Finding Ways Around High Dose Insulin Requirements: U-500 Insulin, Weight Loss, and Future Therapies
|
|
|
- Shanon Malone
- 6 years ago
- Views:
Transcription

1 Finding Ways Around High Dose Insulin Requirements: U-500 Insulin, Weight Loss, and Future Therapies Elaine K. Cochran, MSN, CRNP, BC-ADM National Institute of Diabetes and Digestive and Kidney Diseases Bethesda, Maryland
2 Outline of Talk High Dose Insulin Requirements- History of Treatment Examples of severe insulin resistance Identifying patients with other forms of diabetes Impact of energy intake on insulin sensitivity High-Dose Insulin Requirements Mechanical issues Principles of treating to target glycemia DCCT, DPP, UKPDS Use of Insulin therapy U-500 insulin Pharmacology and Availability Manufactured by Lilly USA, LLC Pharmacologic profile Cost
3 Outline (cont) Deciding when to begin U-500 insulin Principles that guide practice Determining patient s U-500 requirements Dosing of U-500 Insulin > , , >600 units/day Dose adjustments Specifics with Insulin Pumps Practical Issues in Administration Inpatient Setting Outpatient Setting Impact of Diet Examples of diet therapy on insulin requirements
4 Outline (cont) Teaching Points Encourage decrease caloric intake Examples of Regimen Handouts Teaching patients how to express their regimen to others Conclusions Weight loss and decreased caloric intake, and increasing activity are essential to controlling insulin doses U-500 insulin is effective and cost efficient in high dose insulin requiring patient Diabetes educator plays key role in teaching patient to use and administer U-500 insulin

 patients requiring more than 2-3")
5 Patients with High-Dose Insulin Requirements Typically defined as severe insulin resistance Patients requiring more than 200 units of insulin/ day, for > 2 days Pediatric (and in general in terms of weight) patients requiring more than 2-3 units/kg/day
6 Insulin Requirements Influenced by type of diabetes - Influenced by energy intake - Insulin requirements when fasting - Insulin requirements after bariatric surgery Influenced by device/mechanical issues: -Pumps with bolus rate limits of 1 unit per 40 seconds, maximum bolus of units, and cartridge that holds units - Pens with maximum amount of 60 unit or 80 unit bolus

7 ADA Classification of Diabetes Type 1 Diabetes Type 2 Diabetes Gestational Diabetes Other specific types of diabetes *All can be associated with high dose insulin requirements
8 Review of Other Diabetes Genetic defects of β cell function Genetic defects of Insulin Action Studies at NIH of patients with Type A, Leprechaunism, Lipodystrophy. Typically most commonly associated with use of U-500 insulin Type B (also associated with U-500) Endocrinopathies (Acromegaly, Cushing s) Drug induced (steroids, etc)

9 Typical Insulin Requirements for Various Forms of Diabetes Mellitus
10 Theoretical Dose Response Curves for Insulin in Diabetes U/kg/d Therapeutic target U/kg/d 3 to > 500 U/kg/d
11 Type 2 vs Other Simple Screening Laboratory findings Fasting TG s level Severity of insulin resistance (i.e. insulin or c-peptide levels) Insulin requirements on weight maintenance/weight loss diet Physical symptoms of hyperinsulinemia Age of Patient: Young vs Older

 Size of")




12 Type 2 vs Other (cont.) Size of Patient: Obese vs Lean



13 Type 2 vs. Other (cont.) Physical Findings: acanthosis nigricans and polycystic ovarian syndrome
14 Role of Energy Expenditure and Weight Previous graphs show daily insulin requirements as units/kg/day Weight has direct effect on insulin dose Insulin resistance also impacts dose Obesity is related to insulin resistance
15 Role of Excessive Energy Intake Taking in more energy than utilizing When you reduce it with modest changes in body weight (5-6%), decreased energy intake effects glucose energy metabolism Evidence in the literature: Acute dietary DPP Bariatic surgery
16 Excess energy intake (cont.) One of the first articles, describing a study done at our Institute, looking at the acute physiologic effects of decreased energy intake on insulin sensitivity.
17 Excess energy intake (cont.) Findings of the Diabetes Prevention Program: This is another example, and well known, of how weight loss, even modest (5%), results in improvement in insulin sensitivity.

18 Excess energy intake (cont.) Recent example:

19 Putting it all together: Example from Pima Indians Median dose of insulin for a group of Pima Indians: 70 units/day. Average weight: 100 kg. Average HgbA1c: 9.4% High incidence of microvascular disease
20 Why? Principles behind insulin therapy Hyperglycemia over time will lead to microvascular/cardiovascular complications Insulin leads to weight gain and obesity, which also has co-morbidities Complications of weight gain (excess energy intake) vs. hyperglycemia
21 Answer Evidenced based medicine--treat diabetes DCCT, EDIC, UKPDS, ADVANCE and other trials Evidence shows clear rationale for maintaining glucose levels as close to target as possible Yes, obesity is bad, but hyperglycemia can lead to microvascular disease, cardiovascular disease. Looking back to model patient populations : microvascular disease is rampant amongst the Pima Indian populations.
22 Insulin Developments U-80 introduced 1946 Isophane insulin (NPH--Toronto-Hagedorn Labs) 1952 Beef U-500 Regular (Lilly); insulin zinc suspensions developed (Hallas-Moller; Copenhagen-Novo) 1973 U-100 introduced 1980 Pork U-500 Regular (Lilly) 1982 human insulin (pork modification [Novo]; recombinant technology [Humulin Genentech/Lilly]) 1996 Lispro (Humalog -- Lilly) 1997 Human U-500 (Humulin U-500 Regular--Lilly)
23 Use of U-500 Insulin in the Literature First Reports 1976 Kahn et al. wrote about syndromes of insulin resistance 1989 Fain s case report using U-500 with educator perspective 2000 First recorded use of U-500 during pregnancy 2003 Detailed use in pump in T2DM 2005 Cochran et al., U-500 algorithm 2008 Cochran et al., U-500 use in children

24 NIH Patients on U-500
25 Efficacy of U-100 Insulin Delivery in High-Dose Requiring Patients Practically (mechanical influences): Syringes highest volume is 100 units. Pens highest volume is units, with the total insulin pen cartridge only holding up to 300 units. Pump cartridges hold units. Pump bolus rates and limits (25-30 units) Batteries for pumps need to be changed more frequently (every week as opposed to month) Insurance for supplies often at set levels/amounts (often based on Type 1 diabetes model)






26 Chart from: Diabetes Health Professional, Dec-Jan. 2010, pp
27 Efficacy of U-100 (cont.) Patient comfort Multiple large volume injections-difficult/painful Complicated/painful regimen minimizes compliance Risk of abscesses in single injection site i.e. pumps Absorption and Action of Insulin Large injection volume impedes absorption Dose response curves are flattened and shifted to the right, thus potency of larger volume of insulin is actually reduced
28 What is U-500 Insulin? Human Regular Insulin 5 times more concentrated than U-100 Dose Response Onset: within 30 minutes Peak: 1.75 to 4 hours Duration of action: 6 to 10 hours, up to 24 hours Often compared to NPH drug profile



29 U-500 Human Regular

30 Theoretical Time Action Profile
31 Cost Comparisons **Average Wholesale Prices as of August 4, 2010
 277-5742")
32 Availability Allow 24 to 72 hours for pharmacy to obtain U-500 Supplied in 20 mls vials Bright brown stripes on box Complicated clinical issues contact Jeffrey Alan Jackson, MD Lead physician for U-500R at Lilly. USA (317)
33 Safety/Handling Considerations Hypoglycemia (similar incidence to U-100) No syringe currently available to measure actual units of U-500 Hospitals must delineate as CONCENTRATED in formulary Pharmacies cannot stock unless have existing patient on U-500 Stability comparable to other forms Storage and shelf life Pre-draw syringes should be stored with needle upright.
34 Starting U-500 Verify if and how patient is taking current U-100 regimen Is delivery device optimal? Can patient describe regimen well (since they supposedly do it every day) Determine daily insulin requirements Useful method: U-100 Regular four times daily (30%, 25%, 25%, 20%; weight based)
35 Dosing of U-500 1) Stop all forms of insulin U-100 2) HgbA1c <8%, reduce 10-20% HgbA1c>10%, increase 10-20% 3) U-500 Basal/Bolus Therapy A. twice daily B. three times daily C. four times daily, for over 600U/day 4) Determine best delivery method
36 Algorithm for the Administration and Dosing of U-500 Insulin INSULIN DAILY DOSE INJECTION FREQUENCY/SCHEDULE/DELIVERY GUIDE FOR HOW DOSES ARE DIVIDED DAILY VIA PERCENTAGE (%) OF THE TOTAL DAILY DOSE units/day Twice daily (i.e. 8A, 6PM) +/- Basal Insulin Three times daily (i.e. 8A, 12noon, 6PM) +/- Basal Insulin Via insulin pump (1unit = 0.01 mls mls of U-500 insulin = 5 units) 60/40 40/30/30 Three mealtime boluses (30/25/25) In addition a set basal rate of 20% of the total daily dose (minimize basal rate changes per day) Or basal at 50% of total daily dose, and divide up boluses (20/20/10) Nighttime basal may need to be dramatically reduced units/day Three times daily 40/30/30 Four times daily (i.e. 8A, 12noon, 5PM, 10PM) Via insulin pump (1unit = 0.01 mls mls of U-500 insulin = 5 units) 30/30/30/10 Three-four mealtime boluses For basal rate 20% of daily dose, boluses are (30/30/20 or 30/25/20/5). For basal at 50% of total daily dose, and divide up boluses (20/20/10 or 20/15/10/5). Bedtime snack bolus should be 10% or less of total daily dose. > 600 units/day Four times daily ** do not inject more than 2 mls in any one injection site Confidential-NIH/NIDDK 30/30/30/10
37 Theoretical Insulin Action 2x daily
38 Theoretical Insulin Action 3x daily
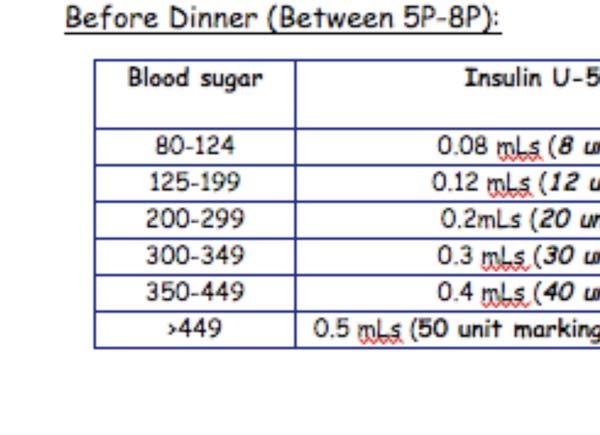
39 Appropriate Prescription Example TB syringe Insulin Human Regular U-500, inject 150 units, 0.3 mls subcutaneously, 3 times daily before meals. Dispense 2 vials. Insulin syringe Insulin Human Regular U-500, inject 150 units, 30 unit markings subcutaneously, 3 times daily before meals. Dispense 2 vials.
40 Dosage Conversion Chart

41 Insulin Pump Use Technically off-label use through pump Doses units/day Not recommended for >600U/day Not in volume, use pump units 1 pump unit = 0.01mLs 0.01mLs = 5U of U500 1 pump unit = 5 actual units of U-500
42 Insulin Pump Use (cont.) Patients on U-500 MDI, 50% of TDD 24, single basal hourly rate. Remaining 50% distributed as pre-meal boluses Patients on U-100, 50% of TDD 5 then 24 to determine basal. Insulin on board: Set at 6 hours Important info: 1) fasting basal, 2) endogenous insulin production

43 Practical Administration: Inpatient Setting Patients on U-500 Insulin Clinicians understand and think in terms of dose. Patients think in terms of practical administration. VERY IMPORTANT! *Have them demonstrate measuring dose.
 Policy for prescribing and administering Write the prescription in terms of volume Use TB syringes when inpatient")
44 Inpatient Setting (cont.) Policy for prescribing and administering Write the prescription in terms of volume Use TB syringes when inpatient Possibly use insulin drip until hospital pharmacy acquires U-500 and/or use of patient s home medication
 Four times daily")


45 Inpatient Setting (cont.) Four times daily Insulin Regular U-100, is also effective up to 300U/day, until U-500 can be obtained in the hospital.

46 Inpatient Setting: Syringe Selection TB Syringe - Recommended for volume measurement mls, 1.0 mls - Available in safety needle form Insulin syringe - unit markings *Prescription must match syringe
47 Inpatient Setting: Resources such as the American Journal of Health-System Pharmacy Standing order insulin vs. Corrective Regimens Pharmacy prepare dose vs. Nurses drawing up dose IMPACT OF DIET Patient may only require U-100 insulin in the hospital, as they are eating less Examples of diet (energy intake) on insulin doses
48 Inpatient Setting (cont.)

49 Outpatient Setting Health insurance coverage issues of insulin and supplies Specialized teaching: Transcribing dose such that patient understands Reinforcing proper regimen communication



50 Outpatient Setting (cont.)










51 Contact Lilly Rx for U-500 Leave Behind
52 Future Therapies-NIDDK Research Research looking at regulating the human thermostat, and energy excess issues Our research with leptin therapy Hormone secreted in adipose tissue Hormone controls appetite
53 Conclusions Insulin requirements are based on type of diabetes, degree of insulin resistance, weight, and energy intake Epidemic of obesity is increasing the incidence of type 2 diabetes, and high dose insulin requirements Evidence from diabetes complications trials provides principles to treat hyperglycemia U-500 insulin has been used since 1952 U-500 has onset and peak of action similar to regular insulin, but duration of action more like NPH Dosing algorithm based on anecdotal experience of hundreds of patients U-500 needs to be weighted more towards morning and mid-day, lesser amounts evening and bedtime.
54 Conclusions (cont.) Hospital use of U-500 TB syringe recommended Hospital policy of use needed Impact of diet on insulin requirements Existing U-500 patients should demonstrate their dose on the syringe they use to prescriber Inpatient and Outpatient Use Specialized diabetes instruction Reinforce caloric reduction, increase exercise Unique written materials When verifying the dose have patient show their dose on the syringe


55 Acknowledgements Phillip Gorden, MD Chris Chamberlain, PharmD U-500 Advisory Panel Jeff Jackson, MD Ilene Corey, CRNP Irl Hirsch, MD Wendy Lane, MD Jay Skyler, MD U-500 colleagues Virginia Valentine, CNS and my courageous patients
 496-2718 Lilly USA, LLC")
56 Questions? Office phone: (301) Lilly USA, LLC LILLY RX
Type I Type II Insulin Resistance
 Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
ADMELOG, NOVOLIN, NOVOLOG, and FIASP
 ADMELOG, NOVOLIN, NOVOLOG, and FIASP Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
ADMELOG, NOVOLIN, NOVOLOG, and FIASP Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
For patients uncontrolled on multiple daily injections of insulin. A quick-start guide for your practice ALL-DAY CONTROL WITH
 For patients uncontrolled on multiple daily injections of insulin A quick-start guide for your practice Dosing guidance 1,* V-Go: 3 options 1 For initiating V-Go in patients switching from MDI The majority
For patients uncontrolled on multiple daily injections of insulin A quick-start guide for your practice Dosing guidance 1,* V-Go: 3 options 1 For initiating V-Go in patients switching from MDI The majority
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Safe use of insulin regular concentrated (500 units/ml) in severe insulin resistance
 in severe insulin resistance") Safe use of insulin regular concentrated (500 units/ml) in severe insulin resistance Jodie S. Gee, Pharm.D., BCACP, CDE Clinical Pharmacy Specialist-Ambulatory Care Harris Health System Objectives To be
Safe use of insulin regular concentrated (500 units/ml) in severe insulin resistance Jodie S. Gee, Pharm.D., BCACP, CDE Clinical Pharmacy Specialist-Ambulatory Care Harris Health System Objectives To be
U-500 Insulin: Not for Ordinary Use
 Page 1 of 7 U-500 Insulin: Not for Ordinary Use Adam Clark, PharmD, BCPS Medical Clinic Pharmacist Gainesville, Florida 5/20/2010 US Pharm. 2010;35(5)(Diabetes suppl):14-17. If not already seeing them,
Page 1 of 7 U-500 Insulin: Not for Ordinary Use Adam Clark, PharmD, BCPS Medical Clinic Pharmacist Gainesville, Florida 5/20/2010 US Pharm. 2010;35(5)(Diabetes suppl):14-17. If not already seeing them,
Insulin 10/11/17. Disclosures. Objectives. Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI)
") Insulin The What, When, Where, Who and Why Disclosures Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI) Objectives Define background and history
Insulin The What, When, Where, Who and Why Disclosures Speaker and Consultant for Jansen and Healthscripts Speaker and Consultant for Boehringer Ingelheim (BI) Objectives Define background and history
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Insulin Regimens: Hitting Glycemia Targets
 Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products
 Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Insulin Prior Authorization Criteria For Individuals Who Purchased BlueCare/KS Solutions/EPO Products FDA LABELED INDICATIONS 1-13,16-21 Rapid-Acting Indication Onset Peak Duration Insulins Admelog (insulin
Diabetes Head to Toe May 31, 2017
 Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products
 Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
Insulin Prior Authorization Criteria For Individuals who Purchased BlueCare / KS Solutions products FDA LABELED INDICATIONS 1-13,16-20 Rapid-Acting Indication Onset Peak Duration Insulins Fiasp (insulin
Disclosures. Learning Objectives 4/26/2017
 Implementation of a quality improvement initiative to ensure the safe transition from prior-to-admission concentrated insulins to a formulary insulin regimen ERICA J. RHEIN, PHARMD PGY1 PHARMACY PRACTICE
Implementation of a quality improvement initiative to ensure the safe transition from prior-to-admission concentrated insulins to a formulary insulin regimen ERICA J. RHEIN, PHARMD PGY1 PHARMACY PRACTICE
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Injectable Therapies in Diabetes Diabetes Specialist Nurse Linda Burns Learning Outcomes Understand the place of injectible therapies in diabetes Understand when patients may require insulin therapy Consider
Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
MANAGEMENT OF TYPE 1 DIABETES MELLITUS
 MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
Faculty. Concentrated Insulin: Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management. Disclosures. Learning Objectives
 Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Objectives. Navigating New Insulins. Disclosures. Diabetes: The Stats. Normal Insulin Release Individuals without diabetes. History of Insulin 5/23/17
 Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
Module 5. Understanding Insulin Therapy
 Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Injecting Insulin into Out Patient Practice
 Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Injecting Insulin into Out Patient Practice Kathleen Colleran, MD Associate Professor UNMHSC 4/22/10 Overview Natural history of Type 2 diabetes Reasons clinicians are reluctant to start insulin therapy
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Introduction. Methods
 A New Perspective On A Difficult Discharge: Ensuring the newly diagnosed diabetic patient gets the proper prescriptions when it s time to go home. Ashley Carter, PGY 3 Introduction A hospitalized patient
A New Perspective On A Difficult Discharge: Ensuring the newly diagnosed diabetic patient gets the proper prescriptions when it s time to go home. Ashley Carter, PGY 3 Introduction A hospitalized patient
Learning Objectives. Are you ready for more insulin formulations?
 Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
A Call to Action: Addressing Diabetes Medication Safety
 A Call to Action: Addressing Diabetes Medication Safety Evan M. Klass, M.D., F.A.C.P. Senior Associate Dean, Statewide Initiatives Reducing ED visits for insulin induced hypoglycemia is a Healthy People
A Call to Action: Addressing Diabetes Medication Safety Evan M. Klass, M.D., F.A.C.P. Senior Associate Dean, Statewide Initiatives Reducing ED visits for insulin induced hypoglycemia is a Healthy People
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Think about when / why patients require insulin therapy
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Think about when / why patients require insulin therapy
APIDRA (insulin glulisine) injection vial APIDRA SOLOSTAR (insulin glulisine) subcutaneous solution pen-injector
 injection vial APIDRA SOLOSTAR (insulin glulisine) subcutaneous solution pen-injector") APIDRA SOLOSTAR (insulin glulisine) subcutaneous solution pen-injector Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
APIDRA SOLOSTAR (insulin glulisine) subcutaneous solution pen-injector Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Premixed Insulin for Type 2 Diabetes. a gu i d e f o r a d u lt s
 Premixed Insulin for Type 2 Diabetes a gu i d e f o r a d u lt s March 2009 What This Guide Covers / 2 Type 2 Diabetes / 3 Learning About Blood Sugar / 4 Learning About Insulin / 5 Comparing Medicines
Premixed Insulin for Type 2 Diabetes a gu i d e f o r a d u lt s March 2009 What This Guide Covers / 2 Type 2 Diabetes / 3 Learning About Blood Sugar / 4 Learning About Insulin / 5 Comparing Medicines
What do diabetes medicines do?
 What do diabetes medicines do? Over time, high levels of blood glucose, also called blood sugar, can cause health problems. These problems include heart disease, heart attacks, strokes, kidney disease,
What do diabetes medicines do? Over time, high levels of blood glucose, also called blood sugar, can cause health problems. These problems include heart disease, heart attacks, strokes, kidney disease,
LEVEMIR (insulin detemir) subcutaneous solution LEVEMIR FLEXTOUCH (insulin detemir) subcutaneous solution pen-injector
 subcutaneous solution LEVEMIR FLEXTOUCH (insulin detemir) subcutaneous solution pen-injector") LEVEMIR FLEXTOUCH (insulin detemir) subcutaneous solution pen-injector Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
LEVEMIR FLEXTOUCH (insulin detemir) subcutaneous solution pen-injector Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Initiation and Adjustment of Insulin Regimens for Type 2 Diabetes
 Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Injectable Therapies in Diabetes
 Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Injectable Therapies in Diabetes Diabetes Specialist Nurse Joyce Robson Learning Outcomes Think about the place of injectible therapies in diabetes Insulin therapy GLP1 antagonists Consider commonly used
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
associated with serious complications, but reduce occurrences with preventive measures
 Wk 9. Management of Clients with Diabetes Mellitus 1. Diabetes Mellitus body s inability to metabolize carbohydrates, fats, proteins hyperglycemia associated with serious complications, but reduce occurrences
Wk 9. Management of Clients with Diabetes Mellitus 1. Diabetes Mellitus body s inability to metabolize carbohydrates, fats, proteins hyperglycemia associated with serious complications, but reduce occurrences
9/16/2013. No Conflict of Interest to Disclose
 Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Insulin Pump Therapy in children. Prof. Abdulmoein Al-Agha, FRCPCH(UK)
") Insulin Pump Therapy in children Prof. Abdulmoein Al-Agha, FRCPCH(UK) aagha@kau.edu.sa Highlights Evolution of insulin pump Pumps mimics Pancreas Goals of diabetes care What lowers HbA1c Criteria for selection
Insulin Pump Therapy in children Prof. Abdulmoein Al-Agha, FRCPCH(UK) aagha@kau.edu.sa Highlights Evolution of insulin pump Pumps mimics Pancreas Goals of diabetes care What lowers HbA1c Criteria for selection
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins. Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP
 These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
Diabetes Medical Management Plan
 Diabetes Medical Management Plan 1 School District: School: School Year: Grade: Student Name: DOB: Provider Name: Phone #: Fax #: Blood Glucose Monitoring at School Blood Glucose Target Range: - mg/dl
Diabetes Medical Management Plan 1 School District: School: School Year: Grade: Student Name: DOB: Provider Name: Phone #: Fax #: Blood Glucose Monitoring at School Blood Glucose Target Range: - mg/dl
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Monitor patient s ability to self-administer insulin. (To evaluate safe administration of drug.)
") Nursing Process Focus: Patients Receiving Regular Insulin (Humulin, Novolin) Assessment Prior to administration: Assess any patient allergies. Older forms of insulin are made from beef and pork and may
Nursing Process Focus: Patients Receiving Regular Insulin (Humulin, Novolin) Assessment Prior to administration: Assess any patient allergies. Older forms of insulin are made from beef and pork and may
SCHOOL HEALTH PLAN: DIABETES
 BRANDON FLORENCE MCLAURIN NORTHWEST PELAHATCHIE RANKIN COUNTY SCHOOL DISTRICT GREAT TO BEST PISGAH PUCKETT RICHLAND RANKIN COUNTY SCHOOL DISTRICT SCHOOL HEALTH PLAN: DIABETES of Plan: Effective s: This
BRANDON FLORENCE MCLAURIN NORTHWEST PELAHATCHIE RANKIN COUNTY SCHOOL DISTRICT GREAT TO BEST PISGAH PUCKETT RICHLAND RANKIN COUNTY SCHOOL DISTRICT SCHOOL HEALTH PLAN: DIABETES of Plan: Effective s: This
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
8/13/2016. Insulin Basics. Rapid-Acting Insulin Analogs. Current Insulin Products and Pens. Basal Insulin Analogs. History of Insulin Therapy
 Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Diabetes Medical Management Plan
 SCHOOL DISTRICT OF LEE COUNTY HEALTH SERVICES Print Form Date of Plan Diabetes Medical Management Plan This plan should be completed by the student's personal health care team and parents/guardian. It
SCHOOL DISTRICT OF LEE COUNTY HEALTH SERVICES Print Form Date of Plan Diabetes Medical Management Plan This plan should be completed by the student's personal health care team and parents/guardian. It
Insulin therapy in gestational diabetes mellitus
 Insulin therapy in gestational diabetes mellitus October 15, 2015 Kyung-Soo Kim Division of Endocrinology & Metabolism, Department of Internal Medicine, CHA Bundang Medical Center, CHA University Contents
Insulin therapy in gestational diabetes mellitus October 15, 2015 Kyung-Soo Kim Division of Endocrinology & Metabolism, Department of Internal Medicine, CHA Bundang Medical Center, CHA University Contents
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection
 New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Diabetes Medical Management Plan
 MADISON CONSOLIDATED SCHOOLS Diabetes Medical Management Plan Date of Plan: Effective Dates : The student s personal health care team and parents/guardian should complete this plan. It should be reviewed
MADISON CONSOLIDATED SCHOOLS Diabetes Medical Management Plan Date of Plan: Effective Dates : The student s personal health care team and parents/guardian should complete this plan. It should be reviewed
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC)
") BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
TO BE COMPLETED BY LICENSED HEALTH CARE PROFESSIONAL
 PART I OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN Student School Date of Birth Date of Diagnosis Grade/ Teacher Physical
PART I OFFICE OF CATHOLIC SCHOOLS DIOCESE OF ARLINGTON DIABETES MEDICAL MANAGEMENT PLAN Page 1 of 5 TO BE COMPLETED BY PARENT OR GUARDIAN Student School Date of Birth Date of Diagnosis Grade/ Teacher Physical
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
Technology for Diabetes: 101 Basic Rules of the Road. Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE
 Technology for Diabetes: 101 Basic Rules of the Road Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE Quick Pump Facts! o Constant insulin supply o Pager-sized mini-computer worn
Technology for Diabetes: 101 Basic Rules of the Road Karen Hamon RN, BSN, CDE Stephen Stone MD, FAAP Neil H. White, MD, CDE Quick Pump Facts! o Constant insulin supply o Pager-sized mini-computer worn
Glycemic Control IU Health Diabetes Centers
 Glycemic Control IU Health Diabetes Centers Central Nursing Orientation 3/10/2014 1 Objectives Identify laboratory results that diagnosis diabetes and reflect glycemic control Describe glycemic control
Glycemic Control IU Health Diabetes Centers Central Nursing Orientation 3/10/2014 1 Objectives Identify laboratory results that diagnosis diabetes and reflect glycemic control Describe glycemic control
4/2/2018. Human U-500 insulin Learning Objectives. Dr. Ken Cathcart FACE
 Human U-500 insulin 2018 Dr. Ken Cathcart FACE Learning Objectives Participants will be able to identify when it is appropriate to use U500 insulin Participants will be able to state how to determine a
Human U-500 insulin 2018 Dr. Ken Cathcart FACE Learning Objectives Participants will be able to identify when it is appropriate to use U500 insulin Participants will be able to state how to determine a
Short-acting insulins. Biphasic insulins. Intermediate- and long-acting insulins
 Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
Recommended Insulin Products This guideline states the Gloucestershire Joint Formulary recommended, first choice insulin products. The intention is to support the choice of treatment for new patients,
What I need to know about Diabetes Medicines
 What I need to know about Diabetes Medicines What do diabetes medicines do? Over time, high levels of blood glucose, also called blood sugar, can can cause health problems. These problems include heart
What I need to know about Diabetes Medicines What do diabetes medicines do? Over time, high levels of blood glucose, also called blood sugar, can can cause health problems. These problems include heart
Types of insulin. Your blood glucose levels. Types of insulin
 Different types of insulin are available for people with diabetes. If you need insulin, you and your diabetes team will look at the options and decide which type fits best with your lifestyle and blood
Different types of insulin are available for people with diabetes. If you need insulin, you and your diabetes team will look at the options and decide which type fits best with your lifestyle and blood
Important Stuff. Basal Bolus What Adjustments? Pt weighs 80kg
 Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Role of Academia In Achieving Targets in Diabetes Care
 Role of Academia In Achieving Targets in Diabetes Care Disclosures Member of NovoNordisk, Lilly, Metavention, Sanofi, and Janssen Diabetes Advisory Boards Role of Academia in Discovering New Treatments
Role of Academia In Achieving Targets in Diabetes Care Disclosures Member of NovoNordisk, Lilly, Metavention, Sanofi, and Janssen Diabetes Advisory Boards Role of Academia in Discovering New Treatments
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Much of what is written on insulin pump use is biased in favor of insulin pump manufacturers.
 CHAPTER 2: ADVANTAGES AND DISADVANTAGES OF INSULIN PUMPS H. Peter Chase, MD Much of what is written on insulin pump use is biased in favor of insulin pump manufacturers. There are many people who are able
CHAPTER 2: ADVANTAGES AND DISADVANTAGES OF INSULIN PUMPS H. Peter Chase, MD Much of what is written on insulin pump use is biased in favor of insulin pump manufacturers. There are many people who are able
LET S TALK INSULIN THE BASICS
 LET S TALK INSULIN THE BASICS AUTHOR S DISCLOSURES Contracted for program development for Lifescan Canada Speaker for Lifescan, Lilly, BI, Consultant for Lilly, Janssen, Novo Nordisk, Lifescan Canada OBJECTIVES
LET S TALK INSULIN THE BASICS AUTHOR S DISCLOSURES Contracted for program development for Lifescan Canada Speaker for Lifescan, Lilly, BI, Consultant for Lilly, Janssen, Novo Nordisk, Lifescan Canada OBJECTIVES
Advances in Diabetes Care Technologies
 1979 Advances in Diabetes Care Technologies 2015 Introduction Insulin pump use: ~ 20% - 30% of patients with T1DM < 1% of insulin-treated patients with T2DM 2007 FDA estimates ~375,000 insulin pumps for
1979 Advances in Diabetes Care Technologies 2015 Introduction Insulin pump use: ~ 20% - 30% of patients with T1DM < 1% of insulin-treated patients with T2DM 2007 FDA estimates ~375,000 insulin pumps for
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Afrezza Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Afrezza (human insulin) Prime Therapeutics will review Prior Authorization requests Prior Authorization
Afrezza Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Afrezza (human insulin) Prime Therapeutics will review Prior Authorization requests Prior Authorization
Insulin Management. By Susan Henry Diabetes Specialist Nurse
 Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Drug Effectiveness Review Project Summary Report Long acting Insulins
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Converting lantus to humalog 75 25
 P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations
 Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations This is a long and important document. It lists the steps for starting insulin pump therapy at the Calgary Diabetes Centre. It
Calgary Diabetes Centre Insulin Pump Therapy: Preparation and Expectations This is a long and important document. It lists the steps for starting insulin pump therapy at the Calgary Diabetes Centre. It
The Growing Future of Diabetes: Insulin Pump Therapy in Type 1 and 2 Diabetes
 The Growing Future of Diabetes: Insulin Pump Therapy in Type 1 and 2 Diabetes Sarah Dombrowski, PharmD, BCACP Pennsylvania Pharmacists Association 10/20/18 1 Objectives At the completion of this activity,
The Growing Future of Diabetes: Insulin Pump Therapy in Type 1 and 2 Diabetes Sarah Dombrowski, PharmD, BCACP Pennsylvania Pharmacists Association 10/20/18 1 Objectives At the completion of this activity,
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
When and how to start insulin therapy in type 2 diabetes
 When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
When and how to start insulin therapy in type 2 diabetes Anne Kilvert MD, FRCP Most patients with type 2 diabetes will eventually require insulin due to the progressive decline in betacell function. Dr
Insulin Pump An information session to help you decide if you are ready to use an insulin pump.
 Insulin Pump An information session to help you decide if you are ready to use an insulin pump. Welcome Welcome to the insulin pump information session. We hope this session helps you to decide whether
Insulin Pump An information session to help you decide if you are ready to use an insulin pump. Welcome Welcome to the insulin pump information session. We hope this session helps you to decide whether
Providing Stability to an Unstable Disease
 Basal Insulin Therapy Providing Stability to an Unstable Disease Thomas A. Hughes, M.D. Professor of Medicine - Retired Division of Endocrinology, Metabolism, and Diabetes University of Tennessee Health
Basal Insulin Therapy Providing Stability to an Unstable Disease Thomas A. Hughes, M.D. Professor of Medicine - Retired Division of Endocrinology, Metabolism, and Diabetes University of Tennessee Health
Topics in Inpatient Glycemic Control
 Topics in Inpatient Glycemic Control Jane Jeffrie Seley DNP MPH MSN GNP BC-ADM CDE CDTC FAADE FAAN Diabetes Nurse Practitioner Program Manager, Inpatient Glycemic Control Program NewYork-Presbyterian/
Topics in Inpatient Glycemic Control Jane Jeffrie Seley DNP MPH MSN GNP BC-ADM CDE CDTC FAADE FAAN Diabetes Nurse Practitioner Program Manager, Inpatient Glycemic Control Program NewYork-Presbyterian/
Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies
 Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies Leigh Briscoe-Dwyer, PharmD, BCPS, FASHP Chief Pharmacy and Medication Safety Officer North Shore Long Island Jewish Health
Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies Leigh Briscoe-Dwyer, PharmD, BCPS, FASHP Chief Pharmacy and Medication Safety Officer North Shore Long Island Jewish Health
Vishwanath Pattan Endocrinology Wyoming Medical Center
 Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Vishwanath Pattan Endocrinology Wyoming Medical Center Disclosure Holdings in Tandem Non for this Training Introduction In the United States, 5 to 6 percent of pregnancies almost 250,000 women are affected
Introduction. Guidelines for patient involvement in the administration of insulin under supervision in hospital (Adult patients)
") Guidelines for patient involvement in the administration of insulin under supervision in hospital (Adult patients) Introduction This guideline is designed to provide a framework for patients to administer
Guidelines for patient involvement in the administration of insulin under supervision in hospital (Adult patients) Introduction This guideline is designed to provide a framework for patients to administer
Basal-Bolus Insulin Therapy. Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January
 Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Patient Education Handouts Table of Contents 2013 General Diabetes Information Monitoring and Management
 Patient Education Handouts Table of Contents 2013 We have highlighted some handouts that may be helpful for the new patient. Select the ones that are most useful to you. Avoid overwhelming the patient
Patient Education Handouts Table of Contents 2013 We have highlighted some handouts that may be helpful for the new patient. Select the ones that are most useful to you. Avoid overwhelming the patient
What do you need to know before you go home?
 What do you need to know before you go home? What is Insulin Types of Insulin Injection Sites How to Inject Insulin Correctly Low Blood Sugar and Treatment Sick Day Management After leaving the Hospital:
What do you need to know before you go home? What is Insulin Types of Insulin Injection Sites How to Inject Insulin Correctly Low Blood Sugar and Treatment Sick Day Management After leaving the Hospital:
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
In-hospital management of diabetes
 Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes Medical Management Plan
 Date of Plan: Diabetes Medical Management Plan Effective Dates: This plan should be completed by the student's personal health care team and parents/guardian. It should be reviewed with relevant school
Date of Plan: Diabetes Medical Management Plan Effective Dates: This plan should be completed by the student's personal health care team and parents/guardian. It should be reviewed with relevant school
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight