Inpatient Diabetes and Hyperglycaemia. Philip Dyer Heart of England NHS Foundation Trust Birmingham
|
|
|
- Juniper Arnold
- 5 years ago
- Views:
Transcription



1 Inpatient Diabetes and Hyperglycaemia Philip Dyer Heart of England NHS Foundation Trust Birmingham
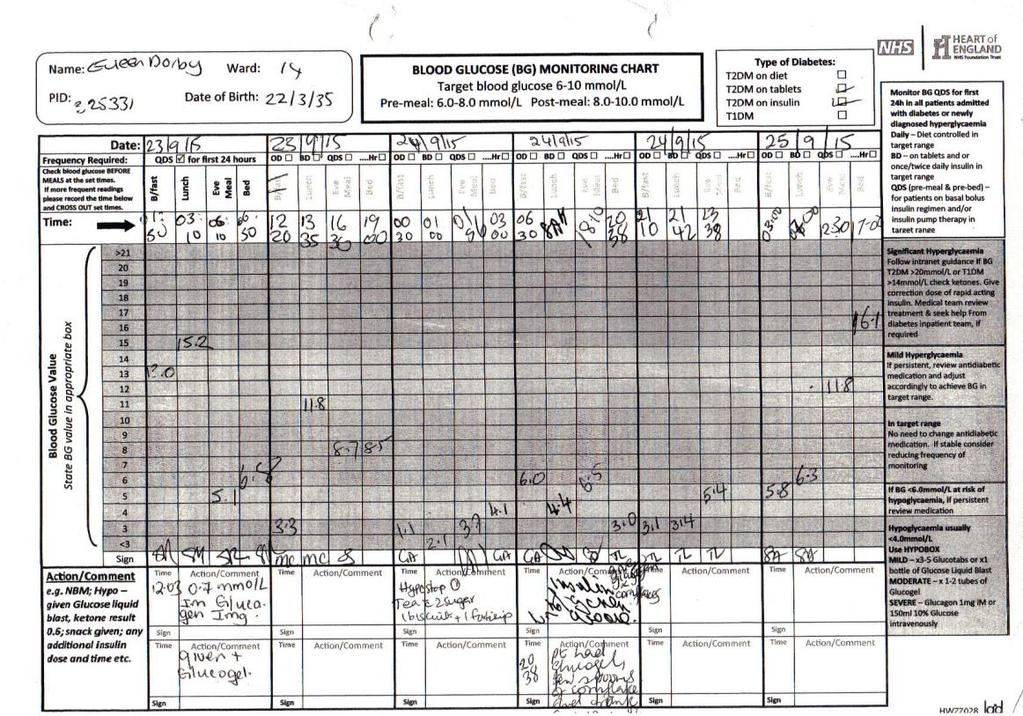
2 A Case of Inpatient Diabetes Mrs DE Ketosis-prone T2DM on bd Humulin-I, Metformin and Linagliptin Admitted with a fall 19:00h nursing note - patient declined most of her evening meal :00h Dr called to review CBG 1.1 mmol/l FY1 note given IM Glucagon, ½ Glucogel and 100mL 10% Glucose - CBG 13.0 mmol/l Stop IV Glucose and monitor CBG hourly :00h JD WR Events overnight noted very low BGs, BGs and. Having frequent hypos. Earlier in the week agreed to sheltered accommodation. No recollection of this. Plan reduce Humulin-I by 4 units Speak to Diabetes consultant Arrange best interest meeting
3 :30h Nursing note - CBG 3.0 mmol/l A Case of Inpatient Diabetes Given Glucogel, cup of tea and 2 biscuits Recheck CBG 5.0 mmol/l :00h JD WR Applying for guardianship BGs high on admission may have not been taking Metformin and Linagliptin HbA1c between % since 2013 Note severe hypo on Not had insulin since the HbA1c (%) eag (mmol/l) Plan stop insulin, PRN Novorapid if required, target HbA1c 9-10% comfortably as all we need to do is limit hyperosmolar symptoms and stop dangerous hypos.
4
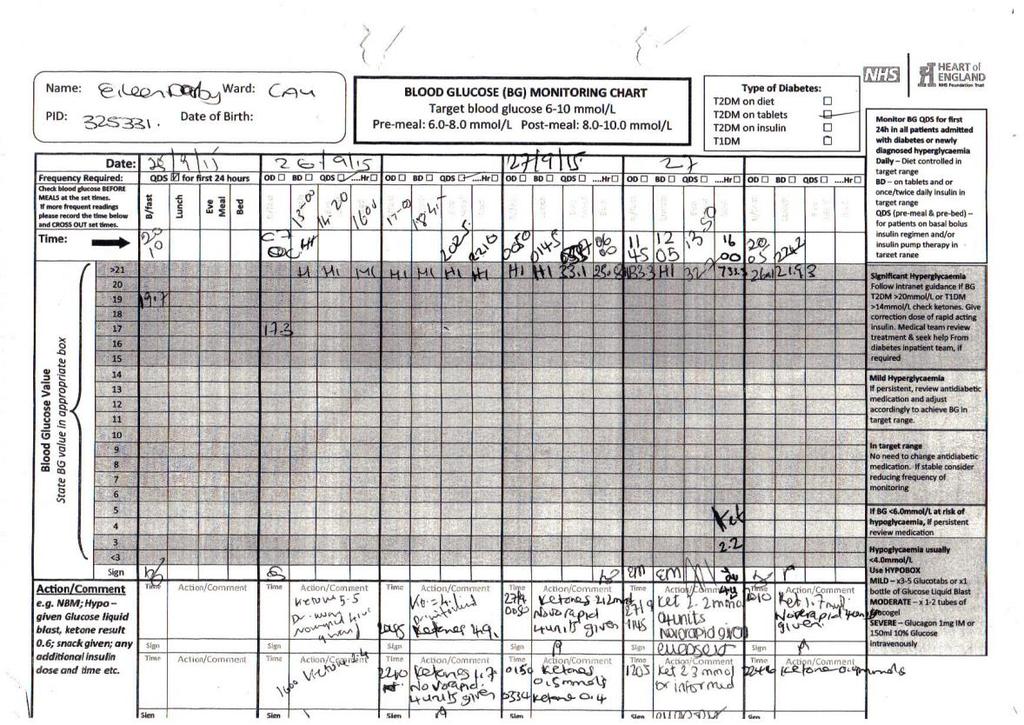
5 A Case of Inpatient Diabetes :10h Nursing note - BGs Hi, ketones 6.0 mmol/l SHO advice 4 units Novorapid 13:30h BGs - Hi, ketones 5.5 mmol/l 16:00h FY2 review Repeat ketones now 2.6 mmol/l Patient had been drinking Lucozade which caused the spike Plan due to receive Metformin Repeat CBG at 1830h Give 5 units Novorapid for one off high BGs Ketones though high responded to Novorapid and with her present state and non-compliance I see it not with starting on sliding scale 22:00h FY1 review Currently BG unrecordable and ketones 1.7 mmol/l Plan repeat Novorapid 4 units and recheck ketones, please contact if >0.6 mmol/l
6 A Case of Inpatient Diabetes (continued) Consultant WR CBGs was 33 over the weekend. Had 3 bottles of Lucozade. CBG coming down. Patients looks well. Plan await court of protection and continue current treatment of Novomix (meant Novorapid) :00h DADOT review AMT4 = 0, Attention obviously altered, very drowsy but rousable. Acute event is evident 4AT = 8, Delirium is evident :15h Nursing note Appears to be getting more confused BGs 33.1 mmol/l and ketones 7.1 mmol/l Dr informed Actrapid 4 units given For IV sliding scale 14:00h CT1 note Patient vomiting O/E MEWS = 2 and mild epigastric tenderness Imp DKA
7
8 Mrs DE Glycaemic Control during her Admission
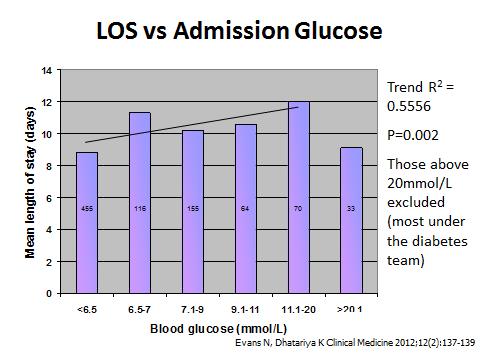
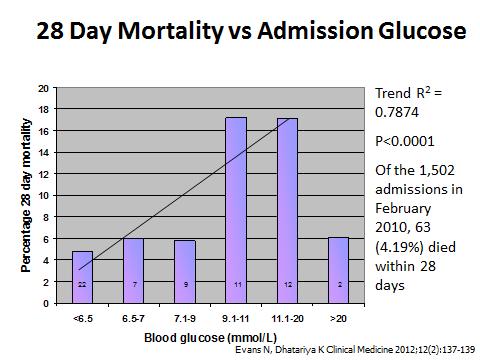
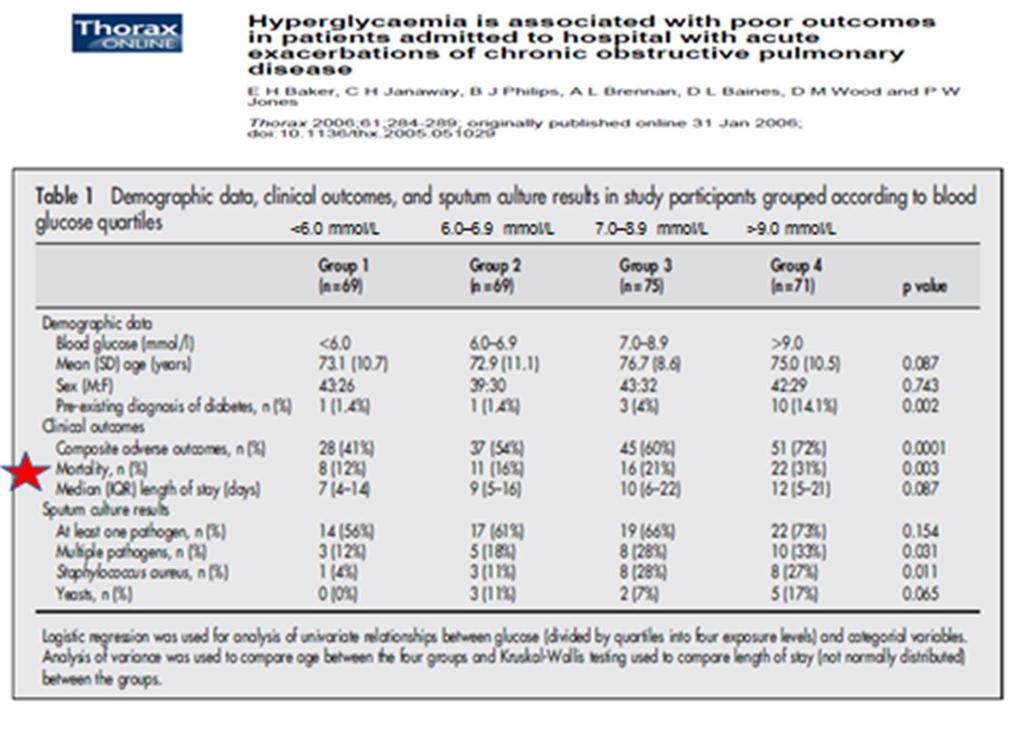
9 Does Glycaemic Control Matter? Hyperglycaemia is important
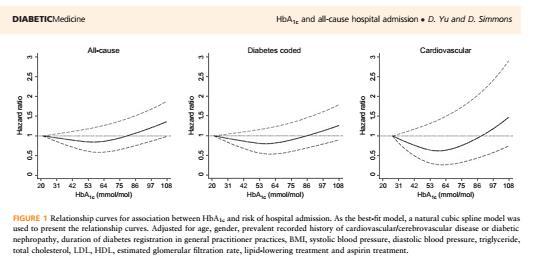
10

11
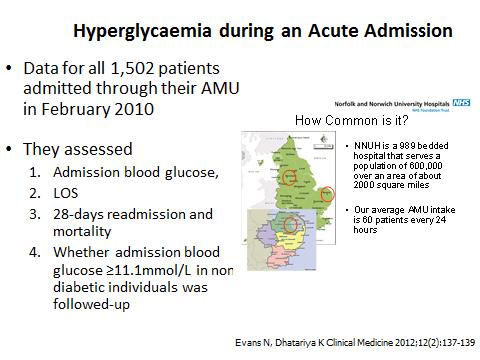

12

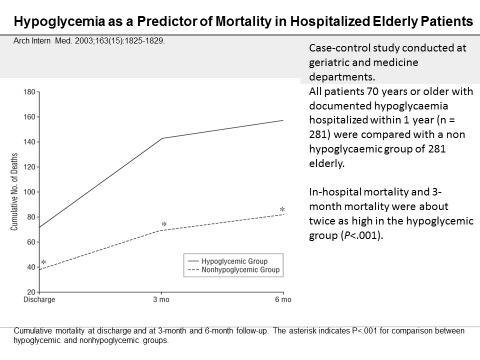
13 Does Glycaemic Control Matter? Hypoglycaemia is important
14

15 Summary of hypothetical relationship(s) between hyperglycaemia and adverse outcomes in patients with ACS and posited mechanisms of the beneficial effects of insulin. Intravenous Insulin Christina H. Wei, and Sheldon E. Litwin Diabetes 2014;63:


16 Update on Mrs DE Admitted 6 weeks later with AMI

17 What should the inpatient blood glucose target be?
18
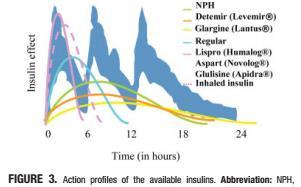
19 Insulin Secretion The Basal Bolus Concept Insulin Component Basal Bolus Properties Near-constant insulin level throughout the day Suppresses hepatic glucose production (glycogenolysis and gluconeogesis), proteolysis and lipolysis. Insulin requirement to suppress hepatic glucose production overnight and between meals. Covers ~50% of the total daily insulin requirement Reflects BG overnight, before breakfast and before meals if there is a 5- hour gap. Immediate rise and sharp peak at 1-hour Limits post-meal hyperglycemia Insulin requirement to maintain normal glucose disposal after eating Cover ~50% of the total daily insulin requirement (10-20% at each meal) Reflects BG 2-hours after meals
20

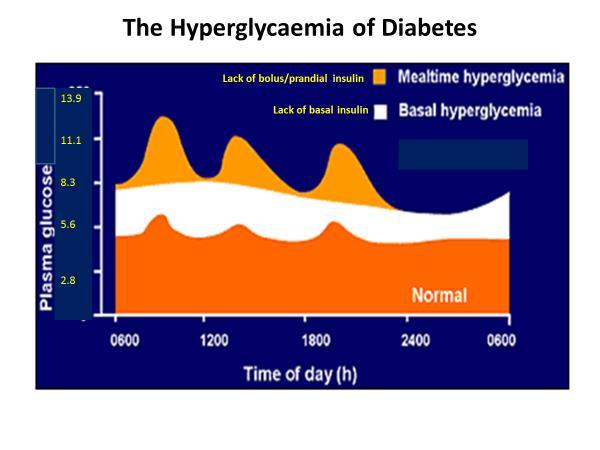
21 Bolus/prandial insulin is necessary for maintaining blood glucose control, after food (prevents post prandial hyperglycaemia). Therefore basal insulin is continuous insulin secreted between meals and bolus/prandial insulin is secreted in burst in response to eating. How would we manage without basal insulin? Because the liver is secreting glucose into the bloodstream continuously, a complete lack of insulin, would result in a sharp rise in blood glucose level (2.5 mmol/l/h). Without basal insulin, cells would resort to burning only fat for energy, and produce ketones. Continuous insulin = basal insulin and switches off ketogenesis and ensures cells get energy between meals. How would we manage without bolus/prandial insulin? Without bolus/prandial insulin, we are unable to control post prandial glucose.
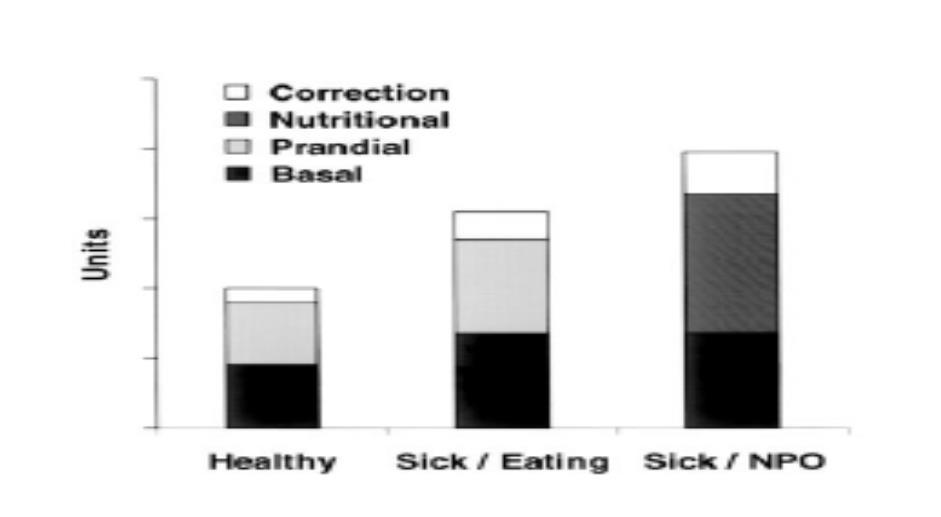
22 Insulin Requirement When Unwell
23 Insulin Regimes for Hospital TYPE OF INSULIN Name What is it Indications Starting TDD Dose BACKGROUND/BASAL INSULIN Glargine (Lantus) Levemir (Detemir) Insulatard or Humulin-I Consists of a long-acting insulin preparation administered regardless of the patient s oral intake status, with the premise of matching hepatic (endogenous) glucose production Not controlled on oral multiple anti-diabetic agents. Course of treatment for specific indication e.g. starting steroids, oral antidiabetic agents suspended. 0.3 units/kg E.g. 80 kg = 0.3 x 80 = 24 units. PRANDIAL/BOLUS INSULIN BASAL BOLUS REGIME PRE-MIXED TWICE DAILY INSULIN Novorapid Combination of basal Novomix 30 Humalog insulin and rapid acting Humalog Mix 50 Glulisine analogue insulin. Humalog Mix 25 Rapid-acting Long-acting basal insulin Pre-mixed analogue insulin administered regardless combination of preparation given to of the patient s oral intermediate acting cover nutritional intake status and rapidacting and rapid acting needs. analogue insulin analogue insulin. preparation given to cover nutritional needs. In combination with basal insulin e.g. basal plus or basal bolus. 0.1 units/kg E.g. 80 kg = 0.1 x 80 = 8 units For tight glycaemic control and flexible regime. 0.5 units/kg E.g. 80 kg = 0.5 x 80 = 40 units. Basal = 50% Bolus =50% Basal = 20 units Bolus = 7 units tds Poor glycaemic control on anti-diabetic agents or basal insulin only not wanting four injections. 0.5 units/kg E.g. 80 kg = 0.5 x 80 = 40 units SUPPLEMENTAL OR CORRECTION INSULIN Novorapid Humalog Glulisine Rapid-acting analogue insulin To correct capillary blood glucose (CBGs) values that exceed predetermined targets. T1DM 1 unit to lower CBG by 2.0 mmol/l T2DM 0.1 unit/kg Consider lower dose in frail elderly, CKD stage 4/5 e.g. 0.2 units/kg for basal insulin and higher doses in obese, on steroids or HbA1c >9.0% (75 mmol/mol) e.g. 0.6 units/kg for pre-mixed insulin.
24 Insulin Regimes for Hospital TYPE OF INSULIN BACKGROUND/BASAL INSULIN PRANDIAL/BOLUS INSULIN BASAL BOLUS REGIME PRE-MIXED TWICE DAILY INSULIN SUPPLEMENTAL OR CORRECTION INSULIN Do you continue when not eating What percentage of the TDD to give when not eating What do when unwell Monitoring required to adjust insulin dose Yes, may require a reduced dose No, as patient is not eating Yes, but at 50% of the TDD OR convert to basal insulin only at 50% of their TDD 100% of the TDD None 100% of the basal 50% Variable Basal insulin requirement may remain constant or often increase. Pre-breakfast (fasting) and pre-evening meal CBG. Depending on whether the patient is eating or not the bolus insulin requirement may increase or decrease 2-hours post meal BG Same as for basal and prandial insulin. Pre-mixed doses may need to increase Pre-breakfast (fasting) and pre-evening meal BG.. Used only to correct CBGs which are above target. Correction doses of insulin may be required to maintain good glycaemic control. If repeated correction doses are required the current regime should be reviewed, probably requiring an increase. Variable
25 Commence New Antidiabetic Medication. When CBG<12.0mmol/L start: 1. Basal Bolus Insulin for T1DM or ketosis prone T2DM - Total daily dose (TDD) units/kg 2. Basal Only Insulinfor T2DMs on 3 different tablets or 1 or 2 tablets and CBG 14.0mmol/L. - TDD units/kg. Continue all the tablets. 3. Premixed Additional Twice new daily class Insulin of antidiabetic 0.5 units/kg. tablet Continue if 1 Metformin 2 tablets stop and all CBG<14.0 other tablets. mmol/l(page 1.) Basal Bolus Regime Rapid acting insulinse.g.humalog or Novorapid Long acting Insulinse.g. Lantus orlevemir For Basal Only Regime Long acting Insulinse.g.Lantus, Levemir or Insulatard Starting Insulin Give 50% of total dose with evening meal in the form of long acting insulin and divide the remaining dose equally with meals for rapid acting insulin Meal Breakfast Lunch Evening Bedtime Rapid acting 6 units 6units 6 units Long acting 18 units Give 50% of total dose with evening meal in the form of long acting insulin and divide the remaining dose equally with meals for rapid acting insulin Meal Breakfast Lunch Evening Bedtime Lantus 22units Levemir 22 units Insulatard 11 units 11 units E.g. Weight 72 Kg, starting total daily dose (TDD) 0.5 x 72 = 36 units. E.g. Weight 72 Kg, starting total daily dose (TDD) 0.3 x 72 = 22 units. NOTE: Pre-mixed BASAL Insulin INSULIN MUST BE GIVEN MealPRIOR TO Breakfast DISCHARGE OTHERWISE Lunch AFTER 4 HOURS Evening THE PATIENT Bedtime WILL NOT HAVE ANY INSULIN ON BOARD AS THE RAPID ACTING INSULIN WOULD HAVE RUN OUT. Novomix 30/Humalog 24 units 12 units Mix 25/Humalog Mix 25 CRITERIA FOR DISCHARGE All are necessary for a safe discharge 1. Able to monitor& record CBG independently 5. Capillary Ketones <0.6 mmol/l 2. Able to administer insulin independently 6.CBG 10.0 mmol/l 3. Access to a telephone Able to attend a follow up appointment in the Diabetes Centre x42034 Fax E.g. Weight 72kg, starting TDD 0.5 x 72 = 36 units
26 What to do if the patient is not eating? Mrs A is a type 1 diabetic on a basal bolus regime Breakfast Lunch Evening Meal Bed Humalog Glargine 30 He presents with symptoms consist with pyelonephritis fever, loin pain, dysuria and a urine dipstick positive for leucocytes and nitrites. Investigations - WCC 24.7, CRP 212 and CBG 8.4 mmol/l. He is feeling nauseous and does not feel like eating What do you do to control his BG? Answer - Continue Glargine and suspend Humalog while not eating Breakfast Lunch Evening Meal Bed Humalog Glargine 30 Mr C is a type 2 diabetic on a premixed bd insulin regime Breakfast Lunch Evening Meal Bed Novomix He presents with diarrhoea. He is fluid resuscitated and started on replacement and with 0.9% NaCl with KCl. CBG is 6.4 mmol/l and capillary ketones 0.1. He does not feel like eating What should be done with his insulin regime to control his BG? Continue current regime at 50% of the usual dose Breakfast Lunch Evening Meal Bed Novomix


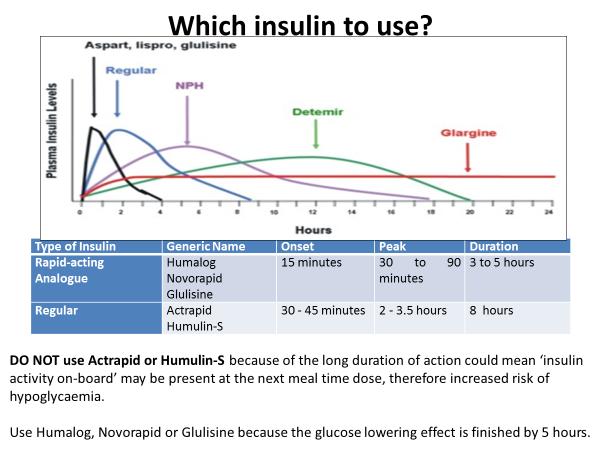
27 How to give a Correction Dose

28 How to Calculate the dose and When to Recheck CBG? Type 1 Diabetes* Assume that 1 unit will drop capillary blood glucose (CBG) by 2.0 mmol/l, to a maximum dose of 10 units initially. Aim to correct to 8.0 mmol/l E.g. if CBG was 28.0 mmol/l, = 20.0, = 10, therefore give 10 units. Type 2 Diabetes* Give 0.1 units/kg of insulin to a maximum dose of 10 units initially. Example 100 kg patient = 100 x 0.1 = 10 units *Wherever possible take advice from the patient about the amount of insulin normally required to correct a high blood glucose (Correction or Insulin Sensitivity Factor) 1st check - 2-hours At peak effect. Is it coming down? 2 nd check - 4-hours Glucose lowering effect almost complete. Decision on further Rx reqd


29 How to Manage Inpatient Diabetes and Hyperglycaemia
30 Now for some cases!!
31 Case 1 Self referral to ED. 54 year old Asian male with T2DM. Presented with hyperglycaemia. On examination she was afebrile, pulse 82 regular, BP 134/76, RS clinically clear, weight 85 kg. Current Regime Breakfast Lunch Evening meal Bedtime Metformin 1g 1g Gliclazide 80mg 80mg Sitagliptin 100mg The laboratory data showed: Na+ 138 mmol/l ( ) WCC 5.4 ( ) K+ 4.9 mmol/l ( ) Hb 155 ( ) Urea 8.6 mmol/l ( ) Plts 300 ( ) Cr 88 mmol/l (60 110) CRP 12 (<10mg/dL) Capillary blood glucose 18.4 mmol/l Capillary ketones 0.4 mmol/l (<0.6) HbA1c 9.4% (79 mmol/mol) What is the diagnosis? Hyperglycaemia
32 How would you manage Case 1? 1. Correction dose of rapid acting insulin such as Humalog. 0.1 unit/kg 85 x 0.1 = 8.5, therefore give 8.0 units 2. Start basal insulin - Humulin-I 0.3 units/kg = 0.8 x 85 = 25.5, therefore 26 units Breakfast Lunch Evening meal Bedtime Humulin-I 13 units 13 units 3. Recheck CBG and ketones in 2 hours - If CBG <12.0 mmol/l and capillary ketones < 0.6 mmol/l, the patient can be discharged. - If CBG >12.0 mmol/l give a 2 nd correction dose and repeat CBG and capillary ketones in 2 hours. Criteria for discharge, same as above. 4. Give ml of Hartmanns over 2 hours to correct the dehydration and help lower CBG 5. Continue all their other oral anti-diabetic medications 6. Contact Inpatient Diabetes Team to organise education on insulin administration, CBG monitoring and the treatment of hypoglycaemia.
33 Case 2 A 19-year-old single diabetic Caucasian woman had been on 22 units of Lantus and 8 units of Novorapid before meals daily for six years. She presented at the ED with nausea and malaise of a 1 day duration. Polyuria, polydipsia and altered CBG values had been present for approximately one month, but were overlooked by the patient. The laboratory data showed: Na+ 134 mmol/l ( ) K+ 4.7 mmol/l ( ) Urea 7.2 mmol/l ( ) Cr 72 mmol/l (60 110) Capillary blood glucose 22.4mmol/L Capillary ketones 2.1 mmol/l (<0.6) Venous Gas ph 7.35 ( ) HCO (24-28) K+ 4.7 ( ) Cl 104 (95-105) Lactate 0.9 mmol/l ( ) Anion gap 8 (8-12) What is the diagnosis?
34 Management of Mild DKA with Subcutaneous Rapid Acting Insulin Management of DKA with Subcutaneous Rapid Acting Insulin Indications - Patients with mild ketosis and acidosis Criteria -Type 1 or Type 2 Diabetes - CBG >14.0 mmol/l - capillary ketones mmol/l - ph 7.25 Type of Insulins to be used Novorapid/Humalog/Glulisine Resolution of ketosis = capillary ketones <0.6 mmol/l Resolution of hyperglycaemia = CBG <12.0 mmol/l If not confident treat as DKA Intravenous Fluids Potassium Replacement Insulin Therapy Subcutaneous Insulin 2 hourly Laboratory % sodium chloride (NaCl) at 500-1,000ml/h for 2 h 1. If serum K + 5.5mmol/L, do not give K,, but check serum K every 2 h a) Initial dose SC: units/kg OR 1 unit to lower CBG by 2.0 units followed by Admission: FBC, U&Es, Glc, venous gas for ph and bicarbonate and K % NaCl at ml/h until blood glucose 14.0mmol/L 2. If K mmol/l, add 20 mmol of KCl to each litre of IV fluid b) SC rapid-acting insulin at units 2 hours later and then Capillary Glucose: Check glucose every hour 3. When blood glucose <14.0mmol/L use NaCl 0.18%, Glucose 4% at ml/h until resolution of ketosis 3. If K mmol/L, add 40 mmol of KCl to each litre of IV fluid c) SC insulin unist/kg every 2 hours to keep glucose at 12.0mmol/L until resolution of ketosis. Capillary Ketones (bhydroxybutyrate): Check ketones every hour 4. If K + <3.0 mmol/l, give mmol of KCl per hour until serum K + >3.0 mmol/l, then add 40 mmol of KCl to each litre of IV fluid Venous Gas for ph and bicarbonate and K + every 2 hours
35 Case 3 A 73 year old woman with T2DM is referred to the AMU from the ED. She has been unwell with thirst, dysuria and urinary frequency for 3 days. On examination she was drowsy with a Glasgow Coma Scale of 9. Blood pressure is 104/76mmHg, pulse 126 bpm and irregular. Capillary blood glucose is reading high. The laboratory data showed: Na+ 139 mmol/l ( ) K+ 5.6 mmol/l ( ) Urea 19.2 mmol/l ( ) Cr 189 µmol/l (60 110) Serum glucose 41.1 mmol/l ( ) Arterial Blood Gas (on air) ph 7.41 ( ) po kpa ( ) pco kpa ( ) bicarbonate 22.2 mmol/l (24-28) base excess 0.8 mmol/l (±2) Calculated Serum Osmolality 2(Na + K) + Urea + Glc = Or (2Na + Glc + Urea) = Hyperosmolality >320
36 How to manage Case 3 INTRAVENOUS fluids 0.9% NaCl to correct circulatory volume and dehydration. Only switch to 0.45% NaCl if the osmolality is not declining An initial rise in Na + is expected Do Not give 0.45% NaCl. The rate of fall of Na + should not exceed 10.0 mmol/l in 24 hrs INSULIN INFUSION Start ONLY if CBG fails to fall with IV fluids Half the DKA calculated dose (0.05 unit/kg/hour) The fall in CBG should be no more than 5.0 mmol/l/hr ANTICOAGULATION Full dose anticoagulation dose unless contraindicated. DISCHARGE ANTIDIABETIC TREATMENT All patient should be discharged on INSULIN not oral agents.
37 DKA Cannula Port 1 Cannula Port 2 INTRAVENOUS 0.9% SALINE Aim/Function: 1. Fluid resuscitation and restoration of circulatory volume 2. Restore total water deficit - 100ml/kg 3. Restore total sodium deficit 7-10mmol/kg 4. Restore total potassium deficit 3-5mmol/kg Shock SBP <90mmHg, HR >100bpm, CRT >2 secs Management: 0.9% Saline aliquots 10mls/kg to max of 30mls/kg or ml aliquots Not Shocked (SBP >100mmHg) >70kg Fluid Rate (mls/h) Time (h) 0.9% Sodium chloride 1L % Sodium chloride 1L With potassium chloride* % Sodium chloride 1L With potassium chloride* % Sodium chloride 1L With potassium chloride* % Sodium chloride 1L With potassium chloride* % Sodium chloride 1L With potassium chloride* % Sodium chloride 1L With potassium chloride* Total 7 Litres 25 hours Potassium level (mmol/l) Replacement/litre fluid >5.5 Nil mmol/L < mmol/L Seek advice from specialist Assess response to treatment targets 1. CRT <2secs 2. SBP >100mmHg (MAP >70) and HR <100bpm 3. Urine output 0.5ml/kg If poor response to treatment Give fluid boluses of 0.9% Saline aliquots 10mls/kg to max of 30mls/kg or ml aliquots INTRAVENOUS INSULIN Aim/Function: 1. Resolution of ketosis 2. Correction of acidosis 3. Resolution of hyperglycaemia if present Fixed dose insulin 0.1unit/kg/hr (round up to the nearest whole number) until resolution of DKA. When CBG <12.0mmol/L Add in 5% Glucose 125mls/hr to enable fixed dose insulin to be continued. When CBG <8.0mmol/L Add in 10% Glucose 125mls/hr to enable fixed dose insulin to be continued. Resolution of DKA: Ketones<0.3mmol/L ph>7.3 Venous bicarbonate>18mmol/l CONTINUE THE 0.9% SALINE WITH THE GLUCOSE Assess response to treatment targets 1. Fall in ketones by mmol/hr 2. Rise in bicarbonate by mmol/hr 3. Fall in CBG by mmol/hr If poor response to treatment Increase insulin by 1.0unit/hr. If after 2 consecutive hours double the fixed dose to 0.2units/kg/hr CRT capillary refill time SBP systolic blood pressure MAP mean arterial pressure CBG = capillary blood glucose

")

38 HbA 1c HbA 1c tells you where you have arrived, but does not tell you how you got there. Capillary Blood Glucose (CBG) monitoring tells you the route you have taken. The medication used is the mode of transport.





39 Daredevil (DD) Double Digits In hospital glucose concentrations in double digits is not good for your patients 6.0 mmol/l In hospital glucose concentrations less than 6 puts your patient's at risk of falling down a slippery slope.
Inpatient Diabetes and Hyperglycaemia. Philip Dyer Heart of England NHS Foundation Trust Birmingham
 Inpatient Diabetes and Hyperglycaemia Philip Dyer Heart of England NHS Foundation Trust Birmingham Outline of the Talk Definitions and the burden The impact and the cost A case The effects of hyperglycaemia
Inpatient Diabetes and Hyperglycaemia Philip Dyer Heart of England NHS Foundation Trust Birmingham Outline of the Talk Definitions and the burden The impact and the cost A case The effects of hyperglycaemia
Please inform the Diabetes Nurse Specialist that this patient has been admitted within 24hrs of admission.
 Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Guidelines for the care of Children with Diabetes Mellitus undergoing Surgery
 Guidelines for the care of Children with Diabetes Mellitus undergoing Surgery Background Surgery places physical and emotional stress on the body. This, alongside new surroundings, parental anxiety and
Guidelines for the care of Children with Diabetes Mellitus undergoing Surgery Background Surgery places physical and emotional stress on the body. This, alongside new surroundings, parental anxiety and
The principles of insulin adjustment guidance
 The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow June 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood Glucose
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow June 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood Glucose
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Country Health SA Local Health Network. Version control and change history
 Country Health SA Local Health Network Protocol (Clinical) Title: Diabetic Ketoacidosis Management in Adults with Type 1 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor: CHSALHN,
Country Health SA Local Health Network Protocol (Clinical) Title: Diabetic Ketoacidosis Management in Adults with Type 1 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor: CHSALHN,
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
Updated August /08/2020
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of adults with diabetes
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Guideline for the management of adults with diabetes
Peri-operative management of the surgical patient with diabetes GL059
 DT Peri-operative management of the surgical patient with diabetes GL059 Approval Approval Group Job Title, Chair of Committee Date Anaesthetics Clinical Governance Chair Anaesthetic governance Nov 2016
DT Peri-operative management of the surgical patient with diabetes GL059 Approval Approval Group Job Title, Chair of Committee Date Anaesthetics Clinical Governance Chair Anaesthetic governance Nov 2016
HHS. Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours. Page 1 of 2 AFFIX PATIENT LABEL ! INFORM DIABETES TEAM OF ADMISSION!
 Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
Hyperglycaemic Hyperosmolar State Care Pathway 1 Presenta8on to 6 hours Page 1 of 2 Time of Arrival Loca8on Date / / Diagnosis the characteris8c features of a person with HHS are a) Hypovolaemia b) Marked
Guidelines for the Management of Diabetic Ketoacidosis (DKA) in Adults Inpatient Diabetes Steering Group
 in Adults Inpatient Diabetes Steering Group") Guidelines for the Management of Diabetic Ketoacidosis (DKA) in Adults Inpatient Diabetes Steering Group 1. Introduction 1.1 This document sets out the University Hospitals of Leicester (UHL) guidelines
Guidelines for the Management of Diabetic Ketoacidosis (DKA) in Adults Inpatient Diabetes Steering Group 1. Introduction 1.1 This document sets out the University Hospitals of Leicester (UHL) guidelines
Staff at the Nottingham Children s Hospital. Guidelines process.
 Diabetes and Surgery Title of Guideline Contact Name and Job Title (author) Guideline for the management of children and young people with diabetes aged 18 or under requiring surgery Dr Priyha Santhanam,
Diabetes and Surgery Title of Guideline Contact Name and Job Title (author) Guideline for the management of children and young people with diabetes aged 18 or under requiring surgery Dr Priyha Santhanam,
Guideline for Children with Type 1 or Type 2 Diabetes on Insulin Requiring Surgery or Sedation
 CHILDREN S SERVICES Guideline for Children with Type 1 or Type 2 Diabetes on Insulin Requiring Surgery or Sedation Background Surgery places stress on the body and will alter glucose control and insulin
CHILDREN S SERVICES Guideline for Children with Type 1 or Type 2 Diabetes on Insulin Requiring Surgery or Sedation Background Surgery places stress on the body and will alter glucose control and insulin
Use this version only
 Integrated Care Pathway PAEDIATRIC DIABETIC KETOACIDOSIS (DKA) Use this version only Patient Label Details Ward: Consultant: Named Nurse: Date of Admission: Date of Discharge/Transfer: ALL STAFF TO WRITE
Integrated Care Pathway PAEDIATRIC DIABETIC KETOACIDOSIS (DKA) Use this version only Patient Label Details Ward: Consultant: Named Nurse: Date of Admission: Date of Discharge/Transfer: ALL STAFF TO WRITE
Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Enteral Feeding Guidelines
 Inpatients Requiring Enteral Feeding Guidelines") Document Control Title Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Author Author s job title Specialist Nurse Consultant Physician Department Directorate Unscheduled Care Version Date
Document Control Title Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Author Author s job title Specialist Nurse Consultant Physician Department Directorate Unscheduled Care Version Date
Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules)
") Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules) SETTING FOR STAFF PATIENTS Medical and nursing staff Children and young
Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules) SETTING FOR STAFF PATIENTS Medical and nursing staff Children and young
Country Health SA Local Health Network
 Country Health SA Local Health Network Protocol (Clinical) Title: Hyperglycaemic Hyperosmolar State Management in Adults with Type 2 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor:
Country Health SA Local Health Network Protocol (Clinical) Title: Hyperglycaemic Hyperosmolar State Management in Adults with Type 2 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor:
Title Peri-operative Guidelines for the Management of Patients with Diabetes. Author s job title Diabetes Specialist Nurse Department.
 Patients with Document Control Title Peri-operative Guidelines for the Management of Patients with Author Directorate Medicine Version Date Issued 0.1 Jan 2011 Status Draft Initial version Author s job
Patients with Document Control Title Peri-operative Guidelines for the Management of Patients with Author Directorate Medicine Version Date Issued 0.1 Jan 2011 Status Draft Initial version Author s job
Pre admission & surgery Pre-admission Nurses Association SIG Catherine Prochilo Credentialled Diabetes Nurse Educator Sat 23 March 2013
 Pre admission & surgery Pre-admission Nurses Association SIG Catherine Prochilo Credentialled Diabetes Nurse Educator Sat 23 March 2013 www.diabetesvic.org.au Plan/ overview Issue/ presenting problems
Pre admission & surgery Pre-admission Nurses Association SIG Catherine Prochilo Credentialled Diabetes Nurse Educator Sat 23 March 2013 www.diabetesvic.org.au Plan/ overview Issue/ presenting problems
SCENARIO. Maternal Medicine -DKA LEARNING OBJECTIVES
 SCENARIO Maternal Medicine -DKA LEARNING OBJECTIVES Recognition of the of the seriously ill patient Diagnosis of DKA in pregnancy Recognition of precipitating factors for DKA Initiate emergency management
SCENARIO Maternal Medicine -DKA LEARNING OBJECTIVES Recognition of the of the seriously ill patient Diagnosis of DKA in pregnancy Recognition of precipitating factors for DKA Initiate emergency management
Peri-Operative Guidelines for Management of Diabetes Patients
 Peri-Operative Guidelines for Management of Diabetes Patients Target blood glucose 6-10 mmol/l for all patients Acceptable blood glucose 4-11 mmol/l for all patients Definitions Non-Insulin Glucose Lowering
Peri-Operative Guidelines for Management of Diabetes Patients Target blood glucose 6-10 mmol/l for all patients Acceptable blood glucose 4-11 mmol/l for all patients Definitions Non-Insulin Glucose Lowering
Lynda Astbury Lead Diabetes Specialist Nurse
 Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
AACN PCCN Review. Endocrine
 AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
MANAGEMENT OF DIABETES IN PREGNANCY
 MANAGEMENT OF DIABETES IN PREGNANCY Ministry of Health Malaysia Malaysian Endocrine & Metabolic Society Perinatal Society of Malaysia Family Medicine Specialists Association of Malaysia Academy of Medicine
MANAGEMENT OF DIABETES IN PREGNANCY Ministry of Health Malaysia Malaysian Endocrine & Metabolic Society Perinatal Society of Malaysia Family Medicine Specialists Association of Malaysia Academy of Medicine
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol. Glycemic Task Force September 2014
 DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
St Helens & Knowsley Teaching Hospitals Adult Inpatient Diabetes Management Guidelines v24
 St Helens & Knowsley Hospitals, 2014-16 Adult Inpatient Diabetes Management Guidelines St Helens & Knowsley Teaching Hospitals Adult Inpatient Diabetes Management Guidelines 2014-2016 v24 Title Adult Inpatient
St Helens & Knowsley Hospitals, 2014-16 Adult Inpatient Diabetes Management Guidelines St Helens & Knowsley Teaching Hospitals Adult Inpatient Diabetes Management Guidelines 2014-2016 v24 Title Adult Inpatient
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Information for Patients
 Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Information for Patients Guidance for Diabetic Persons having an OGD or Bronchoscopy This guidance is provided to assist with your preparation for your endoscopic procedure. If you feel unclear about how
Diabetes, Ketone testing in Type 1 Diabetes
 CLINICAL GUIDELINE Diabetes, Ketone testing in Type 1 Diabetes A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised
CLINICAL GUIDELINE Diabetes, Ketone testing in Type 1 Diabetes A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised
Northumbria Healthcare NHS Foundation Trust. Sick Day Rules for People with Diabetes. Issued by the Diabetes Service
 Northumbria Healthcare NHS Foundation Trust Sick Day Rules for People with Diabetes Issued by the Diabetes Service www.northumbria.nhs.uk Background: How illness may affect your diabetes 3 What to do for
Northumbria Healthcare NHS Foundation Trust Sick Day Rules for People with Diabetes Issued by the Diabetes Service www.northumbria.nhs.uk Background: How illness may affect your diabetes 3 What to do for
PERIOPERATIVE DIABETES GUIDELINE
 PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
PERIOPERATIVE DIABETES GUIDELINE This Guideline does not replace the need for the application of clinical judgment in respect to each individual patient. Background Diabetes mellitus is estimated to affect
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Think about when / why patients require insulin therapy
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Think about when / why patients require insulin therapy
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Inpatient Diabetes 20/01/2015. What should I do? Hyperglycaemia why does it matter? Why are the BSLs unstable? BSL parameters
 Hyperglycaemia why does it matter? Inpatient Diabetes Angela Sheu Endocrine Registrar St George Hospital Hyperglycaemia at admission is a predictor of mortality May be part of stress response (eg post
Hyperglycaemia why does it matter? Inpatient Diabetes Angela Sheu Endocrine Registrar St George Hospital Hyperglycaemia at admission is a predictor of mortality May be part of stress response (eg post
MANAGEMENT OF PREGNANT WOMEN WITH DIABETES WHO ARE IN-PATIENTS IN THE ROYAL INFIRMARY
 MANAGEMENT OF PREGNANT WOMEN WITH DIABETES WHO ARE IN-PATIENTS IN THE ROYAL INFIRMARY Background Management is different in different groups of women with diabetes. Women with Type 1 Diabetes (previously
MANAGEMENT OF PREGNANT WOMEN WITH DIABETES WHO ARE IN-PATIENTS IN THE ROYAL INFIRMARY Background Management is different in different groups of women with diabetes. Women with Type 1 Diabetes (previously
Guideline on Sick day rules for children and young people with diabetes on insulin
 Guideline on Sick day rules for children and young people with diabetes on insulin META DATA Title: Guidelines on Sick day rules for children and young people with Diabetes taking insulin Version: 1.0
Guideline on Sick day rules for children and young people with diabetes on insulin META DATA Title: Guidelines on Sick day rules for children and young people with Diabetes taking insulin Version: 1.0
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period
 Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Fasted and Consented but Blood Glucose 18mmol/L or How to Manage Diabetes in the Peri-Operative Period Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich
Management of Women with Type I Diabetes or Insulin Treated Type II Diabetes
 Management of Women with Type I Diabetes or Insulin Treated Type II Diabetes Author: Women & Child Health Specialty: Labour Ward Forum Date Approved: March 2017 Approved by: W&CH Clinical Governance Committee
Management of Women with Type I Diabetes or Insulin Treated Type II Diabetes Author: Women & Child Health Specialty: Labour Ward Forum Date Approved: March 2017 Approved by: W&CH Clinical Governance Committee
COMPLIANCE WITH THIS DOCUMENT IS MANDATORY
 COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
Diabetes, Type 2 Management
 CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
CLINICAL GUIDELINE Diabetes, Type 2 Management A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised on the applicability
Clinical Guidelines. Management of adult patients with diabetes undergoing endoscopic procedures
 Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Clinical Guidelines Management of adult patients with diabetes undergoing endoscopic s Document Detail Document type Clinical Guideline Management of adult Patients with diabetes Undergoing Document name
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Mellitus undergoing Surgery
 Clinical Guideline Care of children Children and young under people with 18 diabetes years mellitus with Diabetes Mellitus undergoing Surgery SETTING FOR STAFF PATIENTS Insert hospital name Medical and
Clinical Guideline Care of children Children and young under people with 18 diabetes years mellitus with Diabetes Mellitus undergoing Surgery SETTING FOR STAFF PATIENTS Insert hospital name Medical and
TYPE 1 DIABETES MELLITIS CARE OF WOMEN IN BIRTHING SUITE
 TYPE 1 DIABETES MELLITIS CARE OF WOMEN IN BIRTHING SUITE DEFINITION Type 1 Diabetes: described as a total lack of insulin produced by the pancreas for the requirements of the tissues. If left untreated,
TYPE 1 DIABETES MELLITIS CARE OF WOMEN IN BIRTHING SUITE DEFINITION Type 1 Diabetes: described as a total lack of insulin produced by the pancreas for the requirements of the tissues. If left untreated,
Insulin Management. By Susan Henry Diabetes Specialist Nurse
 Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Management of Adults with Diabetes Undergoing Surgery and Elective Procedures Guidelines. Diabetes Inpatient Steering Group June 2016
 Management of Adults with Diabetes Undergoing Surgery and Elective Procedures Guidelines Diabetes Inpatient Steering Group June 2016 1. Introduction 1.1 The aim of the guideline is to improve standards
Management of Adults with Diabetes Undergoing Surgery and Elective Procedures Guidelines Diabetes Inpatient Steering Group June 2016 1. Introduction 1.1 The aim of the guideline is to improve standards
The York Diabetes Care Model
 This Session The York Diabetes Care Model The annual review what s it for and how to do it How to make the diagnosis of diabetes and who to test Categorisation of diabetes at diagnosis Basics of Insulin
This Session The York Diabetes Care Model The annual review what s it for and how to do it How to make the diagnosis of diabetes and who to test Categorisation of diabetes at diagnosis Basics of Insulin
Diabetic Ketoacidosis (DKA)
") Diabetic Ketoacidosis (DKA) Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission February
Diabetic Ketoacidosis (DKA) Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission February
A I Page 1 of 10. SIMPSON CENTRE FOR REPRODUCTIVE HEALTH ROYAL INFIRMARY of EDINBURGH. Clinical Protocol
 SIMPSON CENTRE FOR REPRODUCTIVE HEALTH ROYAL INFIRMARY of EDINBURGH Clinical Protocol DIABETES IN PREGNANCY Diabetes; Management of GlycaemicControl in labour and in the antenatal period. Document Information
SIMPSON CENTRE FOR REPRODUCTIVE HEALTH ROYAL INFIRMARY of EDINBURGH Clinical Protocol DIABETES IN PREGNANCY Diabetes; Management of GlycaemicControl in labour and in the antenatal period. Document Information
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Diabetes Newly Diagnosed with NO evidence of DKA
 1. DIAGNOSIS confirmed by doctor using below guidelines: (a) History of Polyuria (usually nocturia ± enuresis) Polydipsia. ± Weight Loss (b) Glycosuria (c) Blood Glucose (BG) > 11 mmol/l (confirm from
1. DIAGNOSIS confirmed by doctor using below guidelines: (a) History of Polyuria (usually nocturia ± enuresis) Polydipsia. ± Weight Loss (b) Glycosuria (c) Blood Glucose (BG) > 11 mmol/l (confirm from
FBC, HbA1c, U/E, FT4, Blood Gas, Thyroid antibodies, TSH, Coeliac screen, GAD antibodies, Islet cell antibodies, and insulin antibodies.
 1. DIAGNOSIS confirmed by doctor using below guidelines: (a) History of polyuria (usually nocturia ± enuresis) Polydipsia ± weight loss (b) Glycosuria (c) Blood Glucose (BG) > 11 mmol/l (confirm from a
1. DIAGNOSIS confirmed by doctor using below guidelines: (a) History of polyuria (usually nocturia ± enuresis) Polydipsia ± weight loss (b) Glycosuria (c) Blood Glucose (BG) > 11 mmol/l (confirm from a
Information for all patients taking insulin who are admitted to hospital on day of surgery
 Information for all patients taking insulin who are admitted to hospital on day of surgery Exceptional healthcare, personally delivered Introduction Many patients are now admitted to hospital on the day
Information for all patients taking insulin who are admitted to hospital on day of surgery Exceptional healthcare, personally delivered Introduction Many patients are now admitted to hospital on the day
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Acute Stroke - Management of Hyperglycaemia. Contents
 Acute Stroke - Management of Hyperglycaemia Classification: Policy Lead Author: Dr Amir Ahmad Additional author(s): Dr Jouher Kallingal, Professor Bob Young, Professor Pippa Tyrrell Authors Division: :
Acute Stroke - Management of Hyperglycaemia Classification: Policy Lead Author: Dr Amir Ahmad Additional author(s): Dr Jouher Kallingal, Professor Bob Young, Professor Pippa Tyrrell Authors Division: :
GUIDELINES FOR THE TREATMENT OF DIABETIC KETOACIDOSIS (to be used in conjunction with DKA prescription and monitoring chart)
") GUIDELINES FOR THE TREATMENT OF DIABETIC KETOACIDOSIS (to be used in conjunction with DKA prescription and monitoring chart) This guidance does not override the individual responsibility of health professionals
GUIDELINES FOR THE TREATMENT OF DIABETIC KETOACIDOSIS (to be used in conjunction with DKA prescription and monitoring chart) This guidance does not override the individual responsibility of health professionals
Title Management of Children and Young People with Newly Diagnosed Type 1 Diabetes Mellitus Guideline
 Document Control Title Management of Children and Young People with Newly Diagnosed Type 1 Diabetes Mellitus Guideline Author Directorate Version Author s job title Consultant Paediatrician Department
Document Control Title Management of Children and Young People with Newly Diagnosed Type 1 Diabetes Mellitus Guideline Author Directorate Version Author s job title Consultant Paediatrician Department
Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology
 Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology Faculty photo will be placed here Simha.aj@mayo.edu 2015 MFMER 3543652-1 Diabetic Ketoacidosis a few pearls Mayo School of Continuous Professional
Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology Faculty photo will be placed here Simha.aj@mayo.edu 2015 MFMER 3543652-1 Diabetic Ketoacidosis a few pearls Mayo School of Continuous Professional
Diabetic Emergencies DKA, HHS, Hypoglycemia. Disclosure. Learning Objectives
 Diabetic Emergencies DKA, HHS, Hypoglycemia October 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Disclosure Michael McDermott has no conflict
Diabetic Emergencies DKA, HHS, Hypoglycemia October 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Disclosure Michael McDermott has no conflict
DKA Adult ICU Powerplan
 DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version)
") Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Contact Details Name: Hospital Telephone: This protocol has 5 pages ISOVALERIC ACIDAEMIA -ACUTE DECOMPENSATION (standard version) Please read carefully. Meticulous treatment is very important as there
Case TWO. Vital Signs: Temperature 36.6degC BP 137/89 HR 110 SpO2 97% on Room Air
 Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
GUIDELINES FOR THE MANAGEMENT OF DIABETES IN PALLIATIVE CARE
 GUIDELINES FOR THE MANAGEMENT OF DIABETES IN PALLIATIVE CARE 16.1 GENERAL PRINCIPLES Diabetes occurs more frequently in palliative care patients than the general population. 1 Patients with pancreatic
GUIDELINES FOR THE MANAGEMENT OF DIABETES IN PALLIATIVE CARE 16.1 GENERAL PRINCIPLES Diabetes occurs more frequently in palliative care patients than the general population. 1 Patients with pancreatic
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address:
 Name: Ward/Practice Area: Mailing Address:") 1 DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address: 2 Learning Outcomes All nurses, regardless of practice setting, are required to work collaboratively with the person
1 DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address: 2 Learning Outcomes All nurses, regardless of practice setting, are required to work collaboratively with the person
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State. Adam Bursua, Pharm.D., BCPS
 Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Hyperglycaemic Emergencies GRI EDUCATION
 Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Initiating Injectables in Type 2 Diabetes. Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital
 Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Initiating Injectables in Type 2 Diabetes Tara Kadis Team Leader Diabetes Nurse Specialist York Teaching Hospital Increasing levels in delivery of diabetes care Complex Care support 3 3.1 People with diabetes
Case Study: Competitive exercise
 Case Study: Competitive exercise 32 year-old cyclist Type 1 diabetes since age 15 Last HbA1 54 No complications and hypo aware On Humalog 8/8/8 and Levemir 15 Complains about significant hypoglycaemia
Case Study: Competitive exercise 32 year-old cyclist Type 1 diabetes since age 15 Last HbA1 54 No complications and hypo aware On Humalog 8/8/8 and Levemir 15 Complains about significant hypoglycaemia
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
Diabetic Ketoacidosis (DKA) Critical Care Guideline Two Bag System
 Critical Care Guideline Two Bag System") Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Pediatric Diabetic Ketoacidosis (DKA) General Pediatrics Admission Order Set
 General Pediatrics Admission Order Set") Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
THIS IS A PATIENT HAND HELD DOCUMENT CARE PATHWAY FOR MANAGEMENT OF INITIATION OF INSULIN
 Worcestershire Trusts Please attach patient sticker here or record: GP Name: Consultant:. Ward: THIS IS A PATIENT HAND HELD DOCUMENT CARE PATHWAY FOR MANAGEMENT OF INITIATION OF INSULIN This Care Pathway
Worcestershire Trusts Please attach patient sticker here or record: GP Name: Consultant:. Ward: THIS IS A PATIENT HAND HELD DOCUMENT CARE PATHWAY FOR MANAGEMENT OF INITIATION OF INSULIN This Care Pathway
Managing diabetes if you are having a colonoscopy
 Managing diabetes if you are having a colonoscopy Diabetes and Endocrinology Patient Information Leaflet Introduction This leaflet provides advice and instructions to people with diabetes who are going
Managing diabetes if you are having a colonoscopy Diabetes and Endocrinology Patient Information Leaflet Introduction This leaflet provides advice and instructions to people with diabetes who are going
Diabetes Emergency Caesarean section or other unplanned surgery (GL822)
") Diabetes Emergency Caesarean section or other unplanned surgery (GL822) i.e. insulin dependent diabetic having unplanned surgery e.g. a diabetic woman with pre-labour SROM prior to elective Caesarean section.
Diabetes Emergency Caesarean section or other unplanned surgery (GL822) i.e. insulin dependent diabetic having unplanned surgery e.g. a diabetic woman with pre-labour SROM prior to elective Caesarean section.
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS
 Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
Insulin Initiation, titration & Insulin switch in the Primary Care-KISS Rotorua GP CME 9 June 2012 Dr Kingsley Nirmalaraj FRACP Endocrinologist, BOPDHB & Suite 9, Promed House, Tenth Ave, Tauranga Linda
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
Inpatient Diabetes Care
 Inpatient Diabetes Care Data from the National Diabetes Inpatient Audit suggest that the number of hospital inpatients with diabetes ranges from ~10% to over 30%. This does not mean that up to 1 in 3 inpatients
Inpatient Diabetes Care Data from the National Diabetes Inpatient Audit suggest that the number of hospital inpatients with diabetes ranges from ~10% to over 30%. This does not mean that up to 1 in 3 inpatients
Starting Insulin in General Practice
 Starting Insulin in General Practice Timothy Kenealy GP & Assoc Prof of Integrated Care, University of Auckland Auckland DHB / my version + Counties DHB version Starting Insulin surprisingly simple, safe
Starting Insulin in General Practice Timothy Kenealy GP & Assoc Prof of Integrated Care, University of Auckland Auckland DHB / my version + Counties DHB version Starting Insulin surprisingly simple, safe
Clinical Guideline for the management of paediatric patients with Diabetes Type 1 & 2 requiring Surgery or General Anaesthetic. V4
 Clinical Guideline for the management of paediatric patients with Diabetes Type 1 & 2 requiring Surgery or General Anaesthetic. V4 Page 1 of 27 Abbreviation Meaning PDSN DKA BG SC IV RCHT HDU PEWS Paediatric
Clinical Guideline for the management of paediatric patients with Diabetes Type 1 & 2 requiring Surgery or General Anaesthetic. V4 Page 1 of 27 Abbreviation Meaning PDSN DKA BG SC IV RCHT HDU PEWS Paediatric
Short-acting insulins. Biphasic insulins. Intermediate- and long-acting insulins
 Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Nothing to disclose. Disclosure
 Nothing to disclose. Disclosure Inpatient Management of Diabetes Mellitus Cindy Chin, MD Pediatrics in the Red Rocks 2015 Objectives Name 3 diagnostic criteria for diabetes mellitus. Understand and apply
Nothing to disclose. Disclosure Inpatient Management of Diabetes Mellitus Cindy Chin, MD Pediatrics in the Red Rocks 2015 Objectives Name 3 diagnostic criteria for diabetes mellitus. Understand and apply
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
When and how to start insulin therapy in type 2 diabetes
 When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
East of England Children & Young People s (CYP) Diabetes Network
 Diabetes Network") East of England Children & Young People s (CYP) Diabetes Network Management for Children and Young People with diabetes (>6months old 18 th birthday) during Illness Note: This version of the guideline
East of England Children & Young People s (CYP) Diabetes Network Management for Children and Young People with diabetes (>6months old 18 th birthday) during Illness Note: This version of the guideline
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Hypoglyceamia and Exercise
 Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Hypoglyceamia and Exercise Noreen Barker Diabetes Specialist Nurse May 2016 Hypoglyceamia What is a hypo? Why are we concerned? Signs and symptoms Treatments Causes Hypo unawareness Managing diabetes and
Management of adults with diabetes undergoing surgery and elective procedures: improving standards
 Surgical outpatients Hospital admission Theatre and recovery Discharge Primary care referral Pre-operative assessment Post-operative care Management of adults with diabetes undergoing surgery and elective
Surgical outpatients Hospital admission Theatre and recovery Discharge Primary care referral Pre-operative assessment Post-operative care Management of adults with diabetes undergoing surgery and elective
Four is the Floor Symptoms can be felt at higher levels if control is poor Worth confirmation using BG meter if at all possible
 Sandra Coats Diabetes Specialist Nurse 1 Hypoglycaemia Hyperglycaemia Diabetes and Illness sick day Diabetic Ketoacidosis HONK/HHS 2 What is Hypoglycaemia BG levels below 4mmol/l. Four is the Floor Floor
Sandra Coats Diabetes Specialist Nurse 1 Hypoglycaemia Hyperglycaemia Diabetes and Illness sick day Diabetic Ketoacidosis HONK/HHS 2 What is Hypoglycaemia BG levels below 4mmol/l. Four is the Floor Floor
There have been important changes in diabetes care which may not be covered in undergraduate textbooks.
 Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Brief summary of the NICE guidelines December 2013
 Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
Brief summary of the NICE guidelines December 2013 Intravenous fluid therapy in adults in hospital the relevance to Emergency Department Care Applicable to patients 16 years and older receiving i.v. fluids
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with