Case-Based Approach to Common Dermatologic Neoplasms
|
|
|
- Jeremy Carr
- 5 years ago
- Views:
Transcription
1 Case-Based Approach to Common Dermatologic Neoplasms Patrick Retterbush, MD, FAAD Mohs Surgery & Dermatologic Oncology Associate Member of the American College of Mohs Surgery Private Practice: Lockman Dermatology January 27 th 2018
2 Disclosure of Relevant Financial Relationships I do not have any relevant financial relationships, commercial interests, and/or conflicts of interest regarding the content of this presentation.
3 Goals/Objectives Recognize common benign growths Recognize common malignant growths Useful clues & examination for evaluating melanocytic nevi and when to be concerned for melanoma/atypical moles How to perform a basic skin biopsy and which method/type to choose Basic treatment/when to refer
4 Key Questions & Physical Examination Findings for a Growth History How long has the lesion been present? years, months, weeks Has it changed? Size Shape Color Symptoms pain, bleeding, itch? Over what time frame? PMH: prior skin cancers SCC/BCCs vs. melanoma blistering sunburns in childhood tanning bed use sunbather FH melanoma in 1 st degree relatives Physical Examination Describing a growth flat or raised? flat macule (<1cm) or patch (>1cm) raised papule (<1cm) or plaque (>1cm) nodule if deep (majority of lesion in dermis/sq) secondary descriptive features scaly (hyperkeratosis, retention of strateum corneum) crusty (dried serum, blood, or pus on surface) eroded or ulcerated (partial vs. full thickness epidermal loss) color (skin colored, red, pigmented, pearly) feel (hard or soft, mobile or fixed) size: i.e. 6 x 4mm Look at the rest of the skin/region of skin look for similar growths for comparison ugly duckling sign chronic sun exposed areas vs. intermittent sun exposed areas does it occur within background sun damage?

 raised papule (<1cm) or")
5 Primary Lesion Describing a growth flat or raised? flat macule (<1cm) or patch (>1cm) raised papule (<1cm) or plaque (>1cm)

6 Primary Lesion

")
7 Secondary Descriptive Features Describing a growth scaly (hyperkeratosis) crusty (dried serum, blood, or pus on surface) eroded or ulcerated

 shape (irregular or")
8 Secondary Descriptive Features Describing a growth color (skin colored, red, pigmented, pearly, or multiple colors) shape (irregular or symmetric)


9 Secondary Descriptive Features Describing a growth feel (hard or soft, mobile or fixed)
10 A 45-yo male presents with a new mole on his back that his wife noticed 4-months ago Asymptomatic mainly; occasionally itches & it bleed once after picking at it He asks Doc, do I have skin cancer? Case One
11 What is the diagnosis? A. melanoma B. acquired melanocytic nevus C. seborrheic keratosis D. dysplastic nevus E. verruca vulgaris (wart)
12 What is the diagnosis? A. melanoma B. acquired melanocytic nevus C. seborrheic keratosis D. dysplastic nevus E. verruca vulgaris (wart)
13 Seborrheic Keratoses common benign epidermal neoplasm that begin usually in 30s & become ubiquitous in elders range from few hundreds sharply marginated, pigmented lesions & usually raised Waxy, "stuck-on," verrucous-appearing papules or plaques Individual lesions grow rapidly and reach a static size without further growth mostly asymptomatic can occur on any body site except the palms, soles, and mucous membranes



14 Seborrheic Keratoses Color is variable skin-colored, brown, black, pink pigmentation may be variable within a single lesion Texture is variable waxy, wart-like, or velvety

15 Seborrheic Keratoses begin developing usually in 30s & become ubiquitous in elders increase in number throughout life range from few hundreds contrast with melanocytic nevi, which typically appear in the first three decades of life a new nevus at the age 50 should raise concern for melanoma




16 How can I tell if a lesion is a seborrheic keratosis? SKs are superficial epidermal growths. stuck-on quality, like wax-pressed on the skin Flat SKs can have a "postage stamp" like appearance (flat wrinkled macule)

17 How can I tell if a lesion is a seborrheic keratosis? if not sure, gently pick/scratch the edges & surface of the lesion it feels as if you can pick it off the surface may crumble or flake showing a superficial waxy character



18 How can I tell if a lesion is a seborrheic keratosis? Always evaluate the lesion in the context of other growths on the skin look at both the tree & forest seborrheic keratosis seborrheic keratoses


19 How can I tell if a lesion is a seborrheic keratosis? Always evaluate the lesion in the context of other growths on the skin look at both the trees & forest The ugly duckling sign the lesion that appears different from the rest When in doubt, biopsy or refer to rule out melanoma ugly duckling sign invasive melanoma


20 Treatment of SKs Reassurance If irritated, inflamed, or symptomatic, can treat for medically necessary purposes Asymptomatic lesions can be treated for cosmetic purposes Treatment options curettage LN2/cryotherapy electrodessication shave removal
 is an SK variant in darker skin types of African")

21 Dermatosis Papulosa Nigra Dermatosis papulosa nigra (DPN) is an SK variant in darker skin types of African or Asian descent multiple papules that favors cheeks, temples, & neck onset typically during adolescence and F>M

22 Stucco keratoses papular warty white-gray SKs that commonly occur on the lower legs and feet of the elderly men. They are benign and usually asymptomatic. Stucco Keratoses
23 Case 2 45 yo male presents with a red mole which appeared several months ago & has grown. It is asymptomatic and no bleeding
24 What is the diagnosis? A. Basal Cell Carcinoma B. Cherry Angioma C. Congenital Hemangioma D. Petechiae E. Seborrheic Keratosis

25 What is the diagnosis? A. Basal Cell Carcinoma B. Cherry Angioma C. Congenital Hemangioma D. Petechiae E. Seborrheic Keratosis


26 Most common acquired benign vascular cutaneous neoplasms usually first appear during the third decade of life or later Most people over 60 years of age have one or more such lesions increase in number over time small cherry red papules or macules with trunk predilection Cherry Angiomas

 when in doubt, biopsy or")
27 Cherry angioma can mimic melanoma when they get traumatized or thrombose (dark purple or black color) when in doubt, biopsy or refer to r/o melanoma
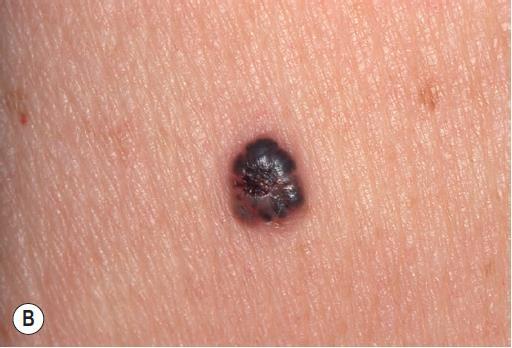
28 27-yo female presents with a new growth on the lower leg She sometimes nicks it while shaving it has gotten darker around the edges over the past few months when you examine the lesion, it feels firm like scar tissue and when you squeeze it it makes a slight dimple Case 3
29 What is the diagnosis? A. Melanoma B. Seborrheic Keratosis C. Basal Cell Carcinoma D. Acquired Melanocytic Nevus E. Dermatofibroma
30 What is the diagnosis? A. Melanoma B. Seborrheic Keratosis C. Basal Cell Carcinoma D. Acquired Melanocytic Nevus E. Dermatofibroma
31 What do you do next? A. Biopsy the lesion B. Refer to Dermatology C. Reassure the patient that it is benign D. Reassure the patient that it will go away

32 What do you do next? A. Biopsy the lesion B. Refer to Dermatology C. Reassure the patient that it is benign if the lesion changes, return to clinic for evaluation D. Reassure the patient that it will go away
")


33 Dermatofibroma second most common bengin fibrohistiocytic tumor of the skin (after skin tags) occur primarily in adults favor the lower extremities firm dome-shaped papules & nodules hyperpigmented in dark skin tan to pink in light skin nodule may be elevated or depressed peripherial rim of darkening pigment common


34 Clue to Diagnosis dimple sign pinching induces dimple due to the scar-like tethering of the dermis
35 Dermatofibroma can be multiple possible secondary to minor trauma shaving, bug bites, etc. scar ball of tissue should remain stable & asymptomatic Tx: reassurance refer for excisional biopsy if changing or symptomatic
36 A 52-year old female presents with several new facial bumps that have slowly been occurring over the last several years Case 4
37 How would you describe these A. pearly, waxy papules with telangiectasia B. yellowish & skin-colored papules with central dell C. stuck-on skincolored papules D. uniformly hyperpigmente d papules growths?
38 How would you describe these A. pearly, waxy papules with telangiectasia (basal cell carcinoma) B. yellowish & skincolored papules with central dell (sebaceous hyperplasia) C. stuck-on skincolored papules (seborrheic keratoses) D. uniformly hyperpigmented papules (melanocytic nevi) growths?
 Occurs in 40s tend to localize on the forehead, temples, and below the eyes Tx: reassurance that not secondary to skin hygiene & can treat for cosmetic purposes main")
39 Sebaceous Hyperplasia Bengin localized enlargement (hypertrophy) of the sebaceous glands (oil glands) yellowish papules with central dell yellow color (oil gland) central dell (gland enlargement around attached hair follicle) Occurs in 40s tend to localize on the forehead, temples, and below the eyes Tx: reassurance that not secondary to skin hygiene & can treat for cosmetic purposes main DDX: basal cell carcinoma


40 Sebaceous Hyperplasia vs. Basal Cell Carcinoma sebaceous hyperplasia yellowish papule with central dell & multiple similar lesions do not bleed or form hemorrhagic crust basal cell carcinoma pearly, waxy papules with telangiectasia bleed or scab with minimal trauma when in doubt, shave biopsy or dermatology referral should be performed to r/o BCC
41 55-yo women presents with brown spots on her dorsal hands & face She is fair skin & has had lots of sun exposure over the years Case 5
42 What is the diagnosis? A. actinic keratoses B. seborrheic keratoses C. solar lentigines D. acquired melanocytic nevi E. lentigo maligna melanoma
43 What is the diagnosis? A. actinic keratoses B. seborrheic keratoses C. solar lentigines D. acquired melanocytic nevi E. lentigo maligna melanoma
44 What is the diagnosis? A. actinic keratoses gritty sandpaper-like macules & papules with red base B. seborrheic keratoses stuck-on papules C. solar lentigines irregular, light brown to black macules on chronically sun-exposed skin D. acquired melanocytic nevi uniform pigmented macules & papules E. lentigo maligna melanoma irregular, variegated macule or patch on chronically sun-exposed skin

45 Solar lentigo (aka senile lentigo, age spot, or liver spot ) are benign pigmented macules appearing on fairskinned individuals chronically sun-exposed skin that is related to ultraviolet radiation No treatment is required but the presence of extensive solar lentigines is an indicator of excessive UV exposure and higher risk of skin cancer monitor for development of AKs, NMSCs, & melanoma emphasize sun protection Solar Lentigines
 MIS/melanoma secondary to chronic UV exposure that is insidious A")
 should be biopsied or refered to derm to r/o")
46 Solar Lentigines Must distinguish solar lentigo from lentigo maligna (MIS) and lentigo maligna melanoma (invasive melanoma) MIS/melanoma secondary to chronic UV exposure that is insidious A solar lentigo that looks different from a patient's other lentigines or that is changing (enlarging, darkening, variegated coloration) should be biopsied or refered to derm to r/o lentigo maligna
47 A 70-yo retired male farmer presents for a non-healing pimple like growth on his ear. It will intermittently bleed when washing. He first noticed it ~3-4 months ago and felt like it got better. What is the next best step? Case 6
48 What is the next best step? A. Follow-up in 3- months to see if resolves B. Liquid Nitrogen/Cryothera py C. Surgical Removal D. Topical Antibiotics E. Shave Biopsy
49 What is the next best step? A. Follow-up in 3- months to see if resolves B. Liquid Nitrogen/Cryothera py C. Surgical Removal D. Topical Antibiotics E. Shave Biopsy


50 Shave Biopsies & Pathology Shave Biopsies quick, safe, & minimally invasive biopsy method for lesions concerning for NMSC only superficial portion of lesion removed can use razor blade or #15 blade scalpel
 a horizontal incision is made and the lesion or portion of lesion removed with sweeping strokes 5.")
51 Shave Biopsy Technique 1. note location, triangulate, &/or digital photograph 2. prep skin with alcohol 3. anesthesia 1% lidocaine with epi (dermal injection & generally <1cc) 4. use either 15-blade scalpel or a razor blade (can be flexed to achieve the desired depth) a horizontal incision is made and the lesion or portion of lesion removed with sweeping strokes 5. hemostasis is attained with 35% aluminum chloride solution & pressure 6. open wound care: petroleum ointment & small bandage no activity restrictions


52 Shave Biopsies & Pathology Shave Biopsies designed for diagnostic purposes and not for therapeutic purposes pathology reports sometimes comment on margins clear margins for a shave biopsy are inadequate help determine if cancer or not and the need for surgical treatment
53 What is the most likely diagnosis? A. Basal Cell Carcinoma B. Squamous Cell Carcinoma C. Intradermal Melanocytic Nevus D. Actinic Keratosis E. Sebaceous Hyperplasia
54 What is the most likely diagnosis? A. Basal Cell Carcinoma B. Squamous Cell Carcinoma C. Intradermal Melanocytic Nevus D. Actinic Keratosis E. Sebaceous Hyperplasia


, male, & immune")
55 Basal Cell Carcinomas most common skin cancer arise from the basal layer of the epidermis 2 cumulative intermittent recreational UV exposure Sonic Hedgehog-Patched Signaling Pathway mutations from signature UV-induced mutations slow growing cancers that are locally destructive and almost never metastasize Risk Factors: fair skin, severe sun damage, elderly (>60 yo), male, & immune suppression Nodular BCC




56 Clinical Spectrum of BCCs: Nodular BCC Superficial BCC Rodent/Ulcerative BCC Morpheaform/Sclerosing BCC Pigmented BCC
57 What is the preferred treatment? A. Liquid Nitrogen/Cryosurger y B. Topical Imiquimod C. Excision with Traditional Surgical Margins D. Excision with Mohs Micrographic Surgery E. Radiation Therapy

58 What is the preferred treatment? A. Liquid Nitrogen/Cryosurger y B. Topical Imiquimod C. Excision with Traditional Surgical Margins D. Excision with Mohs Micrographic Surgery E. Radiation Therapy
59 Treatment of BCCs: There are several surgical Excision with Mohs Micrographic Surgery Excision with 4mm margins Electrodessication & Curettage Non-surgical options Radiation therapy Topical imiquimod (FDA approved for non-facial, hands, & feet superficial BCC) Cryosurgery & more Surgical options are preferred method of treatment/standard of care The best option is selected after consideration of the clinical & pathologic features in context of the patient To select optimal therapy, refer or ask local dermatologist/mohs surgeon

60 Mohs Micrographic Surgery (MMS) MMS offers the highest cure rate for the treatment of both primary & recurrent SCCs, BCCs, MIS, and other cutaneous malignancies when compared to conventional excision and other treatment modalities. evaluate the entire margin (Remove tumor completely) Eliminate tumor/ reduce recurrence spare tissue (Be minimally destructive) peripherally and/or deep smaller wounds less complex reconstruction less scarring




61 Mohs surgery excision, mapping, and histology Microscopically guided, 100 % margin-controlled excision of cancer Physician excising cancer also interprets slides the same day Mohs surgery
 & Recurrent Facial BCC treated via MMS vs.")
62 MMS Excision vs. Conventional Excision 10-year Recurrence Rate for Facial BCC treated via MMS vs. Excision MMS Excision Standard Excision Primary BCC Recurrent BCC 4.4% 12.2% 3.9% 13.5% Netherland RCT of Primary Facial High Risk BCC (diameter at least 1cm, H-zone location or aggressive histological subtype) & Recurrent Facial BCC treated via MMS vs. Standard Excision Source: Eur J Cancer Nov;50(17):

63 MMS Excision vs. Conventional Excision
64 MMS is cost effective

65 MMS is cost effective

66 Indications for MMS Location Head & neck, hands & feet, genitalia Aggressive Histology infiltrative, micronodular, keratinizing BCCs poorly differentiated & acantholytic SCC perineural tumors Poorly/ill-defined tumors Rapidly growing tumors Recurrent tumors Large tumors If you are treating NMSCs NCCN guidelines & Mohs Appropriate Use criteria are excellent resources otherwise refer to dermatology for treatment


67 Mohs Surgery for BCCs


68 Post Mohs Surgery for BCCs Nodular BCC requiring 1 stage Aggressive Infiltrative BCC requiring multiple stages


69 Same Day Reconstruction by Mohs Surgeon 2 Stage Paramedian Forehead Flap Curvilinear Primary Closure


70 Follow-up
71 A 70-yo farmer presents with several scaly areas & growths on his face. He also notes a red bump on his left forehead that is bigger & has been slowing growing. It is occasionally tender & will bleed. What is the most likely diagnosis? Case 7
72 What is the diagnosis? A. actinic keratoses B. seborrheic keratoses C. solar lentigines D. basal cell carcinoma E. squamous cell carcinoma & actinic keratoses

73 What is the diagnosis? A. actinic keratoses gritty sandpaper-like macules & papules with red base B. seborrheic keratoses stuck-on papules C. solar lentigines irregular, light brown to black macules on chronically sunexposed skin D. basal cell carcinoma pearly plaque with telangectasias E. squamous cell carcinoma & actinic keratoses keratotic plaque (SCC) & background of AKs
74 Actinic Keratoses AKs are premalignant keratinocyte growths that can transform into cutaneous squamous cell carcinomas transformation rate low: ~ <0.1%/year/single AK rates of spontaneous regression single lesions ranged between 15-63% per year with recurrence rates of 15 53% p53 mutations 2 signature UV mutations present in early precursors & >90% invasive SCCs Photodamage AK SCC In Situ Invasive SCC Metastatic Potential


75 Actinic Keratoses erythematous gritty sandpaper-like macules & papules occurring on chronically sun-damaged fair skin can feel them better than see them often occur in multitude favor dorsal hands, forearms, temples, nose, cheeks generally asymptomatic & rough feeling discrete or ill-defined in nature


76 Actinic Keratoses Treatments lesion-directed therapy LN2/cryotherapy curettage topical fielddirected therapy 5-fluoruracil imiquimod diclofenac ingenol mebutate photodynamic therapy



77 Actinic Keratoses Treatments lesion-directed therapy LN2/cryotherapy curettage topical field-directed therapy 5-fluoruracil imiquimod diclofenac ingenol mebutate photodynamic therapy combination therapy


78 Squamous Cell Carcinoma ~4 million NMSCs (BCC & SCC) per year in the US Shifting ratio of relative occurrence of BCC to SCC 4 to to 1 of BCC to SCC 700,000 SCC new cases annually & increasing incidence at lower latitudes 2 Cummulative UV Radiation Exposure p53 mutations 2 signature UV mutations present >90% invasive SCCs % will metastasize to nodes and % will die as a result of metastatic SCC A recent study, estimated the U.S death secondary to invasive SCC 3,932-8,791 patients out of 186, ,543 new cases that year Death rates esp. in central & southern U.S. nearly rivaled that of melanoma. SEER 2017 melanoma death estimates 9,730 out of 87,110 new cases






79 Squamous Cell Carcinoma: Clinical majority appear on chronically sun-damaged skin of the head, neck, forearms, and dorsal hands. slow growing > rapidly growing asymptomatic > painful or itch variable morphology most often presents as an erythematous hyperkeratotic papule, plaque, or nodule cutaneous horns exophytic nodules indurated fixed nodules chronic ulcers Presentation



80 Risk Factors for High-Risk Cutaneous Squamous Cell Carcinoma
81 Diagnosis & Treatment of SCC: Shave Biopsy or Refer to Dermatology if suspect SCC Treatment similar to BCCs Surgical options: Excision with Mohs Micrographic Surgery Excision with appropriate margins (for low-risk SCC) Electrodessication & Curettage (for SCC, in situ) Non-surgical options Radiation therapy (poor surgical candidates) Off-Label Topical Therapies (i.e. 5-FU, imiquimod, PDT usually SCC, in situ) Surgical options are preferred method of treatment/standard of care The best option is selected after consideration of the clinical & pathologic features in context of the patient To select optimal therapy, refer or ask local dermatologist/mohs surgeon

82 A 55-yo white male presents to your clinic and said he is there because his wife wanted you to check out his moles on his back. He grew up in South Florida and spent his youth surfing and fishing. He had several blistering sunburns. He doesn t know his FH of skin cancer other than he has a moley father. Case 8
83 Examination: note tan & mild sunburn solar lentigines several melanocytic nevi close inspection of a group of nevi who notice the following Case 8
84 what is the next best step? A. routine skin examination & improve sun protection B. excisional biopsy of A C. excisional biopsy of C D. shave biopsy of C E. reassurance
85 what is the next best step? A. routine skin examination & improve sun protection B. excisional biopsy of A C. excisional biopsy of C D. shave biopsy of C E. reassurance
 and look for outliers (i.e. ugly duckling ) If ugly duckling found, either excisional biopsy or referral to dermatology to r/o melanoma should be performed")
86 Evaluating Melanocytic Lesions when evaluating nevi, it is important to look for symmetry, regular border, uniform color/shape, relative diameter <6mm, & evolution/change (ABCDEs) more practical approach is to look for similar melanocytic nevi on an given individual (i.e. signature nevi ) and look for outliers (i.e. ugly duckling ) If ugly duckling found, either excisional biopsy or referral to dermatology to r/o melanoma should be performed
 pigmented papule lighter pigmented papules (adults) >100 melanocytic nevi risk factor for melanoma rare to develop new ones after age 50")
87 Evaluating Melanocytic Lesions acquired melanocytic nevi are common in childhood & early adulthood related to sun exposure nevi change overtime esp. in adolescent pigmented macule (children) pigmented papule lighter pigmented papules (adults) >100 melanocytic nevi risk factor for melanoma rare to develop new ones after age 50 biopsy or refer to r/o melanoma

88 Evaluating Melanocytic Lesions signature nevi examples include solid brown, solid pink, eclipse, fried-egg, & more.

89 Evaluating Melanocytic Lesions signature nevi examples include solid brown, solid pink, eclipse, fried-egg, & more.


90 Evaluating Melanocytic Lesions signature nevi examples include solid brown, solid pink, eclipse, fried-egg, & more.

91 Evaluating Melanocytic Lesions ugly duckling sign different from signature nevi helpful for identifying potential melanoma or unusual dysplastic nevus
/dysplastic nevi (pathologic) are not precancerous moles however, individuals with >5 dysplastic nevi are at increased risk for melanoma and should be followed by a")
92 Back to the Case: Excisional Biopsy Results Come Back Pathology report for the biopsy reads dysplastic melanocytic nevus, moderate atypia; clear margins.what next? atypical nevi (clinical)/dysplastic nevi (pathologic) are not precancerous moles however, individuals with >5 dysplastic nevi are at increased risk for melanoma and should be followed by a dermatologist atypical nevi can be very difficult to distinguish clinically from melanoma Atypical Melanocytic Nevi Features (3/5) >5 mm in size variable pigmentation irregular and asymmetric shape indistinct borders erythema



93 You find a lesion that you are concerned is a melanoma & plan to biopsy it melanocytic lesions that look atypical to you, can also look atypical for the pathologist thus, it is important for the pathologist to see the entire melanocytic lesion under the microscope to give the most accurate diagnosis second, the most important prognostic information for guiding the treatment of melanoma is the Breslow thickness thus, it is important to take a deep enough biopsy so as not to transect the base of the possible melanoma the best way of ensuring your biopsy technique will accomplish removal of the entire clinical mole & the appropriate depth is to perform an excisional biopsy

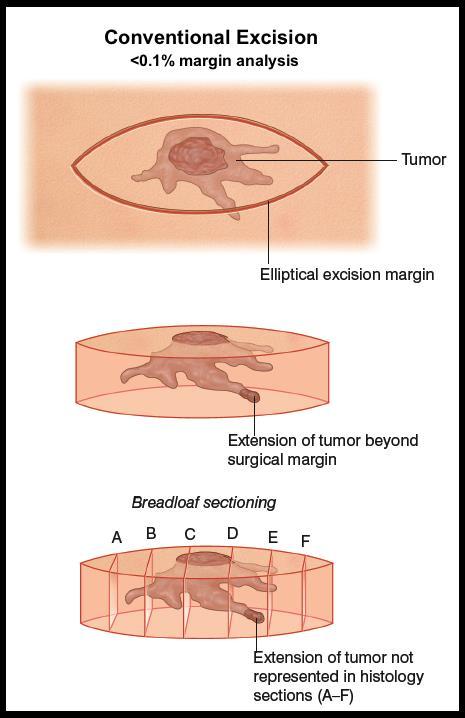
94 excisional biopsy involves full thickness incision to the fat with the entire lesion captured within & can accomplish 2 ways conventional elliptical excision punch excision Excisional Biopsy

95 excisional biopsy involves full thickness incision to the fat with the entire lesion captured within & can accomplish 2 ways conventional elliptical excision punch excision Excisional Biopsy



96 common method performed by dermatologists in when biopysing atypical melanocytic nevi to rule-out melanoma basically a deep shave biopsy with 1-2 margins of normal skin extends to deep (reticular) dermis with to avoid transection of the base of possible melanoma faster, less invasive, & superior cosmesis in certain anatomic regions comparable to excisional biopsy and does not affect survival rate in melanoma treatment Saucerization Biopsy
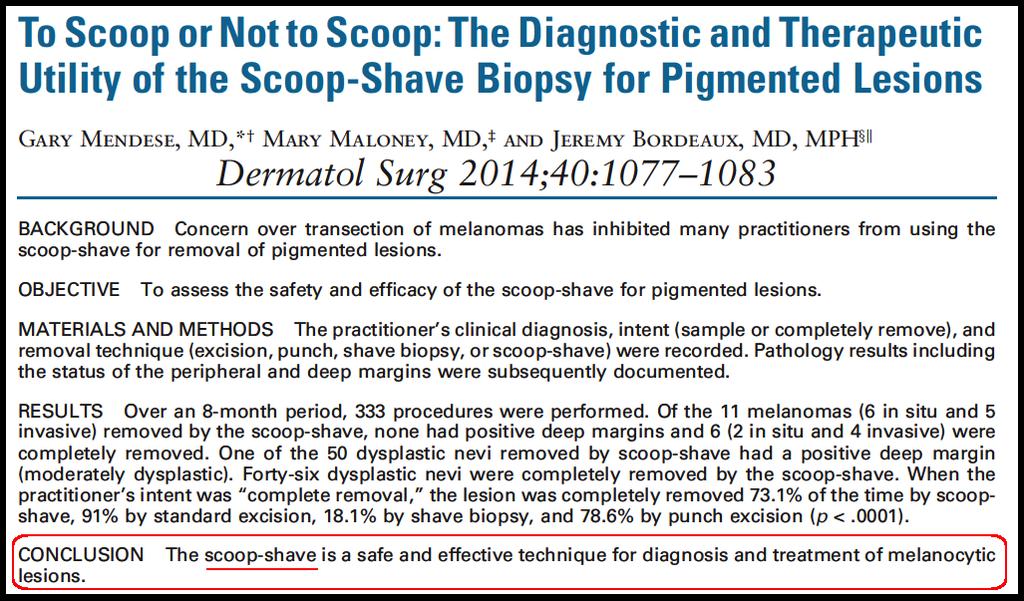
97 Saucerization Biopsy


98 Thank You for Attention Useful Patient & Clinician Resources: American Academy of Dermatology American College of Mohs Surgery Skin Cancer Foundation National Comprehensive Cancer Network Guidelines VisualDx.com
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee
 I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
I have a skin lump doc! What s next? 12 th August 2017 Dr. Sue-Ann Ho Ju Ee Some thoughts Is this skin cancer? How common is this? How likely is this in this patient? What happens next if it s something
Living Beyond Cancer Skin Cancer Detection and Prevention
 Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
Living Beyond Cancer Skin Cancer Detection and Prevention Cutaneous Skin Cancers Identification Diagnosis Treatment options Prevention What is the most common cancer in people? What is the most common
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Identifying Benign and Malignant Skin Lesions. No Disclosures. Common Benign Lesions. Benign Lesions 2/25/2018. Stucco Keratoses.
 Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Skin lesions The Good and the Bad. Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry
 Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Skin lesions The Good and the Bad Dr Virginia Hubbard Ipswich Hospital NHS Trust Barts and the London School of Medicine and Dentistry Case 1 32 year old woman Australian Lesion on back New hair growing
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Skin Cancer 101: Diagnosis and Management of the Most Common Cancer
 Skin Cancer 101: Diagnosis and Management of the Most Common Cancer Sarah Patton, PA-C, MSHS Skin Surgery Center www.skinsurgerycenter.com Seattle/Bellevue, WA Skin cancer Skin cancer is by far the most
Skin Cancer 101: Diagnosis and Management of the Most Common Cancer Sarah Patton, PA-C, MSHS Skin Surgery Center www.skinsurgerycenter.com Seattle/Bellevue, WA Skin cancer Skin cancer is by far the most
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest risk.
 Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Basics of Skin Cancer Detection and Treatment of Non- Melanoma Skin Cancers Large majority caused by sun exposure Often sun exposure before age 20 Persons who burn easily and tan poorly are at greatest
Dermatological Manifestations in the Elderly. Sanjay Siddha Staff Dermatologist UHN & MSH
 Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
Dermatological Manifestations in the Elderly Sanjay Siddha Staff Dermatologist UHN & MSH Disclosure No actual or potential conflicts of interest or commercial relationships to declare Objectives Recognize
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
General information about skin cancer
 Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Skin Malignancies. Presented by Dr. Douglas Paauw
 Skin Malignancies Presented by Dr. Douglas Paauw Disclosure: Dr. Paauw has no significant financial interest in any of the products or manufacturers mentioned. How Common Is Skin Cancer? *½ of all White
Skin Malignancies Presented by Dr. Douglas Paauw Disclosure: Dr. Paauw has no significant financial interest in any of the products or manufacturers mentioned. How Common Is Skin Cancer? *½ of all White
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Lumps and Bumps: An Organized Approach to Diagnosis and Management. Disclosure. Introduction. References. Structure of Skin.
 Lumps and Bumps: An Organized Approach to Diagnosis and Management Nothing to disclose Disclosure Tammy Pifer Than, MS, OD, FAAO Carl Vinson VAMC tammythan@bellsouth.net References Fitzpatrick's Color
Lumps and Bumps: An Organized Approach to Diagnosis and Management Nothing to disclose Disclosure Tammy Pifer Than, MS, OD, FAAO Carl Vinson VAMC tammythan@bellsouth.net References Fitzpatrick's Color
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
 Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
Lid Lesions: Relax or Refer
 Lid Lesions: Relax or Refer Blair Lonsberry, MS, OD, MEd., FAAO Professor of Optometry Pacific University College of Optometry blonsberry@pacificu.edu Agenda Benign vs. Malignant lesions Benign Eyelid
Lid Lesions: Relax or Refer Blair Lonsberry, MS, OD, MEd., FAAO Professor of Optometry Pacific University College of Optometry blonsberry@pacificu.edu Agenda Benign vs. Malignant lesions Benign Eyelid
Actinic keratosis (AK): Dr Sarma s simple guide
: Dr Sarma s simple guide") Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
VACAVILLE DERMATOLOGY
 Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Skin Cancer - Non-Melanoma
 Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
30 Actinic Keratosis (Solar Keratosis)
") 30 Actinic Keratosis (Solar Keratosis) CLINICAL APPLICATION QUESTIONS A 65-year-old white man is seen at your office for multiple scaling lesions over his face, ears, neck, and the V of the chest. These
30 Actinic Keratosis (Solar Keratosis) CLINICAL APPLICATION QUESTIONS A 65-year-old white man is seen at your office for multiple scaling lesions over his face, ears, neck, and the V of the chest. These
Nonmelanoma skin cancers
 Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Skin cancer Philip Clarke Nonmelanoma skin cancers Treatment options Background Australia has one of the highest skin cancer rates in the world. Early detection and treatment of skin cancer is vital to
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
Diagnosis and Management of Actinic Keratosis (AKs)
") Diagnosis and Management of Actinic Keratosis (AKs) Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada
Diagnosis and Management of Actinic Keratosis (AKs) Andrei Metelitsa, MD, FRCPC, FAAD Co-Director, Institute for Skin Advancement Clinical Associate Professor, Dermatology University of Calgary, Canada
Skin Cancers Emerging Trends and Treatment Approaches
 Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Skin Cancers Emerging Trends and Treatment Approaches Andrei Metelitsa, MD, FRCPC, FAAD Clinical Associate Professor, Dermatology, U of C Co-Director, Institute for Skin Advancement Copyright 2017 by Sea
Exenteration. Introduction. The skin. Epidermal malignancies 8/3/2017. Neglected basal cell carcinoma
 Jeremiah Tao, MD, FACS Director, Oculoplastic and Orbital Surgery Associate Professor, UC Irvine Neglected basal cell carcinoma Exenteration Introduction Chief question with any eyelid lesion: Suspicious
Jeremiah Tao, MD, FACS Director, Oculoplastic and Orbital Surgery Associate Professor, UC Irvine Neglected basal cell carcinoma Exenteration Introduction Chief question with any eyelid lesion: Suspicious
Doctors of Optometry Course Notes
 Doctors of Optometry Course Notes OD19 1CE COPE: 43871-AS Eyelid Lumps and Bumps Sunday, February 26, 2017 2:40 pm 3:30 pm Regency C 3 rd Floor Presenter: Blair Lonsberry, OD, FAAO Dr. Lonsberry is a Full
Doctors of Optometry Course Notes OD19 1CE COPE: 43871-AS Eyelid Lumps and Bumps Sunday, February 26, 2017 2:40 pm 3:30 pm Regency C 3 rd Floor Presenter: Blair Lonsberry, OD, FAAO Dr. Lonsberry is a Full
Non-melanoma Skin Cancer
 Non-melanoma Skin Cancer Understanding your diagnosis 1 888 939-3333 cancer.ca Non-melanoma Skin Cancer Understanding your diagnosis When you first hear that you have cancer, you may feel alone and afraid.
Non-melanoma Skin Cancer Understanding your diagnosis 1 888 939-3333 cancer.ca Non-melanoma Skin Cancer Understanding your diagnosis When you first hear that you have cancer, you may feel alone and afraid.
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Dual Wavelength Phototherapy System
 Dual Wavelength Phototherapy System The AKLARUS Blue and Red Combination System is an effective, drugfree alternative for treating acne & photodamaged skin. The non-invasive Aklarus treatment has been
Dual Wavelength Phototherapy System The AKLARUS Blue and Red Combination System is an effective, drugfree alternative for treating acne & photodamaged skin. The non-invasive Aklarus treatment has been
Lagophthalmos. Lagophthalmos: signs. Lagophthalmos: clinical tips. Lagophthalmos: treatment plan. Madarosis
 Lagophthalmos Def: incomplete closure of the eyelid SX: FBS, irritation, red, burn, dry, chronic morning corneal irritation Lagophthalmos: signs 2-5 mm lid separation with slit lamp during blink can force
Lagophthalmos Def: incomplete closure of the eyelid SX: FBS, irritation, red, burn, dry, chronic morning corneal irritation Lagophthalmos: signs 2-5 mm lid separation with slit lamp during blink can force
BL-5010P A NOVEL PRE-FILLED APPLICATOR FOR THE NON-SURGICAL REMOVAL OF SKIN LESIONS
 BL-5010P A NOVEL PRE-FILLED APPLICATOR FOR THE NON-SURGICAL REMOVAL OF SKIN LESIONS 25 Skin lesions Miri Seiberg, PhD 26 Skin lesions A part of the skin that has an abnormal growth or appearance compared
BL-5010P A NOVEL PRE-FILLED APPLICATOR FOR THE NON-SURGICAL REMOVAL OF SKIN LESIONS 25 Skin lesions Miri Seiberg, PhD 26 Skin lesions A part of the skin that has an abnormal growth or appearance compared
Malignant Cutaneous Neoplasms
 Malignant Cutaneous Neoplasms Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP All slides Kathleen Haycraft Objectives: 1. Identify common cutaneous malignant neoplasms. 2. Identify the etiology, pathophysiology
Malignant Cutaneous Neoplasms Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP All slides Kathleen Haycraft Objectives: 1. Identify common cutaneous malignant neoplasms. 2. Identify the etiology, pathophysiology
Gross Appearance & Histology of Skin Cancer. Kyle Mannion M.D. January 21, 2005
 Gross Appearance & Histology of Skin Cancer Kyle Mannion M.D. January 21, 2005 Actinic Keratosis 5-20% will develop squamous/basal cell ca Almost solely from solar damage Usually develop during 4 th decade
Gross Appearance & Histology of Skin Cancer Kyle Mannion M.D. January 21, 2005 Actinic Keratosis 5-20% will develop squamous/basal cell ca Almost solely from solar damage Usually develop during 4 th decade
Talking to Your Clients About Skin Cancer. Objectives 9/9/2017. Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017
 Talking to Your Clients About Skin Cancer Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017 Objectives Provide general information about skin cancer and how skin cancers commonly
Talking to Your Clients About Skin Cancer Amanda Friedrichs, MD, FAAD AMTA National Conference September 14, 2017 Objectives Provide general information about skin cancer and how skin cancers commonly
Richard Turner Consultant Dermatologist
 Old Problems & New Treatments Photo Album by Administrator Richard Turner Consultant Dermatologist Plan for tonight? Refresher on SCC and solar keratosis How to distinguish the two Classic therapy than
Old Problems & New Treatments Photo Album by Administrator Richard Turner Consultant Dermatologist Plan for tonight? Refresher on SCC and solar keratosis How to distinguish the two Classic therapy than
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Thursday 21 st August Skin Problems
 Thursday 21 st August 2014 Skin Problems Skin Problems The Sun and the Skin Sun Damage Recognising the early signs of skin cancer The Big 3 inflammatory condi=ons Acne & Rosacea Eczema (Including Seborrhoeic
Thursday 21 st August 2014 Skin Problems Skin Problems The Sun and the Skin Sun Damage Recognising the early signs of skin cancer The Big 3 inflammatory condi=ons Acne & Rosacea Eczema (Including Seborrhoeic
Disclosures. I have no conflicts of interest to disclose
 Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco 2
Disclosures I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco 2
Skin Cancer. Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts Dr Elizabeth Ogden
 Skin Cancer Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts 13.10.16 Skin Cancer Melanoma mole cancer - is a true cancer which can metastasize and kill Non Melanoma skin cancer
Skin Cancer Dr Elizabeth Ogden Associate Specialist in Dermatology East and North Herts 13.10.16 Skin Cancer Melanoma mole cancer - is a true cancer which can metastasize and kill Non Melanoma skin cancer
See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C
 See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C Learning objectives Discuss malignant and benign skin lesions commonly seen in primary care. Identify
See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C Learning objectives Discuss malignant and benign skin lesions commonly seen in primary care. Identify
Malignant Cutaneous Neoplasms. Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP, FAANP
 Malignant Cutaneous Neoplasms Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP, FAANP Objectives: 1. Identify common cutaneous malignant neoplasms. 2. Identify the etiology, pathophysiology and treatment of common
Malignant Cutaneous Neoplasms Kathleen Haycraft, DNP, FNP/PNP-BC, DCNP, FAANP Objectives: 1. Identify common cutaneous malignant neoplasms. 2. Identify the etiology, pathophysiology and treatment of common
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW
 MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C
 See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C Learning objectives Discuss malignant skin lesions commonly seen in primary care. Identify common treatments
See spot change: Lesion identification and management in primary care ERIN HENNESSEY DNP, APRN, FNP-C Learning objectives Discuss malignant skin lesions commonly seen in primary care. Identify common treatments
Periocular skin cancer
 Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Periocular skin cancer Information for patients Skin cancer involving the skin of the eyelid or around the eye is called a periocular skin cancer. Eyelid skin cancers occur most often on the lower eyelid,
Oliver J. Wisco, DO, FAAD Melanoma Specialist & Mohs Surgeon Bend Memorial Clinic
 A Primary Care Approach to Skin Cancer Oliver J. Wisco, DO, FAAD Melanoma Specialist & Mohs Surgeon Bend Memorial Clinic 1 Disclosures Speaker for MiMedx Consultant for MiMedx NO PERTINENT CONFLICTS OF
A Primary Care Approach to Skin Cancer Oliver J. Wisco, DO, FAAD Melanoma Specialist & Mohs Surgeon Bend Memorial Clinic 1 Disclosures Speaker for MiMedx Consultant for MiMedx NO PERTINENT CONFLICTS OF
Alcohol should be avoided for 3 days prior to surgery and 2 days after the procedure.
 Mohs Surgery Information Packet Be sure to bring the following to your appointment: Insurance Card Insurance Referral ( If required by your insurance) Name and address of your primary care provider as
Mohs Surgery Information Packet Be sure to bring the following to your appointment: Insurance Card Insurance Referral ( If required by your insurance) Name and address of your primary care provider as
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Common skin tumors. Benign Epidermal Tumors. Topic. Clinicopathologic Variants. Seborrheic keratoses
 Common skin tumors Topic Benign epidermal tumors Skin cyst and adnexal neoplasms Other common skin tumor Common skin malignancy สมศ กด ต นร ตนากร 26/02/2015 Benign Epidermal Tumors Seborrheic keratosis
Common skin tumors Topic Benign epidermal tumors Skin cyst and adnexal neoplasms Other common skin tumor Common skin malignancy สมศ กด ต นร ตนากร 26/02/2015 Benign Epidermal Tumors Seborrheic keratosis
Dermatology Procedure Coding
 Dermatology Procedure Coding Anatomy Two layers that make up human skin Epidermis most superficial layer Composed of four to five layers called stratum Anyone remember the mnemonic? Thickness varies based
Dermatology Procedure Coding Anatomy Two layers that make up human skin Epidermis most superficial layer Composed of four to five layers called stratum Anyone remember the mnemonic? Thickness varies based
Oral and Maxillofacial Surgery Department
 Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Disclosures. Melanoma and Non melanoma Skin Cancer: What You Need to Know. I have no conflicts of interest to disclose
 Disclosures Melanoma and Non melanoma Skin Cancer: What You Need to Know I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department
Disclosures Melanoma and Non melanoma Skin Cancer: What You Need to Know I have no conflicts of interest to disclose Lindy P. Fox, MD Associate Professor Director, Hospital Consultation Service Department
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Clinical Policy: Benign Skin Lesion Removal Reference Number: CP.MP.HN150
 Clinical Policy: Reference Number: CP.MP.HN150 Effective Date: 6/04 Last Review Date: 8/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Clinical Policy: Reference Number: CP.MP.HN150 Effective Date: 6/04 Last Review Date: 8/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important regulatory and
Chapter 8 Skin Disorders and Diseases
 Chapter 8 Skin Disorders and Diseases Attitude is more important than the past, than education, than money, than circumstances, than what people do or say. It is more important than appearance, giftedness,
Chapter 8 Skin Disorders and Diseases Attitude is more important than the past, than education, than money, than circumstances, than what people do or say. It is more important than appearance, giftedness,
LENTIGO SIMPLEX. Epidemiology
 LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES)
") NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
NEOPLASMS OF THE SURFACE EPITHELIUM (KERATINOCYTES) Papillary Lesions Precancerous Lesions Keratinocyte Proliferations Carcinomas Melanotic Lesions Melanomas Normal Mucosa Keratin layer Spinous layer Basal
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Moh's Surgery Information Packet
 Moh's Surgery Information Packet BE SURE TO BRING THE FOLLOWING TO YOUR APPOINTMENT Insurance card Insurance referral (if required by your insurance) Name and address of your primary care provider as well
Moh's Surgery Information Packet BE SURE TO BRING THE FOLLOWING TO YOUR APPOINTMENT Insurance card Insurance referral (if required by your insurance) Name and address of your primary care provider as well
Actinic Keratoses and Bowen s disease
 Actinic Keratoses and Bowen s disease Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Actinic Keratoses and Bowen s disease Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Objectives. 1. Recognizing benign skin lesions. 2.Know which patients will likely need surgical intervention.
 The Joy of Pediatric Skin Dr. Claire Sanger University of Kentucky Plastic & Reconstructive Surgery Objectives 1. Recognizing benign skin lesions 2.Know which patients will likely need surgical intervention.
The Joy of Pediatric Skin Dr. Claire Sanger University of Kentucky Plastic & Reconstructive Surgery Objectives 1. Recognizing benign skin lesions 2.Know which patients will likely need surgical intervention.
 Epidermis Dermis Subcutaneous Hypodermis March 16, 2013 Telangiectasia's (spider veins) may develop anywhere within the body but can be easily seen in the skin, mucous membranes, and whites of
Epidermis Dermis Subcutaneous Hypodermis March 16, 2013 Telangiectasia's (spider veins) may develop anywhere within the body but can be easily seen in the skin, mucous membranes, and whites of
Mole mapping and monitoring. Dr Stephen Hayes. Associate Specialist in Dermatology, University Hospital Southampton
 Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Regeneron and Sanofi are financial supporters of The Skin Cancer Foundation and collaborated in the development of this article. US-ONC /2018
 A D E E P E R L O O K When detected early, most cases of local cutaneous squamous cell carcinoma are easily treated and usually cured. But when they become more advanced, this second most common form of
A D E E P E R L O O K When detected early, most cases of local cutaneous squamous cell carcinoma are easily treated and usually cured. But when they become more advanced, this second most common form of
Skin Cancer Awareness
 Skin Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary More than 3.5 million new cases of skin cancer will be diagnosed in
Skin Cancer Awareness Presented by BHS Call: 800-327-2251 Visit: www.bhsonline.com 2016 BHS. All rights reserved. 1 Training Summary More than 3.5 million new cases of skin cancer will be diagnosed in
Skin Cancer of the Nose: Common and Uncommon
 Skin Cancer of the Nose: Common and Uncommon Mark Russell, M.D. Associate Professor of Dermatology, Otolaryngology, and Pathology University of Virginia Objectives Review clinical presentations of select
Skin Cancer of the Nose: Common and Uncommon Mark Russell, M.D. Associate Professor of Dermatology, Otolaryngology, and Pathology University of Virginia Objectives Review clinical presentations of select
Pathology. Skin Tumor. Bayan N. Mohammad 15/10/2015. Mohammad al-orjani. Page 0 of 23
 #7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
#7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
Integumentary System
 Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Disclosure. Objectives. PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016
 PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016 1 Disclosure The speaker has no conflict of interest, financial agreement, or working affiliation with any group or organization.
PAFP CME Conference Lou Mancano MD, FAAFP Reading Health System November 18, 2016 1 Disclosure The speaker has no conflict of interest, financial agreement, or working affiliation with any group or organization.
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Cutaneous Adnexal Tumors
 Cutaneous Adnexal Tumors Lesions with Predominant Follicular Differentiation Special Emphasis on Basal Cell Carcinoma 2014-04-01 Prof. Dr. med. Katharina Glatz Pathologie Cutaneous Adnexal Tumors Hair
Cutaneous Adnexal Tumors Lesions with Predominant Follicular Differentiation Special Emphasis on Basal Cell Carcinoma 2014-04-01 Prof. Dr. med. Katharina Glatz Pathologie Cutaneous Adnexal Tumors Hair
SKIN HISTOLOGY AND FUNCTION
 SKIN HISTOLOGY AND FUNCTION THREE LAYERS : EPIDERMIS BASEMENT MEMBRANE DERMIS EPIDERMIS : COMPOSED OF KERATINOCYTES NO MATRIX DEEP BASAL LAYER MITOTICALLY ACTIVE SPINOUS LAYER MATURE HYALIN HORNY LAYER
SKIN HISTOLOGY AND FUNCTION THREE LAYERS : EPIDERMIS BASEMENT MEMBRANE DERMIS EPIDERMIS : COMPOSED OF KERATINOCYTES NO MATRIX DEEP BASAL LAYER MITOTICALLY ACTIVE SPINOUS LAYER MATURE HYALIN HORNY LAYER
Skin Cancer A Personal Approach. Dr Matthew Strack Dunedin New Zealand
 Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Review of Cutaneous Malignancies
 Review of Cutaneous Malignancies Tanya Nino, MD Department of Dermatology Did You Know? More than 3.5 million skin cancers are diagnosed in the US annually Melanoma incidence rates have been increasing
Review of Cutaneous Malignancies Tanya Nino, MD Department of Dermatology Did You Know? More than 3.5 million skin cancers are diagnosed in the US annually Melanoma incidence rates have been increasing