Hypoglycemia Prevention and Management - Measurement that Matters and the Power of Collaboration
|
|
|
- Barnard Hodge
- 6 years ago
- Views:
Transcription

1 Hypoglycemia Prevention and Management - Measurement that Matters and the Power of Collaboration Greg Maynard M.D., Clinical Professor of Medicine Director, UCSD Center for Innovation and Improvement Science CMO, Society of Hospital Medicine Session 3 of 4: NYSP4P Initiative

2 Greg Maynard - Conflict of Interest Statement AHRQ grants to improve glycemic control and reduce hypoglycemia SHM CMO - SHM is not-for-profit that offers some products for glycemic control QI initiatives and measurement tools. No personal fiscal COI.
3 Session I - Feb 12 th Dr. Greg Maynard Why inpatient glycemic control is important Overview of IV and SC insulin best practices, how to implement Framework for Improvement Session II - Feb 26 th Dr. Kristi Kulasa Inpatient glycemic team structure - Coordination of meals / insulin / testing Top things we teach / reinforce Basal / bolus cases and special situations (TPN, TF, NPO, Steroids, Transition IV to SC insulin) Session III - March 12 th Dr. Greg Maynard Safe use of insulin summary Hypoglycemia Management and Prevention Measurement and Monitoring month to month and day to day SHM and other resources Session IV - March 19 th Drs. Kulasa and Maynard FAQs / Q&A Transitions Barriers and How to Overcome Them
4 Essential Elements Successful PI Efforts Institutional support buy in Staff engagement and training Standardization of order sets, help with measures Teams and Culture of Improvement Understand Current Process Willingness to Redesign process Defined goals Metrics reliable, practical, rapid feedback Guidance in order sets and other venues Hardwire - Reliable Interventions Ongoing informed improvement Educational programs

5 NYS PARTNERSHIP FOR PATIENTS 5 March 11, 2014

6 Enhancing insulin-use safety in hospitals: Practical recommendations from an ASHP Foundation Expert Consensus Panel Cobaugh D, Maynard G, et al. Am J Health-Syst Pharm 2013;70:
7 Prescribing: Recommendation 1 Develop protocol-driven and evidence-based order sets for specific uses of insulin: IV to Subcutaneous insulin transitions Administration via subcutaneous insulin pumps Post-discharge / transition regimens DKA and hyperosmolar states Hyperkalemia Post-cardiac surgery care Integrated hypoglycemia management orders Include decision-support to guide insulin use based on patient s nutritional status and for appropriate monitoring Cobaugh D, Maynard G, et al. Am J Health-Syst Pharm 2013;70:
8 Prescribing: Recommendation 2 and 3. Recommendation 2 Eliminate the routine administration of correction / sliding scale insulin doses as the primary strategy to treat hyperglycemia Recommendation 3 Eliminate the use of free text insulin orders in electronic and paper records. Replace them with protocol-driven and evidence-based order sets that allow for the prescribing of complex insulin regimens.
9 Storing and Dispensing: Recommendation 4 Store only U-100 concentration insulin and U-100 administration devices (e.g., syringes, pens) in patient care areas and ensure they are stored in a secure fashion and segregated from other medications. Recommendation 5 Develop hospital-wide standard concentrations for insulin infusions to be adopted and used in all patient care areas.
10 Administering: Recommendation 6 Limit preparation, including for procedural areas, of all intravenous bolus insulin doses and intravenous insulin infusions to the pharmacy department. Recommendation 7 Hospitals must develop policies and procedures to ensure that insulin pens are used for individual patients only. In addition, hospitals must establish policies and educational programs to ensure the safe use of insulin pens and disposable needle tips.
11 Monitoring: Recommendation 8 Ensure that insulin use is linked directly to patients nutrition status. Meal delivery, point-of-care glucose testing, and insulin administration should be well coordinated and standardized. Patients and family care-givers should be educated to request administration of RAA-I when patient begins her/his meal. In patients with variable nutritional intake, prandial insulin administration should be delayed until completion of the meal. Protocol-driven and evidence-based order sets should be developed for insulin-use and blood glucose monitoring during planned and unplanned interruptions of enteral nutrition or total parenteral nutrition.
12 Evaluating: Recommendation 9 Every hospital should prospectively monitor/measure: rates of hypoglycemia and hyperglycemia Insulin use patterns Coordination of insulin administration, glucose testing, and nutrition delivery Real-time, institution-wide glucose reports should be provided to health care team members to ensure appropriate surveillance and management of patients with unexpected hypoglycemia and hyperglycemia
13 Planning: Recommendation 10 Provide standardized education, including competency assessment, to all hospital-based health professionals who are responsible for the use (e.g., prescribing, compounding, dispensing, administering, monitoring) of insulin.
14 Iatrogenic Hypoglycemia A Top Source of Inpatient Adverse Drug Events (ADEs) ADEs are most common cause of inpatient complications affecting 1.9 million stays annually costing $4.2 billion / year responsible for 1/3 of hospital acquired conditions (HACs) % of ADEs are preventable 57% of ADEs are from hypoglycemic agents > 10% of those on a hypoglycemic agent suffer at least one hypoglycemic ADE Classen DC et al. Health Aff (Millwood) 2011;30: Agency for Healthcare Research and Quality, Rockville, MD, 2011 April. HCUP Statistical Brief #109. Classen DC et al. JAMA 997;277: Bates DW et al. JAMA 1997;277: Classen et al. Jt Comm J Qual Patient Saf. 2010;36:12-21
15 Hypoglycemia Risk Factors - Different Flavors Inherent Low BMI / cachexia / Advanced Malignancy / Age Liver / Kidney disease / CHF Iatrogenic Insulin / oral agents Some risk with appropriate use. Risk magnified with inappropriate use or failure to react / anticipate preventable problems. Overly aggressive targets, inappropriate prescribing Improved Glycemic Control AND Reduced Hypoglycemia possible.
16 Iatrogenic Hypoglycemia Etiologic factor % of hypo cases Reduction in enteral intake 40 Insulin adjustment 6.1 Steroid withdrawal 0.4 Unclear 43 Diverse causes 10.4 Medication error none Poor hypoglycemia management and follow up was the rule < 50% with documented euglycemia within 2 hours of low Average time to documented resolution was 4 hrs, 3mins (median 2 hrs, 25mins) Varghese P, et al. J Hosp Med. 2007; 2: )
17 Iatrogenic Hypoglycemia Risk Factors, Treatment, and Prevention 130 ward inpatients monitored for glucose 65 consecutive cases with iatrogenic hypoglycemic day Matched 1:1 with controls (monitored, similar hospital day, not hypoglycemic) Examine risk factors for hypoglycemia Study hypoglycemia treatment and adjustments made to prevent recurrence Maynard et al, Diabetes Spectrum 2008 Vol 21:

18 Poor adherence to hypoglycemia management protocol. Suboptimal adjustment opportunities to prevent hypoglycemia missed. Basal / nutritional 50:50 ratio lost.too much basal. Unexpected nutritional interruption not handled correctly.
19 Iatrogenic Hypoglycemia from Insulin Most common failures 1. Inappropriate prescribing 2. Failure to respond to unexpected nutritional interruption 3. Poor coordination of nutrition delivery, monitoring, and insulin delivery 4. Failure to respond to a prior hypoglycemic day Cobaugh DJ et al. Am J Health Syst Pharm;70(16): Hellman R. Endocr Pract 2004;10 Suppl 2: Maynard GA, et. Diabetes Spectr 2008;
20 Guidance for Scheduled Temporary NPO Example UC San Diego Basal / Nutritional / Correction insulin terms reinforced across orders, MAR, documentation venues New orders not required for temporary NPO Insulin glargine (LANTUS) injection: basal glargine insulin should still be administered even if the patient is temporarily NPO for a procedure, or has temporary interruption of procedure Nutritional RAA-I guidance for eating patients: Give with first bite of food (or up to 30 minutes after first bite of food if patient is nauseated or has poor appetite). Give 0% if patient ate less than 50%, half if patient eats 50%, and full dose if they eat all / almost all of meal.
21 Case Critically ill 49 yo woman: Unexpected interruption of nutrition 5 days s/p abd surgery and resolving sepsis On full tube feedings Insulin infusion at 4 units / hour, glucose 150 mg/dl No history of DM A1c 8.2 Patient pulls feeding tube out.what do you do?
22 Unexpected interruption of enteral nutrition: Appropriate actions include - a) Stop the insulin infusion immediately, monitor frequently. b) Replace enteral nutrition CHO with equivalent D10 by IV infusion, continue insulin infusion at same or slightly reduced rate. c) Reduce insulin infusion to 1-2 units per hour, insure IV access x 2, monitor frequently until tube feeding can be adjusted. d) Continue insulin infusion at same rate, A1c indicates DM is present and she should tolerate interruption of nutrition. e) Either b) or c) are acceptable
23 Unexpected interruption of enteral nutrition: Appropriate actions include - a) Stop the insulin infusion immediately, monitor frequently. b) Replace enteral nutrition CHO with equivalent D10 by IV infusion, continue insulin infusion at same or slightly reduced rate. c) Reduce insulin infusion to 1-2 units per hour, insure IV access x 2, monitor frequently until tube feeding can be adjusted. d) Continue insulin infusion at same rate, A1c indicates DM is present and she should tolerate interruption of nutrition. e) Either b) or c) are acceptable
24
25 Clinical Informatics and Glycemic Control Clinical Decision Support Order sets with embedded CDS Computerized insulin dosing algorithms Month to Month reporting Flow sheets - Visual cues / graphics / trends Real time reports (hyper- and hypo- glycemic outliers, reports that capture patients off protocol ) An important part of a larger framework for improvement!
26 Active Surveillance Identify patients with a potential deficit in care, who are in the hospital right now. Triage tools to quickly determine if the patient is truly uncontrolled or off protocol. Intervene to bring onto protocol, reduce risk of glycemic excursions and continued deficits in care, provide just in time education. aka measure-vention
27 STROKE CODE - June 10 BG = 8

28 Recurrent hypoglycemia on same insulin doses for several days preceding stroke code

29 Proposed CDS Display for hypoglycemia evaluation Federal Interagency Workgroup to prevent ADE

30 Flow sheets: Useful from primary team AND for Measure-Vention Triage report, investigation, and mitigation all within the EHR.

31 Virginia Mason example
32 Iatrogenic Hypoglycemia from Insulin Most common failures and strategies to address them Inappropriate prescribing Standardized orders with embedded CDS mandatory use Ongoing monitoring for inappropriate prescribing, just in time intervention Failure to respond to unexpected nutritional interruption Protocols and Education Methods to reduce interruptions in tube feeding Poor coordination of nutrition delivery, monitoring, and insulin delivery Clear directions in protocols and order sets Regular education / competency training Redesign process Failure to respond to a prior hypoglycemic day Make sure ASSESSMENT is part of hypoglycemia protocol Competency and case based-training Monitor recurrent hypoglycemia rates
33 The Mentored Implementation Model Based upon model pioneered by Center to Advance Palliative Care Physician coaches with expertise and experience in effective implementation and QI, as well as topical expertise Mentoring occurs via monthly one-to-one calls, site visits and ad hoc communications Timely guidance, advice, and feedback Written summaries, to do tasks, timelines Mentor University training
34
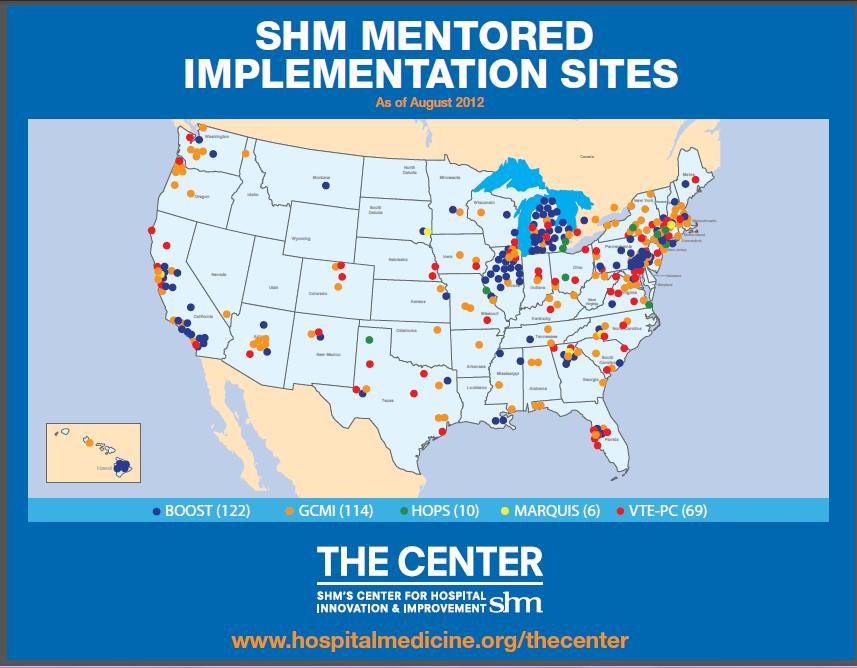
35 Mentored Implementation Collaboratives Data center with data upload and reporting capability Group educational webinars Topic-specific listserves and discussion forums Community website with topic-specific information, news and literature 3 mentored implementation program collaboratives with over 300 participants Glycemic control in over 100 sites
36 Implementation Guides / Resource Rooms Foundation of Mentored Implementation Model QI fundamentals Building a team Metrics and evaluation Gaining institutional support Process mapping and needs assessment Topic-specific interventions Spreading Improvement Tools, links, annotated bibliographies, slide decks, etc

37 2011 Eisenberg Award Winner

38 Mentored Implementation Collaborative
39 Cumulative Incidence NYS PARTNERSHIP FOR PATIENTS NYSPFP Insulin Measure #1 Number of Unique Inpatients with At Least One Blood Glucose Result 200 mg/dl Per 100 Unique Inpatients Prescribed Insulin (n=64) (n=64) (n=66) Oct-13 Nov-13 Dec-13 Reporting Period 39 March 11, 2014
40 Cumulative Incidence NYS PARTNERSHIP FOR PATIENTS NYSPFP Insulin Measure #2 Number of Unique Inpatients with At Least One Blood Glucose Result 50 mg/dl Per 100 Unique Inpatients Prescribed Insulin (n=64) (n=64) 9.33 (n=66) Oct-13 Nov-13 Dec-13 Reporting Period 40 March 11, 2014


41 Society of Hospital Medicine: Data / Reporting for Glucometrics, Community, and More




42

43 Hypoglycemia Reduction at UCSD Simultaneous Improvement in Glycemic Control

44 UCSD - Secondary prevention of Hypoglycemia

45

46 Benchmarking - Ranking bar chart - Hypoglycemia Management

47 Benchmarking Ranking bar chart Glycemic control

48 Benchmarking Ranking Bar Chart Hypoglycemia Rates
49 SHM Benchmarking tools Scatterplot Uncontrolled hyperglycemia Y Axis Hypoglycemia rate - X axis Both are highly variable
50 A Series of Linked Protocols: Reinforce protocols by multiple methods, hardwire whenever possible Basic Protocols SC insulin IV infusion insulin Periop management Hypoglycemia Management Patient Education Always More to Do SC Insulin Pumps Monitoring Coordination: CHO / BG test / insulin Transitions Provider Education / competency

51 Some designs don t make any sense Even if they ve been there a long time.

52 Safe Glycemic Control A Team Sport Questions and Comments? Next Session - March 19 th Dr. Kristi Kulasa and Dr. Greg Maynard FAQs / Q&A Transitions Barriers and How to Overcome Them
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting
 Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting
 Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Avoiding Hypoglycemia Kristen Kulasa, MD
 Avoiding Hypoglycemia Kristen Kulasa, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: Kulasa can come on up and she can take it from here. You have your thing and there's slides. OK. Thanks. KRISTEN
Avoiding Hypoglycemia Kristen Kulasa, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: Kulasa can come on up and she can take it from here. You have your thing and there's slides. OK. Thanks. KRISTEN
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting
 Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
Hypoglycemia Reassessment at Orange Regional Medical Center
 What is the Society of Medicine s Glycemic Control equips Program? The Society of Medicine s (SHM s) Glycemic Control Electronic Quality Improvement Program (GC equips) assists with optimizing glycemic
What is the Society of Medicine s Glycemic Control equips Program? The Society of Medicine s (SHM s) Glycemic Control Electronic Quality Improvement Program (GC equips) assists with optimizing glycemic
Deepika Reddy MD Department of Endocrinology
 Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Improving Glycemic Control in the Critical Care
 Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
Special Situations 1
 Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Lessons Learned: Interdisciplinary collaboration to reduce hypoglycemic events
 Lessons Learned: Interdisciplinary collaboration to reduce hypoglycemic events Ryan ull, Pharm.., BCPS ssistant Professor of Pharmacy Practice Creighton niversity School of Pharmacy legent Health Lakeside
Lessons Learned: Interdisciplinary collaboration to reduce hypoglycemic events Ryan ull, Pharm.., BCPS ssistant Professor of Pharmacy Practice Creighton niversity School of Pharmacy legent Health Lakeside
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
Hypoglycemia Reduction STARTER PACK WEBINAR #1
 Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Welcome Everyone. Monitoring, Sick Days, Inpatient Management - Objectives. Mrs. Jones has new diabetes. She asks you: Page 1
 Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
6/9/2016. Activating Hospital Staff & Physicians to Support Diabetes Education in the Hospital and Through Transition. Diabetes in Scripps Hospitals
 Disclosure to Participants Notice of Requirements For Successful Completion Please refer to learning goals and objectives Learners must attend the full activity and complete the evaluation in order to
Disclosure to Participants Notice of Requirements For Successful Completion Please refer to learning goals and objectives Learners must attend the full activity and complete the evaluation in order to
ANNUAL MEETING 2 #FSHP2017
 FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
LIBERTYHEALTH. Jersey City Medical Center Department of Patient Care Services. Approved by Policy Committee:
 LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes
 Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes Kristi Kulasa, MD Associate Clinical Professor of Medicine Director, Inpatient Glycemic Control University of California
Getting Off the Merry-Go-Round Reducing Readmissions for Patients with Diabetes Kristi Kulasa, MD Associate Clinical Professor of Medicine Director, Inpatient Glycemic Control University of California
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events. September 13, 2016
 Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events September 13, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events September 13, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
CareLink. software REPORT REFERENCE GUIDE. Management Software for Diabetes
 CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
CareLink Management Software for Diabetes software REPORT REFERENCE GUIDE How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used
NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING
 Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
For patients uncontrolled on multiple daily injections of insulin. A quick-start guide for your practice ALL-DAY CONTROL WITH
 For patients uncontrolled on multiple daily injections of insulin A quick-start guide for your practice Dosing guidance 1,* V-Go: 3 options 1 For initiating V-Go in patients switching from MDI The majority
For patients uncontrolled on multiple daily injections of insulin A quick-start guide for your practice Dosing guidance 1,* V-Go: 3 options 1 For initiating V-Go in patients switching from MDI The majority
Report Reference Guide
 Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
Report Reference Guide How to use this guide Each type of CareLink report and its components are described in the following sections. Report data used to generate the sample reports was from sample patient
123 Are You Providing Evidence-Based Diabetes Care? - Martin
 Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Society of Hospital Medicine. to Jumpstart Hospitals
 Using Society of Hospital Medicine (SHM) Mentors to Jumpstart Hospitals to Improve Glycemic Control Society of Hospital Medicine Edited by: Pedro Ramos, MD, FHM Jane Jeffrie Seley, DNP, MPH, BC-ADM, CDE,
Using Society of Hospital Medicine (SHM) Mentors to Jumpstart Hospitals to Improve Glycemic Control Society of Hospital Medicine Edited by: Pedro Ramos, MD, FHM Jane Jeffrie Seley, DNP, MPH, BC-ADM, CDE,
Diabetes Management: Current High Tech Innovations
 Diabetes Management: Current High Tech Innovations How Far We ve Come in the Last 40 Years William V. Tamborlane, MD Department of Pediatrics Yale School of Medicine Disclosures I am a consultant for:
Diabetes Management: Current High Tech Innovations How Far We ve Come in the Last 40 Years William V. Tamborlane, MD Department of Pediatrics Yale School of Medicine Disclosures I am a consultant for:
In - Hospital Diabetes Care. A review and personal experience
 In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
Glycemic Control Hitting the Sweet Spot During Inpatient Care
 Glycemic Control Hitting the Sweet Spot During Inpatient Care Tim R. Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Family Medicine Cleveland Clinic Akron General Professor, Northeast
Glycemic Control Hitting the Sweet Spot During Inpatient Care Tim R. Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Family Medicine Cleveland Clinic Akron General Professor, Northeast
Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia
 Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia Shiv Patil, MD, MPH, BC-ADM Clinical Assistant Professor of Family Medicine Brody School of Medicine at East Carolina
Hypoglycemia Task Force: A Quality Improvement Initiative to Reduce Inpatient Hypoglycemia Shiv Patil, MD, MPH, BC-ADM Clinical Assistant Professor of Family Medicine Brody School of Medicine at East Carolina
5/15/2018 DISCLOSURE OBJECTIVES. FLORIDA HOSPITAL ORLANDO Not for profit organization Acute care medical center 1,368 licensed beds BACKGROUND
 DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes
 Organization: Solution Title: Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes Program/Project Description:What was the problem to be solved? How was
Organization: Solution Title: Montgomery General Hospital- Medstar Healthcare Improving Glycemic Control to Enhance Patient Outcomes Program/Project Description:What was the problem to be solved? How was
The most recent estimates suggest that. A study of inpatient diabetes care on medical wards. Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal
 A study of inpatient diabetes care on medical wards Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal Article points 1. It is well established that poor glycaemic control is associated with increased
A study of inpatient diabetes care on medical wards Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal Article points 1. It is well established that poor glycaemic control is associated with increased
Kacy Aderhold, MSN, APRN-CNS, CMSRN
 Kacy Aderhold, MSN, APRN-CNS, CMSRN Promote and support healthy eating patterns Attain individualized glycemic, blood pressure, and lipid goals Achieve and maintain body weight goals Delay or prevent complications
Kacy Aderhold, MSN, APRN-CNS, CMSRN Promote and support healthy eating patterns Attain individualized glycemic, blood pressure, and lipid goals Achieve and maintain body weight goals Delay or prevent complications
Improving Glycemic Control in Non-Critical Care Units Kristen Kulasa, MD
 Improving Glycemic Control in Non-Critical Care Units Kristen Kulasa, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: So Dr. [INAUDIBLE] will go back out and come back in with her moves. We'll
Improving Glycemic Control in Non-Critical Care Units Kristen Kulasa, MD Glycemic Control Bootcamp December 9, 2016 PRESENTER: So Dr. [INAUDIBLE] will go back out and come back in with her moves. We'll
Presented by Dr. Bruce Perkins, MD MPH Dr. Michael Riddell, PhD
 Type 1 Diabetes and Exercise: Optimizing the Medtronic MiniMed Veo Insulin Pump and Continuous Glucose Monitoring (CGM) for Better Glucose Control 1,2 for Healthcare Professionals Presented by Dr. Bruce
Type 1 Diabetes and Exercise: Optimizing the Medtronic MiniMed Veo Insulin Pump and Continuous Glucose Monitoring (CGM) for Better Glucose Control 1,2 for Healthcare Professionals Presented by Dr. Bruce
Diabetes Survival Skills
 Promoting Patient Survival with Diabetes Survival Skills Need to know skills for persons with diabetes Susan Zontine, NP-C WMC Diabetes Stewardship team May 18, 2015 Diabetes Chronic illness with serious
Promoting Patient Survival with Diabetes Survival Skills Need to know skills for persons with diabetes Susan Zontine, NP-C WMC Diabetes Stewardship team May 18, 2015 Diabetes Chronic illness with serious
April Dear (Editor):
:") April 2014 Dear (Editor): Registered Dietitians (RD) play an integral role in patient care in the medical intensive care unit. RD s have increased knowledge in blood glucose control and reducing adverse
April 2014 Dear (Editor): Registered Dietitians (RD) play an integral role in patient care in the medical intensive care unit. RD s have increased knowledge in blood glucose control and reducing adverse
QUALITY IMPROVEMENT TOOLS
 QUALITY IMPROVEMENT TOOLS QUALITY IMPROVEMENT TOOLS The goal of this section is to build the capacity of quality improvement staff to implement proven strategies and techniques within their health care
QUALITY IMPROVEMENT TOOLS QUALITY IMPROVEMENT TOOLS The goal of this section is to build the capacity of quality improvement staff to implement proven strategies and techniques within their health care
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Improved IPGM: Demonstrating the Value to both Patients and Hospitals
 Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
Improved IPGM: Demonstrating the Value to both Patients and Hospitals Osama Hamdy, MD, PhD, FACE Medical Director, Inpatient Diabetes Program Joslin Diabetes Center Harvard Medical School, Boston, MA Cost
The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles
 The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles Linda M. Siminerio, RN, PhD, CDE Professor of Medicine University of Pittsburgh School of Medicine & Nursing Objectives
The Role of the Diabetes Educator within the Patient-Centered Medical Home & Future Roles Linda M. Siminerio, RN, PhD, CDE Professor of Medicine University of Pittsburgh School of Medicine & Nursing Objectives
Physical Activity/Exercise Prescription with Diabetes
 Physical Activity/Exercise Prescription with Diabetes B R AD H I NTERMEYER C E P A C SM S A NFORD H E ALTH C A RDIAC R E H AB A N D D I ABE TES E XE RCISE The adoption and maintenance of physical activity
Physical Activity/Exercise Prescription with Diabetes B R AD H I NTERMEYER C E P A C SM S A NFORD H E ALTH C A RDIAC R E H AB A N D D I ABE TES E XE RCISE The adoption and maintenance of physical activity
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked
 are unchecked") Available at: BMC-B BMC-D BMC-N BMC-S Condition/Status ***(NOTE)***For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS than 12
Available at: BMC-B BMC-D BMC-N BMC-S Condition/Status ***(NOTE)***For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS than 12
Participants in the Program
 Type 2 Diabetes Performance Improvement Initiative: Chart Reviews Participants in the Program 318 clinicians have registered 192 have started the program 126 have started their initial chart review 26
Type 2 Diabetes Performance Improvement Initiative: Chart Reviews Participants in the Program 318 clinicians have registered 192 have started the program 126 have started their initial chart review 26
Developing a pathway of. and care planning for people with diabetes
 Developing a pathway of preoperative assessment and care planning for people with diabetes Louise Hilton, Marie Digner Diabetes is a common endocrine condition affecting 1.4 million people in the UK, with
Developing a pathway of preoperative assessment and care planning for people with diabetes Louise Hilton, Marie Digner Diabetes is a common endocrine condition affecting 1.4 million people in the UK, with
Section of Endocrinology, Rush University Medical Center, Chicago, Illinois.
 ORIGINAL RESEARCH Treatment of Inpatient Hyperglycemia Beginning in the Emergency Department: A Randomized Trial Using Insulins Aspart and Detemir Compared With Usual Care Jennifer B. Bernard, MD Christina
ORIGINAL RESEARCH Treatment of Inpatient Hyperglycemia Beginning in the Emergency Department: A Randomized Trial Using Insulins Aspart and Detemir Compared With Usual Care Jennifer B. Bernard, MD Christina
In-hospital management of diabetes
 Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Glucose Management in the ICU: The Role of the Pharmacist
 Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Topics in Inpatient Glycemic Control
 Topics in Inpatient Glycemic Control Jane Jeffrie Seley DNP MPH MSN GNP BC-ADM CDE CDTC FAADE FAAN Diabetes Nurse Practitioner Program Manager, Inpatient Glycemic Control Program NewYork-Presbyterian/
Topics in Inpatient Glycemic Control Jane Jeffrie Seley DNP MPH MSN GNP BC-ADM CDE CDTC FAADE FAAN Diabetes Nurse Practitioner Program Manager, Inpatient Glycemic Control Program NewYork-Presbyterian/
Advances in Diabetes Care Technologies
 1979 Advances in Diabetes Care Technologies 2015 Introduction Roughly 20% - 30% of patients with T1DM and fewer than 1% of insulin-treated patients with T2DM use an insulin pump In 2007, the US FDA estimated
1979 Advances in Diabetes Care Technologies 2015 Introduction Roughly 20% - 30% of patients with T1DM and fewer than 1% of insulin-treated patients with T2DM use an insulin pump In 2007, the US FDA estimated
HAP PA-HEN Achieving More Together
 HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς
 Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
9/16/2013. No Conflict of Interest to Disclose
 Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA
 LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018 Objectives 1. Identify common preventable causes of hypoglycemia
LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018 Objectives 1. Identify common preventable causes of hypoglycemia
Dr. Steve Ligertwood Dr. Roderick Tukker Dr. David Wilton
 Dr. Steve Ligertwood Hospitalist Royal Columbian Hospital Regional Department Head-Hospitalist for Fraser Health Authority Project Lead BC Hospitalist VTE Collaborative Clinical Instructor, UBC School
Dr. Steve Ligertwood Hospitalist Royal Columbian Hospital Regional Department Head-Hospitalist for Fraser Health Authority Project Lead BC Hospitalist VTE Collaborative Clinical Instructor, UBC School
Sixth International Hospital Diabetes Meeting
 Sixth International Hospital Diabetes Meeting May 19-20, 2017 Georgia Tech Hotel & Conference Center, Atlanta, Georgia Friday May 19, 2017 08:00 Welcome David C. Klonoff, MD, FACP, FRCP (Edin), Fellow
Sixth International Hospital Diabetes Meeting May 19-20, 2017 Georgia Tech Hotel & Conference Center, Atlanta, Georgia Friday May 19, 2017 08:00 Welcome David C. Klonoff, MD, FACP, FRCP (Edin), Fellow
Live life, less complicated. InPen MOBILE APP. Healthcare Provider INSTRUCTIONS FOR USE. CompanionMedical.com
 InPen MOBILE APP Healthcare Provider INSTRUCTIONS FOR USE TABLE OF CONTENTS Introduction...3 InPen Mobile App...3 Intended Use...3 Indications for Use...3 Contraindications...3 Start Orders...4 General
InPen MOBILE APP Healthcare Provider INSTRUCTIONS FOR USE TABLE OF CONTENTS Introduction...3 InPen Mobile App...3 Intended Use...3 Indications for Use...3 Contraindications...3 Start Orders...4 General
Advances in Diabetes Care Technologies
 1979 Advances in Diabetes Care Technologies 2015 Introduction Insulin pump use: ~ 20% - 30% of patients with T1DM < 1% of insulin-treated patients with T2DM 2007 FDA estimates ~375,000 insulin pumps for
1979 Advances in Diabetes Care Technologies 2015 Introduction Insulin pump use: ~ 20% - 30% of patients with T1DM < 1% of insulin-treated patients with T2DM 2007 FDA estimates ~375,000 insulin pumps for
Current Status: Retired PolicyStat ID: Effective: 03/2017 Approved: 03/2017 Last Revised: 03/2017 Expiration: 03/2020
 Current Status: Retired PolicyStat ID: 3428552 Effective: 03/2017 Approved: 03/2017 Last Revised: 03/2017 Expiration: 03/2020 Owner: Department: References: Dustin Falk: Clinical Coordinator- Pharmacy
Current Status: Retired PolicyStat ID: 3428552 Effective: 03/2017 Approved: 03/2017 Last Revised: 03/2017 Expiration: 03/2020 Owner: Department: References: Dustin Falk: Clinical Coordinator- Pharmacy
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events. November 12, 2016
 Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events November 12, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Implementation of an Interprofessional Team to Prevent Inpatient Hypoglycemic Events November 12, 2016 St Joseph s Health Fast Facts Founded 1869 by Sisters of St. Francis Patient Volumes (2014) Inpatient
Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Enteral Feeding Guidelines
 Inpatients Requiring Enteral Feeding Guidelines") Document Control Title Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Author Author s job title Specialist Nurse Consultant Physician Department Directorate Unscheduled Care Version Date
Document Control Title Managing Hyperglycaemia in Acute (Adult) Inpatients Requiring Author Author s job title Specialist Nurse Consultant Physician Department Directorate Unscheduled Care Version Date
Diabetes Survival Skills
 Promoting Patient Survival with Diabetes Survival Skills Need to know skills for persons with diabetes Susan Zontine, NP-C WMC Diabetes Stewardship team Objectives: Review & understand basic diabetes survival
Promoting Patient Survival with Diabetes Survival Skills Need to know skills for persons with diabetes Susan Zontine, NP-C WMC Diabetes Stewardship team Objectives: Review & understand basic diabetes survival
Important Stuff. Basal Bolus What Adjustments? Pt weighs 80kg
 Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Disclosures. Learning Objectives 4/26/2017
 Implementation of a quality improvement initiative to ensure the safe transition from prior-to-admission concentrated insulins to a formulary insulin regimen ERICA J. RHEIN, PHARMD PGY1 PHARMACY PRACTICE
Implementation of a quality improvement initiative to ensure the safe transition from prior-to-admission concentrated insulins to a formulary insulin regimen ERICA J. RHEIN, PHARMD PGY1 PHARMACY PRACTICE
DIAGNOSIS OF DIABETES NOW WHAT?
 DIAGNOSIS OF DIABETES NOW WHAT? DISCUSS GOALS FOR DIABETES CARE IDENTIFY COMMON COMPLIANCE- ADHERENCE ISSUES DESCRIBE TECHNOLOGY TO ASSIST AND / OR IMPROVE DIABETES CARE WHAT DO WE WANT OUR PATIENTS TO
DIAGNOSIS OF DIABETES NOW WHAT? DISCUSS GOALS FOR DIABETES CARE IDENTIFY COMMON COMPLIANCE- ADHERENCE ISSUES DESCRIBE TECHNOLOGY TO ASSIST AND / OR IMPROVE DIABETES CARE WHAT DO WE WANT OUR PATIENTS TO
Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0
 Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0 Copyright: 2018, Alberta Health Services. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives
Provincial Clinical Knowledge Topic Insulin Pump Therapy, Pediatric and Adult Acute Care V 1.0 Copyright: 2018, Alberta Health Services. This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivatives
Type I Type II Insulin Resistance
 Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Report Reference Guide. THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1
 Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
Report Reference Guide THERAPY MANAGEMENT SOFTWARE FOR DIABETES CareLink Report Reference Guide 1 How to use this guide Each type of CareLink report and its components are described in the following sections.
Insulin Pump Therapy
 Patient and Family Education Insulin Pump Therapy The insulin pump is a device that gives insulin to the body at a steady rate. With the pump you won t need daily shots. This handout describes how insulin
Patient and Family Education Insulin Pump Therapy The insulin pump is a device that gives insulin to the body at a steady rate. With the pump you won t need daily shots. This handout describes how insulin
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Greater clinician knowledge of insulin pump therapy can help patients continue to use their pumps during a hospital stay.
 Boost your confidence in caring for patients with insulin pumps Greater clinician knowledge of insulin pump therapy can help patients continue to use their pumps during a hospital stay. By Julie S. Lampe,
Boost your confidence in caring for patients with insulin pumps Greater clinician knowledge of insulin pump therapy can help patients continue to use their pumps during a hospital stay. By Julie S. Lampe,
Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies
 Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies Leigh Briscoe-Dwyer, PharmD, BCPS, FASHP Chief Pharmacy and Medication Safety Officer North Shore Long Island Jewish Health
Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies Leigh Briscoe-Dwyer, PharmD, BCPS, FASHP Chief Pharmacy and Medication Safety Officer North Shore Long Island Jewish Health
DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL
 AUDIT TOOL") DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL Facility: Date: Data Collector s name: Email/Phone: Purpose: To evaluate your facility practices regarding communication of requisite diabetes
DIABETES MANAGEMENT DISCHARGE COMMUNICATION (DM-DC) AUDIT TOOL Facility: Date: Data Collector s name: Email/Phone: Purpose: To evaluate your facility practices regarding communication of requisite diabetes
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical
 Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
SHINE Study PowerChart Order Set CONTROL
 SHINE Study PowerChart Order Set CONTROL Orders Patient Care Component Blood Glucose Details Hypoglycemia: For BG
SHINE Study PowerChart Order Set CONTROL Orders Patient Care Component Blood Glucose Details Hypoglycemia: For BG
P R O J E C T B U L L E T I N - F A L L I N T H I S I S S U E U P D A T E S F O R
 D I A B E T E S O B E S I T Y & N U T R I T I O N S T R A T E G I C C L I N I C A L N E T W O R K ( D O N S C N ) I N T H I S I S S U E U P D A T E S F O R P R O V I N C I A L D I A B E T E S I N P A T
D I A B E T E S O B E S I T Y & N U T R I T I O N S T R A T E G I C C L I N I C A L N E T W O R K ( D O N S C N ) I N T H I S I S S U E U P D A T E S F O R P R O V I N C I A L D I A B E T E S I N P A T
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
The Growing Future of Diabetes: Insulin Pump Therapy in Type 1 and 2 Diabetes
 The Growing Future of Diabetes: Insulin Pump Therapy in Type 1 and 2 Diabetes Sarah Dombrowski, PharmD, BCACP Pennsylvania Pharmacists Association 10/20/18 1 Objectives At the completion of this activity,
The Growing Future of Diabetes: Insulin Pump Therapy in Type 1 and 2 Diabetes Sarah Dombrowski, PharmD, BCACP Pennsylvania Pharmacists Association 10/20/18 1 Objectives At the completion of this activity,
Perioperative Glucose Control: Creating a Shared Mental Model
 Perioperative Glucose Control: Creating a Shared Mental Model 2017 Dr. Alan Jay Schwartz: Hello. This is Alan Jay Schwartz, Editor-in-Chief of the American Society of Anesthesiologists 2017 Refresher Courses
Perioperative Glucose Control: Creating a Shared Mental Model 2017 Dr. Alan Jay Schwartz: Hello. This is Alan Jay Schwartz, Editor-in-Chief of the American Society of Anesthesiologists 2017 Refresher Courses
Disclosures. Glycemic Control in the Intensive Care Unit. Objectives. Hyperglycemia. Hyperglycemia. History. No disclosures
 Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
SARASOTA MEMORIAL HOSPITAL
 SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE MANAGEMENT OF PATIENT S OWN INSULIN PUMP/CONTINUOUS SUBCUTANEOUS INSULIN INFUSION PUMP (dia13) DATE: REVIEWED: PAGES: 08/84 11/18 1 of 7 PS1094 ISSUED
SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE MANAGEMENT OF PATIENT S OWN INSULIN PUMP/CONTINUOUS SUBCUTANEOUS INSULIN INFUSION PUMP (dia13) DATE: REVIEWED: PAGES: 08/84 11/18 1 of 7 PS1094 ISSUED
Welcome to CareLink Pro
 Reference Guide Welcome to CareLink Pro This guide was developed to serve as a reference for obtaining patient data and reviewing CareLink Pro reports. Getting Started with CareLink Pro Adding New Patients
Reference Guide Welcome to CareLink Pro This guide was developed to serve as a reference for obtaining patient data and reviewing CareLink Pro reports. Getting Started with CareLink Pro Adding New Patients
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Special Situations. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols Special Situations. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Special Situations Askiel Bruno, MD, MS Protocol PI Hypoglycemia Protocol General Concepts The hypoglycemia prevention protocol
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Special Situations Askiel Bruno, MD, MS Protocol PI Hypoglycemia Protocol General Concepts The hypoglycemia prevention protocol
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions
 Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Insulin Pump Therapy. WakeMed Children s Endocrinology & Diabetes WakeMed Health & Hospitals Version 1.3, rev 5/21/13 MP
 Insulin Pump Therapy WakeMed Children s Endocrinology & Diabetes Overview What is an insulin pump? What are the advantages and disadvantages of an insulin pump? Lifestyle Changes Food Management Exercise
Insulin Pump Therapy WakeMed Children s Endocrinology & Diabetes Overview What is an insulin pump? What are the advantages and disadvantages of an insulin pump? Lifestyle Changes Food Management Exercise
Improving Glycemic Control and Insulin Ordering Efficiency for Hospitalized Patients With Diabetes Through Carbohydrate Counting
 e1 Improving Glycemic Control and Insulin Ordering Efficiency for Hospitalized Patients With Diabetes Through Carbohydrate Counting Kristina K. Pearson, Sarah A. Reiland, John G. O Meara, Julie K. Brown,
e1 Improving Glycemic Control and Insulin Ordering Efficiency for Hospitalized Patients With Diabetes Through Carbohydrate Counting Kristina K. Pearson, Sarah A. Reiland, John G. O Meara, Julie K. Brown,
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial
 Trial") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI Agenda General protocol for control group/ intervention group Discussion of meals Hypoglycemia
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI Agenda General protocol for control group/ intervention group Discussion of meals Hypoglycemia
THERAPY MANAGEMENT SOFTWARE FOR DIABETES
 THERAPY MANAGEMENT SOFTWARE FOR DIABETES Report Report Interpretation Reference Guide Guide 2009 Medtronic MiniMed. All rights reserved. 6025274-012_a CareLink Pro Report Reference Guide 0 p.2 Adherence
THERAPY MANAGEMENT SOFTWARE FOR DIABETES Report Report Interpretation Reference Guide Guide 2009 Medtronic MiniMed. All rights reserved. 6025274-012_a CareLink Pro Report Reference Guide 0 p.2 Adherence
VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL
 VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL Background: For some time, the presence of diabetes and hyperglycemia
VANDERBILT UNIVERSITY MEDICAL CENTER MULTIDISCIPLINARY SURGICAL CRITICAL CARE TRAUMA INTENSIVE CARE UNIT GLYCEMIC CONTROL PROTOCOL Background: For some time, the presence of diabetes and hyperglycemia
Insulin Pump An information session to help you decide if you are ready to use an insulin pump.
 Insulin Pump An information session to help you decide if you are ready to use an insulin pump. Welcome Welcome to the insulin pump information session. We hope this session helps you to decide whether
Insulin Pump An information session to help you decide if you are ready to use an insulin pump. Welcome Welcome to the insulin pump information session. We hope this session helps you to decide whether
Team-Based Decision Support in Diabetes Outcomes and Costs
 Team-Based Decision Support in Diabetes Outcomes and Costs Session 89, 8:30 a.m. February 13, 2019 Gary Ozanich, Ph.D. - College of Informatics, Northern Kentucky University 1 Conflict of Interest Gary
Team-Based Decision Support in Diabetes Outcomes and Costs Session 89, 8:30 a.m. February 13, 2019 Gary Ozanich, Ph.D. - College of Informatics, Northern Kentucky University 1 Conflict of Interest Gary
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
In-Hospital Management of Diabetes
 In-Hospital Management of Diabetes Clinical order sets guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Table of Contents Key elements from the Canadian Diabetes Association 2013 Clinical Practice
In-Hospital Management of Diabetes Clinical order sets guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Table of Contents Key elements from the Canadian Diabetes Association 2013 Clinical Practice
STRENGTHENING THE COORDINATION, DELIVERY AND MONITORING OF HIV AND AIDS SERVICES IN MALAWI THROUGH FAITH-BASED INSTITUTIONS.
 STRENGTHENING THE COORDINATION, DELIVERY AND MONITORING OF HIV AND AIDS SERVICES IN MALAWI THROUGH FAITH-BASED INSTITUTIONS. Acknowledgements This project was fully funded by Center For Disease Control
STRENGTHENING THE COORDINATION, DELIVERY AND MONITORING OF HIV AND AIDS SERVICES IN MALAWI THROUGH FAITH-BASED INSTITUTIONS. Acknowledgements This project was fully funded by Center For Disease Control
Faculty. Disclosures. Prescribing. A Multidisciplinary Approach to Preventing Medication Errors Associated with Insulin Therapy. Learning Objectives
 A Multidisciplinary Approach to Preventing Medication Errors Associated with Insulin Therapy Faculty Matthew Grissinger, RPh, FISMP, FASCP Director, Error Reporting Programs Institute for Safe Medication
A Multidisciplinary Approach to Preventing Medication Errors Associated with Insulin Therapy Faculty Matthew Grissinger, RPh, FISMP, FASCP Director, Error Reporting Programs Institute for Safe Medication