End Stage Renal Disease and Renal Replacement Therapies
|
|
|
- Robert Cox
- 6 years ago
- Views:
Transcription
1 End Stage Renal Disease and Renal Replacement Therapies Alexander J. Ansara,, Pharm. D. St. Louis College of Pharmacy and St. Luke s Hospital Therapeutics 1 Fall 2003 Required Reading Materials Dipiro Chapter 47, pp Ifudu O. Care of Patients Undergoing Hemodialysis.. N Engl J Med 1998; 339: Supplemental Pastan S, Bailey J. Dialysis Therapy. N Engl J Med 1998; 338:
2 Epidemiology Overall incidence ESRD: 240/million pts 180/million caucasian patients 758/million african american patients US population with ESRD: > 200,000 pts on any dialysis 20,000 pts on peritoneal dialysis > 70,000 pts with functioning transplants Prevalence Increasing at 7-9% 7 per year Estimated 600,000 dialysis patients by 2010 # transplants remainining stable Increasing Prevalence
3 Mortality and Life Expectancy Importance of Prevention Prevention Cardiac deaths #1 cause Peritonitis #2 cause Limited availability of transplants Cost Cost Avg cost/pt/yr $45,000 US expenditure/yr: $15 billion Estimated cost by 2010: $28 billion
4 Treating ESRD Prevention Treat concurrent diseases HTN Diabetes Dialysis Hemodialysis (HD) Peritoneal Dialysis (PD) Renal transplantation Renal Replacement Therapy: Replacing Kidney Functions H 2 0 balance Electrolyte balance Acid/Base balance Waste Removal (urea, creatinine) Filter, reabsorb, secrete substances Plasma proteins, H 2 0, blood cells, amino acids, glucose, urea, mineral salts Endocrine functions Vitamin D activation Erythropoietin production
5 The Vowels of Renal Replacement Therapy INDICATION SETTING Acid Base Abnormality Electrolyte Disturbance Intoxication Fluid Overload Uremia Metabolic acidosis Hyperkalemia/ magnesemia Salicylates,, Li++, Meth- anol,, Ethylene Glycol Post-op op fluid gain, excessive IV fluids BUN accumulation Principles of Hemodialysis Hemodialysis: The removal of nitrogenous wastes, uremic toxins, and water from the blood via diffusion and convection Diffusion: The process of solute transfer from high concentration to low concentration until equillibrium Convection ( ultrafiltration ultrafiltration ): Primary means of removal of excess body H 2 0, maximized by: hydrostatic pressure permeability of membrane
6 Factors Affecting Diffusion Rate Concentration gradient Blood flow rate Dialysis flow rate Dialysis filter composition Solute characteristics Principles of Hemodialysis Hemodialysis: The removal of nitrogenous wastes, uremic toxins, and water from the blood via diffusion and convection Diffusion: The process of solute transfer from high concentration to low concentration until equillibrium Convection ( ultrafiltration ultrafiltration ): Primary means of removal of excess body H 2 0, maximized by: hydrostatic pressure permeability of membrane
7 Convection Low volume filtration: No significant clearance of toxins or drugs Performed to maintain fluid balance Ultrafiltration rate (UFR) < ml/hr Large volume filtration: Significant clearance of urea and drugs Must replace fluid loss to avoid major electrolyte disturbances UFR L/hr Vascular Access Permanent access to bloodstream necessary Native arteriovenous (AV) fistula Synthetic AV vascular grafts
8 Native AV Fistula Fistula between cephalic vein and radial artery 2 months to mature before use Low rate of complications Longest survival (of access) Used less frequently Native AV Fistula
9 Native AV Fistula Fistula between cephalic vein and radial artery 2 months to mature before use Low rate of complications Longest survival (of access) Used less frequently Synthetic AV Vascular Grafts Synthetic graft between brachial artery and basilic vein Made of polytetrafluoroethylene (PTFE), requires weeks to endothelialize Higher rates of infection and thrombosis Shorter device survival Most commonly used
10 Synthetic AV Vascular Grafts Synthetic AV Vascular Grafts Synthetic graft between brachial artery and basilic vein Made of polytetrafluoroethylene (PTFE), requires weeks to endothelialize Higher rates of infection and thrombosis Shorter device survival Most commonly used Fistula
11 Choosing a Route of Access Immediacy of need for dialysis Acute dialysis, may use central line; used for months as bridge for permanent access Adequacy of vascular access Complications Infection Thrombosis Stenosis 20-40% of hospitalizations Hemodialysis Blood pumped to dialyzer Blood and electrolyte solution (dialysate( dialysate): Seperated by semi-permeable membrane Pumped in countercurrent directions Solutes exchanged until equilibruim Protein bound drugs not removed Low permeability membrane (low to medium flux) HD
12 Goals of Dialysis Achieve desired dry weight Adequate removal of waste products Prevent sequelae of electrolyte disturbances Reduce morbidity and mortality
13 The Hemodialysis Rx Dialyzer manufacturer and size Amount of weight/fluid to remove Duration Frequency Blood flow rate: mL/min Dialysate Composition Flow rate: 500 ml/min Hemodialysate Composition Component (mmol/l) Sodium Potassium Calcium Magnesium Chloride Bicarbonate Glucose (g/dl dl) Hemodialysate Range Typical
14 The Hemodialysis Rx Dialyzer manufacturer and size Amount of weight/fluid to remove Duration Frequency Blood flow rate: mL/min Dialysate Composition Flow rate: 500 ml/min Hemodialysis Flow Rates Conventional Rapid-high efficiency High flux dialysis Blood flow rate (ml/min) Dialysate flow rate (ml( ml/min) Urea clearance rate (ml( ml/min) < 200 > 220 > 220 Required Time 4-55 hrs < 3 hrs < 3 hrs
15 Dosing Dialysis Individualized per patient Survival improves with higher doses Expressed as: Urea-reduction reduction ratio (URR) or Kt/V urea Urea Reduction Ratio Not 100% accurate Does not account for convective removal of urea Urea demonstrates two-compartment behavior (redistributes after dialysis) URR = (pre-dialysis BUN) (post-dialysis BUN) pre-dialysis BUN
16 Kt/V urea Unitless parameter Measures fraction of total body water cleared of urea during a dialysis session Kt/V urea = (urea clearance)(time) urea distribution volume K= dialyzer clearance of urea (L/h) t = duration of dialysis (h) V= urea volume of distribution (calculated) Goal Kt/V urea Values HD (non-diabetic) = 1.2 HD (diabetic) = High-flux dialysis (HFD) = 1.5 CAPD = 1.7/week NIPD and APD = 2.2/week Acute renal failure = much higher
17 Complications of Hemodialysis Fewer with high-flux dialysis Less hypotension with bicarbonate in dialysate Itching Hypotension Cramps Nausea/vomiting Headache Disequillibrium syndrome Dialyzer reactions Anaphylactic (Type A) Nonspecific (Type B) Complications of Hemodialysis Complication Itching Hypotension Cramps Nausea/ Vomiting Headache Incidence (%) Etiology/Risk Factors Uremic toxins, dry skin, Ca/PO 4 product, allergy Excessive UF, low target wt, vasodilation 2/2 acetate, meds or food, bleeding Hypotension, dehydration, low Na + in dialysate,, idiopathic Hypotension, disequilibrium syndrome Idiopathic, vasodilation 2/2 acetate, caffeine withdrawal
18 Anaphylactic Dialyzer Reactions Type A Response to ethylene oxide or heparin Worse with pts on ACEIs Nonspecific Type B More common, less severe Chest pain, back pain within minutes of dialysis Lowest incidence with synthetic high-flux membrances Disequilibrium Syndrome Definition: A central nervous system disorder characterized by neurologic symptoms caused by cerebral edema Sx: Nausea, vomiting, headache, seizures, obtundation,, coma; EEG changes Risk Factors: new dialysis patients, age (old or young), pre-existing existing neurological disorders, metabolic acidosis Treatment: prevention, use of UF, reducing URR, maintaining Na + and glucose levels in dialysate
19 Management of Hypotension Acute - Trendelenburg position - ultrafiltration rate ml saline bolus - mannitol 12.5 grams IV ml 23.4% saline over min Non-pharm Prevention - Set accurate dry weight - Use steady UFR - Keep dialysate Na + > serum Na + - Use bicarbonate dialysate - Avoid food before HD - Maintain Hct > 33% Pharmacologic Prevention - Caffeine 250 mg po 2 hrs into dialysis - Carnitine 20mg/kg during dialysis - Midodrine 5-10 mg 30min before HD Management of Cramps Acute mL saline bolus - 50mL hypertonic glucose mL 23.4% saline over min Non-pharm Prevention - set accurate dry wt - stretching - keep dialysate Na + > serum Na + - stationary bike at bedtime Pharmacologic Prevention - Diphenhydramine - Hydroquinine - Oxazepam - Prazosin - Quinine - Vitamin E
20 Management of Itching Non-pharm Prevention - deliver adequate Kt/V urea - use biocompatible dialyzers - diet phosphate compliance - maintain Hct > 33% - uv B light treatment - acupuncture Pharmacologic Prevention* - Topical emollients or capsaicin BID - hydroxyzine - cyproheptadine - loratidine/fexofenadine - cholestyramine - activated charcoal *Poor response to antihistamines suggests histamine not predominant mediator Peritoneal Dialysis Three components of dialysis: 1) Dialysate filled compartment 2) Blood filled compartment 3) Semi-permeable membrane No way to regulate blood flow, so PD less efficient than HD Larger molecules permitted to pass in PD compared to HD Solute profiles level out, similar to endogenous renal function
21 The Peritoneal Procedure Dialysate flows into peritoneal cavity by gravity over 15 minutes Toxins from blood cross peritoneal membrane and enter dialysate Dialysate removed and exchanged for new dialysate solution Thirty minutes for entire process Peritoneal Dialysis Types of PD Continuous Ambulatory (CAPD) 3 exchanges during waking hours Automated or Alternative (APD) Nocturnal Intermittent (NIPD) No exchange during day, at night via cycling machine Nocturnal Tidal (NTPD) No exchange during day, at night each hour with a constant volume of 1,500 ml in peritoneal cavity Continuous Cyclic (CCPD) Dialysate instilled in AM, dwells during day, removed prior to bed
22 The Peritoneal Rx Dose altered by osmotic gradient across peritoneum ultrafiltration and diffusion 1) # of bag exchanges per day 2) volume of each exchange 3) strength of dextrose in dialysate Recommended Kt/V urea = 1.7/week Must determine total volume drained Multiply x 7 for weekly Kt/V value Kt/V in PD Kt = D/P x volume drained (L/day) Divide by V to give Kt/V per day Multiple x 7 for weekly dose of Kt/V Patients on PD have some Kt/V contributed by residual renal function Initially Kt/V total = Kt/V PD + Kt/V renal As renal fxn declines and reach zero Kt/V total = Kt/V PD
23 Complications of PD Mechanical Medical Infectious Mechanical Complications of PD Kinking of catheter Inflow/outflow obstruction Catheter motion tissue aggravation Pain from catheter tip Rapid dialysate flow inflow pain
24 Medical Complications of PD CAUSE Glucose load COMPLICATION DM exacerbation TREATMENT IP insulin Fluid overload Electrolyte disturbances PD additives Malnutrition Unknown CHF exacerbation, edema, pulmonary congestion Hyper/hypocalcemia Chemical peritonitis Albumin and amino acid loss, muscle wasting, fat tissue Fibrin formation in dialysate UF rate Alter dialysate content Discontinue additives Dietary changes Parenteral nutrition Discontinue PD IP heparin Infectious Complications of PD: Bacterial Peritonitis Major cause of morbidity, mortality, and loss of PD access 40-60% of patients in 1 st year Mean incidence: 1 event Q mos Highest risk: Elderly Diabetic
25 Signs and Symptoms of Peritonitis Sign/Sx Sx Cloudy effluent Abdominal tenderness Fever Nausea/Vomiting Chills Incidence (%) Diagnosing Peritonitis Cloudy dialysate Signs and symptoms Culture dialysate WBC > 100/mm 3 > 50% neutrophils Gram s stain
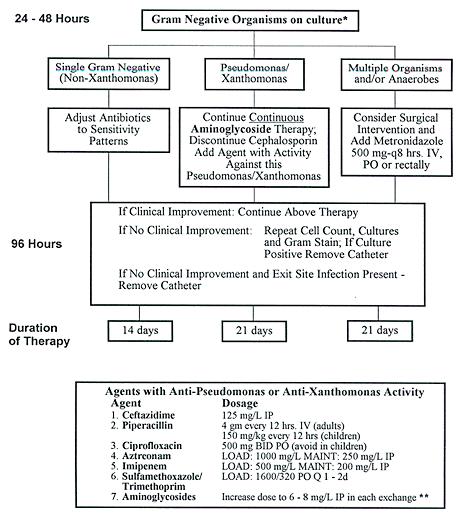
26 Microbiological Etiology Organism Staphylococcus epidermidis Staphylococcus aureus Streptococci Enterococci Escherichia coli Pseudomonas aeruginosa Enterobacter Acinetobacter Klebsiella Proteus Mixed infections Fungi % of Episodes Treatment of Peritonitis Empiric antibiotic therapy Gram positive culture Gram negative culture
27 Empiric Antibiotics for Peritonitis
28
29 Catheter-related related Infections 1 per patient year Nasal carries of S. aureus at highest risk Organism Staphylococcus aureus Staphylococcus epidermidis Pseudomonas aeruginosa Enteric Gram ( )( ) rods Incidence (%)
30 Advantages and Disadvantages of Hemodialysis Advantages Disadvantages High solute clearance Multiple visits/week Clear adequacy Long adjustment for paramters complications Complement activating Low failure rates membranes Better correction of Vascular access hemostasis infections Close monitoring of Faster decline of patient residual renal fxn than PD Advantages and Disadvantages of Peritoneal Dialysis Advantages Disadvantages Patient can do alone High risk of peritonitis No electricity or H 2 O Patient self-image Portable Transport of materials No anticoagulant High protein losses needed Lower urea clearance Minimal CV stress than HD No blood loss Patient burnout IP drug delivery Excessive glucose Clearance of larger absorption obesity solutes Mechanical problems
31 The Pharmacist s Role Knowing pharmacokinetic alterations Adjustment of doses in renal failure Proper use of expensive drugs Antibiotics Epogen IV iron products Replacement of dialyzed drugs Antibiotics Water-soluble vitamins ( Nephrocaps Nephrocaps ) Factors Increasing Drug Removal Dialyzer-specific pore size surface area charge membrane binding Dialysis-specific specific blood flow rate duration dialysis flow rate countercurrent flow Drug-specific molecular wt charge V D concentration gradient (high steady state level) hydrophilicity protein binding
32 Protein Binding Only unbound drugs eliminated by RRT Ability of drug to be filtered determined by sieving coefficient (SC), or non-bound fraction SC determined by: % protein binding membrane charge (i.e. binding to membrane) porosity of membrane Sieving Coefficient SC = C uf /C P SC = sieving coefficient uf = conc. of drug in ultrafiltrate (waste) C P = conc. of drug in plasma (blood) C uf If SC = 1, drug freely filtered If SC = 0, drug not filtered (highly protein bound)
33 Drug Dosing Drugs with renal clearance > 30% of total body clearance require replacement Loading doses: No adjustments necessary Depends on target blood level LD (mg) = desired C P (mg/l) x V d (L) LD = loading dose C P = plasma concentration V d = volume of distribution Drug Dosing Example: Vanco loading dose Pt wt = 65kg V d = 0.7 L/kg C P = 35mg/L LD (mg) = desired C P (mg/l) x V d (L) Vanco dose = 35 mg/l x (65kg x 0.7 L/kg) = 35 mg/l x 45.5 L = mg = 1500mg
34 Drug Dosing Maintenance Dosing Maintain therapeutic levels Use therapeutic drug monitoring (TDM) if possible (i.e. vanco/gent drug levels) Creatinine clearance method Estimates rate of drug removal Does not account for residual renal clearance (unless anuric) ) or non-renal clearance Creatinine Clearance Method CrCl = SC x UFR SC = sieving coefficient UFR = ultrafiltration rate (rate of waste into bag)

35 Creatinine Clearance Method Example: CrCl method for renal clearance Patient on CVVH with an UFR of 1.8 L/hr SC = 1.0 UFR = 1.8 L/hr CrCl = SC x UFR CrCl = 1.0 x 1.8 L/hr = 1,800 ml/hr = 30 ml/min Questions?
Drug Use in Dialysis
 (Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
(Last Updated: 08/22/2018) Created by: Socco, Samantha Drug Use in Dialysis Drambarean, B. (2017). Drug Use in Dialysis. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. DIALYSIS
Objectives. Peritoneal Dialysis vs. Hemodialysis 02/27/2018. Peritoneal Dialysis Prescription and Adequacy Monitoring
 Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
Peritoneal Dialysis Prescription and Adequacy Monitoring Christine B. Sethna, MD, EdM Division Director, Pediatric Nephrology Cohen Children s Medical Center Associate Professor Hofstra Northwell School
End-Stage Renal Disease. Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology
 End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
End-Stage Renal Disease Anna Vinnikova, M.D. Associate Professor of Medicine Division of Nephrology ESRD : Life with renal replacement therapy CASE: 18 month old male with HUS develops ESRD PD complicated
Physiology of Blood Purification: Dialysis & Apheresis. Outline. Solute Removal Mechanisms in RRT
 Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
Physiology of Blood Purification: Dialysis & Apheresis Jordan M. Symons, MD University of Washington School of Medicine Seattle Children s Hospital Outline Physical principles of mass transfer Hemodialysis
UNDERSTANDING THE CRRT MACHINE
 UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
UNDERSTANDING THE CRRT MACHINE Helen Dickie Renal Sister Critical Care Unit Guy s and St.Thomas NHS Foundation Trust 18.10.14 RRT options - IHD vs CRRT (1) Intermittent HaemoDialysis e.g. 4hrs daily or
Management of the patient with established AKI. Kelly Wright Lead Nurse for AKI King s College Hospital
 Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
Management of the patient with established AKI Kelly Wright Lead Nurse for AKI King s College Hospital Medical management Medical management Respiratory- pulmonary oedema, repositioning- upright, oxygen
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Imad Ahmed MD. Renal Associates of West Michigan
 Imad Ahmed MD Renal Associates of West Michigan ESRD Facts: - Medicare funded program - Cost - Significant mortality and morbidity - Reduced quality of life - Shrinking donor pool ESRD CAUSES - DM - Hypertension
Imad Ahmed MD Renal Associates of West Michigan ESRD Facts: - Medicare funded program - Cost - Significant mortality and morbidity - Reduced quality of life - Shrinking donor pool ESRD CAUSES - DM - Hypertension
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
PERITONEAL EQUILIBRATION TEST. AR. Merrikhi. MD. Isfahan University of Medical Sciences
 PERITONEAL EQUILIBRATION TEST AR. Merrikhi. MD. Isfahan University of Medical Sciences INTRODUCTION The peritoneal equilibration test (PET) is a semiquantitative assessment of peritoneal membrane transport
PERITONEAL EQUILIBRATION TEST AR. Merrikhi. MD. Isfahan University of Medical Sciences INTRODUCTION The peritoneal equilibration test (PET) is a semiquantitative assessment of peritoneal membrane transport
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018
 Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
Implementing therapy-delivery, dose adjustments and fluid balance. Eileen Lischer MA, BSN, RN, CNN University of California San Diego March 6, 2018 Objectives By the end of this session the learner will
ONLINE HEMODIALYSIS TRAINING SESSION 1
 ONLINE HEMODIALYSIS TRAINING SESSION 1 This document is a supplement to the Online Training. Do not reproduce. Copyright Dialysis4Career. All Rights Reserved. The Renal System - A highly sophisticated
ONLINE HEMODIALYSIS TRAINING SESSION 1 This document is a supplement to the Online Training. Do not reproduce. Copyright Dialysis4Career. All Rights Reserved. The Renal System - A highly sophisticated
Ana Paula Bernardo. CHP Hospital de Santo António ICBAS/ Universidade do Porto
 Ana Paula Bernardo CHP Hospital de Santo António ICBAS/ Universidade do Porto Clinical relevance of hyperphosphatemia Phosphate handling in dialysis patients Phosphate kinetics in PD peritoneal phosphate
Ana Paula Bernardo CHP Hospital de Santo António ICBAS/ Universidade do Porto Clinical relevance of hyperphosphatemia Phosphate handling in dialysis patients Phosphate kinetics in PD peritoneal phosphate
Hemodialysis is a life-sustaining procedure for the treatment of
 The Dialysis Prescription and Urea Modeling Biff F. Palmer Hemodialysis is a life-sustaining procedure for the treatment of patients with end-stage renal disease. In acute renal failure the procedure provides
The Dialysis Prescription and Urea Modeling Biff F. Palmer Hemodialysis is a life-sustaining procedure for the treatment of patients with end-stage renal disease. In acute renal failure the procedure provides
Renal Replacement Therapies
 Renal Replacement Therapies M I H Á L Y T A P O L Y A I, M D, F A S N, F A C P A s s o c i a t e P r o f e s s o r D e p a r t m e n t o f N e p h r o l o g y L o u i s i a n a S t a t e U n i v e r s
Renal Replacement Therapies M I H Á L Y T A P O L Y A I, M D, F A S N, F A C P A s s o c i a t e P r o f e s s o r D e p a r t m e n t o f N e p h r o l o g y L o u i s i a n a S t a t e U n i v e r s
The Physiology of Peritoneal Dialysis As Related To Drug Removal
 The Physiology of Peritoneal Dialysis As Related To Drug Removal Thomas A. Golper, MD, FACP, FASN Vanderbilt University Medical Center Nashville, TN thomas.golper@vanderbilt.edu Clearance By Dialysis Clearance
The Physiology of Peritoneal Dialysis As Related To Drug Removal Thomas A. Golper, MD, FACP, FASN Vanderbilt University Medical Center Nashville, TN thomas.golper@vanderbilt.edu Clearance By Dialysis Clearance
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
HEALTHYSTART TRAINING MANUAL. Living well with Kidney Disease
 HEALTHYSTART TRAINING MANUAL Living well with Kidney Disease KIDNEY DISEASE CAN AFFECT ANYONE! 1 HEALTHYSTART PROGRAMME HEALTHYSTART is a lifestyle management programme to assist you to remain healthy
HEALTHYSTART TRAINING MANUAL Living well with Kidney Disease KIDNEY DISEASE CAN AFFECT ANYONE! 1 HEALTHYSTART PROGRAMME HEALTHYSTART is a lifestyle management programme to assist you to remain healthy
GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS
 GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS RRCV CMG Nephrology Service 1. Introduction A first acute or chronic haemodialysis session may induce disequilibrium syndrome
GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS RRCV CMG Nephrology Service 1. Introduction A first acute or chronic haemodialysis session may induce disequilibrium syndrome
Continuous Renal Replacement Therapy. Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms SCUF - Slow Continuous Ultrafiltration
UNDERSTANDING PROCESS OF DIALYSIS
 UNDERSTANDING PROCESS OF DIALYSIS Introduction: End-stage renal disease (ESRD), the final stage of chronic kidney disease (CKD), occurs when the kidneys have deteriorated to the point that they are no
UNDERSTANDING PROCESS OF DIALYSIS Introduction: End-stage renal disease (ESRD), the final stage of chronic kidney disease (CKD), occurs when the kidneys have deteriorated to the point that they are no
Peritoneal Dialysis Prescriptions: A Primer for Nurses
 Peritoneal Dialysis Prescriptions: A Primer for Nurses A Primer ABCs of PD R x Betty Kelman RN-EC MEd CNeph (C) Toronto General Hospital University Health Network Toronto, Ontario, Canada A moment to remember
Peritoneal Dialysis Prescriptions: A Primer for Nurses A Primer ABCs of PD R x Betty Kelman RN-EC MEd CNeph (C) Toronto General Hospital University Health Network Toronto, Ontario, Canada A moment to remember
Continuous Renal Replacement Therapy
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD Definition of Terms SCUF - Slow Continuous Ultrafiltration
MODALITIES of Renal Replacement Therapy in AKI
 MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
MODALITIES of Renal Replacement Therapy in AKI Jorge Cerdá, MD, MS, FACP, FASN Clinical Professor of Medicine Albany Medical College Albany, NY, USA cerdaj@mail.amc.edu In AKI, RRT is a multidimensional
Nursing Care of the Dialysis Patient. Adrian Hordon, MSN, RN
 Nursing Care of the Dialysis Patient Adrian Hordon, MSN, RN Understand principles of hemodialysis Recognize different access ports Identify side effects and complications Discuss nursing care for pre and
Nursing Care of the Dialysis Patient Adrian Hordon, MSN, RN Understand principles of hemodialysis Recognize different access ports Identify side effects and complications Discuss nursing care for pre and
Smart APD prescription. Prof. Wai Kei Lo Tung Wah Hospital The University of Hong Kong
 Smart APD prescription Prof. Wai Kei Lo Tung Wah Hospital The University of Hong Kong Costing Comparison of Different Modes of RRT in Hong Kong in 2011 (Per Year) HK$300,000 HK$250,000 HK$200,000 HK$150,000
Smart APD prescription Prof. Wai Kei Lo Tung Wah Hospital The University of Hong Kong Costing Comparison of Different Modes of RRT in Hong Kong in 2011 (Per Year) HK$300,000 HK$250,000 HK$200,000 HK$150,000
Fundamentals of DIALYSIS
 Fundamentals of DIALYSIS Knowing Your Kidneys Healthy Kidneys are the body s cleaning crew These are twin bean shaped organs, of the size of fist They make up a filter system for the blood & reabsorb almost
Fundamentals of DIALYSIS Knowing Your Kidneys Healthy Kidneys are the body s cleaning crew These are twin bean shaped organs, of the size of fist They make up a filter system for the blood & reabsorb almost
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis
 How Wise is Early Dialysis in Critically Ill Patients? Modalities of Dialysis") Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Acute Kidney Injury (AKI) How Wise is Early Dialysis in Critically Ill Patients? A common condition in ICU patients Associated with high mortality and morbidity Renal Replacement Therapy (RRT) is the cornerstone
Gambrosol Trio, clinical studies 91 Glitazone, malnutrition-inflammationatherosclerosis
 Subject Index Acidosis, see Metabolic acidosis Activated carbon, sorbents 337 Adipokines adipose tissue and systemic inflammation 169 functions 167 169 prospects for study in renal patients 171 Adiponectin,
Subject Index Acidosis, see Metabolic acidosis Activated carbon, sorbents 337 Adipokines adipose tissue and systemic inflammation 169 functions 167 169 prospects for study in renal patients 171 Adiponectin,
Managing Acid Base and Electrolyte Disturbances with RRT
 Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Managing Acid Base and Electrolyte Disturbances with RRT John R Prowle MA MSc MD MRCP FFICM Consultant in Intensive Care & Renal Medicine RRT for Regulation of Acid-base and Electrolyte Acid base load
Renal Self Learning Package INTRODUCTION TO PERITONEAL DIALYSIS
 Renal Self Learning Package INTRODUCTION TO PERITONEAL DIALYSIS St George Hospital Renal Department, reviewed 2017 St George Hospital Renal Department RENAL SELF LEARNING PACKAGE INTRODUCTION TO PERITONEAL
Renal Self Learning Package INTRODUCTION TO PERITONEAL DIALYSIS St George Hospital Renal Department, reviewed 2017 St George Hospital Renal Department RENAL SELF LEARNING PACKAGE INTRODUCTION TO PERITONEAL
- SLED Sustained Low-Efficiency Dialysis
 Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
Continuous Renal Replacement Therapy Gregory M. Susla, Pharm.D., F.C.C.M. Associate Director, Medical Information MedImmune, LLC Gaithersburg, MD 1 Definition of Terms - SCUF - Slow Continuous Ultrafiltration
Chapter 2 Peritoneal Equilibration Testing and Application
 Chapter 2 Peritoneal Equilibration Testing and Application Francisco J. Cano Case Presentation FW, a recently diagnosed patient with CKD Stage 5, is a 6-year-old boy who has been recommended to initiate
Chapter 2 Peritoneal Equilibration Testing and Application Francisco J. Cano Case Presentation FW, a recently diagnosed patient with CKD Stage 5, is a 6-year-old boy who has been recommended to initiate
ECMO & Renal Failure Epidemeology Renal failure & effect on out come
 ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
ECMO Induced Renal Issues Transient renal dysfunction Improvement in renal function ECMO & Renal Failure Epidemeology Renal failure & effect on out come With or Without RRT Renal replacement Therapy Utilizes
CRRT Fundamentals Pre- and Post- Test. AKI & CRRT Conference 2018
 CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
CRRT Fundamentals Pre- and Post- Test AKI & CRRT Conference 2018 Question 1 Which ONE of the following statements regarding solute clearance in CRRT is MOST correct? A. Convective and diffusive solute
What is renal failure?
 What is renal failure? The kidney is a very important organ, and cannot be restored to health once it fails. However, it is possible to avoid or retard the deterioration of its functionality if therapy
What is renal failure? The kidney is a very important organ, and cannot be restored to health once it fails. However, it is possible to avoid or retard the deterioration of its functionality if therapy
You can sleep while I dialyze
 You can sleep while I dialyze Nocturnal Peritoneal Dialysis Dr. Suneet Singh Medical Director, PD, VGH Division of Nephrology University of British Columbia Acknowledgements Melissa Etheridge You can sleep
You can sleep while I dialyze Nocturnal Peritoneal Dialysis Dr. Suneet Singh Medical Director, PD, VGH Division of Nephrology University of British Columbia Acknowledgements Melissa Etheridge You can sleep
3/21/2017. Solute Clearance and Adequacy Targets in Peritoneal Dialysis. Peritoneal Membrane. Peritoneal Membrane
 3/21/2017 Solute Clearance and Adequacy Targets in Peritoneal Dialysis Steven Guest MD Director, Medical Consulting Services Baxter Healthcare Corporation Deerfield, IL, USA Peritoneal Membrane Image courtesy
3/21/2017 Solute Clearance and Adequacy Targets in Peritoneal Dialysis Steven Guest MD Director, Medical Consulting Services Baxter Healthcare Corporation Deerfield, IL, USA Peritoneal Membrane Image courtesy
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE
 PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE TABLE OF CONTENTS Introduction.... 3 SECTION 1: FUNDAMENTALS OF THE PRESCRIPTION.... 4 Getting Started: Patient Pathway to First Prescription.... 5 Volume
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT GUIDE TABLE OF CONTENTS Introduction.... 3 SECTION 1: FUNDAMENTALS OF THE PRESCRIPTION.... 4 Getting Started: Patient Pathway to First Prescription.... 5 Volume
Achieving Equilibrium in ESRD Patients
 Achieving Equilibrium in ESRD Patients -Marc Richards MD -South Florida Kidney Disease and HTN Specialists -Chief of Medicine, BRRH -BRRH Grand Rounds: April 18 th, 2017 Outline Dialysis prescription Adequacy
Achieving Equilibrium in ESRD Patients -Marc Richards MD -South Florida Kidney Disease and HTN Specialists -Chief of Medicine, BRRH -BRRH Grand Rounds: April 18 th, 2017 Outline Dialysis prescription Adequacy
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006
 CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006") IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE
Modes of Extracorporeal Therapies For ESRD Patients
 Modes of Extracorporeal Therapies For ESRD Patients Suhail, MD Extracorporeal Therapies: Dialytic Therapies Dialysis: Movement of molecules across a semipermeable membrane (Bi-directional) Movement of
Modes of Extracorporeal Therapies For ESRD Patients Suhail, MD Extracorporeal Therapies: Dialytic Therapies Dialysis: Movement of molecules across a semipermeable membrane (Bi-directional) Movement of
Kidney Failure. Haemodialysis
 Kidneys & Kidney Failure 2 Haemodialysis This booklet will help you to know the process of Haemodialysis in detail. It will also tell you about the disposables of Haemodialysis. In the end the advantages
Kidneys & Kidney Failure 2 Haemodialysis This booklet will help you to know the process of Haemodialysis in detail. It will also tell you about the disposables of Haemodialysis. In the end the advantages
CRRT Fundamentals Pre- and Post- Test Answers. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
CRRT Fundamentals Pre- and Post- Test Answers AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling
PD In Acute Kidney Injury. February 7 th -9 th, 2013
 PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
PD In Acute Kidney Injury February 7 th -9 th, 2013 Objectives PD as a viable initial therapy PD in AKI PD versus dhd PD versus CVVHD Why not PD first PD for AKI Early days (1970 s) PD was the option of
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2001
 CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2001") IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2001 [Before completing please read instructions at the bottom of this page and on pages 4 and 5] PATIENT IDENTIFICATION MAKE
IN-CENTER HEMODIALYSIS (HD) CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2001 [Before completing please read instructions at the bottom of this page and on pages 4 and 5] PATIENT IDENTIFICATION MAKE
What is a PET? Although there are many types of pets, we will be discussing the Peritoneal Equilibration Test
 1 2 3 What is a PET? Although there are many types of pets, we will be discussing the Peritoneal Equilibration Test 4 Background information about the PET 1983 Dr. Twardowski and colleagues began measuring
1 2 3 What is a PET? Although there are many types of pets, we will be discussing the Peritoneal Equilibration Test 4 Background information about the PET 1983 Dr. Twardowski and colleagues began measuring
Chapter 12 PERITONEAL DIALYSIS
 Chapter 12 PERITONEAL DIALYSIS B. Sunita A/P V. Bavanandan Anita Bhajan Manocha Lily Binti Mushahar Mohamad Zaimi Bin Abdul Wahab Sudhaharan Sivathasan PERITONEAL DIALYSIS 22nd Report of the SECTION 12.1:
Chapter 12 PERITONEAL DIALYSIS B. Sunita A/P V. Bavanandan Anita Bhajan Manocha Lily Binti Mushahar Mohamad Zaimi Bin Abdul Wahab Sudhaharan Sivathasan PERITONEAL DIALYSIS 22nd Report of the SECTION 12.1:
CRRT: The Technical Questions Modality & Dose. Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018
 CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CRRT: The Technical Questions Modality & Dose Ashita J. Tolwani, MD, MSc University of Alabama at Birmingham 2018 Case A 24YOM with HTN and OSA presents with acute pancreatitis. Despite aggressive fluid
CSI (Clinical Scenario Investigation): Hyperkalemia
: Hyperkalemia") CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
RENAL FAILURE IN ICU. Jo-Ann Vosloo Department Critical Care SBAH
 RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
RENAL FAILURE IN ICU Jo-Ann Vosloo Department Critical Care SBAH DEFINITION: RIFLE criteria Criteria for initiation of RRT Modes of RRT (options) CRRT = continuous renal replacement therapy SCUF : Ultra-filtration
Renal Replacement Therapies in Kidney Disease
 ORIGINAL ARTICLE Sanjiv Mahajan* Chief Medical Officer, Department of Nephrology & Medicine, Safdarjung Hospital & Vardhman Mahavir Medical College, New Delhi, India ABSTRACT Renal replacement therapy
ORIGINAL ARTICLE Sanjiv Mahajan* Chief Medical Officer, Department of Nephrology & Medicine, Safdarjung Hospital & Vardhman Mahavir Medical College, New Delhi, India ABSTRACT Renal replacement therapy
Renal Replacement Therapy in ICU. Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine
 Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Renal Replacement Therapy in ICU Dr. Sunil Sharma Senior Resident Dept of Pulmonary Medicine Introduction Need for RRT in patients with ARF is a common & increasing problem in ICUs Leading cause of ARF
Drug Dosing in Renal Insufficiency. Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila
 Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Patient Education Programme. Kidney Options Guiding you when kidneys fail
 Patient Education Programme Kidney Options Guiding you when kidneys fail About the kidneys What do healthy kidneys do? Your two kidneys work more than you realise. The kidneys remove excess body water
Patient Education Programme Kidney Options Guiding you when kidneys fail About the kidneys What do healthy kidneys do? Your two kidneys work more than you realise. The kidneys remove excess body water
Chapter Five Clinical indicators & preventive health
 Chapter Five Clinical indicators & preventive health The painter who draws merely by practice and by eye, without any reason, is like a mirror which copies every thing placed in front of it without being
Chapter Five Clinical indicators & preventive health The painter who draws merely by practice and by eye, without any reason, is like a mirror which copies every thing placed in front of it without being
A Review of Renal Diseases
 A Review of Renal Diseases NDFS 356 Amber McArthur April 3, 2014 0 INTRODUCITON Tom Harkin stated, America s health care system is in crisis precisely because we systematically neglect wellness and prevention.
A Review of Renal Diseases NDFS 356 Amber McArthur April 3, 2014 0 INTRODUCITON Tom Harkin stated, America s health care system is in crisis precisely because we systematically neglect wellness and prevention.
* It is proportionate to body size and the reference value is usually expressed after correction for body surface area as 120 ± 25 ml/min/1.
 Ahmad Al-zoubi Glomerular filtration rate : is the sum of the ultrafiltration rates from plasma into the Bowman s space in each nephron and is a measure of renal excretory function *co : 6L *renal blood
Ahmad Al-zoubi Glomerular filtration rate : is the sum of the ultrafiltration rates from plasma into the Bowman s space in each nephron and is a measure of renal excretory function *co : 6L *renal blood
Exer Ex cise Pa P tien tien with End End stag sta e g renal Disease
 Exercise in Patients with End stage Exercise in Patients with End stage renal Disease Chronic renal failure : gradual and progressive loss of the ability of the kidneys to function Structural kidney damage
Exercise in Patients with End stage Exercise in Patients with End stage renal Disease Chronic renal failure : gradual and progressive loss of the ability of the kidneys to function Structural kidney damage
Kidney Decisions Aid
 Kidney Decisions Aid A G U I D E F O R P E O P L E W H O H A V E, O R K N O W S O M E O N E, W I T H C H R O N I C K I D N E Y D I S E A S E, A N D T O A I D I N T H E D E C I S I O N A B O U T W H I C
Kidney Decisions Aid A G U I D E F O R P E O P L E W H O H A V E, O R K N O W S O M E O N E, W I T H C H R O N I C K I D N E Y D I S E A S E, A N D T O A I D I N T H E D E C I S I O N A B O U T W H I C
HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI
 HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI high-flux Hemodiafiltration (HDF) Combination of two dialysis techniques, hemodialysis and hemofiltration:
HEMODIAFILTRATION PRINCIPLES AND ADVANTAGES OVER CONVENTIONAL HD PRESENTATION BY DR.ALI TAYEBI high-flux Hemodiafiltration (HDF) Combination of two dialysis techniques, hemodialysis and hemofiltration:
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
02/21/2017. Assessment of the Peritoneal Membrane: Practice Workshop. Objectives. Review of Physiology. Marina Villano, MSN, RN, CNN
 Assessment of the Peritoneal Membrane: Practice Workshop Marina Villano, MSN, RN, CNN marina.villano@fmc-na.com Objectives Briefly review normal peritoneal physiology including the three pore model. Compare
Assessment of the Peritoneal Membrane: Practice Workshop Marina Villano, MSN, RN, CNN marina.villano@fmc-na.com Objectives Briefly review normal peritoneal physiology including the three pore model. Compare
THE HEMODIALYSIS PRESCRIPTION: TREATMENT ADEQUACY GERALD SCHULMAN MD VANDERBILT UNIVERSITY MEDICAL SCHOOL NASHVILLE, TENNESSEE
 THE HEMODIALYSIS PRESCRIPTION: TREATMENT ADEQUACY GERALD SCHULMAN MD VANDERBILT UNIVERSITY MEDICAL SCHOOL NASHVILLE, TENNESSEE THE DIALYSIS CYCLE /TIME DESIGN OF THE NATIONAL COOPERATIVE DIALYSIS STUDY
THE HEMODIALYSIS PRESCRIPTION: TREATMENT ADEQUACY GERALD SCHULMAN MD VANDERBILT UNIVERSITY MEDICAL SCHOOL NASHVILLE, TENNESSEE THE DIALYSIS CYCLE /TIME DESIGN OF THE NATIONAL COOPERATIVE DIALYSIS STUDY
Proceedings of the 36th World Small Animal Veterinary Congress WSAVA
 www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
www.ivis.org Proceedings of the 36th World Small Animal Veterinary Congress WSAVA Oct. 14-17, 2011 Jeju, Korea Next Congress: Reprinted in IVIS with the permission of WSAVA http://www.ivis.org 14(Fri)
UAB CRRT Primer Ashita Tolwani, MD, MSc University of Alabama at Birmingham
 UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
UAB CRRT Primer 2018 Ashita Tolwani, MD, MSc University of Alabama at Birmingham 1 CRRT Primer Continuous Renal Replacement Therapy (CRRT) is a "catch all" term used for all the continuous modes of renal
PD prescribing for all. QUESTION: Which approach? One size fits all or haute couture? (1) or (2)? The patient 18/03/2014.
 or (2)? The patient 18/03/2014.") PD prescribing for all Pr Max Dratwa Honorary consultant, Nephrology-Dialysis CHU Brugmann Université Libre de Bruxelles BSN 22 March 2014 QUESTION: Which approach? One size fits all or haute couture?
PD prescribing for all Pr Max Dratwa Honorary consultant, Nephrology-Dialysis CHU Brugmann Université Libre de Bruxelles BSN 22 March 2014 QUESTION: Which approach? One size fits all or haute couture?
Acute renal failure ARF
 Acute renal failure ARF Definition ARF is a clinical syndrome characterized by an abrupt decline in GFR and the accumulation of nitrogenous waste (BUN & creatinine). The decrease in GFR occurs relatively
Acute renal failure ARF Definition ARF is a clinical syndrome characterized by an abrupt decline in GFR and the accumulation of nitrogenous waste (BUN & creatinine). The decrease in GFR occurs relatively
Prescriptions for Home Hemodialysis
 9 Prescriptions for Home Hemodialysis Robert Lockridge, MD 1 Tom Cornelis, MD 2 Carolyn van Eps, MBBS, PhD, FRACP 3 1 Lynchburg Nephrology Physicians, Lynchburg, Virginia, USA; 2 Department of Internal
9 Prescriptions for Home Hemodialysis Robert Lockridge, MD 1 Tom Cornelis, MD 2 Carolyn van Eps, MBBS, PhD, FRACP 3 1 Lynchburg Nephrology Physicians, Lynchburg, Virginia, USA; 2 Department of Internal
The goal of dialysis for patients with chronic renal failure is to
 Dialysate Composition in Hemodialysis and Peritoneal Dialysis Biff F. Palmer The goal of dialysis for patients with chronic renal failure is to restore the composition of the body s fluid environment toward
Dialysate Composition in Hemodialysis and Peritoneal Dialysis Biff F. Palmer The goal of dialysis for patients with chronic renal failure is to restore the composition of the body s fluid environment toward
Client going into fluid volume. Fluid replacement = 24 hour fluid loss +.
 VIII. RENAL A. Glomerulonephritis: Acute can lead to chronic. 1. Pathophysiology: a. Inflammatory reaction in the. b. Antibodies lodge in the glomerulus; get scarring & filtering. c. Main cause: 2. S/S:
VIII. RENAL A. Glomerulonephritis: Acute can lead to chronic. 1. Pathophysiology: a. Inflammatory reaction in the. b. Antibodies lodge in the glomerulus; get scarring & filtering. c. Main cause: 2. S/S:
Acid-base profile in patients on PD
 Kidney International, Vol. 6, Supplement 88 (23), pp. S26 S36 Acid-base profile in patients on PD SALIM MUJAIS Renal Division, Baxter Healthcare Corporation, McGaw Park, Illinois Acid-base profile in patients
Kidney International, Vol. 6, Supplement 88 (23), pp. S26 S36 Acid-base profile in patients on PD SALIM MUJAIS Renal Division, Baxter Healthcare Corporation, McGaw Park, Illinois Acid-base profile in patients
Volume Management 2/25/2017. Disclosures statement: Objectives. To discuss evaluation of hypervolemia in peritoneal dialysis patients
 Volume Management Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 14, 2017 Disclosures statement: Consultant: Allena, Becker Professional Education Grant
Volume Management Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 14, 2017 Disclosures statement: Consultant: Allena, Becker Professional Education Grant
Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate
 Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate Summary. The urea reduction ratio (URR) has been rising year on year but now appears to have reached a plateau.. The URR increases the longer
Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate Summary. The urea reduction ratio (URR) has been rising year on year but now appears to have reached a plateau.. The URR increases the longer
UW MEDICINE PATIENT EDUCATION. Peritoneal Dialysis. A treatment option for kidney disease. There are 2 types of PD: continuous ambulatory
 UW MEDICINE PATIENT EDUCATION Peritoneal Dialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and basic principles of continuous ambulatory peritoneal dialysis (CAPD). 2.
UW MEDICINE PATIENT EDUCATION Peritoneal Dialysis A treatment option for kidney disease Class Goals 1. Understand the purpose and basic principles of continuous ambulatory peritoneal dialysis (CAPD). 2.
ad e quate adjective \ˈa-di-kwət\
 PD Prescriptions and Adequacy Monitoring: The Basics Fundamentals of Dialysis in Children Seattle, Washington February 27th, 2016 Colin White Steve Alexander Brad Warady Alicia Neu Franz Schaefer Bruce
PD Prescriptions and Adequacy Monitoring: The Basics Fundamentals of Dialysis in Children Seattle, Washington February 27th, 2016 Colin White Steve Alexander Brad Warady Alicia Neu Franz Schaefer Bruce
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Section 3: Prevention and Treatment of AKI
 http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
http://www.kidney-international.org & 2012 KDIGO Summary of ommendation Statements Kidney International Supplements (2012) 2, 8 12; doi:10.1038/kisup.2012.7 Section 2: AKI Definition 2.1.1: AKI is defined
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT QUICK REFERENCE GUIDE
 PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT QUICK REFERENCE GUIDE This quick reference guide will help serve as a reference tool for clinicians setting a patient s Peritoneal Dialysis (PD) prescription.
PERITONEAL DIALYSIS PRESCRIPTION MANAGEMENT QUICK REFERENCE GUIDE This quick reference guide will help serve as a reference tool for clinicians setting a patient s Peritoneal Dialysis (PD) prescription.
egfr 34 ml/min egfr 130 ml/min Am J Kidney Dis 2002;39(suppl 1):S17-S31
:S17-S31") Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
LLL Session - Nutritional support in renal disease
 ESPEN Congress Leipzig 2013 LLL Session - Nutritional support in renal disease Peritoneal dialysis D. Teta (CH) Nutrition Support in Patients undergoing Peritoneal Dialysis (PD) Congress ESPEN, Leipzig
ESPEN Congress Leipzig 2013 LLL Session - Nutritional support in renal disease Peritoneal dialysis D. Teta (CH) Nutrition Support in Patients undergoing Peritoneal Dialysis (PD) Congress ESPEN, Leipzig
EXCRETION QUESTIONS. Use the following information to answer the next two questions.
 EXCRETION QUESTIONS Use the following information to answer the next two questions. 1. Filtration occurs at the area labeled A. V B. X C. Y D. Z 2. The antidiuretic hormone (vasopressin) acts on the area
EXCRETION QUESTIONS Use the following information to answer the next two questions. 1. Filtration occurs at the area labeled A. V B. X C. Y D. Z 2. The antidiuretic hormone (vasopressin) acts on the area
Home Dialysis. Peritoneal Dialysis. Home Hemodialysis
 Home Dialysis The information provided is not intended to be a substitute for professional medical advice. A licensed healthcare professional should be consulted for diagnosis and treatment of any and
Home Dialysis The information provided is not intended to be a substitute for professional medical advice. A licensed healthcare professional should be consulted for diagnosis and treatment of any and
Blood Vessels. Chapter 20
 Blood Vessels Chapter 20 Summary of the Characteristics of Arteries and Veins Characteristic Artery Vein Wall thickness thick thin Shape in cross section round flattened Thickest tunic media externa Collagen
Blood Vessels Chapter 20 Summary of the Characteristics of Arteries and Veins Characteristic Artery Vein Wall thickness thick thin Shape in cross section round flattened Thickest tunic media externa Collagen
DIALYSIS. Ellie Stanger, Tessie Atwater, Summer White, McKenzie Driscoll
 DIALYSIS Ellie Stanger, Tessie Atwater, Summer White, McKenzie Driscoll PATHOPHYSIOLOGY Chronic Kidney Disease A wide range of kidney lesions characterized by a slow, steady decline in renal function A
DIALYSIS Ellie Stanger, Tessie Atwater, Summer White, McKenzie Driscoll PATHOPHYSIOLOGY Chronic Kidney Disease A wide range of kidney lesions characterized by a slow, steady decline in renal function A
Intradialytic Parenteral Nutrition in Hemodialysis Patients. Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia
 Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Your Kidney Health. Your Choices. Chronic Kidney Disease
 Your Kidney Health Your Choices Your doctor may have told you that you have chronic kidney disease (CKD or advanced kidney disease; or, you may be in kidney failure, and may have to make a decision about
Your Kidney Health Your Choices Your doctor may have told you that you have chronic kidney disease (CKD or advanced kidney disease; or, you may be in kidney failure, and may have to make a decision about
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2
 Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
Operation-Fluids-Electrolytes-Acid Base COMPLICATIONS OF DIALYSIS 2 Maureen Craig, RN, MSN, CNN University of California Davis Medical Center Sacramento, California macraig@ucdavis.edu Hospital Details
KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You
 KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You What Kidneys Do The kidneys are a pair of bean shaped organs located below your ribcage near the middle of your back. Kidneys play a vital
KIDNEY FAILURE TREATMENT OPTIONS Choosing What s Best For You What Kidneys Do The kidneys are a pair of bean shaped organs located below your ribcage near the middle of your back. Kidneys play a vital
Body Fluids and Fluid Compartments
 Body Fluids and Fluid Compartments Bởi: OpenStaxCollege The chemical reactions of life take place in aqueous solutions. The dissolved substances in a solution are called solutes. In the human body, solutes
Body Fluids and Fluid Compartments Bởi: OpenStaxCollege The chemical reactions of life take place in aqueous solutions. The dissolved substances in a solution are called solutes. In the human body, solutes
Practical issues - dosing on extracorporeal circuits
 Practical issues - dosing on extracorporeal circuits Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
Practical issues - dosing on extracorporeal circuits Jason A Roberts B Pharm (Hons), PhD, FSHP Professor of Medicine and Pharmacy The University of Queensland, Australia Royal Brisbane and Women s Hospital,
PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond
 PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond John Burkart, M.D. Wake Forest University Baptist Medical Center CMO Health Systems Management 8/2014 John M. Burkart, MD Educational Grants
PERITONEAL DIALYSIS ADEQUACY: The KDOQI Guidelines and Beyond John Burkart, M.D. Wake Forest University Baptist Medical Center CMO Health Systems Management 8/2014 John M. Burkart, MD Educational Grants
Medical Emergencies in Dialysis Patients
 Medical Emergencies in Dialysis Patients John Anderton Consultant Renal Physician Lancashire Teaching Hospitals NHS Foundation Trust Talk Plan A Flavour of Dialysis patients Emergencies in HD patients
Medical Emergencies in Dialysis Patients John Anderton Consultant Renal Physician Lancashire Teaching Hospitals NHS Foundation Trust Talk Plan A Flavour of Dialysis patients Emergencies in HD patients
I. FILL IN THE BLANKS
 1 BHARAT SEVAK SAMAJ NATIONAL DEVELOPMENT AGENCY, PROMOTED BY GOVERNMENT OF INDIA CENTRAL BOARD OF EXAMINATIONS BSS NATIONAL VOCATIONAL EDUCATION MISSION AHE025-BSS DIPLOMA IN DIALYSIS TECHNOLOGY TWO YEARS
1 BHARAT SEVAK SAMAJ NATIONAL DEVELOPMENT AGENCY, PROMOTED BY GOVERNMENT OF INDIA CENTRAL BOARD OF EXAMINATIONS BSS NATIONAL VOCATIONAL EDUCATION MISSION AHE025-BSS DIPLOMA IN DIALYSIS TECHNOLOGY TWO YEARS
Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents
 Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents Jesus Contreras, D.O. PGY-4 John Yasmer, D.O. Department of Radiology No Disclosures Objectives Introduce
Introduction to the Native Arteriovenous Fistula: A primer for medical students and radiology residents Jesus Contreras, D.O. PGY-4 John Yasmer, D.O. Department of Radiology No Disclosures Objectives Introduce
PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006
 PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE CORRECTIONS
PERITONEAL DIALYSIS CLINICAL PERFORMANCE MEASURES DATA COLLECTION FORM 2006 PATIENT IDENTIFICATION [Before completing please read instructions at the bottom of this page and on pages 5 and 6] MAKE CORRECTIONS
Lesson #7: Quality Assessment and Performance Improvement
 ESRD Update: Transitioning to New ESRD Conditions for Coverage Student Manual Lesson #7: Quality Assessment and Performance Improvement Learning Objectives At the conclusion of this lesson, you will be
ESRD Update: Transitioning to New ESRD Conditions for Coverage Student Manual Lesson #7: Quality Assessment and Performance Improvement Learning Objectives At the conclusion of this lesson, you will be
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Kidney Disease Treatment Options
 Page 1 Fact sheet The kidneys play a number of important roles in your body such as: extracting excess water to make urine (wee) controlling your blood pressure filtering waste products and toxins from
Page 1 Fact sheet The kidneys play a number of important roles in your body such as: extracting excess water to make urine (wee) controlling your blood pressure filtering waste products and toxins from