Pediatrics Protocols. Pediatric Handbook. 3rd Edition. Department of Pediatrics and Neonatology. St Stephens Hospital. Tis Hazari.
|
|
|
- Calvin Hines
- 6 years ago
- Views:
Transcription
1 Pediatrics Protocols Pediatric Handbook 3rd Edition Department of Pediatrics and Neonatology St Stephens Hospital Tis Hazari Delhi
2 Preface This protocol was prepared by Dr Neetu Vashisht, building on the work of previous editions and the work of Dr R S Beri, Dr Nirmal Kumar, Dr Vineet Tyagi and Dr Jyotsna James. The First Edition was published in 2003 and the Second Edition in This third edition has been a long time coming. The 3 rd edition is in the format of a web-based-protocol that allows up-dating and ever-greening. We will appreciate comments and suggestion for corrections at all times. You can send these to Puliyel@gmail.com This book of protocols adapts some standard protocols laid out by others, but elsewhere it merely accepts them without change. Acknowledgement in each instance would by unwieldy. References are quoted mostly for controversial recommendations only. We changed the title for this edition. It is hardly a book of protocols. It is more a handbook a ready reckoner. We used the dummy yardstick to decide what goes into the book and what goes out. Instructions were simplified that we could understand them ourselves. The new book of protocols is called Pediatric Handbook Jacob Puliyel Feburary 2011 Page 1 5/9/2017 1
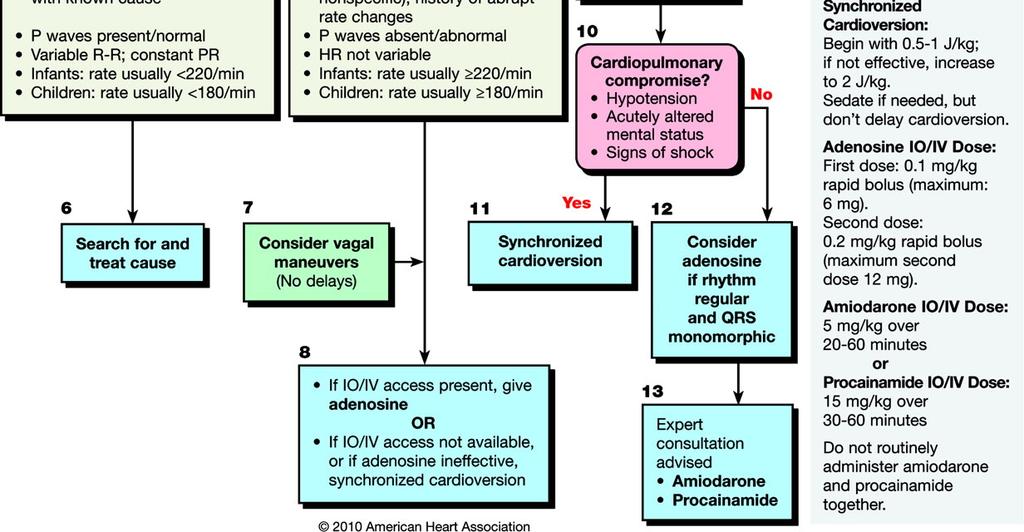
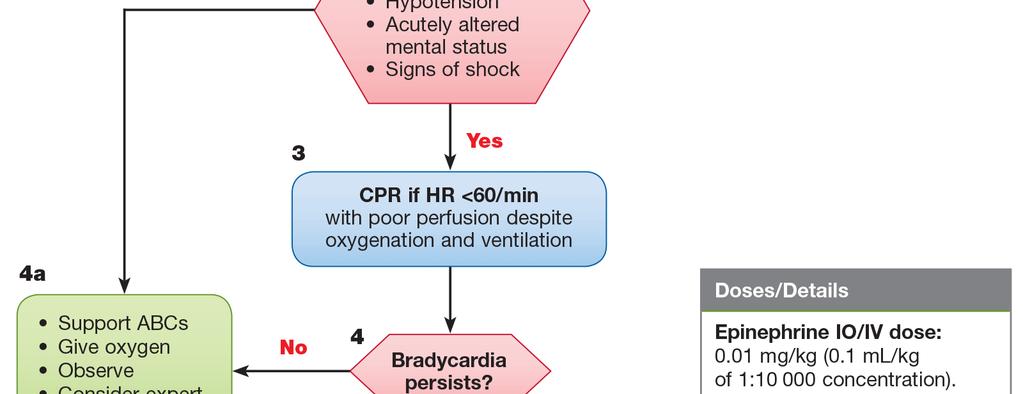
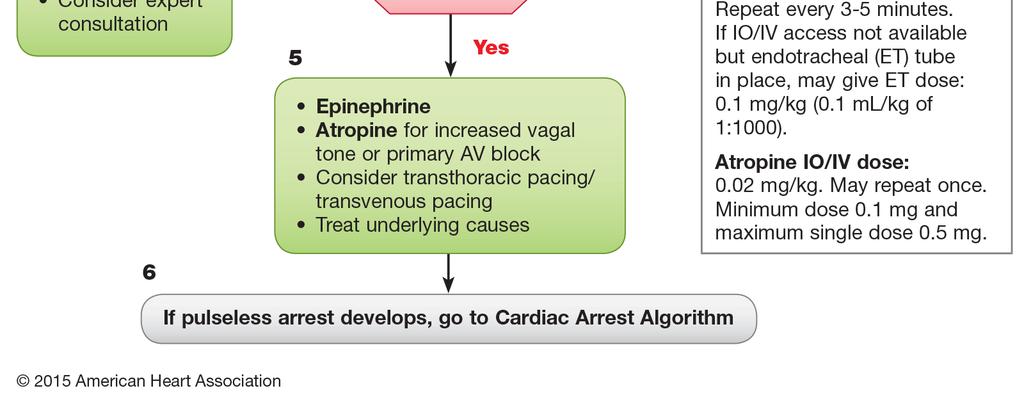
3 Contents Drug Infusions 3 Status Epilepticus 6 Status Asthamaticus/Ventlation 7 Ventilation and ARDS Management 9 Peritoneal dialysis 11 Septic Shock 12 Hypokalemia ( <3.5 meq/l ) 133 Hyperkalemia (>6 meq/l) 144 Hyponatremia (Sodium <130 meq/l) 155 Hypernatremia 166 Hypocalcemia 177 Rapid Sequence Intubation 188 Neonatal Hypoglycemia 199 TPN 20 Dengue 21 Antibiotic Guidelines 23 Miscellaneous 24 PALS Protocol Tachycardia 25 PALS Protocol Bradycardia 26 PALS Protocol Pulseless Arrest 27 Page 2 5/9/2017 2
4 Drugs and Infusions DRUG DOSE CONCENTRATION IN VIAL DILUTION INFUSION RATE DOPAMINE 5-20 microgms/kg/min 40mg/ml (Wt 6 3) mg dilute in 30 ml NS 1ml/hr =10mcg/kg/min DOBUTAMINE 5-20 microgms/kg/min 25mg/ml (Wt 6 3) mg dilute to 30 ml NS 1ml/hr =10mcg/kg/min ADRENALINE microgms/kg/min 1mg/ml (Wt 0.6) mg dilute in 10 ml NS 1ml/hr =1mcg/kg/min FENTANYL 1-4 microgms/kg/hr MPHINE microgm/kg/hr MIDAZOLAM 1-24 microgms/kg/min 50 micrograms/ml (Wt 40) mcg dilute in 40 ml NS 15 mg/ml (Wt 0.5) mg dilute in 50 ml 5% Dextrose 5 mg/ml (Wt 0.6 5) mg dilute in 50 ml NS 1ml/hr =1mcg/kg/hr 1ml/hr =10mcg/kg/hr 1ml/hr =1mcg/kg/min VECURONIUM mic/kg/min or o mg/kg/hr NEPINEPHRINE microgms/kg/min As powder, 10 and 20 mg, dilute 10 mg vial in 2 ml NS (i.e 5mg/ml) 1mg/ml (Wt X0.6 X 5 ) mg dilute in 50 ml NS (Wt 0.6) mg dilute in 10 ml NS 1ml/hr = 1 mcg/kg/min 1ml/hr =1mcg/kg/min VASOPRESSIN 0.02 to 0.06 unit/kg/hour MILRINONE Load 0.5 mcg/kg in 10 minutes follow by to 0.75mcg/kg/min PROSTAGLANDIN microgms/kg/min May need to go up to 0.4 microgram/kg/min 20 units / ml 1 unit/kg in 50 ml 5% dextrose 1mg/ml 0.25mg/ml or 250mcg/ml or 500mcg/ampoule ( 1 ampoule = 2ml = 0.5mg ) Wt X 0.6 mg dilute in 10 ml NS (Wt ) mg dilute in 30 ml NS Works well for babies less than 2.5 kg For 5 kg child add to 15 ml NS (Wt ) For 4 kg child add to 20 ml (Wt ) For 3 kg child add to 25 ml (Wt ) 1-3 ml/hour 1ml/hr = 1 mcg/kg/min 1ml/hr =0.1mcg/kg/min NITROGLYCERINE 0.5mcg/kg/minute - 5mcg/kg/minute Increase every 5 minutes NITROPRUSSIDE KETAMINE 0.3mcg/kg/minute to 4mcg/kg/minute 5mg/ml (10 ml vial = 50 mg) 25mg/ml (Wt 0.6) mg dilute in 10 ml dextrose (Wt X 0.6 X 3) mg dilute in 30 ml 5%D 5-20 mic/kg/min 50mg/ml Wt X 3 X 3 mg dil in 30 ml NS 1ml/hr =1mcg/kg/min Start at 0.5ml/hour. Increase every 5 minutes by 0.5ml/hour 1ml/hour =1mic /kg/min 1 ml/hr= 5 mic/kg/min Ketamine IM 1.5 to 2 mg/kg IM X 1 dose Page 3 5/9/2017 3
5 SILDENAFIL 5-8mg/kg/day given 8 hourly 1mg/kg/dose tid (IJP 2015: page 1131) Available as tablets, suspension to be made from pharmacy, as desired Bosentan 2mg/kg BD Niedipine 2-5 mg/kg/day in 3 divided doses Amlodipine Adenosine (SVT) mg/kg/day in BD doses 0.1mg/kg (max 6 mg as first dose). Repeat with 0.2mg/kg if needed - in absence of response (max 12 mg as repeat dose) 3mg/ml(2ml ampoule) To be administered as rapid IV push followed by NS flush. Dilute 1ml adenosine in 2 ml normal saline as stock solution. (1mg/ml) USE 0.1 to 0.2 ml per Kg Amiodarone (SVT) 5mg/kg IV in minutes. Repeat if needed. 50mg/ml For infusion: Wt X 3 X 3 mg dilute in 30 ml NS 1 ml/hr= 5 mic/kg/min Followed by continuous infusion of 5 mic/kg/min upto a max of 10mic/kg/min Loading dose:1mg/kg Lignocaine followed by continuous infusion of 20-50mic/kg/min Procainamide (SVT) Loading dose :10-15mg/kg max of 1g over 30 to 60 minutes. 100mg/5 ml or 20mg/ml 100mg/ml or 500mg/ml For infusion Wt X 3 X 12 mg dilute in 30 ml NS For infusion Wt X 4.5 X 12 mg dilute in 30 ml NS 1 ml/hr= 20 mic/kg/min 1 ml/hr= 30 mic/kg/min Aropine Digoxin Followed by continuous infusion of 30-80mic/kg/min 0.02mg/kg (min 0.1mg, max 0.5 mg in smaller children and 1mg in adolescents) LOADING DOSES 0.1mg/ml MAINTAINENCE DOSES Available as Preterm neonate IV: mic/kg, Oral:20-30mic/kg Preterm neonate IV: 4-9- mic/kg/day Oral: 4-12mic/kg/day Inj:100,250mic/ml Elixir: 50mic/ml Term neonate IV: 20-30mic/kg, Oral: 25-35mic/kg Term neonate IV: 6-8mic/kg/day Oral: 6-10mic/kg/day 1-2 Years IV: mic/kg, Oral:40-50mic/kg 2-5 Years IV: 25-35mic/kg, oral:30-40mic/kg 5-10 Years IV: 5-30 mic/kg, Oral: 20-35mic/kg 1-2 Years IV: 8-10 mic/kg/day Oral: 10-15mic/kg/day 2-5 Years IV: 6-8mic/kg/day, Oral: 8-10mic/kg/day 5-10 Years IV: 4-8 mic/kg/day, Oral:5-10mic/kg/day Page 4 5/9/2017 4
6 Carnitine Baclofen Enoxaparin (Low molecular weight Heparin) Levothyroxine Enalapril Nifedipine Give half dose stat followed by ¼ dose twice in 8-12 hrs 50 mg/kg as loading dose followed by 50mg/kg/day as maintenance in 4 or 6 divided doses 2-7 years age oral route: mg/day, titrate to effect and increase every 3 days by 5-15mg/day 8 years age: Titrate to effect, max dose of 60mg/day Prophylaxis in > 2 months age for DVT or pulmonary embolism: 0.5mg/kg SC in 2 divided doses Treatment of the same: 1mg/kg SC in 2 doses. Titrate to desired anti factor Xa level (0.1-1u/ml) Do not administer IV or IM 0-6 months:8-10mic/kg/day 6-12months:6-8mic/kg/day 1-5yrs:5-6mic/kg/day 6-12yrs:4-5mic/kg/day >12yrs:2-3mic/kg/day Start with oral dose of 0.1mg/kg/day in 2 divided doses (max 5mg) Titrate upto 0.5mg/kg/day in 2 divided doses (max 40mg/day) mg/kg/day PO in 2 or 4 div doses Divide oral maintenance doses in 2 doses to 4 doses 100mg/ml solution for oral use or 200mg/ml for IV use Available as tablets in strengths of 10,20 mg 100mg/ml only for Sub Cutaneous administration only Tablets strengths: 25, 50, 75, 100, 125, 150, 175, 200, 300 mcg Available as tablets in strengths of 2.5, 5, 10, 20 mg. Available as capsules 10, 20 mg Hypertensive emergency: mg/kg/dose PO/Sublingual (max 10 mg) can repeat in 4-6 hrs Read add in 30 ml NS to mean: Add drug to normal saline (NS) to reach desired volume of 30 ml. Similarly for Dextrose (D). Page 5 5/9/2017 5
7 Status Epilepticus Oxygen Dextrose infusion 0-5 Minutes IV Lorazepam in doses of 0.1 mg/kg/dose Or Medazolam 0.2mg/kg/dose 5-10 Minutes Repeat above dose of IV Lorazepam or Medazolam Minutes IV Phenytoin in dose of 20mg/kg (1g max) (over 20 1mg/kg/min Inj Fosphenytoin dose 20 mg/kg of Phenytoin equivalents. (Can be infused three times 3 mg/kg/min) 35 Minutes Loading dose of Inj Valproate 30 mg/kg (1:1 dilution in NS over 10 minutes) Inj 20 mg/kg Inj mg/kg (@ 5 mg/kg/min ) If Responds 45 Minutes No response 45 Minutes If response is seen to Valproate: Follow the loading dose by continuous 5 mg/kg / hour (till 6 hours seizure free period) and taper by 1 mg/kg/hr every 2 hrs. Start maintenance dose of 10 mg/kg/dose 8 hourly when tapering Valproate. Consider elective intubation at this juncture. Propofol infusion 2-5 mg/kg IV bolus followed by 1-4 mg/kg/hr Midazolam Infusion 2-24 mcg/kg/min (after 24 hr seizure free period taper by 1 mic/kg/min every 3 hours) Thiopentone infusion Of 2-4 mg/kg bolus followed by 2-4 mg/kg/hr infusion (Titrate with EEG, increments of 1 mg/kg/hr every 30 minutes upto max of 6 mg/kg/hr or till burst suppression pattern attained) Reduce Intra cranial tension Mannitol Hypertonic saline Diuretics Hyperventilate ACTH mg ( IU)/kg/day and a total ACTH dose of mg (44-60 IU)/kg resulted in better mental development than smaller doses of ACTH (Ito M Pediatr Neurol. 1990;6: Page 6 5/9/2017 6
8 Status Asthamaticus Oxygen + Nebulised beta agonists + IV Steroids + inhaled Ipratropium bromide IV loading dose followed by maintenance dose of 5mg/kg/dose Q 6 hourly IV 2mg/kg as loading dose followed by maintenance dose of mg/kg Q 6 hourly Reassess in 1 hour Good response No response PICU Transfer IV Terbutaline in bolus dose of 10 mcg/kg in 30 minutes followed by IV infusion of mcg/kg/min SC Terbutaline 0.005mg/kg 6 hourly (max 0.3 mg) (It is to be noted that the sc and iv preparations of terbutaline are separate and cannot be interchanged for administration ) IV Salbutamol 15mcg/kg IV bolus over 10 minutes (Reference: Ped Critical Care Med 2002) IV Magnesium Sulphate mg/kg as infusion over 20 Minutes Dilute to 30 ml (D5 N/5 ) (max dose is g/dose ) IV Aminophylline (with O 2 on flow) at loading dose of 5-6 mg/kg followed by following rates: 2 6 months: 0.4 mg/kg/hr 6 11 months: 0.7 mg/kg/hr 1 9 year: 1 mg/kg/hr 9 12 year: 0.9 mg/kg/hr 12 year & above: 0.5 mg/kg/hr Not to exceed continuous infusion rate > 25 mg/minutes SC Adrenaline 0.01 mg/kg -0.3 mg (max dose) (every 20 minutes for 3 doses) Neutralize Metabolic Acidosis (Base Excess if more than 10) with NaHCO 3 MgSO 4 50 mg/kg (0.1ml/kg) over 30 minutes Methylprednisolone 2-3 mg/kg/day Turbutaline 5-10 ug/kg loading over 10 minutes Follow by 0.4 ug/kg/minutes Increase by 0.2 ug/kg/minute every minutes Maximum 10ug/kg/min Page 7 5/9/2017 7
9 Ventilation indications Exhaustion Lethargic Silent chest Worsening SpO2 Asthma Ventilation Strategy Use ketamine Low PIP (low volume) Slow rate Low PEEP Allow permissive hypercarbia. Page 8 5/9/2017 8
10 Ventilation and ARDS Management Definition ARDS = PaO 2 / FiO 2 < 200. (ALI = PaO 2 / FiO 2 < 300) ARDS = Saturation less than 100% (PaO 2 less than 100) in 50% O Acute onset respiratory distress Radiographic infiltrates (bilateral patchy, diffuse or homogenous consistent with pulmonary edema like in CCF) Normal heart size suggesting absence of CCF Target SpO2 88% to 95% Target P Plateau less than 30 mm of Hg Start with FiO2 0.5 to 0.6 Start with volume ventilation of 8ml/kg Start with PEEP of 10 mm of Hg Start with age appropriate rate (40 in neonate and 20 in older kids) Saturations more than 88% Saturations less than 88% P plat less <30 Every 2 hour Wean till FiO2 0.4 PEEP 8 mm Hg Then try SBT P plat more >30 Reduce volume by 1ml/kg Come down to 6ml/kg P plat more >30 1. Increase PEEP (upto 15) 2. Increase Rate (upto 35) 3. Single dose paralysis 4. Try to reduce P plat. (Reduce volume by 1 ml) P plat less <30 Increase volume by 1ml/kg Permit hypercarbia if ph >7.3 o If ph low (below 7.15) and Not Metabolic Acidosis (See Base Excess) Increase RR up to 35 in older children (or 60 in neonates) or PCO Better? Try SBT NOT BETTER? Lasix Prone ventilation HFO Page 9 5/9/2017 9
11 Spontaneous Breathing Trial (SBT) FiO and PEEP 8. Systolic BP 75 + Age mm Hg. If all above criteria are met for at least 12 hours: Try SBT up to 2 hours Put on FiO2 < 0.5 and PEEP < 5: Place on T-piece with CPAP 5 cm H 2 O PEEP 5 cm H 2 O; PSV < 10 (ET size 3) and <5 for adult ET Assess for tolerance as below for up to two hours. a. SpO 2 90: and/or PaO 2 60 mmhg b. Spontaneous V T 4 ml/kg PBW c. RR 35/min d. ph 7.3 e. No respiratory distress (distress= 2 or more) HR > 120% of baseline Marked accessory muscle use Abdominal paradox Diaphoresis Marked dyspnea Reference NIH NHLBI ARDS Clinical Network Volume ventilation Broad target guidelines Start with 8 ml / kg Safe volume is 6 ml / kg Minute Ventilation is 200 ml/kg/minute in newborns Going down to 100 ml/kg in adults Page 10 5/9/
12 Peritoneal dialysis Monitor Vitals Sedate with Benzodiazepines Empty bladder, prepare abdomen Pre-warm PD fluid to body temperature Add Heparin (1000 u/l) to PD fluid Inject PD fluid through 14 g needle into peritoneal cavity initial infusion is 20 ml/kg Pass stylet through needle and remove needle, to thread 14 gauge canula over stylet Initial infusion volume of ml/kg, Increase upto ml/kg as tolerated. (usual amount is ml/kg ) Stop Heparin after 2 cycles if returns are clear No Potassium to be added to PD fluid unless Serum k < 5 meq/l Dwell time of mins Outflow time of mins 1 Cycle/hr Remove PD Catheter after 3-5 days Monitoring: Monitor Vitals Monitor Urine output Renal function and electrolytes at the end of 3 rd, 10 th and 20 th cycles Blood Gas at the end of 3 rd, 10 th and 20 th cycles 4 Hourly Blood Glucose Blood Counts, Gram staining, Cultures of drained PD fluid once or twice a day Blood cultures at the end of PD PD catheter tip for fungal smear and culture Page 11 5/9/
13 Septic Shock The following should be achieved in the first hour of management: 1. Airway 2. Breathing (Oxygen) 3. Circulation Fluid Bolus 20 ml/kg with Isotonic Crystalloids, going up to 60 ml/kg (may use Colloids instead of Crystalloids) 4. Correct Hypoglycemia and Hypocalcemia 5. Start Antibiotics 6 Stress dose 2mg/kg iv stat, followed by 2 mg/kg/day for 48 hours, as continuous infusion Fluid Responsive: (responding to 2-3 fluid boluses) Capillary filling time improves to< 2 seconds Peripheral core temperature difference becomes < 3 degrees C Heart rate normalizes Urine output improves to > 1 ml/kg/hr Consciousness improves Serum lactates decrease Base deficit decreases B P normalises NON FLUID RESPONSIVE NMOTENSIVE ScVO 2 <70% HYPOTENSIVE VASODILATED ScVO 2>70% Warm Shock Sepsis (High pulse volume) HYPOTENSIVE VASOCONSTRICTED ScVO 2 <70% Cold Shock (Low pulse volume) DOPAMINE 5-20mcg/kg/min DOBUTAMINE 5-20mcg/kg/min HYDROCTISONE Dilute 1mg in 1ml dextrose Give 1mg/kg over 5 minutes follow by 1mg/kg Q8H over 30 minutes (Day 1) 0.5mg/kg Q12H (Day 2) 0.25mg/kg Q12H (Day 3) 0.125mg/kg Q12H (Day 4) Nelson suggests giving Stress dose 50 mg/kg Max dose 300mg DOPAMINE 5-20mcg/kg/min DOBUTAMINE 5-20mcg/kg/min HYDROCTISONE Dilute 1mg in 1ml dextrose Give 1mg/kg over 5 minutes follow by 1mg/kg Q8H over 30 minutes (Day 1) 0.5mg/kg Q12H (Day 2) 0.25mg/kg Q12H (Day 3) 0.125mg/kg Q12H (Day 4) Nelson suggests giving Stress dose 50 mg/kg Max dose 300mg NEPINEPHRINE 0.05 to 1.5 mcg/kg/min DOPAMINE 5-20mcg/kg/min DOBUTAMINE 5-20mcg/kg/min HYDROCTISONE Dilute 1mg in 1ml dextrose Give 1mg/kg over 5 minutes follow by 1mg/kg Q8H over 30 minutes (Day 1) 0.5mg/kg Q12H (Day 2) 0.25mg/kg Q12H (Day 3) 0.125mg/kg Q12H (Day 4) Nelson suggests giving Stress dose 50 mg/kg Max dose 300mg EPINEPHRINE 0.1 to 3 mcg/kg/min Page 12 5/9/
14 MILRINONE 50 mcg/kg (0.05mg/kg)] Preparation: 1mg/ml (Sufficient for 20 kg) Follow by 0.5 to 1mcg/kg/minute (Wt X 0.6)mg dilute in 20ml NS Run at 1ml/hr= 0.5mcg/kg/min VASOPRESSIN 0.02 to 0.06 u/kg/hour Prepare 20 units / ml Add 1 unit per kg in 50 ml of 5% dextrose Dose 1-3 ml/hour NITROPRUSSIDE 0.5 to 4 mcg/kg/min (can be used only in normotensive cold shock and not in hypotensive Hypokalemia ( <3.5 meq/l ) ECG changes in severe Hypokalemia: Prominent u waves, diphasic T waves, ST segment depression, apparent QTC prolongation, PR interval prolongation, sino-atrial block. Serum Potassium Infusion Rates Add IV Potassium 40 meq/l to 60 meq/l ml KCl provides 2O meq/l if added to 100 ml of Potassium free fluid. < 2.5 Severe Symptomatic Hypokalemia Speak to Consultant Rapid correction meq/kg Run in 1 hour and STOP. Remember this is nearly 200mEq/L (Central vein) Wt 0.5/2 ml KCl dilute in 5%Dextrose Add this to 50 ml in child less than 10 kg Add to 100 ml in 10 to 20 kg child Add to 150 ml in kg child Add to 200 ml if more than 30 kg Run in 1 hour Page 13 5/9/
15 Hyperkalemia (>6 meq/l) Normal ECG ( Potassium = 6-7 meq/l) Abnormal ECG ( Potassium >7 meq/l ) (peaked T waves, loss of p waves, widened QRS complex, sine waves, AV blocks, bradycardia, ventricular arrhythmias ) 1. Stop all Enteral AND Parenteral Potassium 1. IV Calcium Gluconate in dose of 1 ml/kg/dose over 3-5 minutes. Repeat the second dose after 10 minutes if required. 2. Sodium polysterene resin 0.25 to 1gm/kg orally or rectally one to 4 times daily 2. IV Sodium Bicarbonate 1-2 meq/kg over 5-10 minutes 3. Subcut Crystalline Insulin in doses of 0.1 u/kg WITH 2 ml/kg of 25% Dextrose (0.5 g/kg ) in 30 minutes. Repeat dose in minutes begin a continuous infusion of Insulin at 0.1u/kg/hr ml/kg/hr of 25 % dextrose 4. Salbutamol inhaled IV Salbutamol of 4 Microgram/kg in 20 minutes 5. Sodium polysterene resin 1gm/kg orally or rectally 6. Dialysis Page 14 5/9/
16 Hyponatremia (Serum Sodium <130 meq/l) GI loss And Dehydration Water Intoxication SIADH Renal Salt Wasting High BUN Fe Na >1 % Fe Na >1% Fe Na >1% High Urine Osmolarity Oliguria Low Urine Osmolarity Polyuria High Urine Osmolarity > 100 mosm/l Oliguria High Urine Osmolarity Polyuria Replace deficit with 0.9% NaCl over 48 Hours Restrict Water + Replace Urine Sodium Losses Restrict Water to 2/3 Maintenance using 0.9% NaCl Replace Urine Sodium Losses + Replace Water Deficit as 0.9% NaCl Treatment of Hyponatraemia SYMPTOMATIC (seizures, deeply comatose, depressed respiration) Consider intubation and ventilation 3% NS through central vein (don t delay while administering anticonvulsants simultaneously): to be given as 2 ml/kg over minutes (1ml/kg of 3% NS raises serum sodium by 1 meq/l). Repeat infusion if symptoms persists up to 3 times. Aim is to raise the plasma sodium till CNS symptoms resolve and/or change in plasma sodium <12 mmol/l/24hrs or plasma sodium becomes 125 mmol/l. Risk of Central Pontine Myelinolysis if rapidly corrected especially in long standing hyponatraemia. Acute hyponatraemia is more symptomatic and is also safer to treat with hypertonic saline. ASYMPTOMATIC Treatment with half normal saline is often all that is needed. Restrict fluids to 60% of maintenance ( IVF or enteral feeds ) 3% NS to achieve change in plasma sodium by 1-2 meq/l/over 30 minutes Lasix if edematous Page 15 5/9/
17 Hypernatremia Free water deficit estimation (FWD) = 0.6 Wt (1 145/current sodium) (As total body water is 60% of the body weight) STRATEGY Use Maintenance fluid +additional 30% of maintenance (for correction of hypernatraemic dehydration slowly) Choice of fluids In Hypernatremia: Replacement fluid in absence of complicating factors: Half Normal Saline If with shock: NS 5% Albumin If due to Sodium overload: add Sodium free fluid like 5% dextrose in addition to loop diuretic If associated with Hyperglycemia: use 2.5 % dextrose. Do not use Insulin for hyperglycemia as that can cause precipitous fall in Plasma Glucose/Osmolarity with subsequent cerebral edema. Monitor Serum Sodium 4 hourly Correct concomitant Hypocalcemia Add 40mEq/l of KCl if patient passes urine well. If Sodium > 200mEq/l: Peritoneal Dialysis If associated with Diabetes Insipidus: use DDAVP, Diuretics, VASOPRESSIN. Page 16 5/9/
18 Hypocalcemia ECG changes in Hypocalcemia: prolonged QTc interval Asymptomatic No Bolus. 10% Ca Gluconate 8ml/Kg/Day 80 mg/kg/day Elemental Calcium PO for 2 Days Repeat Serum Calcium If normal,taper to 4ml/kg/day of IV Calcium 40 mg/kg/day elemental Calcium PO for 1 Day Symptomatic 10% Cal Gluconate as Bolus of 2ml/kg diluted in 1:1 dilution using 5%DEXTROSE. CAN RUN IN 10 TO 20 MINUTES Repeat Bolus if no response occurs Follow it with IV infusion of 8ml/kg/day for 48 hrs of Ca Gluconate Taper to 4ml/Kg/day of Cal Gluconate 40 mg/kg/day of elemental Calcium for 1 Day Hypocalcaemia in an Older Child 1-2 ml/kg of 10% calcium gluconate ( mg/kg) IV stat in minutes under cardiac monitoring Followed by 20-50mg/kg/hr ( ml/kg/hr ) Run this for 4 hours only. Check serum levels before starting infusion for next 4 hours. Stop infusion when calcium levels reach 8mg% May need to supplement with magnesium also Page 17 5/9/
19 Rapid Sequence Intubation 1. PREMEDICATION Atropine Children below 5 years of age Also indicated for all patients where Succinylcholine is used Vecuronium or Pancuronium Defasciculation 0.01 mg/kg if Succinylcholine is used Llidnocaine in cases of head injury and increased ICT in dose of 1mg/kg 2. SEDATION as below Normotensive Lorazepam Hypotensive Ketamine Status Epilepticus Lorazepam Asthama Ketamine 3. PARALYSE Succinylcholine Dose 1 to 1.5mg/kg Vecuronium Dose 0.1mg/kg 4. INTUBATE Page 18 5/9/
20 Neonatal Hypoglycemia (below 45mg/dl) Glucose Delivery Rate (GDR) (mg/kg/min) = % dextrose X Volume (ml/kg/day) ASYMPTOMATIC SYMPTOMATIC Blood Glucose <45 mg/dl but >30mg/dl Blood Glucose < 30 mg/dl 2ml/kg Bolus of 10% GLUCOSE in 10 Minutes Feed Immediately and repeat Blood Glucose in 1 hour If Blood Glucose still <45 mg/dl Immediately follow it up with GDR of 6-8 mg/kg/min Feed 2 Hourly and monitor Blood Glucose 6 Hrly Recheck Blood Glucose in 30 minutes and then every 1 hour till stable, else increase GDR by 2 mg/kg/min up to a max of 15 mg/kg/min Stop monitoring if Blood Glucose normal for 48 hrs 1. If no response occurs, use 5mg/kg/dose 12 hourly. 2. Consider using diazoxide/glucagon 3. Investigate for refractory hypoglycemia If stable for 24 hours, taper by 2mg/kg/min every 6 hrs and stop IV Glucose when GDR is 4mg/kg/min and simultaneously hike feeds. Page 19 5/9/
21 TPN Made Simple Glucose 10% or 12.5% Isolyte P for maintainance electrolytes Heparin 1 unit/ml of above MVI add 1 ml to days fluid Aminoacid From day 1 if enteral feeding not anticipated for 5 days Add 15 ml to 85 ml AA to Isolyte P Day 3 add 20 ml AA to 80 ml Isolyte P Day 5 add 25 ml AA to 75 ml Isolyte P Day 7 add 30 ml AA to 70 ml Isolyte P Run through long line Don t break the line for another infusion After 1 days lipids may be added Infuse 2.5ml/kg of 20% Intralipid Day 3 run 5 ml/kg (0.2ml/kg/hour) Day 5 run 7.5 ml/kg (0.3ml/kg/hour) Day 7 run 10 ml/kg (0.4 ml/kg/hour) Day 9 run 12.5 ml /kg (0.5ml/kg/hour) Day 11 onwards run 15 ml/kg (0.6 ml/kg/hour) This is the maximum of 3 gm/kg/day Run lipid through a peripheral line Page 20 5/9/
22 Dengue Danger signs Persistent vomiting, not drinking. Severe abdominal pain. Lethargy and/or restlessness, sudden behavioral changes. Bleeding: Epistaxis, black stool, haematemesis, excessive menstrual bleeding, dark colored urine (haemoglobinuria) or haematuria. Pale, cold and clammy hands and feet. WHO Protocol for fluid management on next page Page 21 5/9/
23 Page 22 5/9/
24 PICU Antibiotic guide A child being shifted to PICU for worsening sepsis may need up gradation of antibiotics after discussion with the consultant. Following system may be used. GRADE 1: Cefotaxime / Ceftriaxone with or without Amikacin / Gentamycin Amoxycillin with or without Clavulinic acid Ampicillin with or without Gentamycin GRADE II Piperacillin tazobactam (poor CSF penetration) + Amikacin Cefoperazone /sulbactam (Magnex) + Amikacin Ceftazidim (Fortum) with or without vancomycin / Linizolid (compromised CSF Penetration) GRADE III Meropenem / Imipenam cilastatin + Vancomycin / Linizolid Empirical addition of disease/ system specific antibiotic (ATT/ septran / clindamycin / acyclovir / fluconazole / amphotericin) GRADE IV (Must be avoided in the absence of sensitivity evidence / avoid as single agent) Colistin Polymyxin B Phosphomycin Other supportive care / agent: only after multidisciplinary or departmental meeting Exchange transfusion for sepsis IVIG for sepsis Page 23 5/9/
25 Miscellaneous PEF (5 Height in cm) - 400(+/-50) Systolic BP 70 + (Age X 2) Diastolic BP 55 + Age Endotracheal tube For Child over 1 year = (Age[Y] divided by 4 ) + 4 size Preterm 2.5 Term 3 1 year 4 Endotracheal tube (Age[Y] divided by 2) + 12 length ET size X 3 Cricothyroid needle 14 gauge needle with 3 mm ET adapter Drug infusion (Weight 0.6 mg) Add to 10 ml calculation Run 1 ml/hour = 1 microgram/kg/minute Empyema Streptokinase 2.5 to 3 lakh units in 100 ml saline. Retain 4 hours (Cost Rs 1500) SaO 2 between 90 SaO 2 30 = PaO 2 and 60% Weight in <12 Age(in months) +9/2 months of age Weight ( 1-6 yr age) (Age X2)+ 8 Weight(> 6 yrs age) (Age X 7)-5/2 Height( >2 yrs) (Age X 6) +77 pao 2 (760-47) X FiO 2 - paco 2 /0.8 Subcutaneous effusion of IV fluid especially Calcium Apply Nitroglycerine ointment locally every 4 hours Page 24 5/9/

26 Page 25 5/9/

27 Page 26 5/9/

28 Page 27 5/9/
NEWBORN EMERGENCY TRANSPORT SERVICE MEDICAL GUIDELINES
 WOMEN AND NEWBORN HEALTH SERVICE King Edward Memorial Hospital NEWBORN EMERGENCY TRANSPORT SERVICE MEDICAL GUIDELINES Transport Medication List Title of policy: Transport Medication List Date Revised:
WOMEN AND NEWBORN HEALTH SERVICE King Edward Memorial Hospital NEWBORN EMERGENCY TRANSPORT SERVICE MEDICAL GUIDELINES Transport Medication List Title of policy: Transport Medication List Date Revised:
IDS. Pediatric Donor Management
 IDS Guidelines for Clinical Management of Organ Donors: Weight < 40 kg Organ Perfusion & Hormonal Replacement Guidelines: Normal HR, SBP: (see chart below) Urinary output of 1-3 cc/kg/hr CVP 6-10 mmhg
IDS Guidelines for Clinical Management of Organ Donors: Weight < 40 kg Organ Perfusion & Hormonal Replacement Guidelines: Normal HR, SBP: (see chart below) Urinary output of 1-3 cc/kg/hr CVP 6-10 mmhg
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Resuscitation Fluids
 Resuscitation Fluids Acceptable Fluids (also known as): Sodium Chloride Hartmann s Solution (Ringer-Lactate Solution, Compound Sodium Lactate) 4.5% Albumin Solution (PPS) Gelofusine 20ml/kg Bolus Can be
Resuscitation Fluids Acceptable Fluids (also known as): Sodium Chloride Hartmann s Solution (Ringer-Lactate Solution, Compound Sodium Lactate) 4.5% Albumin Solution (PPS) Gelofusine 20ml/kg Bolus Can be
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Drug Max dose approved for IVP Dilution Rate Monitoring Parameters. Dilution not necessary (Available in prefilled syringe)
") Drug Max dose approved for IVP Dilution Rate Monitoring Parameters Acetazolamide 500 mg Reconstitute with at least 5ml sterile water (max concentration should not exceed 100mg/ml) 100-500 mg/min Hypotension
Drug Max dose approved for IVP Dilution Rate Monitoring Parameters Acetazolamide 500 mg Reconstitute with at least 5ml sterile water (max concentration should not exceed 100mg/ml) 100-500 mg/min Hypotension
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
DRUGS FOR VIVA. IAP UG Teaching slides
 DRUGS FOR VIVA 1 Q:1 INJ SODIUM BICARBONATE 1. What all strengths are available? 2. What are the clinical indications for IV sodium bicarbonate? 3. How do you administer this drug? 2 ANS: 1. Available
DRUGS FOR VIVA 1 Q:1 INJ SODIUM BICARBONATE 1. What all strengths are available? 2. What are the clinical indications for IV sodium bicarbonate? 3. How do you administer this drug? 2 ANS: 1. Available
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Paramedic Pediatric Medical Math Practice
 Paramedic Pediatric Medical Math Practice Name: Date: Problem 1 Your 4 year old patient weighs 40 pounds. She is febrile. You need to administer acetaminophen (Tylenol) 15mg/kg. How many mg will you administer?
Paramedic Pediatric Medical Math Practice Name: Date: Problem 1 Your 4 year old patient weighs 40 pounds. She is febrile. You need to administer acetaminophen (Tylenol) 15mg/kg. How many mg will you administer?
Fluid & Electrolyte Balances in Term & Preterm Infants. Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital
 Fluid & Electrolyte Balances in Term & Preterm Infants Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital Objectives Review maintenance fluid & electrolyte requirements in neonates Discuss
Fluid & Electrolyte Balances in Term & Preterm Infants Carolyn Abitbol, M.D. University of Miami/ Holtz Children s Hospital Objectives Review maintenance fluid & electrolyte requirements in neonates Discuss
Organ Donor Management Recommended Guidelines ADULT Brain Death (NDD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
UPDATED Pediatric Donor Management and Dosing Guidelines
 UPDATED Pediatric Donor Management and Dosing Guidelines Compiled by: Thomas A. Nakagawa, MD, FAAP, FCCM Wake Forest University Health Sciences Winston-Salem, North Carolina Department of Anesthesiology
UPDATED Pediatric Donor Management and Dosing Guidelines Compiled by: Thomas A. Nakagawa, MD, FAAP, FCCM Wake Forest University Health Sciences Winston-Salem, North Carolina Department of Anesthesiology
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
** Medication exercises ** NICU Phase II
 ** Medication exercises ** NICU Phase II A) Baby A has had a bowel resection six hours ago. She weighs 3 kg. Post-op, she is quite agitated and she is on a fentanyl drip at 2 micrograms/kg/hr (#1). She
** Medication exercises ** NICU Phase II A) Baby A has had a bowel resection six hours ago. She weighs 3 kg. Post-op, she is quite agitated and she is on a fentanyl drip at 2 micrograms/kg/hr (#1). She
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013
 NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
NUMBERS Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: PALS Revised: 11/2013 Weight in kg = 8 + (age in yrs X 2) Neonate (less than 1 month)
PEDIATRIC EMERGENCY CARE GUIDE Child 70mm. Child 70mm
 PEDIATRIC EMERGENCY CARE GUIDE Pediatric Parameters & Equipment Age Neonate 3mo 6mo 1 yr 2 yr 3 yr 4 yr 6 yr 8 yr 12 yr 14 yr Wt (kg) 3.5 6 8 10 12 14 16 20 25 40 50 ~ BSA (m 2 ) 0.24 0.34 0.42 0.49 0.56
PEDIATRIC EMERGENCY CARE GUIDE Pediatric Parameters & Equipment Age Neonate 3mo 6mo 1 yr 2 yr 3 yr 4 yr 6 yr 8 yr 12 yr 14 yr Wt (kg) 3.5 6 8 10 12 14 16 20 25 40 50 ~ BSA (m 2 ) 0.24 0.34 0.42 0.49 0.56
For The Management Of. Diabetic Ketoacidosis
 Guidelines For The Management Of Diabetic Ketoacidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council
Guidelines For The Management Of Diabetic Ketoacidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council
Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6
 Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
ADENOSINE. ADRENALINE (Epinephrine)
") ADENOSINE Notes Arrhythmias I.V. Initial dose 150 micrograms/kg stat Increase dose if required by 50 micrograms/kg to a maximum of 300 micrograms/kg (or 500 micrograms/kg if over 28 days old) ADMINISTRATION
ADENOSINE Notes Arrhythmias I.V. Initial dose 150 micrograms/kg stat Increase dose if required by 50 micrograms/kg to a maximum of 300 micrograms/kg (or 500 micrograms/kg if over 28 days old) ADMINISTRATION
Nassau Regional Emergency Medical Services. Advanced Life Support Pediatric Protocol Manual
 Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Nassau Regional Emergency Medical Services Advanced Life Support Pediatric Protocol Manual 2014 PEDIATRIC ADVANCED LIFE SUPPORT PROTOCOLS TABLE OF CONTENTS Approved Effective Newborn Resuscitation P 1
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
6 th Floor and 7 East Nurses Guide Intravenous Drip List Approved for RN Administration University of Kentucky Chandler Medical Center
 RATE Abciximab (Reopro) Alteplase (tpa, Activase) All units 6S and 6W ONLY Platelet aggregation inhibitor Thrombolytic agent Bolus: 0.25 mg/kg IV over 5 min Infusion: 0.125 0.9 mg/kg (max 90 mg); 10% of
RATE Abciximab (Reopro) Alteplase (tpa, Activase) All units 6S and 6W ONLY Platelet aggregation inhibitor Thrombolytic agent Bolus: 0.25 mg/kg IV over 5 min Infusion: 0.125 0.9 mg/kg (max 90 mg); 10% of
EMS Region Medication List 2010
 EMT-B MEDICATIONS Patient Assisted Medications (PAM) and Ambulance Stock Medications Medication Protocol/Use Dose Auto-injector (Epi-pen) Glucose (Oral) Metered-Dose Inhaler (MDI) Allergic/Anaphylactic
EMT-B MEDICATIONS Patient Assisted Medications (PAM) and Ambulance Stock Medications Medication Protocol/Use Dose Auto-injector (Epi-pen) Glucose (Oral) Metered-Dose Inhaler (MDI) Allergic/Anaphylactic
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Vitals/Hemodynamic Stability
 UNYTS Pediatric Donor Management Guidelines Obtain an accurate weight on the pediatric donor. Most everything you order will be based on the child s weight Vitals/Hemodynamic Stability Vital Signs - Acceptable
UNYTS Pediatric Donor Management Guidelines Obtain an accurate weight on the pediatric donor. Most everything you order will be based on the child s weight Vitals/Hemodynamic Stability Vital Signs - Acceptable
2
 1 2 3 4 5 6 7 8 Please check regional policy on Tetracaine and Morgan Lens this may be optional in your region. *Ketamine and Fentanyl must be added to your controlled substance license if required by
1 2 3 4 5 6 7 8 Please check regional policy on Tetracaine and Morgan Lens this may be optional in your region. *Ketamine and Fentanyl must be added to your controlled substance license if required by
Titrating Critical Care Medications
 Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
Titrating Critical Care Medications Chad Johnson, MSN (NED), RN, CNCC(C), CNS-cc Clinical Nurse Specialist: Critical Care and Neurosurgical Services E-mail: johnsoc@tbh.net Copyright 2017 1 Learning Objectives
3.Which is not a cause of hypokalemia? a) insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD
 insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD") Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Contra Costa County Emergency Medical Services Drug Reference. Indication Dosing Cautions Comments
 Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Drug Adenosine Albuterol Indication Dosing Cautions Comments Narrow complex tachycardia Bronchospasm Crush injury - hyperkalemia Initial 6mg rapid IV Repeat 12mg rapid IV Follow each dose with 20ml NS
Neonatal Guidelines. Chapter 15: Pharmacy related Version: Date Revised: 24 th January 2017
 Neonatal Guidelines Chapter 15: Pharmacy related Version: 2017.1 Specialty: Neonatal Medicine Revised by: Katherine Wilson Edited by: Sujoy Banerjee Date Revised: 24 th January 2017 Approved by: ABMU Joint
Neonatal Guidelines Chapter 15: Pharmacy related Version: 2017.1 Specialty: Neonatal Medicine Revised by: Katherine Wilson Edited by: Sujoy Banerjee Date Revised: 24 th January 2017 Approved by: ABMU Joint
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
AT TRIAGE. Alberta Acute Childhood Asthma Pathway: Evidence based* recommendations For Emergency / Urgent Care
 1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
2
 1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
1 2 3 4 5 6 7 8 Please check regional policy on this Tetracaine and Morgan lens may be optional in region *Ketamine and Fentanyl must be added to your CS license if required by your region *Midstate will
Post Resuscitation Care
 Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Seizures Emergency Treatment
 Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
Seizures Emergency Treatment Emergency Seizures SEIZURE CLASSIFICATION Cluster seizures - 2 or more generalized convulsive seizures in 24 hours Simon R. Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl.ECVN
PEDIATRIC LIFEGIFT BRAIN DEATH PLAN
 PHYSICIAN S Diagnosis Weight Allergies Admit/Discharge/Transfer THIS PLAN IS TO BE ED ONLY ON THE LIFEGIFT ENCOUNTER, WITH DR LIFEGIFT AS THE ATTENDING. Patient Status Pt Status: Inpatient (Inpatient only
PHYSICIAN S Diagnosis Weight Allergies Admit/Discharge/Transfer THIS PLAN IS TO BE ED ONLY ON THE LIFEGIFT ENCOUNTER, WITH DR LIFEGIFT AS THE ATTENDING. Patient Status Pt Status: Inpatient (Inpatient only
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
PICU Therapeutic Hypothermia Post Cardiac Arrest Re Warming Phase
 Arrest Re Warming Phase Weight Allergies Patient Care ***After 24 hours initiate re warming (or after 72 hours for an infant less than one month old)*** PICU Re Warming Protocol ***See Reference Text***
Arrest Re Warming Phase Weight Allergies Patient Care ***After 24 hours initiate re warming (or after 72 hours for an infant less than one month old)*** PICU Re Warming Protocol ***See Reference Text***
Fundamentals of Pharmacology for Veterinary Technicians Chapter 19
 Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Recurrent wheezing illnesses 24.9% Similar to Australia Above global averages
 Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
Prof Mike South Department of General Medicine Royal Children s Hospital Melbourne Australia www.mikesouth.org.au Asthma is very common in Australia Approx 25% children have recurrent wheezing illnesses
MICHIGAN. Table of Contents. State Protocols. Adult Treatment Protocols
 MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
WEIGHT: KG HEIGHT: CM ALLERGY CAUTION sheet reviewed Code Status Full code
 (Page 1 of 5) Code Status Full code Status/Admit/Transfer/Discharge Surgical Procedure(s) and date performed: Cardiologist: Cardiac Surgeon: Intensivist: Patient Care CMV status Recipient CMV status Donor
(Page 1 of 5) Code Status Full code Status/Admit/Transfer/Discharge Surgical Procedure(s) and date performed: Cardiologist: Cardiac Surgeon: Intensivist: Patient Care CMV status Recipient CMV status Donor
VENTRICULAR FIBRILLATION. 1. Safe scene, standard precautions. 2. Establish unresponsiveness, apnea, and pulselessness. 3. Quick look (monitor)
") LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
LUCAS COUNTY EMS SUMMARY PAGES VENTRICULAR FIBRILLATION 2. Establish unresponsiveness, apnea, and pulselessness 3. Quick look (monitor) 4. Identify rhythm 5. Provide 2 minutes CPR if unwitnessed by EMS
Sample. Affix patient label within this box.
 Instructions for completing orders: Determine PRAM Clinical Score as per the Alberta Acute Childhood Asthma Pathway for Emergent/Urgent Care and select orders based on PRAM Score. Custom orders can be
Instructions for completing orders: Determine PRAM Clinical Score as per the Alberta Acute Childhood Asthma Pathway for Emergent/Urgent Care and select orders based on PRAM Score. Custom orders can be
Physician Orders LEB PICU Status Epilepticus Plan. [ ] No known allergies
![Physician Orders LEB PICU Status Epilepticus Plan. [ ] No known allergies](/thumbs/80/82315048.jpg "Physician Orders LEB PICU Status Epilepticus Plan. [ ] No known allergies") Height: cm Weight: kg Allergies: [ ] No known allergies [ ] Initiate Powerplan Phase T;N, Phase: LEB PICU Admit Phase Admission/Transfer/Discharge [ ] Admit Patient to Dr. [ ] Admit Status: [ ] Inpatient
Height: cm Weight: kg Allergies: [ ] No known allergies [ ] Initiate Powerplan Phase T;N, Phase: LEB PICU Admit Phase Admission/Transfer/Discharge [ ] Admit Patient to Dr. [ ] Admit Status: [ ] Inpatient
TOO SWEET TOO STORMY. CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth. PRESENTOR: Dr. Abhinaya PG I (M.D Paeds)
") TOO SWEET TOO STORMY PRESENTOR: Dr. Abhinaya PG I (M.D Paeds) CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth Unit IV, Dept. Of Paediatrics, SRMC & RI 14year old female complaints of
TOO SWEET TOO STORMY PRESENTOR: Dr. Abhinaya PG I (M.D Paeds) CONSULTANTS: Dr. Saji James Dr. J. Dhivyalakshmi Dr. P. N. Vinoth Unit IV, Dept. Of Paediatrics, SRMC & RI 14year old female complaints of
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
PALS Pulseless Arrest Algorithm.
 PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
PALS Pulseless Arrest Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Bradycardia Algorithm. Kleinman M E et al. Circulation 2010;122:S876-S908 PALS Tachycardia Algorithm. Kleinman M
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL
 CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
CHANGES FOR DECEMBER 2008 PREHOSPITAL CARE MANUAL Item Changed Airway Management Procedure Oral Intubation Procedure Tube Confirmation and Monitoring Procedure C10 Chest Pain/ACS M2 Allergic Reaction/Anaphylaxis
The immediate management of burns patients should be similar to management of trauma.
 CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
CATS Clinical Guideline Burns The National Burn Care Review recommends that children with burns should be treated in a Burn Centre. Chelsea and Westminster may take non-ventilated children, Broomfield
MASTER SYLLABUS
 A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02
 effective 05/01/02") PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
PEDIATRIC TREATMENT GUIDELINES - CARDIAC VENTRICULAR FIBRILLATION - PULSELESS VENTRICULAR TACHYCARDIA (SJ-PO1) effective 05/01/02 Revision #5 04/19/02 Identify Dysrhythmia DEFIBRILLATE: 2 J/kg, 4 J/kg,
Septic Shock. Kathryn Sims, PGY I
 Septic Shock Kathryn Sims, PGY I A 6 y.o. previously healthy boy presents to the ED with 7 days of fever accompanied by chills. Further history reveals the patient has also been experiencing dysuria for
Septic Shock Kathryn Sims, PGY I A 6 y.o. previously healthy boy presents to the ED with 7 days of fever accompanied by chills. Further history reveals the patient has also been experiencing dysuria for
PEDIATRIC ACUTE ASTHMA SCORE (P.A.A.S.) GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze
 GUIDELINES. >97% 94% to 96% 91%-93% <90% Moderate to severe expiratory wheeze") Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
Inclusion: Children experiencing acute asthma exacerbation 24 months to 18 years of age with a diagnosis of asthma Patients with a previous history of asthma (Consider differential diagnosis for infants
MEDICAL KIT - ALGORITHMS
 MEDICAL KIT - ALGORITHMS Page 2 : BRONCHOSPASM / ASTHMA Page 3 : TENSION PNEUMOTHORAX Page 4 : Page 5 : Page 6 : CONGESTIVE HEART FAILURE/ PULMONARY EDEMA ANAPHYLACTIC SHOCK / ALLERGIC REACTION ANGINA
MEDICAL KIT - ALGORITHMS Page 2 : BRONCHOSPASM / ASTHMA Page 3 : TENSION PNEUMOTHORAX Page 4 : Page 5 : Page 6 : CONGESTIVE HEART FAILURE/ PULMONARY EDEMA ANAPHYLACTIC SHOCK / ALLERGIC REACTION ANGINA
Table 3: Management of Acute Reactions to Contrast Media in Adults Last updated: July 2017
 Table 3: Management of Acute Reactions to Contrast Media in Adults Last updated: July 2017 HIVES (Urticaria) Mild (scattered and/ transient) No treatment often needed; however, if symptomatic, can consider:
Table 3: Management of Acute Reactions to Contrast Media in Adults Last updated: July 2017 HIVES (Urticaria) Mild (scattered and/ transient) No treatment often needed; however, if symptomatic, can consider:
PICU CARD SURG Post Operative Cardiac Transplant Age LESS than 6 months (Page 1 of 5)
") (Page 1 of 5) Code Status Full code Status/Admit/Transfer/Discharge Surgical Procedure(s) and date performed (if applicable): Cardiologist: Cardiac Surgeon: Intensivist: Patient Care CMV status Donor CMV
(Page 1 of 5) Code Status Full code Status/Admit/Transfer/Discharge Surgical Procedure(s) and date performed (if applicable): Cardiologist: Cardiac Surgeon: Intensivist: Patient Care CMV status Donor CMV
Diagnosis: Allergies:
 Patient Name: Diagnosis: Allergies: ICU Sepsis Version 5 1/11/17 This order set must be used with an admission order set if patient not already admitted. Nursing Orders Verify that cultures have been obtained
Patient Name: Diagnosis: Allergies: ICU Sepsis Version 5 1/11/17 This order set must be used with an admission order set if patient not already admitted. Nursing Orders Verify that cultures have been obtained
With Dr. Sarah Reid and Dr. Sarah Curtis
 5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
UTMB-Galveston SURGICAL INTENSIVE CARE UNIT ORGAN PROCUREMENT PROTOCOL
 UTMB-Galveston SURGICAL INTENSIVE CARE UNIT ORGAN PROCUREMENT PROTOCOL For questions call: Eugene J. Lian, MD, Marc O. Maybauer, MD, PhD, EDIC, FCCP Department of Anesthesiology Division of Critical Care
UTMB-Galveston SURGICAL INTENSIVE CARE UNIT ORGAN PROCUREMENT PROTOCOL For questions call: Eugene J. Lian, MD, Marc O. Maybauer, MD, PhD, EDIC, FCCP Department of Anesthesiology Division of Critical Care
Pediatric Diabetic Ketoacidosis (DKA) General Pediatrics Admission Order Set
 General Pediatrics Admission Order Set") Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
Admitting MRP: Pediatrics: Dr. / Dr. on call to cover until 08:00 am Service: Medicine Team 1 Medicine Team 2 Medical subspecialty Diagnosis: Diabetic Ketoacidosis (DKA) Estimated length of stay Less than
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
Pediatric Code Blue FOCUS on Medications. Objectives
 Pediatric Code Blue FOCUS on Medications Objectives The learner will be able to: 1. List commonly used pediatric code drugs based on PALS 2015 guidelines 2. Discuss mechanism of action, clinical indications,
Pediatric Code Blue FOCUS on Medications Objectives The learner will be able to: 1. List commonly used pediatric code drugs based on PALS 2015 guidelines 2. Discuss mechanism of action, clinical indications,
COMPLICATED DKA SINDHU BHARATHI S STANLEY MEDICAL COLLEGE MD POST GRADUATE
 COMPLICATED DKA SINDHU BHARATHI S STANLEY MEDICAL COLLEGE MD POST GRADUATE Dr.Shanthi, Professor & Head, Dr. T.S. Ekambaranath Asst Professor, PICU, ISP, Stanley Medical College 9yrs male, previously normal
COMPLICATED DKA SINDHU BHARATHI S STANLEY MEDICAL COLLEGE MD POST GRADUATE Dr.Shanthi, Professor & Head, Dr. T.S. Ekambaranath Asst Professor, PICU, ISP, Stanley Medical College 9yrs male, previously normal
Paediatric Emergency Prompt Cards
 Paediatric Emergency Prompt Cards Introduced July 2016 Prompt cards are designed to be used by any member of the resus team If you have any comments or suggestions, please contact helen.collyer-merritt@sash.nhs.uk
Paediatric Emergency Prompt Cards Introduced July 2016 Prompt cards are designed to be used by any member of the resus team If you have any comments or suggestions, please contact helen.collyer-merritt@sash.nhs.uk
** Note: second generation antihistamines cause less drowsiness; may be beneficial in patients that need to drive themselves home.
 Table 5 : Management of Acute Reactions to Contrast Media in Adults HIVES Mild (scattered and/ transient) No treatment often needed; however, if symptomatic, can consider: Diphenhydramine (Benadryl )*
Table 5 : Management of Acute Reactions to Contrast Media in Adults HIVES Mild (scattered and/ transient) No treatment often needed; however, if symptomatic, can consider: Diphenhydramine (Benadryl )*
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Emergency Department Protocol Initiative
 Emergency Department Protocol Initiative ACUTE ASTHMA MANAGEMENT TOOLKIT March 2006 Provincial Emergency Services Project PHYSICIAN ORDER TEMPLATE FOR CTAS LEVEL 1 ASTHMA ADULT PEDIATRIC Date: Site: Arrival
Emergency Department Protocol Initiative ACUTE ASTHMA MANAGEMENT TOOLKIT March 2006 Provincial Emergency Services Project PHYSICIAN ORDER TEMPLATE FOR CTAS LEVEL 1 ASTHMA ADULT PEDIATRIC Date: Site: Arrival
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Available ONLY at: BMC-B BMC-D BMC-N BMC-S Nursing Orders Communication Order If CVP unavailable, administer fluid boluses every 30 minutes except monitor O2 requirements Comments: Every
DRUG AND TREATMENT Available ONLY at: BMC-B BMC-D BMC-N BMC-S Nursing Orders Communication Order If CVP unavailable, administer fluid boluses every 30 minutes except monitor O2 requirements Comments: Every
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Indian Diploma in Critical Care Nursing
 Indian Diploma in Critical Care Nursing MCQ Section A - Only one answer is correct 1. Four emergency interventions used in resuscitating a patient in cardiac arrest. a. Adrenaline/Atropine/ Amiodarone/Defibrillation
Indian Diploma in Critical Care Nursing MCQ Section A - Only one answer is correct 1. Four emergency interventions used in resuscitating a patient in cardiac arrest. a. Adrenaline/Atropine/ Amiodarone/Defibrillation
PICU BRONCHIOLITIS PLAN
 PICU BRONCHIOLITIS PLAN Diagnosis Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Pt Status: Inpatient (LOS > 2 midnights) Pt Status: Observation (LOS < 2 midnights) Patient Care Code
PICU BRONCHIOLITIS PLAN Diagnosis Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Pt Status: Inpatient (LOS > 2 midnights) Pt Status: Observation (LOS < 2 midnights) Patient Care Code
NICU Nutrition Pathway
 NICU Nutrition Pathway Safely Infusing NICU TPN Starter and Custom TPN April17 th 2018 Pharmacists: Paul Kasprzak RPH BCPS Kelly Kopec PharmD Major Practice Changes in the Preparation and Administration
NICU Nutrition Pathway Safely Infusing NICU TPN Starter and Custom TPN April17 th 2018 Pharmacists: Paul Kasprzak RPH BCPS Kelly Kopec PharmD Major Practice Changes in the Preparation and Administration
Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet
 1 Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet 1 Name of Guideline / Policy/ Procedure MANAGEMENT OF ACUTE PAEDIATRIC ASTHMA Purpose of Procedure/
1 Children & Young People s Directorate Paediatric-Neonatal Guidelines Checklist & Version Control Sheet 1 Name of Guideline / Policy/ Procedure MANAGEMENT OF ACUTE PAEDIATRIC ASTHMA Purpose of Procedure/
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
NonConvulsive Seizure
 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample. Affix patient label within this box.
 Instructions for completing orders Complete pages 1-3 for General Inpatient Orders. All pathway compatible orders (indicated by ) within the General Inpatient Orders will be followed automatically. Optional
Instructions for completing orders Complete pages 1-3 for General Inpatient Orders. All pathway compatible orders (indicated by ) within the General Inpatient Orders will be followed automatically. Optional
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
DONATION AFTER CARDIAC DEATH PLAN
 DONATION AFTER CARDIAC DEATH PLAN Diagnosis Weight Allergies Patient Care Core Body Temperature Monitoring Maintain body temp 96-99 degrees Farenheit. Utilize Hyper/Hypothermia blanket prn Insert Gastric
DONATION AFTER CARDIAC DEATH PLAN Diagnosis Weight Allergies Patient Care Core Body Temperature Monitoring Maintain body temp 96-99 degrees Farenheit. Utilize Hyper/Hypothermia blanket prn Insert Gastric
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
DIABETIC FOOT WITH SEPTIC SHOCK FOR AMPUTATION ANAESTHETIC MANAGEMENT
 DIABETIC FOOT WITH SEPTIC SHOCK FOR AMPUTATION ANAESTHETIC MANAGEMENT CASE HISTORY : - Dr.S.Saravanababu, Salem You are called to assess a 50 year male with gangrenous left lower limb being planned for
DIABETIC FOOT WITH SEPTIC SHOCK FOR AMPUTATION ANAESTHETIC MANAGEMENT CASE HISTORY : - Dr.S.Saravanababu, Salem You are called to assess a 50 year male with gangrenous left lower limb being planned for
Asthma Care in the Emergency Department Clinical Practice Guideline
 Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely