Dr Larry Distiller BSc MB BCh FCP(SA) FRCP FACE Specialist Physician / Endocrinologist Centre for Diabetes and Endocrinology, Houghton Hon Visiting
|
|
|
- Lesley Watts
- 6 years ago
- Views:
Transcription


1 Dr Larry Distiller BSc MB BCh FCP(SA) FRCP FACE Specialist Physician / Endocrinologist Centre for Diabetes and Endocrinology, Houghton Hon Visiting Professor, Cardiff University School of Medicine
2 Obesity Sedentary lifestyle Aging Genetics Glucotoxicity FFA levels Insulin resistance Beta-cell function Blood glucose Adequate Insulin response Inadequate Euglycaemia Type 2 diabetes Adapted from Matthaei et al. Endocrine Reviews 2000;21: Adapted from Edelman. Adv Intern Med 1998;43:

3 And many more in development Bianchi C et al. Diabetes Voice 2011;56:28-31
4 What are the incretins and gliptins? Why should we use them? When should they be used? Should we be using them?
5 What are the incretins and gliptins?
6 Potent enhancers of glucose induced insulin secretion Glucose-dependant insulinotropic polypeptide, (GIP), formerly called gastric inhibitory polypeptide Glucagon-Like Polypeptide 1 (GLP-1)

![37] GIP [1 42] GLP-1 [7](/docs-images/72/67330461/images/7-2.jpg "36 NH 2 ] K-cell")
7 L-cell (ileum) ProGIP Proglucagon GLP-1 [7 37] GIP [1 42] GLP-1 [7 36 NH 2 ] K-cell (jejunum)



8 GLP-1: Secreted upon the ingestion of food Promotes satiety and reduces appetite Alpha cells: Postprandial glucagon secretion Beta cells: Enhances glucose-dependent insulin secretion Liver: Glucagon reduces hepatic glucose output Stomach: Helps regulate gastric emptying Data from Flint A, et al. J Clin Invest. 1998;101: ; Data from Larsson H, et al. Acta Physiol Scand. 1997;160: Data from Nauck MA, et al. Diabetologia. 1996;39: ; Data from Drucker DJ. Diabetes. 1998;47:
9 Slower gastric emptying - Direct effect on gastric emptying Feeling of satiety - Blocks satiety centre centrally Reduction in post-prandial glucose levels - Direct effect on insulin secretion (incretin effect) - Suppression of glucagon
10 Plasma Glucose (mg/dl) C-peptide (nmol/l) Oral Glucose Intravenous (IV) Glucose * * * * Incretin Effect * * * Time (min) Time (min) N = 6; Mean (SE); *P 0.05 Data from Nauck MA, et al. J Clin Endocrinol Metab. 1986;63:
11 Nauck MA, Baller B, Meier JJ. Gastric inhibitory polypeptide and glucagon-like peptide-1 in the pathogenesis of type 2 diabetes. Diabetes. 2004;53(suppl 3):S190-S196. The incretin effect is severely reduced or even abolished in patients with Type 2 diabetes Secretion of GIP is near-normal in most patients with Type 2 diabetes, but insulinotropic effect of GIP is largely ablated in type 2 diabetes, even when infused at supraphysiologic levels The secretion of GLP-1 is significantly impaired Nauck MA, Baller B, Meier JJ. Diabetes.2004;53(suppl 3):S190-S196.
 glucose infusion Adapted from Nauck M et al. Diabetologia. 1986;29:46 52.")
12 IR Insulin, mu/l IR Insulin, mu/l Control Subjects (n=8) Incretin Effect Patients With Type 2 Diabetes (n=14) The incretin effect is diminished in type 2 diabetes Time, min Oral glucose load Time, min 180 Intravenous (IV) glucose infusion Adapted from Nauck M et al. Diabetologia. 1986;29: Copyright 1986 Springer-Verlag.
13 GLP-1 (but not GIP) increases both early- and late-stage insulin secretion Data are mean±sem. GIP, gastric inhibitory peptide; type 2 diabetes patients (n=8) Vilsbøll et al. Diabetologia 2002:45:1111 9
14 Mean (SE); n=10; *p<0.05; type 2 diabetes patients (n=10) Nauck et al. Diabetologia 1993;36:741 4 Placebo (PBO) Native human GLP-1
15 The Problem Native GLP-1 and GIP are broken down by DPP-4 in 1-2 minutes The Solution? - GLP-1 analogues - DPP-4 inhibitors
16 Exenatide (Byetta, Eli Lilly) Liraglutide (Victoza, NovoNordisk) Others in the pipeline

17 Synthetic version of the salivary protein found in the Gila monster More than 50 % amino acid sequence identity with human GLP-1 Binds to known human GLP-1 receptors Resistant to DPP-4 inactivation Following injection, exenatide is measurable in plasma for up to 10 hours Nielsen LL, et al. Regul Pept. 2004;117:77-88 Kolterman OG, et al. Am J Health-Syst Pharm. 2005;62:
18 A slightly modified version of the GLP-1 molecule that attaches to albumin and therefore is released slowly, adopting the pharmacokinetic profile of albumin The plasma half-life for this compound is 12 hours. It therefore provides exposure for over 24 hours following a single subcutaneous injection
19 Vildagliptin (Galvus,Novartis) Saxagliptin (Onglyza, AstraZenica) Sitagliptin (Javunia, Merck) Linagliptin (Tradjenta, BI / Eli Lilly) Alogliptin




 Hepatic glucose")

20 Ingestion of food Release of active incretins GI tract GLP-1 and GIP Pancreas Beta cells Alpha cells Glucose dependent Insulin (GLP-1 & GIP) Glucose uptake by peripheral tissue Blood glucose in fasting and postprandial states DPP-4 inhibitor Inactive GLP-1 X DPP-4 enzyme Inactive GIP Glucosedependent Glucagon (GLP-1) Hepatic glucose production GLP-1=glucagon-like peptide-1; GIP=glucose-dependent insulinotropic polypeptide.
21 GLP-1 Analogues Supra-physiological levels of GLP-1 DPP4-Inhibitors Approaches physiological levels of GLP-1

22 *GLP-1 levels for liraglutide calculated as 1.5% free liraglutide Degn et al. Diabetes 2004;53: ; Mari et al. J Clin Endocrinol Metab 2005;90:
23 GLP-1 Analogues Supra-physiological levels of GLP-1 Significant and sustained weight loss Injected therapy Potential GIT Side-effects Low rates of hypoglycaemia Improved CV risk factors insulin secretion glucagon release food intake, slow gastric emptying DPP4-Inhibitors Approaches physiological levels of GLP-1 Weight neutral Oral therapy Minimal GIT side-effects Low rates of hypoglycaemia Limited data on CV risk factors insulin secretion glucagon release
24 What are the incretins and gliptins? Why should we use them? When should they be used? Should we be using them?
25 Why should we use them?
26 Exenatide (twice daily) Liraglutide (once daily)
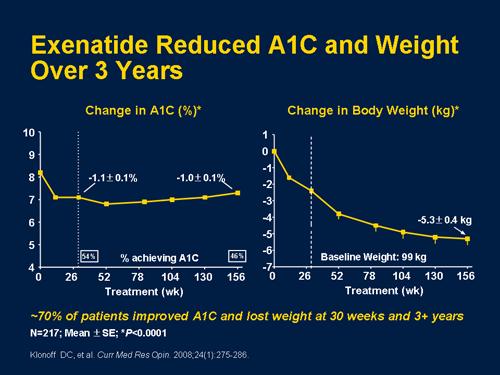
27
28 Change from baseline to 30 weeks HbA 1c (%) Body weight (kg) Existing oral therapy Exenatide 5 µg bid Exenatide 10µg bid Exenatide 5 µg bid Exenatide 10 µg bid Sulphonylurea * Metformin Metformin sulphonylurea 3 *p<0.05; p 0.01; p<0.002; p<0.001; p<0.0001; all versus placebo 1. Buse J, et al DeFronzo R, et al Kendall D, et al
29 A1C (%) Weight (kg) 104-Week Completers at Week Week Completers at Week Mean baseline A1C: 8.2% 0 Mean baseline weight: 101 kg wk Completers; N = 195; Mean (SE); Weight is a secondary endpoint Data on file, Amylin Pharmaceuticals, Inc.
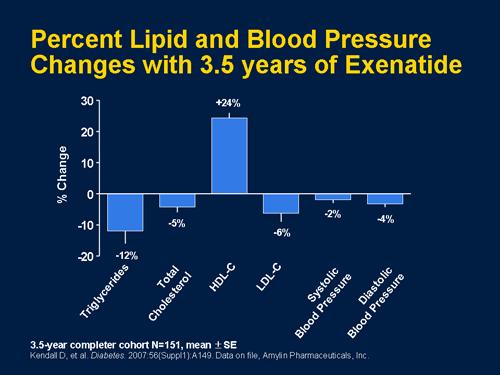
 add-on to diet and exercise failure (LEAD-3); or add-on to previous OAD monotherapy (LEAD-2,-1) Marre et al.")
30 Significant *vs. comparator; # Change in HbA 1c from baseline for overall population (LEAD-4,-5) add-on to diet and exercise failure (LEAD-3); or add-on to previous OAD monotherapy (LEAD-2,-1) Marre et al. Diabetic Medicine 2009;26; (LEAD-1); Nauck et al. Diabetes Care 2009;32;84 90 (LEAD-2); Garber et al. Lancet 2009;373: (LEAD-3); Zinman et al. Diabetes Care 2009; 32: (LEAD-4); Russell-Jones et al. Diabetologia 2009;52: (LEAD-5)
31 Weight and blood pressure did not differ between add-on and switch concept *Change calculated by ANCOVA analysis Nauck et al. Diabetes 2009;58(Suppl. 1):A122 (abstract 459-P)
32 Waist circumference was reduced from baseline by 3.0 cm with liraglutide 1.8 mg Waist circumference increased by 0.4 cm with glimepiride (p<0.0001) Glimepiride 8 mg/day Liraglutide 1.2 mg/day Liraglutide 1.8 mg/day ***p< for change from baseline Garber et al. Lancet 2009;373(9662): (LEAD-3)

33 Both liraglutide and exenatide were combined with met and/or SU Buse et al. Lancet 2009;374:39 47 (LEAD-6)

34 Buse et al. Lancet 2009;374:39 47 (LEAD-6)
35 Mean (2SE) Buse et al. Lancet 2009;374:39 47 (LEAD-6)
36 Buse et al. Lancet 2009;374:39 47 (LEAD-6)
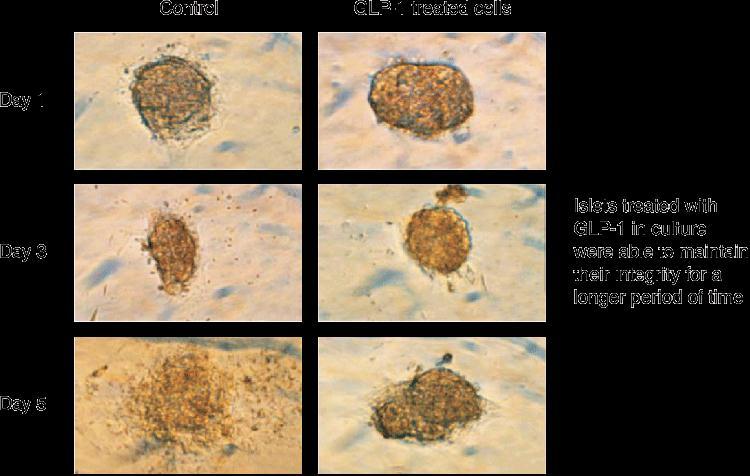
37 GLP-1 receptors are expressed in multiple organs including: Pancreas Peripheral tissue Central nervous system Heart Kidney Lung Gastrointestinal tract GLP-1 appears to have a range of neurotrophic neuroprotective and cardioprotective effects
38 GLP-1 receptors have been localized t0: Cardiomyocytes Endocardium Microvascular endothelium Coronary artery smooth muscle cells;
39 Heart (myocardium) Protects against Ischaemia / reperfusion injury Improves myocardial function Vascular System Improves Endothelial function Vasorelaxation GLP-1 The Kidney Increased diuresis and Na + excretion Adapted from: Chilton R et al. The American Journal of Medicine 2011;124, S35 S53
40 Promote Weight loss Lower Triglyceride and raise HDL Lower Blood pressure (?) Improve endothelial dysfunction Reduce CRP and other inflammatory markers Increase myocardial insulin sensitivity Increase myocardial glucose uptake Koska J et al Diabetes Care 2010;33: Courreges JP et al Diabetes Medicine 2008;25: Nikolaidis LA st al. Circulation 2004;110: Bhashyam S. Et al Circ Heart Fail 2010;3:

41 In Addition: Reduced monocyte adhesion to endothelial cells promoted by inhibition of the inflammatory response to macrophages Development of atherosclerotic lesions was suppressed in mice GLP-1 was found to enhance coronary blood flow after induced ischaemia in rats In one study, exenatide treated animals were shown to have as much as 40 % reduction in MI size when compared with controls Chilton R et al. The American Journal of Medicine 2011;124, S35 S53
42 No effect of Exenatide 10 µg on QT interval No relevant increases in the QTc interval using liraglutide once daily No prolongation of the QT interval using exenatide once weekly Chatterjee DJ et al. J Clin Pharmacol 2009;49: Amylin Pharmaceuticals. Data on file.
43
44 LifeLink Study 39,000 patients treated with exenatide were compared with [approximately] 390,000 patients treated with all other interventional strategies Significant decrease in cardiovascular events with Exenatide (hazard ratio, 0.81; [95 % confidence interval, ; P=0.01]), indicating a 16 % decrease in cardiovascular events Best JH et al. Diabetes Care 2011;34:90-95
45
46

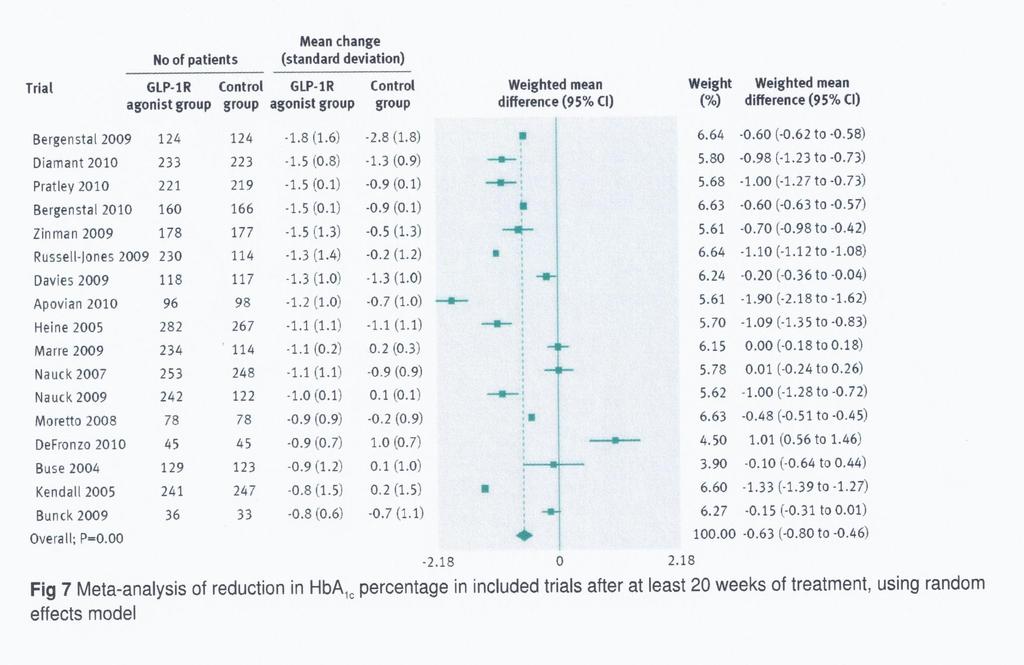
47 Vilsboll T et al. BMJ 2012;344:d7771doi: Published Jan 2012

48 Vilsboll T et al. BMJ 2012;344:d7771doi: Published Jan 2012
49 Exenatide Liraglutide Administration s.c. Twice daily s.c. Once daily Mean Reduction in HbA 1c ~o % ~ % Mean reduction in FPG ~0.6 mmol/l ~1.7 mmol/l Mean reduction in body weight 2.87 kg 3.24 kg Persistence of nausea (after 26 weeks) 10 % 5 % Liraglutide appears the better option on all fronts, but this may change with once-weekly exenatide which seems better than daily liraglutide Adapted from: Buse et al. Lancet 2009;374:39 47 (LEAD-6)
50 Vildagliptin (Galvus,Novartis) Saxagliptin (Onglyza, AstraZenica) Sitagliptin (Javunia, Merck) Linagliptin (Tradjenta, BI / Eli Lilly) Alogliptin
51 Change in A1C, % Change in FPG, mg/dl Change in 2-hr PPG, mg/dl A1C Mean Baseline: 8.0 % P<0.001* 0.8 n=229 (95 % CI: 1.0, 0.6) FPG Mean Baseline: 170 mg/dl P <0.001* 17 (95 % CI: 24, 10) n= hr PPG Mean Baseline: 257 mg/dl P<0.001* 47 n=201 (95 % CI: 59, 34) * Compared with placebo. Least squares means adjusted for prior antihyperglycaemic therapy status & baseline value. Difference from placebo.
52 Triangle, sitagliptin (100 mg qd) Circle, vildagliptin (50 mg bid or 100 mg qd) Square, saxagliptin (5 mg qd); Diamond, alogliptin (25 mg qd) Star, linagliptin (5 mg qd) C. F. Deacon CF. Diabetes, Obesity and Metabolism 2010;13:7-18
53 Sitagliptin administration at a single dose of 100 mg in patients with CAD: Preserved LV function Enhanced LV response to stress Improved global and regional LV performance compared with placebo Read PA. Circ Cardiovasc Imaging 2010; 3:
54 No definitive evidence for this as yet. Awaiting outcome of TECOS, SAVOR and other trials.
55 Why should we use them? When should they be used? Should we be using them?
56 When should they be used?
57 While the effects on glucagon, gastric emptying and satiety may well persist, the major effect of these drugs is still on insulin secretion Therefore, the better the residual insulin secretory capacity (the more β-cell reserve), the better the expected response
58 None of these drugs are registered for first-line or monotherapy But that is probably where they will prove to be most beneficial
59 Makes therapeutic sense: Basal insulin to target FPG; incretin to target PPG. Sitagliptin has registration for use with insulin. Exenatide has FDA approval for use with basal insulin. Liraglutide has been shown to be effective when combined with basal insulin.
60 When should they be used? Should we be using them?

61 DPP-4 is found on endothelial and epithelial cells throughout the vascular bed, and in the kidneys, intestines, exocrine pancreas, gastrointestinal tract, biliary tract, thymus, lymph nodes, uterus, placenta, prostate, myocardium, and brain, as well as the adrenal, sweat, salivary, and mammary glands. In addition, DPP-4 is also expressed on circulating T- lymphocytes and is found in soluble form in seminal and cerebrospinal fluid and plasma.
62 DPP-4 inhibition has not, as yet, been associated with any human disease. 96 DPP-4 inhibitors have shown a very positive safety and tolerability profile in clinical studies involving thousands of patients with type 2 diabetes DPP-4 inhibitor treatment has been associated with slightly elevated risks of nasopharyngitis, bronchitis, urinary tract infection and headaches
63 The debate rages! Case reports have raised concerns about an increased risk of acute pancreatitis in patients treated with GLP-1 agonists But Type 2 diabetes itself is said to be associated with a 3-fold increased risk of developing pancreatitis So - is the incidence of pancreatitis higher with GLP-1 analogues or is it just a case of awareness?
64 A review of 10,000 patients on 19 clinical trials in patients on sitagliptin showed no increased risk of pancreatitis In all animal studies, there is no evidence that DPP4-I cause pancreatitis Engel SS et al. In J Clin Pract 2010;64: C. F. Deacon CF. Diabetes, Obesity and Metabolism 2010;13:7-18
65 German data base identified 11 cases of pancreatic cancer in association with exenatide No such signal with DPP4-I Exenatide promotes pancreatic ductal hyperplasia However, the time between tumour induction, tumour growth and clinical diagnosis is > 10 years Exenatide exposure was 2-33 months? does exenatide promote tumour progression rather than initiation
66 Liraglutide induces thyroid C-cell focal hyperplasia and C-cell tumours in a dose-related manner in rats, which may lead to medullary thyroid cancer In a 104-week exenatide carcinogenicity study in rats, an increased incidence of benign thyroid C-cell adenomas was seen (Rats develop spontaneous C-cell lesions at a high frequency, while C-cell neoplasia is extremely rare in humans) This has not been seen in any of the clinical studies performed to date Knudsen LB. Endocrinology 2010; 151: Parks M. N Engl J Med 2010; 362:
67 Elashoff M et al Gastroenterology 2011;141:
68 We don t know! There are those who remain opposed to these drugs on basis of uncertainty There are those who believe in these drugs implicitly And many in-between! The jury is still out
69 History has taught us that enthusiasm for new classes of drugs, heavily promoted by the pharmaceutical companies that market them, can obscure the caution that should be exercised when long-term consequences are unknown Peter Butler. Diabetes Care 2010
70 We are constantly being pressurised by industry to prescribe newer and more expensive drugs For most of us, there are intangible rewards for doing this
71 Don t trust me, I m a doctor As to the honour and conscience of doctors, they have as much as any other class of men, no more and no less And what other men dare pretend to be impartial where they have a strong pecuniary interest on one side? George Bernard Shaw, 1911

72 Thank you for your attention Prediction is very difficult, especially about the future Niels Bohr
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Role of incretins in the treatment of type 2 diabetes
 Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Scope. History. History. Incretins. Incretin-based Therapy and DPP-4 Inhibitors
 Plasma Glucose (mg/dl) Plasma Insulin (pmol/l) Incretin-based Therapy and Inhibitors Scope Mechanism of action ผศ.ดร.นพ.ว ระเดช พ ศประเสร ฐ สาขาว ชาโภชนว ทยาคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล
Plasma Glucose (mg/dl) Plasma Insulin (pmol/l) Incretin-based Therapy and Inhibitors Scope Mechanism of action ผศ.ดร.นพ.ว ระเดช พ ศประเสร ฐ สาขาว ชาโภชนว ทยาคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล
Novel anti-diabetic therapies
 Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
T2DM is a global epidemic with
 : a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
: a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
Current Status of Incretin Based Therapies in Type 2 Diabetes
 Current Status of Incretin Based Therapies in Type 2 Diabetes DR.M.Mukhyaprana Prabhu Professor of Internal Medicine Kasturba Medical College, Manipal, Manipal University, India 2 nd International Endocrine
Current Status of Incretin Based Therapies in Type 2 Diabetes DR.M.Mukhyaprana Prabhu Professor of Internal Medicine Kasturba Medical College, Manipal, Manipal University, India 2 nd International Endocrine
Optimal glucose control. DM Treatment. Glucose Control one out of many. Many guidelines: Confusing. Theorectically easy
 DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
DM Treatment How to Achieve Optimal Glycaemic Control The Tung Wah Eastern Hospital Experience of DM Share Care Experience Optimal glucose control Theorectically easy More challenging in the real world
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy
 New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
Update on GLP-1 Past Present Future
 Update on GLP-1 p Past Present Future Effects of GLP-1: Glucose Metabolism and Nutritional Balance L-Cells: Glp-1 release Betacellfollowing ingestion Stress Increases satiety reduces appetite Betacell-
Update on GLP-1 p Past Present Future Effects of GLP-1: Glucose Metabolism and Nutritional Balance L-Cells: Glp-1 release Betacellfollowing ingestion Stress Increases satiety reduces appetite Betacell-
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP
 Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes
 Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes Dr Masud Haq Consultant Lead in Diabetes & Endocrinology Maidstone & Tunbridge Wells NHS Trust & The London Preventative
Injectable GLP 1 therapy: weight loss effects seen in obesity with and without diabetes Dr Masud Haq Consultant Lead in Diabetes & Endocrinology Maidstone & Tunbridge Wells NHS Trust & The London Preventative
22 Emerging Therapies for
 22 Emerging Therapies for Treatment of Type 2 Diabetes Siddharth N Shah Abstract: The prevalence of Diabetes is progressively increasing world-wide and the growth of the disease in our country is phenomenal.
22 Emerging Therapies for Treatment of Type 2 Diabetes Siddharth N Shah Abstract: The prevalence of Diabetes is progressively increasing world-wide and the growth of the disease in our country is phenomenal.
PROCEEDINGS CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES * Vivian A. Fonseca, MD, FRCP ABSTRACT
 CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES Vivian A. Fonseca, MD, FRCP ABSTRACT Despite proven lifestyle recommendations and the availability of a range of oral antidiabetic agents,
CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES Vivian A. Fonseca, MD, FRCP ABSTRACT Despite proven lifestyle recommendations and the availability of a range of oral antidiabetic agents,
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.
 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.") GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Type 2 DM in Adolescents: Use of GLP-1 RA. Objectives. Scope of Problem: Obesity. Background. Pathophysiology of T2DM
 Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Sitagliptin: A component of incretin based therapy. Rezvan Salehidoost, M.D., Endocrinologist
 Sitagliptin: A component of incretin based therapy Rezvan Salehidoost, M.D., Endocrinologist Agenda Mode of Action Evidences for sitagliptine cardiovascular safety of sitagliptin Ramadan study Impact of
Sitagliptin: A component of incretin based therapy Rezvan Salehidoost, M.D., Endocrinologist Agenda Mode of Action Evidences for sitagliptine cardiovascular safety of sitagliptin Ramadan study Impact of
DR. SUBHASH K. WANGNOO
 Photograph DR. SUBHASH K. WANGNOO M.D, D.M, FRCP (London) Senior Consultant, Endocrinologist & Diabetologist Apollo Centre for Obesity, Diabetes and Endocrinology Indraprastha Apollo Hospital, Sarita Vihar,
Photograph DR. SUBHASH K. WANGNOO M.D, D.M, FRCP (London) Senior Consultant, Endocrinologist & Diabetologist Apollo Centre for Obesity, Diabetes and Endocrinology Indraprastha Apollo Hospital, Sarita Vihar,
Drug Class Monograph
 Drug Class Monograph Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drugs: alogliptin, alogliptin/metformin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin),
Drug Class Monograph Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drugs: alogliptin, alogliptin/metformin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin),
Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function
 Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function Background. Following meal ingestion, several hormones are released from the gastrointestinal tract. Some
Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function Background. Following meal ingestion, several hormones are released from the gastrointestinal tract. Some
la prise en charge du diabète de
 N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
N21 XIII Congrès National de Diabétologie, 29 mai 2011, Alger Intérêt et place des Anti DPP4 dans la prise en charge du diabète de type 2 Nicolas PAQUOT, MD, PhD CHU Sart-Tilman, Université de Liège Belgique
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Data from an epidemiologic analysis of
 CLINICAL TRIAL RESULTS OF GLP-1 RELATED AGENTS: THE EARLY EVIDENCE Lawrence Blonde, MD, FACP, FACE ABSTRACT Although it is well known that lowering A 1c (also known as glycated hemoglobin) is associated
CLINICAL TRIAL RESULTS OF GLP-1 RELATED AGENTS: THE EARLY EVIDENCE Lawrence Blonde, MD, FACP, FACE ABSTRACT Although it is well known that lowering A 1c (also known as glycated hemoglobin) is associated
Drug Class Monograph
 Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Monograph Drugs: alogliptin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin), Jentadueto (linagliptin/metformin),
Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Monograph Drugs: alogliptin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin), Jentadueto (linagliptin/metformin),
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
Changing Diabetes: The time is now!
 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Efficacy and Safety of Sitagliptin in Various Clinical Settings of T2DM
 Efficacy and Safety of Sitagliptin in arious Clinical Settings of T2DM Young Min Cho, MD, PhD Division of Endocrinology and Metabolism Department of Internal Medicine Seoul National University College
Efficacy and Safety of Sitagliptin in arious Clinical Settings of T2DM Young Min Cho, MD, PhD Division of Endocrinology and Metabolism Department of Internal Medicine Seoul National University College
Exploring Non-Insulin Therapies in Type 1 Diabetes
 Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Approaches to Addressing Incretin Deficiency. Non-Insulin Injectable Agents. Incretin Mimetics. Exendin-4 in the Gila Monster
 Non-Insulin Injectable Agents Approaches to Addressing Incretin Deficiency Longer-acting analogs? (Incretin mimetics) GLP-1 Analogs Inhibition of inactivation? (Incretin enhancers) DPP-4 Inhibitors Drucker
Non-Insulin Injectable Agents Approaches to Addressing Incretin Deficiency Longer-acting analogs? (Incretin mimetics) GLP-1 Analogs Inhibition of inactivation? (Incretin enhancers) DPP-4 Inhibitors Drucker
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Type 2 diabetes and cardiovascular risk: the role of GLP-1
 Type 2 diabetes and cardiovascular risk: the role of GLP-1 Dr Isidora Kitsou-Mylona, PhD Novo Nordisk Regional Medical Advisor Business Area Africa, Gulf & India Disclaimer I am an employee of Novo Nordisk
Type 2 diabetes and cardiovascular risk: the role of GLP-1 Dr Isidora Kitsou-Mylona, PhD Novo Nordisk Regional Medical Advisor Business Area Africa, Gulf & India Disclaimer I am an employee of Novo Nordisk
Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors. Richard E. Pratley and Matthew Gilbert
 REVIEW Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors Richard E. Pratley and Matthew Gilbert Diabetes and Metabolism Translational Medicine Unit, University
REVIEW Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors Richard E. Pratley and Matthew Gilbert Diabetes and Metabolism Translational Medicine Unit, University
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
Liraglutide: First Once-Daily Human GLP-1 Analogue
 DRUG PROFILE KERALA MEDICAL JOURNAL Liraglutide: First Once-Daily Human GLP-1 Analogue Sreejith N Kumar Research Cell, IMA Kerala State, K-5, Kochar Road, Sasthamangalam Thiruvananthapuram* ABSTRACT Published
DRUG PROFILE KERALA MEDICAL JOURNAL Liraglutide: First Once-Daily Human GLP-1 Analogue Sreejith N Kumar Research Cell, IMA Kerala State, K-5, Kochar Road, Sasthamangalam Thiruvananthapuram* ABSTRACT Published
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes. Overview. Prevalence of Overweight in the U.S.
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Abstract. Effect of sitagliptin on glycemic control in patients with type 2 diabetes. Introduction. Abbas Mahdi Rahmah
 Effect of sitagliptin on glycemic control in patients with type 2 diabetes Abbas Mahdi Rahmah Correspondence: Dr. Abbas Mahdi Rahmah Consultant Endocrinologist, FRCP (Edin) Director of Iraqi National Diabetes
Effect of sitagliptin on glycemic control in patients with type 2 diabetes Abbas Mahdi Rahmah Correspondence: Dr. Abbas Mahdi Rahmah Consultant Endocrinologist, FRCP (Edin) Director of Iraqi National Diabetes
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens
 PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens") EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
EXENATIDE (BYETTA ) PROTOCOL, 5mcg and 10mcg SC injection pre-filled pens This document should be read in conjunction with the current Summary of Product Characteristics http://www.medicines.org.uk 1.
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION
 SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
Incretin-Based therapy for type 2 diabetes: overcoming unmet needs
 2 : 15 Incretin-Based therapy for type 2 diabetes: overcoming unmet needs Diabetes is a progressive disease characterised by impaired betacell function, and reduced insulin sensitivity and secretion. Over
2 : 15 Incretin-Based therapy for type 2 diabetes: overcoming unmet needs Diabetes is a progressive disease characterised by impaired betacell function, and reduced insulin sensitivity and secretion. Over
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Expanding Treatment Options for Diabetes: GLP-1 Receptor Agonists. Copyright
 CLINICAL Viewpoint Expanding Treatment Options for Diabetes: GLP-1 Receptor Agonists Advancements in Diabetes Management: A Canadian Diabetes Steering Committee Report Copyright Not for Sale or Commercial
CLINICAL Viewpoint Expanding Treatment Options for Diabetes: GLP-1 Receptor Agonists Advancements in Diabetes Management: A Canadian Diabetes Steering Committee Report Copyright Not for Sale or Commercial
Diabetes Meds Update Disclaimer and Important Info. Objectives. Page 1. Copyright , Diabetes Education Services
 Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
INJECTABLE THERAPIES IN DIABETES. Barbara Ann McKee Diabetes Specialist Nurse
 INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
A New Therapeutic Strategey for Type II Diabetes: Update 2008
 Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
Incretinas e inhibidores de la DPP-4. Dr. Ramon Gomis Hospital Clínic Barcelona
 Incretinas e inhibidores de la DPP-4 Dr. Ramon Gomis Hospital Clínic Barcelona El páncreas normal y el islote de Langerhans lóbulos conducto intralobulillar islote vaso Islote de Langerhans Adaptado de
Incretinas e inhibidores de la DPP-4 Dr. Ramon Gomis Hospital Clínic Barcelona El páncreas normal y el islote de Langerhans lóbulos conducto intralobulillar islote vaso Islote de Langerhans Adaptado de
Exploring Non-Insulin Therapies in Type 1 Diabetes. Objectives. Pre-Assessment Question #1. Disclosures
 Exploring Non-Insulin Therapies in Type 1 Diabetes Disclosures Dr. Cornell: Advanced Practitioner Advisory Board and Speakers Bureau: Novo Nordisk Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate
Exploring Non-Insulin Therapies in Type 1 Diabetes Disclosures Dr. Cornell: Advanced Practitioner Advisory Board and Speakers Bureau: Novo Nordisk Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate
Update on Diabetes Mellitus
 Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Scottish Medicines Consortium
 Scottish Medicines Consortium saxagliptin, 5mg film-coated tablet (Onglyza ) No. (603/10) Bristol-Myers Squibb Pharmaceuticals Ltd 05 February 2010 The Scottish Medicines Consortium (SMC) has completed
Scottish Medicines Consortium saxagliptin, 5mg film-coated tablet (Onglyza ) No. (603/10) Bristol-Myers Squibb Pharmaceuticals Ltd 05 February 2010 The Scottish Medicines Consortium (SMC) has completed
DIABETES IN 2007 What snew
 DIABETES IN 2007 What snew 1 Objectives 1. Review recently published clinical trials in diabetes What does this mean to us? 1. Discuss novel concepts in the treatment of diabetes What should we expect?
DIABETES IN 2007 What snew 1 Objectives 1. Review recently published clinical trials in diabetes What does this mean to us? 1. Discuss novel concepts in the treatment of diabetes What should we expect?
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Diabetes in the UK: Update on Diabetes Treatment and Care. Why is diabetes increasing? Obesity Increased waist circumference.
 Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Update on Diabetes Treatment and Care Tahseen A Chowdhury Consultant Diabetologist Royal London and Mile End Hospitals Diabetes prevalence (thousands) Diabetes in the UK: 1995-21 3 25 2 15 1 5 Type 1 Type
Type 2 Diabetes Novel Therapies and Difficult Cases
 Type 2 Diabetes Novel Therapies and Difficult Cases Matt Dowell, DO Type 2 Diabetes - An Epidemic Is Here 1 Age-Adjusted Prevalence of Diagnosed Diabetes Among US Adults 2005 Missing data
Type 2 Diabetes Novel Therapies and Difficult Cases Matt Dowell, DO Type 2 Diabetes - An Epidemic Is Here 1 Age-Adjusted Prevalence of Diagnosed Diabetes Among US Adults 2005 Missing data
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,