LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA
|
|
|
- Oscar Kennedy
- 5 years ago
- Views:
Transcription



1 LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018
2 Objectives 1. Identify common preventable causes of hypoglycemia in people with diabetes 2. Learn how to advise patients who experience hypoglycemia 3. Recognize fear of hypoglycemia
3 Classification of Hypoglycemia Level Category Blood glucose criteria Description 1 Alert < 70 mg% Requires fast acting carbohydrate and adjustment of therapy 2 Clinically significant < 54 mg% Serious, clinically important 3 Severe No specified level Associated with severe cognitive impairment, requires help to resolve
4 Prevalence of Hypoglycemia 532,542 People with Type 2 Diabetes on Oral Therapies and Insulin: A Systematic Review and Meta-Analysis of Population Based Studies at On average patients with type 2 diabetes on insulin had 23 mild or moderate and one severe episode each year Prevalence of hypoglycemia was 45% for mild/moderate and 6% for severe. Incidence of hypoglycemic episodes per person-year for mild/moderate and for severe was 19 and 0.80, respectively.
5
6

 Wait 15 minutes and check blood sugar")

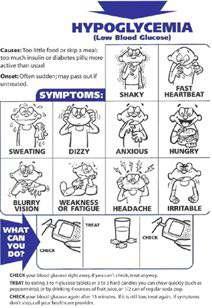
7 Rule Rule of 15 s Administer Wait Administer 15 grams of rapid acting carbohydrate such as 4 ounces juice, 5 pieces of candy (lifesavers, gummy bears, not chocolate) Wait 15 minutes and check blood sugar Treatment for Hypoglycemia Repeat Repeat above and avoid overtreatment Call Call 911 if blood sugar still low after 2 treatments
8 Who is at risk for hypoglycemia? Anyone on insulin or sulfonylurea People with diabetes with variable meals who take a fixed dose of mealtime insulin Elderly who may be losing renal function People on large doses of basal insulin Biggest risk for having hypoglycemia today is having had hypoglycemia yesterday
9 Framework for Targets for Type 2 Patient Chracteristics Rationale A1c BP Lipids Healthy -Intact cognitive and functional status Complex -Multiple comorbidities -Mild/mod CI - 2 or more IADL dependencies Very complex - LTC residents - Mod/severe CI - End stage chronic disease Longer life expectancy Treatment burden Risk of hypoglycemia Fall risk Limited life expectancy Benefits unclear < 7.5% < 140/90 Statins if tolerated < 8 % < 140/90 Statins if tolerated < 8.5% < 150/90 Consider risks vs. benefits
10 Complications from Hypoglycemia Motor vehicle accident, falls, injury Hypoglycemia unawareness with risk of severe hypoglycemia Fear of hypoglycemia that can lead to poor glycemic control Long term study of elderly with type 2 with one or more episodes of severe hypoglycemia had a step wise increase in risk of dementia ACCORD study found that as cognitive function decreased, the risk of severe hypoglycemia increased
11 Impaired Cognitive Function Per ADA standards with Level B evidence page S61 Ongoing assessment of cognitive function is suggested with increased vigilance for hypoglycemia by the clinician, patient and caregivers if low cognition or declining cognition is found.
12
13
14
15 Pharmacotherapeutics for Type 1 Most should be treated with multiple dose injections of a basal and mealtime insulin or a continuous infusion pump (Level A evidence) Most should use rapid acting analogs at mealtime to avoid hypoglycemia (Level A evidence) Consider patient education on matching mealtime insulin dose to carbohydrate intake at meal (nutritional dose), pre-meal blood glucose level (correction dose) and level of physical activity (Level E/ expert opinion) Patients successful on an insulin pump should continue this therapy after age 65 (Level E/expert opinion)



16 Fear of Hypoglycemia Should be treated per ADA recommendations Can be a barrier to achieving A1c target HFS II screening tool for assessment
17 Sample of Items on HFS II Ate large snack Kept BG >150 mmol/l Reduced insulin when BG low Measured BG six or more times per day Take someone with me when out Limited out-of-town travel Limited driving Avoided visiting friends Stayed home more than liked Limited physical activity Made sure others were around Avoided sex Kept BG high during important tasks Had others check on me Not recognizing low BG Not having food available Passing out in public Embarrassing myself in social situation Having hypoglycemic episode alone Appearing drunk or stupid
18 Hypoglycemia Unawareness Per ADA standards with Level A evidence page S34 People with hypoglycemia unawareness should be treated using blood glucose awareness training (or other evidence-based intervention) to help reestablish awareness of hypoglycemia and reduce fear of hypoglycemia
19 Medical management of hypoglycemia unawareness Per ADA standards with level A evidence page S61 Patients treated with insulin of with an episode of clinically significant hypoglycemia [<54 mg%] should be advised to raise their glycemic targets to strictly avoid hypoglycemia for at least several weeks in order to partially reverse hypoglycemia unawareness and reduce the risk of future episodes
20 Population Management Ideas Identifying elderly patients with A1c < 7% on insulin or sulfonyl urea Ensure all patients on insulin or sulfonylurea are taught about recognition and treatment of hypoglycemia Consider insulin pump, continuous glucose monitor and glucagon for injection at home for patients with frequent severe hypoglycemia
21 Situations for mental health referral (1) Impaired self-care with diabetes distress after education Positive screen for depression Disordered eating, eating disorder, disrupted patterns of eating Intentional omission of meds/insulin to lose weight Positive screen for anxiety or fear of hypoglycemia
22 Situations for mental health referral (2) Serious mental illness suspected Youth and families with behavioral self-care difficulties, repeated DKA admissions Positive screening for cognitive impairment Declining or impaired ability to perform diabetes self-care behaviors Before bariatric or metabolic surgery, and after surgery if adjustment support needed
23 Case studies
24 Elderly woman with failing kidneys Subjective 74 year old Filipino woman with Stage 5 CKD recently consulted to nephrologist to consider dialysis On basal/bolus insulin with good control and increasing frequency of hypoglycemia. Basal insulin slowly decreased from 40 units to 18 units, bolus from 10 units to 5 units lunch and dinner only On multiple meds for HTN, HLD, gout, epopoetin injections for anemia q2weeks Objective BMI = 32, abdominal obesity BP 116/78 P = 70 A1c = 6.1% Hemoglobin = 8 Creatinine = 7.8 mg%, GFR < 10 SMBG for past 2 weeks AC Breakfast range 87 to 99 median 94 AC Lunch 126 to 140 median 132 AC Dinner range 140 to 189 median 152
25 Young adult on 3 oral agents 35 yo Asian man diagnosed 1 year ago Diabetes diagnosed with routine screening, A1c = 9%. No HTN, no HLD Started on metformin, then a DPP-4 was added, and 1 month ago glipizide 5 mg at breakfast was added. He started feeling hungry and shaky after breakfast requiring daily mid-morning snack. Checked BG once = 62 Walks briskly 30 to 60 minutes every day Gained 5 pounds since starting glipizide Objective BMI = 24, waist = 32 BP 124/78 P = 70 A1c = 7.2% Lipids, chemistry panel normal SMBG for past 2 weeks AC Breakfast range 108 to 128 median 118 AC Lunch (post snack) 126 to 155 median 130 AC Dinner range 140 to 178 median 152
26 References AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM 2018, Endocr Pract.2018,doi: /CS on line at Inzucchi SE et al. Management of Hyperglycemia in Type 2 diabetes, Diabetes Care 2015; 38: Khunti K et al. Clinical inertia with regard to intensifying therapy in people with type 2 diabetes treated with basal insulin. Diabetes Obes Metab 2016; 18: on line at Munshi MN et al. Simplification of insulin regimen in older adults and risk of hypoglycemia [published online June 6, 2016]. JAMA Intern Med. doi: /jamainternmed Standards of Medical Care in Diabetes. Diabetes Care 2018; 41 (Suppl. 1): S1-S159
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia
 It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia Jacqueline LaManna, PhD, ANP BC, BC ADM, CDE Holly Divine, PharmD, BCACP, CGP, CDE, FAPhA Disclosures Dr. Jacqueline LaManna
It Happens Even in Type 2! When to Start Thinking Seriously About Hypoglycemia Jacqueline LaManna, PhD, ANP BC, BC ADM, CDE Holly Divine, PharmD, BCACP, CGP, CDE, FAPhA Disclosures Dr. Jacqueline LaManna
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address:
 Name: Ward/Practice Area: Mailing Address:") 1 DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address: 2 Learning Outcomes All nurses, regardless of practice setting, are required to work collaboratively with the person
1 DIABETES Self Directed Test (12 Hours) Name: Ward/Practice Area: Mailing Address: 2 Learning Outcomes All nurses, regardless of practice setting, are required to work collaboratively with the person
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Glycemic Control IU Health Diabetes Centers
 Glycemic Control IU Health Diabetes Centers Central Nursing Orientation 3/10/2014 1 Objectives Identify laboratory results that diagnosis diabetes and reflect glycemic control Describe glycemic control
Glycemic Control IU Health Diabetes Centers Central Nursing Orientation 3/10/2014 1 Objectives Identify laboratory results that diagnosis diabetes and reflect glycemic control Describe glycemic control
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
Diabetes Management in New Brunswick Nursing Homes
 Diabetes Management in New Brunswick Nursing Homes Prepared by Dr. Angela McGibbon March, 2016 As the population ages and with the rising incidence of diabetes, there are increasing numbers of people with
Diabetes Management in New Brunswick Nursing Homes Prepared by Dr. Angela McGibbon March, 2016 As the population ages and with the rising incidence of diabetes, there are increasing numbers of people with
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per
 4 times per") APPENDIX 1 Insulin Titration Algorithm Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per day. All subjects will be contacted weekly to review hypoglycemia and adverse
APPENDIX 1 Insulin Titration Algorithm Subjects are requested to perform self-monitoring of blood glucose (SMBG) 4 times per day. All subjects will be contacted weekly to review hypoglycemia and adverse
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Journal Club September 29, Vanessa AKIKI PGYlII Internal Medicine
 Journal Club September 29, 2017 Vanessa AKIKI PGYlII Internal Medicine AUBMC 2017 Case Presentation 41-year-old man who was diagnosed with type 1 diabetes 21 years ago presents to your clinic. He believes
Journal Club September 29, 2017 Vanessa AKIKI PGYlII Internal Medicine AUBMC 2017 Case Presentation 41-year-old man who was diagnosed with type 1 diabetes 21 years ago presents to your clinic. He believes
Hypoglycemia. Patient Education Diabetes Care Center. How to cope with low blood sugar. General Facts on Low Blood Sugar. Causes
 Patient Education How to cope with low blood sugar Recognizing the causes and symptoms of hypoglycemia can help you prepare for and respond to this condition when it arises. General Facts on Low Blood
Patient Education How to cope with low blood sugar Recognizing the causes and symptoms of hypoglycemia can help you prepare for and respond to this condition when it arises. General Facts on Low Blood
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Welcome Everyone. Monitoring, Sick Days, Inpatient Management - Objectives. Mrs. Jones has new diabetes. She asks you: Page 1
 Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
 Diabetes Care Center Box 356176 1959 N.E. Pacific St. Seattle, WA 98195 206-598-4882 120457 University of Washington Medical Center Diabetes Care Center Arabic r02/2000 Patient Education Diabetes Care
Diabetes Care Center Box 356176 1959 N.E. Pacific St. Seattle, WA 98195 206-598-4882 120457 University of Washington Medical Center Diabetes Care Center Arabic r02/2000 Patient Education Diabetes Care
Incorporating CGM Into Clinical Decision Making. Etie Moghissi, MD, FACE Clinical Associate Professor, David Geffen School of Medicine UCLA
 Incorporating CGM Into Clinical Decision Making Etie Moghissi, MD, FACE Clinical Associate Professor, David Geffen School of Medicine UCLA 1 Limitations of Current Glucose Monitoring Methods A1c Standard
Incorporating CGM Into Clinical Decision Making Etie Moghissi, MD, FACE Clinical Associate Professor, David Geffen School of Medicine UCLA 1 Limitations of Current Glucose Monitoring Methods A1c Standard
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Older Adults & Optimal Outcome. Individualizing Diabetes Management. Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC
 Older Adults & Optimal Outcome Individualizing Diabetes Management Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC What is Diabetes? METABOLIC DISEASE Food breakdown (carbohydrates,
Older Adults & Optimal Outcome Individualizing Diabetes Management Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC What is Diabetes? METABOLIC DISEASE Food breakdown (carbohydrates,
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical
 Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
Case Study. Patient Profile. Baseline Report - Daily Patterns. Insights
 Case Study Patient Profile Sex/Age: Female, 48 years old Disease diagnosis: Type 2 for past 13 years, coronary artery disease for 3 years, complains of severe tiredness HbA1c: 9.0% Diabetes medication
Case Study Patient Profile Sex/Age: Female, 48 years old Disease diagnosis: Type 2 for past 13 years, coronary artery disease for 3 years, complains of severe tiredness HbA1c: 9.0% Diabetes medication
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
nocturnal hypoglycemia percentage of Hispanics in the insulin glargine than NPH during forced patients who previously This study excluded
 Clinical Trial Design/ Primary Objective Insulin glargine Treat-to-Target Trial, Riddle et al., 2003 (23) AT.LANTUS trial, Davies et al., 2005 (24) INSIGHT trial, Gerstein et al., 2006 (25) multicenter,
Clinical Trial Design/ Primary Objective Insulin glargine Treat-to-Target Trial, Riddle et al., 2003 (23) AT.LANTUS trial, Davies et al., 2005 (24) INSIGHT trial, Gerstein et al., 2006 (25) multicenter,
!"#$%&'()*+,-./012&3!"#$%N!"#$%&'()OMMM QMMM!"#$%&'!"#()*+,-.!"#$%&'()*+,-./012priclJ kvirob^=e ÖäóÄìêáÇÉI=ÖäáéáòáÇÉF=!"
*+,-./012&3!#$%N!#$%&'()OMMM QMMM!#$%&'!#()*+,-.!#$%&'()*+,-./012priclJ kvirob^=e ÖäóÄìêáÇÉI=ÖäáéáòáÇÉF=!") !"#$!"#$%!"#$%&!"#$%&!"#$%&!"#$%&!"#$%&!"#$%&'()*+,-./012&3!"#$%N!"#$%&'()OMMM QMMM!"#$%&'!"#()*+,-.!"#$%&'()*+,-./012priclJ kvirob^=e ÖäóÄìêáÇÉI=ÖäáéáòáÇÉF=!"!"#$%&'()*+,-'()./012!"#$%&'%()*+,-./0$%1!"#$%&'()*+,-./0!"123
!"#$!"#$%!"#$%&!"#$%&!"#$%&!"#$%&!"#$%&!"#$%&'()*+,-./012&3!"#$%N!"#$%&'()OMMM QMMM!"#$%&'!"#()*+,-.!"#$%&'()*+,-./012priclJ kvirob^=e ÖäóÄìêáÇÉI=ÖäáéáòáÇÉF=!"!"#$%&'()*+,-'()./012!"#$%&'%()*+,-./0$%1!"#$%&'()*+,-./0!"123
Long-Term Care Updates
 Long-Term Care Updates January 2019 By Kristina Nikl, PharmD Several recent studies evaluating the management of diabetes in older adults have concluded that 25-52% of elderly patients are currently being
Long-Term Care Updates January 2019 By Kristina Nikl, PharmD Several recent studies evaluating the management of diabetes in older adults have concluded that 25-52% of elderly patients are currently being
DIABETES MEDICAL MANAGEMENT PLAN (DMMP) School Year: Student s Name: Date of Birth:
 School Year: Student s Name: Date of Birth:") DIABETES MEDICAL MANAGEMENT PLAN (DMMP) School Year: Student s Name: Date of Birth: BLOOD GLUCOSE (BG) MONITORING: (Treat BG below 80mg/dl or above 150 mg/dl as outlined below.) Before meals as needed
DIABETES MEDICAL MANAGEMENT PLAN (DMMP) School Year: Student s Name: Date of Birth: BLOOD GLUCOSE (BG) MONITORING: (Treat BG below 80mg/dl or above 150 mg/dl as outlined below.) Before meals as needed
Current Clinical Practice Guideline for Diabetes Management
 Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Module 5. Understanding Insulin Therapy
 Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Module 5. Understanding Insulin Therapy EDUCATIONAL OBJECTIVES Upon completion of this activity, participants will be better able to: 1. Define the basic physiologic concept of basal-bolus insulin; 2.
Managing Special Circumstances Key Points
 Managing Special Circumstances Key Points Hypoglycaemia Dr Arla Ogilvie Diabetes Consultant (Watford) Sick Day Rules Janet Guest Community DSN (Hertford) Preparing for Colonoscopy Carolyn Jones In-Patient
Managing Special Circumstances Key Points Hypoglycaemia Dr Arla Ogilvie Diabetes Consultant (Watford) Sick Day Rules Janet Guest Community DSN (Hertford) Preparing for Colonoscopy Carolyn Jones In-Patient
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting
 Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
Meeting the Challenge of Inpatient Glycemic Management in the Non-Critical Care Setting Jane Jeffrie Seley, DNP, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner, Inpatient Diabetes
CGM Use in Pregnancy & Unique Populations ELIZABETH O. BUSCHUR, MD THE OHIO STATE UNIVERSITY WEXNER MEDICAL CENTER
 CGM Use in Pregnancy & Unique Populations ELIZABETH O. BUSCHUR, MD THE OHIO STATE UNIVERSITY WEXNER MEDICAL CENTER Case 1: CGM use during pregnancy 29 yo G1P0000 at 10 5/7 weeks gestation presents to set
CGM Use in Pregnancy & Unique Populations ELIZABETH O. BUSCHUR, MD THE OHIO STATE UNIVERSITY WEXNER MEDICAL CENTER Case 1: CGM use during pregnancy 29 yo G1P0000 at 10 5/7 weeks gestation presents to set
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
Diabetes: Three Core Deficits
 Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018
 Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018 Disclosures I have no Objectives Use a case-based format to discuss diabetes management pearls Discuss
Management: How Can We Do Better? Lori B. Sweeney, MD 2018 Virginia ACP Clinical Update March 17, 2018 Disclosures I have no Objectives Use a case-based format to discuss diabetes management pearls Discuss
Presented by Dr. Bruce Perkins, MD MPH Dr. Michael Riddell, PhD
 Type 1 Diabetes and Exercise: Optimizing the Medtronic MiniMed Veo Insulin Pump and Continuous Glucose Monitoring (CGM) for Better Glucose Control 1,2 for Healthcare Professionals Presented by Dr. Bruce
Type 1 Diabetes and Exercise: Optimizing the Medtronic MiniMed Veo Insulin Pump and Continuous Glucose Monitoring (CGM) for Better Glucose Control 1,2 for Healthcare Professionals Presented by Dr. Bruce
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES
 RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
RISK FACTORS OR COMPLICATIONS AND RECOMMENDED TREATMENT GOALS AND FREQUENCY OF EVALUATION FOR ADULTS WITH DIABETES Risk Factors or Complications Glycemic Control Fasting & Capillary Plasma Glucose Anti-platelet
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic
 Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Special thanks to the EJC Foundation for their support of Sanford Center Geriatric Specialty Clinic Sanford Center for Aging 775-784-4744 med.unr.edu/aging Diabetes Management Series: From Selfmanagement
Diabetes Medical Management Plan
 Date of Plan: Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian. It should be reviewed with relevant school staff and copies
Date of Plan: Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian. It should be reviewed with relevant school staff and copies
American Diabetes Association Standards of Medical Care in Diabetes 2018: Latest Updates
 American Diabetes Association Standards of Medical Care in Diabetes 2018: Latest Updates Juan Pablo Frias, MD President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty, University
American Diabetes Association Standards of Medical Care in Diabetes 2018: Latest Updates Juan Pablo Frias, MD President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty, University
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Individualizing Treatment Plans for Older Adults With T2DM
 Individualizing Treatment Plans for Older Adults With T2DM Key Slides from the Interactive Newsletter Hypoglycemia y in Older Adults Particularly dangerous, especially for those on insulin or secretagogues
Individualizing Treatment Plans for Older Adults With T2DM Key Slides from the Interactive Newsletter Hypoglycemia y in Older Adults Particularly dangerous, especially for those on insulin or secretagogues
CASE A2 Managing Between-meal Hypoglycemia
 Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
Managing Between-meal Hypoglycemia 1 I would like to discuss this case of a patient who, overall, was doing well on her therapy until she made an important lifestyle change to lose weight. This is a common
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 5 PURPOSE To assure that DOP inmates with Diabetes are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers are to follow these guidelines when treating
PAGE 1 of 5 PURPOSE To assure that DOP inmates with Diabetes are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers are to follow these guidelines when treating
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
Diabetes Medical Management Plan
 Diabetes Medical Management Plan 1 School District: School: School Year: Grade: Student Name: DOB: Provider Name: Phone #: Fax #: Blood Glucose Monitoring at School Blood Glucose Target Range: - mg/dl
Diabetes Medical Management Plan 1 School District: School: School Year: Grade: Student Name: DOB: Provider Name: Phone #: Fax #: Blood Glucose Monitoring at School Blood Glucose Target Range: - mg/dl
Physical Activity/Exercise Prescription with Diabetes
 Physical Activity/Exercise Prescription with Diabetes B R AD H I NTERMEYER C E P A C SM S A NFORD H E ALTH C A RDIAC R E H AB A N D D I ABE TES E XE RCISE The adoption and maintenance of physical activity
Physical Activity/Exercise Prescription with Diabetes B R AD H I NTERMEYER C E P A C SM S A NFORD H E ALTH C A RDIAC R E H AB A N D D I ABE TES E XE RCISE The adoption and maintenance of physical activity
Insulin Intensification: A Patient-Centered Approach
 MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
MARTIN J. ABRAHAMSON, MD Harvard Medical School, Boston, MA Insulin Intensification: A Patient-Centered Approach Dr Abrahamson is associate professor of medicine at Harvard Medical School and medical director
Insulin Basics. Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology
 Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Deepika Reddy MD Department of Endocrinology
 Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Afrezza Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Afrezza (human insulin) Prime Therapeutics will review Prior Authorization requests Prior Authorization
Afrezza Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Afrezza (human insulin) Prime Therapeutics will review Prior Authorization requests Prior Authorization
LOW BLOOD GLUCOSE (Hypoglycemia)
") Section Four DAILY CRISES In this section, you will learn about: Low blood glucose High blood glucose Diabetic Ketoacidosis Hyperosmolar Hyperglycemic Nonketotic Syndrome LOW BLOOD GLUCOSE (Hypoglycemia)
Section Four DAILY CRISES In this section, you will learn about: Low blood glucose High blood glucose Diabetic Ketoacidosis Hyperosmolar Hyperglycemic Nonketotic Syndrome LOW BLOOD GLUCOSE (Hypoglycemia)
Case Study. Patient Profile. Baseline Report - Daily Patterns. Insights
 Case Study Patient Profile Sex/Age: Male, elderly Disease diagnosis: Type 2 for the past 30 years, recurrent episodes of hunger HbA1c: 6.2% Diabetes medication profile: DPP-4 inhibitor 50 mg twice a day,
Case Study Patient Profile Sex/Age: Male, elderly Disease diagnosis: Type 2 for the past 30 years, recurrent episodes of hunger HbA1c: 6.2% Diabetes medication profile: DPP-4 inhibitor 50 mg twice a day,
A Guidance Statement from the American College of Physicians
 Hemoglobin A1c Targets for Glycemic Control with Pharmacologic Therapy in Non-Pregnant Adults with Type 2 Diabetes Mellitus: A Guidance Statement from the American College of Physicians Timothy J. Wilt,
Hemoglobin A1c Targets for Glycemic Control with Pharmacologic Therapy in Non-Pregnant Adults with Type 2 Diabetes Mellitus: A Guidance Statement from the American College of Physicians Timothy J. Wilt,
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Understanding Diabetes
 Patient Education Understanding Diabetes This handout describes diabetes, the complications related to the disease, and how you can prevent these complications. Blood Sugar Control Diabetes is a disease
Patient Education Understanding Diabetes This handout describes diabetes, the complications related to the disease, and how you can prevent these complications. Blood Sugar Control Diabetes is a disease
N ovel Strategies to M anage D iabetes in O lder A dults
 N ovel Strategies to M anage D iabetes in O lder A dults M edha M unshi, M.D. Beth Israel D eaconess M edical Center Joslin Diabetes Center Harvard M edical School Goals and Objectives Unique aspects of
N ovel Strategies to M anage D iabetes in O lder A dults M edha M unshi, M.D. Beth Israel D eaconess M edical Center Joslin Diabetes Center Harvard M edical School Goals and Objectives Unique aspects of
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
CASE STUDY #3 - NUT 116AL Diabetes Mellitus DUE Monday 12/9/13 (by 1:00pm in Meyer 3241)
") Last Name Reagan First Name Jason Section 2_ CASE STUDY #3 - NUT 116AL Diabetes Mellitus DUE Monday 12/9/13 (by 1:00pm in Meyer 3241) Patricia C. is a 30 yo Asian American woman with T1DM. She was diagnosed
Last Name Reagan First Name Jason Section 2_ CASE STUDY #3 - NUT 116AL Diabetes Mellitus DUE Monday 12/9/13 (by 1:00pm in Meyer 3241) Patricia C. is a 30 yo Asian American woman with T1DM. She was diagnosed
123 Are You Providing Evidence-Based Diabetes Care? - Martin
 Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Glycemic Management Hypoglycemic & Hyperglycemic Treatment Continuing Care
 Approved by: Glycemic Management Hypoglycemic & Hyperglycemic Continuing Care Senior Operating Officer, Addiction & Mental Health and Continuing Care, Edmonton Senior Operating Officer, Rural Services
Approved by: Glycemic Management Hypoglycemic & Hyperglycemic Continuing Care Senior Operating Officer, Addiction & Mental Health and Continuing Care, Edmonton Senior Operating Officer, Rural Services
Treatment guideline for adult patients with type 1 diabetes?
 Treatment guideline for adult patients with type 1 diabetes? Jae Hyeon Kim Division of Endocrinology and Metabolism, Samsung Medical Center, Sungkyunkwan University School of Medicine ICDM 2014 Treatment
Treatment guideline for adult patients with type 1 diabetes? Jae Hyeon Kim Division of Endocrinology and Metabolism, Samsung Medical Center, Sungkyunkwan University School of Medicine ICDM 2014 Treatment
Fine-tuning of The Dose of Insulin Pump
 Fine-tuning of The Dose of Insulin Pump The manual does not guarantee specific individual or specific applicability of the environment, there is no express or implied warranties. Contents of this manual
Fine-tuning of The Dose of Insulin Pump The manual does not guarantee specific individual or specific applicability of the environment, there is no express or implied warranties. Contents of this manual
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, :15 a.m. 11:00 a.m.
 Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, 2018 10:15 a.m. 11:00 a.m. Type 2 diabetes mellitus (T2DM) is closely associated with obesity, primarily through the link
Obesity Management in Patients with Diabetes Jamy D. Ard, MD Sunday, February 11, 2018 10:15 a.m. 11:00 a.m. Type 2 diabetes mellitus (T2DM) is closely associated with obesity, primarily through the link
DIABETES CARE TASKS AT SCHOOL: What Key Personnel Need to Know
 DIABETES CARE TASKS AT SCHOOL: What Key Personnel Need to Know HYPOGLYCEMIA Goal: Optimal Student Health and Learning Managing hypoglycemia is a vital piece of a comprehensive plan. 2 Learning Objectives
DIABETES CARE TASKS AT SCHOOL: What Key Personnel Need to Know HYPOGLYCEMIA Goal: Optimal Student Health and Learning Managing hypoglycemia is a vital piece of a comprehensive plan. 2 Learning Objectives
Current Glucometers. Junior s s Glucose Log. All have advantages and disadvantages Answer 2
 Diabetes Dilemmas: Using Technology To Solve Clinical Conundrums Stephen E. Gitelman, MD UCSF A teenager with type 1 diabetes for 5 years comes into your office for a follow- up visit. You want to review
Diabetes Dilemmas: Using Technology To Solve Clinical Conundrums Stephen E. Gitelman, MD UCSF A teenager with type 1 diabetes for 5 years comes into your office for a follow- up visit. You want to review
Disclosures. Glycemic Control in the Intensive Care Unit. Objectives. Hyperglycemia. Hyperglycemia. History. No disclosures
 Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
To test your basal rates it will be important that you keep the same schedule on the days you are testing. Do not do basal rate testing if you:
 Basal Rate Testing: Your provider has recommended that you complete one or more basal rate tests. These worksheets will help you in testing your pump settings and making small changes to make sure your
Basal Rate Testing: Your provider has recommended that you complete one or more basal rate tests. These worksheets will help you in testing your pump settings and making small changes to make sure your
Diabetes Medical Management Plan (DMMP) Adapted from Helping the Student with Diabetes Succeed: A Guide for School Personnel (2016)
 Adapted from Helping the Student with Diabetes Succeed: A Guide for School Personnel (2016)") Diabetes Medical Management Plan (DMMP) Adapted from Helping the Student with Diabetes Succeed: A Guide for School Personnel (2016) This plan should be completed by the student's personal diabetes health
Diabetes Medical Management Plan (DMMP) Adapted from Helping the Student with Diabetes Succeed: A Guide for School Personnel (2016) This plan should be completed by the student's personal diabetes health
Diabetes and Kids- Keeping them Safe at School. Presented by Vanessa Skolness, DNP, APRN-CNP, CDE March 30 th, Diabetes Summit
 Diabetes and Kids- Keeping them Safe at School Presented by Vanessa Skolness, DNP, APRN-CNP, CDE March 30 th, 2017- Diabetes Summit Objectives Brief review of type 1 and type 2 diabetes in children Discuss
Diabetes and Kids- Keeping them Safe at School Presented by Vanessa Skolness, DNP, APRN-CNP, CDE March 30 th, 2017- Diabetes Summit Objectives Brief review of type 1 and type 2 diabetes in children Discuss
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
APPENDIX #1: SAMPLE Diabetes Medical Management Plan (DMMP)
") APPENDIX #1: SAMPLE Diabetes Medical Management Plan (DMMP) Date of Plan: Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian.
APPENDIX #1: SAMPLE Diabetes Medical Management Plan (DMMP) Date of Plan: Diabetes Medical Management Plan This plan should be completed by the student s personal health care team and parents/guardian.
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING
 Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
Team-Based Approaches to Help Older Adults With Type 2 Diabetes Achieve Individualized Glycemic Goals
 Team-Based Approaches to Help Older Adults With Type 2 Diabetes Achieve Individualized Glycemic Goals 1. Which one of the agents listed here is widely considered the first-line therapy in type 2 diabetes
Team-Based Approaches to Help Older Adults With Type 2 Diabetes Achieve Individualized Glycemic Goals 1. Which one of the agents listed here is widely considered the first-line therapy in type 2 diabetes
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Date of birth: Type 2 Other: Parent/guardian 1: Address: Telephone: Home: Work: Cell: address: Camper physician / health care provider:
 Day & Evening Camp 2018 Specialized Health Care Diabetes Medical Management Plan Must be completed if your camper has diabetes. Parent/guardian and physician signature required. **We will also accept copies
Day & Evening Camp 2018 Specialized Health Care Diabetes Medical Management Plan Must be completed if your camper has diabetes. Parent/guardian and physician signature required. **We will also accept copies
Sample Exam Questions
 Disclaimer These are not validated questions. They have been created to enhance your learning and provide practice in reading and answering multiple choice questions. Some questions have been created to
Disclaimer These are not validated questions. They have been created to enhance your learning and provide practice in reading and answering multiple choice questions. Some questions have been created to
Special Situations 1
 Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Advanced Pharmacology Diabetes Homework
 Advanced Pharmacology Diabetes Homework Points: 25 Comments: Name: Tracy Hill WU ID #: 20015608 E-mail: tracy.hill@washburn.edu _TH I hereby certify that the work submitted is my own, and that I have not
Advanced Pharmacology Diabetes Homework Points: 25 Comments: Name: Tracy Hill WU ID #: 20015608 E-mail: tracy.hill@washburn.edu _TH I hereby certify that the work submitted is my own, and that I have not
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Understanding Type 1 Diabetes. Coach Training and Education
 Understanding Type 1 Diabetes Coach Training and Education 1 Training and Quiz When you have completed this slide presentation, please take the quiz at the end to check your understanding of this information.
Understanding Type 1 Diabetes Coach Training and Education 1 Training and Quiz When you have completed this slide presentation, please take the quiz at the end to check your understanding of this information.
Diabetes Medical Management Plan (DMMP)
") Diabetes Medical Management Plan (DMMP) This plan should be completed by the student s personal diabetes health care team, including the parents/guardian. It should be reviewed with relevant school staff
Diabetes Medical Management Plan (DMMP) This plan should be completed by the student s personal diabetes health care team, including the parents/guardian. It should be reviewed with relevant school staff
LEON COUNTY SCHOOLS DIABETES MEDICAL MANAGEMENT PLAN & NURSING CARE PLAN (School Year - ) Plan Effective Date(s):
 Plan Effective Date(s):") Student s Name: LEON COUNTY SCHOOLS DIABETES MEDICAL MANAGEMENT PLAN & NURSING CARE PLAN (School Year -) Plan Effective Date(s): Date of Diabetes Diagnosis: Type 1 Type 2 School Name: Date of Birth: School
Student s Name: LEON COUNTY SCHOOLS DIABETES MEDICAL MANAGEMENT PLAN & NURSING CARE PLAN (School Year -) Plan Effective Date(s): Date of Diabetes Diagnosis: Type 1 Type 2 School Name: Date of Birth: School
Diabetes Survival Skills
 Promoting Patient Survival with Diabetes Survival Skills Need to know skills for persons with diabetes Susan Zontine, NP-C WMC Diabetes Stewardship team May 18, 2015 Diabetes Chronic illness with serious
Promoting Patient Survival with Diabetes Survival Skills Need to know skills for persons with diabetes Susan Zontine, NP-C WMC Diabetes Stewardship team May 18, 2015 Diabetes Chronic illness with serious
CASE STUDY Diabetes Mellitus FH: PMH: Social Hx PE: Labs: Rx: CAM: Dx: Plan:
 CASE STUDY Diabetes Mellitus Patricia C. is a 30 yo Asian American woman with T1DM. She was diagnosed at age 13. Her insulin regimen is 50 units of insulin (Glargine) every evening and 3 units of Lispro
CASE STUDY Diabetes Mellitus Patricia C. is a 30 yo Asian American woman with T1DM. She was diagnosed at age 13. Her insulin regimen is 50 units of insulin (Glargine) every evening and 3 units of Lispro