Dyspepsia and Chronic Gastritis
|
|
|
- Muriel Dennis
- 6 years ago
- Views:
Transcription
1
2 Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Dyspepsia and Chronic Gastritis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun, L. Martymianova, O. Bychkova, N. Lysenko, N. Makienko V.N. Karazin National University Medical School Internal Medicine Dept.

3 Plan of the Lecture Definition Epidemiology Mechanisms Classification Clinical presentation Diagnosis Treatment Prognosis Prophylaxis Abbreviations Diagnostic guidelines i.imgur.com/zgjb2di.png edc2.healthtap.com/ht-staging/user_answer/avatars/ /large/open-uri vk4qva.jpeg?
4 Definition Dyspepsia (Indigestion) is defined as one or more of the symptoms (Rome III criteria) : postprandial fullness (postprandial distress syndrome), early satiation due to inability to finish a normal sized meal (postprandial distress syndrome) and epigastric pain or burning (epigastric pain syndrome). Gastritis is a result of inflammation, irritation, or erosion of the lining of the stomach that can occur suddenly (acute) or gradually (chronic) and clinically may manifest with symptoms of upper abdominal pain, nausea, vomiting, bloating, loss of appetite and heartburn, sometimes with possible complications in forms of bleeding, stomach ulcers, and stomach tumors, etc.
5 Epidemiology: Dyspepsia Dyspepsia is a common problem worldwide In the United States, the point prevalence is approximately 25%, excluding those people who have typical gastroesophageal reflux disease (GERD) symptoms Approximately 9% of people who had no symptoms of dyspepsia annually in the prior year reported new symptoms on follow-up In Scandinavia, an incidence rate of less than 1% over 3 months has been reported Whatever the incidence, the number of subjects who develop dyspepsia is matched by a similar number of subjects who lose their symptoms, explaining the observation that the prevalence remains stable.
6 Epidemiology: Chronic Gastritis An estimated 50% of the world population is infected with H pylori; consequently, chronic gastritis is extremely frequent H pylori infection is highly prevalent in Asia and in developing countries, and multifocal atrophic gastritis and gastric adenocarcinomas are more prevalent in these areas Autoimmune gastritis is a relatively rare disease, most frequently observed in individuals of northern European descent and black people The frequency of pernicious anemia is increased in patients with autoimmune gastritis and other immunologic diseases, including Graves disease, myxedema, thyroiditis, vitiligo and hypoparathyroidism.
7 kjim.org/upload//thumbnails/kjim f1.gif hindawi.com/journals/grp/2012/562393/ Risk Factors: Dyspepsia Female gender Concomitant IBS Unemployment Alcohol 48 Smoking 44 NSAID IBS: irritable bowel syndrome NSAID: nonsteroidal anti-inflammatory drug

8 Risk Factors: Dyspepsia Some Medications that cause Dyspepsia Nonsteroidal anti-inflammatory drugs (NSAIDs) Cox-2 inhibitors Bisphosphonates Erythromycin Tetracyclines Iron Potassium supplements Acarbose Digitalis Theophylline Orlistat dealpain.net/wp-content/uploads/2016/03/oral-nsaids.jpg ncbi.nlm.nih.gov/pmc/articles/pmc /

9 Risk Factors: Chronic Gastritis African-American, Northern- European, Hispanic or Asian descent Infection Regular use of pain relievers Older age Excessive alcohol use Smoking Distress Erosion Bile reflux disease Major surgery Chronic autoimmune conditions images.medicinenet.com/images/appictures/gastritis-s3-causes.jpg
10 Etiology: Dyspepsia Eating too much Eating too rapidly Consuming fatty or greasy foods Consuming spicy foods Consuming too much coffee Consuming too much alcohol Consuming too much chocolate Consuming too many fizzy drinks Emotional trauma Gallstones Gastritis) Hiatus hernia Infection, especially with H pylori Nervousness Obesity Pancreatitis Peptic ulcers Smoking Some medications, such as antibiotics and NSAIDs Stomach cancer

11 Etiology: Dyspepsia Endoscopic findings in individuals with dyspepsia in the Italian population
12 Etiology: Chronic Gastritis Chronic gastritis may be caused by either infectious or noninfectious conditions Infectious forms include gastritis caused by H pylori and Helicobacter heilmannii infection; mycobacteriosis, syphilis, histoplasmosis, mucormycosis, South American blastomycosis, anisakiasis, or anisakidosis (granulomatous gastritis ); Strongyloides species, schistosomiasis, or Diphyllobothrium latum (parasitic gastritis); viral (e.g., CMV or herpesvirus) infection, etc. Noninfectious forms include autoimmune gastritis, chemical gastropathy (chronic bile reflux, NSAID and aspirin intake), uremic gastropathy, chronic noninfectious granulomatous gastritis (Crohn disease, sarcoidosis, Wegener granulomatosis, foreign bodies, cocaine use, rheumatoid nodules, gastric lymphoma), radiation injury to the stomach, etc.).
13 Mechanisms: Dyspepsia Patients may have abnormal motor function of the proximal stomach Increased perception of physiological or minor noxious stimuli has been demonstrated in both the fasting and postprandial states Although gastric sensorimotor dysfunction is the main pathophysiological finding, the relationship and relevance of these disorders to symptoms is largely unknown Studies attempting to identify a relation between H pylori infection and functional dyspepsia have yielded inconsistent and often confusing results.
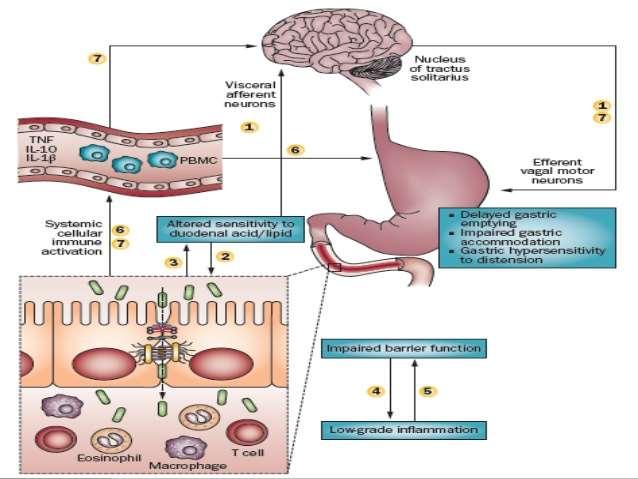
14 Mechanisms: Dyspepsia
15 Mechanisms: Chronic Gastritis Chronic gastritis is a progressive, irreversible decay (atrophy) of the lining (gastric mucosa) and glandular tissue within the stomach In some disorders the body targets the stomach as if it were a foreign protein or pathogen; it makes antibodies against, severely damages, and may even destroy the stomach or its lining In some cases bile, normally used to aid digestion in the small intestine, will enter through the pyloric valve of the stomach if it has been removed during surgery or does not work properly, also leading to gastritis Since 1992, chronic gastritis lesions are classified according to the Sydney system.

16 Mechanisms: Chronic Gastritis H pylori and NSAID have synergistic effects on gastric mucosal damage. Both H pylori infection and NSAID use have been found to independently and significantly increase the risk of gastric and duodenal mucosa damage and ulceration.

17 Mechanisms: Chronic Gastritis Natural history of Helicobacter pylori (H. pylori) infection

18 Classification: Dyspepsia & Chronic Gastritis (International Classification of Diseases (ICD)) XI Diseases of the digestive system K30 Functional dyspepsia K29 Gastritis and duodenitis K29.3 Chronic superficial gastritis K29.4 Chronic atrophic gastritis K29.5 Chronic gastritis, unspecified K29.6 Other gastritis (giant hypertrophic gastritis, granulomatous gastritis, Ménétrier disease) K29.7 Gastritis, unspecified
19 Classification: Dyspepsia Rome III Diagnostic Criteria for Functional Dyspepsia At least 3 months, with onset at least 6 months previously, of 1 or more of the following: Bothersome postprandial fullness Early satiation Epigastric pain Epigastric burning And No evidence of structural disease (including at upper endoscopy) that is likely to explain the symptoms
20 Classification: Dyspepsia Rome III Diagnostic Criteria for Functional Dyspepsia At least 3 months, with onset at least 6 months previously, of 1 or more of the following: Bothersome postprandial fullness Early satiation Epigastric pain Epigastric burning And No evidence of structural disease (including at upper endoscopy) that is likely to explain the symptoms
21 Classification: Dyspepsia Rome III Diagnostic Criteria for Epigastric Pain Syndrome At least 3 months, with onset at least 6 months previously, with ALL of the following: Pain and burning that is: intermittent localized to the epigastrium of at least moderate severity, at least once per week, and NOT: generalized or localized to other abdominal or chest regions relieved by defecation or flatulence fulfilling criteria for gallbladder or sphincter of Oddi disorders
22 Classification: Dyspepsia Rome III Diagnostic Criteria for Postprandial Distress Syndrome At least 3 months, with onset at least 6 months previously, of 1 or more of the following: Bothersome postprandial fullness Or 1. occurring after ordinary-sized meals 2. at least several times a week Early satiation 1. that prevents finishing a regular meal 2. and occurs at least several times a week.
23 Classification: Chronic Gastritis There are follows forms of chronic gastritis: Type A gastritis (autoimmune atrophic gastritis) may be triggered by a physical or psycho-emotional stressor that causes the individual's immune system to produce antibodies against certain cells in the stomach (parietal cells); destruction of these cells results in atrophy of the stomach tissue Type B gastritis (simple atrophic gastritis) is more common and is strongly associated with the presence of a certain bacterium (Helicobacter pylori) in the stomach mucosa Type AB gastritis (environmental) Chemical gastritis (reflux gastritis) Uncommon forms

24 Classification: Chronic Gastritis The updated Sydney System: Classification and Grading of Gastritis as the Basis of Diagnosis and Treatment Chart designed for the histological division of the original Sydney System as presented to the World Congress of Gastroenterology
25 Classification: Chronic Gastritis Operative Link for Gastritis Assessment (OLGA)
26 Classification: Chronic Gastritis There are two forms of chronic gastritis: Type A gastritis (also known as autoimmune atrophic gastritis) may be triggered by a physical or psychoemotional stressor that causes the individual's immune system to produce antibodies against certain cells in the stomach (parietal cells); destruction of these cells results in atrophy of the stomach tissue Type B gastritis (or simple atrophic gastritis) is more common and is strongly associated with the presence of a certain bacterium (Helicobacter pylori) in the stomach mucosa.
, vomiting, early satiety, and abdominal distention (swelling). image.shutterstock.")
27 Signs and Symptoms: Dyspepsia Most people feel pain and discomfort in the stomach or chest area generally soon after consuming food or drink, and in some cases during a meal or some time after a meal The following symptoms are also common: nausea, belching, feeling bloated (very full), vomiting, early satiety, and abdominal distention (swelling). image.shutterstock.com/z/stock-photo-indigestion-or-dyspepsia-stomach-disease-sign-and-symptoms jpg medicalnewstoday.com/articles/ php
28 History: Dyspepsia A detailed history is necessary to narrow the differential diagnosis and to identify gastroesophageal reflux disease (GERD) and nonsteroidal anti-inflammatory drug (NSAID)- induced dyspepsia, as well as patients with alarm Radiation of the pain to the back or personal or family history of pancreatitis may be indicative of chronic pancreatitis Significant weight loss, anorexia, vomiting, dysphagia, odynophagia, and a family history of gastrointestinal cancers suggest the presence of an underlying malignancy The presence of severe episodic epigastric or right upper quadrant abdominal pain lasting more than an hour or pain that occurs at any time is suggestive of symptomatic cholelithiasis.
29 Physical Exam: Dyspepsia The physical examination is usually normal, except for epigastric tenderness The presence of epigastric tenderness cannot accurately distinguish organic dyspepsia from functional dyspepsia Abdominal tenderness on palpation should be evaluated with the Carnett sign to determine if it is due to pain arising from the abdominal wall rather than due to inflammation of the underlying viscera: if the pain is decreased (negative Carnett s sign), the origin of pain is not from the abdominal wall and likely from an intra-abdominal organ, as the tensed abdominal wall muscles protect the viscera.
30 Complications: Dyspepsia The complications are relatively limited Since symptoms are most often provoked by eating, patients who alter their diets and reduce their intake of calories may lose weight Symptoms that awaken patients from sleep are more likely to be due to non-functional than functional disease Most commonly, dyspepsia interfere with patients' comfort and daily activities The interference with daily activities also can lead to problems with interpersonal relationships, especially with spouses Most patients live with their symptoms and infrequently visit physicians for diagnosis and treatment.
31 Red flags for people: Dyspepsia Age 50 years or older at first presentation Family history of gastric cancer with age of onset < 50 years Severe or persistent dyspepsia Previous peptic ulcer disease, particularly if complicated Ingestion of NSAIDs, including aspirin Signs and symptoms of chronic gastrointestinal bleeding Iron deficiency anemia Difficulty in swallowing Persistent or protracted vomiting Palpable abdominal mass Coughing spells or nocturnal aspiration Unexplained weight loss
32 Signs and Symptoms: Chronic Gastritis Many people experience no symptoms at all Upper central abdominal pain is the most common symptom; the pain may be dull, vague, burning, aching, gnawing, sore, or sharp; the pain is usually located in the upper central portion of the abdomen, but it may occur anywhere from the upper left portion of the abdomen around to the back Other signs and symptoms may include nausea, vomiting (if present, may be clear, green or yellow, blood-streaked, or completely bloody, depending on the severity of the stomach inflammation), belching (if present, usually does not relieve the pain much), bloating, early satiety, loss of appetite, unexplained weight loss.
33 History: Chronic Gastritis Patients may report vague stomach distress, a sensation of fullness, nausea, malaise, a heavy feeling in the stomach after meals, or ulcer-like symptoms Symptoms typically occur within 1 to 5 hours after meals With severe gastritis, the individual may also report chest pain, sweating, and feeling faint There may be a history of ulcers, recent use of NSAIDs, recent ingestion of highly acidic food or chemicals, recent radiation or surgical procedure, or past gastrointestinal illness Patients may report having eaten raw fish Patients history should include information regarding eating, drinking, and smoking habits as well as prescription and nonprescription drug use.
34 Physical Exam: Chronic Gastritis The exam results are most often normal Rarely, there is abdominal tenderness, pale skin, tachycardia, dyspnea, or hypotension Some findings are specifically associated with the particular complications of H pylori (associated gastritis and autoimmune gastritis) If gastric ulcers coexist, guaiac-positive stool may result from occult blood loss With severe cobalamin deficiency, the patient is pale and has slightly icteric skin and eyes The individual may have foul-smelling breath (halitosis), with bloating associated with bacterial overgrowth syndrome.
35 Complications: Chronic Gastritis Although gastritis may not produce symptoms, its complications do Left untreated, gastritis may lead to stomach ulcers and stomach bleeding, or even cancer of the stomach Another potential complication is a severe loss of blood Others include: intestinal metaplasia (the last stage of Barrett's esophagus), pernicious anemia caused by vitamin B12 insufficiency, peptic ulcers, stomach cancer.
36 Diagnosis: Dyspepsia Dyspepsia is diagnosed on the basis of typical symptoms and the absence of other gastrointestinal diseases Patients >55, or those with alarm features should undergo prompt endoscopy to rule out other gastrointestinal diseases In patients <55 with no alarm features, the clinician may consider two approximately equivalent management options: (i) test and treat for H. pylori using a validated noninvasive test and a trial of acid suppression if eradication is successful but symptoms do not resolve or (ii) an empiric trial of acid suppression with a proton pump inhibitor (PPI) for 4 8 wk. Repeat upper endoscopy (EGD) is not recommended once a firm diagnosis of functional dyspepsia has been made, unless completely new symptoms or alarm features develop.
37 Diagnosis: Chronic Gastritis The diagnosis may be established by a complete history and physical examination Some cases may require blood tests and other tests (endoscopy) or a consultation with a specialist (usually a gastroenterologist) The tests which may be used to verify gastritis include: evaluation for H. pylori by way of blood, breath or stool testing; blood cell counts (looking for anemia); liver and kidney functions, urinalysis, gallbladder and pancreas functions; pregnancy test; stool test (looking for blood); X-rays (an upper gastrointestinal series or a barium swallow); an electrocardiogram (ECG, EKG), endoscopy, stomach biopsy.

38 Diagnosis: Chronic Gastritis
39 Management: Dyspepsia Diet and lifestyle changes (consuming less fatty foods, coffee, alcohol and chocolates; sleeping at least 7 hours every night; and avoiding spicy foods) Antacids (over-the-counter, no prescription needed) H-2-receptor antagonists Proton pump inhibitors (PPIs) Prokinetics (the efficacy has been questioned) Antidepressants, if no causes for indigestion are found and the patient has not responded to treatments Psychological treatments Psychotherapy and behavioral therapy may also provide benefit in selected patients.

40 Management: Dyspepsia Schematic Diagram
41 Management: Chronic Gastritis Approach Considerations Treatment can be aimed at a specific etiologic agent, if such an agent is known When gastritis represents gastric involvement of a systemic disease, treatment is directed toward the primary disease Some entities manifested by chronic gastritis do not have wellestablished treatment protocols For example, in lymphocytic gastritis, some cases of spontaneous healing have been reported, however, because the disease has a chronic course, treatment is recommended (some studies have reported successful treatment of exudative lymphocytic gastritis with omeprazole).
42 Management: Chronic Gastritis Pharmacotherapy for H pylori If H pylori is identified as the underlying cause of gastritis, it should be eradicated Antibiotics that have proven effective against H pylori include clarithromycin, amoxicillin, metronidazole, tetracycline, and furazolidone Cure rates with single antibiotics have been poor (0-35%), that's why five regimens are approved by the US Food and Drug Administration (FDA) for the treatment of H pylori infection The most effective of these regimens is bismuth-metronidazoletetracycline (BMT) triple therapy, followed by ranitidine bismuth citrate plus clarithromycin and then by omeprazole plus clarithromycin. Quadruple therapies are recommended as second-line treatment when triple therapies fail.
43 Management: Chronic Gastritis Triple and Quadruple Pharmacotherapy for H pylori Triple therapies (with indicated adult dosing): Lansoprazole 30 mg, omeprazole 20 mg, or ranitidine bismuth citrate 400 mg orally twice daily Clarithromycin 500 mg orally twice daily Amoxicillin 1000 mg or metronidazole 500 mg orally twice daily Quadruple therapies (with indicated adult dosing): lansoprazole 30 mg or omeprazole 20 mg orally twice daily Tetracycline HCl 500 mg orally 4 times daily Bismuth subsalicylate 120 mg orally 4 times daily Metronidazole 500 mg orally 3 times daily
44 Management: Chronic Gastritis Long-Term Monitoring Pharmacotherapy for H pylori If a patient was treated for H pylori infection, confirm that the organism has been eradicated Evaluate eradication at least 4 weeks after the beginning of treatment. Eradication may be assessed by means of noninvasive methods such as the urea breath test or the stool antigen test Follow-up may be individualized, depending on findings during endoscopy (for example, if dysplasia is found at endoscopy, increased surveillance is necessary) For patients with atrophic gastritis or dysplasia, follow-up endoscopy is recommended after 6 months.
45 Prognosis: Dyspepsia Dyspepsia is not a disease, but rather a symptom of other diseases or disorders Consequently, the predicted outcome ultimately depends on the underlying cause of the dyspeptic symptoms.
46 Prognosis: Chronic Gastritis The prognosis is strongly related to the underlying cause Chronic gastritis may progress asymptomatically in some patients, whereas other patients report dyspeptic symptoms The clinical course may be worsened when patients develop any of the possible complications of H pylori infection, such as peptic ulcer or gastric malignancy Eradication of H pylori results in rapid cure of the infection with disappearance of the inflammatory infiltration of the gastric mucosa In patients with autoimmune gastritis, the major effects are consequent to the loss of parietal and chief cells and include achlorhydria, hypergastrinemia, loss of pepsin and pepsinogen, anemia, and an increased risk of gastric neoplasms.
47 Prophylaxis Prevention is by avoiding things that cause dyspepsia and gastritis Proper hygiene, hand washing, and eating and drinking only adequately cleaned or treated foods and fluids are first healthy ways to decrease risk of getting these conditions
48 Abbreviations ECG, EKG - electrocardiogram EGD - upper endoscopy FDA - Food and Drug Administration GERD - gastroesophageal reflux disease IBS - irritable bowel syndrome NSAIDs nonsteroidal anti-inflammatory drugs PPI - proton pump inhibitor
49 Diagnostic and treatment guidelines Approach to the adult with dyspepsia Evaluation and management of dyspepsia Evidence-based clinical practice guidelines for functional dyspepsia Gastritis Kyoto global consensus report on Helicobacter pylori gastritis Management of Dyspepsia Management of Helicobacter pylori infection the Maastricht IV/ Florence Consensus Report
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Helicobacter Pylori Testing HELICOBACTER PYLORI TESTING HS-131. Policy Number: HS-131. Original Effective Date: 9/17/2009
 Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Easy Choice Health Plan, Inc. Harmony Health Plan of Illinois, Inc. Missouri Care, Inc. Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona, Inc. WellCare Health Insurance of Illinois,
Management of dyspepsia and of Helicobacter pylori infection
 Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
Management of dyspepsia and of Helicobacter pylori infection The University of Nottingham John Atherton Wolfson Digestive Diseases Centre University of Nottingham, UK Community management of dyspepsia
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA
 MANAGEMENT OF DYSPEPSIA") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA o Patients of any age with ALARM signs should be referred through the 2-week referral system o Routine endoscopic investigation
KK College of Nursing Peptic Ulcer Badil D ass Dass, Lecturer 25th July, 2011
 KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
Gastritis National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is gastritis? Gastritis is a condition in which the stomach
GASTROINTESTINAL AND ANTIEMETIC DRUGS. Submitted by: Shaema M. Ali
 GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
GASTROINTESTINAL AND ANTIEMETIC DRUGS Submitted by: Shaema M. Ali GASTROINTESTINAL AND ANTIEMETIC DRUGS by: Shaema M. Ali There are four common medical conditions involving the GI system 1) peptic ulcers
SUPPLEMENTARY INFORMATION Associated with
 Table1: Rome III and Rome IV diagnostic criteria for IBS, functional constipation and functional dyspepsia. Rome III diagnostic criteria 1,2 Rome IV diagnostic criteria 3,4 Diagnostic criteria for IBS
Table1: Rome III and Rome IV diagnostic criteria for IBS, functional constipation and functional dyspepsia. Rome III diagnostic criteria 1,2 Rome IV diagnostic criteria 3,4 Diagnostic criteria for IBS
MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) MANAGEMENT OF DYSPEPSIA AND GASTRO-OESOPHAGEAL REFLUX DISEASE (GORD) Routine endoscopic investigation of patients of any age, presenting with dyspepsia
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA
 GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
GASTROINTESTINAL SYSTEM MANAGEMENT OF DYSPEPSIA MANAGEMENT Dyspepsia refers to a spectrum of usually intermittent upper gastrointestinal symptoms, including epigastric pain and heartburn. For the majority
6/25/ % 20% 50% 19% Functional Dyspepsia Peptic Ulcer GERD Cancer Other
 Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
Peptic Ulcer Disease and Dyspepsia John M. Inadomi, MD Professor of Medicine UCSF Chief, Clinical Gastroenterology San Francisco General Hospital Case History 49 y/o woman complains of several months of
QUICK QUERIES. Topical Questions, Sound Answers
 QUICK QUERIES Topical Questions, Sound Answers Dyspepsia: An Evidence-Based Approach Alan B. R. Thomson, MD, PhD, FRCPC, FACP, FACG Presented at the University of Alberta s Medical Grand Rounds, University
QUICK QUERIES Topical Questions, Sound Answers Dyspepsia: An Evidence-Based Approach Alan B. R. Thomson, MD, PhD, FRCPC, FACP, FACG Presented at the University of Alberta s Medical Grand Rounds, University
PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD. Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School
 PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School No disclosures Disclosures Overview Causes of peptic ulcer disease
PEPTIC ULCER DISEASE JOHN R SALTZMAN, MD Director of Endoscopy Brigham and Women s Hospital Professor of Medicine Harvard Medical School No disclosures Disclosures Overview Causes of peptic ulcer disease
Management of Dyspepsia
 MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
MPharm Programme Management of Dyspepsia Slide 1 of 28 Learning Objectives Understand the principles and wider implications underpinning evidence based therapeutics in the key clinical specialities Objectively
Treatment of Helicobacter pylori Infection
 Treatment of Helicobacter pylori Infection Epidemiology of H. pylori infection (North America) Which are the high risk groups? Epidemiology of H. pylori infection (North America) Which are the high risk
Treatment of Helicobacter pylori Infection Epidemiology of H. pylori infection (North America) Which are the high risk groups? Epidemiology of H. pylori infection (North America) Which are the high risk
What Is Peptic Ulcer Disease?
 What Is Peptic Ulcer Disease? Peptic ulcer disease is when painful sores form in the lining of the stomach, duodenum (start of the small intestine) or bowels. An ulcer can cause belly pain and, in some
What Is Peptic Ulcer Disease? Peptic ulcer disease is when painful sores form in the lining of the stomach, duodenum (start of the small intestine) or bowels. An ulcer can cause belly pain and, in some
Functional Heartburn and Dyspepsia
 Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Functional Heartburn and Dyspepsia Nicholas Shaheen, MD, MPH Center for Esophageal Diseases and Swallowing University of North Carolina Objectives Understand the means of diagnosing functional heartburn
Non-Ulcer Dyspepsia: what is it? What can we do with these patients? Overview. Dyspepsia Definition. Functional Dyspepsia. Dyspepsia the Basics
 Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
Non-Ulcer : what is it? What can we do with these patients? Temporal Changes and Geographic Variations in Developing Peptic Ulcer Disease Gastric Cancer 1900 Eamonn M M Quigley MD FACG Alimentary Pharmabiotic
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Guidelines for the Management of Dyspepsia and GORD. Gastroenterology/ Acute Adult Governance. Drugs and Therapeutics Committee
 Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Guidelines for the Management of Dyspepsia and GORD Document type: Version: 3.0 Author (name): Author (designation): Validated by Prescribing Dr. G. Lipscomb Date validated October 2015 Ratified by: Date
Helicobacter 2008;13:1-6. Am J Gastroent 2007;102: Am J of Med 2004;117:31-35.
 An Update on Helicobacter pylori and Its Treatment Trenika Mitchell, PharmD, BCPS Clinical Assistant Professor University of Kentucky College of Pharmacy October 18, 2008 Objectives Review the epidemiology
An Update on Helicobacter pylori and Its Treatment Trenika Mitchell, PharmD, BCPS Clinical Assistant Professor University of Kentucky College of Pharmacy October 18, 2008 Objectives Review the epidemiology
GI update. Common conditions and concerns my patients frequently asked about
 GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
GI update Common conditions and concerns my patients frequently asked about Specific conditions I ll try to cover today 1. Colon polyps, colorectal cancer and colonoscopy 2. Crohn s disease 3. Peptic ulcer
Proton Pump Inhibitors Drug Class Prior Authorization Protocol
 Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Proton Pump Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review
Urea Breath Test for Diagnosis of Helicobactor pylori. Original Policy Date 12:2013
 MP 2.04.04 Urea Breath Test for Diagnosis of Helicobactor pylori Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index
MP 2.04.04 Urea Breath Test for Diagnosis of Helicobactor pylori Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index
SASKATCHEWAN REGISTERED NURSES ASSOCIATION
 DEFINITION Reflux of gastric contents into the esophagus, which results in esophageal irritation or inflammation. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dysphagia (solid food, progressive)
DEFINITION Reflux of gastric contents into the esophagus, which results in esophageal irritation or inflammation. IMMEDIATE CONSULTATION REQUIRED IN THE FOLLOWING SITUATIONS Dysphagia (solid food, progressive)
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
DYSPEPSIA Dyspepsia indigestion during or after eating Full Heat, burning or pain Note: one of every four people
 What Is Dyspepsia? Dyspepsia, also known as indigestion, can have multiple symptoms. Feelings of indigestion happen during or after eating. If you have indigestion you might feel: Full during a meal. Painful
What Is Dyspepsia? Dyspepsia, also known as indigestion, can have multiple symptoms. Feelings of indigestion happen during or after eating. If you have indigestion you might feel: Full during a meal. Painful
UPPER GI DISEASES 11/15/2014. Lesson Objectives. GI Tract Review. NUTR 2050 Nutrition for Nursing Professionals. Mrs. Deborah A. Hutcheon, MS, RD, LD
 UPPER GI DISEASES NUTR 2050 Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Describe causes and contributing
UPPER GI DISEASES NUTR 2050 Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Describe causes and contributing
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: helicobacter_pylori_testing 01/01/2019 N/A 01/01/2020 01/01/2019 Policy Effective April 1, 2019 Description
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: helicobacter_pylori_testing 01/01/2019 N/A 01/01/2020 01/01/2019 Policy Effective April 1, 2019 Description
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)?
?") WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
WHAT IS GASTROESOPHAGEAL REFLUX DISEASE (GERD)? The term gastroesophageal reflux describes the movement (or reflux) of stomach contents back up into the esophagus, the muscular tube that extends from the
CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS. 1. Which of the following is not a common cause of peptic ulcer disease (PUD)?
?") CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS 1. Which of the following is not a common cause of peptic ulcer disease (PUD)? A. Chronic alcohol ingestion B. Nonsteroidal antiinflammatory
CHAPTER 18. PEPTIC ULCER DISEASE, SELF-ASSESSMENT QUESTIONS 1. Which of the following is not a common cause of peptic ulcer disease (PUD)? A. Chronic alcohol ingestion B. Nonsteroidal antiinflammatory
ACG Clinical Guideline: Treatment of Helicobacter pylori Infection
 ACG Clinical Guideline: Treatment of Helicobacter pylori Infection William D. Chey, MD, FACG 1, Grigorios I. Leontiadis, MD, PhD 2, Colin W. Howden, MD, FACG 3 and Steven F. Moss, MD, FACG 4 1 Division
ACG Clinical Guideline: Treatment of Helicobacter pylori Infection William D. Chey, MD, FACG 1, Grigorios I. Leontiadis, MD, PhD 2, Colin W. Howden, MD, FACG 3 and Steven F. Moss, MD, FACG 4 1 Division
Peptic Ulcer Disease Update
 Peptic Ulcer Disease Update Col Pat Storms RAM 2005 Disclosure Information 84th Annual AsMA Scientific Meeting Col Patrick Storms I have no financial relationships to disclose. I will discuss the following
Peptic Ulcer Disease Update Col Pat Storms RAM 2005 Disclosure Information 84th Annual AsMA Scientific Meeting Col Patrick Storms I have no financial relationships to disclose. I will discuss the following
Heartburn, also referred to acid reflux, happens when stomach acid flows back (refluxes) into your esophagus.
 into your esophagus.") WHILE almost everyone experiences mild heartburn from time to time and many individuals have some antacids or another medication on hand for its relief, talk to your doctor, if you have heartburn more
WHILE almost everyone experiences mild heartburn from time to time and many individuals have some antacids or another medication on hand for its relief, talk to your doctor, if you have heartburn more
Gastro-oesophageal reflux disease and peptic ulcer disease. By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D
 Gastro-oesophageal reflux disease and peptic ulcer disease By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D Gastro-oesophageal reflux disease and peptic ulcer disease Learning objectives:
Gastro-oesophageal reflux disease and peptic ulcer disease By: Dr. Singanamala Suman Assistant Professor Department of Pharm.D Gastro-oesophageal reflux disease and peptic ulcer disease Learning objectives:
Management of dyspepsia in adults in primary care
 Dyspepsia Management of dyspepsia in adults in primary care June 2005. The recommendations on referral for endoscopy in this NICE guideline have been amended in line with the recommendation in the NICE
Dyspepsia Management of dyspepsia in adults in primary care June 2005. The recommendations on referral for endoscopy in this NICE guideline have been amended in line with the recommendation in the NICE
THE CONNECTIVE TISSUE AND EPITHELIUM
 THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies
 Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Optimizing the Upper GI: Mind, Mouth, and Stomach What Can Go Wrong With Dr. Ritamarie Loscalzo
 Optimizing the Upper GI: Mind, Mouth, and Stomach What Can Go Wrong With Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one-onone relationship
Optimizing the Upper GI: Mind, Mouth, and Stomach What Can Go Wrong With Dr. Ritamarie Loscalzo Medical Disclaimer: The information in this presentation is not intended to replace a one-onone relationship
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
Heartburn. Understanding and Treating. Heal n Cure For appointments call
 A C P S P E C I A L R E P O R T Understanding and Treating Heartburn What is Heartburn? It begins as a burning pain in the middle of your chest, behind the breastbone, often after a big meal. The burning
A C P S P E C I A L R E P O R T Understanding and Treating Heartburn What is Heartburn? It begins as a burning pain in the middle of your chest, behind the breastbone, often after a big meal. The burning
Reflux of gastric contents, particularly acid, into the esophagus
 Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
Heartburn Reflux of gastric contents, particularly acid, into the esophagus Patient assessment with GERD 1-signs and symptoms The hallmark of typical symptom of GERD is heartburn (restrosternal),acid regurgitation,
TBURN TBURN BURN ARTBURN EARTBURN EART HEARTBURN: HOW TO GET IT OFF YOUR CHEST
 TBURN BURN TBURN ARTBURN. EARTBURN EART N EARTBURN HEARTBURN: HOW TO GET IT OFF YOUR CHEST Do you sometimes wake up at night with a sharp, burning sensation in your chest? Does this sometimes happen during
TBURN BURN TBURN ARTBURN. EARTBURN EART N EARTBURN HEARTBURN: HOW TO GET IT OFF YOUR CHEST Do you sometimes wake up at night with a sharp, burning sensation in your chest? Does this sometimes happen during
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON
 HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON Indigestion is a condition that is often a symptom of another, underlying condition and is associated with various forms of discomfort in the stomach including
HOW TO NATURALLY TREAT INDIGESTION YOGI CAMERON Indigestion is a condition that is often a symptom of another, underlying condition and is associated with various forms of discomfort in the stomach including
Outline. Definition (s) Epidemiology Pathophysiology Management With an emphasis on recent developments
 Epidemiology Pathophysiology Management With an emphasis on recent developments") Chronic Dyspepsia Eamonn M M Quigley MD FRCP FACP MACG FRCPI Lynda K and David M Underwood Center for Digestive Disorders Houston Methodist Hospital Houston, Texas Outline Definition (s) Epidemiology Pathophysiology
Chronic Dyspepsia Eamonn M M Quigley MD FRCP FACP MACG FRCPI Lynda K and David M Underwood Center for Digestive Disorders Houston Methodist Hospital Houston, Texas Outline Definition (s) Epidemiology Pathophysiology
Peptic Ulcer Disease and NSAIDs
 Peptic Ulcer Disease and NSAIDs National Digestive Diseases Information Clearinghouse What is a peptic ulcer? A peptic ulcer is a sore on the inner lining of the stomach or duodenum the first part of the
Peptic Ulcer Disease and NSAIDs National Digestive Diseases Information Clearinghouse What is a peptic ulcer? A peptic ulcer is a sore on the inner lining of the stomach or duodenum the first part of the
Laparoscopic Anti-Reflux (GERD) Surgery Patient Information from SAGES
 Surgery Patient Information from SAGES") SAGES Society of American Gastrointestinal and Endoscopic Surgeons https://www.sages.org Laparoscopic Anti-Reflux (GERD) Surgery Patient Information from SAGES Author : SAGES Webmaster Surgery for Heartburn
SAGES Society of American Gastrointestinal and Endoscopic Surgeons https://www.sages.org Laparoscopic Anti-Reflux (GERD) Surgery Patient Information from SAGES Author : SAGES Webmaster Surgery for Heartburn
Epidemiology of Peptic Ulcer Disease
 Epidemiology of Peptic Ulcer Disease Introduction Peptic Ulcer Disease (PUD) is disruption of the mucosal integrity of the stomach and/or duodenum leading to a local defect or excavation due to active
Epidemiology of Peptic Ulcer Disease Introduction Peptic Ulcer Disease (PUD) is disruption of the mucosal integrity of the stomach and/or duodenum leading to a local defect or excavation due to active
Barrett s Oesophagus Information Leaflet THE DIGESTIVE SYSTEM. gutscharity.org.
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about Barrett s Oesophagus Barrett s Oesophagus is the term used for a pre-cancerous condition where the normal
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
GI Pharmacology. Dr. Alia Shatanawi 5/4/2018
 GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
GI Pharmacology Dr. Alia Shatanawi 5/4/2018 Drugs Used in Gastrointestinal Diseases Drugs used in Peptic Ulcer Diseases. Drugs Stimulating Gastrointestinal Motility &Laxatives. Antidiarrheal Agents. Drugs
PATIENT INFORMATION FROM YOUR SURGEON & SAGES Laparoscopic Anti-Reflux (GERD) Surgery
 Surgery") Patient Information published on: 03/2004 by the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) PATIENT INFORMATION FROM YOUR SURGEON & SAGES Laparoscopic Anti-Reflux (GERD) Surgery
Patient Information published on: 03/2004 by the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) PATIENT INFORMATION FROM YOUR SURGEON & SAGES Laparoscopic Anti-Reflux (GERD) Surgery
National Digestive Diseases Information Clearinghouse
 Gastritis National Digestive Diseases Information Clearinghouse What is gastritis? Gastritis is a condition in which the stomach lining known as the mucosa is inflamed, or swollen. The stomach lining contains
Gastritis National Digestive Diseases Information Clearinghouse What is gastritis? Gastritis is a condition in which the stomach lining known as the mucosa is inflamed, or swollen. The stomach lining contains
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Update on the pathological classification of gastritis. Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada
 Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University
 Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University") CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
CHAPTER 11 Functional Gastrointestinal Disorders (FGID) Mr. Ashok Kumar Dept of Pharmacy Practice SRM College of Pharmacy SRM University 1 Definition of FGID Chronic and recurrent symptoms of the gastrointestinal
Heartburn Overview. Causes & Risk Factors
 Return to Web version Heartburn Overview What is heartburn? Despite its name, heartburn doesn't affect the heart. Heartburn is a burning feeling in the lower chest, along with a sour or bitter taste in
Return to Web version Heartburn Overview What is heartburn? Despite its name, heartburn doesn't affect the heart. Heartburn is a burning feeling in the lower chest, along with a sour or bitter taste in
June By: Reza Gholami
 ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
ACG/CAG guideline on Management of Dyspepsia June 2017 By: Reza Gholami DEFINITION OF DYSPEPSIA AND SCOPE OF THE GUIDELINE Dyspepsia was originally defined as any symptoms referable to the upper gastrointestinal
B. Cystic Teratoma: Refer to virtual microscope slide p_223 ovary, teratoma and compare to normal virtual microscope slide 086 ovary.
 LAB 2: THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
LAB 2: THE CONNECTIVE TISSUE AND EPITHELIUM The focus of this week s lab will be pathology of connective tissue and epithelium. The lab will introduce you to the four basic tissue types: epithelium, connective
Functional Dyspepsia. Norbert Welkovics Heine van der Walt
 Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
Norbert Welkovics Heine van der Walt Characteristics: Central abdomen Pain or discomfort Not associated with bowel movements No structural or biochemical abnormalty Definition Part of Gastroduodenal disorders
GERD. Gastroesophageal reflux disease, or GERD, occurs when acid from the. stomach backs up into the esophagus. Normally, food travels from the
 GERD What is GERD? Gastroesophageal reflux disease, or GERD, occurs when acid from the stomach backs up into the esophagus. Normally, food travels from the mouth, down through the esophagus and into the
GERD What is GERD? Gastroesophageal reflux disease, or GERD, occurs when acid from the stomach backs up into the esophagus. Normally, food travels from the mouth, down through the esophagus and into the
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Putting Chronic Heartburn On Ice
 Putting Chronic Heartburn On Ice Over the years, gastroesophageal reflux disease has proven to be one of the most common complaints facing family physicians. With quicker diagnosis, this pesky ailment
Putting Chronic Heartburn On Ice Over the years, gastroesophageal reflux disease has proven to be one of the most common complaints facing family physicians. With quicker diagnosis, this pesky ailment
Diarrhea may be: Acute (short-term, usually lasting several days), which is usually related to bacterial or viral infections.
, which is usually related to bacterial or viral infections.") Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
PATIENT HISTORY FORM
 PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
PATIENT HISTORY FORM Date: Page 1 of 5 Last Name: First Name: Middle Initial: Referred By: Age: Primary Care Doctor: Please provide name(s) of other physician(s) that you have visited within the last year:
Esophageal Disorders. Learning Objectives. Introduction. Gastroesophageal Reflux Disease. Reza Shaker, MD, and Benson T.
 Esophageal Disorders Reza Shaker, MD, and Benson T. Massey, MD, FACP Learning Objectives AFTER COMPLETING THIS CHAPTER, THE LEARNER SHOULD BE ABLE TO: 1. Recognize the typical and atypical presentations
Esophageal Disorders Reza Shaker, MD, and Benson T. Massey, MD, FACP Learning Objectives AFTER COMPLETING THIS CHAPTER, THE LEARNER SHOULD BE ABLE TO: 1. Recognize the typical and atypical presentations
SURGERY LAPAROSCOPIC ANTI-REFLUX (GORD) SURGERY
 SURGERY") LAPAROSCOPIC ANTI-REFLUX (GORD) If you suffer from heartburn, your surgeon may have recommended Laparoscopic Anti-reflux Surgery to treat this condition, technically referred to as Gastro-oesophageal Reflux
LAPAROSCOPIC ANTI-REFLUX (GORD) If you suffer from heartburn, your surgeon may have recommended Laparoscopic Anti-reflux Surgery to treat this condition, technically referred to as Gastro-oesophageal Reflux
University Medical Center at Brackenridge. Gastroenterology Clinic Worksheet
 Gastroenterology Clinic Worksheet 1. GI Bleeding (occult or symptomatic) a. CBC b. Iron, Ferritin b. Medication history 2. Iron Deficiency Anemia and no evident source (if no iron deficiency consider hematological
Gastroenterology Clinic Worksheet 1. GI Bleeding (occult or symptomatic) a. CBC b. Iron, Ferritin b. Medication history 2. Iron Deficiency Anemia and no evident source (if no iron deficiency consider hematological
Sequioa Education Systems, Inc. 1
 Functional Diagnostic Medicine Training Program Module 2 The Functional Diagnostic Medicine Approach in the Treatment of Gastrointestinal Dysfunction and Disease Dr. Wayne L. Sodano, D.C., D.A.B.C.I. &
Functional Diagnostic Medicine Training Program Module 2 The Functional Diagnostic Medicine Approach in the Treatment of Gastrointestinal Dysfunction and Disease Dr. Wayne L. Sodano, D.C., D.A.B.C.I. &
Acid-Peptic Diseases of the Stomach and Duodenum Including Helicobacter pylori and NSAIDs Prof. Sheila Crowe
 Acid-Peptic Diseases of the Stomach and Duodenum Including Helicobacter pylori and NSAIDs 1 Division of Gastroenterology UC San Diego School of Medicine Clinical presentations of Helicobacter pylori infection
Acid-Peptic Diseases of the Stomach and Duodenum Including Helicobacter pylori and NSAIDs 1 Division of Gastroenterology UC San Diego School of Medicine Clinical presentations of Helicobacter pylori infection
Speaker disclosure. Objectives. GERD: Who and When to Treat 7/21/2015
 GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
GERD: Who and When to Treat Eugenio J Hernandez, MD Gastrohealth, PL Assistant Professor of Clinical Medicine, FIU Herbert Wertheim School of Medicine Speaker disclosure I do not have any relevant commercial
Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery.
 Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery. Everything you ever wanted to know about gastric sleeve surgery. What
Surgery while taking Protonix? 1,368 conversations on the web about experiences with taking Protonix before or after having a Surgery. Everything you ever wanted to know about gastric sleeve surgery. What
Indigestion (dyspepsia)
") Commissioning pathways Indigestion (dyspepsia) Supplementary information to be read in conjunction with the pathway Reference Supplementary Information 1.1 Symptom Description Annual incidence 40%. Prevalence
Commissioning pathways Indigestion (dyspepsia) Supplementary information to be read in conjunction with the pathway Reference Supplementary Information 1.1 Symptom Description Annual incidence 40%. Prevalence
Chronic Pancreatitis
 Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Chronic Pancreatitis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun,
Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Chronic Pancreatitis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun,
Indigestion (1 of 5) What is indigestion? What causes indigestion?
 What is indigestion? What causes indigestion?") i If you need your information in another language or medium (audio, large print, etc) please contact Customer Care on 0800 374 208 or send an email to: customercare@ salisbury.nhs.uk You are entitled
i If you need your information in another language or medium (audio, large print, etc) please contact Customer Care on 0800 374 208 or send an email to: customercare@ salisbury.nhs.uk You are entitled
GASTROESOPHAGEAL REFLUX
 DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (404) 270-7479 GASTROESOPHAGEAL REFLUX DEFINITION: *MONTREAL CONSENSUS DEFINED GERD AS A CONDITION WHICH
DR. PHILIP K. BLUSTEIN M.D. F.R.C.P.(C) 415 14 TH ST. NW. CALGARY AB T2N2A1 PHONE (403) 270-9555 FAX (404) 270-7479 GASTROESOPHAGEAL REFLUX DEFINITION: *MONTREAL CONSENSUS DEFINED GERD AS A CONDITION WHICH
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Helicobacter and gastritis
 1 Helicobacter and gastritis Dr. Hala Al Daghistani Helicobacter pylori is a spiral-shaped gram-negative rod. H. pylori is associated with antral gastritis, duodenal (peptic) ulcer disease, gastric ulcers,
1 Helicobacter and gastritis Dr. Hala Al Daghistani Helicobacter pylori is a spiral-shaped gram-negative rod. H. pylori is associated with antral gastritis, duodenal (peptic) ulcer disease, gastric ulcers,
Stomach Pain Evidence-Based Methods in the Diagnosis and Treatment of Dyspepsia
 1 (11) Stomach Pain Evidence-Based Methods in the Diagnosis and Treatment of Dyspepsia Summary and Conclusions Introduction Following headache and fatigue, stomach problems represent one of the most common
1 (11) Stomach Pain Evidence-Based Methods in the Diagnosis and Treatment of Dyspepsia Summary and Conclusions Introduction Following headache and fatigue, stomach problems represent one of the most common
EMILOK Global. (omeprazole) Composition: Each capsule contains 20 mg omeprazole as enteric-coated
 Composition: Each capsule contains 20 mg omeprazole as enteric-coated") EMILOK Global (omeprazole) Composition: Each capsule contains 20 mg omeprazole as enteric-coated granules. Properties: Emilok (omeprazole) belongs to the group of proton pump inhibitors, inhibits both
EMILOK Global (omeprazole) Composition: Each capsule contains 20 mg omeprazole as enteric-coated granules. Properties: Emilok (omeprazole) belongs to the group of proton pump inhibitors, inhibits both
FEDERAL BUREAU OF PRISONS CLINICAL PRACTICE GUIDELINES GASTROESOPHAGEAL REFLUX DISEASE (GERD) DYSPEPSIA, AND PEPTIC ULCER DISEASE, NOVEMBER, 2001
 DYSPEPSIA, AND PEPTIC ULCER DISEASE, NOVEMBER, 2001") FEDERAL BUREAU OF PRISONS CLINICAL PRACTICE GUIDELINES GASTROESOPHAGEAL REFLUX DISEASE (GERD) DYSPEPSIA, AND PEPTIC ULCER DISEASE, NOVEMBER, 2001 PURPOSE The Federal Bureau of Prisons Clinical Practice
FEDERAL BUREAU OF PRISONS CLINICAL PRACTICE GUIDELINES GASTROESOPHAGEAL REFLUX DISEASE (GERD) DYSPEPSIA, AND PEPTIC ULCER DISEASE, NOVEMBER, 2001 PURPOSE The Federal Bureau of Prisons Clinical Practice
Last Revised: September 15 Last Reviewed: September EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)
/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE)") 7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
7.0 GASTROENTEROLOGY Last Revised: September 5 Last Reviewed: September 5 7. EOSINOPHILIC ESOPHAGITIS (EOE)/PPI-RESPONSIVE ESOPHAGEAL EOSINOPHILIA (PPI-REE) Significant changes: ) Addition of PPI-REE as
Disclosures. Co-founder and Chief Science Officer, TechLab
 H. pylori testing Disclosures Co-founder and Chief Science Officer, TechLab Learning Objectives Evaluate the appropriate testing methodology by balancing performance, economics, and workflow. Discuss the
H. pylori testing Disclosures Co-founder and Chief Science Officer, TechLab Learning Objectives Evaluate the appropriate testing methodology by balancing performance, economics, and workflow. Discuss the
Dyspepsia: alarm symptoms, investigation and management
 Drug review Dyspepsia Dyspepsia: alarm symptoms, investigation and management SPL Steven Fong MRCP and Jason Dunn PhD, MRCP Dyspepsia is a common symptom and the priority is to identify alarm signals that
Drug review Dyspepsia Dyspepsia: alarm symptoms, investigation and management SPL Steven Fong MRCP and Jason Dunn PhD, MRCP Dyspepsia is a common symptom and the priority is to identify alarm signals that
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
James Paget University Hospitals. NHS Foundation Trust. Hiatus hernia. Patient Information
 James Paget University Hospitals NHS Foundation Trust Hiatus hernia Patient Information What is a hiatus hernia? A hiatus hernia can cause highly irritating stomach contents, such as acid, to move up into
James Paget University Hospitals NHS Foundation Trust Hiatus hernia Patient Information What is a hiatus hernia? A hiatus hernia can cause highly irritating stomach contents, such as acid, to move up into
Policy Evaluation: Proton Pump Inhibitors (PPIs)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION. OSCE 2: Abdominal Pain
 BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 2: Abdominal Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and
BATES VISUAL GUIDE TO PHYSICAL EXAMINATION OSCE 2: Abdominal Pain This video format is designed to help you prepare for objective structured clinical examinations, or OSCEs. You are going to observe and
GI -A & P Review PUD. Peptic Ulcer Disease (PUD) Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer
 Objectives: Identify different types Gastric Ulcer Duodenal Ulcer Stress Ulcer") GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
GI -A & P Review Lemone and Burke Chapters 21-26 Mouth Pharynx Esophagus Stomach Small Intestines Large Intestines Liver and Gallbladder Pancreas Peptic Ulcer Disease (PUD) Objectives: Identify different
Gastroesophageal Reflux Disease (GERD)
") Gastroesophageal Reflux Disease (GERD) Acid Reflux Acid reflux occurs when acid from the stomach moves backwards into the esophagus. Heartburn Heartburn is a symptom of acid reflux and GERD. It may feel
Gastroesophageal Reflux Disease (GERD) Acid Reflux Acid reflux occurs when acid from the stomach moves backwards into the esophagus. Heartburn Heartburn is a symptom of acid reflux and GERD. It may feel
-Mohammad Ashraf. -Anas Raed. -Alia Shatnawi. 1 P a g e
 -1 -Mohammad Ashraf -Anas Raed -Alia Shatnawi 1 P a g e Dr. Alia started the lecture by talking about subjects we are going to cover through this course; you can refer to the record if you are interested.
-1 -Mohammad Ashraf -Anas Raed -Alia Shatnawi 1 P a g e Dr. Alia started the lecture by talking about subjects we are going to cover through this course; you can refer to the record if you are interested.
Dyspepsia is a problem commonly seen by primary
 Concise Review for Clinicians Nonulcer Dyspepsia: What It Is and What It Is Not G. RICHARD LOCKE III, MD Nonulcer dyspepsiais a description of persistent or recurrent upper abdominal pain or discomfort
Concise Review for Clinicians Nonulcer Dyspepsia: What It Is and What It Is Not G. RICHARD LOCKE III, MD Nonulcer dyspepsiais a description of persistent or recurrent upper abdominal pain or discomfort
Gastrointestinal Markers
 Gastrointestinal Markers Session 2 Gastrointestinal System Reference Ranges Optimal Range Ttl Total Protein ti 69 6.9 74 7.4 Globulin 2.4 2.8 BUN 10 16 Creatinine 0.8 1.1 Phosphorous 3.0 4.0 Eosinophils
Gastrointestinal Markers Session 2 Gastrointestinal System Reference Ranges Optimal Range Ttl Total Protein ti 69 6.9 74 7.4 Globulin 2.4 2.8 BUN 10 16 Creatinine 0.8 1.1 Phosphorous 3.0 4.0 Eosinophils