Peripheral Arterial Disease
|
|
|
- Elaine Preston
- 5 years ago
- Views:
Transcription


1 Peripheral Arterial Disease None Disclosures Michael R. Go, MD Division of Vascular Diseases and Surgery Department of Surgery The Ohio State University Wexner Medical Center Anatomy Pathophysiology Demographics Diagnosis Treatment Objectives Author: Mcstrother CC BY 3.0 1





2 Intima Luminal surface to IEL Endothelial cells Few leukocytes, connective tissue fibers, smooth muscle cells Author: Mcstrother CC BY 3.0 IEL to EEL and adventitia Smooth muscle cells Elastin Collagen type III Media Fibrocellular connective tissue Vasa vasorum Some collagen and elastin Normally does not contribute to tensile strength In atherosclerosis, a diseased media relies on adventitia for tensile strength Adventitia Author: BruceBlaus CC BY 3.0 Blausen.com staff. "Blausen gallery 2014". Wikiversity Journal of Medicine. DOI: /wjm/ ISSN



3 Elastic Arteries Muscular Arteries Prominent elastic fibers in proximal vessels High compliance Recoil Interspersed with type I collagen bundles Smaller distal vessels Less collagen and elastin, more smooth muscle cells Constrict and dilate more effectively Vasa Vasorum Diffusion supports 0.5 mm or 30 musculoelastic bundles Vasa vasorum supply the rest Atherosclerosis Most common cause of peripheral arterial disease Preferentially involves the internal carotid, infrarenal aorta, and superficial femoral arteries Typically occurs at bifurcations Author: Nephron CC BY-SA 3.0 3
4 Pathology Intimal thickening Fatty streaks Fibrous plaques Plaque complication Intimal Thickening Increased wall tensile stress Increased wall thickness Occurs at bifurcations and areas of redistribution of wall stress in fetuses No lipid accumulation Occurs in same places as plaque, but not necessarily a precursor Fatty Streaks Intimal accumulation of foam cells Affect all ages Do not compromise lumen Abnormal overlying endothelial cells Occurs throughout vascular tree Not necessarily a precursor of plaque Fibrous Plaques Earliest definitive atherosclerotic lesion Appear by second decade Subendothelial smooth muscle Fibrous cap of connective tissue Intact but fragile endothelium Attenuated media 4


5 Plaque Complications Necrotic core of lipid, macrophages, and smooth muscle cells Calcification Endothelial disruption Ulceration Hemorrhage Embolism Pathophysiology Atherosclerosis may cause symptoms via stenosis or occlusion of axial vessels Inadequate tissue perfusion Risk Factors Peripheral Arterial Disease Tobbaco use Diabetes Hyperlipidemia Genetics Hypertension 200,000,000 people affected 2/3 live in low income countries Rutherford: Vascular Surgery, 6 th ed. 5


6 Peripheral Arterial Disease 8,500,000 people in the US Affects 20% of people over age 80 Asymptomatic Claudication Critical limb ischemia Rest pain Ulceration Claudication Pain in the large muscle groups distal to an arterial lesion after exercise Cramping, heaviness, fatigue Occurs consistently after a certain distance of walking Reliably abates when patient stops The patient is asymptomatic at rest because there are adequate collaterals for perfusion without increased metabolic demand Rutherford: Vascular Surgery, 9 th ed. Bloor K. Natural history of arteriosclerosis of the lower extremities. Ann R Coll Surg Engl 1961; 28: Affects 5% of the population over 50 75% of claudicants will remain stable 25% will deteriorate 7-9% in first year 2-3% per year after first year 5% will progress to critical limb ischemia Claudication 90% have concomitant CAD 5 year overall amputation 5% 5 year incidence of symptomatic coronary artery disease 23% 5 year incidence of stroke 13% 5 year mortality 20% 10 year mortality 50% 15 year mortality 70% 2% will progress to major amputation 6



7 Critical Limb Ischemia Ischemic rest pain intense pain across distal foot and arch burning, stabbing, constant worsened with elevation dependent rubor Ulceration Gangrene dry wet Critical Limb Ischemia / 1 million new cases annually 1 3% of PAD population Outcomes of CLI Five Year Mortality 7



8 Diabetic Foot Problems Diabetic foot ulcers and amputations cost US health care providers over 10 billion dollars per year Diabetic Foot Problems 24,000,000 diabetic patients in the US 3,500,000 people with DM and PAD in the US Diabetes and PAD Diabetic Foot Problems Lifetime risk of ulcers or gangrene is 15-25% > 15% of patients with ulcers will end up with an amputation Every 30 seconds a leg is amputated somewhere in the world as a consequence of diabetes 8
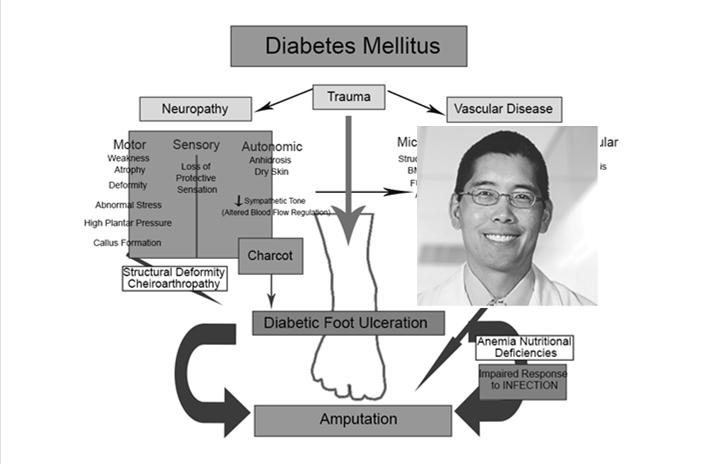
9 Diabetic Foot Problems Highest incidence in ethnic minority groups 2 4X higher rate of amputation compared to non-minority groups Native Americans, Hispanics, African Americans A problem requiring intensive follow up and management is compounded by difficult access to care Diabetic Foot Problems Neuropathy Deformity Trauma Ischemia Infection Neuropathy Sensory nerves affected first Small diameter pain and temperature fibers are initially damaged Predisposes to pressure related trauma and minor skin Injuries Neuropathy Motor neuropathy is late Affects both long fibers innervating both intrinsic muscles of the foot and leg muscles 9




10 Neuropathy Atrophy of intrinsic foot muscles Preserved flexor muscle strength results in clawed position Abnormal pressure points emerge at tips of toes Metatarsal heads relax Neuropathy Calluses form which later may ulcerate Small muscles of the foot atrophy Autonomic Neuropathy Dry skin Loss of sweat and oil gland function Dry skin predisposes to fissures Calluses and fissures breakdown Portals of entry for bacteria Ischemia Neuropathy causes shunting of blood through AV connections in the microcirculation Results in decreased tissue perfusion even with normal axial vessels Cutaneous oxygen saturation is decreased Compounded with neuropathy, ulceration results 10
11 Ischemia Diabetes causes structural and functional changes in the capillary bed Thickened basement membrane Impaired migration of leukocytes Impaired vasodilation response to injury Blunted inflammatory response to injury Infection Because of this blunted inflammatory response, diabetic patients lack a crucial component of the body s first line defense against pathogens and thus are more susceptible to foot infection Peripheral Arterial Disease Differential Neurogenic claudication spinal stenosis or nerve root compression history of back pain burning or shooting pain radiating down posterior leg numbness or paresthesias Neuropathy Arthritis Neuropathic ulceration History Coronary artery disease MI CHF arrhythmia recent cardiac evaluation DM Smoking Hypertension Hypercholesterolemia Family history of atherosclerotic disease Cerebrovascular disease stroke TIA amaurosis 11



12 Physical Exam Complete heart and lung exam Neurologic exam carotid bruits superficial temporal pulses cranial nerves motor sensory Vascular Exam Complete bilateral pulse exam Doppler monophasic multiphasic 0, 1+, 2+, 3+, widened pulses Bruits and thrills Vascular Exam Dependent rubor Shiny skin Loss of hair Diminished nail growth Ulceration and gangrene Vascular Lab Testing ABI Can be affected by vascular calcification or edema 12

13 ABI Claudication 0.6 Rest pain 0.3 Tissue loss 0.2 Exercise Testing Treadmill or calf raises decrease peripheral resistance Flow increases based on Ohm s law If there is a proximal stenosis, flow increase is limited and pressure will drop Vascular Lab Testing Pulse volume recordings normal blunted Doppler waveforms multiphasic monophasic Digital pressures Not limited by vessel calcification Complements pressure testing 13


 P 0.05 vs placebo P 0.05 vs pentoxifylline Dawson et al.")
14 Angiography Diagnostic Therapeutic Complications nephrotoxicity contrast allergy arterial injury embolization hematoma pseudoaneurysm Treatment of Claudication Risk factor modification smoking cessation hypertension hyperlipidemia diabetes Supervised exercise program 30 minutes of cardiovascular exercise daily 5 days per week Cilostazol Cilostazol 100 mg bid (n=205) Pentoxifylline 400 mg tid (n=212) Placebo (n=226) P 0.05 vs placebo P 0.05 vs pentoxifylline Dawson et al. Am J Med
15 Cilostazol 2 to 4 weeks prior to response 12 weeks of treatment are recommended to assess effectiveness Improvement was noted throughout the trial period (up to 24 weeks) and did not plateau by study s end Treatment must be continued to maintain increases in walking distance Procedural Intervention for Claudication Procedural intervention for claudication is reserved for patients with lifestyle-limiting claudication and failure of medical therapy Often, this is related to single level, proximal disease aortoiliac femoral ABI 0.6 Treatment of Rest Pain or Tissue Loss Risk factor modification Restoration of in-line vascular flow Management of the wound Often, this is related to multi level or distal disease popliteal tibial ABI 0.3 Endovascular Intervention 15
16 16
17 Angioplasty 1 year primary patency 50-60% (in optimal lesions) Bare Metal Stenting 1 year primary patency 73-81% (in optimal lesions) Laird JR et al. Circ Cardiovasc Interv : Matsumura JS et al. J Vasc Surg : Dake MD et al. Circ Cardiovasc Interv : The Common Modality Of Failure: Drug Elution Therapy Inhibition of SMC proliferation and migration Decreased restenosis Intimal Hyperplasia 17



18 IN.PACT SFA Trial Summary Tepe G et al. Circ : IN.PACT SFA 1 year Results (@360d) IN.PACT Admiral Standard PTA P value Delta Primary patency 82.2% 52.4% < % Freedom from TLR 97.5% 79.3% < % 18



19 Percutaneous Treatment Results Are Better Proximal vessels (aorta > iliacs > SFA > tibials) Short lesions Focal lesions Stenoses > occlusions Percutaneous Treatments Are Worse Distal or smaller vessels Long lesions Diffuse lesions Occlusions At joints or bifurcations common femoral profunda popliteal Percutaneous Treatments Local anesthesia Fewer cardiopulmonary complications Outpatient procedure Radiation Nephrotoxicity Arterial injury Embolization Pseudoaneurysm Rarely as durable as bypass or open repair Surgery Procedural intervention for claudication is reserved for patients with lifestyle-limiting claudication and failure of medical therapy Rest pain Tissue loss 19

 Extensive tissue loss (consider primary")


20 Contraindications to Surgery Prohibitive medical comorbidities coronary pulmonary Unreconstructible vessels Nonambulatory status (consider primary amputation) Extensive tissue loss (consider primary amputation) Level of Disease Determines Options Aortoiliac aortoiliac endarterectomy aortofemoral bypass axillary femoral bypass Femoropopliteal femoral endarterectomy femoropopliteal bypass Tibial femorotibial bypass popliteal tibial or pedal bypass 20




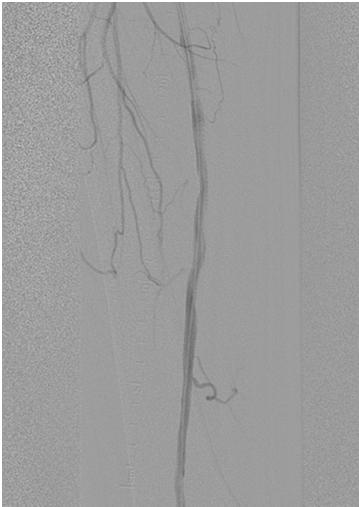
21 Native SFA occluded 21
 Amputation Nonambulatory patients with CLI Patients with extensive")


22 Bypass Conduit Greater saphenous vein Other autogenous vein lesser saphenous cephalic basilic Prosthetic (polyester or Polytetrafluoroethylene) Amputation Nonambulatory patients with CLI Patients with extensive tissue loss Unreconstructible patients foot sepsis intractable pain Amputation The more distal the amputation, the better the functional outcome The more proximal the amputation, the better the likelihood of healing Feel for a pulse one level above the proposed amputation The skin should be warm and pink at the level of the proposed amputation A pressure of 50 mmhg at the level of the proposed amputation predicts healing 22






23 Peripheral Arterial Disease and Limb Preservation Said Atway, DPM, FACFAS Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center 23




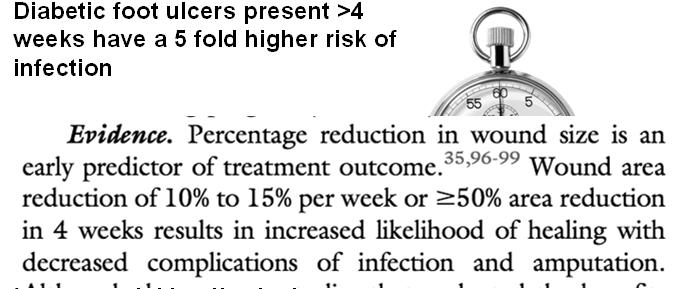
24 Foot Infection Foot Infection Any infra-malleolar infection in a person with diabetes Common and costly problem DM related amputation cost 3B per year Diabetes Care 2003 Most common reason for a diabetic to be admitted National Hospital Discharge Data Most common non-traumatic cause of amputation 60% of LEA Most common cause of nontraumatic lower extremity amputation Lancet 2005 Any infra-malleolar infection in a person with diabetes Common and costly problem DM related amputation cost 3B per year Diabetes Care 2003 Most common reason for a diabetic to be admitted National Hospital Discharge Data Most common non-traumatic cause of amputation 60% of LEA Most common cause of nontraumatic lower extremity amputation Lancet 2005 Importance of Diabetic Wound care Diabetic foot ulcers present >4 weeks have a 5 fold higher risk of infection Infection in a foot ulcer increases the risk for hospitalization 55.7 times and risk for amputation 155 times 5 year mortality after limb amputation is 68% NIH publication 1995 Importance of Diabetic Wound care Diabetic foot ulcers present >4 weeks have a 5 fold higher risk of infection Infection in a foot ulcer increases the risk for hospitalization 55.7 times and risk for amputation 155 times 5 year mortality after limb amputation is 68% NIH publication
25 25
26 26




27 Angiosome directed vascularization 27




28 Clinical Practice Guidelines Management of etiologic factors Adequate perfusion PAD (Twice as common in DM) Gregg et al 2004 Rarely lead to ulcer directly Contributes to 50% of ulcers Diabetes Metab 2008 Debridement Sharp debridement of infection Urgent for gas/necrotizing infection Infection Control IDSA guidelines Pressure Mitigation Offloading Surgical Nonsurgical Total contact cast 28


29 Debridement? 29




30 30



31 Hindfoot osteomyelitis a challenge met by all those treating the foot and ankle Osteomyelitis secondary to diabetic foot ulceration is an unfortunate complication that may require Long term intravenous antibiotics Operative debridement Amputation, and commonly a combination of these. Debridement/complete excision of infected bone Soft tissue coverage Compliance of patients Antoniou D, Conner AN. Osteomyelitis of the calcaneus and talus. J Bone Joint Surg Am 1974;56:



32 Hindfoot osteomyelitis a challenge met by all those treating the foot and ankle Osteomyelitis secondary to diabetic foot ulceration is an unfortunate complication that may require Long term intravenous antibiotics Operative debridement Amputation, and commonly a combination of these. Debridement/complete excision of infected bone Soft tissue coverage Compliance of patients Antoniou D, Conner AN. Osteomyelitis of the calcaneus and talus. J Bone Joint Surg Am 1974;56:







33 Pathophysiologic mechanism complex Neuropathy Repetitive trauma Focal tissue ischemia Tissue Destruction Deformity Charcot Neuroarthropathy/Abnormal pressure Foot deformities Charcot Neuroarthropathy Limited joint mobility Glycosylation of soft tissue 33





34 The Majority of foot ulcers appear to result from minor trauma in the presence of sensory neuropathy McNeely Critical Triad: (65% of diabetic foot ulcers) Neuropathy Deformity Trauma The Majority of foot ulcers appear to result from minor trauma in the presence of sensory neuropathy McNeely Critical Triad: (65% of diabetic foot ulcers) Neuropathy Deformity Trauma Prevention Ulcer Prevention Diabetic foot exams Offloading Surgical offloading Prosthetic offloading Ulcer Care Debridement Infection prevention Optimize wound healing Foot Care 34






35 Venous Majority of Leg ulcers Innactivates normal antibacterial property Inhibits mitogenic activity Etiology uncertain Fibrin cuff Fibrin leaks creating cuff WBC Increased inflammatory mediators Mast cell stimulation Venous Thank You 35
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease
 Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
The Diabetic Foot. Michael Anthony, DPM. 422 million diabetic million % adult population 90% Type II
 The Diabetic Foot Michael Anthony, DPM Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center Prevalence of Diabetes 422 million diabetic 2016 382 million
The Diabetic Foot Michael Anthony, DPM Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center Prevalence of Diabetes 422 million diabetic 2016 382 million
The Diabetic Foot. Prevalence of Diabetes United States. Prevalence of Diabetes
 The Diabetic Foot Prevalence of Diabetes Michael Anthony, DPM Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center 422 million diabetic 2016 382 million
The Diabetic Foot Prevalence of Diabetes Michael Anthony, DPM Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center 422 million diabetic 2016 382 million
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Objectives. Abdominal Aortic Aneuryms 11/16/2017. The Vascular Patient: Diagnosis and Conservative Treatment
 The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
Approach to the Patient with (suspected) Arterial Insufficiency Related Ulceration
 Arterial Insufficiency Related Ulceration") Approach to the Patient with (suspected) Arterial Insufficiency Related Ulceration Elisa C. Taffe, MD, CWSP Vascular Medicine Medical Director Allegheny General Advanced Wound Healing and Lymphedema Center
Approach to the Patient with (suspected) Arterial Insufficiency Related Ulceration Elisa C. Taffe, MD, CWSP Vascular Medicine Medical Director Allegheny General Advanced Wound Healing and Lymphedema Center
Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital
 Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Evidence-Based Optimal Treatment for SFA Disease
 Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014
 PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
Peripheral arterial disease for primary care Ed Aboian, MD
 Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Disclosures. Talking Points. An initial strategy of open bypass is better for some CLI patients, and we can define who they are
 An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC
 Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists
 EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC
 High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC A new paradigm? Foot ulceration 101 Assessing Perfusion a new challenge Pressure
High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC A new paradigm? Foot ulceration 101 Assessing Perfusion a new challenge Pressure
Peripheral Arterial Disease. Westley Smith MD Vascular Fellow
 Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Introduction. Epidemiology Pathophysiology Classification Treatment
 Diabetic Foot Introduction Epidemiology Pathophysiology Classification Treatment Epidemiology DM largest cause of neuropathy in N.A. 1 million DM patients in Canada Half don t know Foot ulcerations is
Diabetic Foot Introduction Epidemiology Pathophysiology Classification Treatment Epidemiology DM largest cause of neuropathy in N.A. 1 million DM patients in Canada Half don t know Foot ulcerations is
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
Perfusion Assessment in Chronic Wounds
 Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
DCB in my practice: How the evidence influences my strategy. Yang-Jin Park
 DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Introduction to Peripheral Arterial Disease. Stacey Clegg, MD Interventional Cardiology August
 Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Peripheral Vascular Disease
 Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Aortoiliac occlusive disease
 Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Limb Salvage in Diabetic Ischemic Foot. Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017
 Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Watermark. Interaction between Neuropathy and PAD
 Interaction between Neuropathy and PAD Javier La Fontaine, DPM, MS Associate Professor Department of Plastic Surgery UT Southwestern Medical Center Dallas, Texas Objectives Understand vascular disease
Interaction between Neuropathy and PAD Javier La Fontaine, DPM, MS Associate Professor Department of Plastic Surgery UT Southwestern Medical Center Dallas, Texas Objectives Understand vascular disease
Peripheral Arterial Disease Extremity
 Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Pathology of Coronary Artery Disease
 Pathology of Coronary Artery Disease Seth J. Kligerman, MD Pathology of Coronary Artery Disease Seth Kligerman, MD Assistant Professor Medical Director of MRI University of Maryland Department of Radiology
Pathology of Coronary Artery Disease Seth J. Kligerman, MD Pathology of Coronary Artery Disease Seth Kligerman, MD Assistant Professor Medical Director of MRI University of Maryland Department of Radiology
Case Discussion. Disclosures. Critical Limb Ischemia: A Selective Approach to Revascularization Works Best 4/28/2012. None. 58 yo M, DM, CAD, HTN
 Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Pedal Bypass With Deep Venous Arterialization:
 Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Will it heal? How to assess the probability of wound healing
 Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Combat Extremity Vascular Trauma
 Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Critical Limb Ischemia A Collaborative Approach to Patient Care. Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017
 Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Vascular disease. Structural evaluation of vascular disease. Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital
 Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Radiologic Evaluation of Peripheral Arterial Disease
 January 2003 Radiologic Evaluation of Peripheral Arterial Disease Grace Tye, Harvard Medical School Year III Patient D.M. CC: 44 y/o male with pain in his buttocks Occurs after walking 2 blocks. Pain is
January 2003 Radiologic Evaluation of Peripheral Arterial Disease Grace Tye, Harvard Medical School Year III Patient D.M. CC: 44 y/o male with pain in his buttocks Occurs after walking 2 blocks. Pain is
Disclosures. Tips and Tricks for Tibial Intervention. Tibial intervention overview
 Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome
 Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Diabetic Foot Pathophysiology. Professor Donald G. MacLellan Executive Director Health Education & Management Innovations
 Diabetic Foot Pathophysiology Professor Donald G. MacLellan Executive Director Health Education & Management Innovations AGEs & RAGEs in Diabetes AGE levels increased & RAGEs highly expressed in diabetic
Diabetic Foot Pathophysiology Professor Donald G. MacLellan Executive Director Health Education & Management Innovations AGEs & RAGEs in Diabetes AGE levels increased & RAGEs highly expressed in diabetic
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
The Peripheral Vascular System
 The Peripheral Vascular System Anatomy and Physiology Arteries Arteries contain 3 concentric layers of tissue: - the intima - the media - the adventitia The intima The endothelium of the intima has metabolic
The Peripheral Vascular System Anatomy and Physiology Arteries Arteries contain 3 concentric layers of tissue: - the intima - the media - the adventitia The intima The endothelium of the intima has metabolic
Imaging for Peripheral Vascular Disease
 Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Guidelines for Management of Peripheral Arterial Disease
 Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Fluorescent Angiography: Practical uses in the Clinical Setting
 Fluorescent Angiography: Practical uses in the Clinical Setting Charles Andersen MD, FACS, MAPWCA Chief Vascular/Endovascular/ Limb Preservation Surgery Service (Emeritus) Chief of Wound Care Service Madigan
Fluorescent Angiography: Practical uses in the Clinical Setting Charles Andersen MD, FACS, MAPWCA Chief Vascular/Endovascular/ Limb Preservation Surgery Service (Emeritus) Chief of Wound Care Service Madigan
V.A. is a 62-year-old male who presents in referral
 , LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
, LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures
 Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Definitions and criteria
 Several disciplines are involved in the management of diabetic foot disease and having a common vocabulary is essential for clear communication. Thus, based on a review of the literature, the IWGDF has
Several disciplines are involved in the management of diabetic foot disease and having a common vocabulary is essential for clear communication. Thus, based on a review of the literature, the IWGDF has
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria
 Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria") Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
9/7/2018. Disclosures. CV and Limb Events in PAD. Challenges to Revascularization. Challenges. Answering the Challenge
 Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
BC Vascular Surgery Day
 BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care
 Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular
Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular
The Diabetic Foot Screen and Management Foundation Series of Modules for Primary Care
 The Diabetic Foot Screen and Management Foundation Series of Modules for Primary Care Anita Murray - Senior Podiatrist Diabetes, SCH Learning Outcomes Knowledge of the Model of Care For The Diabetic Foot
The Diabetic Foot Screen and Management Foundation Series of Modules for Primary Care Anita Murray - Senior Podiatrist Diabetes, SCH Learning Outcomes Knowledge of the Model of Care For The Diabetic Foot
Diabetic Foot Ulcers. Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C. Advanced Practice Nurse / Adult Clinical Nurse Specialist
 Diabetic Foot Ulcers Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist Organization of Wound Care Nurses www.woundcarenurses.org Objectives Identify Diabetic/Neuropathic
Diabetic Foot Ulcers Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist Organization of Wound Care Nurses www.woundcarenurses.org Objectives Identify Diabetic/Neuropathic
Garland Green, MD Interventional Cardiologist. Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management
 Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
There are multiple endovascular options for treatment
 Peripheral Rotablator Atherectomy: The Below-the-Knee Approach to Address Calcium Head On Peripheral Rotablator s front-cutting, diamond-tipped burr provides stable rotation in calcified lesions. BY SONYA
Peripheral Rotablator Atherectomy: The Below-the-Knee Approach to Address Calcium Head On Peripheral Rotablator s front-cutting, diamond-tipped burr provides stable rotation in calcified lesions. BY SONYA
Non-invasive examination
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Diabetic Foot Complications
 Diabetic Foot Complications Podiatry Specialty Clinic YKHC Bethel, Alaska August 1-3, 2017 Charles C. Edwards, DPM Alaska Native Tribal Health Consortium Peripheral Neuropathy Diabetic Peripheral Neuropathy
Diabetic Foot Complications Podiatry Specialty Clinic YKHC Bethel, Alaska August 1-3, 2017 Charles C. Edwards, DPM Alaska Native Tribal Health Consortium Peripheral Neuropathy Diabetic Peripheral Neuropathy
Introduction to Saphenous Vein Ablations: When/Why/How?
 John Ligush, MD SMJH Vascular and Vein Center Introduction to Saphenous Vein Ablations: When/Why/How? Saphenous Vein Ablations: When/Why/How? Venous disease is easy Treatment is straightforward The patients
John Ligush, MD SMJH Vascular and Vein Center Introduction to Saphenous Vein Ablations: When/Why/How? Saphenous Vein Ablations: When/Why/How? Venous disease is easy Treatment is straightforward The patients
DON T LET LEG PAIN BECOME A REAL THREAT.
 DON T LET LEG PAIN BECOME A REAL THREAT. These three words have the power to change lives. Between 8 to 10 million Americans are estimated to suffer from poor blood flow to the legs and feet potentially
DON T LET LEG PAIN BECOME A REAL THREAT. These three words have the power to change lives. Between 8 to 10 million Americans are estimated to suffer from poor blood flow to the legs and feet potentially
John E. Campbell, MD. Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Boca Raton Regional Hospital Grand Rounds September 13, 2016
 Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Peripheral Arterial Disease: A Practical Approach
 Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
National Vascular Registry
 National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
ULCERS 1/12/ million diabetics in the US (2012) Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years
 Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years") Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
ATHEROSCLEROSIS. Secondary changes are found in other coats of the vessel wall.
 ATHEROSCLEROSIS Atherosclerosis Atherosclerosis is a disease process affecting the intima of the aorta and large and medium arteries, taking the form of focal thickening or plaques of fibrous tissue and
ATHEROSCLEROSIS Atherosclerosis Atherosclerosis is a disease process affecting the intima of the aorta and large and medium arteries, taking the form of focal thickening or plaques of fibrous tissue and
The present status of selfexpanding. for CLI: Why and when to use. Sean P Lyden MD Cleveland Clinic Cleveland, Ohio
 The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
RevIewS. Interventions for lower extremity peripheral artery disease
 RevIewS Interventions for lower extremity peripheral artery disease Jade S. Hiramoto 1, Martin Teraa 2, Gert J. de Borst 2 and Michael S. Conte 1 * Abstract Peripheral artery disease (PAD) of the lower
RevIewS Interventions for lower extremity peripheral artery disease Jade S. Hiramoto 1, Martin Teraa 2, Gert J. de Borst 2 and Michael S. Conte 1 * Abstract Peripheral artery disease (PAD) of the lower
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report G. Biro, M. Bosiers on behalf of ZILVERPASS Study Group Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report G. Biro, M. Bosiers on behalf of ZILVERPASS Study Group Disclosure Speaker
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI
 Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Disclosures. Critical Limb Ischemia. Vascular Testing in the CLI Patient. Vascular Testing in Critical Limb Ischemia UCSF Vascular Symposium
 Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
How to manage leg ulcers in the elderly
 How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Intended Learning Outcomes
 2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
Rapid Recovery Hyperbarics 9439 Archibald Ave. Suite 104 Rancho Cucamonga CA,
 Foot at risk Age Well By Dr LIEW NGOH CHIN Are limb amputations due to diabetes preventable? DIABETES mellitus is a major global health problem and has reached epidemic proportions in many developed and
Foot at risk Age Well By Dr LIEW NGOH CHIN Are limb amputations due to diabetes preventable? DIABETES mellitus is a major global health problem and has reached epidemic proportions in many developed and
Algorithm for Managing Acute Lower Extremity Ischemia. Peter A. Schneider, MD Honolulu, Hawaii
 Algorithm for Managing Acute Lower Extremity Ischemia Peter A. Schneider, MD Honolulu, Hawaii Disclosure Peter A. Schneider, MD... I have the following potential conflicts of interest to report: Consulting:
Algorithm for Managing Acute Lower Extremity Ischemia Peter A. Schneider, MD Honolulu, Hawaii Disclosure Peter A. Schneider, MD... I have the following potential conflicts of interest to report: Consulting:
Patient Brochure. Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland. PK Rev. 0 05/17
 Patient Brochure Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland PK1411100 Rev. 0 05/17 LIFESTREAM Patient Brochure If you or a member of your family has been diagnosed with
Patient Brochure Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland PK1411100 Rev. 0 05/17 LIFESTREAM Patient Brochure If you or a member of your family has been diagnosed with
Blood Vessels. Dr. Nabila Hamdi MD, PhD
 Blood Vessels Dr. Nabila Hamdi MD, PhD ILOs Understand the structure and function of blood vessels. Discuss the different mechanisms of blood pressure regulation. Compare and contrast the following types
Blood Vessels Dr. Nabila Hamdi MD, PhD ILOs Understand the structure and function of blood vessels. Discuss the different mechanisms of blood pressure regulation. Compare and contrast the following types
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
Lower Extremity Arterial Disease
 Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
National Clinical Conference 2018 Baltimore, MD
 National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
Clinical Approach to CLI and Related Diagnostics: What You Need to Know
 Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
MICHAEL R. JAFF, DO MASSACHUSETTS, UNITED STATES. Medtronic Further. Together
 DRUG-COATED BALL0ON TREATMENT FOR PATIENTS WITH INTERMITTENT CLAUDICATION: INSIGHTS FROM THE IN.PACT GLOBAL FULL CLINICAL COHORT MICHAEL R. JAFF, DO MASSACHUSETTS, UNITED STATES Medtronic Further. Together
DRUG-COATED BALL0ON TREATMENT FOR PATIENTS WITH INTERMITTENT CLAUDICATION: INSIGHTS FROM THE IN.PACT GLOBAL FULL CLINICAL COHORT MICHAEL R. JAFF, DO MASSACHUSETTS, UNITED STATES Medtronic Further. Together
Fluorescence Angiography in Limb Salvage
 Fluorescence Angiography in Limb Salvage Ryan H. Fitzgerald, DPM, FACFAS Associate Professor of Surgery-University Of South Carolina School of Medicine, Greenville Etiology of Lower extremity wounds Neuropathy
Fluorescence Angiography in Limb Salvage Ryan H. Fitzgerald, DPM, FACFAS Associate Professor of Surgery-University Of South Carolina School of Medicine, Greenville Etiology of Lower extremity wounds Neuropathy
Peripheral Arterial Disease: the growing role of endovascular management
 Peripheral Arterial Disease: the growing role of endovascular management Poster No.: C-1931 Congress: ECR 2012 Type: Educational Exhibit Authors: E. M. C. Guedes Pinto, E. Rosado, D. Penha, P. Cabral,
Peripheral Arterial Disease: the growing role of endovascular management Poster No.: C-1931 Congress: ECR 2012 Type: Educational Exhibit Authors: E. M. C. Guedes Pinto, E. Rosado, D. Penha, P. Cabral,
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT
 VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
Christian Wissgott MD, PhD Assistant Director, Radiology Westküstenkliniken Heide
 2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian