Lipids What s new (and what s not)
|
|
|
- Joanna Allison
- 5 years ago
- Views:
Transcription

1
2 Lipids What s new (and what s not)
3 Overview Background evidence Obesity Guidelines Treatment options Pragmatic lipidology Side effects Familial Hypercholesterolaemia Cases Summary
4 Background evidence

 Serum total cholesterol, mg/dl (mmol/l) Adapted from Castelli WP.")
5 CHD incidence per 1000 The Framingham Study: Relationship Between Cholesterol and CHD Risk <204 (<5.3) ( ) ( ) ( ) >295 (>7.6) Serum total cholesterol, mg/dl (mmol/l) Adapted from Castelli WP. Am J Med 1984;76:4 12
 3.25 (125) 3.90 (150) 4.50 (175) 5.15 (200) 5.80 (225) 6.45 (250) 7.10 (275) 7.75 (300) 8.40 (325) 9.")
6 Death rate from CHD/1000 men Seven Countries Study: Relationship of 35 Serum Cholesterol to Mortality 30 Northern Europe 25 United States Serbia Southern Europe, inland Southern Europe, Mediterranean Japan (100) 3.25 (125) 3.90 (150) 4.50 (175) 5.15 (200) 5.80 (225) 6.45 (250) 7.10 (275) 7.75 (300) 8.40 (325) 9.05 (350) Serum total cholesterol, mmol/l (mg/dl) Adapted from Verschuren WM et al. J Am Med Assoc 1995;274(2):
7 Distribution of Plasma LDL Cholesterol Levels (Panel A) and Incidence of Coronary Heart Disease (Panel B) among Black Subjects, According to the Presence or Absence of a PCSK9 142X or PCSK9 679X Allele Cohen, J. et al. N Engl J Med 2006;354:




8 Key Statin Trials and Spectrum of Risk Increasing absolute CHD risk 4S 1 LIPID 2 CARE 3 HPS 4 PROSPER 5 ALLHAT-LLT 6 WOSCOPS 7 ASCOT-LLA 8 CHD/high cholesterol CHD/average-to-high cholesterol MI/average cholesterol CHD or diabetes/average cholesterol CVD or risk factors/average cholesterol some CHD/average cholesterol no MI/high cholesterol >3 risk factors/average cholesterol AFCAPS/TexCAPS 9 no CHD/average cholesterol
9 What else? Sugar Increasing evidence that the amount of refined sugar in the diet is linked to obesity Too much emphasis on fat alone and insufficient emphasis on a sensible diet Dietary advice Not too much, mostly plants Count the legs Come back Professor Yudkin all is forgiven
10

11 The evolution of man Human Banker evolution the shape of things GP to come? Surgeon Patient



12
13 Obesity
14 All cause mortality
15 CVD mortality
16 Body-Mass Index (BMI) during Adolescence and Subsequent Cardiovascular Mortality. Twig G et al. N Engl J Med 2016;374:
17 Guidelines
18 Guidelines Guideline groups from Europe, UK and US have taken the same evidence base and produced different guidelines
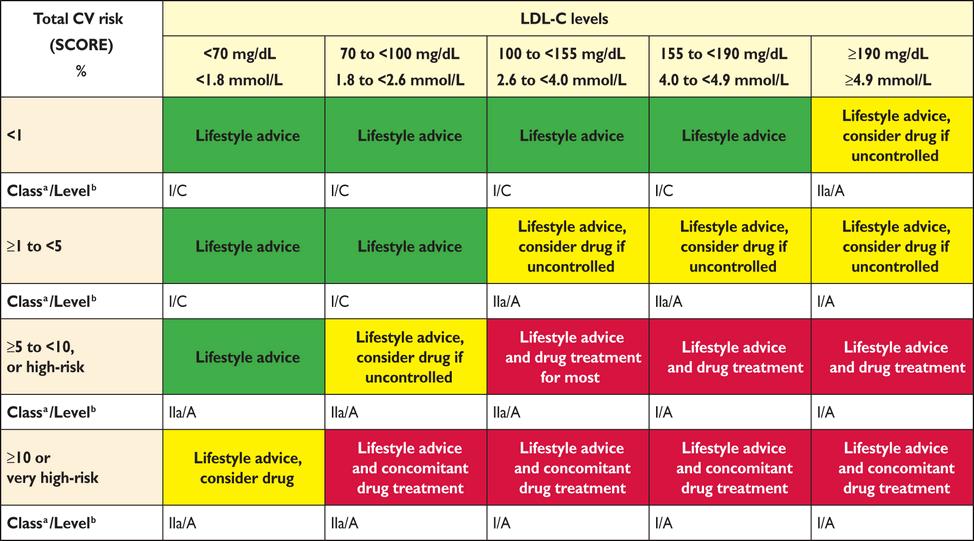
19 ESC
20 NICE Before 20% risk intervention by QRISK LDL target of 3.0 mmol/l After - NICE guidelines [CG181] Published date: July 2014 Last updated: July % risk intervention by QRISK2 Use non-hdl cholesterol 40% reduction in non-hdl cholesterol
21 Treatment options
22 Treatment options Statins No nicotinic acid Ezetimibe is now accepted RCT evidence from Improve-IT PCSK9 inhibitors
23 PCSK9 mechanism of action LDLR recycling PCSK9 mediated degradation of LDLR deadly chaperone Endosome Endosome Lysosome
24 Without CVD With CVD Primary non-familial hypercholesterolaemi a or mixed dyslipidaemia Not recommended at any LDL-C concentration High risk of CVD 1 Recommended only if LDL-C concentration is persistently above 4.0 mmol/litre Very high risk of CVD 2 Recommended only if LDL-C concentration is persistently above 3.5 mmol/litre Primary heterozygousfamilial hypercholesterolaemi a Recommended only if LDL-C concentration is persistently above 5.0 mmol/litre Recommended only if LDL-C concentration is persistently above 3.5 mmol/litre 1 High risk of CVD is defined as a history of any of the following: acute coronary syndrome (such as myocardial infarction or unstable angina needing hospitalisation); coronary or other arterial revascularisation procedures; chronic heart disease; ischaemic stroke; peripheral arterial disease. 2 Very high risk of CVD is defined as recurrent cardiovascular events or cardiovascular events in more than 1 vascular bed (that is, polyvascular disease).
25 Pragmatic lipidology
26 Presentation Family history of premature CVD or sudden death Males <55, females <65 (<60) Incidental finding Opportunistic check Health screening Investigation of chest pain Presentation with clinical sequelae of hyperlipidaemia Myocardial infarction/pvd/cas/cva Acute pancreatitis Xanthelasma / xanthomata
27 Classification of hyperlipidaemia Primary Secondary Hypothyroidism Diabetes Renal disease Liver disease Alcohol
28 Baseline investigations on all patients with lipid disorders Lipid profile (no longer requirement for fasting) (TC, HDL, non-hdl, LDL,Tg) U and E LFT and GT Fasting glucose / HbA1c TFT Urine dipstick
29 Initial assessment Exclude secondary causes of dyslipidaemia Consider the possibility of familial hypercholesterolaemia if total cholesterol > 7.5 mmol/l and family history of premature (<60) heart disease Can you classify the hyperlipidaemia?? Genetic Who needs specialist referral? Specialist referral if TC > 9.0 mmol/l or non-hdl >7.5mmol/L even if no FH Urgent specialist review if TG > 20 mmol/l (unless XS ETOH or poor glycaemic control)
30 Classification Chol +++ Type IIA Chol +++ TG+ Type IIB Chol ++ TG ++ Type III Chol +++ TG +++ Type IV Chol + TG +++ Type I Type V Familial Hypercholesterolaemia (FH) (1/500) FH Familial Combined Hyperlipida emia Type III Often secondary Familial Hypertriglyceridaemia Polygenic Polygenic Polygenic LPL deficiency Apo CII deficiency LDL LDL VLDL Increased IDL VLDL Chylomicrons Chylomicrons VLDL
31 Who to treat? Familial hypercholesterolaemia Secondary prevention - All patients with established vascular disease Angina, MI, PVD,CAS,CVA Primary prevention (specific groups) Type 1 diabetes Type 2 diabetes CKD (egfr <60) Primary prevention Depends on risk
32 Risk scoring A holistic approach to risk factors Various scoring systems Predicts 10 year risk of cardiovascular disease All utilise the same risk factors Age Gender Blood pressure Total cholesterol or TC/HDL ratio NICE specify QRISK 2 (soon 3) Recognition that they may under score for some groups
33
34 Side effects
35 Side effects Side effects do occur in statin therapy The current debate is ill-informed by statements that say No one in clinical trials had side effects Side effects occur in 10-20% Side effects have a strong psychological component
36
37 How well can we extrapolate from clinical trial studies?
38 Clinical trial data Well screened, highly selected patients Frequent and intensive monitoring Good compliance
39 Real life practice Unselected patients Co-morbidities Polyphramacy Variable understanding and drug compliance Monitoring may be problematic
40 What to do Prove that it is due to the statin Did the side effect stop when the statin stopped Exclude hypothyroidism, Vitamin D deficiency and muscle disease (check CK) Replete Vitamin D if deficient Re-challenge at a lower dose Stop if the side effect occurs Stop for one week does it go away Re-challenge - does it come back
41 Then Try a low dose of a different statin Try once weekly Rosuvastatin 5mg with dose escalation Twice a week Three times a week Alternate days Then add ezetimibe
42 Familial hypercholesterolaemia
43 A diagnosis of FH should be made using the Simon Broome criteria, which include a combination of family history, clinical signs (specifically tendon xanthomata), cholesterol concentration and DNA testing
44 Diagnose a person with definite familial hypercholesterolaemia (FH) if they have: cholesterol concentrations as defined in table 1 and tendon xanthomas, or evidence of these signs in first- or second-degree relative or DNA-based evidence of an LDL-receptor mutation, familial defective apo B- 100, or a PCSK9 mutation. Diagnose a person with possible FH if they have cholesterol concentrations as defined in table 1 and at least one of the following. Family history of myocardial infarction: aged younger than 50 years in second-degree relative or aged younger than 60 years in first-degree relative. Family history of raised total cholesterol: greater than 7.5 mmol/l in adult firstor second-degree relative or greater than 6.7 mmol/l in child, brother or sister aged younger than 16 years. Total cholesterol Child/young person > 6.7 mmol/l LDL-C > 4.0 mmol/l Adults > 7.5 mmol/l > 4.9 mmol/l
45 What does this really mean? Genetic testing is required for FH diagnosis This is (relatively) cheap and will get cheaper and is essential for cascade testing It is only required if treatment decisions are uncertain or cascade testing is contemplated
46 Cases


47 Case studies - typical patients
48 Case Female 55 years Referred with TC of 7.9 mmol/l FH of IHD Details of history Brother had AMI age 66 and was a heavy smoker Non smoker having never smoked Weight 55 kg, BMI 20 BP 110/70 No medication Caucasian genes
49 Investigations TC 8.0 mmol/l HDL 3.5 mmol/l Tg 1.1 mmol/l LDL 4.0 mmol/l TC/HDL ratio 2.3 Risk score?
50 Investigations TC 8.0 mmol/l HDL 3.5 mmol/l Tg 1.1 mmol/l LDL 4.0 mmol/l Tc/HDL ratio 2.3 Risk score 2.7% QRISK2 and <1% by HeartSCORE Additional data CRP 0.4 mg/l(high risk >3) Lp(a) <20 (high risk >300)
51 Male 55 years TC 6.5 mmol/l FH IHD Details of history Case Father had AMI age 64, smoker Brother had CABG age 59, smoker Smoker 20/day from age 20 Weight 70 kg BMI 29.1 BP 150/95 Asian genes
52 Investigations TC 6.5 mmol/l HDL 0.7 mmol/l Tg 1.1 mmol/l LDL 5.3 mmol/l TC/HDL ratio 9.3 Risk score?
53 Investigations TC 6.5 mmol/l HDL 0.7 mmol/l Tg 1.1 mmol/l LDL 5.3 mmol/l TC/HDL ratio 9.3 Risk score 54.2$ QRISK2 and 8-13% HeartSCORE Increase by 50% for ethnicity Increase by 50% for FH IHD Note that the non-smoking risk is still 34.4% by QRISK2 4-7% HeartSCORE so enters the treatment band due to ethnicity and FH
54 Investigations CRP 6 mg/l (high risk >3) Lp(a) 450 mg/l (>300 high risk)
55 Case Female 55 years TC 15.0 mmol/l Tg 27.4 mmol/l Glucose 35.5 mmol/l HbA1c 120 mmol/mol Panic Panic Panic
56 Case Treatment Manage diabetes Metformin initially 500mg bd then 1000mg bd
57 1 month later Case TC 6.5 mmol/l Tg 2.2 mmol/l HDL 1.0 mmol/l LDL 4.5 mmol/l Glucose 6.9 mmol/l HbA1c 82 mmol/mol Add atorvastatin 20 mg od
58 Case Male 46 TC 12.1 mmol/l Tg 35.2 mmol/l Glucose 4.5 mmol/l HbA1c 23 mmol/mol LFT including GGT normal TFT - normal
59 Case BMI 26.9 Lipoprotein electrophoresis Type III pattern Apo E genotype Rx E2/E2 Fenofibrate micronised 160 mg od
60 Case 3 months later TC 5.2 Tg 1.1 HDL 1.5 LDL 3.2
61 Case Female 52 years TC 13.4 mmol/l Tg 4.9 mmol/l HDL 1.8 mmol/l Non HDLC 11.6 mmol/l
62 Case Referred urgently as FH Commenced on Atorvastatin 40mg Severe myalgia stopped statin (an avid Daily Mail reader)
63 Case CK 850 U/L Vitamin D - <17 nmol/l Statin induced myopathy? Glucose 7.1 mmol/l HbA1c 32 mmol/mol LFT ALT 65U/L (<40) GGT 85 U/L (<40) BMI 29.9
64 Case BUT ft4 3.2 nmol/l TSH mu/l Thyroxine 50 > 75 > 100 mcg/l
65 Case 6 months later TC 5.2 mmol/l Tg 0.8 mmol/l HDL 2.2 mmol/l LDL 2.6 mmol/l But what was she most pleased about BMI 26.8
66 Familial hyperlipidaemia implementation of clinical guidelines A family history should always be obtained from an individual being investigated for FH to determine if a dominant pattern of inheritance is present
67 Case Male 41 years FH IHD father had quadruple bypass age 65 on a background of familial hypercholesterolemia Lipid profile Total cholesterol Trigs HDL LDL Non-HDL Apo a Apo b S-CRP
68 Treat? Splice mutation of LDLR N G>A Yes 1. HDL raising 2. LDL lowering 3. Both
69 What next GE TE ME LE SE
70 GE TE N G>A ME LE (11) N G>A TC 7.1 SE (10) N G>A TC 7.6
71 Treatment Both boys started on simvastatin 10mg
72 Learning points Paternal diagnosis on the basis of LDLR mutation Treatment indicated Boys detected by cascade screening NICE guidelines All patients with FH IHD and TC >7.5 should be reviewed All LDLR mutation positive should be tested
73 Conclusion Lipid lowering therapy will have clinical benefits in all groups Risk/benefit must may favourable Risk reduction must be greater that the risk of co-morbid conditions Therapy was a success but the patient died Clinical judgement is required
74 Paul s guide to lipids Its never THAT urgent (except very high triglycerides) You do not have to fast to do cholesterol Never believe one reading always do two (preferably 3) Risk factor management before pills (death cures smoking) and Benecol drinks do work. Do risk stratification first Look at the HDL Look at the TC and Tg and think Tg >5 Exclude secondary causes Refer
Southern Derbyshire Shared Care Pathology Guidelines. Dyslipidaemia
 Southern Derbyshire Shared Care Pathology Guidelines Dyslipidaemia This guideline applies to patients with significantly abnormal lipid profiles, which may be primary (genetic), secondary to other diseases
Southern Derbyshire Shared Care Pathology Guidelines Dyslipidaemia This guideline applies to patients with significantly abnormal lipid profiles, which may be primary (genetic), secondary to other diseases
APPENDIX 2F Management of Cholesterol
 Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Cardiovascular risk reduction in diabetes Lipids (NICE CG181)
") Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Cardiovascular risk reduction in diabetes Lipids (NICE CG181) Primary Prevention T1DM Offer Atorvastatin 20mg if >40 years old Diabetes duration >10 years Established nephropathy Other CVS risk factors
Primary Prevention Patients aged 85yrs and over
 Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Rotherham Guideline for the management of Non-Familial Hypercholesterolaemia Type 1 Diabetes Offer lifestyle advice Over 40yrs of age? Diabetic for more than 10 years? Established nephropathy? Other CVD
Identification and management of familial hypercholesterolaemia (FH) - An overview
 - An overview") Identification and management of familial hypercholesterolaemia (FH) - An overview National Collaborating Centre for Primary Care and Royal College of General Practitioners NICE Guideline CG 71 (August
Identification and management of familial hypercholesterolaemia (FH) - An overview National Collaborating Centre for Primary Care and Royal College of General Practitioners NICE Guideline CG 71 (August
Volume 2; Number 11 July 2008
 Volume 2; Number 11 July 2008 CONTENTS Page 1 NICE Clinical Guideline 67: Lipid Modification (May 2008) Page 7 NICE Technology Appraisal 132: Ezetimibe for the treatment of primary (heterozygous familial
Volume 2; Number 11 July 2008 CONTENTS Page 1 NICE Clinical Guideline 67: Lipid Modification (May 2008) Page 7 NICE Technology Appraisal 132: Ezetimibe for the treatment of primary (heterozygous familial
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines Lipid Lowering Therapy for the Prevention of Cardiovascular Disease
 Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
Royal Wolverhampton Hospital Adult Lipid Lowering Therapy Guidelines 1 This guideline is intended to assist rational and cost-effective prescribing of lipid regulating medications across both primary and
SECONDARY PREVENTION OF CORONARY HEART DISEASE AND ISCHAEMIC STROKE/TIA
 PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol)
") CLINICAL GUIDELINE Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol) A guideline is intended to assist healthcare professionals in the choice of disease-specific
CLINICAL GUIDELINE Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol) A guideline is intended to assist healthcare professionals in the choice of disease-specific
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Death is inevitable but premature death is not. Sir Richard Doll
 Welcome to the Diabetes Care for You webinar Please log onto the conference call so you can hear our presenter From any SCFT Cisco phone dial 800800 From a mobile phone or any other phone dial 01273 242
Welcome to the Diabetes Care for You webinar Please log onto the conference call so you can hear our presenter From any SCFT Cisco phone dial 800800 From a mobile phone or any other phone dial 01273 242
Dyslipidaemia. Dr NM Oosthuizen Dept of Chemical Pathology SA
 Dyslipidaemia Dr NM Oosthuizen Dept of Chemical Pathology SA13 2014 Endogenous and exogenous pathways Endogenous Exogenous Reverse cholesterol transport Dyslipidaemias Causes can be primary or secondary
Dyslipidaemia Dr NM Oosthuizen Dept of Chemical Pathology SA13 2014 Endogenous and exogenous pathways Endogenous Exogenous Reverse cholesterol transport Dyslipidaemias Causes can be primary or secondary
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Appendix F Simon Broome Diagnostic criteria for index individuals and relatives
 Appendix F Simon Broome Diagnostic criteria for index individuals and relatives 1 SIMON BROOME DIAGNOSTIC CRITERIA FOR INDEX INDIVIDUALS (PROBANDS) 2 2 GENDER- AND AGE-SPECIFIC LDL-C CRITERIA FOR THE DIAGNOSIS
Appendix F Simon Broome Diagnostic criteria for index individuals and relatives 1 SIMON BROOME DIAGNOSTIC CRITERIA FOR INDEX INDIVIDUALS (PROBANDS) 2 2 GENDER- AND AGE-SPECIFIC LDL-C CRITERIA FOR THE DIAGNOSIS
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Cost effectiveness of cascade testing for FH:
 Cost effectiveness of cascade testing for FH: Background In 2008, NICE published evidence-based guidelines for identification and management of FH Updated 2017 Recommended all Clinical FH DNA test to confirm
Cost effectiveness of cascade testing for FH: Background In 2008, NICE published evidence-based guidelines for identification and management of FH Updated 2017 Recommended all Clinical FH DNA test to confirm
Helen Williams Consultant Pharmacist for CV Disease - South London
 Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
Helen Williams Consultant Pharmacist for CV Disease - South London CVD remains the leading cause of death in the UK Accounts for a third of all deaths 46,000 deaths in people < 75 years (70% of these
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
4/14/2018 DYSLIPIDEMIA CASES. Mary Malloy, MD. I have nothing to disclose
 DYSLIPIDEMIA CASES Mary Malloy, MD I have nothing to disclose 1 Case 1 A 24 year old healthy, slender woman is referred because she has a family history of premature CAD (mother, age 59, had onset of angina
DYSLIPIDEMIA CASES Mary Malloy, MD I have nothing to disclose 1 Case 1 A 24 year old healthy, slender woman is referred because she has a family history of premature CAD (mother, age 59, had onset of angina
THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS
 THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS Hormonal regulation INSULIN lipid synthesis, lipolysis CORTISOL lipolysis GLUCAGON lipolysis GROWTH HORMONE lipolysis CATECHOLAMINES lipolysis LEPTIN catabolism
THE CLINICAL BIOCHEMISTRY OF LIPID DISORDERS Hormonal regulation INSULIN lipid synthesis, lipolysis CORTISOL lipolysis GLUCAGON lipolysis GROWTH HORMONE lipolysis CATECHOLAMINES lipolysis LEPTIN catabolism
Familial hypercholesterolaemia
 Familial hypercholesterolaemia Jaimini Cegla MRCP FRCPath PhD Consultant in Chemical Pathology and Metabolic Medicine Hammersmith Hospital Lipid Clinic 20 April 2017 An unrecognised, potentially fatal,
Familial hypercholesterolaemia Jaimini Cegla MRCP FRCPath PhD Consultant in Chemical Pathology and Metabolic Medicine Hammersmith Hospital Lipid Clinic 20 April 2017 An unrecognised, potentially fatal,
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME Briefing paper QOF indicator area: Primary prevention of CVD Potential output:
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March Crowne Plaza, Dublin
 2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
In 2008 NICE issued guidelines on lipid modification. Key points are summarised below.
 Hyperlipidaemia: management In 2008 NICE issued guidelines on lipid modification. Key points are summarised below. Primary prevention A systematic strategy should be used to identify people aged 40-74
Hyperlipidaemia: management In 2008 NICE issued guidelines on lipid modification. Key points are summarised below. Primary prevention A systematic strategy should be used to identify people aged 40-74
Focus on FH (Familial Hypercholesterolemia) Joshua W. Knowles, MD PhD for PCNA May, 2013
 Joshua W. Knowles, MD PhD for PCNA May, 2013") Focus on FH (Familial Hypercholesterolemia) Joshua W. Knowles, MD PhD for PCNA May, 2013 Conflicts CMO for The FH Foundation Pre-talk quiz What is cascade screening? 1. screening all family members 2.
Focus on FH (Familial Hypercholesterolemia) Joshua W. Knowles, MD PhD for PCNA May, 2013 Conflicts CMO for The FH Foundation Pre-talk quiz What is cascade screening? 1. screening all family members 2.
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia
 and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia") PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
PCSK9 Inhibitors Praluent (Alirocumab) and Repatha (Evolocumab) For the Treatment of Familial Hypercholesterolemia Policy Number: Original Effective Date: MM.04.037 08/01/2016 Line(s) of Business: HMO;
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
REPATHA (PCSK9 INHIBITORS)
") REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
REPATHA (PCSK9 INHIBITS) Indications: PCSK9 Inhibitors are indicated for treatment of adults with heterozygous familial hypercholesterolemia (HeFH) or clinical atherosclerotic cardiovascular disease as
FORTH VALLEY. LIPID LOWERING GUIDELINE v5 2016
 FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Cardiovascular Disease Prevention: Current Knowledge, Future Directions
 Cardiovascular Disease Prevention: Current Knowledge, Future Directions Daniel Levy, MD Director, Framingham Heart Study Professor of Medicine, Boston University School of Medicine Editor-in-Chief, Journal
Cardiovascular Disease Prevention: Current Knowledge, Future Directions Daniel Levy, MD Director, Framingham Heart Study Professor of Medicine, Boston University School of Medicine Editor-in-Chief, Journal
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 6 October 2010
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 6 October 2010 CRESTOR 5 mg, film-coated tablet B/30 (CIP code: 369 853-8) B/90 (CIP code: 391 690-0) CRESTOR 10 mg,
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 6 October 2010 CRESTOR 5 mg, film-coated tablet B/30 (CIP code: 369 853-8) B/90 (CIP code: 391 690-0) CRESTOR 10 mg,
Calculating RR, ARR, NNT
 Calculating RR, ARR, NNT In a trial RR = Event rate (eg # of people with one stroke/ total people) in treatment group/event rate in the control group. ARR = Event rate in control group minus the event
Calculating RR, ARR, NNT In a trial RR = Event rate (eg # of people with one stroke/ total people) in treatment group/event rate in the control group. ARR = Event rate in control group minus the event
Need Help.. 4. Resources Abbreviations used in the FH Registry Eligibility Criteria for Inclusion in the FH Registry..
 The purpose of the National Familial Hypercholesterolaemia Registry is to collate data to facilitate clinical service planning and to inform clinical best practice. The Registry will also enable research
The purpose of the National Familial Hypercholesterolaemia Registry is to collate data to facilitate clinical service planning and to inform clinical best practice. The Registry will also enable research
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Dyslipidemia. Team Members: Laila Mathkour, Khalid Aleedan, Bayan Al-Mugheerha, Fatima AlTassan
 Dyslipidemia Objectives: Not given. Team Members: Laila Mathkour, Khalid Aleedan, Bayan Al-Mugheerha, Fatima AlTassan Team Leader: Amal Alshaibi Revised By: Yara Aldigi and Basel almeflh Resources: 435
Dyslipidemia Objectives: Not given. Team Members: Laila Mathkour, Khalid Aleedan, Bayan Al-Mugheerha, Fatima AlTassan Team Leader: Amal Alshaibi Revised By: Yara Aldigi and Basel almeflh Resources: 435
WORKSHOP 1. Management of Patients with Familial Hypercholesterolemia
 WORKSHOP 1 Management of Patients with Familial Hypercholesterolemia Tutors: Manal Al-Kindi (Oman)/ Gilles Lambert (France) (Case 1) Zuhier Awan (KSA)/ Raul Santos (Brazil) (Case 2) Khalid Al-Waili (Oman)/
WORKSHOP 1 Management of Patients with Familial Hypercholesterolemia Tutors: Manal Al-Kindi (Oman)/ Gilles Lambert (France) (Case 1) Zuhier Awan (KSA)/ Raul Santos (Brazil) (Case 2) Khalid Al-Waili (Oman)/
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Debates
 The Clinical Debates Speakers: Round 2: Statins for Primary Prevention of Cardiovascular Disease Matthew Cantrell, PharmD, BCPS, is a 2000 graduate of Mt. Mercy College and 2005 graduate from the University
The Clinical Debates Speakers: Round 2: Statins for Primary Prevention of Cardiovascular Disease Matthew Cantrell, PharmD, BCPS, is a 2000 graduate of Mt. Mercy College and 2005 graduate from the University
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Drug Prior Authorization Guideline PCSK9 Inhibitors -
 Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Drug Prior Authorization Guideline PCSK9 Inhibitors - REPATHA (evolocumab) PRALUENT (alirocumab) PA9911 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes-as shown below Additional
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
Hyperlipidaemia, dyslipidaemia and hypercholesterolaemia
 Medicine > Cardiology > Hyperlipidaemia, dyslipidaemia and Background information Patient information including patient decision aid Key messages for this pathway FH specialist nurse contact details Local
Medicine > Cardiology > Hyperlipidaemia, dyslipidaemia and Background information Patient information including patient decision aid Key messages for this pathway FH specialist nurse contact details Local
Dyslipidemia. (Med-341)
") Dyslipidemia (Med-341) Anwar A Jammah, MD, FRCPC, FACP, CCD, ECNU. Associate Professor of Medicine Consultant Medicine, Endocrinology, Thyroid Oncology Department of Medicine, King Saud University The
Dyslipidemia (Med-341) Anwar A Jammah, MD, FRCPC, FACP, CCD, ECNU. Associate Professor of Medicine Consultant Medicine, Endocrinology, Thyroid Oncology Department of Medicine, King Saud University The
LIST OF ABBREVIATIONS
 Diabetes & Endocrinology 2005 Royal College of Physicians of Edinburgh Diabetes and lipids 1 G Marshall, 2 M Fisher 1 Research Fellow, Department of Cardiology, Glasgow Royal Infirmary, Glasgow, Scotland,
Diabetes & Endocrinology 2005 Royal College of Physicians of Edinburgh Diabetes and lipids 1 G Marshall, 2 M Fisher 1 Research Fellow, Department of Cardiology, Glasgow Royal Infirmary, Glasgow, Scotland,
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors
 Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Request for Prior Authorization for PCSK9 inhibitor therapy Website Form Submit request via: Fax
 Request for Prior Authorization for PCSK9 inhibitor therapy Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 PCSK9 is a protein that reduces the hepatic removal of low-density
Request for Prior Authorization for PCSK9 inhibitor therapy Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 PCSK9 is a protein that reduces the hepatic removal of low-density
Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges
 ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
ESC 2015 London Accumulating Clinical data on PCSK9 Inhibition: Key Lessons and Challenges Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Hyperlipidemia. Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi
 Hyperlipidemia Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi Outline The story of lipids Definition of hyperlipidemia Classification of hyperlipidemia Causes of hyperlipidemia
Hyperlipidemia Prepared by : Muhannad Mohammed Supervisor professor : Dr. Ahmed Yahya Dallalbashi Outline The story of lipids Definition of hyperlipidemia Classification of hyperlipidemia Causes of hyperlipidemia
ADMINISTRATIVE POLICY AND PROCEDURE
 ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
ADMINISTRATIVE POLICY PROCEDURE Policy #: Subject: PCSK9 INHIBITS (ex: Repatha) Section: Care Management Effective Date: January 1, 2015 Revision Date(s): NA Review Date(s): NA Responsible Parties: Patryce
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Metabolic Syndrome. Shon Meek MD, PhD Mayo Clinic Florida Endocrinology
 Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Low HDL-levels: leave it or treat it?
 Cardiology Update 2011 Davos, 14 02 2011 Low HDL-levels: leave it or treat it? Experts: J.P. Kastelein, Amsterdam and U. Landmesser, Zurich Cases: C. Besler, Zurich and I. Sudano, Zurich Mr H.B., 1960
Cardiology Update 2011 Davos, 14 02 2011 Low HDL-levels: leave it or treat it? Experts: J.P. Kastelein, Amsterdam and U. Landmesser, Zurich Cases: C. Besler, Zurich and I. Sudano, Zurich Mr H.B., 1960
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo?
 Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo? Alberto Zambon University of Padova - Italy DISCLOSURE - CONFLICT OF INTEREST Prof. A. Zambon reports having received grants,
Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo? Alberto Zambon University of Padova - Italy DISCLOSURE - CONFLICT OF INTEREST Prof. A. Zambon reports having received grants,
Lipids Board Review. Ira Goldberg, MD New York University School of Medicine. Which of the following is the best initial therapy choice?
 Lipids Board Review Ira Goldberg, MD New York University School of Medicine 1. A 22 year old male college student is referred for severe hypertriglyceridemia ( 1500 mg/dl [ 17.0 mmol/l]). He has a history
Lipids Board Review Ira Goldberg, MD New York University School of Medicine 1. A 22 year old male college student is referred for severe hypertriglyceridemia ( 1500 mg/dl [ 17.0 mmol/l]). He has a history
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
This is a lipid lowering drug strategy which should only be used within an overall lifestyle and clinical management strategy.
 Treatment Guideline Statin Prescribing Objective These guidelines represent the views of the Gloucestershire Hospitals NHS Foundation Trust, which were arrived at after consideration of the available evidence
Treatment Guideline Statin Prescribing Objective These guidelines represent the views of the Gloucestershire Hospitals NHS Foundation Trust, which were arrived at after consideration of the available evidence
ATP III (Adult Treatment Panel III) CLASSIFICATION C IN ADULTS
 CLASSIFICATION C IN ADULTS") LABORATORY AND RISK FACTORS OF ATHEROSCLEROSIS S R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty RISK FACTORS FOR CHD Clinical Risk Factors Laboratory Risk Factors MAJOR CLINICAL RISK
LABORATORY AND RISK FACTORS OF ATHEROSCLEROSIS S R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty RISK FACTORS FOR CHD Clinical Risk Factors Laboratory Risk Factors MAJOR CLINICAL RISK
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS
 BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
DYSLIPIDEMIA PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
CVD Prevention, Who to Consider
 Continuing Professional Development 3rd annual McGill CME Cruise September 20 27, 2015 CVD Prevention, Who to Consider Dr. Guy Tremblay Excellence in Health Care and Lifelong Learning Global CV risk assessment..
Continuing Professional Development 3rd annual McGill CME Cruise September 20 27, 2015 CVD Prevention, Who to Consider Dr. Guy Tremblay Excellence in Health Care and Lifelong Learning Global CV risk assessment..
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Appendix E Health Economic modelling
 Appendix E Health Economic modelling Appendix E: Health economic modelling Page 1 of 55 1 Use of high intensity statin compared to low intensity statin in the management of FH patients 1.1 Introduction
Appendix E Health Economic modelling Appendix E: Health economic modelling Page 1 of 55 1 Use of high intensity statin compared to low intensity statin in the management of FH patients 1.1 Introduction