Improving Glycemic Control in the Critical Care
|
|
|
- Allen Ernest Hudson
- 6 years ago
- Views:
Transcription

1 Improving Glycemic Control in the Critical Care Setting /Hospitalists
2 Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition from IV to SQ insulin Special Situations
3 Society of Hospital Medicine Guidelines Antihyperglycemic Therapy Any patient with a blood glucose >180 Check every patient at least once Insulin Recommended Oral Hypoglycemics Not appropriate Intravenous Insulin Critically ill patients Goal Subcutaneous Insulin Non-critically ill patients Scheduled Daily Dose As needed SHM Glycemic Control Task Force. The Glycemic Control Implementation Guide: Improving Glycemic Control, Preventing Hypoglycemia, and Optimizing Care of the Inpatient with Hyperglycemia and Diabetes. Society of Hospital Medicine website, Glycemic Control Quality Improvement implementation toolkit accessed 04/08/2017 Basal Nutritional Correctional
4 ADA/SCC Target Glucose Levels in Critical Care/ICU Patients American Diabetes Association Starting threshold >180 mg/dl Once IV insulin is started, glucose level should be maintained between 140 and 180 mg/dl Lower glucose targets ( mg/dl) may be appropriate in selected patients Targets <110 mg/dl or >180 mg/dl are not recommended Society of Critical Care Medicine Starting threshold of >150 mg/dl and absolutely at 180 mg/dl Use protocol to achieve low rate of hypoglycemia <70 mg/dl Minimal excursions of <100 mg/dl 1. Diabetes Care 2016; 39 (Suppl. 1):S99- S Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit. Care Med 2012 Vol 40, No 12. Not recommended < Acceptable Recommended Not recommended >180
5 Insulin Infusions: Indications DKA/HHS; aggressive and intended to lower blood glucose rapidly Critical Illness with hyperglycemia; initiate infusion when BG: ADA/AACE: BG >180 mg/dl SCCM: BG >150 mg/dl 1. Diabetes Care 2016; 39 (Suppl. 1):S99-S Guidelines for the use of an insulin infusion for the management of hyperglycemia in critically ill patients. Crit. Care Med 2012 Vol 40, No 12. 5

6 Hydration Electrolytes Insulin DKA: Treatment Co-morbid conditions and/or precipitating factors Kitabchi Diabetes Care 2006
7 Fluids Normal saline initially, 1-2L in the first hour If (corrected) sodium is normal or elevated, use ½ NS thereafter (+/- dextrose, +/- potassium) Dextrose if BG <200 Potassium if K is Monitor Electrolytes, q2h to start Blood pressure Urine output Osmolality if renal or cardiac disease
8 Potassium Electrolytes <3.3; replace by IV before insulin ; add 20-30mEq to IVF Bicarbonate, only for ph <6.9 3 amps in 1L d5w until ph>7 Phosphate Treat if <1.0mg/dL or if severe cardiacpulmonary compromise
9 Insulin Infusion Bolus of 0.1Unit/kg Infusion at 0.1 unit/kg/hr (Alternatively, infuse at 0.15 units/kg, no bolus) Goal is to decrease BG 50-75/hr Evaluate hourly and adjust accordingly What about the diet?
10 Diagnostic Work Up Urinalysis Complete Blood Count Electrolytes with calculated anion gap Na (Cl +CO2) Corrected Sodium Osmolality Osmolar gap = Osm (2xNa + BG/18) EKG Rule out infection Blood Gas (optional)

11 Insulin Infusions: Highs and Lows Top Causes of Hyperglycemia in the ICU Insulin infusion protocol ineffective Poor utilization of protocol Top Causes of Hypoglycemia in the ICU Insulin infusion protocol ineffective Not following insulin infusion protocol Carbohydrate mismatch

12 Ingredients for Insulin Infusion Order Sets and Protocols
13 Patient Receiving TPN or Continuous Tube Feeds Matching Insulin and Intake Insulin Infusion (Units/hr) Blood Glucose (mg/dl) Basal Insulin requirements Infusion Nutritional Insulin Requirements Blood Glucose (mg/dl)
14 An interruption in nutrition requires a response! Mismatched Insulin and Intake Insulin Infusion (Units/hr) Blood Glucose (mg/dl) Basal Insulin requirements Infusion Nutritional Insulin Requirements Blood Glucose (mg/dl)
15 Option 1: You can adjust the insulin Adjust the Insulin Insulin Infusion (Units/hr) Blood Glucose (mg/dl) Basal Insulin requirements Infusion Nutritional Insulin Requirements Blood Glucose (mg/dl)
16 Option 2: Start alternative dextrose 4.5 source Matching Insulin and Intake Insulin Infusion (Units/hr) Blood Glucose (mg/dl) 0 0 Basal Insulin requirements Infusion Nutritional Insulin Requirements Blood Glucose (mg/dl)

17 Have a plan

18 Example of EMR Alert: TF on hold + Insulin Adjustment Will appear for pt s with 0 charted for TF rate + on insulin Potential Problems RNs don t consistently chart TF interruptions in I/O Charting not always timely if at all

19 Laminated pink caution sign has Nutrition on Hold Unexpectedly Algorithm On the back for quick reference
20 Special Case: Eating while receiving insulin infusion Breakfast Lunch Dinner Plasma insulin Nutritional Insulin (SubQ analog) Basal Insulin (infusion) Time 8:00 12:00 16:00 20:00 24:00 4:00
21 Insulin Concentration Prepare all insulin infusions in pharmacy Use one standard insulin concentration throughout the hospital if possible or confined to special patient populations e.g. PEDS, L&D Most common concentration recommended is 1 unit/ml Jacobi Crit Care Med 2012, ASHP, ISMP
22 Some Approaches UCSD VMMC NYPH Order Set (s) Computer (EPIC) Computer (Cerner) Computer (Sunrise) Protocol(s) Computerizedweb-based Paper (3 sets) Paper (2 sets) BG Target (ICU) (Stepdown) (OR) (eg SICU) And/or (eg Neuro ICU) Formula BG value and rate of change BG value and rate of change BG value and rate of change UCSD University of California San Diego VMMC Virginia Mason Medical NYPH New York Presbyterian Hospital

23 VMMC (Cerner EMR): 3 Insulin Infusion Order Sets 23

24 UCSD (Epic EMR): Insulin Infusion Order set
 RNs utilize the Insulin Computer")

 where")
25 UCSD: Insulin Infusion Calculator (web-based, lives outside of EPIC) RNs utilize the Insulin Computer Calculator per UCSD protocol Log-in to the secure web-based insulin computer protocol site Select the patient s unit and patient Enter the blood glucose levels as directed Add comments (as needed) where indicated

26 UCSD: Insulin Infusion Calculator (web-based, lives outside of EPIC) Computer program provides recommendation for bolus and rate on initiation and then recommendations for hourly adjustment of infusion rate per hourly BG checks thereafter.

27 NYPH Critical Care Drips 27
28 Criteria for Transition to SubQ Insulin DKA HHS Hyperglycemia in CC BG <200 BG <300 Resolution critical illness Two of the following: Gap <12 Bicarbonate >15 ph >7.3 Normal osmolality Off vasopressors Normal mentation Stable infusion rate for ~6hrs Kitabchi Diabetes Care 2006
29 Transition to SubQ Overlap IV and SubQ by two hours Know the home regimen and whether or not it was adequate. Formula Average rate method Weight based dosing Individualize
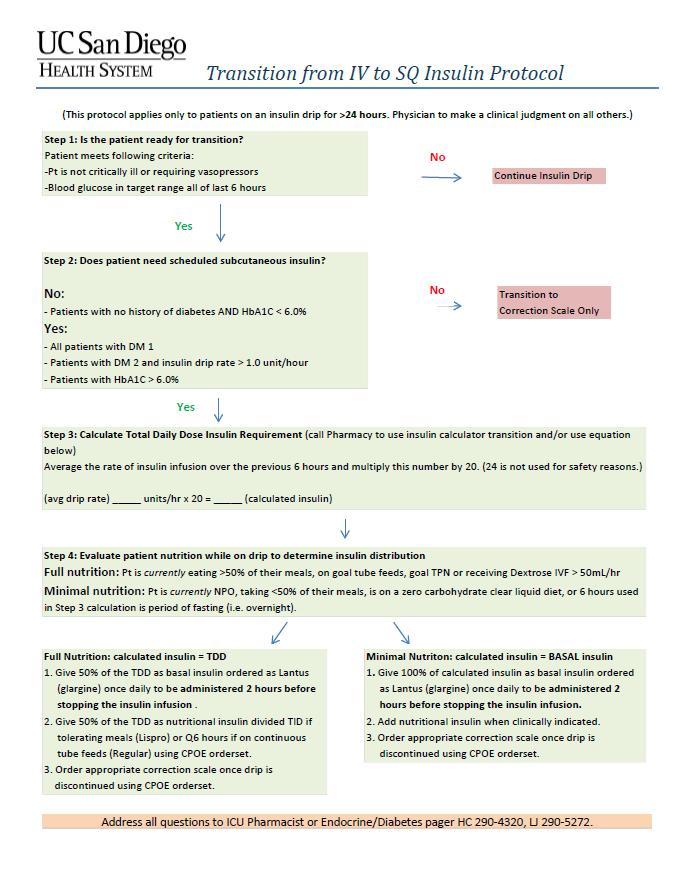
30 Step 1 Transition to SubQ Insulin Is patient ready for transition from IV to SubQ insulin? Critical illness resolved? Off pressors? DKA/HHS resolved? Rate stable for ~ 6hrs?
31 Transition to SubQ Insulin (Cont.) Step 2 Does patient have history of DM? A1C? No DM and A1C <6.0% --> correction scale only Yes DM or A1C >6.0% --> basal bolus regimen
32 Transition to SubQ Insulin (Cont.) Step 3 Use 80% of the lowest of the following to determine TDD: the dose administered over the last 12 hours multiplied by 2 the dose administered over the last 24 hours Use average hourly rate over the last 6 hrs (if stable) and multiply by 20 (80%) Weight
33 Transition to SubQ Insulin (Cont.) Step 4 Determine if TDD = basal or basal + nutritional If basal dose only, then dose can be doubled and divided accordingly when nutrition added If basal + nutritional, then give 50% as basal and 50% as bolus Give basal insulin dose and turn off insulin drip 2 hrs later
34

35 Example of hardwired transition algorithm at VMMC

36 Common Pitfalls No overlap between infusion & subcutaneous insulin Premature transition, difficult to determine a stable rate Mismatch between insulin infusion & nutritional status on infusion and at transition Interruptions of tube feeds/tpn Unclear whether or not infusion used to meet nutritional needs
37 Key Points Insulin infusion protocols (IIPs) indicated for: DKA/HHS Critically ill patients BG >180 mg/dl DKA Treatment: Focus on hydration, electrolytes, insulin, and precipitating factors Safe & effective IIPs: clear, concise, BG direction & rate of change and hypoglycemia management & prevention Transition from IIP to subcutaneous regimen is complex and involves a delicate balance of art & science
38 Special Situations Continuous Nutrition Tube feeds TPN Steroids Perioperative BG Control
39 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular q6hr Intermediate q12hr Long acting q12-24hr
40 Tube Feedings and TPN Super Nutrition Often requires higher ratio of nutritional insulin compared to basal given continuous delivery of high levels of carbohydrates Can be as much as 40:60, 30:70 or even 20:80 ratio of basal:nutrition
41 Tube Feeding and TPN: Insulin Strategies Several options to cover nutritional component Rapid acting q4hr Regular q6hr Intermediate (NPH) q12hr Long acting q12-24hr For TPN- regular insulin can be added to TPN Choice should be uniform across institution Indication and holding parameters should be included in every nutritional insulin order so RN knows when to give and when to hold Increase basal insulin carefully in case nutrition is interrupted
42 Interruption in Nutrition Unexpected Pt on continuous TF pulls out NG tube Middle of the night? 1 hour after nutritional insulin given? 5 hours after nutritional insulin given? Expected Pt on continuous TF going to Radiology 1 hr for CT? 6 hrs for procedure? HAVE A PLAN & AN Order!!


43 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Rapid acting q4hr Regular q6hr Intermediate q12hr Long acting q12-24hr

44 1 Hour After Nutritional Insulin Given


45 5 Hours After Nutritional Insulin Given

46 Steroids Steroids commonly prescribed in hospital COPD & asthma exacerbations Transplant patients Anti-emetic for chemotherapy Post-operatively, e.g. orthopedics Steroids cause general insulin resistance w/ much less effect on gluconeogenesis Glucose elevation predominantly postprandial hyperglycemia, relative lack of fasting hyperglycemia


47 8am Once Daily Steroid Dosing Steroid Effect a 8a 10a 12p 2p 4p 6p 8p 10p 12a 2a 4a

48 Steroid Use

49 Relative Potencies of Systemic Glucocorticoids Equivalent Physiologic Replacement Doses: Dexamethasone: mg Prednisone: mg Hydrocortisone: mg
50 Treatment of Steroid Induced Hyperglycemia Insulin dosing depends on frequency/timing of steroid administration (eg once daily, BID, TID, QID) Treatment may consists of : Large doses of rapid-acting pre meal +/- basal insulin OR NPH alone or in addition to usual basal + bolus regimen Avoid significant increases in basal insulin with once daily steroid dosing, as overnight hypoglycemia may occur Insulin doses should be adjusted in concert with steroid dose changes

51 Basal heavy regimen to cover BID-QID steroids when steroid tapered to once daily significantly increases risk of hypos Titrate insulin simultaneously with steroids!!
52 Tapering Steroids Decrease nutritional insulin dose and/or NPH dose as you taper steroids Be sure to adjust basal insulin dose if dose was increased to cover BID-QID dosed steroids
53 Perioperative Glycemic Control Perioperative hyperglycemia associated with worse outcomes Malglycemia causes oxidative stress Increased risk of inflammation & infection Increased risk of thrombosis Association between hyperglycemia in postop period & adverse outcomes, e.g. infections, arrhythmias and renal impairment Published studies show interventions to improve glycemic control reduces risk of complications Akhtar Anesth Analg 2010, Diabetes Care 2009 Whitcomb et al. (2005), Freire et al. (2005), Zerr KJ, et al. (1997)
54 Standards of Care A1c value should be obtained preoperatively for those with diabetes or diabetes risk factors, with appropriate adjustment in the outpatient regimen prior to surgery. Use intravenous insulin infusions in patients with type 1 or type 2 diabetes treated with insulin and undergoing major surgical procedures, with target glucose between 120 and 180 mg/dl. Administer subcutaneous correction dose insulin or an intravenous insulin infusion during minor or short surgical procedures, with target glucose between 140 and 180 mg/dl, and monitoring every 1 2 hours, depending on insulin used and type of surgery.
55 Standards of Care (Cont.) Anesthesiologist and OR team should make sure that: Glucose levels are monitored at least every hour for patients on infusion. If using insulin during surgery, potassium levels are measured every 4 to 6 hours during surgery Glucose is measured in the recovery room immediately after surgery Source: AACE / ADA guidelines for Perioperative Care: American College of Phyisicians (PIER): Society for Ambulatory Anesthesia Guidelines on Perioperative Management of the Adult Patient with Diabetes.
56 Thank you! Questions?
Special Situations 1
 Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol. Glycemic Task Force September 2014
 DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker,
DKA Adult ICU Powerplan
 DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
Implementing Hospital Policies & Protocols
 Implementing Hospital Policies & Protocols Jane Jeffrie Seley DNP MPH GNP BC-ADM CDE CDTC FAADE FAAN Division of Endocrinology, Diabetes & Metabolism NewYork-Presbyterian Hospital Weill Cornell Medicine
Implementing Hospital Policies & Protocols Jane Jeffrie Seley DNP MPH GNP BC-ADM CDE CDTC FAADE FAAN Division of Endocrinology, Diabetes & Metabolism NewYork-Presbyterian Hospital Weill Cornell Medicine
Diabetes: Inpatient Glucose control
 Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked
 are unchecked") Available at: BMC-B BMC-D BMC-N BMC-S Condition/Status ***(NOTE)***For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS than 12
Available at: BMC-B BMC-D BMC-N BMC-S Condition/Status ***(NOTE)***For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS than 12
DKA/HHS Pathway Phase 1 (Adult) Insulin Potassium Bicarbonate
 Insulin Potassium Bicarbonate") Approved by Diabetes Steering Committee, MMC, 2015 DKA/HHS Pathway Phase 1 (Adult) DKA Diagnostic Criteria (See page 3 for more details): Blood glucose >250 mg/dl, Arterial ph
Approved by Diabetes Steering Committee, MMC, 2015 DKA/HHS Pathway Phase 1 (Adult) DKA Diagnostic Criteria (See page 3 for more details): Blood glucose >250 mg/dl, Arterial ph
In - Hospital Diabetes Care. A review and personal experience
 In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
SHINE Study PowerChart Order Set CONTROL
 SHINE Study PowerChart Order Set CONTROL Orders Patient Care Component Blood Glucose Details Hypoglycemia: For BG
SHINE Study PowerChart Order Set CONTROL Orders Patient Care Component Blood Glucose Details Hypoglycemia: For BG
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
Diabetic Ketoacidosis (DKA) Critical Care Guideline Two Bag System
 Critical Care Guideline Two Bag System") Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Disclosure. Disclosure. Disclosure. Course Outline. Objectives. A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings 7/25/2013
 47 th Annual Meeting August 2-4, 2013 Orlando, FL A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings Kevin Forbush, Pharm. D Central Maine Medical Center Lewiston, Maine Disclosure I do
47 th Annual Meeting August 2-4, 2013 Orlando, FL A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings Kevin Forbush, Pharm. D Central Maine Medical Center Lewiston, Maine Disclosure I do
Transforming Diabetes Care
 Transforming Diabetes Care Meeting the Challenge of Inpatient Glycemic Management in the Critical Care Setting Jane Jeffrie Seley, DNP, MSN, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner,
Transforming Diabetes Care Meeting the Challenge of Inpatient Glycemic Management in the Critical Care Setting Jane Jeffrie Seley, DNP, MSN, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner,
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting
 Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
LIBERTYHEALTH. Jersey City Medical Center Department of Patient Care Services. Approved by Policy Committee:
 LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
ADMIT DIABETIC KETOACIDOSIS (DKA) PLAN - Phase: Begin Immediately/Emergency Center
 PLAN - Phase: Begin Immediately/Emergency Center") - Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
- Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
Disclosures. Glycemic Control in the Intensive Care Unit. Objectives. Hyperglycemia. Hyperglycemia. History. No disclosures
 Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
Improving Glycemic Control in Critical Care Units Thérèse Franco, MD
 Improving Glycemic Control in Critical Care Units Thérèse Franco, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: Have to fly her in from sunny San Diego. She is a hospitalist at Virginia Mason
Improving Glycemic Control in Critical Care Units Thérèse Franco, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: Have to fly her in from sunny San Diego. She is a hospitalist at Virginia Mason
DONATION AFTER CARDIAC DEATH PLAN
 DONATION AFTER CARDIAC DEATH PLAN Diagnosis Weight Allergies Patient Care Core Body Temperature Monitoring Maintain body temp 96-99 degrees Farenheit. Utilize Hyper/Hypothermia blanket prn Insert Gastric
DONATION AFTER CARDIAC DEATH PLAN Diagnosis Weight Allergies Patient Care Core Body Temperature Monitoring Maintain body temp 96-99 degrees Farenheit. Utilize Hyper/Hypothermia blanket prn Insert Gastric
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Deepika Reddy MD Department of Endocrinology
 Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Hypoglycemia Prevention and Management - Measurement that Matters and the Power of Collaboration
 Hypoglycemia Prevention and Management - Measurement that Matters and the Power of Collaboration Greg Maynard M.D., Clinical Professor of Medicine Director, UCSD Center for Innovation and Improvement Science
Hypoglycemia Prevention and Management - Measurement that Matters and the Power of Collaboration Greg Maynard M.D., Clinical Professor of Medicine Director, UCSD Center for Innovation and Improvement Science
Perioperative Management of the Patient with Endocrine Disease: A Focus on Diabetes & Thyroid Dysfunction
 Perioperative Management of the Patient with Endocrine Disease: A Focus on Diabetes & Thyroid Dysfunction Luigi Meneghini, MD, MBA Professor, Internal Medicine (Endocrinology), UT Southwestern Medical
Perioperative Management of the Patient with Endocrine Disease: A Focus on Diabetes & Thyroid Dysfunction Luigi Meneghini, MD, MBA Professor, Internal Medicine (Endocrinology), UT Southwestern Medical
In-hospital management of diabetes
 Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Pharmacy Plan Guidance
 Pharmacy Plan Guidance The pharmacy plan is a tool used during the site readiness process to develop and document the site-specific procedures for study drug ordering, labeling and dispensing for the SHINE
Pharmacy Plan Guidance The pharmacy plan is a tool used during the site readiness process to develop and document the site-specific procedures for study drug ordering, labeling and dispensing for the SHINE
Glucose Management in the ICU: The Role of the Pharmacist
 Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It
 The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
Glycemic care pathway patient and/or Diabetes noted preoperatively. confirm BG order / write order holding area. TARGET mg/dL
 BG check options POCT glucometer (pre/pacu) POCT istat (intraop) venous/arterial BG venous BG (lab) Glycemic care pathway patient and/or Diabetes noted preoperatively confirm BG order / write order holding
BG check options POCT glucometer (pre/pacu) POCT istat (intraop) venous/arterial BG venous BG (lab) Glycemic care pathway patient and/or Diabetes noted preoperatively confirm BG order / write order holding
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL
 VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL Background: For some time, the presence of diabetes and hyperglycemia
VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL Background: For some time, the presence of diabetes and hyperglycemia
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Diabetic Emergencies DKA, HHS, Hypoglycemia. Disclosure. Learning Objectives
 Diabetic Emergencies DKA, HHS, Hypoglycemia October 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Disclosure Michael McDermott has no conflict
Diabetic Emergencies DKA, HHS, Hypoglycemia October 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Disclosure Michael McDermott has no conflict
Glycemic Control Insulin In The Hospital Setting
 Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
PHYSICIAN S ORDERS Page 1 of 1 Providence Hospital ICU Insulin Drip Protocol
 DTE PROVIDENCE HOSPITL 6801 irport Boulevard, Mobile L 36608, PHYSICIN S ORDERS Page 1 of 1 Providence Hospital ICU Insulin Drip Protocol 1. Discontinue all previous insulin and oral diabetic medications
DTE PROVIDENCE HOSPITL 6801 irport Boulevard, Mobile L 36608, PHYSICIN S ORDERS Page 1 of 1 Providence Hospital ICU Insulin Drip Protocol 1. Discontinue all previous insulin and oral diabetic medications
Learning Objectives. Perioperative SWEET Success
 Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting
 Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
Physician Orders PEDIATRIC: LEB DKA Diabetes Mellitus Admit Plan
 Initiate Orders Phase Non Categorized R Powerplan Open Care Sets/Protocols/PowerPlans Initiate Powerplan Phase Phase: Admit DKA Two-Bag Calculations Phase, When to Initiate: Initiate Powerplan Phase Phase:
Initiate Orders Phase Non Categorized R Powerplan Open Care Sets/Protocols/PowerPlans Initiate Powerplan Phase Phase: Admit DKA Two-Bag Calculations Phase, When to Initiate: Initiate Powerplan Phase Phase:
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine
 The Approach to Inpatient Hyperglycemia Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine Great Lakes Hospital Medical Symposium May 7th 2010 Further Increases in the Prevalence of Diabetes
The Approach to Inpatient Hyperglycemia Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine Great Lakes Hospital Medical Symposium May 7th 2010 Further Increases in the Prevalence of Diabetes
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Welcome Everyone. Monitoring, Sick Days, Inpatient Management - Objectives. Mrs. Jones has new diabetes. She asks you: Page 1
 Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Improving Glycemic Control in Non-Critical Care Units Kristen Kulasa, MD
 Improving Glycemic Control in Non-Critical Care Units Kristen Kulasa, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: So Dr. [INAUDIBLE] will go back out and come back in with her moves. We'll
Improving Glycemic Control in Non-Critical Care Units Kristen Kulasa, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: So Dr. [INAUDIBLE] will go back out and come back in with her moves. We'll
Position Statement of ADA / EASD 2012
 Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
Improved IPGM: Demonstrating the Value to both Patients and Hospitals
 Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial
 Trial") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI Agenda General protocol for control group/ intervention group Discussion of meals Hypoglycemia
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI Agenda General protocol for control group/ intervention group Discussion of meals Hypoglycemia
Clinical Guideline DKA
 Clinical Guideline DKA Pediatric Emergency & Critical Care Medicine! This guideline should not replace clinical judgment. Inclusion criteria: Known Diabetes Mellitus Concern for new onset Diabetes Mellitus
Clinical Guideline DKA Pediatric Emergency & Critical Care Medicine! This guideline should not replace clinical judgment. Inclusion criteria: Known Diabetes Mellitus Concern for new onset Diabetes Mellitus
HAP PA-HEN Achieving More Together
 HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
123 Are You Providing Evidence-Based Diabetes Care? - Martin
 Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
9/23/09. What are the key components of preoperative, intraoperative, & postoperative care of diabetes management? Rebecca L. Sturges, M.D.
 RMHS Perioperative Summit: Perioperative Diabetes Management Rebecca L. Sturges, M.D. Oct 6, 2009 Mrs. B was referred by her orthopedic surgeon to your preoperative clinic to discuss medical management
RMHS Perioperative Summit: Perioperative Diabetes Management Rebecca L. Sturges, M.D. Oct 6, 2009 Mrs. B was referred by her orthopedic surgeon to your preoperative clinic to discuss medical management
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Special Situations. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols Special Situations. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Special Situations Askiel Bruno, MD, MS Protocol PI Hypoglycemia Protocol General Concepts The hypoglycemia prevention protocol
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Special Situations Askiel Bruno, MD, MS Protocol PI Hypoglycemia Protocol General Concepts The hypoglycemia prevention protocol
Endocrine and Metabolic Complications in the ICU
 Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Arterial blood gas Capillary blood glucose every hour. Continue to monitor hourly capillary blood glucose as per protocol (See Appendix A and B)
") Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Inpatient and perioperative management of hyperglycemia
 Inpatient and perioperative management of hyperglycemia Department of Internal Medicine Grand Rounds July 7, 2017 Luigi Meneghini discloses that he has served on advisory boards and as consultant for both
Inpatient and perioperative management of hyperglycemia Department of Internal Medicine Grand Rounds July 7, 2017 Luigi Meneghini discloses that he has served on advisory boards and as consultant for both
COMPLIANCE WITH THIS DOCUMENT IS MANDATORY
 COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING
 Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Arterial blood gas Capillary blood glucose every hour. Continue to monitor hourly capillary blood glucose as per protocol (See Appendix A and B)
") Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Diabetic Emergencies in Pregnancy. Brian A. Mason, MS, MD
 Diabetic Emergencies in Pregnancy Brian A. Mason, MS, MD Objectives Recognize the three major risks of major morbidity in the diabetic gravida. Treat these 3 risks promptly and effectively. Diabetic Emergencies
Diabetic Emergencies in Pregnancy Brian A. Mason, MS, MD Objectives Recognize the three major risks of major morbidity in the diabetic gravida. Treat these 3 risks promptly and effectively. Diabetic Emergencies
Hypoglycemia Reduction STARTER PACK WEBINAR #1
 Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action
 Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action Learning Objectives Identify patient situations where specific attention to glycemic control is warranted Determine
Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action Learning Objectives Identify patient situations where specific attention to glycemic control is warranted Determine
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting
 Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
CareLink. software REPORT REFERENCE GUIDE. Management Software for Diabetes
 CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State. Adam Bursua, Pharm.D., BCPS
 Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE GLYCEMIC MANAGEMENT - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity & Nutrition Strategic Clinical Network PARENT DOCUMENT
TITLE GLYCEMIC MANAGEMENT - ADULT SCOPE Provincial: Acute Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Diabetes, Obesity & Nutrition Strategic Clinical Network PARENT DOCUMENT
GLYCEMIC CONTROL SURVEY
 GLYCEMIC CONTROL SURVEY Objective: To gain an understanding of the current state of glycemic control (ie, intensive insulin therapy and frequent blood glucose testing) protocol use in hospital inpatients.
GLYCEMIC CONTROL SURVEY Objective: To gain an understanding of the current state of glycemic control (ie, intensive insulin therapy and frequent blood glucose testing) protocol use in hospital inpatients.
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς
 Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Please inform the Diabetes Nurse Specialist that this patient has been admitted within 24hrs of admission.
 Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Physician Orders PEDIATRIC: LEB ED Hx of DKA with Hyperglycemia Plan
 LEB ED Triage Hx of DKA w Hyperglycemia Non Categorized Criteria for use: Patients less than 18 years of age with known or suspected Diabetes Mellitus and blood glucose greater than 300mg/dL.(NOTE)* Vital
LEB ED Triage Hx of DKA w Hyperglycemia Non Categorized Criteria for use: Patients less than 18 years of age with known or suspected Diabetes Mellitus and blood glucose greater than 300mg/dL.(NOTE)* Vital
Case TWO. Vital Signs: Temperature 36.6degC BP 137/89 HR 110 SpO2 97% on Room Air
 Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
ANNUAL MEETING 2 #FSHP2017
 FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
DRUG ORDERING & DISPENSING:
 STUDY DRUG: List the study drugs that will be used at your site based on your hospital formulary 1. Insulin Humulin R 2. Insulin Humalog 3. Insulin Lantus DRUG SUPPLY & STORAGE: Since study drugs are not
STUDY DRUG: List the study drugs that will be used at your site based on your hospital formulary 1. Insulin Humulin R 2. Insulin Humalog 3. Insulin Lantus DRUG SUPPLY & STORAGE: Since study drugs are not
Intensive Insulin in the Intensive Care Unit
 TABLE OF CONTENTS Introduction to Intensive Insulin in Adult Critical Care Patients - UIMCC Guideline for Insulin Infusion in Adult ICU Patients - P&T Committee Formulary Action Intensive Insulin in the
TABLE OF CONTENTS Introduction to Intensive Insulin in Adult Critical Care Patients - UIMCC Guideline for Insulin Infusion in Adult ICU Patients - P&T Committee Formulary Action Intensive Insulin in the
Report Reference Guide. THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1
 Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
The principles of insulin adjustment guidance
 The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
Peripartum and Postpartum Management of Diabetes
 Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
Report Reference Guide
 Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
5/15/2018 DISCLOSURE OBJECTIVES. FLORIDA HOSPITAL ORLANDO Not for profit organization Acute care medical center 1,368 licensed beds BACKGROUND
 DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
Evidence for Basal Bolus Insulin Versus Slide Scale Insulin
 Curr Emerg Hosp Med Rep (2014) 2:26 34 DOI 10.1007/s40138-013-0032-4 DIABETES AND METABOLIC DISEASE (W FORD, SECTION EDITOR) Evidence for Basal Bolus Insulin Versus Slide Scale Insulin Sameer Badlani William
Curr Emerg Hosp Med Rep (2014) 2:26 34 DOI 10.1007/s40138-013-0032-4 DIABETES AND METABOLIC DISEASE (W FORD, SECTION EDITOR) Evidence for Basal Bolus Insulin Versus Slide Scale Insulin Sameer Badlani William
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline
 Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Division of Acute Care Surgery Clinical Practice Policies, Guidelines, and Algorithms: Enteral Nutrition Algorithm Clinical Practice Guideline Original Date: 08/2011 Purpose: To promote the early use of
Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool
 Frequency & Pattern Tool") Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
4/10/2015. Foundations to Managing Inpatient Hyperglycemia. Learning Objectives
 Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
April Dear (Editor):
:") April 2014 Dear (Editor): Registered Dietitians (RD) play an integral role in patient care in the medical intensive care unit. RD s have increased knowledge in blood glucose control and reducing adverse
April 2014 Dear (Editor): Registered Dietitians (RD) play an integral role in patient care in the medical intensive care unit. RD s have increased knowledge in blood glucose control and reducing adverse
Metabolic Precautions & ER Recommendations
 Metabolic Precautions & ER Recommendations * To whom correspondence Sumit Parikh, should MD be addressed Center for Pediatric Neurology Cleveland Clinic Cleveland, OH UMDF 2010 The catabolic state Entering
Metabolic Precautions & ER Recommendations * To whom correspondence Sumit Parikh, should MD be addressed Center for Pediatric Neurology Cleveland Clinic Cleveland, OH UMDF 2010 The catabolic state Entering
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia preope
 Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Preoperative Evaluation In Endocrine Disorders Dr Nahid Zirak 2012 Perioperative Decision Making The decision has been made to proceed with operative management timing and site of surgery the type of anesthesia
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules)
") Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules) SETTING FOR STAFF PATIENTS Medical and nursing staff Children and young
Executive Summary Management of Type 1 Diabetes Mellitus during illness in children and young people under 18 years (Sick Day Rules) SETTING FOR STAFF PATIENTS Medical and nursing staff Children and young
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi