CKD FOR PRIMARY CARE MINNESOTA ACADEMY OF PHYSICIANS 2017 HEATHER ANN MUSTER, MD MS
|
|
|
- Allison Parrish
- 5 years ago
- Views:
Transcription
1 CKD FOR PRIMARY CARE MINNESOTA ACADEMY OF PHYSICIANS 2017 HEATHER ANN MUSTER, MD MS

 had >50% likelihood of identifying")
 had a likelihood of < 50%, and 209 (47.")
2 PLoS One Nov 26;9(11):e Of the 445 PCPs who enrolled at least 10 patients, 19 (4.3%) had >50% likelihood of identifying patients with CKD, 217 (48.8%) had a likelihood of < 50%, and 209 (47.0%) didn t identify any of their CKD patients (had a 0% sensitivity).
3 A 45 yo AA man is referred to renal clinic for newly diagnosed CKD. Labs: BUN: 24mg/dL, Cr: 1.4 mg/dl. MDRD 55 Height 72 inches, 190 pounds. Exam was normal. Blood pressure was 129/82. UA: SG: 1025, 0 RBC s, 0 WBC s, trace protein. Pr:cr: <30 mg/g Which of the following statements is MOST CORRECT regarding his reported MDRD? It is adjusted for his BSA It isn t valid for him It represents CKD stage 3 It is based upon a non-standardized creatinine


4 Serum Creatinine: Serum Cystatin C: Age: Gender: Race: Standardized Assays: Remove body surface adjustment: mg/dl μmol/ L mg/l Years Male Female Black Other Yes No Not Sure Yes No Not Sure BSA MDRD study equation 55 ml/min/1.73m2 MDRD study equation 66 ml/min/1.73m2 MDRD study equation 80 ml/min
5 83 yo woman 155 cm tall, 41.5 kg, BMI of 17.3 diagnosed with a pathologic sternal fracture and multiple myeloma. Chemotherapy is planned. Reported labs are as follows: Cr: 1.2, BUN: 12, MDRD: 41. Which of the following statements regarding her renal function for drug dosing is MOST correct? The MDRD equation will underestimate renal function The CKD-epi equation is the most valid in this population The Cockroft-Gault equation should not be used A cystatin C is required to accurately estimate function A 24 hour urine must be performed prior to drug dosing
6 For Drug Dosing: If High risk drug, obtain measurement If unstable creatinine, no estimation equation is valid Equations less valid in extremes of size Impact of various body weights and serum creatinine concentrations on the bias and accuracy of the Cockcroft-Gault equation. Pharmacotherapy. 2012; 32(7):60 Two Novel Equations to Estimate Renal Function in persons aged 70 or older. Ann Intern Med Oct 2;157(7):
7 A 67 yo woman returns to clinic for follow-up of her DM and HTN. Routine labs are as follows: Na: 139 mmol/l, K: 3.9 mmol/l, Cl: 92 mmol/l, tco2: 22 mmol/l, BUN: 24 mg/dl, Cr: 1.3 mg/dl. CKD-Epi 39 ml/min/1.73m2. Urinalysis reveals 1-2 RBC s/hpf, 0 WBC, 0 casts. Albumin:Cr ratio: 572 mg/g. Which of the following is the appropriate CKD classification? G3aA1 G3aA2 G3bA4 G3bA3


8 Pts with CKD stage 3 in 2008, followed to % progressed to dialysis 42% died For comparison: In the general Medicare population without CKD, 22% died in the same time frame
9 A 28 yo Caucasion man presents to clinic for a DOT exam. PMH is significant only for being overweight. He takes no medications. BP: 130/76, HR: 72. He reports no significant findings on ROS. UA demonstrates a ph of 5.5, no protein, no bili, no ketones, 5-10 RBC s/hpf, 0 WBC s/hpf. BMP shows a BUN of 19 mg/dl and a Cr of 1.1 mg/dl. A repeat UA with micro 1 month later reveals a ph of 6, no protein, no bili, no ketones. 3-5 RBC s/hpf, 0 WBC s/hpf. The previous year you note he also demonstrated 5-10 RBC/s/hpf on his UA. Which of the following is the MOST appropriate next step? Order a non-contrast CT Refer to nephrology Order a urine Culture Refer to urology No further follow-up required
10 Risks for Malignancy Age >35 years Smoking history in which the risk correlates with the extent of exposure Occupational exposure to chemicals or dyes (benzenes or aromatic amines), such as printers, painters, and chemical plant workers History of gross hematuria History of chronic cystitis or irritative voiding symptoms History of pelvic irradiation History of exposure to cyclophosphamide History of a chronic indwelling foreign body History of exposure to aristolochic acid History of analgesic abuse, which is also associated with an increased incidence of carcinoma of the kidney
11 A 63 yo man with CKD G2A2 (baseline cr 1.2 mg/dl), DM X 8 years (last A1C was 7.5%), and HTN comes to clinic for a 6 month follow-up. BP is 145/86 (baseline 132/70), pulse 72. On exam nothing notable except some edema at his ankles. Labs are as follows: Na: 135 mmol/l, K: 5.3 mmol/l, tco2: 20 mmol/l, BUN: 42 mg/dl, Cr: 1.7 mg/dl UA: SG: 1.010, ketones neg, RBC s 3-5/hpf, WBC s 0, 1+ protein Alb:Cr: 2.8mg/g (1 year prior 324 mg/g) Which of the following actions is the next BEST step to address his proteinuria? Increase his insulin, follow-up in 3 months Increase his diuretic, follow up in 1 month Increase his Lisinopril, recheck labs in 2 weeks Refer to nephrology for biopsy Repeat labs in 1 week, modify meds if no change in labs
:")
12 Diabetes Care 2017 Jan; 40(1):
13 A 72 yo man with CKD G4A2 presents to clinic with complaints of SOB, orthopnea, DOE and increased LE edema. Home medications include 80 mg oral furosemide daily, Lisinopril 40 mg orally daily, carvedilol 25 mg orally twice daily, and amlodipine 10 mg orally daily. Home medications include 80 mg oral furosemide daily, Lisinopril 40 mg orally daily, carvedilol 25 mg orally twice daily, and amlodipine 10 mg orally daily. BMP: Na: 132 mmol/l, K: 5.2 mmol/l, tco2: 18 mmol/l, BUN: 56 mg/dl, Cr: 2.4 mg/dl Albumin 2.3 g/dl Assuming you now admit the patient, what is the MOST appropriate diuretic prescription? 40 mg IV furosemide 100 mg IV furosemide 2 mg IV bumetanide 40 IV furosemide plus 5 mg oral metolazone
14 Maximum Effective IV Dose (Ceiling Dose) Normal Kidney Function Moderate CKD (GFR mls/min) Severe CKD (GFR <20 mls/min) furosemide 40 mg 120 mg 200 mg bumetanide 1 mg 3 mg 10 mg torsemide 20 mg 50 mg 100 mg ethacrynic acid 100 mg???? 40 mg PO furosemide = 20 mg IV furosemide = 1 mg bumetanide (IV or PO) = 20 mg torsemide (IV or PO) = 50 mg ethacrynic acid (IV or PO) Sharp Trial: No benefit to continuous infusion. Starting dose should be times home dose - given IV. If no response in 2 hours, double dose and an administer again.
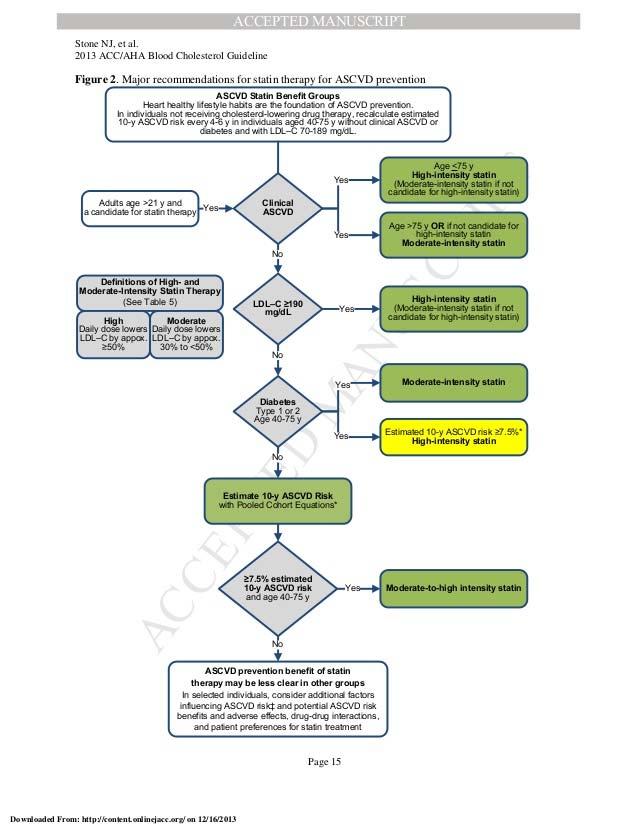
15 A 51 yo woman with HTN and CKD stage G3bA2 (CKD-Epi 44) nephropathy presents to clinic for routine follow-up. Blood pressure is controlled on Lisinopril and HCTZ and her in clinic reading is 130/72 mmhg. She takes no other medications. She does not smoke and there is no family history of cardiovascular disease. Her lipid panel is as follows: Total Cholesterol: 205 mg/dl. LDL 140 mg/dl. HDL: 42 mg/dl. (AHA/ACC CV risk prediction is 2.5% over 10 years. Which of the following statements regarding cardiovascular risk protection in her is MOST correct? She has CKD so initiate a statin LDL is >130 mg/dl so initiate a statin Her 10 yr cardiovascular risk prediction is <7.5 % so no statin is advised Her HDL is >40 mg/dl so no statin is advised
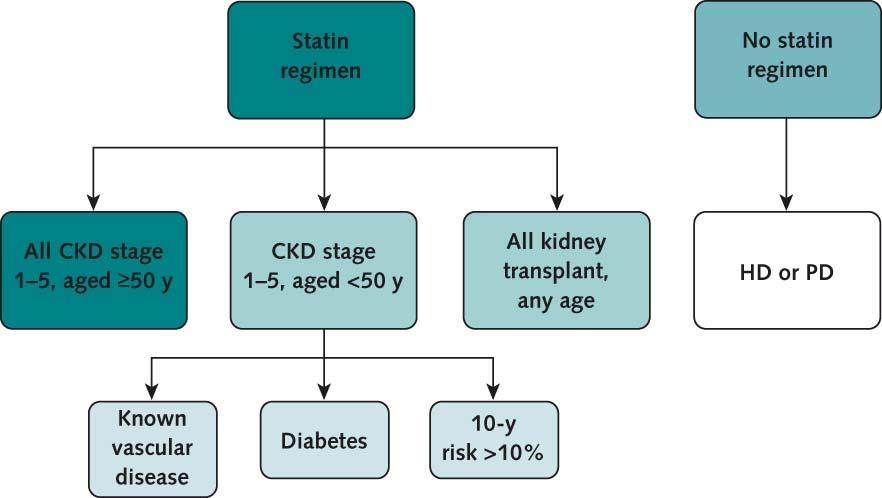
16 KDIGO Guidelines
17 A 42 yo man presents to clinic with complaints of fatigue. PMH significant G3bA1CKD secondary to ADPKD. Current egfr is 44 ml/min/1.73m2. K: 4.9 mmol/l, BUN: 55 mg/dl, Cr: 1.4. Hgb: 8 g/dl. Iron studies show: serum iron = 48 mcg/dl, ferritin = 95 ng/ml, and TIBC = 290 mg/dl TSAT: 17% Which of the following is the MOST appropriate next step? Initiate erythropoietin Initiate oral iron Obtain a bone marrow biopsy Obtain a colonoscopy
18 AJKD. 47 (5), Suppl 3; May 2006: S23 If ANEMIC, findings of iron deficiency CKD Dialysis Ferritin May be as high 500 May be as high 1000 (or higher!) TSAT <20% <20% Note that Anemia of CKD and Iron deficiency is associated with a Ferritin >100: This is different than for non CKD patients!
19 A 57 yo woman with CKD G4A2, egfr 28 ml/min/1.73m2, is seen in nephrology and is being counseled regarding kidney transplant and dialysis. As part of her evaluation, immunization status is reviewed and discussed. Which of the following statements regarding her CKD and immunizations is MOST correct? She cannot receive live vaccinations (Zoster) Hepatitis B vaccination is recommended Influenza vaccinations reduce mortality Pneumococcal vaccine is not recommended

20 CKD patients are considered immunocompromised Hepatits B Seroconversion Rate T-Cell, B-cell and macrophage function are all diminished Increased risk of infections With vaccination Decreased hospitalizations Influenza and pneumococcal Reduced risk of death Post-transplant disseminated varicella Always be preparing for potential transplant VACCINATE. EARLIER IS BETTER.
21 A 72 yo woman is seen in clinic for routine follow-up of her CKD G4A2, HTN, dyslipidemia, CAD. Today her Cr is 3.0 mg/dl, BUN is 48 mg/dl. K is 4.9 mmol/l. BP is 142/84. Lungs are clear. She has trace edema. You haven t seen her for a while as she lives an hour away and her car was in for repairs so missed her last appointment. At her last visit her Cr was 2.5 mg/dl Which of the following statements regarding dialysis and transplant is MOST correct? An AVF should be placed (HD), she is not a candidate for transplant A PD catheter should be placed and she should be referred for transplant A tunneled catheter should be placed, she should be referred for transplant She is not a candidate for dialysis or transplant and hospice should be recommended Every available renal replacement choice (home hemodialysis, center dialysis, peritoneal dialysis, transplant) is an option and all must be discussed
22 Key Points: There is NO specific disease state or age at which a Renal replacement modality is not recommended Outcomes are best when modality matches patient choice which can be dependent upon many factors. Pts should receive information, tour facilities, meet staff and patients No access can be placed until a modality has been chosen (unless and emergency) it takes ~ 3 months to mature a fistula, 6 weeks to mature a PD catheter. Tunneled access (catheter) is considered sub standard and is for emergency use only. Transplant referral should be initiated once below 20 ml/min. Patients may choose to forgo any renal replacement therapy. However, all options should still be presented as few patients have any real understanding of what dialysis is or is not (many myths out there). In those situations hospice is completely appropriate. Note: Acute, ICU dialysis chronic dialysis. They are NOT the same thing, outcomes are different and the purpose is different. Generic living wills that say No dialysis often fail to make this distinction.
23
24 A 47 yo woman presents to her clinic with complaints of headache and elevated blood pressures at home. PMH is positive only for 2 prior pregnancies and live births. She denies any new medications. BP: 165/84 mmhg. Previously 3 months ago she was 128/70. BMP: K: 5.6 mmol/l, BUN: 56 mg/dl, Cr: 3.8 mg/dl (baseline 1.0 mg/dl) Albumin 3.4 g/dl UA: SG: 1: protein, + ketones, RBC s/hpf, 3-5 WBC s/hpf, few hyaline casts Pr:Cr = 1000 mg/g Which of the following serologic tests would be MOST helpful in narrowing your differential? ANCA s Complements HIV and Hepatitis studies ANA
25 WHAT W/U WOULD BE APPROPRIATE TO DISTINGUISH THE ETIOLOGY? 1) Hematuria / RBC Casts 2) HTN 3) Renal Failure Low complements (immune complex disease) Normal complements 1) Post infectious 2) Infective Endocarditis 3) Lupus 4) Cryoglobulinemia 5) Membranoproliferative ANCA + 1) Granulomatosis with polyangitis 2) Microscopic Polyangitis 3) Churg Strauss 4) Renal limited ANCA Anti GBM + 1) Good pastures syndrome 2) Anti GBM renal disease
The future is here. It s just not widely distributed yet. William Gibson
 The future is here. It s just not widely distributed yet. William Gibson CHRONIC KIDNEY DISEASE MANAGEMENT A NEW PARADIGM Aaron Cass, MD, FRCPC Nephrologist, Fraser Health January 22, 2014 Where Are We
The future is here. It s just not widely distributed yet. William Gibson CHRONIC KIDNEY DISEASE MANAGEMENT A NEW PARADIGM Aaron Cass, MD, FRCPC Nephrologist, Fraser Health January 22, 2014 Where Are We
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Objectives. Pre-dialysis CKD: The Problem. Pre-dialysis CKD: The Problem. Objectives
 The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Section Questions Answers
 Section Questions Answers Guide to CKD Screening and Evaluation -Alec Otteman, MD Delaying Progression - Paul Drawz, MD, MHS, MS 1. Modifiable risk factors for CKD include: a. Diabetes b. Hypertension
Section Questions Answers Guide to CKD Screening and Evaluation -Alec Otteman, MD Delaying Progression - Paul Drawz, MD, MHS, MS 1. Modifiable risk factors for CKD include: a. Diabetes b. Hypertension
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6
 Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL. Revised May 30, 2012
 CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe III, MD Revised May 30, 2012 The information contained in this protocol
CONCORD INTERNAL MEDICINE CHRONIC KIDNEY DISEASE PROTOCOL Douglas G. Kelling, Jr., MD C. Gismondi-Eagan, MD, FACP George C. Monroe III, MD Revised May 30, 2012 The information contained in this protocol
11/9/2015. Childhood Nephrotic Syndrome: The Clinical Pathway. Learning Objectives. Nephrotic Syndrome - Definition. Proteinuria.
 Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Cardiovascular Pharmacotherapy in Special Population: Cardio-Nephrology
 49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, Jeffrey P. Harris MD, FACP
 8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, 2008 The Internist and the Pre-End Stage Renal Disease Patient Jeffrey P. Harris MD, FACP Country: Bangladesh Population:
8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, 2008 The Internist and the Pre-End Stage Renal Disease Patient Jeffrey P. Harris MD, FACP Country: Bangladesh Population:
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Disclosures. Outline. Outline 7/27/2017 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Disclosures. Outline. Outline 5/23/17 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Acknowledgements. National Kidney Foundation of Connecticut Mark Perazella. Co-PI Slowing the progression of chronic kidney disease to ESRD
 A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006
 PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE CORRECTIONS
PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE CORRECTIONS
Updates in Chronic Kidney Disease Management. Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG
 Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
KEEP 2.0 Annual Data Report Chapter Five
 KEEP 2. Annual Data Report Chapter Five Figure 5.1 percent distribution of KEEP participants with elevated serum creatinine levels, overall & by age 16 Percent of participants 12 8 4 All
KEEP 2. Annual Data Report Chapter Five Figure 5.1 percent distribution of KEEP participants with elevated serum creatinine levels, overall & by age 16 Percent of participants 12 8 4 All
Chronic Kidney Disease: Optimal and Coordinated Management
 Chronic Kidney Disease: Optimal and Coordinated Management Michael Copland, MD, FRCPC Presented at University of British Columbia s 42nd Annual Post Graduate Review in Family Medicine Conference, Vancouver,
Chronic Kidney Disease: Optimal and Coordinated Management Michael Copland, MD, FRCPC Presented at University of British Columbia s 42nd Annual Post Graduate Review in Family Medicine Conference, Vancouver,
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006
 CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006") IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality
 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality Shannon H. Norris, BSN, RN June 6, 2018 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality DISCUSSION: End Stage
Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality Shannon H. Norris, BSN, RN June 6, 2018 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality DISCUSSION: End Stage
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Chapter Five Clinical indicators & preventive health
 Chapter Five Clinical indicators & preventive health The painter who draws merely by practice and by eye, without any reason, is like a mirror which copies every thing placed in front of it without being
Chapter Five Clinical indicators & preventive health The painter who draws merely by practice and by eye, without any reason, is like a mirror which copies every thing placed in front of it without being
Topic: Chronic Heart Failure Cases for Monday s March 21th lecture.
 1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
1 Phar6122: CV section Date: 3/10/05 Topic: Chronic Heart Failure Cases for Monday s March 21th lecture. Directions: This handout includes three chronic heart failure cases of increasing difficulty. In
Chronic Kidney Disease
 Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Slide #1 Case Presentation: Kidney Disease
 Slide #1 Case Presentation: Kidney Disease Christina Wyatt, MD Mount Sinai, New York Slide #2 Disclosures Investigator-initiated research support Gilead Sciences Honoraria for internal education Bristol
Slide #1 Case Presentation: Kidney Disease Christina Wyatt, MD Mount Sinai, New York Slide #2 Disclosures Investigator-initiated research support Gilead Sciences Honoraria for internal education Bristol
Lab Values Explained. working at full strength. Other possible causes of an elevated BUN include dehydration and heart failure.
 Patient Education Lab Values Explained Common Tests to Help Diagnose Kidney Disease Lab work, urine samples and other tests may be given as you undergo diagnosis and treatment for renal failure. The test
Patient Education Lab Values Explained Common Tests to Help Diagnose Kidney Disease Lab work, urine samples and other tests may be given as you undergo diagnosis and treatment for renal failure. The test
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Elevation of Serum Creatinine: When to Screen, When to Refer. Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC
 Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Identifying and Managing Chronic Kidney Disease: A Practical Approach
 Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Identifying and Managing Chronic Kidney Disease: A Practical Approach S. Neil Finkle, MD, FRCPC Associate Professor Division of Nephrology, Department of Medicine, Dalhousie University Program Director,
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Faculty/Presenter Disclosure
 CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
Applying clinical guidelines treating and managing CKD
 Applying clinical guidelines treating and managing CKD Develop patient treatment plan according to level of severity. Source: Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012
Applying clinical guidelines treating and managing CKD Develop patient treatment plan according to level of severity. Source: Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012
Renal Remission Clinic Protocols
 Renal Remission Clinic Protocols Bremerton WA, USA Version 1.2 Issued November 5, 2009 Update January 11, 2011* *Updated items appear in red Please Read This First The protocols represent ever changing
Renal Remission Clinic Protocols Bremerton WA, USA Version 1.2 Issued November 5, 2009 Update January 11, 2011* *Updated items appear in red Please Read This First The protocols represent ever changing
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Narender Goel et al. Middletown Medical PC, Montefiore Medical Center & Albert Einstein College of Medicine, New York
 Narender Goel et al. Middletown Medical PC, Montefiore Medical Center & Albert Einstein College of Medicine, New York 4th International Conference on Nephrology & Therapeutics September 14, 2015 Baltimore,
Narender Goel et al. Middletown Medical PC, Montefiore Medical Center & Albert Einstein College of Medicine, New York 4th International Conference on Nephrology & Therapeutics September 14, 2015 Baltimore,
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES
 RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
Professor Suetonia Palmer
 Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Final Case Study: Renal Disease Due 3/19/14 60 points
 NUT 116BL Name: CHRISTINE WOO Winter 2014 Section: 1 Final Case Study: Renal Disease Due 3/19/14 60 points Part I: Initial Presentation Present Illness: Jenny is a 19 yo F student referred to the renal
NUT 116BL Name: CHRISTINE WOO Winter 2014 Section: 1 Final Case Study: Renal Disease Due 3/19/14 60 points Part I: Initial Presentation Present Illness: Jenny is a 19 yo F student referred to the renal
Screen annually for patients with any of the following risk factors:
 CASE DEFINITION Chronic Kidney Disease (CKD) is either of the following, persisting for at least three months, repeated on at least two occasions: 1. Markers of kidney damage (e.g. proteinuria, haematuria
CASE DEFINITION Chronic Kidney Disease (CKD) is either of the following, persisting for at least three months, repeated on at least two occasions: 1. Markers of kidney damage (e.g. proteinuria, haematuria
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
i. Where is the participant seen?
 PFU01 method used: Phone/in-person interview 1 Enter PIP # here: Online survey 2 Enter Web # here: Initials of person completing form: Date Form Completed: / / Form Version: 03 / 01 / 18 Is the participant
PFU01 method used: Phone/in-person interview 1 Enter PIP # here: Online survey 2 Enter Web # here: Initials of person completing form: Date Form Completed: / / Form Version: 03 / 01 / 18 Is the participant
What should you do next? Presenter Disclosure Information. Learning Objectives. Case: George
 2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
2:45 3:45pm Optimizing the Management of Patients with Chronic Kidney Disease SPEAKER Jay B. Wish, MD, FACP Presenter Disclosure Information The following relationships exist related to this presentation:
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Case 1. Case 2. What do you think about reducing or discontinuing some of the above now that his LVEF has normalized?
 Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Case 1 A primary care colleague inquires what to do with a patient (HFrEF in NSR) who has a digoxin level of 2.8ng/ml. Level was obtained at 10am, patient takes all medications at one time upon arising
Manitoba Primary Care Quality Indicators Full Guide Version 3.0 Quick Reference Summary
 PREVENTION 2.01 Cervical Cancer 2.02 Colon Cancer 2.03 Breast Cancer 2.04 Dyslipidemia for Women 2.05 Dyslipidemia for Men Female 21-69 PAP 36 Percentage of female enrolled patients 21 to 69 years of age
PREVENTION 2.01 Cervical Cancer 2.02 Colon Cancer 2.03 Breast Cancer 2.04 Dyslipidemia for Women 2.05 Dyslipidemia for Men Female 21-69 PAP 36 Percentage of female enrolled patients 21 to 69 years of age
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Section 1: 1: Trends. Section 2: 2: Comparisons to to Overall Portland Area Area Results for for
 Section 1: 1: Trends 1 Patients in the Diabetes Register 2 Gender of Patients with Diabetes 2 Age of Patients with Diabetes 3 Diabetes Type 3 Duration of Diabetes 4 Weight Control 5 Hemoglobin A1c 6 Blood
Section 1: 1: Trends 1 Patients in the Diabetes Register 2 Gender of Patients with Diabetes 2 Age of Patients with Diabetes 3 Diabetes Type 3 Duration of Diabetes 4 Weight Control 5 Hemoglobin A1c 6 Blood
Session 9: Optimizing the Management of Patients with Chronic Kidney Disease Learning Objectives
 Session 9: Optimizing the Management of Patients with Chronic Kidney Disease Learning Objectives 1. Understand the impact of chronic kidney disease (CKD) as a common condition of the adult US population.
Session 9: Optimizing the Management of Patients with Chronic Kidney Disease Learning Objectives 1. Understand the impact of chronic kidney disease (CKD) as a common condition of the adult US population.
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Creatinine & egfr A Clinical Perspective. Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC
 Creatinine & egfr A Clinical Perspective Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC CLINICAL CONDITIONS WHERE ASSESSMENT OF GFR IS IMPORTANT Stevens et al. J Am Soc Nephrol 20: 2305
Creatinine & egfr A Clinical Perspective Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC CLINICAL CONDITIONS WHERE ASSESSMENT OF GFR IS IMPORTANT Stevens et al. J Am Soc Nephrol 20: 2305
Case #1. Current Management Strategies in Chronic Kidney Disease. Serum creatinine cont. Pitfalls of Serum Cr
 Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
Current Management Strategies in Chronic Kidney Disease Grace Lin, MD Assistant Professor of Medicine, University of California San Francisco Case #1 50 y.o. 70 kg man with long-standing hypertension is
CKD and CVD. Jamal Salameh, MD, FACP, FASN First Coast Nephrology
 CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
CKD and CVD Jamal Salameh, MD, FACP, FASN First Coast Nephrology An Epidemic of Kidney Disease Prevalence CKD stages 1-4 10% 1988-94 13% 1999-2004 Coresh, JAMA 298:2038, 2007 Stage 5: GFR
Transforming Diabetes Care
 Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
S150 KEEP Analytical Methods. American Journal of Kidney Diseases, Vol 55, No 3, Suppl 2, 2010:pp S150-S153
 S150 KEEP 2009 Analytical Methods American Journal of Kidney Diseases, Vol 55, No 3, Suppl 2, 2010:pp S150-S153 S151 The Kidney Early Evaluation program (KEEP) is a free, communitybased health screening
S150 KEEP 2009 Analytical Methods American Journal of Kidney Diseases, Vol 55, No 3, Suppl 2, 2010:pp S150-S153 S151 The Kidney Early Evaluation program (KEEP) is a free, communitybased health screening
NATIONAL QUALITY FORUM Renal EM Submitted Measures
 NATIONAL QUALITY FORUM Renal EM Submitted Measures Measure ID/ Title Measure Description Measure Steward Topic Area #1662 Percentage of patients aged 18 years and older with a diagnosis of CKD ACE/ARB
NATIONAL QUALITY FORUM Renal EM Submitted Measures Measure ID/ Title Measure Description Measure Steward Topic Area #1662 Percentage of patients aged 18 years and older with a diagnosis of CKD ACE/ARB
MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY
 MHD I, Session VIII, Student Copy Page 1 MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY MHD I, Session VIII, Student Copy Page 2 Case #1 Chief Complaint: I have been feeling just lousy
MHD I, Session VIII, Student Copy Page 1 MHD I Session VIII Renal Disease November 6, 2013 STUDENT COPY MHD I, Session VIII, Student Copy Page 2 Case #1 Chief Complaint: I have been feeling just lousy
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Analytical Methods: the Kidney Early Evaluation Program (KEEP) The Kidney Early Evaluation program (KEEP) is a free, community based health
 The Kidney Early Evaluation program (KEEP) is a free, community based health") Analytical Methods: the Kidney Early Evaluation Program (KEEP) 2000 2006 Database Design and Study Participants The Kidney Early Evaluation program (KEEP) is a free, community based health screening program
Analytical Methods: the Kidney Early Evaluation Program (KEEP) 2000 2006 Database Design and Study Participants The Kidney Early Evaluation program (KEEP) is a free, community based health screening program
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Concept and General Objectives of the Conference: Prognosis Matters. Andrew S. Levey, MD Tufts Medical Center Boston, MA
 Concept and General Objectives of the Conference: Prognosis Matters Andrew S. Levey, MD Tufts Medical Center Boston, MA General Objectives Topics to discuss What are the key outcomes of CKD? What progress
Concept and General Objectives of the Conference: Prognosis Matters Andrew S. Levey, MD Tufts Medical Center Boston, MA General Objectives Topics to discuss What are the key outcomes of CKD? What progress
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Primary Care Physicians and Clinicians. XXX on behalf of the Upper Midwest Fistula First Coalition. Chronic Kidney Disease (CKD) Resources
 Resources") August 10, 2007 To: From: RE: Primary Care Physicians and Clinicians XXX on behalf of the Upper Midwest Fistula First Coalition Chronic Kidney Disease (CKD) Resources Caring for patients with chronic kidney
August 10, 2007 To: From: RE: Primary Care Physicians and Clinicians XXX on behalf of the Upper Midwest Fistula First Coalition Chronic Kidney Disease (CKD) Resources Caring for patients with chronic kidney
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Renal Failure Update in Treatment Part 1. DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602)
") Renal Failure Update in Treatment Part 1 DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602) 263 5446 dwalton@akdhc.com DISCLOSURES NONE OFF LABEL USE POSSIBLY LEARNING OBJECTIVES USE
Renal Failure Update in Treatment Part 1 DANIEL WALTON, DO, FACP,FACOI,FASN PARTNER, AKDHC, LLC PHOENIX AZ (602) 263 5446 dwalton@akdhc.com DISCLOSURES NONE OFF LABEL USE POSSIBLY LEARNING OBJECTIVES USE
Outpatient Management of Chronic Kidney Disease for the Internist
 Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Status of the CKD and ESRD treatment: Growth, Care, Disparities
 Status of the CKD and ESRD treatment: Growth, Care, Disparities United States Renal Data System Coordinating Center An J. Collins, MD FACP Director USRDS Coordinating Center Robert Foley, MB Co-investigator
Status of the CKD and ESRD treatment: Growth, Care, Disparities United States Renal Data System Coordinating Center An J. Collins, MD FACP Director USRDS Coordinating Center Robert Foley, MB Co-investigator
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree
 and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree") Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
CKD IN THE CLINIC. Session Content. Recommendations for commonly used medications in CKD. CKD screening and referral
 CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
Section 1: 1: Trends. Section 2: 2: Comparisons to to Overall Portland Area Area Results for for
 Section 1: 1: Trends 2 Patients in the Diabetes Register 3 Diabetes Type 3 Gender of Patients with Diabetes 4 Age of Patients with Diabetes 4 Duration of Diabetes 5 Weight Control 6 Hemoglobin A1c 7 Blood
Section 1: 1: Trends 2 Patients in the Diabetes Register 3 Diabetes Type 3 Gender of Patients with Diabetes 4 Age of Patients with Diabetes 4 Duration of Diabetes 5 Weight Control 6 Hemoglobin A1c 7 Blood
Disclosures. CKD/ESRD care among vulnerable populations. Objectives. Case: Ms. S 3/12/2016. Delphine Tuot, MDCM, MAS Assistant Professor of Medicine
 Disclosures CKD/ESRD care among vulnerable populations I have nothing to disclose Delphine Tuot, MDCM, MAS Assistant Professor of Medicine Objectives Recognize disparities related to kidney health Learn
Disclosures CKD/ESRD care among vulnerable populations I have nothing to disclose Delphine Tuot, MDCM, MAS Assistant Professor of Medicine Objectives Recognize disparities related to kidney health Learn
Renal function vs chemotherapy dosing
 Renal function vs chemotherapy dosing Jenny Casanova Senior Clinical Pharmacist Repatriation General Hospital Daw Park 1 Methods of estimating renal function Cockcroft-Gault (1976) C-G using ideal vs actual
Renal function vs chemotherapy dosing Jenny Casanova Senior Clinical Pharmacist Repatriation General Hospital Daw Park 1 Methods of estimating renal function Cockcroft-Gault (1976) C-G using ideal vs actual
ANEMIA & HEMODIALYSIS
 ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
A New Approach for Evaluating Renal Function and Predicting Risk. William McClellan, MD, MPH Emory University Atlanta
 A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function