When is the best to treat? Dr Munglani and Dr Spencer Cambridge Medicolegal conference Peterhouse 2016
|
|
|
- Jody Paul
- 6 years ago
- Views:
Transcription
1 When is the best to treat? Dr Munglani and Dr Spencer Cambridge Medicolegal conference Peterhouse 2016

2 When to treat in Chronic Pain cases? The Psychiatrist's Perspective

3 Why does The Psychiatrist s Perspective matter in chronic pain?
4 the nature of pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage It is unquestionably a sensation in a part or parts of the body, but it is also always unpleasant and therefore also an emotional experience (International Association for the Study of Pain)
5 4-stage model of pain processing (Price and Wade) immediate appraisal sensory features of the pain immediate emotional response immediate implications: moment-tomoment suffering, annoyance and distress only limited cognitive processing longer-term reflective processes meanings and implications of pain suffering, frustration, anger, anxiety, depression overt behavioural expression of pain moaning; lying down during the day; declining to participate in daily responsibilities
6 4-stage model of pain processing (Price and Wade) immediate appraisal sensory features of the pain immediate emotional response immediate implications: moment-tomoment suffering, annoyance and distress only limited cognitive processing longer-term reflective processes meanings and implications of pain suffering, frustration, anger, anxiety, depression overt behavioural expression of pain moaning; lying down during the day; declining to participate in daily responsibilities successive stages more psychological all stages influenced by psychological factors
7 depression heightening pain perception experimentally induced depressed mood enhances pain perception clinically depressed subjects show increased pain processing, both in anticipation of and during, pain stimulation
8 PTSD symptoms maintaining pain PTSD symptoms (particularly hyperarousal symptoms) predict the persistence and severity of pain and disability [eg. following whiplash injuries from RTAs; Buitenhuiset al, 2006] Treatment of PTSD in chronic pain patients (following RTA) symptoms gave rise to a reduction in pain-related disability [eg. Shipherd et al, 2003] The anxiety features and hypervigilance in PTSD may alter the perception and experience of physical complaints PTSD symptoms may fuel a catastrophic interpretation of the pain, inflating pain intensity, disability and psychological distress Development of mutually-maintaining interactions between PTSD symptoms and pain-related disability
9 Chronic pain as a persistent reminder of the traumatic event triggering PTSD symptoms and accompanying distressing emotions in turn triggering avoidance of the cause of the pain sensations and the associated memories of the trauma setting up a pattern of mutual maintenance where avoidance of sensations associated with the trauma leads to escalating levels of disability and distress and the distress further fuels the avoidance and enhanced pain perception


10 Chronic pain as a persistent reminder of the traumatic event triggering PTSD symptoms and accompanying distressing emotions in turn triggering avoidance of the cause of the pain sensations and the associated memories of the trauma setting up a pattern of mutual maintenance where avoidance of sensations associated with the trauma leads to escalating levels of disability and distress and the distress further fuels the avoidance and enhanced pain perception
.")

11 impact of blame / perceived injustice High levels of perceived injustice predicted the persistence of post-traumatic stress symptoms (in RTA whiplash patients). (Sullivan et al, 2009) Perceived injustice: encompasses elements of blame and the sense of a loss that is severe, irreparable and unfair. Patients seeking treatment for chronic pain who felt that their pain was someone else's fault, relative to those not identifying a fault source, reported significantly more concurrent distress and significantly less expected benefit from treatment


12 psychological factors contributing to chronification / transfer from acute to chronic pain and disability Chronification Psychological factors include: anxiety, depression, fear-avoidance and catastrophization in addition to important neuronal / biological factors incl. central sensitization and wind-up
13 Timing of Pain treatment in relation to addressing untreated psychological problems Depression? PTSD symptoms? Anxiety?

14 Timing of Pain treatment in relation to levels of insight & acceptance Readiness to change; Readiness to accept and adopt a self-management approach to managing pain and associated problems; The conscious embrace of psychological experiences, when to otherwise attempt to avoid them negatively impacts on overall functioning; Insight into and acceptance of the interactions between psychological factors and the pain Acceptance = the most important predictor of treatment outcome on a multidisciplinary pain treatment programme pain-related life interference, including interference with: family and marital functioning; work and work-related activities; and social-recreational activities (n=409; Akerblom et al, 2015)




15 CHRONIC PAIN ACCEPTANCE QUESTIONNAIRE



16 Our culture does not prepare patients to learn to live with pain They learn that the presence of a symptom indicates the need to consult a physician; They maintain their attempts to avoid pain; However, this simply serves to move the person increasingly away from the things that are important to them
17 The Pain Medicine perspective...
18 The (?inhibitory) role of the medicolegal process on recovery. There is a widespread belief that the very process of going through the medicolegal process inhibits outcome.
19
20 Pre-biopsychosocial model of pain: no effect of compensation


21 Post 1985 the biopsychosocial model of pain
22 Financial and emotional factors

23 Rohling et al conclusion re: CLBP and compensation

24 Does compensation effect outcome in relation to the magnitude of injury
25 What does claiming compensation do to outcome? The NDI scores of both the mild and moderate trajectories increased by 8 10%. In practical terms, claim submission within 12 months will be associated with an increase in symptoms of those who would have recovered such that they will be estimated to report ongoing mild pain/disability. of those left with residual mild pain and disability will now be estimated to be moderate. This change did not extend to the chronic severe patients where there was no significant association with claim lodgement.
26 What about reverse causality? Rather than the perceived route that compensation claims leads to reduction in function Alternatively those who have been badly effected by an injury are more likely to claim Fortunately, it is possible to adjust for the effects of joint causal pathways by using statistical techniques that are commonly applied in the social sciences to address this problem This study uses the relationship between claiming for injury compensation and recovery from whiplash neck pain as an example,
27 You can not differentiate between the presence of high pain scores and the decision to litigate

28 Does the medicolegal process lead to poorer care post accident?
29 What did they find? These examined the effect of lawyer involvement, litigation, claim submission, or previous claims on pain and other health outcomes. Among the 16 results reported were 9 statistically significant negative associations between compensation-related factors and health outcomes. Three studies acknowledged the possibility that negative associations between compensation related factors and health might reflect worse health among claimants (reverse causality).

30 Is the best therapy the ending of the medicolegal process?
31 Among the three reviews of prognostic factors in whiplash, two reviews concluding that compensation is a mediating factor in whiplash recovery both accepted claim duration as a proxy for recovery. So limit the clam duration (BC scenario no whiplash can exist after 24 months ) Conversely, the review by Scholten-Peeters specifically limited their focus to measures of symptoms and disability (i.e., health outcomes) and found strong evidence of no association between the legal process of litigation and recovery from whiplash.

32 Expectation of outcome (and the desire to litigate)
33
34 So we rush in and treat early
35
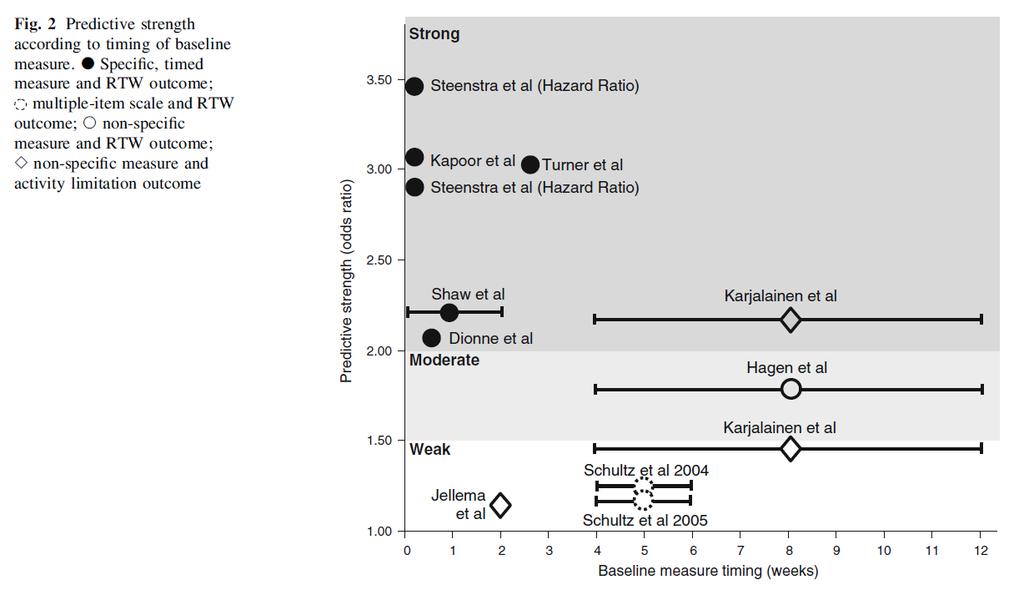
36 What patient factors should you consider when considering therapy?
37
38
39 Minimally invasive treatment for CLBP leads to significant pain reduction, including potential placebo effects. However, psychologically vulnerable patients, characterized by, reduced life control, disturbed mood, negative self-efficacy, catastrophizing, high anxiety levels, inadequacy, and poor mental health, tend not to respond to this treatment. Patients charac-terized by a.o. reduced pain and interference levels, positive expectations, and reasonable physical and social functioning, react more favorably. From both a clinical and a financial perspective, psychosocial evaluation and selection of patients seems appropriate, before applying minimally invasive procedures for CLBP.
40 Minimally invasive treatment for CLBP leads to significant pain reduction, including potential placebo effects. However, psychologically vulnerable patients, characterized by, reduced life control, disturbed mood, negative self-efficacy, catastrophizing, high anxiety levels, inadequacy, and poor mental health, tend not to respond to this treatment. Patients characterized by a.o. reduced pain and interference levels, positive expectations, and reasonable physical and social functioning, react more favorably. From both a clinical and a financial perspective, psychosocial evaluation and selection of patients seems appropriate, before applying minimally invasive procedures for CLBP.

41 Conclusion The most helpful components for predicting persistent disabling low back pain were maladaptive pain coping behaviours, nonorganic signs, functional impair-ment, general health status, and presence of psychiatric comorbidities.
42 According to their litigation and employment status these patients were divided into four groups, a non-litigating non-working group, a non-litigating working group, a litigating non-working group and a litigating working group. three questionnaires, one at intake, one at a minimum of 2 years later with the final questionnaire completed at a minimum of 15 months thereafter (for litigants after they had settled their claim).

43 The litigation effect
44 The working effect the non-working group had experienced more severe injuries than the working group; working generates a feeling of satisfaction that alleviates the perception of pain and disability; working facilitates recovery from injury.
45 Summary of paper Pain management efforts should thus be directed towards minimising nomogenic factors while maximising the chances of returning injured workers with back pain to their workplace, even if this is in an alternative, reduced capacity. If inclusion in a return to work program is not viable due to the severity of injury, vocational rehabilitation efforts should be redirected towards avocational activities integrating the perceived benefits of working (namely inclusion in a social support system, provision of financial certainty, and the obtaining of activity/work satisfaction) into the treatment/rehabilitation programs of those severely injured individuals with back pain unable to return to work.

46 Does all rehab work in this context?
47 Exclusions 3 treatments cf usual care. Fitness/gym program Out patient MDT program 2-4 hrs per day In patient MDT program C.f usual care
48 Intervention did not help

49 How do we define susceptibility and effect size of the vulnerability to be influenced by the context of litigation? ICD 9,10 but not DSM 4,5
50 Compensation neurosis The more modern definition of the condition is seen in the 1946 quote from Foster Kennedy that Compensation neurosis is a state of mind, born out of fear, kept alive by avarice, stimulated by lawyers, and cured by a verdict
51
52 What Is Compensation Neurosis? We propose that compensation neurosis is an exaggeration of symptoms that occur as a result of the unique stressor of seeking legally awarded compensation. It is brought about primarily by internal mo-tivators coupled with a lesser degree of anticipation of secondary gain. Financial reward can clearly be a component in the condition and may influence the course, but the overall constellation of symptoms is due to more than just the pursuit of money.
53 The place of compensation neurosis in predicting response to treatment in the context of litigation Who Contracts Compensation Neurosis? least likely to have the condition are generally young, wellmotivated, and better-educated, with clearly identifiable illnesses or deficits (e.g., amputees) and without the tendency to engage in prolonged self
54 Who is likely to be affected by compensation neurosis? Individuals who were believed to be prone to the condition often have diagnoses of more ambiguous and subjective symptombased injuries such as soft tissue in-jury (e.g., back strain or whiplash), pain syndromes (e.g., causalgia, fibromyalgia, reflex sympathetic dystrophy), primary psychiatric injuries (PTSD, depression, or anxiety). In addition, those with only pain symptoms also frequently have a comorbid psy-chiatric condition, with onset either before or after the injury, and frequently downplay or deny the ex-istence of the preexisting psychiatric condi-tion. People prone to the condition have characteristics of lower preinjury cognitive abilities, poor preinjury psychosocial functioning, low preexisting job satisfaction, hypochondriacal person-ality components, high suggestibility, tendency to assign blame for their difficulties to others, cluster B personality traits and defense mechanisms (e.g., en-titlement, hysteria, or narcissism), and cluster C per-sonality disorders (e.g., dependency).these characteristics at times are also found in pop-ulations of patients who malinger or have factitious disorder.
55

56 So do we wait to treat?
57 How about your perspective? open to the floor
Early Intervention and Psychological Injury
 Early Intervention and Psychological Injury SISA Conference 22 July 2008 Dr Peter Cotton FAPS Clinical & Organisational Psychologist Session Overview Key drivers of psychological injury The difference
Early Intervention and Psychological Injury SISA Conference 22 July 2008 Dr Peter Cotton FAPS Clinical & Organisational Psychologist Session Overview Key drivers of psychological injury The difference
Why study perceived injustice in individuals with disabilities?
 Perceptions of Injustice as a Risk Factor for Prolonged Work-Disability: Assessment and Intervention Why study perceived injustice in individuals with disabilities? If only he could see what he has done
Perceptions of Injustice as a Risk Factor for Prolonged Work-Disability: Assessment and Intervention Why study perceived injustice in individuals with disabilities? If only he could see what he has done
Perceptions of Injustice Predict Poor Recovery Following Debilitating Injury: Implications for Claim Management and Rehabilitation
 Perceptions of Injustice Predict Poor Recovery Following Debilitating Injury: Implications for Claim Management and Rehabilitation F Michael Sullivan, PhD Professor and Director of Recover Injury Research
Perceptions of Injustice Predict Poor Recovery Following Debilitating Injury: Implications for Claim Management and Rehabilitation F Michael Sullivan, PhD Professor and Director of Recover Injury Research
Individual Planning: A Treatment Plan Overview for Individuals with Somatization Disorder
 COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals with Somatization Disorder Individual Planning: A Treatment Plan Overview for Individuals with Somatization
COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals with Somatization Disorder Individual Planning: A Treatment Plan Overview for Individuals with Somatization
Annual Insurance Seminar. Tuesday 26 September 2017
 Annual Insurance Seminar Tuesday 26 September 2017 Dublin Dublin London London New New York York San San Franscisco Francisco Welcome Emer Gilvarry, Chairperson Dublin Dublin London London New New York
Annual Insurance Seminar Tuesday 26 September 2017 Dublin Dublin London London New New York York San San Franscisco Francisco Welcome Emer Gilvarry, Chairperson Dublin Dublin London London New New York
RE Options for reforming Green Slip Insurance in NSW: Motor Accidents Compulsory Third Party (CTP) scheme
 scheme") 28 April 2016 CTP Review State Insurance Regulatory Authority Level 25 580 George Street Sydney NSW 2000 Via email: CTP_Review@sira.nsw.gov.au To whom it may concern, RE Options for reforming Green Slip
28 April 2016 CTP Review State Insurance Regulatory Authority Level 25 580 George Street Sydney NSW 2000 Via email: CTP_Review@sira.nsw.gov.au To whom it may concern, RE Options for reforming Green Slip
BEHAVIORAL ASSESSMENT OF PAIN MEDICAL STABILITY QUICK SCREEN. Test Manual
 BEHAVIORAL ASSESSMENT OF PAIN MEDICAL STABILITY QUICK SCREEN Test Manual Michael J. Lewandowski, Ph.D. The Behavioral Assessment of Pain Medical Stability Quick Screen is intended for use by health care
BEHAVIORAL ASSESSMENT OF PAIN MEDICAL STABILITY QUICK SCREEN Test Manual Michael J. Lewandowski, Ph.D. The Behavioral Assessment of Pain Medical Stability Quick Screen is intended for use by health care
Behavioral Comorbidities in Chronic Pain. Christopher Sletten, Ph.D. Mayo Clinic Florida MFMER slide-1
 Behavioral Comorbidities in Chronic Pain Christopher Sletten, Ph.D. Mayo Clinic Florida 2015 MFMER slide-1 Chronic Pain 2015 MFMER slide-2 Chronic Pain Characteristics Enduring symptoms Elusive causes
Behavioral Comorbidities in Chronic Pain Christopher Sletten, Ph.D. Mayo Clinic Florida 2015 MFMER slide-1 Chronic Pain 2015 MFMER slide-2 Chronic Pain Characteristics Enduring symptoms Elusive causes
Are Somatisation Disorders any use to clinicians or patients? February 13th 2013 Charlotte Feinmann
 Are Somatisation Disorders any use to clinicians or patients? February 13th 2013 Charlotte Feinmann Outline Context and Definitions Changing Classification Changing Medical Attitudes Understanding Psychological
Are Somatisation Disorders any use to clinicians or patients? February 13th 2013 Charlotte Feinmann Outline Context and Definitions Changing Classification Changing Medical Attitudes Understanding Psychological
1/22/2015. Contemporary Psychiatric-Mental Health Nursing Third Edition. Theories: Dissociative Disorders. Theories: Dissociative Disorders (cont'd)
") Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 19 Dissociative, Somatoform, and Factitious Disorders Theories: Dissociative Disorders Biological factors Serotonin Limbic system Physical
Contemporary Psychiatric-Mental Health Nursing Third Edition CHAPTER 19 Dissociative, Somatoform, and Factitious Disorders Theories: Dissociative Disorders Biological factors Serotonin Limbic system Physical
Drug Overdoses A Public Health Problem. Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013. Objectives
 Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
THE PSYCHOLOGY OF CHRONIC PAIN
 THE PSYCHOLOGY OF CHRONIC PAIN Nomita Sonty, Ph.D, M.Phil Associate Professor of Medical Psychology @ CUMC Depts. of Anesthesiology &Psychiatry College of Physicians & Surgeons Columbia University New
THE PSYCHOLOGY OF CHRONIC PAIN Nomita Sonty, Ph.D, M.Phil Associate Professor of Medical Psychology @ CUMC Depts. of Anesthesiology &Psychiatry College of Physicians & Surgeons Columbia University New
A Family Affair: Effects of Brain Injury on Family Dynamics
 A Family Affair: Effects of Brain Injury on Family Dynamics Dr. Kyle Haggerty, PhD By: Kyle Haggerty Bancroft NeuroRehab TBI Stats The Centers for Disease Control and Prevention reported that in 2010 that
A Family Affair: Effects of Brain Injury on Family Dynamics Dr. Kyle Haggerty, PhD By: Kyle Haggerty Bancroft NeuroRehab TBI Stats The Centers for Disease Control and Prevention reported that in 2010 that
A TRIAD OF PERSPECTIVES ON PSYCHOLOGICAL INJURIES IN THE WORKPLACE THE PSYCHOLOGIST
 A TRIAD OF PERSPECTIVES ON PSYCHOLOGICAL INJURIES IN THE WORKPLACE THE PSYCHOLOGIST Presented by Dr. Beverley Kirk Centre For Emotional Intelligence www.centre4ei.com.au info@centre4ei.com.au ABSTRACT
A TRIAD OF PERSPECTIVES ON PSYCHOLOGICAL INJURIES IN THE WORKPLACE THE PSYCHOLOGIST Presented by Dr. Beverley Kirk Centre For Emotional Intelligence www.centre4ei.com.au info@centre4ei.com.au ABSTRACT
Balancing the Challenges of Mental Health Claims in Insurance
 Balancing the Challenges of Mental Health Claims in Insurance Jane Dorter, Michael Dermody, and Joshua Martin. 2017 KPMG, an Australian partnership and a member firm of the KPMG network of independent
Balancing the Challenges of Mental Health Claims in Insurance Jane Dorter, Michael Dermody, and Joshua Martin. 2017 KPMG, an Australian partnership and a member firm of the KPMG network of independent
MODULE IX. The Emotional Impact of Disasters on Children and their Families
 MODULE IX The Emotional Impact of Disasters on Children and their Families Outline of presentation Psychological first aid in the aftermath of a disaster Common reactions to disaster Risk factors for difficulty
MODULE IX The Emotional Impact of Disasters on Children and their Families Outline of presentation Psychological first aid in the aftermath of a disaster Common reactions to disaster Risk factors for difficulty
PSYCHOSOCIAL EVALUATION AND TREATMENT IN CHRONIC RESPIRATORY DISEASES
 PSYCHOSOCIAL EVALUATION AND TREATMENT IN CHRONIC RESPIRATORY DISEASES Prof Behcet Coşar M.D. Gazi Uni. School of Med. Psychiatry Dep Consultation Liaison Psychiatry Unit HUMAN Bio Psycho Social 11/6/2009
PSYCHOSOCIAL EVALUATION AND TREATMENT IN CHRONIC RESPIRATORY DISEASES Prof Behcet Coşar M.D. Gazi Uni. School of Med. Psychiatry Dep Consultation Liaison Psychiatry Unit HUMAN Bio Psycho Social 11/6/2009
Treating Children and Adolescents with PTSD. William Yule Prague March 2014
 Treating Children and Adolescents with PTSD William Yule Prague March 2014 In the beginning. When DSM III first identified PTSD, it was thought that children would rarely show it Why did professionals
Treating Children and Adolescents with PTSD William Yule Prague March 2014 In the beginning. When DSM III first identified PTSD, it was thought that children would rarely show it Why did professionals
Biopsychosocial Characteristics of Somatoform Disorders
 Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Noteworthy Decision Summary. Decision: WCAT Panel: Susan Marten Decision Date: September 8, 2004
 Decision Number: -2004-04737 Noteworthy Decision Summary Decision: -2004-04737 Panel: Susan Marten Decision Date: September 8, 2004 Adjustment Disorder Mental Stress Distinction between Compensation for
Decision Number: -2004-04737 Noteworthy Decision Summary Decision: -2004-04737 Panel: Susan Marten Decision Date: September 8, 2004 Adjustment Disorder Mental Stress Distinction between Compensation for
Pain-related Distress: Recognition and Appropriate Interventions. Tamar Pincus Professor in psychology Royal Holloway University of London
 Pain-related Distress: Recognition and Appropriate Interventions Tamar Pincus Professor in psychology Royal Holloway University of London Remit (and limitations) of presentation Mostly, research in low
Pain-related Distress: Recognition and Appropriate Interventions Tamar Pincus Professor in psychology Royal Holloway University of London Remit (and limitations) of presentation Mostly, research in low
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1421/15
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1421/15 BEFORE: B. Kalvin : Vice-Chair A.D.G. Purdy : Member Representative of Employers J. A. Crocker : Member Representative of Workers HEARING:
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1421/15 BEFORE: B. Kalvin : Vice-Chair A.D.G. Purdy : Member Representative of Employers J. A. Crocker : Member Representative of Workers HEARING:
Mental Health and Stress
 Mental Health and Stress Learning Objectives Ø Define mental health and discuss the characteristics of mentally healthy and selfactualized people Ø Describe the various mental disorders and appropriate
Mental Health and Stress Learning Objectives Ø Define mental health and discuss the characteristics of mentally healthy and selfactualized people Ø Describe the various mental disorders and appropriate
Stress Disorders. Stress and coping. Stress and coping. Stress and coping. Parachute for sale: Only used once, never opened.
 Stress Disorders Parachute for sale: Only used once, never opened. Stress and coping The state of stress has two components: Stressor: event creating demands Stress response: reactions to the demands Stress
Stress Disorders Parachute for sale: Only used once, never opened. Stress and coping The state of stress has two components: Stressor: event creating demands Stress response: reactions to the demands Stress
Aetiology of medically unexplained neurological symptoms
 Aetiology of medically unexplained neurological symptoms Richard J. Brown PhD, ClinPsyD University of Manchester, UK Manchester Mental Health and Social Care NHS Trust Overview 1. Are symptoms simply made
Aetiology of medically unexplained neurological symptoms Richard J. Brown PhD, ClinPsyD University of Manchester, UK Manchester Mental Health and Social Care NHS Trust Overview 1. Are symptoms simply made
Pain Psychology: Disclosure Slide. Learning Objectives. Bio-psychosocial Model 8/12/2014. What we won t cover (today) What influences chronic pain?
 What influences chronic pain?") Disclosure Slide Pain Psychology: No commercial interests to disclose Screening for distress and maladaptive attitudes and beliefs Paul Taenzer PhD, CPsych Learning Objectives At the end of the session,
Disclosure Slide Pain Psychology: No commercial interests to disclose Screening for distress and maladaptive attitudes and beliefs Paul Taenzer PhD, CPsych Learning Objectives At the end of the session,
Understanding Parkinson s for health and social care staff. The phases of Parkinson s
 Understanding for health and social care staff The phases of The phases of Diagnosis 11% 1.6 Post diagnosis before symptoms have become significant Maintenance 40.4% 5.9 Symptoms significant but largely
Understanding for health and social care staff The phases of The phases of Diagnosis 11% 1.6 Post diagnosis before symptoms have become significant Maintenance 40.4% 5.9 Symptoms significant but largely
The Psychology of Pain within the Biological Model. Michael Coupland, CPsych, CRC Integrated Medical Case Solutions (IMCS Group)
") The Psychology of Pain within the Biological Model Michael Coupland, CPsych, CRC Integrated Medical Case Solutions (IMCS Group) Integrated Medical Case Solutions National Panel of Psychologists Biopsychosocial
The Psychology of Pain within the Biological Model Michael Coupland, CPsych, CRC Integrated Medical Case Solutions (IMCS Group) Integrated Medical Case Solutions National Panel of Psychologists Biopsychosocial
Functional Tools Pain and Activity Questionnaire
 Job dissatisfaction (Bigos, Battie et al. 1991; Papageorgiou, Macfarlane et al. 1997; Thomas, Silman et al. 1999; Linton 2001), fear avoidance and pain catastrophizing (Ciccone and Just 2001; Fritz, George
Job dissatisfaction (Bigos, Battie et al. 1991; Papageorgiou, Macfarlane et al. 1997; Thomas, Silman et al. 1999; Linton 2001), fear avoidance and pain catastrophizing (Ciccone and Just 2001; Fritz, George
Concepts for Understanding Traumatic Stress Responses in Children and Families
 The 12 Core Concepts, developed by the NCTSN Core Curriculum Task Force during an expert consensus meeting in 2007, serve as the conceptual foundation of the Core Curriculum on Childhood Trauma and provide
The 12 Core Concepts, developed by the NCTSN Core Curriculum Task Force during an expert consensus meeting in 2007, serve as the conceptual foundation of the Core Curriculum on Childhood Trauma and provide
(Appendix 1) Hong Kong HIV Stigma Watch Brief Report. Basic Demographics
 Hong Kong HIV Stigma Watch Brief Report. Basic Demographics") (Appendix 1) Hong Kong HIV Stigma Watch Brief Report Basic Demographics 291 people living with HIV (PLHIV) were recruited in the study. 96% (n=277) of the participants were male and majority (95%, n=271)
(Appendix 1) Hong Kong HIV Stigma Watch Brief Report Basic Demographics 291 people living with HIV (PLHIV) were recruited in the study. 96% (n=277) of the participants were male and majority (95%, n=271)
Look to see if they can focus on compassionate attention, compassionate thinking and compassionate behaviour. This is how the person brings their
 Compassionate Letter Writing Therapist Notes The idea behind compassionate mind letter writing is to help people engage with their problems with a focus on understanding and warmth. We want to try to bring
Compassionate Letter Writing Therapist Notes The idea behind compassionate mind letter writing is to help people engage with their problems with a focus on understanding and warmth. We want to try to bring
It s Mental Health Week!
 It s Mental Health Week! This year, the Canadian Mental Health Association (CMHA) presents Mental Health Week from May 5 th to May 11 th. CMHA is launching a Be Mind Full initiative asking Canadians if
It s Mental Health Week! This year, the Canadian Mental Health Association (CMHA) presents Mental Health Week from May 5 th to May 11 th. CMHA is launching a Be Mind Full initiative asking Canadians if
SUMMARY. Chronic pain; Significant contribution (of compensable accident to development of condition).
.") SUMMARY DECISION NO. 2042/00 Chronic pain; Significant contribution (of compensable accident to development of condition). The worker suffered a low back strain in 1996. The worker appealed a decision
SUMMARY DECISION NO. 2042/00 Chronic pain; Significant contribution (of compensable accident to development of condition). The worker suffered a low back strain in 1996. The worker appealed a decision
Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME)
 / Myalgic Encephalomyelitis/Encephalopathy (ME)") Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME) This intervention (and hence this listing of competences) assumes that practitioners are familiar with, and able to deploy,
Chronic Fatigue Syndrome (CFS) / Myalgic Encephalomyelitis/Encephalopathy (ME) This intervention (and hence this listing of competences) assumes that practitioners are familiar with, and able to deploy,
Taking Control of Anger. About Anger
 Taking Control of Anger About Anger About the course This course is for anyone who is concerned about his or her anger. Throughout the course you can expect to learn: How to reduce the frequency and intensity
Taking Control of Anger About Anger About the course This course is for anyone who is concerned about his or her anger. Throughout the course you can expect to learn: How to reduce the frequency and intensity
Preventing delayed recovery by adopting a biopsychosocial approach
 Preventing delayed recovery by adopting a biopsychosocial approach IFDM 2018 October 15, 2018 Vancouver, BC Marcos Iglesias MD, MMM, FAAFP, FACOEM OBJECTIVES 01. Review the importance of addressing disability
Preventing delayed recovery by adopting a biopsychosocial approach IFDM 2018 October 15, 2018 Vancouver, BC Marcos Iglesias MD, MMM, FAAFP, FACOEM OBJECTIVES 01. Review the importance of addressing disability
Emotional Problems After Traumatic Brain Injury (TBI)
") Emotional Problems After Traumatic Brain Injury (TBI) A resource for individuals with TBI and their supporters This presentation is based on TBI Model Systems research and was developed with support from
Emotional Problems After Traumatic Brain Injury (TBI) A resource for individuals with TBI and their supporters This presentation is based on TBI Model Systems research and was developed with support from
ARCHIVE. Alberta WCB Policies & Information
 1. Under what circumstances is a psychiatric or psychological injury 2. How does WCB determine whether a psychiatric or psychological injury is WCB will consider a claim for psychiatric or psychological
1. Under what circumstances is a psychiatric or psychological injury 2. How does WCB determine whether a psychiatric or psychological injury is WCB will consider a claim for psychiatric or psychological
Stress & Health. } This section covers: The definition of stress Measuring stress
 Stress & Health } This section covers: The definition of stress Measuring stress Stress } Stress: any event or environmental stimulus (i.e., stressor) that we respond to because we perceive it as challenging
Stress & Health } This section covers: The definition of stress Measuring stress Stress } Stress: any event or environmental stimulus (i.e., stressor) that we respond to because we perceive it as challenging
4. A consensus definition of CFS/ME has been agreed by international experts for the purposes of research and includes the following:-
 DWP MEDICAL GUIDANCE VERSION 10 (May 2007) CHRONIC FATIGUE SYNDROME AND MYALGIC ENCEPHALOMYELITIS/ENCEPHALOPATHY What is it? (Definition) 1. The term chronic fatigue syndrome (CFS) is used to describe
DWP MEDICAL GUIDANCE VERSION 10 (May 2007) CHRONIC FATIGUE SYNDROME AND MYALGIC ENCEPHALOMYELITIS/ENCEPHALOPATHY What is it? (Definition) 1. The term chronic fatigue syndrome (CFS) is used to describe
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1820/13
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1820/13 BEFORE: J. P. Moore: Vice-Chair HEARING: September 18, 2013 at Kitchener Oral Post-hearing activity completed on March 20, 2014 DATE
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1820/13 BEFORE: J. P. Moore: Vice-Chair HEARING: September 18, 2013 at Kitchener Oral Post-hearing activity completed on March 20, 2014 DATE
Spinal Cord Injury Research. By the Department of Clinical Psychology, National Spinal Injuries Centre
 Stoke Mandeville Hospital Spinal Cord Injury Research By the Department of Clinical Psychology, National Spinal Injuries Centre 2008-2009 Department of Clinical Psychology, National Spinal Injuries Centre,
Stoke Mandeville Hospital Spinal Cord Injury Research By the Department of Clinical Psychology, National Spinal Injuries Centre 2008-2009 Department of Clinical Psychology, National Spinal Injuries Centre,
New Criteria for Posttraumatic Stress Disorder in DSM-5: Implications for Causality
 New Criteria for Posttraumatic Stress Disorder in DSM-5: Implications for Causality Paul A. Arbisi, Ph.D. ABAP, ABPP. Staff Psychologist Minneapolis VA Medical Center Professor Departments of Psychiatry
New Criteria for Posttraumatic Stress Disorder in DSM-5: Implications for Causality Paul A. Arbisi, Ph.D. ABAP, ABPP. Staff Psychologist Minneapolis VA Medical Center Professor Departments of Psychiatry
WHAT ARE PERSONALITY DISORDERS?
 CHAPTER 16 REVIEW WHAT ARE PERSONALITY DISORDERS? How is abnormal behaviour defined? Statistically infrequent Violates of social norms Personally distressful Disability or dysfunction Unexpected DSM-IV
CHAPTER 16 REVIEW WHAT ARE PERSONALITY DISORDERS? How is abnormal behaviour defined? Statistically infrequent Violates of social norms Personally distressful Disability or dysfunction Unexpected DSM-IV
Understanding Mental Health and Mental Illness. CUSW Health & Safety
 Understanding Mental Health and Mental Illness CUSW Health & Safety Outline Mental Health / Mental Illness Statistics Lifestyle Factors Stress Stigma Resources Burlington TS Health Services What does mental
Understanding Mental Health and Mental Illness CUSW Health & Safety Outline Mental Health / Mental Illness Statistics Lifestyle Factors Stress Stigma Resources Burlington TS Health Services What does mental
BUILDING A PTSD PREVENTION PLAN DR. ASH BENDER, MD, FRCPC KIM SLADE, DIRECTOR RESEARCH AND PRODUCT DEVELOPMENT PSHSA
 BUILDING A PTSD PREVENTION PLAN DR. ASH BENDER, MD, FRCPC KIM SLADE, DIRECTOR RESEARCH AND PRODUCT DEVELOPMENT PSHSA 1 THIS SESSION IS DESIGNED TO HELP YOU Understand what PTSD is and how it might present
BUILDING A PTSD PREVENTION PLAN DR. ASH BENDER, MD, FRCPC KIM SLADE, DIRECTOR RESEARCH AND PRODUCT DEVELOPMENT PSHSA 1 THIS SESSION IS DESIGNED TO HELP YOU Understand what PTSD is and how it might present
Your experiences. It s all in the brain? Deciphering Neurological Presentations a Perspective From Neuropsychiatry
 Your experiences Deciphering Neurological Presentations a Perspective From Neuropsychiatry Mike Dilley Maudsley Hospital michael.dilley@slam.nhs.uk Think about the last patient that your saw with a neurological
Your experiences Deciphering Neurological Presentations a Perspective From Neuropsychiatry Mike Dilley Maudsley Hospital michael.dilley@slam.nhs.uk Think about the last patient that your saw with a neurological
What s Trauma All About
 What s Trauma All About Because early abuse impacts on the developing brain of these infants, it has enduring effects. There is extensive evidence that trauma in early life impairs the development of the
What s Trauma All About Because early abuse impacts on the developing brain of these infants, it has enduring effects. There is extensive evidence that trauma in early life impairs the development of the
DECISION OF THE WORKERS COMPENSATION APPEAL TRIBUNAL
 Decision Number: A1701323 (January 5, 2018) DECISION OF THE WORKERS COMPENSATION APPEAL TRIBUNAL Decision Number: A1701323 Decision Date: January 5, 2018 Introduction [1] By letter dated September 26,
Decision Number: A1701323 (January 5, 2018) DECISION OF THE WORKERS COMPENSATION APPEAL TRIBUNAL Decision Number: A1701323 Decision Date: January 5, 2018 Introduction [1] By letter dated September 26,
Northwest Territories and Nunavut 03.09
 POLICY STATEMENT The Workers Safety and Compensation Commission (WSCC) may provide compensation benefits to workers who develop a psychiatric or psychological disability arising out of and during the course
POLICY STATEMENT The Workers Safety and Compensation Commission (WSCC) may provide compensation benefits to workers who develop a psychiatric or psychological disability arising out of and during the course
PTSD Ehlers and Clark model
 Problem-specific competences describe the knowledge and skills needed when applying CBT principles to specific conditions. They are not a stand-alone description of competences, and should be read as part
Problem-specific competences describe the knowledge and skills needed when applying CBT principles to specific conditions. They are not a stand-alone description of competences, and should be read as part
The Impact of Changes to the DSM and ICD Criteria for PTSD
 The Impact of Changes to the DSM and ICD Criteria for PTSD Jonathan I Bisson Institute of Psychological Medicine and Clinical Neursociences Cardiff University What is PTSD? Question Diagnosing PTSD DSM-IV
The Impact of Changes to the DSM and ICD Criteria for PTSD Jonathan I Bisson Institute of Psychological Medicine and Clinical Neursociences Cardiff University What is PTSD? Question Diagnosing PTSD DSM-IV
Post-Traumatic Stress Disorder
 Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
Post-Traumatic Stress Disorder Teena Jain 2017 Post-Traumatic Stress Disorder What is post-traumatic stress disorder, or PTSD? PTSD is a disorder that some people develop after experiencing a shocking,
What the heck is PTSD? And what do I do if I have it?
 What the heck is PTSD? And what do I do if I have it? Dr. Dion Goodland, Psychologist Goodland Psychology November 2015 Outline for today What is Posttraumatic Stress Disorder (PTSD)? How do I get it?
What the heck is PTSD? And what do I do if I have it? Dr. Dion Goodland, Psychologist Goodland Psychology November 2015 Outline for today What is Posttraumatic Stress Disorder (PTSD)? How do I get it?
Introduction into Psychiatric Disorders. Dr Jon Spear- Psychiatrist
 Introduction into Psychiatric Disorders Dr Jon Spear- Psychiatrist Content Stress Major depressive disorder Adjustment disorder Generalised anxiety disorder Post traumatic stress disorder Borderline personality
Introduction into Psychiatric Disorders Dr Jon Spear- Psychiatrist Content Stress Major depressive disorder Adjustment disorder Generalised anxiety disorder Post traumatic stress disorder Borderline personality
What are we talking about? Patients presenting with Physical symptoms No obvious organic cause In addition, identifiable Psychological } Emotional } F
 Medically Unexplained Symptoms - an approach to rehabilitation Prof Lynne Turner-Stokes Herbert Dunhill Chair of Rehabilitation King s College London Director, Regional Rehabilitation Unit Northwick Park
Medically Unexplained Symptoms - an approach to rehabilitation Prof Lynne Turner-Stokes Herbert Dunhill Chair of Rehabilitation King s College London Director, Regional Rehabilitation Unit Northwick Park
The Role of Psychology and Psychological Approaches in Pain Management
 The Role of Psychology and Psychological Approaches in Pain Management Jennifer L. Murphy, Ph.D. CBT for Chronic Pain Trainer, VA Central Office Clinical Director and Pain Section Supervisor James A. Haley
The Role of Psychology and Psychological Approaches in Pain Management Jennifer L. Murphy, Ph.D. CBT for Chronic Pain Trainer, VA Central Office Clinical Director and Pain Section Supervisor James A. Haley
Emotional Symptoms in Athletes With PCS. David Westerdahl, MD FAAFP Cleveland Clinic Florida 6/24/2012
 Emotional Symptoms in Athletes With PCS David Westerdahl, MD FAAFP Cleveland Clinic Florida 6/24/2012 Objectives Discuss Post-Concussion symptoms and functional problems Identify pre-injury factors that
Emotional Symptoms in Athletes With PCS David Westerdahl, MD FAAFP Cleveland Clinic Florida 6/24/2012 Objectives Discuss Post-Concussion symptoms and functional problems Identify pre-injury factors that
SOMEONE I CARE ABOUT IS NOT DEALING WITH HIS OCD: WHAT CAN I DO ABOUT IT?
 SOMEONE I CARE ABOUT IS NOT DEALING WITH HIS OCD: WHAT CAN I DO ABOUT IT? By Heidi J. Pollard, RN, MSN and C. Alec Pollard, Ph.D., Anxiety Disorders Center, Saint Louis Behavioral Medicine Institute and
SOMEONE I CARE ABOUT IS NOT DEALING WITH HIS OCD: WHAT CAN I DO ABOUT IT? By Heidi J. Pollard, RN, MSN and C. Alec Pollard, Ph.D., Anxiety Disorders Center, Saint Louis Behavioral Medicine Institute and
Defence mechanisms. Dr. Radwan Bani Mustafa MD
 Defence mechanisms Dr. Radwan Bani Mustafa MD Functions of Defense/Mental Mechanisms Facilitates the resolution of emotional conflict To provide relief from stress To cushion emotional pain To avoid or
Defence mechanisms Dr. Radwan Bani Mustafa MD Functions of Defense/Mental Mechanisms Facilitates the resolution of emotional conflict To provide relief from stress To cushion emotional pain To avoid or
ADHD Explanation 2: Oppositional defiant disorder and MERIM
 ADHD Explanation 2: Oppositional Oppositional defiant disorder (ODD) ODD is very frequently associated with ADHD. People with ODD typically overreact with anger in response to minor frustration. The lack
ADHD Explanation 2: Oppositional Oppositional defiant disorder (ODD) ODD is very frequently associated with ADHD. People with ODD typically overreact with anger in response to minor frustration. The lack
Chapter 5 - Somatic Symptom, Dissociative, and Factitious Disorders
 Chapter 5 - Somatic Symptom, Dissociative, and Factitious Disorders SOMATIC SYMPTOM AND RELATED DISORDERS -Physical symptoms (eg. pain) or concerns about an illness cannot be explained by a medical or
Chapter 5 - Somatic Symptom, Dissociative, and Factitious Disorders SOMATIC SYMPTOM AND RELATED DISORDERS -Physical symptoms (eg. pain) or concerns about an illness cannot be explained by a medical or
Overview of DSM Lecture DSM DSM. Multiaxial system. Multiaxial system. Axis I
 DSM Overview of DSM Lecture Brief history Brief overview How to use it Differentials & R/Os malingering, factitious dis, meds/medical, substance, organic Co-morbidity/dual-diagnosis Substance Use/Abuse
DSM Overview of DSM Lecture Brief history Brief overview How to use it Differentials & R/Os malingering, factitious dis, meds/medical, substance, organic Co-morbidity/dual-diagnosis Substance Use/Abuse
The ABC s of Trauma- Informed Care
 The ABC s of Trauma- Informed Care AGENDA What do we mean by trauma? How does trauma affect people? What can we learn from listening to the voices of people who have experienced trauma? Why is understanding
The ABC s of Trauma- Informed Care AGENDA What do we mean by trauma? How does trauma affect people? What can we learn from listening to the voices of people who have experienced trauma? Why is understanding
TRAUMA INFORMED CARE: THE IMPORTANCE OF THE WORKING ALLIANCE
 TRAUMA INFORMED CARE: THE IMPORTANCE OF THE WORKING ALLIANCE Justin Watts PhD. NCC, CRC Assistant Professor, Rehabilitation Health Services The University of North Texas Objectives Upon completion of this
TRAUMA INFORMED CARE: THE IMPORTANCE OF THE WORKING ALLIANCE Justin Watts PhD. NCC, CRC Assistant Professor, Rehabilitation Health Services The University of North Texas Objectives Upon completion of this
Case Study. Salus. May 2010
 Case Study Salus May 2010 Background Based within Coatbridge, Salus consists of one of the largest NHS based multidisciplinary teams in Scotland. Through its various services Salus Case Management Services
Case Study Salus May 2010 Background Based within Coatbridge, Salus consists of one of the largest NHS based multidisciplinary teams in Scotland. Through its various services Salus Case Management Services
March 29, 2017 Debra K. Smith, Ph.D. St. Charles Hospital Port Jefferson, New York
 Traumatic Brain Injury: Management of Psychological and Behavioral Sequelae March 29, 2017 Debra K. Smith, Ph.D. St. Charles Hospital Port Jefferson, New York The Functional Impact of
Traumatic Brain Injury: Management of Psychological and Behavioral Sequelae March 29, 2017 Debra K. Smith, Ph.D. St. Charles Hospital Port Jefferson, New York The Functional Impact of
The Role of the Psychologist in an Early Intervention in Psychosis Team Dr Janice Harper, Consultant Clinical Psychologist Esteem, Glasgow, UK.
 The Role of the Psychologist in an Early Intervention in Psychosis Team Dr Janice Harper, Consultant Clinical Psychologist Esteem, Glasgow, UK. Ferrara, Italy, 5 th May 2017 Overview Essential Components
The Role of the Psychologist in an Early Intervention in Psychosis Team Dr Janice Harper, Consultant Clinical Psychologist Esteem, Glasgow, UK. Ferrara, Italy, 5 th May 2017 Overview Essential Components
A compensable claim for psychological injury can arise as an injury by itself with no physical injury or as a result of a physical injury.
 Section Policy 40 44.05.30 Section Title: Subject: Effective Date: Benefits Administration Adjudication and Compensation Adjudication of Psychological Injuries November 1, 2012, for all claims regardless
Section Policy 40 44.05.30 Section Title: Subject: Effective Date: Benefits Administration Adjudication and Compensation Adjudication of Psychological Injuries November 1, 2012, for all claims regardless
9/3/2014. Which impairs the ability to integrate these experiences in an adaptive manner.
 Presented by DaLene Forester Thacker, PhD Licensed Marriage and Family Therapist Licensed Professional Clinical Counselor Director and Trainer with AEI daleneforester@yahoo.com I was not able to use EMDR
Presented by DaLene Forester Thacker, PhD Licensed Marriage and Family Therapist Licensed Professional Clinical Counselor Director and Trainer with AEI daleneforester@yahoo.com I was not able to use EMDR
Anger and Chronic Pain
 What is anger? Anger is a natural emotional response that everyone experiences from time to time. It is an emotion that can range from mild irritation to intense rage. The experience of anger is related
What is anger? Anger is a natural emotional response that everyone experiences from time to time. It is an emotion that can range from mild irritation to intense rage. The experience of anger is related
Embedding Workplace Mental Health First Aid & Stress Management Summit 2018
 Embedding Workplace Mental Health First Aid & Stress Management Summit 2018 TAKE CONTROL Victoria Walford BA MBPs PGdip EMDR (Registered Psychologist & Psychotherapist) A successful global well-being strategy
Embedding Workplace Mental Health First Aid & Stress Management Summit 2018 TAKE CONTROL Victoria Walford BA MBPs PGdip EMDR (Registered Psychologist & Psychotherapist) A successful global well-being strategy
Copyright 2012 The Guilford Press. Cognitive impairment following workplace injuries can be time-limited or
 This is a chapter excerpt from Guilford Publications. Neuropsychological Assessment of Work-Related Injuries. Edited by Shane S. Bush and Grant L. Iverson. Copyright 2012. Purchase this book now: www.guilford.com/p/bush
This is a chapter excerpt from Guilford Publications. Neuropsychological Assessment of Work-Related Injuries. Edited by Shane S. Bush and Grant L. Iverson. Copyright 2012. Purchase this book now: www.guilford.com/p/bush
Understanding Chronic Pain: An Educational Session on Chronic Pain
 Understanding Chronic Pain: An Educational Session on Chronic Pain Matilda Nowakowski, Ph.D., C.Psych. Linette Savage Chronic Pain Clinic, St. Joseph s Healthcare Hamilton Objectives To better understand
Understanding Chronic Pain: An Educational Session on Chronic Pain Matilda Nowakowski, Ph.D., C.Psych. Linette Savage Chronic Pain Clinic, St. Joseph s Healthcare Hamilton Objectives To better understand
DR. GATCHEL HAS NO CONFLICTS OF INTEREST TO DISCLOSE. Gatchel
 Robert J. Gatchel, Ph.D., ABPP Nancy P. and John G. Penson Endowed Professor of Clinical Health Psychology Distinguished Professor of Psychology, College of Science Director, Center of Excellence for the
Robert J. Gatchel, Ph.D., ABPP Nancy P. and John G. Penson Endowed Professor of Clinical Health Psychology Distinguished Professor of Psychology, College of Science Director, Center of Excellence for the
Stress, Health, and Coping
 Stress, Health, and Coping. Health Psychology The field concerned with the promotion of health and the prevention and treatment of illness as it relates to psychological factors Stress The general term
Stress, Health, and Coping. Health Psychology The field concerned with the promotion of health and the prevention and treatment of illness as it relates to psychological factors Stress The general term
St George Hospital Renal Supportive Care Psychosocial Day, 10 th August Michael Noel, Supportive and Palliative Care Physician, Nepean Hospital
 St George Hospital Renal Supportive Care Psychosocial Day, 10 th August 2017 Michael Noel, Supportive and Palliative Care Physician, Nepean Hospital Michael.Noel@health.nsw.gov.au Hannah Burgess, Renal
St George Hospital Renal Supportive Care Psychosocial Day, 10 th August 2017 Michael Noel, Supportive and Palliative Care Physician, Nepean Hospital Michael.Noel@health.nsw.gov.au Hannah Burgess, Renal
SUMMARY DECISION NO. 1505/00. Chronic pain. DECIDED BY: Marafioti DATE: 21/03/2001 NUMBER OF PAGES: 6 pages ACT: WCA
 SUMMARY DECISION NO. 1505/00 Chronic pain. DECIDED BY: Marafioti DATE: 21/03/2001 NUMBER OF PAGES: 6 pages ACT: WCA 2001 ONWSIAT 869 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1505/00
SUMMARY DECISION NO. 1505/00 Chronic pain. DECIDED BY: Marafioti DATE: 21/03/2001 NUMBER OF PAGES: 6 pages ACT: WCA 2001 ONWSIAT 869 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 1505/00
Royal College of Psychiatrists Consultation Response
 Royal College of Psychiatrists Consultation Response DATE: 10 March 2017 RESPONSE OF: RESPONSE TO: THE ROYAL COLLEGE OF PSYCHIATRISTS in WALES HSCS Committee, Isolation and Loneliness The Royal College
Royal College of Psychiatrists Consultation Response DATE: 10 March 2017 RESPONSE OF: RESPONSE TO: THE ROYAL COLLEGE OF PSYCHIATRISTS in WALES HSCS Committee, Isolation and Loneliness The Royal College
Pain in People With Developmental Disabilities. Dr. Eileen Trigoboff and Dr. Daniel Trigoboff.
 Pain in People With Developmental Disabilities Dr. Eileen Trigoboff and Dr. Daniel Trigoboff Module 1 The Mechanics of Pain Outline Module 1 General Principles of Pain Individual Variables How Medications
Pain in People With Developmental Disabilities Dr. Eileen Trigoboff and Dr. Daniel Trigoboff Module 1 The Mechanics of Pain Outline Module 1 General Principles of Pain Individual Variables How Medications
1. Stress: any circumstances that threaten or are perceived to threaten one's well-being and thereby tax one's coping abilities
 Chapter Three Outline: Stress and Its Effects I. The nature of stress A. Stress is an everyday event 1. Stress: any circumstances that threaten or are perceived to threaten one's well-being and thereby
Chapter Three Outline: Stress and Its Effects I. The nature of stress A. Stress is an everyday event 1. Stress: any circumstances that threaten or are perceived to threaten one's well-being and thereby
Recognising and Treating Psychological Trauma. Dr Alastair Bailey Dr Andrew Eagle -
 Recognising and Treating Psychological Trauma Dr Alastair Bailey alastair.bailey@nhs.net Dr Andrew Eagle - andrew.eagle@nhs.net Normal Human Distress Risk of pathologising normal human behaviour It is
Recognising and Treating Psychological Trauma Dr Alastair Bailey alastair.bailey@nhs.net Dr Andrew Eagle - andrew.eagle@nhs.net Normal Human Distress Risk of pathologising normal human behaviour It is
Neurotic and Personality Disorders
 Neurotic and Personality Disorders LPT Gondar Mental Health Group www.le.ac.uk Neurosis Originally coined by the Scottish physician William Cullen in 1769. Included a range of conditions e.g. epilepsy,
Neurotic and Personality Disorders LPT Gondar Mental Health Group www.le.ac.uk Neurosis Originally coined by the Scottish physician William Cullen in 1769. Included a range of conditions e.g. epilepsy,
How to Find a Therapist for Emetophobia. Even if they don t know what it is. By Lori Riddle-Walker, EdD, MFT
 How to Find a Therapist for Emetophobia Even if they don t know what it is By Lori Riddle-Walker, EdD, MFT How to Find a Therapist for Emetophobia Emetophobia, also known as specific phobia of vomiting
How to Find a Therapist for Emetophobia Even if they don t know what it is By Lori Riddle-Walker, EdD, MFT How to Find a Therapist for Emetophobia Emetophobia, also known as specific phobia of vomiting
Recovery Oriented Prescribing Why take any medication?
 Recovery Oriented Prescribing Why take any medication? June 15, 2012 University of Wisconsin Department of Psychiatry Medical Director, Journey Mental Health Center of Dane County Consultant, Wisconsin
Recovery Oriented Prescribing Why take any medication? June 15, 2012 University of Wisconsin Department of Psychiatry Medical Director, Journey Mental Health Center of Dane County Consultant, Wisconsin
Violence and Mental Illness Resources Wednesday, August 16, :30 PM 5:00 PM
 Resources Wednesday, August 16, 2017 3:30 PM 5:00 PM Violence and Mental Illness Veronique N. Valliere, Psy.D. Licensed Psychologist Types of Violence/Aggression Affective or Reactive/Defensive High Level
Resources Wednesday, August 16, 2017 3:30 PM 5:00 PM Violence and Mental Illness Veronique N. Valliere, Psy.D. Licensed Psychologist Types of Violence/Aggression Affective or Reactive/Defensive High Level
Overview of Peer Support Programs
 Supporting Mental Health in First Responders Overview of Peer Support Programs BCFirstRespondersMentalHealth.com Introduction First responders attend calls and witness events that can cause them to experience
Supporting Mental Health in First Responders Overview of Peer Support Programs BCFirstRespondersMentalHealth.com Introduction First responders attend calls and witness events that can cause them to experience
Determining causation of traumatic versus preexisting. conditions. David Fisher, Ph.D., ABPP, LP Chairman of the Board PsyBar, LLC
 Determining causation of traumatic versus preexisting psychological conditions David Fisher, Ph.D., ABPP, LP Chairman of the Board PsyBar, LLC 952 285 9000 Part 1: First steps to determine causation Information
Determining causation of traumatic versus preexisting psychological conditions David Fisher, Ph.D., ABPP, LP Chairman of the Board PsyBar, LLC 952 285 9000 Part 1: First steps to determine causation Information
IMPORTANCE OF SELF-CARE. Dr. Heather Dye, LCSW, CSAC East Tennessee State University Johnson City, TN
 IMPORTANCE OF SELF-CARE Dr. Heather Dye, LCSW, CSAC East Tennessee State University Johnson City, TN Define and differentiate: Vicarious Trauma Secondary Traumatic Stress/Compassion Fatigue Burnout Discuss
IMPORTANCE OF SELF-CARE Dr. Heather Dye, LCSW, CSAC East Tennessee State University Johnson City, TN Define and differentiate: Vicarious Trauma Secondary Traumatic Stress/Compassion Fatigue Burnout Discuss
STRESS AND HEALTH CHAPTER 16
 1 STRESS AND HEALTH CHAPTER 16 STRESS & HEALTH Where are we going today? Definitions of stress Causes: Bring on the stressors! How does stress affect us physically? Physiological Stress Response Stress
1 STRESS AND HEALTH CHAPTER 16 STRESS & HEALTH Where are we going today? Definitions of stress Causes: Bring on the stressors! How does stress affect us physically? Physiological Stress Response Stress
SUMMARY DECISION NO. 1015/01. Psychotraumatic disability. DECIDED BY: McIntosh-Janis DATE: 05/04/2001 NUMBER OF PAGES: 8 pages ACT: WCA
 SUMMARY DECISION NO. 1015/01 Psychotraumatic disability. DECIDED BY: McIntosh-Janis DATE: 05/04/2001 NUMBER OF PAGES: 8 pages ACT: WCA 2001 ONWSIAT 1207 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL
SUMMARY DECISION NO. 1015/01 Psychotraumatic disability. DECIDED BY: McIntosh-Janis DATE: 05/04/2001 NUMBER OF PAGES: 8 pages ACT: WCA 2001 ONWSIAT 1207 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL
Tailoring Complex Pain Treatments: Strategies for Working With Providers
 Tailoring Complex Pain Treatments: Strategies for Working With Providers Graves Owen, MD, Paradigm Medical Director Steven Moskowitz, MD, Paradigm Senior Medical Director First, a Few Housekeeping Points
Tailoring Complex Pain Treatments: Strategies for Working With Providers Graves Owen, MD, Paradigm Medical Director Steven Moskowitz, MD, Paradigm Senior Medical Director First, a Few Housekeeping Points
Dr Lisa Bunting (Lecturer in Social Work, QUB) Mairead Lavery (title, SEHSCT) Nov 2017
 Mairead Lavery (title, SEHSCT) Nov 2017") Dr Lisa Bunting (Lecturer in Social Work, QUB) Mairead Lavery (title, SEHSCT) Nov 2017 STRUCTURE Defining Trauma and Adversity The Prevalence and Impact of Multiple Adversities How adversity causes poor
Dr Lisa Bunting (Lecturer in Social Work, QUB) Mairead Lavery (title, SEHSCT) Nov 2017 STRUCTURE Defining Trauma and Adversity The Prevalence and Impact of Multiple Adversities How adversity causes poor
Psychosocial Factors and Functional Capacity Evaluation Among Persons With Chronic Pain
 Journal of Occupational Rehabilitation, Vol. 13, No. 4, December 2003 ( C 2003) Psychosocial Factors and Functional Capacity Evaluation Among Persons With Chronic Pain Michael E. Geisser, 1,4 Michael E.
Journal of Occupational Rehabilitation, Vol. 13, No. 4, December 2003 ( C 2003) Psychosocial Factors and Functional Capacity Evaluation Among Persons With Chronic Pain Michael E. Geisser, 1,4 Michael E.
GEPIC. An Introduction to Guide for the Evaluation of Psychiatric Impairment for Clinicians. Dr Michael Duke Senior Forensic Psychiatrist
 GEPIC An Introduction to Guide for the Evaluation of Psychiatric Impairment for Clinicians Dr Michael Duke Senior Forensic Psychiatrist What is psychiatric impairment? A psychiatric impairment is any loss
GEPIC An Introduction to Guide for the Evaluation of Psychiatric Impairment for Clinicians Dr Michael Duke Senior Forensic Psychiatrist What is psychiatric impairment? A psychiatric impairment is any loss
DEPARTMENT <EXPERIMENTAL-CLINICAL AND HEALTH PSYCHOLOGY... > RESEARCH GROUP <.GHPLAB.. > PSYCHOLOGICAL EVALUATION. Geert Crombez
 DEPARTMENT RESEARCH GROUP PSYCHOLOGICAL EVALUATION Geert Crombez PSYCHOLOGICAL EVALUATION Why is psychological evaluation important? What
DEPARTMENT RESEARCH GROUP PSYCHOLOGICAL EVALUATION Geert Crombez PSYCHOLOGICAL EVALUATION Why is psychological evaluation important? What
The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain
 The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain IM4US CONFERENCE 25 AUGUST 2017 EMILY HURSTAK, MD, MPH, MAS SAN FRANCISCO DEPARTMENT OF
The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain IM4US CONFERENCE 25 AUGUST 2017 EMILY HURSTAK, MD, MPH, MAS SAN FRANCISCO DEPARTMENT OF
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 18/17
 WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 18/17 BEFORE: J. P. Moore : Vice-Chair E. Tracey : Member Representative of Employers S. Roth : Member Representative of Workers HEARING: January
WORKPLACE SAFETY AND INSURANCE APPEALS TRIBUNAL DECISION NO. 18/17 BEFORE: J. P. Moore : Vice-Chair E. Tracey : Member Representative of Employers S. Roth : Member Representative of Workers HEARING: January
 Psychopathology Psychopathy (con t) Psychopathy Characteristics High impulsivity Thrill seeking Low empathy Low anxiety What is the common factor? Callous Self-Centeredness N M P Dr. Robert Hare
Psychopathology Psychopathy (con t) Psychopathy Characteristics High impulsivity Thrill seeking Low empathy Low anxiety What is the common factor? Callous Self-Centeredness N M P Dr. Robert Hare