Drug Dosing During Renal Replacement Therapy. Myrna Y. Munar, Pharm.D., BCPS
|
|
|
- Wesley Hood
- 6 years ago
- Views:
Transcription
1 Drug Dosing During Renal Replacement Therapy Myrna Y. Munar, Pharm.D., BCPS
2 Outline Overview of the processes involved in solute (including drug) & fluid removal during renal replacement therapy: HD, CAPD, SCUF, CAVH, CVVH, CVVHDF Factors influencing drug removal during renal replacement therapy Use various medications (prototypes) to illustrate drug removal Review PK calculations to determine clearance Guidelines for determining dosing adjustments in renal patients undergoing hemodialysis or hemofiltration

3 Hemodialysis
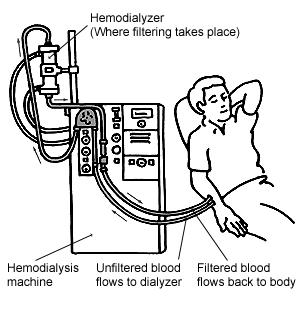
4 Procedure
5 Vascular Access
6 Countercurrent Flow
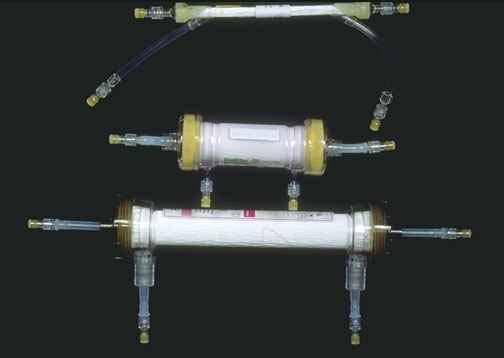
7 Dialyzers
8 Types of Dialyzers
9 Conventional Hemodialysis
10 Hemodialysis Blood Dialyzer Dialysate Dialysate Dialysate
11 Diffusion Blood Waste Waste Dialysate Dialyzer Dialysate
12 Ultrafiltration Pressure Waste Waste Dialysate Dialyzer Dialysate
13 Dialysate Components meq/l Acute HD Chronic HD Na K 3.5 varies 2.5 varies Ca Mg PO 4 None None Dextrose mg/dl HCO acetate 4
14 Factors Affecting Drug Removal during Hemodialysis Concentration gradient Molecular weight Related to speed and size Membrane thickness Pore size Degree of protein binding
15 Characteristics of Drugs Likely to be Removed by Hemodialysis Small molecular weight Low volume of distribution Non-protein bound or low protein binding Water soluble Renal excretion is the main mode of drug elimination
16 High Flux Dialysis Highly permeable membrane Thinner membrane Larger pores Greater removal of middle molecules (evil humours) Convection & diffusion are optimized
17 High Flux Hemodialysis
18 Example Vancomycin HD No replacement doses are needed High flux HD Significant vancomycin removal has been reported (range: 39-92%) Replacement doses may be needed Eg. Vancomycin 250 mg IV after high flux HD» Ref: AJKD 1995;26(3):469-74» Kidney Int 1994;45:232-7» AJKD 1992;20(4):354-60» AAC 1992;36(7):1424-6
19 Vancomycin Removal by Hi-Flux HD Am J Kidney Dis 1995;26(3): N = 8 critically ill patients Age years Purpose Define PK during high-flux HD Characterize rebound phenomenon
20 Methods Interdialytic Vanco MD HD HD Rebound Intradialytic Intradialytic Concentration 6-hr 20-hr Vanco IV x 1 p HD Time
21 PK Calculations Intradialytic t 1/2 Data to use: pre- and post- HD levels k intradialytic = ln (pre HD level/post HD level) delta t t 1/2 intradialytic = 0.693/k
22 PK Calculations Intradialytic clearance Data to use: Arterial samples - AUC 0-end of dialysis Dialysate samples - amount of drug in dialysate (R) R = dialysate concentration x volume of dialysate Cl intradialytic = R/AUC 0-end of dialysis
23 PK Calculations Interdialytic t 1/2 Data to use: 6-hr & 20-hr post-dose levels k interdialytic = ln (6-hr level/20-hr level) delta t t 1/2 interdialytic = 0.693/k
24 PK Calculations % rebound Data to use: C mr = maximum drug concentration during rebound phase C end = drug concentration at the end of HD % rebound = (C mr C end )/C end x 100
25 PK Parameter Results F-80 (n=5) F60 (n=3) Interdialytic t 1/2 (hrs) Intradialytic t 1/2 (hrs) Intradialytic CL (ml/min) Vancomycin Recovered (mg) % Rebound Range:15-38%
26 Guidelines Supplemental vancomycin doses should be given after high-flux HD (approx 250 mg) in addition to the patient s regular dose or baseline requirement. Reflects amount recovered in dialysate True trough levels should be obtained at least 6 hours following dialysis. The rebound effect occurred 2-6 hours following highflux HD
27 Vancomycin Dosing in HD Mohamed, O, Munar, MY, Earle SB, Wahba I. American Society of Nephrology Annual Mtg. October 30, 2004 Simplified, proposed method LD 15 mg/kg x 1 MD 10 mg/kg last 1 hr of each HD

28 Continuous Ambulatory Peritoneal Dialysis (CAPD)

29 Continuous Ambulatory Peritoneal Dialysis (CAPD) Uses the peritoneal membrane for exchange of fluid and solutes Parietal: underlies the abdominal wall Visceral: overlies the abdominal organs Both are highly vascularized
30 CAPD Access
31 Dialysate flows into the peritoneal cavity by gravity (15 min.) and allowed to dwell (approx. 4 hours) At the end of dwell time, the empty dialysate bag is placed in a dependent position Tube is unclamped & dialysate (effluent) flows into bag, detached, discarded New bag is attached & process is repeated CAPD Process
32 Pre-attached bags Double-bag Flush-before-fill Fresh dialysis solution flows into the Y-tubing and into the drainage bag Flushes out air, bacteria Y-Set System
33 Fresh solution flows into the rinsed tubing Y-Set System
34 CAPD Components Standard volumes 2, 2.5 liters (1.5, 2.0, 2.25, 2.5, or 3 L) Dextrose concentrations 1.5, 2.5, 4.25%
35 CAPD Components 3 Standard Formulations (meq/l) Na K Cl Mg Ca Lactate
36 Intraperitoneal Drug Therapy 3 main drug classes Antibiotics Insulin Heparin
37 Peritonitis Incidence varies Related to patient s technique and ability to perform an exchange Caused by a variety of microorganisms Gram-positive organisms, eg. Staph aureus & Staph epidermidis are most common Many treatment regimens exist. No single regimen has proven to be the most efficacious
38 Initial treatment of peritonitis Abdominal Pain +/- Cloudy Fluid +/- Unexplained Fever Cell Count/Differential Gram s Stain, Culture Initiate Empiric Antibiotic Therapy Cefazolin or Cephalothin & Ceftazidime ISPD 2005 Update Peritoneal Dialysis International 2005;24:107.
39 Empiric Therapy Drug Intermittent Dose in 1 Exchange/Day Cefazolin or cephalothin Ceftazidime Gentamicin or tobramycin Amikacin Residual Urine Output (<100 ml/d) 1 g/bag QD or 15 mg/kg/bag QD 1 g/bag QD 0.6 mg/kg/bag QD 2 mg/kg/bag QD Residual Urine Output (>100 ml/d) 20 mg/kg/bag QD 20 mg/kg/bag QD Not recommended Not recommended See ISPD guidelines for further therapy
40 Treatment of Exit Site Infection Ref: Peritoneal Dialysis International 1996;16: Purulent Discharge from Exit Site Gram Stain Culture Gram Positive Organism Gram Negative Organism Penicillinase Resistant PCN po eg. dicloxacillin or 1st generation cephalosporin ciprofloxacin 500 mg po bid (Adults only) 1 week If no improvement, add rifampin 600 mg/d po If Pseudomonas and no improvement, add ceftazidime
41 Exit Site Infections Purulent Discharge from Exit Site Gram s Stain, Culture Gram Positive Organism Penicillinase Resistant PCN po or 1 st generation cephalosporin po 1 week, no improvement add 1 week of rifampin 600 mg/d po
42 Exit Site Infections Purulent Discharge from Exit Site Gram s Stain, Culture Gram Negative Organism Ciprofloxacin mg po BID or ofloxacin 400 mg po 1 st day, then 200 mg po QD; Stagger doses to avoid chelation reactions
43 Intraperitoneal Drug Therapy Heparin CAPD patients can secrete fibrinogen into the peritoneal cavity resulting in fibrin formation Can lead to: Intraperitoneal adhesions Outflow obstruction Heparin u/l is added to the dialysis solution Not absorbed thru peritoneum Minimal systemic anticoagulation effects
44 Intraperitoneal Drug Therapy Regular insulin is used for IP administration Insulin IP is 2-3 x insulin SQ Incomplete absorption of insulin IP (F = 25-30%) Adsorption of insulin to the PVC bag and administration set Advantages: Convenient Avoids SQ injection site complications
45 AVOID Certain oral hypoglycemics Glyburide (DiaBeta, Micronase, Glynase) Tolazamide (Tolinase) Acetohexamide (Dymelor) Chlorpropamide (Diabinese) Why? Excreted to a large extent in urine Half-life may be greatly prolonged Use may result in severe & prolonged hypoglycemia
46 Slow Continuous Renal Replacement Therapy (CRRT)
47 From Arteriovenous to Venovenous Arteriovenous A systolic BP of mm Hg is necessary to produce ultrafiltrate Efficiency of hemofiltration depends on arterial pressure low or unstable in ICU patients Low blood flow - frequent clotting Leak in the circuit - rapid blood loss Venovenous Made possible by development of double lumen catheters and blood pumps
48 Vascular Access Example of PermCath Percutaneously inserted into the right internal jugular vein right IJ
49 Vascular Access Example of double lumen catheter Inserted into left femoral vein
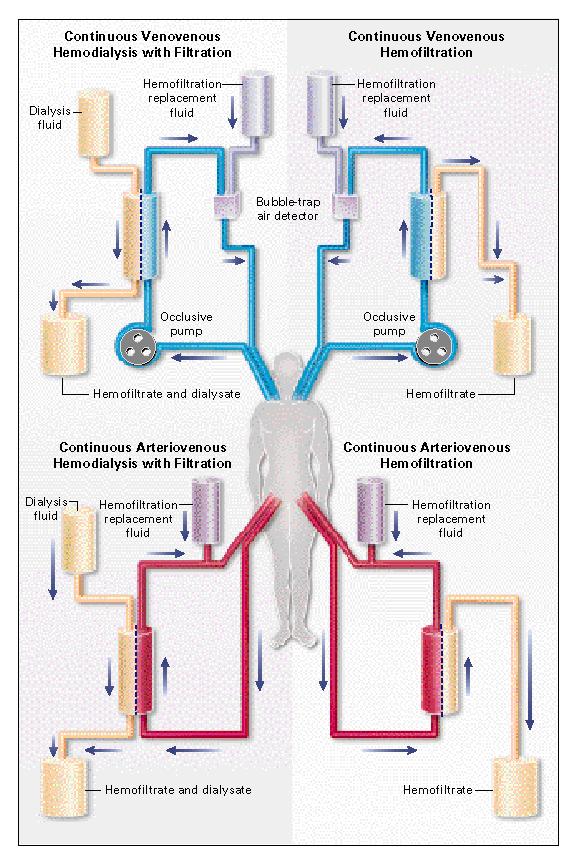
50 Slow Continuous Ultrafiltration (SCUF) Arteriovenous or venovenous Highly permeable filter Ultrafiltrate not replaced Used only for fluid control/removal Artery Vein Ultrafiltrate

51 Hemofilter

52 Prisma
53 Continuous Hemofiltration (CVVH or CAVH) Features Arteriovenous or venovenous Highly permeable filter Ultrafiltration > weight/volume loss & replacement fluid is needed Solute CL is by convection Replacement Fluid Artery Vein Ultrafiltrate
54 Continuous Hemodiafiltration (CVVHDF or CAVHDF) Features Arteriovenous or venovenous Highly permeable filter Includes dialysate Ultrafiltration > weight/volume loss & replacement fluid is needed Solute CL is by convection & diffusion Replacement Fluid Artery Vein Dialysate inlet Ultrafiltrate & Dialysate Outlet
55 CVVHDF
56
57 HD vs CVVHD HD Low permeable filter Efficiency is limited to small molecules MW daltons No replacement fluid CVVHDF Highly permeable filter Efficiency is extended to larger molecules MW daltons Replacement fluid Sterile dialysate Dialysate inlet Outlet Replacement Fluid Dialysate inlet Outlet
58 CVVH or CVVHDF Orders Replacement Fluid +/-Dialysate inlet Blood flow rate 150 ml/min Range ml/min Vein Ultrafiltrate +/- dialysate outlet
59 CVVH or CVVHDF Orders Bicarbonate solution 500 ml bottle of NaHCO 3 (300 meq/500 ml) Starting rate: 50 ml/hr Titrate to maintain serum HCO 3 between meq/l and ph Replacement Fluid +/-Dialysate inlet Ultrafiltrate +/- dialysate outlet
60 CVVH or CVVHDF Orders Replacement fluid 3 L bags NaCl 110 meq/l (careful D5W). Add: KCl 2-4 meq/l MgSO 4 2 meq/l CaCl 2 2 meq/l per ica for heparin anticoag only Rate ml/hr Eg. Adjust to maintain a NET LOSS of ml/hr (0-100 ml/hr) If the patient s BP declines eg. MAP < 60, set at zero balance Replacement Fluid +/- Dialysate inlet Ultrafiltrate +/- dialysate outlet
61 Fluid Removal Rate Fluid removal rate (HCO 3 )+(Replacement fluid & IV s)+(net loss) Example Initial HCO 3 rate = 100 ml/hr Replacement fluid rate = 1000 ml/hr All IV s = 300 ml/hr Net loss = 100 ml/hr net negative balance 100 ml/hr Fluid removal rate= ml/hr =1500 ml/hr = output Input = ml/hr = 1400 ml/hr
62 CVVH or CVVHDF Orders Heparin Minimum infusion rate: 500 U/hr for PTT Or if ACT < 170 increase rate 5%. If ACT > 200 decrease rate 5%. Heparin +/-Dialysate inlet Ultrafiltrate +/- dialysate outlet
63 CVVHDF Orders Dialysate 5 L bags with: KCl Rate: ml/hr Dialysate inlet Ultrafiltrate & dialysate outlet
64 CVVH & CVVHDF Labs Before procedure: Tx panel, ionized Ca, PO 4, Mg, PT, PTT, post filter ACT, CBC Na, K, HCO 3, Ca, PO 4, Mg, PT, PTT/ACT, q 4 h until stable, then q 8-12 h or after any event Adjustments: Mg: meq/l w/ 1-2 g MgSO 4 over min. Ionized Ca: meq/l w/ 1 amp CaCl 2 (1g) over 60 min. PO 4 : meq/l with NaPO 4 at 5 mm per hr (15 or 20 mm) K: with central KCl
65 Drug Removal by CVVH/DF Estimation Sieving Coefficient (SC) Quantitative index of a drug s ability to traverse the hemofilter membrane Ratio of the drug concentration in the ultrafiltrate (C uf ) to the drug concentration in the arterial line Similar to the fraction unbound to plasma proteins (f up ) for many drugs
66 Phenytoin Ther Drug Monit 1994;16:53 N=2 ICU patients 36 yo, phenytoin 100 mg IV q 8 h 17 yo, phenytoin 300 mg IV qd On CAVH Polysulfone hollow fiber filter Replacement fluid = LR or TPN UFR ml/hr Evidence Replacement Fluid Ultrafiltrate
67 Results Pt. [Phenytoin] mg/l [Free Phenytoin] mg/l % Free Total Protein g/l Serum Albumi n g/l Arterial Ultrafiltrate
68 Drug Removal by CVVH/DF Estimation Clearance by convection CL convection CL convection = Q f x SC, where Q f = ultrafiltration rate OR CL convection = Q f x f up If CVVHDF: CL diffusion = Q dialysis x f up, where Q dialysis = dialysate flow rate CL CVVHDF = CL convection + CL diffusion
69 Drug Removal by CVVH/DF Estimation CL total = CL CVVHDF + CL residual CL residual is from published literature Recall, Dose/tau = (C pss )(CL)/S F
70 Published Guidelines Can serve as a point of reference when drug concentration monitoring is not available For continuous renal replacement therapy (CRRT), clearances achieved simulate GFR in the range of ml/min Therefore, when specific drug information is unavailable, drug doses may be initiated as if the patient had a GFR of ml/min
71 Example Ultrafiltration rate (UFR) URF 2000 ml/hr x 60 min/hr = 33 ml/min UFR 1800 ml/hr x 60 min/hr = 30 ml/min
72 Imipenem-Cilastatin Removal During CVVH N=12 ICU patients CVVH: Polyacrylonitrile hemofilter (AN69 HF) Blood flow rate: ml/min Replacement fluids: 1000 ml/hr UFR: ml/hr Balance: ml/hr Imipenem-cilastatin 500 mg IV q 6-8 h Ref: AAC 1997;41(12) Replacement Fluid Ultrafiltrate
73 Imipenem-Cilastatin Removal During CVVH CL CVVH = CL convection = Q f x SC CL CVVH = 1100 ml/hr x 1.2 = 1320 ml/hr or 22 ml/min Reported CL CVVH = ml/min Determined CL total = Dose/AUC 0- inf = ml/min = 7.3 L/hr AUC 0- inf determined from serial samples thru arterial line
74 Clearance Recall, CL total = CL Renal + CL nonrenal CL total = CL CVVHDF + CL nonrenal CL nonrenal can be calculated CL total -CL CVVHDF CL nonrenal = = ml/min = ml/min Represents metabolism or nonspecific plasma hydrolysis
75 Imipenem Dose During CVVH Recall, Dose/tau = (C ssaver )(CL)/S F Dose/tau = (12 mg/l)(7.3 L/hr) = 87.6 mg/hr Target imipenem C ssaver was chosen to ensure that the plasma concentration remained above the MIC 90 for intermediately resistant Pseudomonas aeruginosa for the majority of the dosing interval Daily dose = 87.6 mg/hr x 24 hrs = 2100 mg Typically dosed q 6 h, therefore recommended dose during CVVH = 500 mg IV q 6h. Corresponds to the recommended dose for GFR ml/min
76 PK and PD of Imipenem-Cilastatin Removal During CRRT N=12 ICU patients n=6 CVVH; n=6cvvhdf CRRT: Polyacrylonitrile hemofilter (AN69 HF) Blood flow rate: ml/min Replacement fluids: 1000 ml/hr UFR: 19 ml/min CVVHD dialysate rate 973 ml/hr Imipenem-cilastatin 1 2 g per day IV Ref: AAC 2005;49(6) CVVHDF: Dialysate Replacement Fluid Ultrafiltrate + Spent Dialysate
77 Similar PK results as in previous study
78 Imipenem PD Time above the MIC (T > MIC) should be at least 40 50% of the dosing interval for maximum killing effects Imipenem usually displays MICs < 2 mcg/ml against most Gm (-) aerobic pathogens T > MIC = % T > MIC Cmax, free ln MIC + k T > MIC = tau x100
79 Median % (Range) T > MIC MIC Imipenem 0.5 g IV Q 8 h CVVH n = 2 CVVHDF n = 3 MIC < 1 mcg/ml MIC = 2 mcg/ml MIC = 4 mcg/ml MIC = 8 mcg/ml (100) (78-92) (53-58) (24-28) 74 (68-100) 56 (51-93) 38 (34-54) 16 (15-19) Time above the MIC (T > MIC) should be at least 40 50% of the dosing interval
80 Median % (Range) T > MIC MIC Imipenem 0.5 g IV Q 12 h CVVH n = 3 CVVHDF n = 4 MIC < 1 mcg/ml MIC = 2 mcg/ml MIC = 4 mcg/ml MIC = 8 mcg/ml 62 (46-100) 46 (35-92) 35 (31-53) 14 (14-22) 64 (56-100) 47 (40-99) 29 (26-53) 11 (6-12) Time above the MIC (T > MIC) should be at least 40 50% of the dosing interval
81 Conclusions Imipenem should be dosed at 1.0 to 1.5 g/day due to susceptible pathogens with a MIC < 2 mcg/ml Imipenem 2.0 g/day appears to be required for pathogens such as Pseudomonas aeruginosa with potentially higher MICs (4-8 mcg/ml) or for empiric therapy of serious nosocomial infections in patients undergoing CRRT
82 CVVH vs CVVHDF What is the effect of different modalities on drug clearance? What is the effect of increasing dialysate flow rate on drug clearance during CVVHDF?
83 Fluconazole Removal During CVVH/DF N = 6 ARF patients Polysulfone filter Replacement Fluid (Fresenius AV400) Pump flow = 100 ml/min Day 1: CVVH Day 2: CVVHDF Dialysate flow rate: 1L/hr Day 3: CVVHDF Dialysate flow rate: 2 L/hr Fluconazole 200 mg IV qd J Antimicrob Chemother 1997;40: /-Dialysate inlet Ultrafiltrate +/- dialysate outlet
84 Fluconazole Removal During CVVH/DF Patient CL CVVH ml/min CL CVVHDF ml/min CL CVVHDF ml/min Dialysate 1L/hr Dialysate 2L/hr Mean+SD
85 Fluconazole Removal During CVVH/DF CL CVVHDF significantly different (p < 0.05) from CL CVVH Observe greater CL as dialysate flow rate is increased Characteristics: MW 306 daltons Small V D = 0.7 L/kg Low plasma protein binding
86 Cefpirome PK During CVVH N=8 anuric ICU patients CVVH: High-flux polysulfone capillary hemofilter (Diafilter 30, Amicon) Blood flow rate: 150ml/min UFR: ml/min Zero balance Bicarb-based replacement fluid Cefpirome 2 g IV q 8 h Ref: Clin Pharmacol Ther 2000;67(4): Replacement Fluid Ultrafiltrate
87 Cefpirome Semisynthetic 4 th generation cephalosporin Extended spectrum against gram (-) & (+) pathogens including strains resistant to 3 rd generation cephalosporins MW 512 daltons Small V D Protein binding < 10% Renal elimination
88 Is cefpirome likely to be removed during CRRT? Yes.
89 Cefpirome Pharmacodynamics Killing is time-dependent [Drug] needs to exceed the MIC for at least 25-40% of dosing interval [Drug] 4x 8x MIC are required MIC 90 of cefpirome against Enterobacteriaceae mcg/ml MIC 90 of cefpirome against GPC 1 2 mcg/ml MIC 90 of cefpirome against P aeruginosa 8 mcg/ml
90 Cefpirome MIC 90 < 8 mcg/ml MIC 90 <4 mcg/ml Plasma [cefpirome] remained above 4 mcg/ml 62% of the dosing interval Plasma [cefpirome] remained above 8 mcg/ml 25% of the dosing interval Cefpirome [trough] mg/ml
91 Dosing Recommendation Cefpirome 2 g IV q 8 h for gram (-) & (+) pathogens MIC mcg/ml vs usual adult dose in patients with normal renal function: cefpirome 1-2 g IV q 12 h Higher doses are required to cover severe infections caused by P aeruginosa. Can cefpirome 2 g IV q 12 achieve the same targets for gram (-) & (+) pathogens MIC mcg/ml?
92 Double Check t1/2 (h) k (h -1 ) V D (L) CL (L/hr) ml/min =35.35 L/hr Mean data reported
93 Target Recall, killing is time-dependent [Drug] need to exceed the MIC for at least 25-40% of dosing interval [Drug] 4x 8x MIC are requiredmic 90 of mcg/ml for gram (-) & (+) pathogens
94 Short IV Infusions C max1 -t C C C C max1 min1 max, ss min, ss = = C dose / t V k D max1 e max, ss kt dose / t kt ( 1 e ) OR ( 1 e ) k ( τ t) dose / t = CL = C e kt ( 1 e ) k ( τ t) CL 1 1 e kτ small t = t = infusion time tau = dosing interval C min1
95 Short IV Infusions C C C C max1 min1 max, ss min, ss dose / t = CL = C e = = max1 C max, ss ( kt 1 e ) k ( τ t) dose / t CL e ( kt 1 e ) k ( τ t) R ac 1 1 e kτ Recall, dose/t = rate of drug infusion 1 e -kt = fraction of SS achieved by time t OR fraction of drug lost during time t e -k( -t) = fraction of drug remaining at end of dosing interval = time tau minus t R ac = accumulation factor
96 PK Calculations C max ( )( kt dose / t 1 e ) ( V )( k)( kτ 1 e ) D ( hr )( 0. 5hr) ( 2000mg / 05. hr)( 1 e ) Cmax = 1 1 ( hr )( 12h) ( L)( hr )( 1 e ) C = 13mg/ L max = V D & k determined from mean C max 14.8 & C min 3.1 for cefpirome 2g IV q8h 1
97 What is C min? C = C e min max ( k)( τ t) C = 13mg/ Le min C = 12. mg/ L min 1 ( hr )( hr)
98 Cefpirome Log C vs time LOG [cefpirome] (mg/l Time (hrs)
99 Cefpirome C vs time 16 [cefpirome] (mg/l Time (hrs) Cefpirome 2 g IV q 8: C max 14.8 mg/l; C min 3.1 mg/l Cefpirome 2 g IV q 12h: C max 13 mg/l; C min 1.2 mg/l
100 Are there differences in drug clearance between filters?
101 Ceftriaxone MW 556 daltons V D = 0.16 L/kg (range L/kg) 40% excreted unchanged Protein binding f up concentration dependent ceftriaxone C p 115 mg/l -> f up ceftriaxone C p 65 mg/l -> f up Ref: Pharmacotherapy 2000;20(6):
102 Ceftriaxone CL by CVVH & CVVHD N=8 chronic HD patients 12-hr CVVH, CVVHD via 3 filters: AN 69, Hospal Multiflow 60, CGH Medical PMMA, Filtryzer B1-2.1U, Toray Industries PS (Polysulfone) hemofilter, Fresenius F40 Ceftriaxone 1 g IV over 1h Ref: Pharmacotherapy 2000;20(6): /-Dialysate inlet Ultrafiltrate
103 Effect of Blood Flow Rate on CL Constant: dialysate flow rate 33.3 ml/min UFR 0 ml/min Increasing blood flow rate at hourly intervals 75 ml/min 125 ml/min 150 ml/min 250 ml/min Dialysate inlet Spent dialysate
104 Effect of Blood Flow Rate on CL Clearances were essentially constant at all blood flow rates for all 3 filters.
105 Effect of Dialysate Flow Rate on CL Constant: blood flow rate 100 ml/min UFR 0 ml/min Increasing dialysate flow rate at hourly intervals 8.3 ml/min 16.7 ml/min 25.0 ml/min 33.3 ml/min Dialysate inlet Spent dialysate
106 Ceftriaxone Clearance in Relation to Dialysate Flow Rate PMMA PS AN69 PMMA PS AN69 Open: Total ceftriaxone Solid: Unbound ceftriaxone
107 Slopes of Unbound Ceftriaxone and Dialysate Flow Rate PMMA Slope 1.00, r 2 = PS Slope 1.04, r 2 = AN 69 Slope 0.48, r 2 = Analysis of slopes for total ceftriaxone were similar. Data not reported
108 Sieving Coefficients (SC) Constant: Blood flow rate 100 ml/min Dialysate flow rate 0 ml/min Sieving coefficient (SC) SC = C UF /C plasma for total & unbound ceftriaxone C Plasma IN Ultrafiltrate C UF OUT
109 Sieving Coefficients (SC) Filter PS (PS, Amicon) AN 69 f up * * SC of unbound ceftriaxone ** PMMA SC of total ceftriaxone was less than *p < 0.01; **p < 0.05 SC of unbound ceftriaxone for all filters (data not reported).
110 Sieving Coefficients (SC) Observed SC of unbound ceftriaxone was 2-3 fold higher than f up? Passage through the extracorporeal circuit may alter the fraction of drug available for transport across the filter membrane. Suggests ceftriaxone may be weakly bound to plasma proteins
111 Recall CL CVVH = CL convection CL convection = Q f x SC, where Q f = ultrafiltration rate OR CL convection = Q f x f up If CVVHDF: CL CVVHDF = CL convection + Cl diffusion CL diffusion = Q dialysis x f up, where Q dialysis = dialysate flow rate
112 For Ceftriaxone SC = f up Concentration dependent protein binding Large degree of interpatient variability in protein binding Therefore, cannot use a mean value of f up as a predictor of CVVH/DF CL
113 Constant: CVVHD &CVVH CL Blood flow rate 100 ml/min Dialysate flow rate 0 ml/min UFR = 500 ml/hr (low); 1000ml/hr (high) CVVHD & CVVH CL CL=[UFRx C UF ]/C pmidpoint UFR = ultrafiltration rate C UF = concentration in ultrafiltrate C pmidpoint = concentration in the plasma at the midpoint of the collection period (6-hours) urea,total & unbound ceftriaxone Ultrafiltrate
114 Convective Clearance of Unbound Ceftriaxone p = p = p = 0.18 Lo (500 L/hr) and Hi (1000 L/hr) UFR No significant increase with AN69 filter
115 Comparison of Membranes Clearance of unbound ceftriaxone with all 3 filters increased when UFR was doubled from low 500 ml/hr to high 1000 ml/h SC and convective CL of unbound ceftriaxone were significantly lower with the AN69 than the PS & PMMA filters at low and high UFR (p=0.0001). Speculate may be due to adsorption onto filter or a repulsive interaction between the membrane surface and drug that limit membrane transport
116 Urea Clearance AN69 CL=0.57[Cl urea ] r 2 = p= PS CL=1.02[Cl urea ] r 2 = p= PMMA CL=0.90[Cl urea ] r 2 = p= Recall, y = mx + b or ceftriaxone CL = m[cl urea ] + b, where b=0
117 Empiric Ceftriaxone Dosing Recommendations/Increments ARF no CRRT (CrCl < 10 ml/min): CVVH: CVVHD: ceftriaxone mg IV q 12 h ceftriaxone 30 mg IV q 12 h for each 0.5 L/hr UFR Dialysate ceftriaxone IV PMMA & PS AN69 1 L/hr 2 L/hr 1-2 L/h 80 mg IV q 12 h 115 mg IV q 12 h 50 mg IV q 12 h
118 Ceftriaxone Dose Individualization Recall, Cl total = Cl renal + Cl nonrenal Eg. PMMA Cl renal = CL=0.90[Cl urea ] + residual renal function eg residual renal function GFR 20 ml/min Cl nonrenal approximately 30 ml/min in patients with ARF longer than 7-10 days Cl nonrenal = 93 ml/min in patients with normal renal function Cl nonrenal reduced by up to 67% in patients w/arf of longer than 7-10 days; Cl nonrenal ARF approx 32 ml/min
119 C PK Calculations max = Solvefordose: ( )( kt dose / t 1 e ) ( CL)( kτ 1 e ) Dose / t = ( )( )( ) C CL 1 e kτ max ( ) 1 e kt C min = e ( k )( τ t)


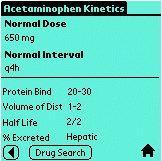
120 Drug Prescribing in Renal Failure Palm OS c/renal_failure.htm
Continuous Renal Replacement Therapy. Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
- SLED Sustained Low-Efficiency Dialysis
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
MODALITIES of Renal Replacement Therapy in AKI
 MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
The Physiology of Peritoneal Dialysis As Related To Drug Removal
 The Physiology of Peritoneal Dialysis As Related To Drug Removal Thomas A. Golper, MD, FACP, FASN Vanderbilt University Medical Center Nashville, TN thomas.golper@vanderbilt.edu Clearance By Dialysis Clearance
The Physiology of Peritoneal Dialysis As Related To Drug Removal Thomas A. Golper, MD, FACP, FASN Vanderbilt University Medical Center Nashville, TN thomas.golper@vanderbilt.edu Clearance By Dialysis Clearance
Practical issues - dosing on extracorporeal circuits
 Practical issues - dosing on extracorporeal circuits Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
Practical issues - dosing on extracorporeal circuits Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
UNDERSTANDING THE CRRT MACHINE
 UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
UAB CRRT Primer Ashita Tolwani, MD, MSc University of Alabama at Birmingham
 UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
Physiology of Blood Purification: Dialysis & Apheresis. Outline. Solute Removal Mechanisms in RRT
 Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Drug Use in Dialysis
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
(Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
ST. DOMINIC-JACKSON MEMORIAL HOSPITAL JACKSON, MISSISSIPPI. CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT) HEPARIN ANTICOAGULATION Page 1 of 5
 HEPARIN ANTICOAGULATION Page 1 of 5") HEPARIN ANTICOAGULATION Page 1 of 5 Pharmacy Mnemonic: CRRTHEP1 PATIENT DATA: DIAGNOSIS: AKI ESRD Other: WEIGHT: Today: kg Admission Weight:: kg Dry Weight: kg Access TYPE: Temporary Dialysis Catheter
HEPARIN ANTICOAGULATION Page 1 of 5 Pharmacy Mnemonic: CRRTHEP1 PATIENT DATA: DIAGNOSIS: AKI ESRD Other: WEIGHT: Today: kg Admission Weight:: kg Dry Weight: kg Access TYPE: Temporary Dialysis Catheter
ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO
 ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland NO CONFLICT OF INTERESTS Important concept
ANTIBIOTIC DOSE AND DOSE INTERVALS IN RRT and ECMO Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland NO CONFLICT OF INTERESTS Important concept
CRRT and Drug dosing. Karlee Johnston Lead Pharmacist Division of Critical Care ICU Education June 2017
 CRRT and Drug dosing Karlee Johnston Lead Pharmacist Division of Critical Care ICU Education June 2017 This talk In scope CRRT modalities with regard to medicine Principles of drugs with regard to dialysis
CRRT and Drug dosing Karlee Johnston Lead Pharmacist Division of Critical Care ICU Education June 2017 This talk In scope CRRT modalities with regard to medicine Principles of drugs with regard to dialysis
Renal Replacement Therapy in ICU. Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine
 Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Pharmacokinetics pharmacodynamics issues relevant for the clinical use of betalactam antibiotics in critically ill patients
 Veiga and Paiva Critical Care (2018) 22:233 https://doi.org/10.1186/s13054-018-2155-1 REVIEW Pharmacokinetics pharmacodynamics issues relevant for the clinical use of betalactam antibiotics in critically
Veiga and Paiva Critical Care (2018) 22:233 https://doi.org/10.1186/s13054-018-2155-1 REVIEW Pharmacokinetics pharmacodynamics issues relevant for the clinical use of betalactam antibiotics in critically
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2
 Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
Is the package insert correct? PK considerations
 Is the package insert correct? PK considerations Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
Is the package insert correct? PK considerations Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
Medication Dosing in CRRT
 Medication Dosing in CRRT Linda Awdishu, PharmD, MAS Associate Clinical Professor of Pharmacy and Medicine Learning Objectives 1. List the pharmacokinetic changes associated with AKI. 2. Determine the
Medication Dosing in CRRT Linda Awdishu, PharmD, MAS Associate Clinical Professor of Pharmacy and Medicine Learning Objectives 1. List the pharmacokinetic changes associated with AKI. 2. Determine the
Active UMMC Protocols
 UMMC CRRT 2018 Active UMMC Protocols 1. Standard CRRT Protocol PrismaFlex & NxStage CVVH with Fixed Ratio Regional Citrate Anticoagulation 2. No Anticoagulation Protocol PrismaFlex & NxStage CVVH with
UMMC CRRT 2018 Active UMMC Protocols 1. Standard CRRT Protocol PrismaFlex & NxStage CVVH with Fixed Ratio Regional Citrate Anticoagulation 2. No Anticoagulation Protocol PrismaFlex & NxStage CVVH with
CRRT: The Technical Questions Modality & Dose. Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018
 CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
SHC Vancomycin Dosing Guide
 SHC Vancomycin Dosing Guide A: Initial dosing considerations B. Pharmacodynamic Targets: goal AUC and troughs C. Loading dose D: Initial Vancomycin Maintenance Dosing and Serum Concentration Monitoring
SHC Vancomycin Dosing Guide A: Initial dosing considerations B. Pharmacodynamic Targets: goal AUC and troughs C. Loading dose D: Initial Vancomycin Maintenance Dosing and Serum Concentration Monitoring
Session 1: Circuit, Anticoagulation and Monitoring. Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019
 Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Session 1: Circuit, Anticoagulation and Monitoring Ashita Tolwani, MD, MSc Noel Oabel, BSN, RN, CNN 2019 Goals n Learn how to set up citrate anticoagulation for CVVH, CVVHD, CVVHDF using Prismaflex n Determine
Pediatric Continuous Renal Replacement Therapy
 Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
Pediatric Continuous Renal Replacement Therapy Farahnak Assadi Fatemeh Ghane Sharbaf Pediatric Continuous Renal Replacement Therapy Principles and Practice Farahnak Assadi, M.D. Professor Emeritus Department
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Drug dosing in patients with acute kidney injury
 Drug dosing in patients with acute kidney injury They don t know what they are doing Jan Jan T. T. Kielstein Department of of Nephrology and and Hypertension Medical School School Hannover Drug dosing
Drug dosing in patients with acute kidney injury They don t know what they are doing Jan Jan T. T. Kielstein Department of of Nephrology and and Hypertension Medical School School Hannover Drug dosing
Drug Management in CRRT
 Drug Management in CRRT Jeffrey Lipman, FCICM, MD Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland Bruce A. Mueller, PharmD, FCCP, FASN Clinical, Social & Administrative
Drug Management in CRRT Jeffrey Lipman, FCICM, MD Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland Bruce A. Mueller, PharmD, FCCP, FASN Clinical, Social & Administrative
Recent advances in CRRT
 Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
Recent advances in CRRT JAE IL SHIN, M.D., Ph.D. Department of Pediatrics, Severance Children s Hospital, Yonsei University College of Medicine, Seoul, Korea Pediatric AKI epidemiology and demographics
higher dose with progress in technical equipment. Continuous Dialysis: Dose and Antikoagulation. prescribed and delivered
 1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
1 2 Continuous Dialysis: Dose and Antikoagulation higher dose with progress in technical equipment Comparison of pump-driven and spontaneous continuous haemofiltration in postoperative acute renal failure.
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Prolonged Dialysis: 24-hr SLED Is It CRRT? Balazs Szamosfalvi, MD
 Prolonged Dialysis: 24-hr SLED Is It CRRT? Balazs Szamosfalvi, MD Medical Director, In-patient Dialysis and CRRT Henry Ford Hospital, Detroit, Michigan, USA Presenter Disclosure Information I will discuss
Prolonged Dialysis: 24-hr SLED Is It CRRT? Balazs Szamosfalvi, MD Medical Director, In-patient Dialysis and CRRT Henry Ford Hospital, Detroit, Michigan, USA Presenter Disclosure Information I will discuss
Renal Replacement Therapies in Kidney Disease
 ORIGINAL ARTICLE Sanjiv Mahajan* Chief Medical Officer, Department of Nephrology & Medicine, Safdarjung Hospital & Vardhman Mahavir Medical College, New Delhi, India ABSTRACT Renal replacement therapy
ORIGINAL ARTICLE Sanjiv Mahajan* Chief Medical Officer, Department of Nephrology & Medicine, Safdarjung Hospital & Vardhman Mahavir Medical College, New Delhi, India ABSTRACT Renal replacement therapy
CRRT for the Experience User 1. Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018
 CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
CRRT for the Experience User 1 Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference March, 2018 Disclosures I have no actual or potential conflict of interest
CRRT Procedures. and Guidelines. CRRT: Guidelines
 CRRT Procedures 2013 and Guidelines Guidelines for the utilization of CRRT (Continuous Renal Replacement Therapies) at Monroe Carell Jr. Children s Hospital at Vanderbilt CRRT: Guidelines CRRT Contacts:
CRRT Procedures 2013 and Guidelines Guidelines for the utilization of CRRT (Continuous Renal Replacement Therapies) at Monroe Carell Jr. Children s Hospital at Vanderbilt CRRT: Guidelines CRRT Contacts:
Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy
 Cedarville University DigitalCommons@Cedarville Pharmacy Faculty Presentations School of Pharmacy 2-23-2012 Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy Jeb Ballentine
Cedarville University DigitalCommons@Cedarville Pharmacy Faculty Presentations School of Pharmacy 2-23-2012 Nurse-Pharmacist Collaboration in the Delivery of Continuous Renal Replacement Therapy Jeb Ballentine
Modes of Extracorporeal Therapies For ESRD Patients
 Modes of Extracorporeal Therapies For ESRD Patients Suhail, MD Extracorporeal Therapies: Dialytic Therapies Dialysis: Movement of molecules across a semipermeable membrane (Bi-directional) Movement of
Modes of Extracorporeal Therapies For ESRD Patients Suhail, MD Extracorporeal Therapies: Dialytic Therapies Dialysis: Movement of molecules across a semipermeable membrane (Bi-directional) Movement of
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
PHA Spring First Exam. 8 Aminoglycosides (5 points)
") PHA 5128 Spring 2012 First Exam 1 Aminoglycosides (5 points) 2 Aminoglycosides (10 points) 3 Basic Principles (5 points) 4 Basic Principles (5 points) 5 Bioavailability (5 points) 6 Vancomycin (5 points)
PHA 5128 Spring 2012 First Exam 1 Aminoglycosides (5 points) 2 Aminoglycosides (10 points) 3 Basic Principles (5 points) 4 Basic Principles (5 points) 5 Bioavailability (5 points) 6 Vancomycin (5 points)
End Stage Renal Disease and Renal Replacement Therapies
 End Stage Renal Disease and Renal Replacement Therapies Alexander J. Ansara,, Pharm. D. St. Louis College of Pharmacy and St. Luke s Hospital Therapeutics 1 Fall 2003 Required Reading Materials Dipiro
End Stage Renal Disease and Renal Replacement Therapies Alexander J. Ansara,, Pharm. D. St. Louis College of Pharmacy and St. Luke s Hospital Therapeutics 1 Fall 2003 Required Reading Materials Dipiro
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Acute Kidney Injury- What Is It and How Do I Treat It?
 Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
Acute Kidney Injury- What Is It and How Do I Treat It? Jayant Kumar, MD Renal Medicine Assoc., Albuquerque, NM Incidence of ARF in ICU Causes of ARF Non -ICU ICU 1 KDIGO criteria for AKI Increase in serum
7/17/2017 FSHP 2017 ANNUAL MEETING. Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy
 FSHP Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy Disclosure I do not have (nor does any immediate family member have) a vested interest in or affiliation
FSHP Medication Considerations for the Adult/Pediatric ICU Patient Receiving Renal Replacement Therapy Disclosure I do not have (nor does any immediate family member have) a vested interest in or affiliation
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Peritoneal Dialysis Prescriptions: A Primer for Nurses
 Peritoneal Dialysis Prescriptions: A Primer for Nurses A Primer ABCs of PD R x Betty Kelman RN-EC MEd CNeph (C) Toronto General Hospital University Health Network Toronto, Ontario, Canada A moment to remember
Peritoneal Dialysis Prescriptions: A Primer for Nurses A Primer ABCs of PD R x Betty Kelman RN-EC MEd CNeph (C) Toronto General Hospital University Health Network Toronto, Ontario, Canada A moment to remember
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Vancomycin: Class: Antibiotic.
 Vancomycin: Class: Antibiotic. Indications: Treatment of patients with infections caused by staphylococcal species and streptococcal Species. Available dosage form in the hospital: 1G VIAL, 500MG VIAL.
Vancomycin: Class: Antibiotic. Indications: Treatment of patients with infections caused by staphylococcal species and streptococcal Species. Available dosage form in the hospital: 1G VIAL, 500MG VIAL.
RENAL FAILURE IN ICU. Jo-Ann Vosloo Department Critical Care SBAH
 RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
ICU Volume 11 - Issue 3 - Autumn Series
 ICU Volume 11 - Issue 3 - Autumn 2011 - Series Impact of Pharmacokinetics of Antibiotics in ICU Clinical Practice Introduction The efficacy of a drug is mainly dependent on its ability to achieve an effective
ICU Volume 11 - Issue 3 - Autumn 2011 - Series Impact of Pharmacokinetics of Antibiotics in ICU Clinical Practice Introduction The efficacy of a drug is mainly dependent on its ability to achieve an effective
Citrate Anticoagulation
 Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Strategies for Optimizing the CRRT Circuit Citrate Anticoagulation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum Berlin, Germany
Metabolismo del citrato nei pazienti critici. Filippo MARIANO Dipartimento di Area Medica, SCDO di Nefrologia e Dialisi Ospedale CTO, Torino
 Metabolismo del citrato nei pazienti critici Filippo MARIANO Dipartimento di Area Medica, SCDO di Nefrologia e Dialisi Ospedale CTO, Torino Regional citrate anticoagulation: the history First in hemodialysis
Metabolismo del citrato nei pazienti critici Filippo MARIANO Dipartimento di Area Medica, SCDO di Nefrologia e Dialisi Ospedale CTO, Torino Regional citrate anticoagulation: the history First in hemodialysis
Continuous Renal Replacement Therapy (CRRT)
") ISPUB.COM The Internet Journal of Anesthesiology Volume 21 Number 1 Continuous Renal Replacement Therapy (CRRT) S Sarkar Citation S Sarkar. Continuous Renal Replacement Therapy (CRRT). The Internet Journal
ISPUB.COM The Internet Journal of Anesthesiology Volume 21 Number 1 Continuous Renal Replacement Therapy (CRRT) S Sarkar Citation S Sarkar. Continuous Renal Replacement Therapy (CRRT). The Internet Journal
Solute clearances during continuous venovenous haemofiltration at various ultrafiltration flow rates using Multiflow-100 and HF1000 filters
 Nephrol Dial Transplant (2003) 18: 961 966 DOI: 10.1093/ndt/gfg055 Original Article Solute clearances during continuous venovenous haemofiltration at various ultrafiltration flow rates using Multiflow-100
Nephrol Dial Transplant (2003) 18: 961 966 DOI: 10.1093/ndt/gfg055 Original Article Solute clearances during continuous venovenous haemofiltration at various ultrafiltration flow rates using Multiflow-100
The general Concepts of Pharmacokinetics
 The general Concepts of Pharmacokinetics What is this jargon? Is it useful? C max, clearance, Vd, half-life, AUC, bioavailability, protein binding F. Van Bambeke, E. Ampe, P.M. Tulkens (Université catholique
The general Concepts of Pharmacokinetics What is this jargon? Is it useful? C max, clearance, Vd, half-life, AUC, bioavailability, protein binding F. Van Bambeke, E. Ampe, P.M. Tulkens (Université catholique
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Use of Antibacterial Agents in Renal Failure
 Use of Antibacterial Agents in Renal Failure Brett Gilbert, DO a, *, Paul Robbins, DO b, Lawrence L. Livornese Jr, MD, FIDSA c KEYWORDS Antibiotics Renal failure Volume of distribution MDRD Dosing antibiotics
Use of Antibacterial Agents in Renal Failure Brett Gilbert, DO a, *, Paul Robbins, DO b, Lawrence L. Livornese Jr, MD, FIDSA c KEYWORDS Antibiotics Renal failure Volume of distribution MDRD Dosing antibiotics
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital
 Renal Dialysis Centre Hong Kong Sanatorium & Hospital") Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
Karen Mak R.N. (Team Leader) Renal Dialysis Centre Hong Kong Sanatorium & Hospital - Renal Transplantation - Peritoneal Dialysis - Extracorporeal Therapy Extracorporeal Therapy It is the procedure in
Drug Dosing in Renal Insufficiency. Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila
 Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
CONTINUOUS RENAL REPLACEMENT THERAPY
 Acta clin Croat 2000; 39:99-116 Review CONTINUOUS RENAL REPLACEMENT THERAPY Petar Kes Department of Nephrology and Dialysis, Sestre milosrdnice University Hospital, Zagreb, Croatia SUMMARY - Acute renal
Acta clin Croat 2000; 39:99-116 Review CONTINUOUS RENAL REPLACEMENT THERAPY Petar Kes Department of Nephrology and Dialysis, Sestre milosrdnice University Hospital, Zagreb, Croatia SUMMARY - Acute renal
CRRT in Pediatrics: Indications, Techniques & Outcome. Overview
 CRRT in Pediatrics: Indications, Techniques & Outcome Timothy E. Bunchman Pediatric Nephrology & Transplantation Grand Rapids, MI Overview (Please interrupt me at any time) Access Solutions Anticoagulation
CRRT in Pediatrics: Indications, Techniques & Outcome Timothy E. Bunchman Pediatric Nephrology & Transplantation Grand Rapids, MI Overview (Please interrupt me at any time) Access Solutions Anticoagulation
Vancomycin Pharmacokinetics. Myrna Y. Munar, Pharm.D., BCPS Associate Professor of Pharmacy
 Vancomycin Pharmacokinetics Myrna Y. Munar, Pharm.D., BCPS Associate Professor of Pharmacy Goals Review the PK properties of vancomycin Compare and contrast methods of dosage regimen design for vancomycin
Vancomycin Pharmacokinetics Myrna Y. Munar, Pharm.D., BCPS Associate Professor of Pharmacy Goals Review the PK properties of vancomycin Compare and contrast methods of dosage regimen design for vancomycin
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Technical aspects of RRT in AKI: access, anticoagulation, drug dosage and nutrition. Marlies Ostermann
 Technical aspects of RRT in AKI: access, anticoagulation, drug dosage and nutrition Marlies Ostermann AKI guideline Chapter 3: Nutrition Chapter 5.3: Anticoagulation Chapter 5.4: Vascular access for RRT
Technical aspects of RRT in AKI: access, anticoagulation, drug dosage and nutrition Marlies Ostermann AKI guideline Chapter 3: Nutrition Chapter 5.3: Anticoagulation Chapter 5.4: Vascular access for RRT
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 1.0 (July 2016) PICANet Renal Custom Audit Data s Manual Version 1.0 July 2016 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
egfr 34 ml/min egfr 130 ml/min Am J Kidney Dis 2002;39(suppl 1):S17-S31
:S17-S31") Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
PHA Final Exam Fall 2006
 PHA 5127 Final Exam Fall 2006 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
PHA 5127 Final Exam Fall 2006 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
PHA Final Exam. Fall On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5127 Final Exam Fall 2010 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
PHA 5127 Final Exam Fall 2010 On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name Please transfer the answers onto the bubble sheet. The question number refers
Who? Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011
 Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Dialysis for Acute Renal Failure: Who, What, How, and When? Kathleen D. Liu, MD, PhD, MAS June 2011 Dorre Nicholau MD PhD Clinical Professor Department of Anesthesia and Perioperative Care University of
Dialysis Dose Prescription and Delivery. William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012
 Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Dialysis Dose Prescription and Delivery William Clark, M.D. Claudio Ronco, M.D. Rolando Claure-Del Granado, M.D. CRRT Conference February 15, 2012 Dose in RRT: Key concepts Dose definition Quantifying
Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background
 Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background Index: 1. Introduction Pg. 1 1.1 Definitions Pg. 2 1.2 Renal replacement therapy principles Pg. 2 2. Continuous
Continuous Renal Replacement Therapy in PICU: explanation/definitions/rationale/background Index: 1. Introduction Pg. 1 1.1 Definitions Pg. 2 1.2 Renal replacement therapy principles Pg. 2 2. Continuous
Continuous renal replacement therapy. David Connor
 Continuous renal replacement therapy David Connor Overview Classification of AKI Indications Principles Types of CRRT Controversies RIFL criteria Stage GFR Criteria Urine Output Criteria Risk Baseline
Continuous renal replacement therapy David Connor Overview Classification of AKI Indications Principles Types of CRRT Controversies RIFL criteria Stage GFR Criteria Urine Output Criteria Risk Baseline
Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of
 Update on CRRT: Pearls for the Clinician Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of Medicine tbunchman@mcvh-vcu.edu
Update on CRRT: Pearls for the Clinician Timothy E. Bunchman Professor and Director Pediatric Nephrology & Transplantation Children s Hospital of Richmond Virginia Commonwealth U School of Medicine tbunchman@mcvh-vcu.edu
Can We Achieve Precision Solute Control with CRRT?
 Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
Can We Achieve Precision Solute Control with CRRT? Claudio Ronco, M.D. David Selewski, M.D. Rolando Claure-Del Granado, M.D. AKI & CRRT Conference February, 2019 Disclosures I have no actual or potential
PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS
 PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS SITI HIR HURAIZAH MD TAHIR Bpharm (UKM), MSc (Clinical Microbiology) (UoN) CLINICAL PHARMACIST HOSPITAL MELAKA WHY STUDY PHARMACOKINETICS (PK) AND PHARMACODYNAMICS
PHARMACOKINETIC & PHARMACODYNAMIC OF ANTIBIOTICS SITI HIR HURAIZAH MD TAHIR Bpharm (UKM), MSc (Clinical Microbiology) (UoN) CLINICAL PHARMACIST HOSPITAL MELAKA WHY STUDY PHARMACOKINETICS (PK) AND PHARMACODYNAMICS
Management of the patient with established AKI. Kelly Wright Lead Nurse for AKI King s College Hospital
 Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
Continuous Renal Replacement Therapy Based Dose Adjustments - Adult - Inpatient Clinical Practice Guideline
 Continuous Renal Replacement Therapy Based Dose Adjustments - Adult - Inpatient Clinical Practice Guideline Note: Active Table of Contents Click to follow link Table of Contents EXECUTIVE SUMMARY... 3
Continuous Renal Replacement Therapy Based Dose Adjustments - Adult - Inpatient Clinical Practice Guideline Note: Active Table of Contents Click to follow link Table of Contents EXECUTIVE SUMMARY... 3
Imad Ahmed MD. Renal Associates of West Michigan
 Imad Ahmed MD Renal Associates of West Michigan ESRD Facts: - Medicare funded program - Cost - Significant mortality and morbidity - Reduced quality of life - Shrinking donor pool ESRD CAUSES - DM - Hypertension
Imad Ahmed MD Renal Associates of West Michigan ESRD Facts: - Medicare funded program - Cost - Significant mortality and morbidity - Reduced quality of life - Shrinking donor pool ESRD CAUSES - DM - Hypertension
CONTINUOUS RENAL REPLACEMENT THERAPY (CRRT)
") TABLE OF CONTENTS The purpose of this practice support document is to outline the procedures and guidelines related to care of the patient having continuous renal replacement therapy (CRRT) in the pediatric
TABLE OF CONTENTS The purpose of this practice support document is to outline the procedures and guidelines related to care of the patient having continuous renal replacement therapy (CRRT) in the pediatric
Continuous Infusion of Antibiotics In The ICU: What Is Proven? Professor of Medicine Vice-Chairman, Department of Medicine SUNY at Stony Brook
 Continuous Infusion of Antibiotics In The ICU: What Is Proven? Michael S. Niederman, M.D. Chairman, Department of Medicine Winthrop-University Hospital Mineola, NY Professor of Medicine Vice-Chairman,
Continuous Infusion of Antibiotics In The ICU: What Is Proven? Michael S. Niederman, M.D. Chairman, Department of Medicine Winthrop-University Hospital Mineola, NY Professor of Medicine Vice-Chairman,
Renal Physiology Intro to CRRT Concepts. Catherine Jones September 2017
 Renal Physiology Intro to CRRT Concepts Catherine Jones September 2017 Learning Outcomes To revise anatomy & physiology of kidney in health: To understand basic principles of continuous renal replacement
Renal Physiology Intro to CRRT Concepts Catherine Jones September 2017 Learning Outcomes To revise anatomy & physiology of kidney in health: To understand basic principles of continuous renal replacement
Development of C sporins. Beta-lactam antibiotics - Cephalosporins. Second generation C sporins. Targets - PBP s
 Beta-lactam antibiotics - Cephalosporins Development of C sporins Targets - PBP s Activity - Cidal - growing organisms (like the penicillins) Principles of action - Affinity for PBP s Permeability properties
Beta-lactam antibiotics - Cephalosporins Development of C sporins Targets - PBP s Activity - Cidal - growing organisms (like the penicillins) Principles of action - Affinity for PBP s Permeability properties
RENAL REPLACEMENT THERAPY IN ACUTE KIDNEY FAILURE - AN OVERVIEW
 RENAL REPLACEMENT THERAPY IN ACUTE KIDNEY FAILURE - AN OVERVIEW Treesa P. Varghese, Department of pharmacy practice St. James College of Pharmaceutical Sciences, Thrissure treesapv510@gmail.com Abstract
RENAL REPLACEMENT THERAPY IN ACUTE KIDNEY FAILURE - AN OVERVIEW Treesa P. Varghese, Department of pharmacy practice St. James College of Pharmaceutical Sciences, Thrissure treesapv510@gmail.com Abstract
PICANet Custom Audit Definitions Renal Dataset
 PICANet Custom Audit s Renal Dataset Version 2.0 (March 2017) PICANet Renal Custom Audit Data s Manual Version 2.0 29/03/2017 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
PICANet Custom Audit s Renal Dataset Version 2.0 (March 2017) PICANet Renal Custom Audit Data s Manual Version 2.0 29/03/2017 Renal Dataset Contents PICANet Custom Audit s... 1 Renal Dataset... 1 Version
ASN Board Review: Acute Renal Replacement Therapies
 ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
ASN Board Review: Acute Renal Replacement Therapies Ashita Tolwani, M.D., M.Sc. University of Alabama at Birmingham 2014 Key issues for boards: RRT for AKI When should therapy be initiated? What are the
New method of blood purification (Recycle Filtration System)
") Tokai J Exp Clin Med., Vol. 33, No. 3, pp. 124-129, 2008 New method of blood purification (Recycle Filtration System) Hajime SUZUKI 1), Miho HIDA 1), Makoto KITAMURA 1), Shin-ichi TANAKA 2), Takayo MIYAKOGAWA
Tokai J Exp Clin Med., Vol. 33, No. 3, pp. 124-129, 2008 New method of blood purification (Recycle Filtration System) Hajime SUZUKI 1), Miho HIDA 1), Makoto KITAMURA 1), Shin-ichi TANAKA 2), Takayo MIYAKOGAWA
Technical Considerations for Renal Replacement Therapy in Children
 Technical Considerations for Renal Replacement Therapy in Children Timothy E. Bunchman, MD,* Patrick D. Brophy, MD, and Stuart L. Goldstein, MD Summary: Provision of renal replacement therapy to the critically
Technical Considerations for Renal Replacement Therapy in Children Timothy E. Bunchman, MD,* Patrick D. Brophy, MD, and Stuart L. Goldstein, MD Summary: Provision of renal replacement therapy to the critically
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
Dialysis in the Acute Setting
 Dialysis in the Acute Setting medicine2.missouri.edu/jahm/dialysis-in-the-acute-setting/ October 8, 2015 Kunal Malhotra, MD Division of Nephrology, Department of Medicine, University of Missouri School
Dialysis in the Acute Setting medicine2.missouri.edu/jahm/dialysis-in-the-acute-setting/ October 8, 2015 Kunal Malhotra, MD Division of Nephrology, Department of Medicine, University of Missouri School
PERITONEAL EQUILIBRATION TEST. AR. Merrikhi. MD. Isfahan University of Medical Sciences
 PERITONEAL EQUILIBRATION TEST AR. Merrikhi. MD. Isfahan University of Medical Sciences INTRODUCTION The peritoneal equilibration test (PET) is a semiquantitative assessment of peritoneal membrane transport
PERITONEAL EQUILIBRATION TEST AR. Merrikhi. MD. Isfahan University of Medical Sciences INTRODUCTION The peritoneal equilibration test (PET) is a semiquantitative assessment of peritoneal membrane transport
NIH Public Access Author Manuscript Am J Nephrol. Author manuscript; available in PMC 2015 January 22.
 NIH Public Access Author Manuscript Published in final edited form as: Am J Nephrol. 2012 ; 36(2): 144 150. doi:10.1159/000339937. Gentamicin Pharmacokinetics and Pharmacodynamics during Short-daily Hemodialysis
NIH Public Access Author Manuscript Published in final edited form as: Am J Nephrol. 2012 ; 36(2): 144 150. doi:10.1159/000339937. Gentamicin Pharmacokinetics and Pharmacodynamics during Short-daily Hemodialysis
Department of Clinical Pharmacy, University of Michigan College of Pharmacy, Pharmacy Faculty, Siam University, Bangkok, Thailand
 1 2 Article Type: Guest Ed Mistakes We Make in Dialysis 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 We underdose antibiotics in patients on CRRT Alexander R. Shaw Weerachai Chaijamorn Bruce A. Mueller 1 Ann
1 2 Article Type: Guest Ed Mistakes We Make in Dialysis 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 We underdose antibiotics in patients on CRRT Alexander R. Shaw Weerachai Chaijamorn Bruce A. Mueller 1 Ann
UW MEDICINE PATIENT EDUCATION. Peritoneal Dialysis. A treatment option for kidney disease. There are 2 types of PD: continuous ambulatory
 UW MEDICINE PATIENT EDUCATION Peritoneal Dialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and basic principles of continuous ambulatory peritoneal dialysis (CAPD). 2.
UW MEDICINE PATIENT EDUCATION Peritoneal Dialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and basic principles of continuous ambulatory peritoneal dialysis (CAPD). 2.
Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience
 Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience Casey N. Gashti, MD, Susana Salcedo, MD, Virginia Robinson, RN, and Roger A. Rodby, MD Background: Renal replacement therapies
Accelerated Venovenous Hemofiltration: Early Technical and Clinical Experience Casey N. Gashti, MD, Susana Salcedo, MD, Virginia Robinson, RN, and Roger A. Rodby, MD Background: Renal replacement therapies
PHA 5128 Final Exam Spring 2004 Version A. On my honor, I have neither given nor received unauthorized aid in doing this assignment.
 PHA 5128 Final Exam Spring 2004 Version A On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name There are 18 questions. Total /120 pts Final 2004 1 1. T.P., a 66-year-old,
PHA 5128 Final Exam Spring 2004 Version A On my honor, I have neither given nor received unauthorized aid in doing this assignment. Name There are 18 questions. Total /120 pts Final 2004 1 1. T.P., a 66-year-old,
Renal replacement therapy in Pediatric Acute Kidney Injury
 Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Renal replacement therapy in Pediatric Acute Kidney Injury ASCIM 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Important topic: AKI
Essential in Renal Replacement Therapy Pediatrics CRRT
 Essential in Renal Replacement Therapy Pediatrics CRRT Konggrapun Srisuwan MD. Dialysis and Transplantation Program, Department of Pediatrics, Phramongkutklao Hospital Correction of fluid overload in patients
Essential in Renal Replacement Therapy Pediatrics CRRT Konggrapun Srisuwan MD. Dialysis and Transplantation Program, Department of Pediatrics, Phramongkutklao Hospital Correction of fluid overload in patients