Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting
|
|
|
- Dulcie Marsh
- 6 years ago
- Views:
Transcription



1 Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA
2 Greg Maynard Disclosure SHM Glycemic Control Tools No personal financial interest -

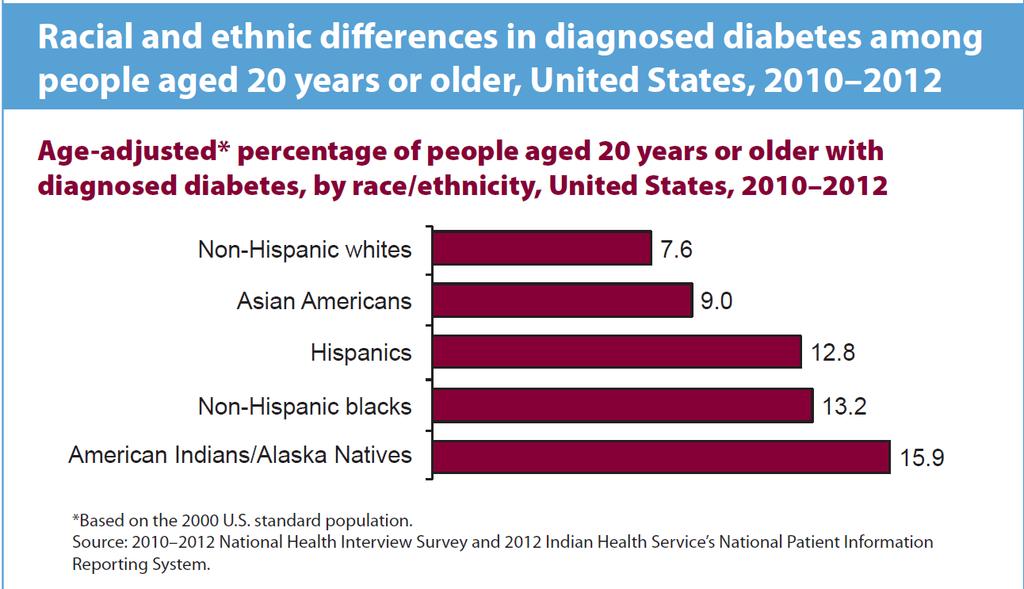
3 21 million in US with dx of DM 8.1 million with undiagnosed DM
4
5 Why Glycemic Control? (It s about more than infusion insulin glycemic targets!) DM / Hyperglycemia Very Common Opportunity to identify and intervene poorly controlled DM, previously undiagnosed DM, stress hyperglycemia (pre-diabetes) Hypoglycemia and extreme hyperglycemia Safety problem and a Quality problem Inpatient Care Complex w/ unique challenges Education alone insufficient, need systems change Huge Implementation Gap Chaotic baseline Public reporting, regulatory guidelines etc. pdf/gc_workbook.pdf.

6 Blood glucose >250 mg/dl Altered Mental Status Marked hypovolemia Electrolyte disturbances +/- Acidosis/Acidemia Underlying illness: Infection, MI, Stroke
7
8 Achieving good glycemic control AND low hypoglycemia Institutional / system support Will to standardize, goals, help with metrics Empowered centralized steering team Local teams addressing barriers Protocols / order sets Common approach for special populations and failure modes Metrics (balanced approach) Active surveillance (aka measure-vention) EHR tools Automation / closed loop algorithms / computerized glucose management
9 Algorithms Best practices to reinforce Actionable glycemic target Consistent carbohydrate / dietary / consult A1c Patient education plan Hypoglycemia protocol Guidance for transitions (linked protocols) Coordinated monitoring / nutrition / insulin DC oral agents, insulin preferred Insulin regimens for different conditions Dosing guidance
10 Glycemic Targets in Non-ICU Setting 1. Premeal BG target of <140 mg/dl and random BG <180 mg/dl for the majority of patients. 2. Glycemic targets be modified according to clinical status. For patients who achieve and maintain glycemic control without hypoglycemia, a lower target range may be reasonable. For patients with terminal illness and/or with limited life expectancy or at high risk for hypoglycemia, a higher target range (BG <200 mg/dl) may be reasonable. 3. For avoidance of hypoglycemia, we suggest that antidiabetic therapy be reassessed when BG values are 100 mg/dl). Modification of glucose-lowering treatment is usually necessary when BG values are <70 mg/dl. Endocrine Society Non-ICU Guideline. J Clin Endocrinol Metabol 97(1):16-38, 2012


11
12 A1C for Diagnosis of Diabetes in the Hospital In-hospital hyperglycemia is defined as an admission or inhospital BG > 140 mg/dl. A1c > 6.5% can be identified as having diabetes, < 5.2% can exclude diabetes. Implementation of A1C testing can be useful: assist with differentiation of newly diagnosed diabetes from stress hyperglycemia assess glycemic control prior to admission designing an optimal regimen at the time of discharge Moghissi ES, et al; AACE/ADA Endocr Pract. 2009;15(4). Umpierrez et al,. J Clin Endocrinol Metabol 97(1):16-38, 2012
13 Pharmacological Treatment of Hyperglycemia in Non-ICU Setting Antihyperglycemic Therapy SC Insulin Recommended for most medicalsurgical patients OADs Not Generally Recommended Continuous IV Infusion Selected medical-surgical patients 1.ACE/ADA Task Force on Inpatient Diabetes. 2.Diabetes Care & Umpierrez et al,. J Clin Endocrinol Metabol 97: January 2012

14

15 Source: University of California, San Diego Health System

16 Algorithmic guidance based on four simple factors Johns Hopkins example Source: Epic Electronic Medical Record. More at:
17 Pre-op recommendations for insulin treated patients with diabetes Give 70 to 100% of usual dose of glargine or detemir insulin or 50 to 70 % of NPH insulin PLEASE don t hold basal insulin altogether! Nurses, this means you too! For patients undergoing prolonged procedures (e.g. CABG) hold SQ insulin and start IV insulin infusion DiNardo MM et al Endo Pract 17:
18 Anesthesia and Analgesia :1041 Preoperative Fasting Guidelines: Why Are We Not Following Them?: The Time to Act Is NOW Ramon E. Abola, MD, and Tong J. Gan, MD, MHS, FRCA Your patient should be drinking clear liquids until 2 hours before surgery. If they are not, you should stop reading and change your hospital practices. Your patients will thank you. They will be less thirsty, be less anxious, and have improved patient satisfaction without an increase in the rate of pulmonary aspiration. 1 Traditional NPO after Midnight still common, but should it be?


19 Cochrane Collaboration review March 2014 Carb loading: Not just because it tastes good!
20 ASHP Foundation Recommendation Every hospital should prospectively monitor/measure: rates of hypoglycemia and hyperglycemia Insulin use patterns Coordination of insulin administration, glucose testing, and nutrition delivery Real-time, institution-wide glucose reports should be provided to health care team members to ensure appropriate surveillance and management of patients with unexpected hypoglycemia and hyperglycemia Cobaugh D, Maynard G, et al. Am J Health-Syst Pharm 2013;70:
21 Glucometrics Unit of measure Operational definitions Unit of analysis the individual reading (not recommended) the patient-day the patient-stay No consensus on best methods yet, but SHM offers a variety of measures Hypoglycemia:< 70 mg/dl Severe hypoglycemia: < 40 mg/dl DWM 180 mg/dl Percent patient-days with BG > 299 mg/dl Recurrent hypoglycemia: > 1 hypoglycemic day


22 Society of Hospital Medicine: Data / Reporting for Glucometrics, Community, and More

23 Benchmarking Ranking Bar Chart Hypoglycemia Rates
 How do these hospitals get low hypoglycemia AND good glycemic control?")
24 SHM Benchmarking Hypoglycemia (x axis) Scatterplot Uncontrolled Hyperglycemia (y axis) How do these hospitals get low hypoglycemia AND good glycemic control?
25 Iatrogenic Hypoglycemia A Top Source of Inpatient Adverse Drug Events (ADEs) ADEs: most common cause of inpatient complications affecting 1.9 million stays annually costing $4.2 billion / year responsible for 1/3 of hospital acquired conditions (HACs) % of ADEs are preventable 57% of ADEs are from hypoglycemic agents > 10% of those on a hypoglycemic agent suffer at least one hypoglycemic ADE Classen DC et al. Health Aff (Millwood) 2011;30: Agency for Healthcare Research and Quality, Rockville, MD, 2011 April. HCUP Statistical Brief #109. Classen DC et al. JAMA 997;277: Bates DW et al. JAMA 1997;277: Classen et al. Jt Comm J Qual Patient Saf. 2010;36:12-21
26 Hypoglycemia Risk Factors Different Flavors Inherent Low BMI / cachexia / Advanced Malignancy / Age Liver / Kidney disease / CHF Iatrogenic Insulin / oral agents Some risk with appropriate use. Risk magnified with inappropriate use or failure to react / anticipate preventable problems. Overly aggressive targets, inappropriate prescribing Hypoglycemic (< 70 mg/dl) events - 50% preventable Severe Hypoglycemic events ( < 40 mg/dl) % preventable Improved Glycemic Control AND Reduced Hypoglycemia possible.
27 Iatrogenic Hypoglycemia from Insulin Most common failures and strategies to address them Inappropriate prescribing Standardized orders with embedded CDS mandatory use Ongoing monitoring for inappropriate prescribing, just in time intervention Failure to respond to unexpected nutritional interruption Protocols and Education Methods to reduce interruptions in tube feeding Poor coordination of nutrition delivery, monitoring, and insulin delivery Clear directions in protocols and order sets Regular education / competency training Redesign process Failure to respond to a prior hypoglycemic day Make sure ASSESSMENT is part of hypoglycemia protocol Competency and case based-training Monitor recurrent hypoglycemia rates Cobaugh DJ et al. Am J Health Syst Pharm;70(16): Hellman R. Endocr Pract 2004;10 Suppl 2: Maynard GA, et. Diabetes Spectr 2008;
28 Impact of Hypoglycemia Reduction Bundle and a Systems Approach to Inpatient Glycemic Management Greg Maynard, MD, MS, SFHM 1,2 ; Kristen Kulasa, MD 3 ; Pedro Ramos, MD 1 ; Diana Childers, MD 1 ; Brian Clay, MD 1 ; Meghan Sebasky, MD 1 ; Ed Fink MHSM 2 ; Aaron Field 2 ; Marian Renvall, MS 2 ; Patricia S. Juang, MD 3 ; Charles Choe, MD 3 ; Diane Pearson, RN, BSN, MPH, PHN, CDE 4 ; Brittany Serences, MSC, RN, FNP-BC, BC-ADM 4 ; Suzanne Lohnes, MA, BSN, RN, CDE 4 RR 2013 vs baseline hypoglycemic stay 0.71 (0.65,0.79) severe hypoglycemic stay 0.44 (0.34,0.58) recurrent hypoglycemia 0.78 (0.64,0.94) hypoglycemic day 0.73 (0.66,0.79) severe hypoglycemic day 0.48 (0.37,0.62) Days with BG > 299 mg/dl 0.76 (0.73,0.80)

29
30 New BPA for Tube Feedings on hold + Insulin Appears for pt s w/ 0 charted for TF rate + on insulin Hypoglycemic Risk Patient is at risk for hypoglycemia since on insulin and tube feeds held. Please refer to the insulin and nutrition on hold unexpectedly guidelines. Potential Problems RNs don t consistently chart TF interruptions in I/O Charting, if done, not always timely Source: University of California, San Diego Health System

31 Source: University of California, San Diego Health System

32 Source: University of California, San Diego Health System

33 Source: University of California, San Diego Health System STROKE CODE June 10

34 Recurrent hypoglycemia on same insulin doses for several days preceding stroke code Source: University of California, San Diego Health System
35 Proposed CDS Display for Hypoglycemia Evaluation Federal Interagency Workgroup to Prevent ADE Report etiology of hypoglycemic event after event resolution Etiology of hypoglycemic event Nutritional interruption without reducing insulin or adding carbohydrate Prior hypoglycemic event without medication or carbohydrate adjustment Excessive basal insulin dosing that inappropriately covered nutritional needs, as well as basal needs Glycemic target that is too stringent for patient condition/co-morbidities Failure to discontinue oral hypoglycemic agents in the inpatient setting Time interval between testing was too long Other failure mode: No preventable factors detected Report ACTION taken to MITIGATE hypoglycemia ACTION Call to reduce hypoglycemic agent Call to increase CHO Education/reinforcement of policy/protocols Other


36 Why was patient Hypoglycemic? Critical Thinking to prevent next episode! Source: University of California, San Diego Health System
37 Active Surveillance Identify patients with a potential deficit in care, who are in the hospital right now. Triage tools to quickly determine if the patient is truly uncontrolled or off protocol. Intervene to bring onto protocol, reduce risk of glycemic excursions and continued deficits in care, provide just in time education. aka measure-vention

38 Glucose Rounding Report Dashboard RED: Any POC Glucose result in the past 24 hours > 299 OR Any POC Glucose result in the past 24 hours < 70 YELLOW: Any POC Glucose result in the past 24 hours between Or Any POC Glucose result in the past 24 hours between GREEN: All POC Glucose result in the past 24 hours between Source: Epic Electronic Medical Record. More at:
39 Annals of Internal Medicine ORIGINAL RESEARCH Association Between a Virtual Glucose Management Service and Glycemic Control in Hospitalized Adult Patients An Observational Study Robert J. Rushakoff, MD; Mary M. Sullivan, DNP; Heidemarie Windham MacMaster, PharmD; Arti D. Shah, MD; Alvin Rajkomar, MD; David V. Glidden, PhD; and Michael A. Kohn, MD, MPP Big Brother Daily Reports: 2 or more glucoses>225 Glucose <70 On insulin pump Dx type 1 DM

40 Source: Epic Electronic Medical Record. More at:
41 Annals of Internal Medicine ORIGINAL RESEARCH Association Between a Virtual Glucose Management Service and Glycemic Control in Hospitalized Adult Patients An Observational Study Robert J. Rushakoff, MD; Mary M. Sullivan, DNP; Heidemarie Windham MacMaster, PharmD; Arti D. Shah, MD; Alvin Rajkomar, MD; David V. Glidden, PhD; and Michael A. Kohn, MD, MPP The Impact of the Virtual Glucose Management Services Decrease in Hyperglycemia: 39% decrease in number of patients on daily hyperglycemia morning list Decrease in Hypoglycemia: 38% decrease in glucoses >70 mg/dl* 64% decrease in glucoses >40 mg/dl* (only 15 total last year) Decreased by 50% number of patients with high glucoses for more than 1 day Decreased by 40% the time patients remain hyperglycemic Ann Inter Med May 2; 166(9):
42 Factors to consider in crafting transition regimen Outpatient regimen / control Major changes from recent illness / hospitalization Inpatient regimen / control Changing stress levels, weaning prednisone A1c Patient preferences Financial / social / insurance picture Access to follow up Patients with poor health literacy, new insulin, and advanced age at highest risk of transitional problems
43 Transition Guide Inpatient to Outpatient Regimen A1c <7% A1c 7-10%* Return to same regimen as prior to admission (oral agents and/or insulin) Restart outpatient oral agents, optimize orals, consider adding basal insulin once daily at 50% inpt dose A1c >10%* Restart outpatient oral agents, optimize orals, add basal insulin once daily at 75% inpt dose Alternative: stop orals and start 70/30 or basal/bolus at same inpt dose *Ensure compliance with home regimen, maximize lifestyle changes, optimize orals and add insulin according to funding, compliance and lifestyle on individual basis Adapted with permission from algorithm by Umpierrez, G.,Emory University School of Medicine, 2011.

44 Additional Discharge Orders for Diabetic Patients Most defaults on these orders are already set in order to save clicks. These are ambulatory orders/prescriptions; they file to the After Visit Summary. Source: University of California, San Diego Health System
45 EDRP at Boston Medical Center Emergency Department Diabetes Rapid Referral Program Acute Management 10/2011 Education Follow-up


46 How the EDRP Model Works There is a 10 a.m. and a 2 p.m. slot in the diabetes clinic. This is part of your ED care Can you commit to going to this appointment? Case Managers in the ED can directly book into generic Acute Diabetes provider slots (10 a.m. and 2 p.m. M F)
47
48 Computerized Glucose Management Now available for IV, SubQ, and Transitions Timely adjustment of dosing Adjusts for variable carbohydrate intake Embedded glucometrics Improved glycemic control with low hypoglycemia rates in research and real world settings CV Surgery J Diabetes Sci Technol 2(3); Basal bolus J Diabetes Sci Technol 11(1) Coronary Artery Bypass Graphs (CABG) J Diabetes Complications (4): CABG Diabetes Care (9): BMT Bone Marrow Transplant 2016 S1,

49 Now Available at the Society of Hospital Medicine Glycemic Control Website Best Practice Review Assess Current State Metrics and Data Collection High Performing Teams SC Insulin Orders / Protocols Insulin infusion protocols DKA protocols / order sets Perioperative DM management Transitions and Reliability Education programs Hypoglycemia reduction bundle Coordination of nutrition / insulin Insulin pens Insulin pumps Example order sets and tools
50 Questions and Comments? Thank you!
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting
 Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Hypoglycemia Prevention and Management - Measurement that Matters and the Power of Collaboration
 Hypoglycemia Prevention and Management - Measurement that Matters and the Power of Collaboration Greg Maynard M.D., Clinical Professor of Medicine Director, UCSD Center for Innovation and Improvement Science
Hypoglycemia Prevention and Management - Measurement that Matters and the Power of Collaboration Greg Maynard M.D., Clinical Professor of Medicine Director, UCSD Center for Innovation and Improvement Science
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting
 Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING
 Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
HAP PA-HEN Achieving More Together
 HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
Special Situations 1
 Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes
 Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes Kristi Kulasa, MD Associate Clinical Professor of Medicine Director, Inpatient Glycemic Control University of California
Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes Kristi Kulasa, MD Associate Clinical Professor of Medicine Director, Inpatient Glycemic Control University of California
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
Improving Glycemic Control in the Critical Care
 Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
Society of Hospital Medicine. to Jumpstart Hospitals
 Using Society of Hospital Medicine (SHM) Mentors to Jumpstart Hospitals to Improve Glycemic Control Society of Hospital Medicine Edited by: Pedro Ramos, MD, FHM Jane Jeffrie Seley, DNP, MPH, BC-ADM, CDE,
Using Society of Hospital Medicine (SHM) Mentors to Jumpstart Hospitals to Improve Glycemic Control Society of Hospital Medicine Edited by: Pedro Ramos, MD, FHM Jane Jeffrie Seley, DNP, MPH, BC-ADM, CDE,
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia
 Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia Shiv Patil, MD, MPH, BC-ADM Clinical Assistant Professor of Family Medicine Brody School of Medicine at East Carolina
Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia Shiv Patil, MD, MPH, BC-ADM Clinical Assistant Professor of Family Medicine Brody School of Medicine at East Carolina
123 Are You Providing Evidence-Based Diabetes Care? - Martin
 Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Deepika Reddy MD Department of Endocrinology
 Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
ANNUAL MEETING 2 #FSHP2017
 FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
9/23/09. What are the key components of preoperative, intraoperative, & postoperative care of diabetes management? Rebecca L. Sturges, M.D.
 RMHS Perioperative Summit: Perioperative Diabetes Management Rebecca L. Sturges, M.D. Oct 6, 2009 Mrs. B was referred by her orthopedic surgeon to your preoperative clinic to discuss medical management
RMHS Perioperative Summit: Perioperative Diabetes Management Rebecca L. Sturges, M.D. Oct 6, 2009 Mrs. B was referred by her orthopedic surgeon to your preoperative clinic to discuss medical management
Avoiding Hypoglycemia Kristen Kulasa, MD
 Avoiding Hypoglycemia Kristen Kulasa, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: Kulasa can come on up and she can take it from here. You have your thing and there's slides. OK. Thanks. KRISTEN
Avoiding Hypoglycemia Kristen Kulasa, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: Kulasa can come on up and she can take it from here. You have your thing and there's slides. OK. Thanks. KRISTEN
Section of Endocrinology, Rush University Medical Center, Chicago, Illinois.
 ORIGINAL RESEARCH Treatment of Inpatient Hyperglycemia Beginning in the Emergency Department: A Randomized Trial Using Insulins Aspart and Detemir Compared With Usual Care Jennifer B. Bernard, MD Christina
ORIGINAL RESEARCH Treatment of Inpatient Hyperglycemia Beginning in the Emergency Department: A Randomized Trial Using Insulins Aspart and Detemir Compared With Usual Care Jennifer B. Bernard, MD Christina
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, :30 a.m. 11:15 a.m.
 Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, 2018 10:30 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US.
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, 2018 10:30 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US.
Welcome Everyone. Monitoring, Sick Days, Inpatient Management - Objectives. Mrs. Jones has new diabetes. She asks you: Page 1
 Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς
 Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin
 Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin David Newman, MD University of North Dakota School of Medicine Sanford Health Big Sky Conference 2017 Dr. David Newman, Personal/Professional
Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin David Newman, MD University of North Dakota School of Medicine Sanford Health Big Sky Conference 2017 Dr. David Newman, Personal/Professional
LIBERTYHEALTH. Jersey City Medical Center Department of Patient Care Services. Approved by Policy Committee:
 LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
A Call to Action: Addressing Diabetes Medication Safety
 A Call to Action: Addressing Diabetes Medication Safety Evan M. Klass, M.D., F.A.C.P. Senior Associate Dean, Statewide Initiatives Reducing ED visits for insulin induced hypoglycemia is a Healthy People
A Call to Action: Addressing Diabetes Medication Safety Evan M. Klass, M.D., F.A.C.P. Senior Associate Dean, Statewide Initiatives Reducing ED visits for insulin induced hypoglycemia is a Healthy People
Lessons Learned: Interdisciplinary collaboration to reduce hypoglycemic events
 Lessons Learned: Interdisciplinary collaboration to reduce hypoglycemic events Ryan ull, Pharm.., BCPS ssistant Professor of Pharmacy Practice Creighton niversity School of Pharmacy legent Health Lakeside
Lessons Learned: Interdisciplinary collaboration to reduce hypoglycemic events Ryan ull, Pharm.., BCPS ssistant Professor of Pharmacy Practice Creighton niversity School of Pharmacy legent Health Lakeside
Improved IPGM: Demonstrating the Value to both Patients and Hospitals
 Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Sixth International Hospital Diabetes Meeting
 Sixth International Hospital Diabetes Meeting May 19-20, 2017 Georgia Tech Hotel & Conference Center, Atlanta, Georgia Friday May 19, 2017 08:00 Welcome David C. Klonoff, MD, FACP, FRCP (Edin), Fellow
Sixth International Hospital Diabetes Meeting May 19-20, 2017 Georgia Tech Hotel & Conference Center, Atlanta, Georgia Friday May 19, 2017 08:00 Welcome David C. Klonoff, MD, FACP, FRCP (Edin), Fellow
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, :30 a.m. 11:15 a.m.
 Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 1, 218 1:3 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US. About
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 1, 218 1:3 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US. About
Transforming Diabetes Care
 Transforming Diabetes Care Meeting the Challenge of Inpatient Glycemic Management in the Critical Care Setting Jane Jeffrie Seley, DNP, MSN, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner,
Transforming Diabetes Care Meeting the Challenge of Inpatient Glycemic Management in the Critical Care Setting Jane Jeffrie Seley, DNP, MSN, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner,
Learning Objectives. Perioperative SWEET Success
 Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
In - Hospital Diabetes Care. A review and personal experience
 In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
5/15/2018 DISCLOSURE OBJECTIVES. FLORIDA HOSPITAL ORLANDO Not for profit organization Acute care medical center 1,368 licensed beds BACKGROUND
 DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
Welcome to CareLink Pro
 Reference Guide Welcome to CareLink Pro This guide was developed to serve as a reference for obtaining patient data and reviewing CareLink Pro reports. Getting Started with CareLink Pro Adding New Patients
Reference Guide Welcome to CareLink Pro This guide was developed to serve as a reference for obtaining patient data and reviewing CareLink Pro reports. Getting Started with CareLink Pro Adding New Patients
Glycemic Control Insulin In The Hospital Setting
 Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Improving Glycemic Control and Insulin Ordering Efficiency for Hospitalized Patients With Diabetes Through Carbohydrate Counting
 e1 Improving Glycemic Control and Insulin Ordering Efficiency for Hospitalized Patients With Diabetes Through Carbohydrate Counting Kristina K. Pearson, Sarah A. Reiland, John G. O Meara, Julie K. Brown,
e1 Improving Glycemic Control and Insulin Ordering Efficiency for Hospitalized Patients With Diabetes Through Carbohydrate Counting Kristina K. Pearson, Sarah A. Reiland, John G. O Meara, Julie K. Brown,
Implementing Hospital Policies & Protocols
 Implementing Hospital Policies & Protocols Jane Jeffrie Seley DNP MPH GNP BC-ADM CDE CDTC FAADE FAAN Division of Endocrinology, Diabetes & Metabolism NewYork-Presbyterian Hospital Weill Cornell Medicine
Implementing Hospital Policies & Protocols Jane Jeffrie Seley DNP MPH GNP BC-ADM CDE CDTC FAADE FAAN Division of Endocrinology, Diabetes & Metabolism NewYork-Presbyterian Hospital Weill Cornell Medicine
BACKGROUND: Structured subcutaneous insulin order sets and insulin protocols
 ORIGINAL RESEARCH Improved Inpatient Use of Basal Insulin, Reduced Hypoglycemia, and Improved Glycemic Control: Effect of Structured Subcutaneous Insulin Orders and an Insulin Management Algorithm Greg
ORIGINAL RESEARCH Improved Inpatient Use of Basal Insulin, Reduced Hypoglycemia, and Improved Glycemic Control: Effect of Structured Subcutaneous Insulin Orders and an Insulin Management Algorithm Greg
Impact of an Interactive Online Nursing Educational Module on Insulin Errors in Hospitalized Pediatric Patients
 Diabetes Care Publish Ahead of Print, published online May 26, 2010 Impact of an Interactive Online Nursing Educational Module on Insulin Errors in Hospitalized Pediatric Patients Short Title: Impact of
Diabetes Care Publish Ahead of Print, published online May 26, 2010 Impact of an Interactive Online Nursing Educational Module on Insulin Errors in Hospitalized Pediatric Patients Short Title: Impact of
Disclosures. Glycemic Control in the Intensive Care Unit. Objectives. Hyperglycemia. Hyperglycemia. History. No disclosures
 Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
In Brief. From Research to Practice/Inpatient Care of Hyperglycemia and Diabetes
 In Brief We performed a 130-patient case-control study to examine the patient and hospital care risk factors for experiencing a hypoglycemic patient-day, comparing these factors to similar control patients
In Brief We performed a 130-patient case-control study to examine the patient and hospital care risk factors for experiencing a hypoglycemic patient-day, comparing these factors to similar control patients
April Dear (Editor):
:") April 2014 Dear (Editor): Registered Dietitians (RD) play an integral role in patient care in the medical intensive care unit. RD s have increased knowledge in blood glucose control and reducing adverse
April 2014 Dear (Editor): Registered Dietitians (RD) play an integral role in patient care in the medical intensive care unit. RD s have increased knowledge in blood glucose control and reducing adverse
Hypoglycemia Reduction STARTER PACK WEBINAR #1
 Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Report Reference Guide
 Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
Topics in Inpatient Glycemic Control
 Topics in Inpatient Glycemic Control Jane Jeffrie Seley DNP MPH MSN GNP BC-ADM CDE CDTC FAADE FAAN Diabetes Nurse Practitioner Program Manager, Inpatient Glycemic Control Program NewYork-Presbyterian/
Topics in Inpatient Glycemic Control Jane Jeffrie Seley DNP MPH MSN GNP BC-ADM CDE CDTC FAADE FAAN Diabetes Nurse Practitioner Program Manager, Inpatient Glycemic Control Program NewYork-Presbyterian/
4/10/2015. Foundations to Managing Inpatient Hyperglycemia. Learning Objectives
 Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions
 Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting:
 T h e E n d o c r i n e S o c i e t y s Clinical Guidelines Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline Authors:
T h e E n d o c r i n e S o c i e t y s Clinical Guidelines Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline Authors:
6/9/2016. Activating Hospital Staff & Physicians to Support Diabetes Education in the Hospital and Through Transition. Diabetes in Scripps Hospitals
 Disclosure to Participants Notice of Requirements For Successful Completion Please refer to learning goals and objectives Learners must attend the full activity and complete the evaluation in order to
Disclosure to Participants Notice of Requirements For Successful Completion Please refer to learning goals and objectives Learners must attend the full activity and complete the evaluation in order to
Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine
 The Approach to Inpatient Hyperglycemia Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine Great Lakes Hospital Medical Symposium May 7th 2010 Further Increases in the Prevalence of Diabetes
The Approach to Inpatient Hyperglycemia Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine Great Lakes Hospital Medical Symposium May 7th 2010 Further Increases in the Prevalence of Diabetes
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events. November 12, 2016
 Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events November 12, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events November 12, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Evidence for Basal Bolus Insulin Versus Slide Scale Insulin
 Curr Emerg Hosp Med Rep (2014) 2:26 34 DOI 10.1007/s40138-013-0032-4 DIABETES AND METABOLIC DISEASE (W FORD, SECTION EDITOR) Evidence for Basal Bolus Insulin Versus Slide Scale Insulin Sameer Badlani William
Curr Emerg Hosp Med Rep (2014) 2:26 34 DOI 10.1007/s40138-013-0032-4 DIABETES AND METABOLIC DISEASE (W FORD, SECTION EDITOR) Evidence for Basal Bolus Insulin Versus Slide Scale Insulin Sameer Badlani William
Hypoglycemia Reassessment at Orange Regional Medical Center
 What is the Society of Medicine s Glycemic Control equips Program? The Society of Medicine s (SHM s) Glycemic Control Electronic Quality Improvement Program (GC equips) assists with optimizing glycemic
What is the Society of Medicine s Glycemic Control equips Program? The Society of Medicine s (SHM s) Glycemic Control Electronic Quality Improvement Program (GC equips) assists with optimizing glycemic
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE TREATMENT OF HYPERGLYCEMIA - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity & Nutrition Strategic Clinical Network PARENT
TITLE TREATMENT OF HYPERGLYCEMIA - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity & Nutrition Strategic Clinical Network PARENT
Glycemic Control Hitting the Sweet Spot During Inpatient Care
 Glycemic Control Hitting the Sweet Spot During Inpatient Care Tim R. Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Family Medicine Cleveland Clinic Akron General Professor, Northeast
Glycemic Control Hitting the Sweet Spot During Inpatient Care Tim R. Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Family Medicine Cleveland Clinic Akron General Professor, Northeast
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events. September 13, 2016
 Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events September 13, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events September 13, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It
 The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
Physical Activity/Exercise Prescription with Diabetes
 Physical Activity/Exercise Prescription with Diabetes B R AD H I NTERMEYER C E P A C SM S A NFORD H E ALTH C A RDIAC R E H AB A N D D I ABE TES E XE RCISE The adoption and maintenance of physical activity
Physical Activity/Exercise Prescription with Diabetes B R AD H I NTERMEYER C E P A C SM S A NFORD H E ALTH C A RDIAC R E H AB A N D D I ABE TES E XE RCISE The adoption and maintenance of physical activity
Parenteral Nutrition The Sweet and Sour Truth. From: Division of Endocrinology, Diabetes and Bone Disease Icahn School of Medicine at Mount Sinai
 ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset
ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Glucose Management in the ICU: The Role of the Pharmacist
 Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
CareLink. software REPORT REFERENCE GUIDE. Management Software for Diabetes
 CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL
 AUDIT TOOL") DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL Facility: Date: Data Collector s name: Email/Phone: Purpose: To evaluate your facility practices regarding communication of requisite diabetes
DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL Facility: Date: Data Collector s name: Email/Phone: Purpose: To evaluate your facility practices regarding communication of requisite diabetes
Peripartum and Postpartum Management of Diabetes
 Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
Glycemic care pathway patient and/or Diabetes noted preoperatively. confirm BG order / write order holding area. TARGET mg/dL
 BG check options POCT glucometer (pre/pacu) POCT istat (intraop) venous/arterial BG venous BG (lab) Glycemic care pathway patient and/or Diabetes noted preoperatively confirm BG order / write order holding
BG check options POCT glucometer (pre/pacu) POCT istat (intraop) venous/arterial BG venous BG (lab) Glycemic care pathway patient and/or Diabetes noted preoperatively confirm BG order / write order holding
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical
 Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
Disclosure. Disclosure. Disclosure. Course Outline. Objectives. A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings 7/25/2013
 47 th Annual Meeting August 2-4, 2013 Orlando, FL A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings Kevin Forbush, Pharm. D Central Maine Medical Center Lewiston, Maine Disclosure I do
47 th Annual Meeting August 2-4, 2013 Orlando, FL A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings Kevin Forbush, Pharm. D Central Maine Medical Center Lewiston, Maine Disclosure I do
Diabetes Survival Skills
 Promoting Patient Survival with Diabetes Survival Skills Need to know skills for persons with diabetes Susan Zontine, NP-C WMC Diabetes Stewardship team May 18, 2015 Diabetes Chronic illness with serious
Promoting Patient Survival with Diabetes Survival Skills Need to know skills for persons with diabetes Susan Zontine, NP-C WMC Diabetes Stewardship team May 18, 2015 Diabetes Chronic illness with serious
The Art and Science of Infusion Nursing Gwen Klinkner, MS, RN, APRN, BC-ADM, CDE
 The Art and Science of Infusion Nursing Gwen Klinkner, MS, RN, APRN, BC-ADM, CDE The Importance of Glycemic Control in the Hospital and the Role of the Infusion Nurse ABSTRACT Diabetes is reaching epidemic
The Art and Science of Infusion Nursing Gwen Klinkner, MS, RN, APRN, BC-ADM, CDE The Importance of Glycemic Control in the Hospital and the Role of the Infusion Nurse ABSTRACT Diabetes is reaching epidemic
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
9/16/2013. No Conflict of Interest to Disclose
 Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
GLYCEMIC CONTROL SURVEY
 GLYCEMIC CONTROL SURVEY Objective: To gain an understanding of the current state of glycemic control (ie, intensive insulin therapy and frequent blood glucose testing) protocol use in hospital inpatients.
GLYCEMIC CONTROL SURVEY Objective: To gain an understanding of the current state of glycemic control (ie, intensive insulin therapy and frequent blood glucose testing) protocol use in hospital inpatients.
Inpatient Glycemic Management 2016
 2016 Jim Chamberlain MD Medical Director for Diabetes Services St. Mark s Hospital and St. Mark s Diabetes Center Salt Lake City, Utah Disclosures Speakers Bureaus Merck & Co. Janssen Pharmaceutical Companies
2016 Jim Chamberlain MD Medical Director for Diabetes Services St. Mark s Hospital and St. Mark s Diabetes Center Salt Lake City, Utah Disclosures Speakers Bureaus Merck & Co. Janssen Pharmaceutical Companies
Diabetic Ketoacidosis (DKA) Critical Care Guideline Two Bag System
 Critical Care Guideline Two Bag System") Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Glucose Management in NON-ICU Hospitalized Patients
 Glucose Management in NON-ICU Hospitalized Patients October 15, 2016 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill Cornell
Glucose Management in NON-ICU Hospitalized Patients October 15, 2016 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill Cornell
Report Reference Guide. THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1
 Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care
 Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Director of Evidence-Based Outcomes
Session 15 Improved Outcomes and a Proven ROI Model for Quality Improvement: Transforming Diabetes Care Charles G Macias MD, MPH Chief Clinical Systems Integration Officer Director of Evidence-Based Outcomes
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
Intensive Insulin in the Intensive Care Unit
 TABLE OF CONTENTS Introduction to Intensive Insulin in Adult Critical Care Patients - UIMCC Guideline for Insulin Infusion in Adult ICU Patients - P&T Committee Formulary Action Intensive Insulin in the
TABLE OF CONTENTS Introduction to Intensive Insulin in Adult Critical Care Patients - UIMCC Guideline for Insulin Infusion in Adult ICU Patients - P&T Committee Formulary Action Intensive Insulin in the
Recent Advances in the Management of Diabetes
 Recent Advances in the Management of Diabetes Raja Hanania, R.Ph,CDM,CDE,LDE,BCPS Clinical Pharmacy Specialist IU Health Bloomington Hospital Bloomington, Indiana Indiana Pharmacists Alliance Annual Convention
Recent Advances in the Management of Diabetes Raja Hanania, R.Ph,CDM,CDE,LDE,BCPS Clinical Pharmacy Specialist IU Health Bloomington Hospital Bloomington, Indiana Indiana Pharmacists Alliance Annual Convention
Ask the Experts: Real-world Approaches for Managing Hyperglycemia in Hospitalized Patients
 Ask the Experts: Real-world Approaches for Managing Hyperglycemia in Hospitalized Patients Presented as a Live Webinar Wednesday, March 19, 2014 1:00 p.m. 2:00 p.m. ET Planned and conducted by ASHP Advantage
Ask the Experts: Real-world Approaches for Managing Hyperglycemia in Hospitalized Patients Presented as a Live Webinar Wednesday, March 19, 2014 1:00 p.m. 2:00 p.m. ET Planned and conducted by ASHP Advantage
How to manage type 2 diabetes in medical and surgical patients in the hospital
 MEDICAL GRAND ROUNDS CME CREDIT EDUCATIONAL OBJECTIVE: Readers will learn the relationship between glycemic control and clinical outcomes in hospitalized medical and surgical patients who are not in an
MEDICAL GRAND ROUNDS CME CREDIT EDUCATIONAL OBJECTIVE: Readers will learn the relationship between glycemic control and clinical outcomes in hospitalized medical and surgical patients who are not in an
Insulin Delivery and Glucose Monitoring Methods for Diabetes Mellitus: Comparative Effectiveness
 Insulin Delivery and Glucose Monitoring Methods for Diabetes Mellitus: Comparative Effectiveness Prepared for: Agency for Healthcare Research and Quality (AHRQ) www.ahrq.gov Outline of Material Introduction
Insulin Delivery and Glucose Monitoring Methods for Diabetes Mellitus: Comparative Effectiveness Prepared for: Agency for Healthcare Research and Quality (AHRQ) www.ahrq.gov Outline of Material Introduction
Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action
 Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action Learning Objectives Identify patient situations where specific attention to glycemic control is warranted Determine
Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action Learning Objectives Identify patient situations where specific attention to glycemic control is warranted Determine
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial
 Trial") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI Agenda General protocol for control group/ intervention group Discussion of meals Hypoglycemia
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI Agenda General protocol for control group/ intervention group Discussion of meals Hypoglycemia
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
Accurate Timing of Insulin Administration.
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Accurate Timing of Insulin Administration. Elizabeth Ajamu BSN, RN Lehigh Valley Health Network, elizabeth_o.ajamu@lvhn.org
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Accurate Timing of Insulin Administration. Elizabeth Ajamu BSN, RN Lehigh Valley Health Network, elizabeth_o.ajamu@lvhn.org
What s so sweet about glycemic control? June 3, 2016
 What s so sweet about glycemic control? June 3, 2016 Objectives Provide an overview of why glucose control is important in surgical patient outcomes. Demonstrate an understanding of how anesthetics and
What s so sweet about glycemic control? June 3, 2016 Objectives Provide an overview of why glucose control is important in surgical patient outcomes. Demonstrate an understanding of how anesthetics and
Targeting Glycemic Control in Non-Critically Ill Patients at a Tertiary Teaching Hospital. Brian Gilbert, Pharm.D. PGY-1 Pharmacy Resident
 Targeting Glycemic Control in Non-Critically Ill Patients at a Tertiary Teaching Hospital Brian Gilbert, Pharm.D. PGY-1 Pharmacy Resident Objectives Discuss rationale for the development of a glycemic
Targeting Glycemic Control in Non-Critically Ill Patients at a Tertiary Teaching Hospital Brian Gilbert, Pharm.D. PGY-1 Pharmacy Resident Objectives Discuss rationale for the development of a glycemic
AACE Module on Patient Safety in Inpatient Diabetes Care
 AACE Module on Patient Safety in Inpatient Diabetes Care Richard Hellman, MD, FACP, FACE Past President, American Association of Clinical Endocrinologists Clinical Professor of Medicine, University of
AACE Module on Patient Safety in Inpatient Diabetes Care Richard Hellman, MD, FACP, FACE Past President, American Association of Clinical Endocrinologists Clinical Professor of Medicine, University of
The most recent estimates suggest that. A study of inpatient diabetes care on medical wards. Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal
 A study of inpatient diabetes care on medical wards Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal Article points 1. It is well established that poor glycaemic control is associated with increased
A study of inpatient diabetes care on medical wards Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal Article points 1. It is well established that poor glycaemic control is associated with increased
The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles
 The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles Linda M. Siminerio, RN, PhD, CDE Professor of Medicine University of Pittsburgh School of Medicine & Nursing Objectives
The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles Linda M. Siminerio, RN, PhD, CDE Professor of Medicine University of Pittsburgh School of Medicine & Nursing Objectives
Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes
 Organization: Solution Title: Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes Program/Project Description:What was the problem to be solved? How was
Organization: Solution Title: Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes Program/Project Description:What was the problem to be solved? How was