Jasmine Zain, M.D. Erin Kopp, M.S.N, A.C.N.P B.C., N.P. Christiane Querfeld, M.D., Ph.D Director, Cutaneous Lymphoma Program
|
|
|
- James Blankenship
- 6 years ago
- Views:
Transcription
1 MANAGEMENT OF CUTANEOUS LYMPHOMAS AND CHRONIC GVHD Jasmine Zain, M.D. Erin Kopp, M.S.N, A.C.N.P B.C., N.P. Christiane Querfeld, M.D., Ph.D Director, Cutaneous Lymphoma Program How the Experts Treat Hematologic Malignancies Las Vegas, NV Click March to 17, edit 2017 Master Presentation Date
2 GVHD Jasmine Zain, M.D. Director, T Cell Lymphoma Program Associate Clinical Professor, Dept. of Hematology & Hematopoietic Cell Transplantation Click to edit Master Presentation Date
3 Disclosures Speakers bureau Spectrum Seattle Genetics Celgene Advisory boards Celgene Spectrum
4 OBJECTIVES Classification of GVHD Pathophysiology of GVHD Risk ikfactors for GVHD Clinical features of ch GVHD Treatment outline for GVHD
5 WHAT IS A HEMATOPOEITIC STEM CELL? o Ability to provide life long hematopoiesis of all blood- cell lineages after transplantation into lethally irradiated recipients
6 THERAPEUTIC PRINCIPLES BY ALLOGENEIC SCT Ablation of host hematopoiesis, normal and malignant or immunosuppression of host immunity to allow engraftment Re-establishment of donor hematopoiesis Donor immune reconstitution (donor derived) Donor anti-tumor effect (GVL)
7 MAJOR COMPLICATIONS OF ALLOGENEIC HEMATOPOIETIC CELL TRANSPLANTATION Acute graft versus host disease (GVHD) Skin, liver, gastrointestinal tract Chronic graft vs host disease skin, mucous membranes, liver,lung All patients require immunosuppression or T cell depletion risk of infection, relapse Incidence of grade II IV GVHD: 10 40% Incidence of ch GVHD 60 80%
8 PATHOGENESIS Criteria for the development of GVHD are: The graft must contain immunologically i ll competent t cells. The host must possess important transplantation alloantigens that are lacking in the donor graft, so that the host appears foreign to the graft, and is, therefore, capable of stimulating it antigenically. The host itself must be incapable of mounting an effective immunological reaction against the graft, at least for sufficient time for the latter to manifest its immunological capabilities; that is, it must have the security of tenure. Billingham, 1966.
9 INCIDENCE OF GRAFT VS HOST DISEASE
10 INCIDENCE OF ACUTE GRAFT VS HOST DISEASE Cumulative probability of grade II IV IV acute graft-vs.-host disease (GVHD) after allogeneic bone marrow transplantation (BMT) from a genotypically human leukocyte antigen (HLA) identical sibling or other family members mismatched for 0 3 3loci on the non-shared haplotype.
11 Risk factors for GVHD Higher degree of HLA mismatching Older age of donor and/or recipient Donor and recipient gender disparity (female donor to male recipient) Alloimmunization i of fthe donor (history of pregnancy, transfusions) Source of stem cells (peripheral blood precursor cells [PBPC] rather than bone marrow or umbilical cord blood) Prior acute GVHD Administration of unirradiated donor buffy coat transfusions (eg, donor lymphocyte infusions) i Previous splenectomy Cytomegalovirus seropositivity (donor and/or recipient) Donor Epstein-Barr virus seropositivity
12 Classification of GVHD Classic acute GVHD Cases present within 100 days of hematopoieticcell cell transplant (HCT) anddisplayfeatures display of acute GVHD. Features of chronic GVHD are absent. Persistent, recurrent, late onset acute GVHD Cases present greater than 100 days post HCT HCTwith features of acute GVHD. Features of chronic GVHD are absent. Classic chronic GVHD Cases may present at any time post HCT. Features of chronic GVHD are present. There are no features of acute GVHD. Overlap syndrome Cases may present at any time post HCT with features of both chronic GVHD and acute GVHD.
13 Clinical features of chronic GVHD Skin 67 percent Mouth 60 percent Liver 52 percent Lung 50 percent Eye 48 percent Joints and fascia 48 percent Gastrointestinal tract 30 percent Genitalia 12 percent
14 DIAGNOSIS OF ch GVHD Diagnosis of ch GVHD requires the presence of at least one diagnostic clinical sign of ch GVHD or at least one confirmed biopsy or relevant test. Exclude other diagnosis
15 GRADING OF ch GVHD NIH consensus criteria for GVHD severity Mild Involves two or fewer organs/sites with no clinically significant functional impairment Moderate Involves three or more organs/sites with no clinically significant functional impairment or at least one organ/site with clinically significant functional impairment, but no major disability Severe Major disability caused by chronic GVHD
16 PREVENTION OF GVHD T cell depletion Methotrexate plus calcineurin inhibitor Sirolimus + tacrolimus Mycophenolate Mofetil Combination with Post transplant Cytoxan ATG Novel approaches like inclusion i of ECP, HDACi prior to transplant
17 GVHD TREATMENT Steroids- high dose ( most important ) topical or systemic Calcineurin inhibitors Rapimmune Mycophenolate Mofetil ATG, anti CD3, Cytoxan Denileukin Diftitox, alemtuzumab, dacluzimab JAK/STAT inhibitors Immunemodulation Mesenchymal stem cells
18 Chronic GVHD Symptom Management Erin Kopp M.S.N, A.C.N.P-B.C., N.P.
19 Disclosures No Disclosures
20 Objectives Identify common presentations of chronic GVHD by body system Discuss prevalence of cgvhd in the post allo transplant population Review available assessment tools for the cgvhd patient Discuss management options including both medial and nursing approaches
21 Goals of Treatment Is there a cure? Reduce symptom burden to patient Control objective symptoms related to GVHD Prevent further damage and resulting disability Balance potential toxicity from treatment with actual benefit perceived by the patient



22 Realistic Goals: Response to Treatment
23 Cutaneous GVHD Presentation and Management Seen in approximately 67% of patients Dry skin, pruritus, pigment changes, edema, erythema, stippling, lichen planus, hardening of skin, hidebound Daily use of emollients for management of dry skin minimizes pruritus and risk for infection-prefer ointment to lotion and cream Higher risk for skin cancer (especially SCC) Teach prevention including sun protection ti and surveillance May need hydrocortisone, sarna, or amlactin for pruritus Doxepin, gabapentin, naloxone used for systemic control of itching NBUVB for pruritus, PUVA, ECP Corticosteroid use *


24 Cutaneous Manifestations

25 Corticosteroid Choices and Potency
26 Corticosteroid Topical Topical application of corticosteroids may lead to atrophy of treated skin Utilization of lower potency (class VI-VII) on face and intertriginous t i i areas recommended d Aceniform rash, dry scaly eruption with follicular pustules around mouth, rosacea like rash, purpura, hyper/hypo pigmentation
27 Ulcerations and Infection Risk for Cutaneous GVHD Culture and biopsy as appropriate Keeping area moist and without fissure Minimize colonization with bleach bath Engage wound care specialists/plastic l ti surgery as indicated d









28 Ulcerations in cutaneous GVHD
29 Sclerotic Changes to Skin Affected areas can be minimal or diffuse Superficial tightening Deep sclerotic changes Hidebound d ECP, IL2, Monoclonal antibodies
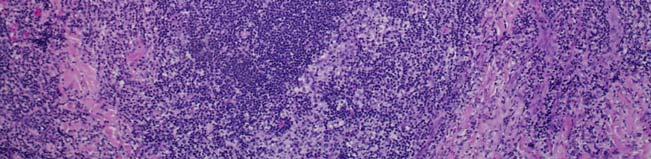
30 Physiologic Changes in Cutaneous GVHD Epidermal inflammation
31 Physiologic Changes in Cutaneous GVHD Dermal inflammation




32 Physiologic Changes in Cutaneous GVHD Fascial inflammation
33 Patient Education Teaching the patient about signs of progression and/or complication is key Tightness- edema vs infiltrative disease mediated by GVHD Change in ROM- identify specific activities iti that t patient t can be comfortable evaluating SOB, decrease in appetite with feeling of bloat, muscle cramping- all more insidious signs of progression
34 Mucosal Presentation and Management Approximately 60% of patients with GVHD Xerostomia Biotene products, lemon candy, gum, muscarinic agents (Pilocarpine, cevemeline) Avoid caffeine and alcoholic beverages Oral lesions- leukoplakia (cancer vs GVHD), lichenoid, mucoceles, ulcerations, oral candidiasis Surveillance for cancerous lesions (biopsy as needed) Topical dexamethasone, budesonide, tacrolimus, clobetasol, fluocinonide, tacrolimus Apply gel to affected area. No food or drink for 15minutes. Cover with gauze Topical rinse- 5ml for 5-15 minutes then spit. No food or drink for 15 minutes after Episil Treatment for oral candidiasis (high risk with immunosuppressive therapy and topical corticosteroid)



35 Mucosal Manifestations
36 11/4/2016 while on Dexamethasone swish & spit 1/6/ weeks of Budesonide sol swish & spit for 1 min, TID
37 Mucosal Management Sensitivity to temperature change, spicy food, toothpaste Utilization of children s toothpaste Episil Minimize consumption of spicy food Appropriate treatment of GVHD
38 Patient Education Oral hygiene is paramount Regular dental appointments with a dentist familiar with GVHD Signs of worsening of GVHD- increase in symptoms, new lesions, subtle changes Surveillance for cancerous lesions
39 Eye Presentation and Management 40-60% of patients with chronic GVHD Photophobia and significant pain common Cataracts Eye drops Punctal plugging, prose lenses Protective eye wear New treatments- Xiidra
40 Gastrointestinal Presentation and Management Approximately 30% of patients Esophageal involvement leading to esophageal web and tapering of esophagus Choking on pills/food, weight loss, painful ulcers Encourage fluid with each bite of food/pills GI consult, speech therapy possible esophageal dilatation Nutritionist Small and large bowel involvement Loose stools, malabsorption Gastric pain, gastric bloating Anorexia, nausea, vomiting, weight loss Budesonide, carafate, anti-diarrheals, pancreatic enzymes
41 Liver Manifestations and Management 50% of patients will have inbolvement of the liver Abnormal LFTs-elevation alkaline phosphatase, AST, ALT, and bilirubin Can mimic i other hepatic disease Rule out other potential causative factors May need to adjust immunosuppression; Actigall
42 Pulmonary Presentation and Management Approximately 50% of patients with GVHD Obstructive versus restrictive Bronchiolitis obliterans and bronchiolitis obliterans organizing pneumonia Evaluation for shortness of breath PFT Assess for subtle signs Chronic dry cough, exercise intolerance, decreased activity Overlying infection Idiopathic pneumonia syndrome Diffuse alveolar hemorrhage Management involves identification and reversal of causative factors when possible Pulmonary rehab Immunosuppression therapy Smoking Cessation
43 Musculoskeletal Presentation and Management Up to 50% patients, but often presents months to years after transplant Fasciitis- joint mobility limitation often in the continuum of skin findings Myositis- weakness with or without myalgia, symmetrical proximal muscles Check serum creatine kinase Edema of extremities- generally non-pitting Massage by lymphedema experts Compression stockings Muscle atrophy Physical and Occupational therapy to minimize destruction Assess utilization of corticosteroids Muscle cramping R/O electrolyte imbalance (calcineurin inhibitors cause hypomagnesemia and hyperkalemia) R/O neuropathy Tonic water
44 Gynecologic Manifestations and Management Exact incidence is unknown Reports range between 11-48% Often under reported and not assessed Vaginal dryness, itching, burning, and pain, loss of libido, inflammation and stenosis Diagnostic-lichen planus features, vaginal scarring or stenosis Erosions, fissures, and ulcers may occur Treatment-hormone replacement, dilators-gyn referral
45 Other Manifestations Recurrent sterile effusions Polyserositis Pericardial effusion Renal manifestations Nephrotic syndrome Any new symptom should be evaluated by hematologist
46 Assessment Tools Need for consistency as many components of assessment are subjective Must include both subjective and objective components to be comprehensive NIH consensus recommendations 2014 Paul Carpenter outlines specific GVHD assessment
47 Review on Each Visit
48
49 Summary Chronic GVHD manifests differently for individual patients Many symptoms are nuanced and require an astute provider/nurse to identify Patient education is critical Early intervention may prevent permanent disability Be Aware. Educate. Act
50 References Clinical manifestations, diagnosis, and grading of chronic graft vs host disease Treatment of chronic graft versus host disease Ruutu, et al (2014) Prophylaxis and treatment of GVHD: EBMT-ELN working group recommendations for a standardized practice Hematopoietic Stem Cell Transplantation: A manual for nursing practice. Second edition. () Carpenter, (2011). How I conduct a comprehensive chronic graftversus-host disease assessment. Blood, 118(10) Flowers, Mary E.D. & Martin, Paul J. (2015) How we treat t chronic graft-versus-host-disease. Blood 125:
51 Cutaneous Lymphomas Christiane Querfeld, M.D., Ph.D Director, Cutaneous Lymphoma Program
52 Disclosures Advisory Board - MiRagen, Actelion, Celgene, Therakos Consultant - Mindera Investigator - Celgene, MiRagen, Trillium Therapeutics, Actelion, Kyowa, Soligenix
53 Objectives Discuss the classification and staging of cutaneous T-cell lymphoma and state the prognosis associated with each stage. List and describe the skin-directed and systemic treatment options that are appropriate for each stage and cutaneous manifestation of cutaneous T-cell lymphoma. Recognize the impact of disease and disease symptoms on quality of life in patients with CTCL Recognize the major subtypes of cutaneous B cell lymphomas, the clinical features, prognosis, management and outcome.
54 THE 2016 UPDATED WHO CLASSIFICATION OF HEMATOLOGICAL MALIGNANCIES Mycosis fungoides Folliculotropic type Pagetoid reticulosis Granulomatous slack skin Sézary syndrome Cutaneous T cell lymphomas Primary cutaneous CD30+ lymphoproliferative disorders Lymphomatoid papulosis (type A-E) Primary cutaneous anaplastic large cell lymphoma Subcutaneous panniculitis-like T cell lymphoma Primary cutaneous γδ T cell lymphoma Primary cutaneous aggressive epidermotropic CD8+ cytotoxic T cell lymphoma Primary cutaneous acral CD8+ T cell lymphoma CD4 + small/medium-sized pleomorphic T-cell lymphoproliferative disorder Primary cutaneous peripheral T cell lymphoma, NOS Swerdlow SH et al. Blood :
55 Mycosis Fungoides Prototype of CTCL Low-grade lymphoma Post-thymic T-cell malignancy (CD4 + /CD45RO + ) Malignancy of 3 different T-cell populations: - Features of T-regulatory (CD25+FoxP3+), Th 2 - and Th 17 -cell phenotype Th2-driven di immunosuppressive i properties - Secretion of IL-4, IL-5, IL-6, IL-10 - Peripheral eosinophilia, elevated IgE - Decreased antigen-specific T-cell response - Impaired cell mediated cytotoxicity Patch, plaque, tumors and erythroderma Berger C et al. 2005; Dummer R et al. 1996; Krejsgaard T et al. 2010










56















57 Folliculotropic MF


58 Sézary Syndrome Systemic and aggressive variant Exfoliative erythroderma Ectropion, alopecia, palmoplantar keratoderma Severe pruritus Circulating, atypical, malignant T-lymphocytes (Sézary cells)
59
60 CTCL Staging All patients Selected patients Physical exam - Skin burden, nodes Skin biopsy -Immunophenotyping -TCR analysis Sézary cell counts by flow cytometry - CD4+/CD7-; CD4+/CD26- - CD4:CD8 ratio TCR analysis in PBMCs CBC, CMP, LDH HTLV-1 titer PET/CT scans Lymph node biopsy Bone marrow biopsy
61 Mycosis Fungoides/Sézary Syndrome Clinical signs Skin pathology Laboratory tests Molecular tests Prognostication Management What are the key prognostic markers that can help guide clinical management of CTCL?
62 Stage-based Treatment Algorithm for Mycosis Fungoides and Sézary Syndrome
63 Care and Quality of Life Monitor for cutaneous infections - Bacterial (S. aureus) ) - Viral (HSV, VZV, HHV6) Monitor for other skin cancers Pruritus, pain Nutritional deficiencies ce ces Psychological needs

64 Disabling Pruritus and Pain
65 CD 30 + Lymphoproliferative Disorders
66 Lymphomatoid Papulosis Recurrent papulonodular lesions Frequent ulceration Spontaneous involution Indolent course 10-20% associated with malignancy Fascin and CD134 predict progression TRAF1 expression distinguishes from ALCL
67 Cutaneous Anaplastic Large Cell Lymphoma Solitary or localized (ulcerating) nodules or tumors CD4 + CD30 + helper T-cell phenotype Overlap with LyP, transformed mycosis fungoides and cutaneous Hodgkin s disease Anaplastic morphology, non-epidermotropic, large lymphocytes No t(2;5) translocation; ALK negative
68 H&E H&E CD30
69 Treatment Regimens LyP: Observation PUVA Low dose weekly oral methotrexate NB-UVB and low dose oral Targretin (150 mg daily) topical steroid, topical bexarotene I.V. Brentuximab ALCL: Radiation (solitary/localized) Weekly oral methotrexate Pegylated doxorubicin I.V. Brentuximab
70 25% -30% of all cutaneous lymphomas are B-cell derived: WHO-EORTC Classification Cutaneous B-cell Lymphomas Type Frequency (%) 5 Year Survival (%) Indolent Primary cutaneous marginal zone 7 99 lymphoma Primary cutaneous follicular lymphoma Aggressive Primary cutaneous diffuse large B cell lymphoma, leg type Primary cutaneous diffuse large B cell lymphoma, other 4 55 <1 50 WHO EORTC (1905 patients), Blood 2005
71 Primary Cutaneous Follicle Center Lymphoma Most common type of cutaneous B cell lymphoma Solitary plaques/tumors on trunk, head or scalp; rarely grouped lesions CD20 +, Bcl 6 +, CD10 +, Bcl 2, MUM 1 (germinal center origin) Follicular, diffuse or mixed dermal infiltrate Neoplastic follicle center cells > Centrocytes (small to large cleaved cells) in low grade PFCL > Centroblasts (large round cells with prominent nuclei) in high grade PFCL No t(14:18) Cutaneous relapses ~50%, extracutaneous dissemination 5 10%











72
73
74 Primary Cutaneous Marginal Zone Lymphoma (Immunocytoma) MALT-type lymphoma Solitary or multiple red-violaceous papules, plaques, nodules on trunk and arms Association with B. afzelii (Europe), but not USA Frequent relapses, rarely extracutaneous dissemination CD20 +, CD79a +, CD5 -, CD10 -, Bcl-6 -, Bcl-2 +, phenotype MUM-1 + (plasma cells) Transformation to diffuse large B-cell lymphoma possible Relapse rate 40-45%












75 Marginal Zone Lymphoma Clinicopathologic Features K L
76 Primary cutaneous Diffuse Large B-cell Lymphoma, Leg Type Elderly females Solitary or multiple red-violaceous tumors mostly on lower legs, rarely at other sites CD20 +,CD5,C - CD79a 9a, + Bcl-2 +/-, Bcl-6 +/-, CD10-, MUM-1 +, FOXP1 +/- Frequent cutaneous relapses and extracutaneous dissemination No t(14:18) Chromosomal gains on chromosome 7p and 18q, loss of 6q Sheets of centroblasts and immunoblasts 5-year survival (multiple lesions): 50%





77 Primary Cutaneous DLBCL- Leg Type
78 5-y DSS: 71 pcmzl 98% 171 pcfcl 95% 58 DLBCL-LT 50% Multivariate analysis for pcfcl: FoxP1 expression and localization on leg carries poor prognosis
79 Rubio-Gonzalez, Zain, Rosen, Querfeld. Brit J Dermatol 2016





80 City of Hope Steven Rosen Larry Kwak Dennis Weisenburger Steven Forman Xiweii Wu Tijana Talisman Sung Hee Kil Joycelynne Palmer James Sanchez Peter Lee Yuan Yuan Chen Chongkai Wang Jasmine Zain Erin Kopp Karen Huelsman Estella Barrios Belen Gonzalez Linda Lee Donna Bui Thank You! Supported by: Toni Stephenson Lymphoma Center City of Hope Young Innovators Fund
Disclosures. Advisory Board. Consultant. Investigator. MiRagen, Actelion, Celgene, Therakos. Mindera
 Cutaneous Lymphomas Christiane Querfeld, MD, PhD Director, Cutaneous Lymphoma Program City of Hope ~ How the Experts Treat Hematologic Malignancies Symposium March 10 13, 2017 Disclosures Advisory Board
Cutaneous Lymphomas Christiane Querfeld, MD, PhD Director, Cutaneous Lymphoma Program City of Hope ~ How the Experts Treat Hematologic Malignancies Symposium March 10 13, 2017 Disclosures Advisory Board
Jasmine Zain, M.D. Erin Kopp, M.S.N, A.C.N.P-B.C., N.P. Director, Cutaneous Lymphoma Program
 MANAGEMENT OF CUTANEOUS LYMPHOMAS AND CGVHD Jasmine Zain, M.D. Erin Kopp, M.S.N, A.C.N.P-B.C., N.P. Christiane Querfeld, M.D., Ph.D Director, Cutaneous Lymphoma Program How the Experts Treat Hematologic
MANAGEMENT OF CUTANEOUS LYMPHOMAS AND CGVHD Jasmine Zain, M.D. Erin Kopp, M.S.N, A.C.N.P-B.C., N.P. Christiane Querfeld, M.D., Ph.D Director, Cutaneous Lymphoma Program How the Experts Treat Hematologic
Overview of Cutaneous Lymphomas: Diagnosis and Staging. Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology
 Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology
 Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology Agenda Overview of cutaneous T and B- cell lymphomas Diagnosis, Staging, Prognosis
Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology Agenda Overview of cutaneous T and B- cell lymphomas Diagnosis, Staging, Prognosis
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
BMT CTN 0801 Protocol. Chronic GVHD Provider Survey ENROLLMENT
 BMT CTN 0801 Protocol Chronic GVHD Provider Survey ENROLLMENT Instructions: Please score a symptom only if you know or suspect it be related to chronic GVHD. Subjective are acceptable. For example, joint
BMT CTN 0801 Protocol Chronic GVHD Provider Survey ENROLLMENT Instructions: Please score a symptom only if you know or suspect it be related to chronic GVHD. Subjective are acceptable. For example, joint
BMT CTN 0801 Protocol. Chronic GVHD Provider Survey. FOLLOW-UP v3.0
 BMT CTN 0801 Protocol Chronic GVHD Provider Survey FOLLOW-UP v3.0 Instructions: Please score a symptom only if you know or suspect it be related to chronic GVHD. Subjective are acceptable. For example,
BMT CTN 0801 Protocol Chronic GVHD Provider Survey FOLLOW-UP v3.0 Instructions: Please score a symptom only if you know or suspect it be related to chronic GVHD. Subjective are acceptable. For example,
Therapeutic Management of Early Cutaneous Mycosis Fungoides
 Therapeutic Management of Early Cutaneous Mycosis Fungoides L Frank Glass, MD Cutaneous Lymphoma Programs H Lee Moffitt Cancer Center and Research Institute George Washington University Dermatology and
Therapeutic Management of Early Cutaneous Mycosis Fungoides L Frank Glass, MD Cutaneous Lymphoma Programs H Lee Moffitt Cancer Center and Research Institute George Washington University Dermatology and
Trends in Hematopoietic Cell Transplantation. AAMAC Patient Education Day Oct 2014
 Trends in Hematopoietic Cell Transplantation AAMAC Patient Education Day Oct 2014 Objectives Review the principles behind allogeneic stem cell transplantation Outline the process of transplant, some of
Trends in Hematopoietic Cell Transplantation AAMAC Patient Education Day Oct 2014 Objectives Review the principles behind allogeneic stem cell transplantation Outline the process of transplant, some of
ISPUB.COM. Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose Methotrexate. S Parker INTRODUCTION
 ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose S Parker Citation S Parker.. The Internet Journal of
ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose S Parker Citation S Parker.. The Internet Journal of
Cutaneous Lymphoid Proliferations: A Comprehensive Textbook of Lymphocytic Infiltrates of the Skin
 Cutaneous Lymphoid Proliferations: A Comprehensive Textbook of Lymphocytic Infiltrates of the Skin Magro, Cynthia M., MD ISBN-13: 9780471695981 Table of Contents Chapter One: Introduction to the Classification
Cutaneous Lymphoid Proliferations: A Comprehensive Textbook of Lymphocytic Infiltrates of the Skin Magro, Cynthia M., MD ISBN-13: 9780471695981 Table of Contents Chapter One: Introduction to the Classification
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma and Pseudolymphoma
 Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
Acute Graft-versus-Host Disease (agvhd) Udomsak Bunworasate Chulalongkorn University
 Udomsak Bunworasate Chulalongkorn University") Acute Graft-versus-Host Disease (agvhd) Udomsak Bunworasate Chulalongkorn University Graft-versus-Host Disease (GVHD) Background GVHD is an immunologic reaction of the donor immune cells (Graft) against
Acute Graft-versus-Host Disease (agvhd) Udomsak Bunworasate Chulalongkorn University Graft-versus-Host Disease (GVHD) Background GVHD is an immunologic reaction of the donor immune cells (Graft) against
Chronic graft-versus-host disease
 Chronic graft-versus-host disease Badri Modi, MD Assistant Clinical Professor Division of Dermatology City of Hope Erin Kopp, ACNP-BC Nurse Practitioner Department of Hematology City of Hope HOW THE EXPERTS
Chronic graft-versus-host disease Badri Modi, MD Assistant Clinical Professor Division of Dermatology City of Hope Erin Kopp, ACNP-BC Nurse Practitioner Department of Hematology City of Hope HOW THE EXPERTS
An Overview of Blood and Marrow Transplantation
 An Overview of Blood and Marrow Transplantation October 24, 2009 Stephen Couban Department of Medicine Dalhousie University Objectives What are the types of blood and marrow transplantation? Who may benefit
An Overview of Blood and Marrow Transplantation October 24, 2009 Stephen Couban Department of Medicine Dalhousie University Objectives What are the types of blood and marrow transplantation? Who may benefit
CUTANEOUS T-CELL LYMPHOMA PROFORMA
 STATE OF KUWAIT MINISTRY OF HEALTH AS AD ALHAMAD DERMATOLOGY CENTER ALSABAH HOSPITAL دولة الكویت وزارة الصحة مرآز أسعد الحمد للا مراض الجلدیة مستشفى الصباح بسم االله الرحمن الرحيم CUTANEOUS TCELL LYMPHOMA
STATE OF KUWAIT MINISTRY OF HEALTH AS AD ALHAMAD DERMATOLOGY CENTER ALSABAH HOSPITAL دولة الكویت وزارة الصحة مرآز أسعد الحمد للا مراض الجلدیة مستشفى الصباح بسم االله الرحمن الرحيم CUTANEOUS TCELL LYMPHOMA
2. Sézary syndrome (SS)
") Go Back to the Top To Order, Visit the Purchasing Page for Details Clinical images are available in hardcopy only. Clinical images are available in Clinical images are available in d e f g h i j Fig..36-2
Go Back to the Top To Order, Visit the Purchasing Page for Details Clinical images are available in hardcopy only. Clinical images are available in Clinical images are available in d e f g h i j Fig..36-2
Introduction to Clinical Hematopoietic Cell Transplantation (HCT) George Chen, MD Thursday, May 03, 2018
 George Chen, MD Thursday, May 03, 2018") Introduction to Clinical Hematopoietic Cell Transplantation (HCT) George Chen, MD Thursday, May 03, 2018 The transfer of hematopoietic progenitor and stem cells for therapeutic purposes Hematopoietic Cell
Introduction to Clinical Hematopoietic Cell Transplantation (HCT) George Chen, MD Thursday, May 03, 2018 The transfer of hematopoietic progenitor and stem cells for therapeutic purposes Hematopoietic Cell
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
SCORE 0 SCORE 1 SCORE 2 SCORE 3 Asymptomatic and fully active (ECOG 0; KPS or LPS 100%)
") Organ Scoring of Chronic GVHD PERFORMANCE SCORE: KPS ECOG LPS SKIN SCORE % BSA GVHD features to be scored by BSA: applies: Maculopapular rash/erythema Lichen planus-like features Sclerotic features Papulosquamous
Organ Scoring of Chronic GVHD PERFORMANCE SCORE: KPS ECOG LPS SKIN SCORE % BSA GVHD features to be scored by BSA: applies: Maculopapular rash/erythema Lichen planus-like features Sclerotic features Papulosquamous
Allogeneic Stem Cell Transplantation for Cutaneous T-cell Lymphoma: Updated results from a single center
 Allogeneic Stem Cell Transplantation for Cutaneous T-cell Lymphoma: Updated results from a single center Madeleine Duvic, MD Professor and Deputy Chairman Blanche Bender Professor in Cancer Research Departments
Allogeneic Stem Cell Transplantation for Cutaneous T-cell Lymphoma: Updated results from a single center Madeleine Duvic, MD Professor and Deputy Chairman Blanche Bender Professor in Cancer Research Departments
Stem Cell Transplantation for Severe Aplastic Anemia
 Number of Transplants 10/24/2011 Stem Cell Transplantation for Severe Aplastic Anemia Claudio Anasetti, MD Professor of Oncology and Medicine Chair, Blood and Marrow Transplant Dpt Moffitt Cancer Center
Number of Transplants 10/24/2011 Stem Cell Transplantation for Severe Aplastic Anemia Claudio Anasetti, MD Professor of Oncology and Medicine Chair, Blood and Marrow Transplant Dpt Moffitt Cancer Center
Clinical Commissioning Policy Proposition: Treatments for Graft versus Host Disease (GvHD) following Haematopoietic Stem Cell Transplantation
 following Haematopoietic Stem Cell Transplantation") Clinical Commissioning Policy Proposition: Treatments for Graft versus Host Disease (GvHD) following Haematopoietic Stem Cell Transplantation Reference: NHS England F01X08/01 1 Information Reader Box (IRB)
Clinical Commissioning Policy Proposition: Treatments for Graft versus Host Disease (GvHD) following Haematopoietic Stem Cell Transplantation Reference: NHS England F01X08/01 1 Information Reader Box (IRB)
Classification of Cutaneous T cell Lymphomas (CTCLs) Hernani Cualing, MD
 Hernani Cualing, MD") Classification of Cutaneous T cell Lymphomas (CTCLs) Hernani Cualing, MD Pathology and Cell Biology, USF IFLOW, Inc. CTCL, MF, and Sézary syndrome In 1806, mycosis fungoides (MF) was first described 1
Classification of Cutaneous T cell Lymphomas (CTCLs) Hernani Cualing, MD Pathology and Cell Biology, USF IFLOW, Inc. CTCL, MF, and Sézary syndrome In 1806, mycosis fungoides (MF) was first described 1
A middle-aged man with self-healing papulonecrotic lesions over the trunk and proximal limbs
 Hong Kong J. Dermatol. Venereol. (2011) 19, 30-34 Case Report A middle-aged man with self-healing papulonecrotic lesions over the trunk and proximal limbs JC Chan, N Trendell-Smith, CK Yeung Lymphomatoid
Hong Kong J. Dermatol. Venereol. (2011) 19, 30-34 Case Report A middle-aged man with self-healing papulonecrotic lesions over the trunk and proximal limbs JC Chan, N Trendell-Smith, CK Yeung Lymphomatoid
5/9/2018. Bone marrow failure diseases (aplastic anemia) can be cured by providing a source of new marrow
 can be cured by providing a source of new marrow") 5/9/2018 or Stem Cell Harvest Where we are now, and What s Coming AA MDS International Foundation Indianapolis IN Luke Akard MD May 19, 2018 Infusion Transplant Conditioning Treatment 2-7 days STEM CELL
5/9/2018 or Stem Cell Harvest Where we are now, and What s Coming AA MDS International Foundation Indianapolis IN Luke Akard MD May 19, 2018 Infusion Transplant Conditioning Treatment 2-7 days STEM CELL
The World of Dermatology
 The World of Dermatology, F.A.A.D. Assistant Professor of Dermatology University of Nevada School of Medicine Director of J. Woodson Dermatology & Associates, LTD Objectives Cite the advances in management
The World of Dermatology, F.A.A.D. Assistant Professor of Dermatology University of Nevada School of Medicine Director of J. Woodson Dermatology & Associates, LTD Objectives Cite the advances in management
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia
 Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia Liat Shragian Alon, MD Rabin Medical Center, ISRAEL #EBMT15 www.ebmt.org Patient: 25-year-old male No prior medical history
Severe Viral Related Complications Following Allo-HCT for Severe Aplastic Anemia Liat Shragian Alon, MD Rabin Medical Center, ISRAEL #EBMT15 www.ebmt.org Patient: 25-year-old male No prior medical history
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Istodax) Reference Number: CP.PHAR.314 Effective Date: 01.01.17 Last Review Date: 11.18 Line of Business: Medicaid, HIM-Medical Benefit Coding Implications Revision Log See Important
Clinical Policy: (Istodax) Reference Number: CP.PHAR.314 Effective Date: 01.01.17 Last Review Date: 11.18 Line of Business: Medicaid, HIM-Medical Benefit Coding Implications Revision Log See Important
New Haven, Connecticut
 New Haven, Connecticut Yale University Main Campus Yale mascot: Handsome Dan Cutaneous Lymphomas Tony Subtil, MD, MBA Associate Professor Yale University Cutaneous Lymphomas: 1. Intro 2. CTCL/NK 3. CBCL
New Haven, Connecticut Yale University Main Campus Yale mascot: Handsome Dan Cutaneous Lymphomas Tony Subtil, MD, MBA Associate Professor Yale University Cutaneous Lymphomas: 1. Intro 2. CTCL/NK 3. CBCL
Supportive Care in the Management of T-cell Lymphomas
 Supportive Care in the Management of T-cell Lymphomas Erin Kopp, ACNP-BC City of Hope Comprehensive Cancer Center NCCN.org For Clinicians NCCN.org/patients For Patients Objectives Discuss the role of supportive
Supportive Care in the Management of T-cell Lymphomas Erin Kopp, ACNP-BC City of Hope Comprehensive Cancer Center NCCN.org For Clinicians NCCN.org/patients For Patients Objectives Discuss the role of supportive
How I treat patients whose biopsies are reported descriptively Youn H Kim, MD
 How I treat patients whose biopsies are reported descriptively Youn H Kim, MD Director, Multidisciplinary Cutaneous Lymphoma Group Stanford Cancer institute & School of Medicine NCCN NHL Panel Member Disclosure
How I treat patients whose biopsies are reported descriptively Youn H Kim, MD Director, Multidisciplinary Cutaneous Lymphoma Group Stanford Cancer institute & School of Medicine NCCN NHL Panel Member Disclosure
Renaissance of Low-Dose Radiotherapy Concepts for Cutaneous Lymphomas
 Review Article DOI: 10.1159/000470845 Received: February 06, 2017 Accepted: March 13, 2017 Published online: April 6, 2017 Renaissance of Low-Dose Radiotherapy Concepts for Cutaneous Lymphomas Bouthaina
Review Article DOI: 10.1159/000470845 Received: February 06, 2017 Accepted: March 13, 2017 Published online: April 6, 2017 Renaissance of Low-Dose Radiotherapy Concepts for Cutaneous Lymphomas Bouthaina
Cutaneous Lymphomas New Aspects
 Cutaneous Lymphomas New Aspects Christiane Querfeld, MD, PhD Chief, Div. of Dermatology Director, Cutaneous Lymphoma Program City of Hope ~ How the Experts Treat Hematologic Malignancies Symposium March
Cutaneous Lymphomas New Aspects Christiane Querfeld, MD, PhD Chief, Div. of Dermatology Director, Cutaneous Lymphoma Program City of Hope ~ How the Experts Treat Hematologic Malignancies Symposium March
EXTRACORPOREAL PHOTOPHERESIS MAGGIE FOSTER MANAGER ROTHERHAM PHOTOPHERESIS UNIT
 EXTRACORPOREAL PHOTOPHERESIS MAGGIE FOSTER MANAGER ROTHERHAM PHOTOPHERESIS UNIT AIM OF PRESENTATION Explain about Photopheresis. Rotherham service. Conditions treated Advantages /disadvantages of XTS &
EXTRACORPOREAL PHOTOPHERESIS MAGGIE FOSTER MANAGER ROTHERHAM PHOTOPHERESIS UNIT AIM OF PRESENTATION Explain about Photopheresis. Rotherham service. Conditions treated Advantages /disadvantages of XTS &
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/2010 holds various files of this Leiden University dissertation. Author: Benner, Marchina Frederika Title: Cutaneous CD30-positive lymphoproliferations
Cover Page The handle http://hdl.handle.net/1887/2010 holds various files of this Leiden University dissertation. Author: Benner, Marchina Frederika Title: Cutaneous CD30-positive lymphoproliferations
Index. derm.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acitretin and cutaneous T-cell lymphomas, 716 719, 722, 725 ADCC. See Antibody-dependent cell-mediated cytotoxicity. Adjunctive therapies and
Note: Page numbers of article titles are in boldface type. A Acitretin and cutaneous T-cell lymphomas, 716 719, 722, 725 ADCC. See Antibody-dependent cell-mediated cytotoxicity. Adjunctive therapies and
Approach to the Transplant Patient. Amy Musiek, MD AAD Annual Meeting 2018
 Approach to the Transplant Patient Amy Musiek, MD AAD Annual Meeting 2018 Disclosures Actelion: speaker, advisory board, investigator Elorac: investigator Kyowa: investigator, advisory board Seattle genetics:
Approach to the Transplant Patient Amy Musiek, MD AAD Annual Meeting 2018 Disclosures Actelion: speaker, advisory board, investigator Elorac: investigator Kyowa: investigator, advisory board Seattle genetics:
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Cell Transplantation for CLL and SLL File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_cll_and_sll 2/2001
Corporate Medical Policy Hematopoietic Cell Transplantation for CLL and SLL File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_cell_transplantation_for_cll_and_sll 2/2001
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
CASE 15 Patient: A 41-year-old Thai female Chief Compliant: Generalized papulovesicular rash for 1 month Present Illness: She presented with a 1-week
 CASE 15 Patient: A 41-year-old Thai female Chief Compliant: Generalized papulovesicular rash for 1 month Present Illness: She presented with a 1-week history of the generalized asymptomatic erythematous
CASE 15 Patient: A 41-year-old Thai female Chief Compliant: Generalized papulovesicular rash for 1 month Present Illness: She presented with a 1-week history of the generalized asymptomatic erythematous
(Chronic) Graft Versus Host Disease: When the transplant is just the beginning of the journey
 Graft Versus Host Disease: When the transplant is just the beginning of the journey") (Chronic) Graft Versus Host Disease: When the transplant is just the beginning of the journey Kitsada Wudhikarn, MD Division of Hematology, Department of Medicine King Chulalongkorn Memorial Hospital Disclosure
(Chronic) Graft Versus Host Disease: When the transplant is just the beginning of the journey Kitsada Wudhikarn, MD Division of Hematology, Department of Medicine King Chulalongkorn Memorial Hospital Disclosure
Case Report A Severe Case of Lymphomatoid Papulosis Type E Successfully Treated with Interferon-Alfa 2a
 Hindawi Case Reports in Dermatological Medicine Volume 2017, Article ID 3194738, 5 pages https://doi.org/10.1155/2017/3194738 Case Report A Severe Case of Lymphomatoid Papulosis Type E Successfully Treated
Hindawi Case Reports in Dermatological Medicine Volume 2017, Article ID 3194738, 5 pages https://doi.org/10.1155/2017/3194738 Case Report A Severe Case of Lymphomatoid Papulosis Type E Successfully Treated
SKIN CANCER AFTER HSCT
 SKIN CANCER AFTER HSCT David Rice, PhD, MSN, RN, NP, NEA-BC Director, Education, Evidence-based Practice and Research City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES
SKIN CANCER AFTER HSCT David Rice, PhD, MSN, RN, NP, NEA-BC Director, Education, Evidence-based Practice and Research City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES
Corporate Medical Policy
 Corporate Medical Policy Extracorporeal Photopheresis File Name: Origination: Last CAP Review: Next CAP Review: Last Review: extracorporeal_photopheresis 9/2010 8/2017 8/2018 8/2017 Description of Procedure
Corporate Medical Policy Extracorporeal Photopheresis File Name: Origination: Last CAP Review: Next CAP Review: Last Review: extracorporeal_photopheresis 9/2010 8/2017 8/2018 8/2017 Description of Procedure
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Corporate Medical Policy Hematopoietic Stem-Cell Transplant for Non-Hodgkin Lymphomas File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem-cell_transplant_for_non_hodgkin_lymphomas
Indolent Lymphomas: Current. Dr. Laurie Sehn
 Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
Indolent Lymphomas: Current Dr. Laurie Sehn Why does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with current standard
4100: Cellular Therapy Essential Data Follow-Up Form
 4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
4100: Cellular Therapy Essential Data Follow-Up Form Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Event date: Visit: 100 day 6 months 1 year 2 years >2 years, Specify:
Acknowledgements. Department of Hematological Malignancy and Cellular Therapy, University of Kansas Medical Center
 The Addition of Extracorporeal Photopheresis (ECP) to Tacrolimus and Methotrexate to Prevent Acute and Chronic Graft- Versus Host Disease in Myeloablative Hematopoietic Cell Transplant (HCT) Anthony Accurso,
The Addition of Extracorporeal Photopheresis (ECP) to Tacrolimus and Methotrexate to Prevent Acute and Chronic Graft- Versus Host Disease in Myeloablative Hematopoietic Cell Transplant (HCT) Anthony Accurso,
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation. Dermatopathology Specialists Needed. Changing Trends
 Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Lung Injury after HCT
 Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Objectives. Hematopoietic Stem Cell Transplant. Approaches to Transplant. Indications for HSCT. Define HSCT. Provide overview of HSCT process
 Objectives Hematopoietic Stem Cell Transplant Karen Anderson, MN, RN, OCN University of Washington Medical Center Define HSCT Provide overview of HSCT process Discuss acute complications of HSCT Discuss
Objectives Hematopoietic Stem Cell Transplant Karen Anderson, MN, RN, OCN University of Washington Medical Center Define HSCT Provide overview of HSCT process Discuss acute complications of HSCT Discuss
ISPUB.COM. Management of Co-existing Mycosis Fungoides and Lymphomatoid Papulosis. E Kim PHYSICAL FINDINGS INTRODUCTION INITIAL PRESENTATION
 ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Management of Co-existing Mycosis Fungoides and Lymphomatoid Papulosis E Kim Citation E Kim. Management of Co-existing Mycosis Fungoides
ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Management of Co-existing Mycosis Fungoides and Lymphomatoid Papulosis E Kim Citation E Kim. Management of Co-existing Mycosis Fungoides
ISPUB.COM. Bexarotene in Tumor stage Mycosis Fungoides. R Talpur, M Duvic INITIAL PRESENTATION TREATMENT COURSE INTRODUCTION
 ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Bexarotene in Tumor stage Mycosis Fungoides R Talpur, M Duvic Citation R Talpur, M Duvic. Bexarotene in Tumor stage Mycosis Fungoides. The
ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Bexarotene in Tumor stage Mycosis Fungoides R Talpur, M Duvic Citation R Talpur, M Duvic. Bexarotene in Tumor stage Mycosis Fungoides. The
Fig. 3.1 Fig Past history: She was previously healthy and not taking any medication.
 Case 3 A 41-year-old Thai female from Bangkok Chief compliant: Erythematous patch at left thigh for 2 months Present illness: The patient presented with a 10- year history of erythematous patch on her
Case 3 A 41-year-old Thai female from Bangkok Chief compliant: Erythematous patch at left thigh for 2 months Present illness: The patient presented with a 10- year history of erythematous patch on her
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Cutaneous Lymphomas: Novel Immune Therapies for Cutaneous T-cell Lymphoma
 Cutaneous Lymphomas: Novel Immune Therapies for Cutaneous T-cell Lymphoma Christiane Querfeld, MD, PhD Chief, Division of Dermatology Director, Cutaneous Lymphoma Program City of Hope ~ How the Experts
Cutaneous Lymphomas: Novel Immune Therapies for Cutaneous T-cell Lymphoma Christiane Querfeld, MD, PhD Chief, Division of Dermatology Director, Cutaneous Lymphoma Program City of Hope ~ How the Experts
What s a Transplant? What s not?
 What s a Transplant? What s not? How to report the difference? Daniel Weisdorf MD University of Minnesota Anti-cancer effects of BMT or PBSCT [HSCT] Kill the cancer Save the patient Restore immunocompetence
What s a Transplant? What s not? How to report the difference? Daniel Weisdorf MD University of Minnesota Anti-cancer effects of BMT or PBSCT [HSCT] Kill the cancer Save the patient Restore immunocompetence
Reduced-intensity Conditioning Transplantation
 Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
Reduced-intensity Conditioning Transplantation Current Role and Future Prospect He Huang M.D., Ph.D. Bone Marrow Transplantation Center The First Affiliated Hospital Zhejiang University School of Medicine,
clinical recommendations
 19 (Supplement 2): ii72 ii76, 2008 doi:10.1093/annonc/mdn095 Primary cutaneous lymphoma: ESMO Clinical Recommendations for diagnosis, treatment and follow-up R. Dummer 1 & M. Dreyling 2 On behalf of the
19 (Supplement 2): ii72 ii76, 2008 doi:10.1093/annonc/mdn095 Primary cutaneous lymphoma: ESMO Clinical Recommendations for diagnosis, treatment and follow-up R. Dummer 1 & M. Dreyling 2 On behalf of the
Kavita Raj Consultant Haematologist KHP
 Kavita Raj Consultant Haematologist KHP 1950s Billingham and Brent injection of spleen cells from adult mice into newborn mice Thickening and loss elasticity of skin, red soles, exfoliation, diarrhoea
Kavita Raj Consultant Haematologist KHP 1950s Billingham and Brent injection of spleen cells from adult mice into newborn mice Thickening and loss elasticity of skin, red soles, exfoliation, diarrhoea
Treatment of Chronic Graft versus Host Disease. Daniel Weisdorf MD University of Minnesota
 Treatment of Chronic Graft versus Host Disease Daniel Weisdorf MD University of Minnesota October 2013 Infections Transplant Events d-8 0 1mo 3mo 6mo Conditioning Transplant Engraftment Mucositis Organ
Treatment of Chronic Graft versus Host Disease Daniel Weisdorf MD University of Minnesota October 2013 Infections Transplant Events d-8 0 1mo 3mo 6mo Conditioning Transplant Engraftment Mucositis Organ
S003 CPC Self-Assessment
 S003 CPC Self-Assessment Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo
S003 CPC Self-Assessment Alina G. Bridges, D.O. Associate Professor Program Director, Dermatopathology Fellowship Department of Dermatology, Division of Dermatopathology and Cutaneous Immunopathology Mayo
Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center
 What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
Non-Hodgkin Lymphoma. Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract.
 Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
10/31/2017. Immunodeficiencies. Outline. Discuss EBV. Non-destructive Polymorphic Monomorphic Therapies Challenges
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
Change Summary - Form 2018 (R3) 1 of 12
 1 of 12") Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
11/2/2017. Immunodeficiencies. Joo Y. Song, MD Assistant Professor of Clinical Pathology. I have no financial disclosures.
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
Corporate Medical Policy
 Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem_cell_transplantation_for_waldenstrom_macroglobulinemia
Corporate Medical Policy Hematopoietic Stem-Cell Transplantation for Waldenstrom Macroglobulinemia File Name: Origination: Last CAP Review: Next CAP Review: Last Review: hematopoietic_stem_cell_transplantation_for_waldenstrom_macroglobulinemia
Transplantation in CTCL using TLI/ATG Conditioning
 Transplantation in CTCL using TLI/ATG Conditioning Liam Smyth Heidelberg (Germany), September 24-26, 2015 #EBMTLymphoma www.ebmt.org 65 year old male Case Report Presented in 2004 54yrs ECOG 0/1 Erythrodermic
Transplantation in CTCL using TLI/ATG Conditioning Liam Smyth Heidelberg (Germany), September 24-26, 2015 #EBMTLymphoma www.ebmt.org 65 year old male Case Report Presented in 2004 54yrs ECOG 0/1 Erythrodermic
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Vorinostat (Zolinza) Reference Number: CP.PHAR.83 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end
Clinical Policy: Vorinostat (Zolinza) Reference Number: CP.PHAR.83 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end
Clinical Policy: Vorinostat (Zolinza) Reference Number: CP.PHAR.83 Effective Date: 10/11
 Reference Number: CP.PHAR.83 Effective Date: 10/11") Clinical Policy: (Zolinza) Reference Number: CP.PHAR.83 Effective Date: 10/11 Last Review Date: 12/16 Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Clinical Policy: (Zolinza) Reference Number: CP.PHAR.83 Effective Date: 10/11 Last Review Date: 12/16 Revision Log See Important Reminder at the end of this policy for important regulatory and legal information.
Late Complications. Objectives. Long-term Survival after HCT. Long-term Survival and Late Complications after HCT. Long-term Survival after HCT
 Objectives Late Complications Navneet Majhail, MD, MS Review late complications in hematopoietic cell transplant (HCT) recipients Review screening and prevention guidelines for HCT survivors Review upcoming
Objectives Late Complications Navneet Majhail, MD, MS Review late complications in hematopoietic cell transplant (HCT) recipients Review screening and prevention guidelines for HCT survivors Review upcoming
Late Complications. Navneet Majhail, MD, MS
 Late Complications Navneet Majhail, MD, MS Medical Director, Health Services Research, NMDP Assistant Scientific Director, CIBMTR Adjunct Associate Professor of Medicine University of Minnesota Objectives
Late Complications Navneet Majhail, MD, MS Medical Director, Health Services Research, NMDP Assistant Scientific Director, CIBMTR Adjunct Associate Professor of Medicine University of Minnesota Objectives
SH/EAHP Workshop 2011 Los Angeles, California, USA
 SH/EAHP Workshop 2011 Los Angeles, California, USA October 27-29, 2011 Session 3 Non-Mycosis Fungoides CTCL Patty Jansen & Rein Willemze Introduction Submitted: 101 cases + 7 cases group 1: 108 Deactivated
SH/EAHP Workshop 2011 Los Angeles, California, USA October 27-29, 2011 Session 3 Non-Mycosis Fungoides CTCL Patty Jansen & Rein Willemze Introduction Submitted: 101 cases + 7 cases group 1: 108 Deactivated
Review Article. Cutaneous lymphoproliferative disorders. NJ Trendell-Smith
 Hong Kong J. Dermatol. Venereol. (2010) 18, 190-201 Review Article Cutaneous lymphoproliferative disorders NJ Trendell-Smith Cutaneous lymphoproliferative disorders (CLD) include reactive lymphoid hyperplasias,
Hong Kong J. Dermatol. Venereol. (2010) 18, 190-201 Review Article Cutaneous lymphoproliferative disorders NJ Trendell-Smith Cutaneous lymphoproliferative disorders (CLD) include reactive lymphoid hyperplasias,
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
What is Graft Vs Host Disease?
 Acute Graft Versus Host Disease Objectives Review pathophysiology of Acute Graft vs. Host Disease (agvhd) Identify Risk factors for agvhd Alison Thomsen RN, CPON Clinical Educator Inpatient Cancer Care
Acute Graft Versus Host Disease Objectives Review pathophysiology of Acute Graft vs. Host Disease (agvhd) Identify Risk factors for agvhd Alison Thomsen RN, CPON Clinical Educator Inpatient Cancer Care
Oral & Vulvovaginal GVHD. Rachel Kornik, MD Assistant Professor of Dermatology University of Wisconsin Hospital and Clinics
 Oral & Vulvovaginal GVHD Rachel Kornik, MD Assistant Professor of Dermatology University of Wisconsin Hospital and Clinics DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Rachel Kornik, MD S001 Advanced Medical
Oral & Vulvovaginal GVHD Rachel Kornik, MD Assistant Professor of Dermatology University of Wisconsin Hospital and Clinics DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Rachel Kornik, MD S001 Advanced Medical
What is Graft Vs Host Disease?
 Graft Failure Graft Versus Host Disease Graft Versus Leukemia Objectives Define graft failure Describe Graft vs. Leukemia effect Review pathophysiology and risk factors for Graft vs. Host Disease (GVHD)
Graft Failure Graft Versus Host Disease Graft Versus Leukemia Objectives Define graft failure Describe Graft vs. Leukemia effect Review pathophysiology and risk factors for Graft vs. Host Disease (GVHD)
Stem cell transplantation. Dr Mohammed Karodia NHLS & UP
 Stem cell transplantation Dr Mohammed Karodia NHLS & UP The use of haemopoeitic stem cells from a donor harvested from peripheral blood or bone marrow, to repopulate recipient bone marrow. Allogeneic From
Stem cell transplantation Dr Mohammed Karodia NHLS & UP The use of haemopoeitic stem cells from a donor harvested from peripheral blood or bone marrow, to repopulate recipient bone marrow. Allogeneic From
Immunosuppressive therapy for graft-versus-host disease. Mohamad Mohty Institut Paoli-Calmettes, Marseille
 Immunosuppressive therapy for graft-versus-host disease Mohamad Mohty Institut Paoli-Calmettes, Marseille Survival according to GVHD grade (Joint SFGM-TC, DFCI and IBMTR data; N=607) Cahn et al., Blood
Immunosuppressive therapy for graft-versus-host disease Mohamad Mohty Institut Paoli-Calmettes, Marseille Survival according to GVHD grade (Joint SFGM-TC, DFCI and IBMTR data; N=607) Cahn et al., Blood
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Immune Reconstitution Following Hematopoietic Cell Transplant
 Immune Reconstitution Following Hematopoietic Cell Transplant Patrick J. Kiel, PharmD, BCPS, BCOP Clinical Pharmacy Specialist Indiana University Simon Cancer Center Conflicts of Interest Speaker Bureau
Immune Reconstitution Following Hematopoietic Cell Transplant Patrick J. Kiel, PharmD, BCPS, BCOP Clinical Pharmacy Specialist Indiana University Simon Cancer Center Conflicts of Interest Speaker Bureau
U006 Primary Cutaneous Lymphomas: Diagnosis, Staging and When to Refer M. Yadira Hurley, MD
 U006 Primary Cutaneous Lymphomas: Diagnosis, Staging and When to Refer M. Yadira Hurley, MD hurleyy@slu.edu DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Actelion: Speaker Honoraria, Investigator Grants, Consultant
U006 Primary Cutaneous Lymphomas: Diagnosis, Staging and When to Refer M. Yadira Hurley, MD hurleyy@slu.edu DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Actelion: Speaker Honoraria, Investigator Grants, Consultant
Non-Hodgkin Lymphoma in Clinically Difficult Situations
 Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
MUD SCT. Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University
 MUD SCT Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outlines Optimal match criteria for unrelated adult donors Role of ATG in MUD-SCT Post-transplant
MUD SCT Pimjai Niparuck Division of Hematology, Department of Medicine Ramathibodi Hospital, Mahidol University Outlines Optimal match criteria for unrelated adult donors Role of ATG in MUD-SCT Post-transplant
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307
 Reference Number: PA.CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
WISKOTT-ALDRICH SYNDROME. An X-linked Primary Immunodeficiency
 WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
WISKOTT-ALDRICH SYNDROME An X-linked Primary Immunodeficiency WHAT IS WISKOTT ALDRICH SYNDROME? Wiskott-Aldrich Syndrome (WAS) is a serious medical condition that causes problems both with the immune system
Dr. Yi-chi M. Kong August 8, 2001 Benjamini. Ch. 19, Pgs Page 1 of 10 TRANSPLANTATION
 Benjamini. Ch. 19, Pgs 379-399 Page 1 of 10 TRANSPLANTATION I. KINDS OF GRAFTS II. RELATIONSHIPS BETWEEN DONOR AND RECIPIENT Benjamini. Ch. 19, Pgs 379-399 Page 2 of 10 II.GRAFT REJECTION IS IMMUNOLOGIC
Benjamini. Ch. 19, Pgs 379-399 Page 1 of 10 TRANSPLANTATION I. KINDS OF GRAFTS II. RELATIONSHIPS BETWEEN DONOR AND RECIPIENT Benjamini. Ch. 19, Pgs 379-399 Page 2 of 10 II.GRAFT REJECTION IS IMMUNOLOGIC
Dental Management of the Organ or Stem Cell Transplant Patient
 Dental Management of the Organ or Stem Cell Transplant Patient KEY POINTS Before and after organ or stem cell transplantation, patients require specialized dental management. Optimal dental management
Dental Management of the Organ or Stem Cell Transplant Patient KEY POINTS Before and after organ or stem cell transplantation, patients require specialized dental management. Optimal dental management
Subject Index. Dry desquamation, see Skin reactions, radiotherapy
 Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s