Donation after Brain-Stem Death DBD
|
|
|
- Geraldine Copeland
- 6 years ago
- Views:
Transcription



1 Donation after Brain-Stem Death DBD Dr Sri Nagaiyan Dr Dale Gardiner Dr Gerlinde Mandersloot 17 th May
2 Session Objectives Present regional data for DBD Understand that DBD gives better organs than DCD Increase rate of neurological confirmation of death by increasing confidence in the Diagnosis of Death Increase quality of DBD organs adoption of extended care bundle and compliance with the six early interventions in donor optimisation collaboration in Scout pilot 2
3 MIDLANDS Regional Data Dr Sri Nagaiyan North Staffordshire CLOD 3
4 Donation after Brain Death (DBD) Mechanically ventilated patient where death has been confirmed using neurological criteria. 85 donors ( ) Kidneys Liver Pancreas Lungs Heart Small Intestine 26.9% increase (last five years) MIDLANDS

5 Donations over time: Midlands Team 87.5 % MIDLANDS 26.9% 400% 5
6 Donations over time: Midlands Team MIDLANDS 26.9% 6





7 DCD DBD kidneys intestine lungs pancreas liver heart
8 MIDLANDS
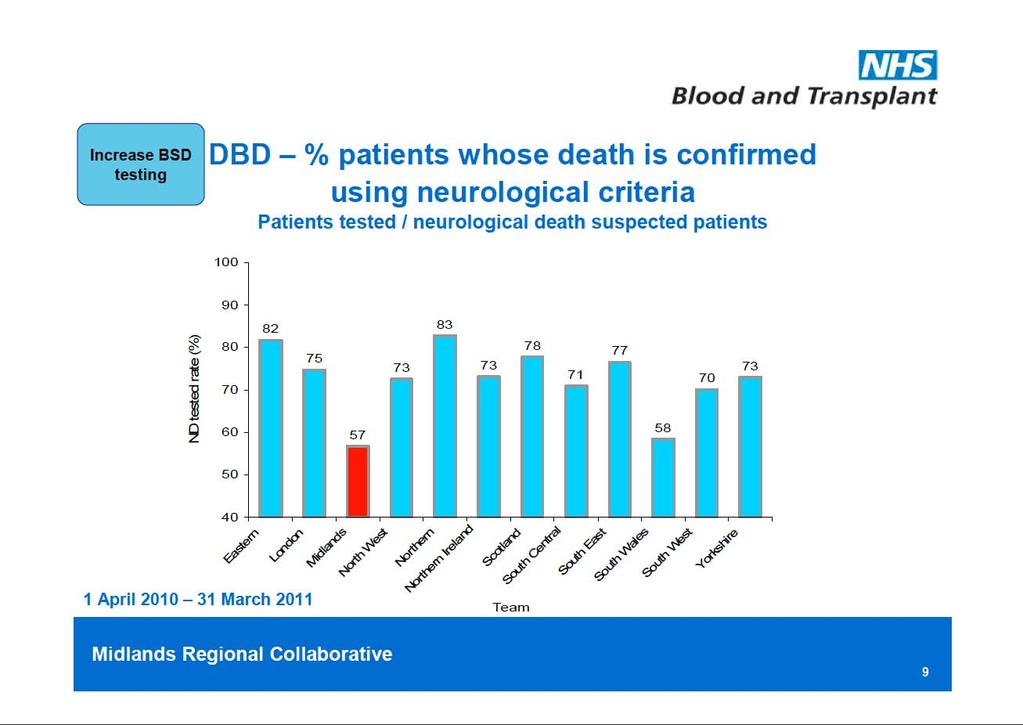
9 MIDLANDS DBD- Neurological death testing rate 100 2nd ND tested (%) 20 0 Eastern London Midlands North West Northern Northern Ireland Scotland South Central South East South Wales South West Yorkshire Team 1 April 2012 to 30 September 2012, data as at 4 October National rate 9
10 Ireland Scotland South Central South East South Wales South West Yorkshire MIDLANDS Tied 5th with 3 others National rate ND tested (%) 20 0 DBD- Neurological death testing rate Team Eastern London Midlands North West Northern Northern 1 April 2012 to 31 March 2013, data as at 4 April
11 DBD- Midlands Neurological death testing rate ND tested (%) Number of neurological death suspected patients Walsall (hidden behind 9) 2 South Warwickshire 3 Mid Staffordshire 4 North Staffordshire 5 Burton 6 Sherwood Forest 7 Coventry 8 Wolverhampton 9 George Eliot 10 The Dudley Group 11 Birmingham Children s 12 Heart of England 13 QE 14 Derby 15 Leicester 16 Worcestershire 17 Nottingham 18 City & Sandwell 19 Shrewsbury and Telford 1 April 2012 to 31 March 2013, data as at 4 April


12 Mean no. of organs donated per DBD donor Tied 3 rd MIDLANDS Northern (1 st ) : Every 5 donors save 1 more life than we do 1 April 2012 to 31 March 2013, data as at 4 April


13 Diagnosis of brain stem death years on 2008 Dr Dale Gardiner Adult Intensive Care Consultant, Nottingham Midlands, Clinical Lead for Organ Donation Member of the UK Donation Ethics Committee 13


14 not inventors. We are explorers
15 15
16 16




17 Brain death: Discovered not Invented (by intensive care) 17



18 1964, Keith Simpson there is life so long as circulation of oxygenated blood is maintained to live brainstem centres 18

19 1976 (clarified 1979) UK Criteria for Diagnosing Death using Neurological Criteria Published. 19





20 Rene Laennec 1819 Eugene Bouchut UK Criteria for Circulatory Criteria published for the 1 st time. 5 minutes. 20
21 UK Definition of Death irreversible loss of the capacity for consciousness, combined with irreversible loss of the capacity to breathe 2008 therefore irreversible cessation of the integrative function of the brain stem equates with the death of the individual. 21

22 UK Definition of Death irreversible loss of the capacity for consciousness, combined with irreversible loss of the capacity to breathe All human death is anatomically located to the brain therefore irreversible cessation of the integrative function of the brain stem equates with the death of the individual. 22


23 1 death : 3 sets of criteria Neurological Criteria Circulatory Criteria DEATH Irreversible loss of the capacity for consciousness Irreversible loss of the capacity to breathe Somatic Criteria
24 Dx Death using Neurological 1. An established aetiology capable of causing structural damage to the brain which has led to the irreversible loss of the capacity for consciousness combined with the irreversible loss of the capacity to breathe. Criteria DEATH Irreversible loss of the capacity for consciousness Irreversible loss of the capacity to breathe Cause tells you irreversibility, based on the natural history of the disease Cause tells you how long you should observe before testing: Typical Hypoxia Atypical > 6 hours 24 hours? longer 24

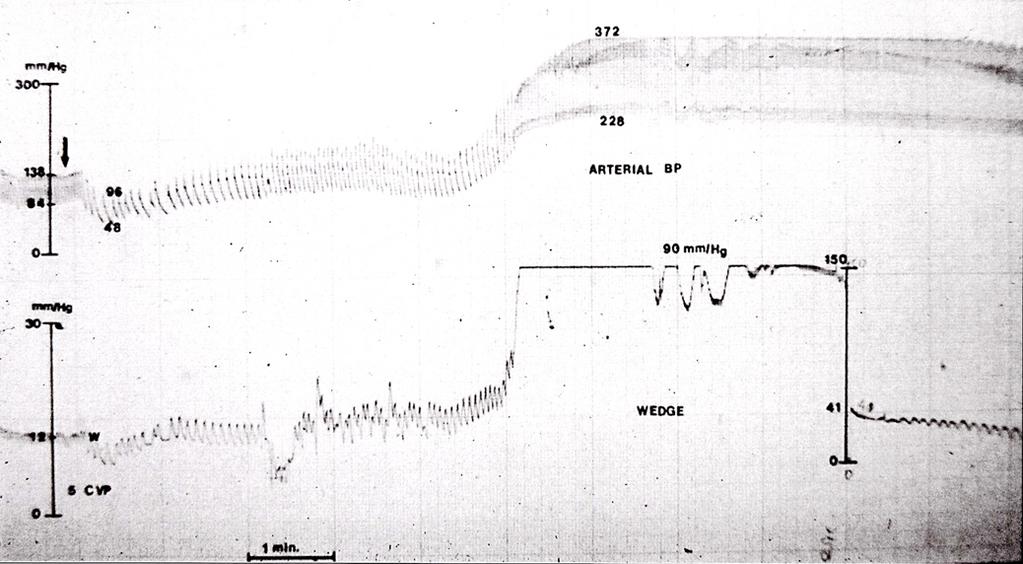
25
26 > patients 10 years 37 years

27 D. Alan Shewmon, MD

28 Although we were unable to restore his consciousness or spontaneous breathing, the boy lived several more years. (page 195)

29
30 Dx Death using Neurological 1. An established aetiology capable of causing structural damage to the brain which has led to the irreversible loss of the capacity for consciousness combined with the irreversible loss of the capacity to breathe. Criteria DEATH Irreversible loss of the capacity for consciousness Irreversible loss of the capacity to breathe 2. An exclusion of reversible conditions capable of mimicking or confounding the diagnosis of death using neurological criteria. 30
31 Dx Death using Neurological Clinical judgement essential Impossible to create rules covering every situation Difficulties mainly with thiopentone and midazolam Criteria 2. An exclusion of reversible conditions capable of mimicking or confounding the diagnosis of death using neurological criteria. Plasma concentrations not good predictors of effect Use of antagonists DEATH Irreversible loss of the capacity for consciousness Irreversible loss of the capacity to breathe 31
32 Dx Death using Neurological 1. An established aetiology capable of causing structural damage to the brain which has led to the irreversible loss of the capacity for consciousness combined with the irreversible loss of the capacity to breathe. Criteria 2. DEATH Irreversible loss of the capacity for consciousness Irreversible loss of the capacity to breathe An exclusion of reversible conditions capable of mimicking or confounding the diagnosis of death using neurological criteria. 3. A clinical examination of the patient, which demonstrates profound coma, apnoea and absent brainstem reflexes. 32
 Oculovestibular (III, VI, VIII) Oculocephalic Paediatric Suck")

33 Brain stem reflexes Pupils (II, III) Corneals (V, VII) Pain (V, VII) Gag (IX, X) Cough (IX, X) Oculovestibular (III, VI, VIII) Oculocephalic Paediatric Suck Consciousness Ascending reticular activity system Breathe Medulla Oblongata Wijdicks EFM. The diagnosis of brain death. N Engl J Med 2001;344: AoMRC (2008) 33

34 Apnoea Test Starting: paco 2 > 6.0 Kpa ph <7.4 Stopping: 5 minutes observation paco 2 rise > 0.5 KPa Recommended method: After pre oxygenation, disconnect the patient from the ventilator and administer oxygen via a suction catheter in the endotracheal tube at a rate of >6 L/minute. If oxygenation is a problem, consider the use of a CPAP circuit (eg Mapleson B). The apnoea test is performed only twice in total. 34
35 Dx Death using Neurological 1. An established aetiology capable of causing structural damage to the brain which has led to the irreversible loss of the capacity for consciousness combined with the irreversible loss of the capacity to breathe. Criteria 2. DEATH Irreversible loss of the capacity for consciousness Irreversible loss of the capacity to breathe An exclusion of reversible conditions capable of mimicking or confounding the diagnosis of death using neurological criteria. 3. A clinical examination of the patient, which demonstrates profound coma, apnoea and absent brainstem reflexes. In 2012,1238 tests performed, death confirmed in 1220 =
 A Code of Practice for the Diagnosis and Confirmation")

36 Testing for Brain stem Death This form is consistent with and should be used in conjunction with, the AoMRC (2008) A Code of Practice for the Diagnosis and Confirmation of Death and has been endorsed for use by the following institutions: Faculty of Intensive Care Medicine, Intensive Care Society and the National Organ Donation Committee. Abbreviated Full 36
37 37
38 WHY TEST?
39 WHY TEST? 1. To eliminate all possible doubt regarding survivability 2. To confirm diagnosis for families 3. To protect doctors in cases subject to medico legal scrutiny 4. To provide choice regarding organ donation

40 diagnosis decision
41 Brainstem death in the

42 TWO TESTS or ONE? 2008 Dr A performs Dr B observes SWAP Dr B performs Dr A observes = 2 TESTS (regardless of organ donation) Legal support from case law & Bolam & Bolithio tests
43 TWO TESTS or ONE? 2008 Dr A performs Dr B observes SWAP Dr B performs Dr A observes = 2 TESTS (regardless of organ donation) Legal support from case law & Bolam & Bolithio tests
44 TWO TESTS or ONE? 2008 Dr A performs Dr B observes SWAP ALIVE Test 1 Time of Death Dr B performs Dr A observes ALIVE = 2 TESTS (regardless of organ donation) Legal support from case law & Bolam & Bolithio tests Test 2 DECEASED


45 Lesson 1





46 Lesson 2

47 Lesson 3 Take your time Slow down (minimum 6 hours) Don t over-read coning on CT Atypical presentation = wait Hypoxic brain injury >24 hours

48 Lesson 4 Induced hypothermia has unpredictable consequences See Lesson 3 Advice: warm to normothermia and then wait 24 hours

49 Lesson 5 NO EEG

50 Lesson 6 Start with Lesson 2 = use your brain and examine your patient 1. Clinical brain death + NO flow = Death 2. Clinical brain death + flow = Wait See Lesson 3 = take your time and ask Is reversibility possible?


51 Gardiner, Shemie, Manara & Opdam International Perspective on the Diagnosis of Death Br J Anaesthesia Supplement January 2012 Username: Password: Dale Gardiner
52 Optimising the brainstem dead donor Dr Gerlinde Mandersloot National Clinical Lead - Donor Optimisation Dr Gerlinde Mandersloot 20 th April
53
54
55 Donor optimisation Ameliorate systemic effects of brain stem death Why? Increase number of donors Increase number of organs per donor Increase quality of organs Who takes responsibility? ICU staff: medical and nursing SN-ODs Retrieval teams Scout Cardio-thoracic teams 55

56 Collateral damage Hormonal Diabetes insipidus Hypovolaemia Hypernatraemia T3 / T4 reduces ACTH Blood glucose Hypothermia 56
57 Incidence of organ involvement Hypotension 81% Diabetes insipidus 65% DIC 28% Cardiac dysrrhythmias 25% Pulmonary oedema 18% Metabolic acidosis 11% J Heart Lung Transplantation 2004 (suppl) 57
58 58
59 Evidence Totsuka Transplant Proc. 2000; 32; High sodium in liver donor doubles graft loss Rosendale Transplantation (4): Protocol increased organs per donor 3.1 to 3.8. Increased probability of transplant. Snell J Heart Lung Transplant 2008;27: % of Australian lung donations used for transplant vs. 13% in UK 59
60 Principles Ameliorate systemic effects of brain stem death Why? Increase number of donors Increase number of organs per donor Increase quality of organs Who takes responsibility? ICU staff: medical and nursing SN-ODs Retrieval teams Scout : who are they attached to? Cardio-thoracic teams Abdominal teams Free standing 60
61 What do we aim for? General stability Examples of target values MAP: mm Hg Heart rate: / min SR CI: > 2.1 l/min/m 2 Guidelines Australian Canadian Map of Medicine ICS NHSBT 61
62 Cardiovascular management Summary of cardio vascular target values MAP: mm Hg CVP: 4 10 mm Hg Heart rate: /min SR CI: > 2.1 l/min/m 2 (can be higher, be aware of myocardial stunning) Filling targets: no good evidence for any specific targets, depends on device SvO 2 > 60% SVRI target Secondary target Dehydration temptation to maintain MAP with vasopressors rather than filling 62
63 Respiratory management Recruitment manoeuvre Post BSD testing: apnoea test resulting in atelectasis After suctioning / disconnection When SpO 2 drops / FiO 2 increases Lung protective ventilation: 4 8 ml/kg ideal body weight Permissive hypercapnia with ph > 7.25 Optimum PEEP (5 10 cm H 2 O) and FiO 2 (aim for < 0.4 as able) Head up positioning (30-45 ) Suctioning, physiotherapy as required Antibiotics for purulent secretions: local microbiology surveillance Avoid over-hydration 63
64 Managing Diabetes insipidus Very common occurrence Pathophysiology Posterior pituitary failure Polyuria: output > 4ml/kg/h Dehydration with Na + Usually at least partially addressed with stabilisation for BSD testing Treatment: Fluids Vasopressin DDAVP Aim for u-output ml / kg / h 64
65 Hormonal treatment Vasopressin Reduction in other vaso-active drugs Dose: 1 4 units/h (can start with boluses of 1 unit at a time) Liothyronine (T3) No clear evidence yet for either use or not May add haemodynamic stability in very unstable donor Dose: 3 units/h, sometimes bolus of 4 units asked for by retrieval team Methylprednisolone in all cases Dose: 15 mg/kg up to 1g Insulin At least 1 unit/h (Occasionally may need to add glucose infusion) Tight glycaemic control (4-10 mmol/l) 65
66 Haematological management DIC seen occasionally as direct consequence of BSD May require correcting prior to BSD testing if bleeding Hb > 8 g/dl (~ 10 g/dl traditionally advocated) (even > 7g/dl?) No evidence on harm with lower Hb, but some evidence of harm with blood transfusions and organ function post transplant Where Hb borderline, ensure blood available for retrieval procedure: local protocols and antibodies will determine whether G&S only, or units to be cross matched Use of clotting factors Only where bleeding is an issue Monitor clotting status Use local hospital protocol Retrieval procedure may require additional products 66
67 General measures Maintain normothermia (active warming may be required) Thrombo-embolism prophylaxis Stockings Sequential compression devices LMWH Positioning Head-up Side to side Attention to cuff pressures and leaks to prevent aspiration Continue NG feeding (may be reduced/ stopped for bowel transplant) Antibiotics according to sensitivities or empirical according to Trust guidelines 67
68 Monitoring optimisation Implementation: use of care bundle Adherence easy to monitor Audit first 5 priorities Results of optimisation evaluated Number of organs retrieved Increase in cardiothoracic organs retrieved Quality of organs: organ function in recipients Delayed graft function Quality: biomarkers Duration of graft function: long term project 68
69
Donation after Brain-Stem Death DBD
 Donation after Brain-Stem Death DBD Dr Peter Hall Dr Dale Gardiner Dr Gerlinde Mandersloot 22 nd May 2013 1 YORKSHIRE Regional Data Dr Peter Hall CLOD Calderdale and Huddersfield NHS Trust 2 Session Objectives
Donation after Brain-Stem Death DBD Dr Peter Hall Dr Dale Gardiner Dr Gerlinde Mandersloot 22 nd May 2013 1 YORKSHIRE Regional Data Dr Peter Hall CLOD Calderdale and Huddersfield NHS Trust 2 Session Objectives
Using Service Improvement Methodology to improve DCD referral Rates Anne-Marie Hill & Ben Cole
 Using Service Improvement Methodology to improve DCD referral Rates Anne-Marie Hill & Ben Cole Midlands DCD referral rate 1 Walsall Healthcare NHS Trust 2 South Warwickshire NHS Foundation Trust 3 University
Using Service Improvement Methodology to improve DCD referral Rates Anne-Marie Hill & Ben Cole Midlands DCD referral rate 1 Walsall Healthcare NHS Trust 2 South Warwickshire NHS Foundation Trust 3 University
Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010
 Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010 The brainstem: Midbrain, pons, medulla Consciousness Cardiovascular and respiratory regulation Sleep- wake cycle Integration of
Dr Richard Pugh Consultant Anaesthetics/ Intensive Care Medicine May 2010 The brainstem: Midbrain, pons, medulla Consciousness Cardiovascular and respiratory regulation Sleep- wake cycle Integration of
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol
 Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Organ Donation Activity
 3 Organ Donation Activity Organ Donation Activity Key messages There has been a 11% increase in deceased donors (to 1,574) and a
3 Organ Donation Activity Organ Donation Activity Key messages There has been a 11% increase in deceased donors (to 1,574) and a
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities. Report for 2016/2017 (1 April March 2017)
 communities. Report for 2016/2017 (1 April March 2017)") Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 6/7 ( April March 7) CONTENTS EXECUTIVE SUMMARY... INTRODUCTION... ORGAN DONOR REGISTER (ODR)...
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 6/7 ( April March 7) CONTENTS EXECUTIVE SUMMARY... INTRODUCTION... ORGAN DONOR REGISTER (ODR)...
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities. Report for 2017/2018 (1 April March 2018)
 communities. Report for 2017/2018 (1 April March 2018)") Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 07/0 ( April 0 March 0) CONTENTS EXECUTIVE SUMMARY... INTRODUCTION... ORGAN DONOR REGISTER (ODR)...
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 07/0 ( April 0 March 0) CONTENTS EXECUTIVE SUMMARY... INTRODUCTION... ORGAN DONOR REGISTER (ODR)...
Form for the Diagnosis of Death using Neurological Criteria in Children >2 months to <18 years {full guidance version}
 This form is consistent with and should be used in conjunction with, the AoMRC (2008) A Code of Practice for the Diagnosis and Confirmation of Death 1 and has been endorsed for use by the following institutions:
This form is consistent with and should be used in conjunction with, the AoMRC (2008) A Code of Practice for the Diagnosis and Confirmation of Death 1 and has been endorsed for use by the following institutions:
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities. Report for 2015/2016 (1 April March 2016)
 communities. Report for 2015/2016 (1 April March 2016)") Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 2015/2016 (1 April 2010 31 March 2016) INTRODUCTION This report provides information related to
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 2015/2016 (1 April 2010 31 March 2016) INTRODUCTION This report provides information related to
GUIDELINE for the diagnosis and confirmation of death within Adult Critical Care
 Guideline for the diagnosis and confirmation of death within adult critical care 1. Introduction Death occurs when there is permanent loss of capacity for consciousness and loss of all brainstem functions.
Guideline for the diagnosis and confirmation of death within adult critical care 1. Introduction Death occurs when there is permanent loss of capacity for consciousness and loss of all brainstem functions.
Experiences as a Donation Support Physician. Dead or not Dead? Are the following statements consistent with neurological
 Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Brain Death Determination: Outline. Definition. Brain Death Determination. Brain Death Determination. No conflict of interest
 No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
Organ Donation and Transplantation in Wales
 Organ Donation and Transplantation in Wales How are we doing? Cornea: 119 Lung: 9 Liver: 37 Heart: 12 Kidneys: 127 Pancreas: 4 Small bowel: 0 Number of Transplants in Wales in 2016/17 Report 2016/17 Referrals
Organ Donation and Transplantation in Wales How are we doing? Cornea: 119 Lung: 9 Liver: 37 Heart: 12 Kidneys: 127 Pancreas: 4 Small bowel: 0 Number of Transplants in Wales in 2016/17 Report 2016/17 Referrals
Overview of Organ Donation and Transplantation
 2 Overview of Organ Donation and Transplantation Overview of Organ Donation and Transplantation A summary of organ donation and transplantation activity in the UK during the financial year from April 207
2 Overview of Organ Donation and Transplantation Overview of Organ Donation and Transplantation A summary of organ donation and transplantation activity in the UK during the financial year from April 207
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL
 YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
Organ Donation and Transplantation. Activity Report 2017/18
 Organ Donation and Transplantation Activity Report 2017/18 Preface This report has been produced by Statistics and Clinical Studies, NHS Blood and Transplant. All figures quoted in this report are as reported
Organ Donation and Transplantation Activity Report 2017/18 Preface This report has been produced by Statistics and Clinical Studies, NHS Blood and Transplant. All figures quoted in this report are as reported
Organ Donation and Transplantation. Activity Report 2015/16
 Organ Donation and Transplantation Activity Report 2015/16 Preface This report has been produced by Statistics and Clinical Studies, NHS Blood and Transplant. All figures quoted in this report are as reported
Organ Donation and Transplantation Activity Report 2015/16 Preface This report has been produced by Statistics and Clinical Studies, NHS Blood and Transplant. All figures quoted in this report are as reported
This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant.
 Preface This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report are as reported to NHS Blood and Transplant by 17 June 2012 for the UK
Preface This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report are as reported to NHS Blood and Transplant by 17 June 2012 for the UK
This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant.
 Preface This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report are as reported to NHS Blood and Transplant by 20 May 2013 for the UK
Preface This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report are as reported to NHS Blood and Transplant by 20 May 2013 for the UK
Faith Borunda, MSN-RN, CCRN, CPTC Senior Director of Regional Operations Southwest Transplant Alliance
 Faith Borunda, MSN-RN, CCRN, CPTC Senior Director of Regional Operations Southwest Transplant Alliance The Never -Ending Need 114,401 in the U.S. wait for a lifesaving transplant * United Network for Organ
Faith Borunda, MSN-RN, CCRN, CPTC Senior Director of Regional Operations Southwest Transplant Alliance The Never -Ending Need 114,401 in the U.S. wait for a lifesaving transplant * United Network for Organ
Neurological Determination of Death Adult
 Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
TRANSPLANT ACTIVITY IN THE UK
 Activity Report 2010/11 TRANSPLANT ACTIVITY IN THE UK www.nhsbt.nhs.uk PREFACE This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report
Activity Report 2010/11 TRANSPLANT ACTIVITY IN THE UK www.nhsbt.nhs.uk PREFACE This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report
DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010
 Chicago, Illinois PAGE: 1 of 7 DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010 Key Content Expert: Medical Center Ethics Committee in consultation with Chiefs of Service for Neurology
Chicago, Illinois PAGE: 1 of 7 DETERMINATION OF NEUROLOGIC DEATH IN ADULTS AND CHILDREN April 2010 Key Content Expert: Medical Center Ethics Committee in consultation with Chiefs of Service for Neurology
Policy No: Title: Determination of Death by Brain Criteria Department: PATIENT CARE. Originated: May 1992
 Title: Determination of Death by Brain Criteria Department: PATIENT CARE Policy No: Page 1 of 6 Revised: April 2009 Previous revisions: 9/96, 7/99, 7/07 Reviewed: August 2010 Originated: May 1992 I. POLICY:
Title: Determination of Death by Brain Criteria Department: PATIENT CARE Policy No: Page 1 of 6 Revised: April 2009 Previous revisions: 9/96, 7/99, 7/07 Reviewed: August 2010 Originated: May 1992 I. POLICY:
Organ Donation Annual Report. April 2011 to March 2012.
 Organ Donation Annual Report April 2011 to March 2012. Dr RM Kitson Consultant ITU and Anaesthesia Clinical Lead for Organ donation. Final report: 15 th May 2012. 1 Introduction Promotion of organ donation
Organ Donation Annual Report April 2011 to March 2012. Dr RM Kitson Consultant ITU and Anaesthesia Clinical Lead for Organ donation. Final report: 15 th May 2012. 1 Introduction Promotion of organ donation
The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033
 5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033 The number of deceased kidney donors increased by
5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033 The number of deceased kidney donors increased by
The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275
 5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275 The number of deceased kidney donors increased by 7%
5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275 The number of deceased kidney donors increased by 7%
Brain Stem Death & Management of the Organ Donor. Author: Tim Thiruchelvam & Quen Mok, May 2006 Updated by: Joe Brierley, 2007; Mehrengise Cooper 2013
 Disclaimer: Great Ormond Street Hospital Modular ITU Training Programme 2008-2009 The Great Ormond Street Paediatric Intensive Care Training Programme was developed in 2004 by the clinicians of that Institution,
Disclaimer: Great Ormond Street Hospital Modular ITU Training Programme 2008-2009 The Great Ormond Street Paediatric Intensive Care Training Programme was developed in 2004 by the clinicians of that Institution,
CHECKLIST FOR CLINICAL DIAGNOSIS OF BRAIN DEATH (ICSI 2010)
") ICSI A4 Guide MAY10 5/30/10 4:30 PM Page 7 CHECKLIST FOR CLINICAL DIAGNOSIS OF BRAIN DEATH (ICSI 2010) Name Address Date of birth Condition which led to irremediable brain damage: Onset of apnoeic coma;
ICSI A4 Guide MAY10 5/30/10 4:30 PM Page 7 CHECKLIST FOR CLINICAL DIAGNOSIS OF BRAIN DEATH (ICSI 2010) Name Address Date of birth Condition which led to irremediable brain damage: Onset of apnoeic coma;
The number of patients waiting on the pancreas transplant list fell by 7% during the year, to 252 at 31 March 2015
 6 Pancreas Activity Pancreas Activity Key messages The number of patients waiting on the pancreas transplant list fell by 7% during the year, to 252 at 31 March 2015 The number of pancreas donors after
6 Pancreas Activity Pancreas Activity Key messages The number of patients waiting on the pancreas transplant list fell by 7% during the year, to 252 at 31 March 2015 The number of pancreas donors after
Deceased Donation - Why Data? Damon C. Scales MD PhD
 Deceased Donation - Why Data? Damon C. Scales MD PhD Deceased Donation Why Data? Deceased Donation Why Data? Describe and explain variation Understand trends Performance measurement and comparisons Evaluate
Deceased Donation - Why Data? Damon C. Scales MD PhD Deceased Donation Why Data? Deceased Donation Why Data? Describe and explain variation Understand trends Performance measurement and comparisons Evaluate
Defining Death. Defining Death. Defining Death. Death at 50 & Organ Donation ORGAN TRANSPLANTATION. Dying (obvious) Death (not so obvious)
 Death (not so obvious)") Page 2 Page 4 Page 2 Page 4 Page 3 Page 5 Page 3 Page 5 Death at 50 & Organ Donation Dr. Mark Twite MA MB BChir FRCP Director of Congenital Cardiac Anesthesiology Associate Professor Department of Anesthesiology
Page 2 Page 4 Page 2 Page 4 Page 3 Page 5 Page 3 Page 5 Death at 50 & Organ Donation Dr. Mark Twite MA MB BChir FRCP Director of Congenital Cardiac Anesthesiology Associate Professor Department of Anesthesiology
Determination of Death
 Policy Legal Standard UTMB physicians will determine death in accordance with this policy which is based on Texas law and the practice parameters recommended by the American Academy of Neurology for adults
Policy Legal Standard UTMB physicians will determine death in accordance with this policy which is based on Texas law and the practice parameters recommended by the American Academy of Neurology for adults
The number of patients waiting on the pancreas transplant list fell by 1% during the year, to 224 at 31 March 2017
 6 Pancreas Activity Pancreas Activity Key messages The number of patients waiting on the pancreas transplant list fell by 1% during the year, to 224 at 31 March 2017 The number of pancreas donors after
6 Pancreas Activity Pancreas Activity Key messages The number of patients waiting on the pancreas transplant list fell by 1% during the year, to 224 at 31 March 2017 The number of pancreas donors after
Respiratory Care and Organ Donation
 Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
The number of patients on the active liver transplant list at 31 March 2017 was 530, a fall of 8% from 2016
 8 Liver Activity Liver Activity Key messages The number of patients on the active liver transplant list at 31 March 2017 was 530, a fall of 8% from 2016 The number of liver donors after brain death increased
8 Liver Activity Liver Activity Key messages The number of patients on the active liver transplant list at 31 March 2017 was 530, a fall of 8% from 2016 The number of liver donors after brain death increased
Transplant Activity in the UK
 Transplant Activity in the UK 2006-2007 This document has been produced by the Statistics and Audit Directorate. UK Transplant August 2007 Cover pictures: Members of Glamorgan County cricket team help
Transplant Activity in the UK 2006-2007 This document has been produced by the Statistics and Audit Directorate. UK Transplant August 2007 Cover pictures: Members of Glamorgan County cricket team help
Organ Donor Management Recommended Guidelines ADULT Brain Death (NDD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Neurological Determination of Death (NDD) has been performed by at least 2 licensed physicians Contact initiated with BC Transplant
Deceased donor. Solid organ transplantation
 Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Deceased donor Solid organ transplantation Deceased donor donation process 1. Potential donor detection 2. Brain death diagnosis 3. Donor management 4. Organ allocation 5. Organ retrieval Brain death Irreversible
Neurologic Determination of Death. Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015
 Neurologic Determination of Death Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015 Format Definition of Brain Death Historical Perspectives International consistency / inconsistency
Neurologic Determination of Death Ian Ball FRCPC Regional Medical Lead for Organ Donation October 26, 2015 Format Definition of Brain Death Historical Perspectives International consistency / inconsistency
The Determination of Brain Death. James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY
 The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine
 Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine") Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine 2016 MFMER 3583421-1 Brain Death or 2016 MFMER 3583421-2 Where
Brain Death Its History (and Some Controversies ) Eelco F.M. Wijdicks, MD, PhD Division of Critical Care Neurology Mayo College of Medicine 2016 MFMER 3583421-1 Brain Death or 2016 MFMER 3583421-2 Where
Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin
 Prepared by Reviewed By Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin Dr. M. Salim Khan Medical Director Approved by Dr. Manzoor H Qazi Chief Executive
Prepared by Reviewed By Name Signature Date IRB & Ethics Committee Dr. Ejaz A. Khan Chairman IRB & EC Dr. Shoukat Matabddin Dr. M. Salim Khan Medical Director Approved by Dr. Manzoor H Qazi Chief Executive
Hospital of the University of Pennsylvania POLICY MANUAL
 Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
GUIDELINES: The following guidelines for determining brain death in adults are accepted practice parameters of the American Academy of Neurology 1
 Page 1 of 5 PURPOSE: The purpose of this policy is to provide licensed staff and medical personnel with a guideline to determine when a patient on a ventilator demonstrates clinical brain death. POLICY
Page 1 of 5 PURPOSE: The purpose of this policy is to provide licensed staff and medical personnel with a guideline to determine when a patient on a ventilator demonstrates clinical brain death. POLICY
Deceased donation data in the UK. Paul Murphy National Clinical Lead for Organ Donation United Kingdom
 Deceased donation data in the UK Paul Murphy National Clinical Lead for Organ Donation United Kingdom Deceased donation data in the UK And the story behind it Paul Murphy National Clinical Lead for Organ
Deceased donation data in the UK Paul Murphy National Clinical Lead for Organ Donation United Kingdom Deceased donation data in the UK And the story behind it Paul Murphy National Clinical Lead for Organ
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria
 Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria A. SUBJECT: Guidelines for the Determination of Death: Including Death by Neurologic Criteria B. POLICY: The Medical
Sample Guidelines for the Determination of Death: Including Death by Neurologic Criteria A. SUBJECT: Guidelines for the Determination of Death: Including Death by Neurologic Criteria B. POLICY: The Medical
First Person Consent Uniform Anatomical Gift Act of 1968
 Andrew Wilson, Medicolegal Death Investigator Not-for-profit Organ Procurement Organization (OPO) & Tissue Recovery Agency Regulated by Centers for Medicaid and Medicare Services (CMS) and FDA Offices
Andrew Wilson, Medicolegal Death Investigator Not-for-profit Organ Procurement Organization (OPO) & Tissue Recovery Agency Regulated by Centers for Medicaid and Medicare Services (CMS) and FDA Offices
Med 536 Communicating About Prognosis Workshop. Case 2
 Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Post Resuscitation (ROSC) Care
 Care") Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Standard Operating Procedure 2.10 Post Resuscitation (ROSC) Care Position Responsible: Medical Director Approved: Clinical Governance Committee Related Documents: This document is the intellectual property
Donation After Circulatory Death From Adults to Pediatrics
 Donation After Circulatory Death From Adults to Pediatrics Matthew Weiss, M.D., Pediatric Intensivist, Québec, Québec President of Canadian pdcd Guideline Development Committee CACCN Webinar, February
Donation After Circulatory Death From Adults to Pediatrics Matthew Weiss, M.D., Pediatric Intensivist, Québec, Québec President of Canadian pdcd Guideline Development Committee CACCN Webinar, February
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Heart Transplantation & MCS in 2017 Advances & Challenges
 Heart Transplantation & MCS in 2017 Advances & Challenges Steven Tsui Papworth Hospital, Cambridge, UK Papworth Hospital Heart Transplantation ADVANCES AND CHALLENGES Heart Transplants 100 75 Adult Heart
Heart Transplantation & MCS in 2017 Advances & Challenges Steven Tsui Papworth Hospital, Cambridge, UK Papworth Hospital Heart Transplantation ADVANCES AND CHALLENGES Heart Transplants 100 75 Adult Heart
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Committee on Organ Donor Intervention Research
 National Academics of Science, Engineering, Medicine Committee on Organ Donor Intervention Research Galen V. Henderson, MD Director, Neurocritical Care Brigham and Women s Hospital Harvard Medical School
National Academics of Science, Engineering, Medicine Committee on Organ Donor Intervention Research Galen V. Henderson, MD Director, Neurocritical Care Brigham and Women s Hospital Harvard Medical School
heart-beating organ donors.
 Management of the potential heart-beating organ donor Paul Edgar FCARCSI Robert Bullock FRCP FRCA Stephen Bonner MRCP FRCA Key points There is a severe shortage of organs for donation from brainstem-dead
Management of the potential heart-beating organ donor Paul Edgar FCARCSI Robert Bullock FRCP FRCA Stephen Bonner MRCP FRCA Key points There is a severe shortage of organs for donation from brainstem-dead
Summary of Significant Changes. Policy
 This Policy replaces POL193/6 Copy Number Effective 13/05/16 Summary of Significant Changes Para 1.3.1.6 - Amendment to donor and recipient age match points to reflect the fact that paediatric recipients
This Policy replaces POL193/6 Copy Number Effective 13/05/16 Summary of Significant Changes Para 1.3.1.6 - Amendment to donor and recipient age match points to reflect the fact that paediatric recipients
Management of the Potential Organ Donor
 s C ll Management of the Potential Organ Donor ( 2018-2 nd edition) s C ll Intensive Care Society of Ireland www.intensivecare.ie The Intensive Care Society of Ireland Page Table of Contents Introduction
s C ll Management of the Potential Organ Donor ( 2018-2 nd edition) s C ll Intensive Care Society of Ireland www.intensivecare.ie The Intensive Care Society of Ireland Page Table of Contents Introduction
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
SAQ Example Questions
 Question 1 A -year-old man has a major haemorrhage following significant trauma and is admitted to your emergency department. He does not have a head injury. Give one definition of major haemorrhage. (1
Question 1 A -year-old man has a major haemorrhage following significant trauma and is admitted to your emergency department. He does not have a head injury. Give one definition of major haemorrhage. (1
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
Surgical Care at the District Hospital 1 13 Resuscitation and Preparation for Anesthesia & Surgery Key Points 2 13.1 Management of Emergencies and Cardiopulmonary Resuscitation The emergency measures that
West Midlands epilepsy network. Dougall McCorry
 West Midlands epilepsy network Dougall McCorry Plan Update on the network meetings where are improvements being made The cost of failure to improve The challenges and barriers to improving epilepsy care
West Midlands epilepsy network Dougall McCorry Plan Update on the network meetings where are improvements being made The cost of failure to improve The challenges and barriers to improving epilepsy care
The NJ Sharing Network Organ and Tissue Donation as an End of Life option for Families
 The NJ Sharing Network Organ and Tissue Donation as an End of Life option for Families NJ Sharing Network Private non-profit service organization Federal designation to provide recovery services State
The NJ Sharing Network Organ and Tissue Donation as an End of Life option for Families NJ Sharing Network Private non-profit service organization Federal designation to provide recovery services State
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Waiting for a Kidney. Objectives
 Waiting for a Kidney Department of Urologic Sciences Grand Rounds William Gourlay Christopher Nguan April 25, 2007 Objectives 1. review the waiting times for deceased-donor kidney transplants in BC and
Waiting for a Kidney Department of Urologic Sciences Grand Rounds William Gourlay Christopher Nguan April 25, 2007 Objectives 1. review the waiting times for deceased-donor kidney transplants in BC and
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
6/13/18. Objectives. Who is the NJ Sharing Network?
 The Gift of Life: Organ and Tissue Donation Amanda Trabilsy Hospital Services Manager Objectives Understand what an Organ Procurement Organization (OPO) is and how they are involved with donation Recognize
The Gift of Life: Organ and Tissue Donation Amanda Trabilsy Hospital Services Manager Objectives Understand what an Organ Procurement Organization (OPO) is and how they are involved with donation Recognize
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders
![Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders](/thumbs/83/87321224.jpg "Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders") Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
BRAIN DEATH. Frequently Asked Questions 04for the General Public
 BRAIN DEATH Frequently Asked Questions 04for the General Public Neurocritical Care Society BRAIN DEATH FAQ s FOR THE GENERAL PUBLIC NEUROCRITICAL CARE SOCIETY 1. Q: Why was this FAQ created? A: Several
BRAIN DEATH Frequently Asked Questions 04for the General Public Neurocritical Care Society BRAIN DEATH FAQ s FOR THE GENERAL PUBLIC NEUROCRITICAL CARE SOCIETY 1. Q: Why was this FAQ created? A: Several
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Organ Donation after Circulatory Death. Report of a consensus meeting. 2 P a g e
 Organ Donation after Circulatory Death Report of a consensus meeting 2 P a g e This document is a report of a Donation after Circulatory Death Consensus meeting held in June 2010. 3 P a g e DCD CONSENSUS
Organ Donation after Circulatory Death Report of a consensus meeting 2 P a g e This document is a report of a Donation after Circulatory Death Consensus meeting held in June 2010. 3 P a g e DCD CONSENSUS
Prepared on behalf of the Intensive Care Society by the Society s Working Group on Organ and Tissue Donation (November 2004)
") INTENSIVE CARE SOCIETY Guidelines for Adult Organ and Tissue Donation Prepared on behalf of the Intensive Care Society by the Society s Working Group on Organ and Tissue Donation (November 2004) Chapter
INTENSIVE CARE SOCIETY Guidelines for Adult Organ and Tissue Donation Prepared on behalf of the Intensive Care Society by the Society s Working Group on Organ and Tissue Donation (November 2004) Chapter
DCD Heart Transplantation Papworth Perspective
 DCD Heart Transplantation Papworth Perspective Simon Messer Stephen Large Objectives Heart transplantation in the UK DCD donation in the UK DCD impact on heart function Normothermic Regional Perfusion
DCD Heart Transplantation Papworth Perspective Simon Messer Stephen Large Objectives Heart transplantation in the UK DCD donation in the UK DCD impact on heart function Normothermic Regional Perfusion
Brain Death Examination Importance and Pitfalls. Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota
 Brain Death Examination Importance and Pitfalls Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota Conflict No Conflicts to report Will not discuss off label use of any medication. Presentation
Brain Death Examination Importance and Pitfalls Dr. Reshi Professor of Neurology/Neurosurgery University of Minnesota Conflict No Conflicts to report Will not discuss off label use of any medication. Presentation
Paediatric Emergency Prompt Cards
 Paediatric Emergency Prompt Cards Introduced July 2016 Prompt cards are designed to be used by any member of the resus team If you have any comments or suggestions, please contact helen.collyer-merritt@sash.nhs.uk
Paediatric Emergency Prompt Cards Introduced July 2016 Prompt cards are designed to be used by any member of the resus team If you have any comments or suggestions, please contact helen.collyer-merritt@sash.nhs.uk
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Addendum/database Part 1 demographics
 Addendum/database Part 1 demographics Part 1 General demographics Section finished? Date Time of alarm 08.00-17.00h 17.00-23.00h 23.00-08.00h Transport unit MICU / ITW IC ambulance Standard ambulance Helicopter
Addendum/database Part 1 demographics Part 1 General demographics Section finished? Date Time of alarm 08.00-17.00h 17.00-23.00h 23.00-08.00h Transport unit MICU / ITW IC ambulance Standard ambulance Helicopter
Take A Breath: Pulmonary Management of the Organ Donor. Whitni Noyes, RN, CPTC Midwest Transplant Network
 Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
Pulse normal; brain dead
 Page 1 of 5 w w w. h a a r e t z. c o m Last update - 03:03 25/09/2007 Pulse normal; brain dead By Avinoam Reches There is no more difficult moment in medicine than when a doctor is required to inform
Page 1 of 5 w w w. h a a r e t z. c o m Last update - 03:03 25/09/2007 Pulse normal; brain dead By Avinoam Reches There is no more difficult moment in medicine than when a doctor is required to inform
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Ethical Challenges With Documenting Brain Death
 Ethical Challenges With Documenting Brain Death William Reitsma, BSN, CPTC Consultant AOPO Accreditation Surveyor 2015 Doug Miller Symposium Wisconsin Dells, Wisconsin When are You Dead? History of Brain
Ethical Challenges With Documenting Brain Death William Reitsma, BSN, CPTC Consultant AOPO Accreditation Surveyor 2015 Doug Miller Symposium Wisconsin Dells, Wisconsin When are You Dead? History of Brain
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
MUSCULOSKELETAL CALCULATOR 42,103. 1in6 SUMMARY. Second Local Authority Bulletin Prevalence of back pain in England and Wolverhampton
 MUSCULOSKELETAL CALCULATOR Second Local Authority Bulletin Prevalence of back pain in England and Wolverhampton 42,103 estimated people in Wolverhampton live with back pain SUMMARY Arthritis Research UK
MUSCULOSKELETAL CALCULATOR Second Local Authority Bulletin Prevalence of back pain in England and Wolverhampton 42,103 estimated people in Wolverhampton live with back pain SUMMARY Arthritis Research UK
Summary of Significant Changes. Policy. Purpose. Responsibilities
 This Management Process Description replaces NEW Copy Number Summary of Significant Changes N/A Effective 17/03/16 Policy All processes included within this document should be adopted by NHS Blood and
This Management Process Description replaces NEW Copy Number Summary of Significant Changes N/A Effective 17/03/16 Policy All processes included within this document should be adopted by NHS Blood and
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on