopic retrograde cholangiopancreatography (ERCP)
") 240 BILIARY DISEASE Endoscopic transpapillary biopsies and intraductal ultrasonography in the diagnostics of bile duct strictures: a prospective study D Domagk, C Poremba, K-H Dietl, N Senninger, A Heinecke,
240 BILIARY DISEASE Endoscopic transpapillary biopsies and intraductal ultrasonography in the diagnostics of bile duct strictures: a prospective study D Domagk, C Poremba, K-H Dietl, N Senninger, A Heinecke,
Direct peroral cholangioscopy using an ultrathin endoscope: Making technique easier
 1130-0108/2014/106/1/30-36 Revista Española de Enfermedades Digestivas Copyright 2014 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 106, N.º 1, pp. 30-36, 2014 ORIGINAL PAPERS Direct peroral cholangioscopy
1130-0108/2014/106/1/30-36 Revista Española de Enfermedades Digestivas Copyright 2014 Arán Ediciones, S. L. Rev Esp Enferm Dig (Madrid Vol. 106, N.º 1, pp. 30-36, 2014 ORIGINAL PAPERS Direct peroral cholangioscopy
Management of Indeterminate Biliary Strictures. Indeterminate Biliary Strictures
 Management of Indeterminate Biliary Strictures Professor of Medicine Director of Therapeutic Endoscopy Huntsman Cancer Center University of Utah School of Medicine Indeterminate Biliary Strictures Common
Management of Indeterminate Biliary Strictures Professor of Medicine Director of Therapeutic Endoscopy Huntsman Cancer Center University of Utah School of Medicine Indeterminate Biliary Strictures Common
Biliary Strictures: the Long and the Short of It. Willis Parsons, M.D. Medical Director of GI Lab Northwest Community Hospital Arlington Heights, IL
 Biliary Strictures: the Long and the Short of It Willis Parsons, M.D. Medical Director of GI Lab Northwest Community Hospital Arlington Heights, IL Consultant to Cook Medical Disclosure Objectives 1) Understand
Biliary Strictures: the Long and the Short of It Willis Parsons, M.D. Medical Director of GI Lab Northwest Community Hospital Arlington Heights, IL Consultant to Cook Medical Disclosure Objectives 1) Understand
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
MedSurg: Endoscopy Presentation for the Investment Community at DDW. Art Butcher Senior Vice President and President, Endoscopy
 MedSurg: Endoscopy Presentation for the Investment Community at DDW Art Butcher Senior Vice President and President, Endoscopy Safe Harbor for Forward-Looking Statements This presentation contains forward-looking
MedSurg: Endoscopy Presentation for the Investment Community at DDW Art Butcher Senior Vice President and President, Endoscopy Safe Harbor for Forward-Looking Statements This presentation contains forward-looking
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, by Am. Coll. of Gastroenterology ISSN /01/$20.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, 2001 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00 Published by Elsevier Science Inc. PII S0002-9270(01)02807-6 Can Endoscopic
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, 2001 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00 Published by Elsevier Science Inc. PII S0002-9270(01)02807-6 Can Endoscopic
Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary Mucinous Neoplasm
 Case Reports in Surgery Volume 2015, Article ID 816960, 4 pages http://dx.doi.org/10.1155/2015/816960 Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary
Case Reports in Surgery Volume 2015, Article ID 816960, 4 pages http://dx.doi.org/10.1155/2015/816960 Case Report Heterotopic Pancreas within the Proximal Hepatic Duct, Containing Intraductal Papillary
RX Biliary System. Start
 Start We re in! When you control the wire, efficiency comes along for the ride. The of Physician-Controlled Wireguided Cannulation Physician-controlled wireguided cannulation (WGC) facilitates deep biliary
Start We re in! When you control the wire, efficiency comes along for the ride. The of Physician-Controlled Wireguided Cannulation Physician-controlled wireguided cannulation (WGC) facilitates deep biliary
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
The Endoscopic Management of PSC
 The Endoscopic Management of PSC Raj J. Shah, M.D. Associate Professor of Medicine Director, Pancreaticobiliary Endoscopy Services University of Colorado at Denver and the Health Sciences Center Why did
The Endoscopic Management of PSC Raj J. Shah, M.D. Associate Professor of Medicine Director, Pancreaticobiliary Endoscopy Services University of Colorado at Denver and the Health Sciences Center Why did
Principles of ERCP: papilla cannulation, indications/contraindications and risks. Dr. med. Henrik Csaba Horváth PhD
 Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
CPT COD1NG UPDATES Gastroenterology CPT Advisors
 2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
EDUCATION PRACTICE. Biliary Stricture and Negative Cytology: What Next? AClinical Scenario. The Dilemma
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:739 743 EDUCATION PRACTICE Biliary Stricture and Negative Cytology: What Next? GREGORY A. COTÉ and STUART SHERMAN Division of Gastroenterology, Indiana University
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:739 743 EDUCATION PRACTICE Biliary Stricture and Negative Cytology: What Next? GREGORY A. COTÉ and STUART SHERMAN Division of Gastroenterology, Indiana University
Research Article The Utility of Repeat Endoscopic Ultrasound-Guided Fine Needle Aspiration for Suspected Pancreatic Cancer
 Gastroenterology Research and Practice Volume 2010, Article ID 268290, 4 pages doi:10.1155/2010/268290 Research Article The Utility of Repeat Endoscopic Ultrasound-Guided Fine Needle Aspiration for Suspected
Gastroenterology Research and Practice Volume 2010, Article ID 268290, 4 pages doi:10.1155/2010/268290 Research Article The Utility of Repeat Endoscopic Ultrasound-Guided Fine Needle Aspiration for Suspected
Intraductal biliopancreatic imaging: European Society of Gastrointestinal Endoscopy (ESGE) technology review
 technology review") Review 739 Intraductal biliopancreatic imaging: European Society of Gastrointestinal Endoscopy (ESGE) technology review Authors Andrea Tringali 1, Arnaud Lemmers 2, Volker Meves 3, Grischa Terheggen 4,
Review 739 Intraductal biliopancreatic imaging: European Society of Gastrointestinal Endoscopy (ESGE) technology review Authors Andrea Tringali 1, Arnaud Lemmers 2, Volker Meves 3, Grischa Terheggen 4,
Endoscopic Retrograde Cholangiopancreatography (ERCP)
") Endoscopic Retrograde Cholangiopancreatography (ERCP) Medical Imaging and Treatment of the Bile and Pancreatic Ducts CIE-02718 Understanding ERCP Brochure Update_F.indd 1 7/11/18 9:51 A Minimally Invasive
Endoscopic Retrograde Cholangiopancreatography (ERCP) Medical Imaging and Treatment of the Bile and Pancreatic Ducts CIE-02718 Understanding ERCP Brochure Update_F.indd 1 7/11/18 9:51 A Minimally Invasive
Crohn s disease is a heterogeneous inflammatory disorder
 ORIGINAL ARTICLE Application of the Montreal classification for Crohn s disease to a single clinician database of 1015 patients Hugh J Freeman MD HJ Freeman. Application of the Montreal classification
ORIGINAL ARTICLE Application of the Montreal classification for Crohn s disease to a single clinician database of 1015 patients Hugh J Freeman MD HJ Freeman. Application of the Montreal classification
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Index. Springer Nature Singapore Pte Ltd K.-H. Lai et al. (eds.), Biliopancreatic Endoscopy,
, Biliopancreatic Endoscopy,") A Acute cholangitis biliary endoprosthesis, 70 intraductal ultrasonography, 243 Acute cholecystitis, 33, 143, 226 Acute intracystic hemorrhage, EUS-FNA, 241 Acute pancreatitis EUS-FNA, 240 intraductal
A Acute cholangitis biliary endoprosthesis, 70 intraductal ultrasonography, 243 Acute cholecystitis, 33, 143, 226 Acute intracystic hemorrhage, EUS-FNA, 241 Acute pancreatitis EUS-FNA, 240 intraductal
ACUTE CHOLANGITIS AS a result of an occluded
 Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Introduction ORIGINAL RESEARCH
 Cancer Medicine ORIGINAL RESEARCH Open Access Diagnostic approach using ERCP- guided transpapillary forceps biopsy or EUS- guided fine- needle aspiration biopsy according to the nature of stricture segment
Cancer Medicine ORIGINAL RESEARCH Open Access Diagnostic approach using ERCP- guided transpapillary forceps biopsy or EUS- guided fine- needle aspiration biopsy according to the nature of stricture segment
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic Stents
 Gastroenterology Research and Practice Volume 2015, Article ID 365457, 6 pages http://dx.doi.org/10.1155/2015/365457 Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic
Gastroenterology Research and Practice Volume 2015, Article ID 365457, 6 pages http://dx.doi.org/10.1155/2015/365457 Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic
Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating Symptoms Suggestive of Common Bile Duct Stones
 Gastroenterology Research and Practice Volume 2016, Article ID 6957235, 5 pages http://dx.doi.org/10.1155/2016/6957235 Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating
Gastroenterology Research and Practice Volume 2016, Article ID 6957235, 5 pages http://dx.doi.org/10.1155/2016/6957235 Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating
Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria
 ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-6 Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria Ankit Chhoda
ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-6 Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria Ankit Chhoda
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Pulmonary. Pulmonary Endoscopy. Alair Bronchial Thermoplasty System. Transbronchial Aspiration Needles. Cytology Brushes.
 Pulmonary Endoscopy Alair Bronchial Thermoplasty System Alair Bronchial Thermoplasty System... 79 Airway Stents Dynamic (Y) Stent... 79 Polyflex Self-Expanding Silicone Airway Stent... 82 Ultraflex Partially
Pulmonary Endoscopy Alair Bronchial Thermoplasty System Alair Bronchial Thermoplasty System... 79 Airway Stents Dynamic (Y) Stent... 79 Polyflex Self-Expanding Silicone Airway Stent... 82 Ultraflex Partially
High-frequency miniprobe endoscopic ultrasonography for evaluation of indeterminate esophageal strictures
 ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-5 High-frequency miniprobe endoscopic ultrasonography for evaluation of indeterminate esophageal strictures Surinder Singh Rana a, Ravi Sharma a,
ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-5 High-frequency miniprobe endoscopic ultrasonography for evaluation of indeterminate esophageal strictures Surinder Singh Rana a, Ravi Sharma a,
The authors have declared no conflicts of interest.
 Diagnostic Accuracy of Magnetic Resonance Cholangiopancreatography Versus Endoscopic Retrograde Cholangiopancreatography Findings in the Postorthotopic Liver Transplant Population Authors: *Ashok Shiani,
Diagnostic Accuracy of Magnetic Resonance Cholangiopancreatography Versus Endoscopic Retrograde Cholangiopancreatography Findings in the Postorthotopic Liver Transplant Population Authors: *Ashok Shiani,
Endoscopic treatment of primary sclerosing cholangitis: Is there something new?
 Endoscopic treatment of primary sclerosing cholangitis: Is there something new? Arnaud Lemmers, MD, PhD Gastroenterology Department, Erasme Hospital, ULB, Brussels BASL December 1st 2017 AGENDA Introduction
Endoscopic treatment of primary sclerosing cholangitis: Is there something new? Arnaud Lemmers, MD, PhD Gastroenterology Department, Erasme Hospital, ULB, Brussels BASL December 1st 2017 AGENDA Introduction
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction
 A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
Journal of Interventional Gastroenterology A Combination of Snare Polypectomy and APC Therapy for Prolapsing Common Bile Duct Adenoma
 Journal of Interventional Gastroenterology A Combination of Snare Polypectomy and APC Therapy for Prolapsing Common Bile Duct Adenoma --Manuscript Draft-- Manuscript Number: Full Title: Article Type: Section/Category:
Journal of Interventional Gastroenterology A Combination of Snare Polypectomy and APC Therapy for Prolapsing Common Bile Duct Adenoma --Manuscript Draft-- Manuscript Number: Full Title: Article Type: Section/Category:
Agreement between endoscopic ultrasound-guided fine-needle aspiration and endobiliary brush cytology in suspected pancreaticobiliary malignancies
 Agreement between endoscopic ultrasound-guided fine-needle aspiration and endobiliary brush cytology in suspected pancreaticobiliary malignancies Authors Matthew J. Sullivan 1, Hope Kincaid 2, Shashin
Agreement between endoscopic ultrasound-guided fine-needle aspiration and endobiliary brush cytology in suspected pancreaticobiliary malignancies Authors Matthew J. Sullivan 1, Hope Kincaid 2, Shashin
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Diagnosis and Management of Primary Sclerosing Cholangitis:
 Diagnosis and Management of Primary Sclerosing Cholangitis: The Role of the Endoscopist Adam Slivka MD-PhD Associate Chief of the Division Gastroenterology Hepatology and Nutrition University of Pittsburgh
Diagnosis and Management of Primary Sclerosing Cholangitis: The Role of the Endoscopist Adam Slivka MD-PhD Associate Chief of the Division Gastroenterology Hepatology and Nutrition University of Pittsburgh
SURGERY? COMMON BILE DUCT STONES ERCP OR. Room 759. Maryland
 HPB INTERNATIONAL 277 alter the natural history of the disease, and delay or prevent the development or cirrhosis. Data from our unit as well as others suggests that to be the case. The current series,
HPB INTERNATIONAL 277 alter the natural history of the disease, and delay or prevent the development or cirrhosis. Data from our unit as well as others suggests that to be the case. The current series,
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine
 Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Approach hto Indeterminate Biliary Strictures
 Approach hto Indeterminate t Biliary Strictures Andrew Y. Wang, MD, FACG, FASGE Associate Professor of Medicine Co-Medical Director of Endoscopy Director of Pancreatico-Biliary Services Division of Gastroenterology
Approach hto Indeterminate t Biliary Strictures Andrew Y. Wang, MD, FACG, FASGE Associate Professor of Medicine Co-Medical Director of Endoscopy Director of Pancreatico-Biliary Services Division of Gastroenterology
Primary Sclerosing Cholangitis diagnosis, surveillance, and management.
 HKASLD 27 th Annual Scientific Meeting 2014 Primary Sclerosing Cholangitis diagnosis, surveillance, and management. Dr George Webster University College London and Royal Free Hospitals London UK george.webster@uclh.nhs.uk
HKASLD 27 th Annual Scientific Meeting 2014 Primary Sclerosing Cholangitis diagnosis, surveillance, and management. Dr George Webster University College London and Royal Free Hospitals London UK george.webster@uclh.nhs.uk
Title: Fasciola hepatica in the common bile duct: spyglass visualization and endoscopic extraction
 Title: Fasciola hepatica in the common bile duct: spyglass visualization and endoscopic extraction Authors: Edson Guzmán Calderón, Augusto Vera Calderón, Ramiro Díaz Ríos, Ronald Arcana López, Edgar Alva
Title: Fasciola hepatica in the common bile duct: spyglass visualization and endoscopic extraction Authors: Edson Guzmán Calderón, Augusto Vera Calderón, Ramiro Díaz Ríos, Ronald Arcana López, Edgar Alva
Jennifer Hsieh 1, Amar Thosani 1, Matthew Grunwald 2, Satish Nagula 1, Juan Carlos Bucobo 1, Jonathan M. Buscaglia 1. Introduction
 How We Do It Serial insertion of bilateral uncovered metal stents for malignant hilar obstruction using an 8 Fr biliary system: a case series of 17 consecutive patients Jennifer Hsieh 1, Amar Thosani 1,
How We Do It Serial insertion of bilateral uncovered metal stents for malignant hilar obstruction using an 8 Fr biliary system: a case series of 17 consecutive patients Jennifer Hsieh 1, Amar Thosani 1,
Is There a Role for Cholangioscopy in Patients with Primary Sclerosing Cholangitis?
 American Journal of Gastroenterology ISSN 0002-9270 C 2006 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2006.00383.x Published by Blackwell Publishing Is There a Role for Cholangioscopy in
American Journal of Gastroenterology ISSN 0002-9270 C 2006 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2006.00383.x Published by Blackwell Publishing Is There a Role for Cholangioscopy in
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience
 Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Advanced Cannulation Techniques
 Advanced Cannulation Techniques Priya A. Jamidar, M.D., FASGE Professor of Medicine, Director of Endoscopy Yale School Disclosures Consultant to Boston Scientific and Olympus America Cannulation at ERCP
Advanced Cannulation Techniques Priya A. Jamidar, M.D., FASGE Professor of Medicine, Director of Endoscopy Yale School Disclosures Consultant to Boston Scientific and Olympus America Cannulation at ERCP
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Expandable stents in digestive pathology present use in an emergency hospital
 ORIGINAL ARTICLES Article received on November30, 2015 and accepted for publishing on December15, 2015. Expandable stents in digestive pathology present use in an emergency hospital Mădălina Ilie 1, Vasile
ORIGINAL ARTICLES Article received on November30, 2015 and accepted for publishing on December15, 2015. Expandable stents in digestive pathology present use in an emergency hospital Mădălina Ilie 1, Vasile
Clinical study of the use of gastroscopy as oral choledochoscopy
 EXPERIMENTAL AND THERAPEUTIC MEDICINE 16: 1333-1337, 2018 Clinical study of the use of gastroscopy as oral choledochoscopy SHUNHUI HE 1, XUEHUA LIU 1, GUOPING DU 1, WENZHI CHEN 1 and WEIQING RUAN 2 1 Department
EXPERIMENTAL AND THERAPEUTIC MEDICINE 16: 1333-1337, 2018 Clinical study of the use of gastroscopy as oral choledochoscopy SHUNHUI HE 1, XUEHUA LIU 1, GUOPING DU 1, WENZHI CHEN 1 and WEIQING RUAN 2 1 Department
WallFlex Stents Technique Spotlights
 WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
WallFlex Stents Technique Spotlights OPEN TO THE POSSIBILITIES SEAN E. McGarr, do Kennebec Gastrointestinal Associates Maine General Medical Center, Augusta, ME 04330, United States Director of Gastrointestinal
Endoscopic Retrograde Cholangiopancreatography
 REVIEW Endoscopic Retrograde Cholangiopancreatography Sumit Singla, MD,* and Cyrus Piraka, MD Introduction Since its introduction in 1968, endoscopic retrograde cholangiopancreatography (ERCP) has revolutionized
REVIEW Endoscopic Retrograde Cholangiopancreatography Sumit Singla, MD,* and Cyrus Piraka, MD Introduction Since its introduction in 1968, endoscopic retrograde cholangiopancreatography (ERCP) has revolutionized
Bilirubin levels predict malignancy in patients with obstructive jaundice
 DOI:1.1111/j.1477-2574.211.312.x HPB ORIGINAL ARTICLE Bilirubin levels predict malignancy in patients with obstructive jaundice Giuseppe Garcea, Wee Ngu, Christopher P. Neal, Ashley R. Dennison & David
DOI:1.1111/j.1477-2574.211.312.x HPB ORIGINAL ARTICLE Bilirubin levels predict malignancy in patients with obstructive jaundice Giuseppe Garcea, Wee Ngu, Christopher P. Neal, Ashley R. Dennison & David
Research Article Endoscopic Closure for EUS and ERCP Related Duodenal Perforation by Endoclips
 Gastroenterology Research and Practice Volume 2016, Article ID 1051597, 5 pages http://dx.doi.org/10.1155/2016/1051597 Research Article Endoscopic Closure for EUS and ERCP Related Duodenal Perforation
Gastroenterology Research and Practice Volume 2016, Article ID 1051597, 5 pages http://dx.doi.org/10.1155/2016/1051597 Research Article Endoscopic Closure for EUS and ERCP Related Duodenal Perforation
Endoscopic Management of the Iatrogenic CBD Injury
 The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
Clinical Practice KPBA Guideline for Common Bile Duct Stones: The Endoscopic Management of Difficult and Recurrent Common Bile Duct Stones
 PBS-I Pancreatobiliary Endoscopist's Rule of Thumb Clinical Practice KPBA Guideline for Common Bile Duct Stones: The Endoscopic Management of Difficult and Recurrent Common Bile Duct Stones Byung Moo Yoo,
PBS-I Pancreatobiliary Endoscopist's Rule of Thumb Clinical Practice KPBA Guideline for Common Bile Duct Stones: The Endoscopic Management of Difficult and Recurrent Common Bile Duct Stones Byung Moo Yoo,
Endoscopic extraction of large common bile duct stones: A review article
 Online Submissions: http://www.wjgnet.com/1948-5190office wjge@wjgnet.com doi:10.4253/wjge.v4.i5.167 World J Gastrointest Endosc 2012 May 16; 4(5): 167-179 ISSN 1948-5190 (online) 2012 Baishideng. All
Online Submissions: http://www.wjgnet.com/1948-5190office wjge@wjgnet.com doi:10.4253/wjge.v4.i5.167 World J Gastrointest Endosc 2012 May 16; 4(5): 167-179 ISSN 1948-5190 (online) 2012 Baishideng. All
ACG Clinical Guideline: Primary Sclerosing Cholangitis
 ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
ACG Clinical Guideline: Primary Sclerosing Cholangitis Keith D. Lindor, MD, FACG 1, Kris V. Kowdley, MD, FACG 2, and M. Edwyn Harrison, MD 3 1 College of Health Solutions, Arizona State University, Phoenix,
Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic Duct Obstruction: Is Endoscopic Sphincterotomy Needed?
 Gastroenterology Research and Practice Volume 2013, Article ID 375613, 6 pages http://dx.doi.org/10.1155/2013/375613 Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic
Gastroenterology Research and Practice Volume 2013, Article ID 375613, 6 pages http://dx.doi.org/10.1155/2013/375613 Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
The Usefulness of Percutaneous Transhepatic Cholangioscopy for Identifying Malignancies in Distal Commom Bile Duct Strictures
 J Korean Med Sci 2008; 23: 579-85 ISSN 1011-8934 DOI: 10.3346/jkms.2008.23.4.579 Copyright The Korean Academy of Medical Sciences The Usefulness of Percutaneous Transhepatic Cholangioscopy for Identifying
J Korean Med Sci 2008; 23: 579-85 ISSN 1011-8934 DOI: 10.3346/jkms.2008.23.4.579 Copyright The Korean Academy of Medical Sciences The Usefulness of Percutaneous Transhepatic Cholangioscopy for Identifying
Tratamiento endoscópico de la CEP. En quien como y cuando?
 Tratamiento endoscópico de la CEP. En quien como y cuando? Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques University of Barcelona
Tratamiento endoscópico de la CEP. En quien como y cuando? Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques University of Barcelona
Bile Ducts Bile Duct Brushing
 Techniques for Cytologic Sampling of Pancreatic and Bile Duct Lesions William Brugge, M.D., 1 * John DeWitt, M.D., 2 Jason B. Klapman, M.D., 3 Raheela Ashfaq, M.D., 4 Vinod Shidham, M.D., 5 David Chhieng,
Techniques for Cytologic Sampling of Pancreatic and Bile Duct Lesions William Brugge, M.D., 1 * John DeWitt, M.D., 2 Jason B. Klapman, M.D., 3 Raheela Ashfaq, M.D., 4 Vinod Shidham, M.D., 5 David Chhieng,
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
Ontario Association of Gastroenterology
 FEE GUIDE Ontario Association of Gastroenterology OHIP Gastroenterology Fee Guide October 2003* *The fee guide is derived from the Ontario Schedule of Benefits for Physician Services (OHIP fee guide) which
FEE GUIDE Ontario Association of Gastroenterology OHIP Gastroenterology Fee Guide October 2003* *The fee guide is derived from the Ontario Schedule of Benefits for Physician Services (OHIP fee guide) which
CME Article Clinics in diagnostic imaging (115) Wai C T, Seto K Y, Sutedja D S
 Wai C T, Seto K Y, Sutedja D S") Medical Education Singapore Med.1 2007, 48 (4) : 361 CME Article Clinics in diagnostic imaging (115) Wai C T, Seto K Y, Sutedja D S fit. B CD - -0 o -5 r t -10 Fig. I US images of the upper right abdomen
Medical Education Singapore Med.1 2007, 48 (4) : 361 CME Article Clinics in diagnostic imaging (115) Wai C T, Seto K Y, Sutedja D S fit. B CD - -0 o -5 r t -10 Fig. I US images of the upper right abdomen
Gastric / EUS Metal Stents
 Gastric / EUS Metal Stents In a fast paced and maturing market, Diagmed Healthcare s Hanarostent has managed to continue to innovate and add unique and clinically superior features to its already premium
Gastric / EUS Metal Stents In a fast paced and maturing market, Diagmed Healthcare s Hanarostent has managed to continue to innovate and add unique and clinically superior features to its already premium
Tissue Acquisition. Introducing our large range of single use accessories for the collection of histology and cytology in the GI tract.
 Tissue Acquisition Introducing our large range of single use accessories for the collection of histology and cytology in the GI tract. MAKING A DIFFERENCE TO HEALTH Infinity ERCP Sampling Device STIFFER
Tissue Acquisition Introducing our large range of single use accessories for the collection of histology and cytology in the GI tract. MAKING A DIFFERENCE TO HEALTH Infinity ERCP Sampling Device STIFFER
STRICTURES OF THE BILE DUCTS Session No.: 5. Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy
 STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica
 Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica Authors: Sergio López-Durán, Celia Zaera, Juan Ángel
Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica Authors: Sergio López-Durán, Celia Zaera, Juan Ángel
Intraductal Ultrasonography for the Assessment of Preoperative Biliary and Pancreatic Strictures
 CLINICAL IMAGING Intraductal Ultrasonography for the Assessment of Preoperative Biliary and Pancreatic Strictures Marcel Tantau 1, Teodora Pop 1, Radu Badea 1, Zeno Spirchez 1, Ofelia Moşteanu 1, Alina
CLINICAL IMAGING Intraductal Ultrasonography for the Assessment of Preoperative Biliary and Pancreatic Strictures Marcel Tantau 1, Teodora Pop 1, Radu Badea 1, Zeno Spirchez 1, Ofelia Moşteanu 1, Alina
Advances in Hepato Biliary Pancreatic Endoscopy
 Advances in Hepato Biliary Pancreatic Endoscopy 24-26th February 2012, Hyderabad, India Organised by Asian Institute of Gastroenterology Hyderabad VENUE Hyderabad International Convention Centre (HICC)
Advances in Hepato Biliary Pancreatic Endoscopy 24-26th February 2012, Hyderabad, India Organised by Asian Institute of Gastroenterology Hyderabad VENUE Hyderabad International Convention Centre (HICC)
Biliary cancers: imaging diagnosis. Study of 30 cases
 Biliary cancers: imaging diagnosis. Study of 30 cases N Hammoune, S Semlali, M Eddarai, T. Amil, M Zentar, S. El Kandri,, M Benameur,, S Chaouir. Radiology Department. Mohamed V Military Hospital. Rabat-
Biliary cancers: imaging diagnosis. Study of 30 cases N Hammoune, S Semlali, M Eddarai, T. Amil, M Zentar, S. El Kandri,, M Benameur,, S Chaouir. Radiology Department. Mohamed V Military Hospital. Rabat-
SpyGlass DS-guided lithotripsy for pancreatic duct stones in symptomatic treatment-refractory chronic calcifying pancreatitis
 SpyGlass DS-guided lithotripsy for pancreatic duct stones in symptomatic treatment-refractory chronic calcifying pancreatitis Authors Christian Gerges *, 1, David Pullmann *, 1,FarzanBahin 1,MarkusSchneider
SpyGlass DS-guided lithotripsy for pancreatic duct stones in symptomatic treatment-refractory chronic calcifying pancreatitis Authors Christian Gerges *, 1, David Pullmann *, 1,FarzanBahin 1,MarkusSchneider
Endoscopic pancreatic necrosectomy in 2017
 Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
ENDOSCOPY IN COMPETITION DIAGNOSTICS. Dr. med. Dirk Hartmann Klinikum Ludwigshafen
 Falk Symposium 166 GI Endoscopy Standards and Innovations Mainz, 18. 19. September 2008 ENDOSCOPY IN COMPETITION DIAGNOSTICS Dr. med. Dirk Hartmann Klinikum Ludwigshafen ENDOSCOPY IN COMPETITION Competing
Falk Symposium 166 GI Endoscopy Standards and Innovations Mainz, 18. 19. September 2008 ENDOSCOPY IN COMPETITION DIAGNOSTICS Dr. med. Dirk Hartmann Klinikum Ludwigshafen ENDOSCOPY IN COMPETITION Competing
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Maximize Control. Minimize Migration.
 Maximize Control. Minimize Migration. New SHORT WIRE Delivery System SHORT W IRE BILIARY ENDOPROSTHESIS Improved treatment of biliary strictures The self-expanding, fully covered metal stent is intended
Maximize Control. Minimize Migration. New SHORT WIRE Delivery System SHORT W IRE BILIARY ENDOPROSTHESIS Improved treatment of biliary strictures The self-expanding, fully covered metal stent is intended
original article Improving access to care by allowing self-referral to a hepatitis C clinic
 original article Improving access to care by allowing self-referral to a hepatitis C clinic Karen Doucette MD MSc FRCPC 1, Vicki Robson RN 2, Stephen Shafran MD 1, Dennis Kunimoto MD 1 K Doucette, V Robson,
original article Improving access to care by allowing self-referral to a hepatitis C clinic Karen Doucette MD MSc FRCPC 1, Vicki Robson RN 2, Stephen Shafran MD 1, Dennis Kunimoto MD 1 K Doucette, V Robson,
Chronic pancreatitis is a fibroinflammatory disease of the
 Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct