NMQF. Washington DC 2014
|
|
|
- Georgia Farmer
- 5 years ago
- Views:
Transcription
1 NMQF Washington DC 2014

2 ACE/AACE Treatment Algorithm Jaime A. Davidson, MD, FACP, MACE Prof. of Medicine Division of Endocrinology, Diabetes and Metabolism President WorldWIDE Diabetes Advisor to the AACE BOD
3 Jaime Davidson, MD Disclosure Information Consultant, and/or an Advisory or Speaker s Board member: AstraZeneca Pharmaceuticals, Bristol-Myers Squibb Company, Bayer Pharmaceuticals, Eli Lilly & Co., Janssen, Roche Diagnostic, Johnson & Johnson, Merck-Sharp and Dome, Novo Nordisk and Sanofi. Dr. Davidson intends to reference unlabeled/unapproved uses of SGLT 2 inhibitors in his presentation.

4 Relationship between Glycemia and Complications DCCT and UKPDS Event Rate per 1000 Pt-Y 43% reduction in risk for every 10% decrease in HbA1c 37% reduction in risk for every 1% decrease in HbA1c DCCT UKPDS Current Mean HbA1c (%)
5 Why Does Diabetes Cost Us So Much? 1. Complications due to poor control 2. Litigious societies adding unnecessary cost to doctors visits, hospitals, pharmacies, medications, etc. 3. Access to care 4. Health education 5. Chronic and complex condition
6 Patients NOT receiving recommended care Diabetes: worst treated US illness 60% 55% Percentage NOT receiving recommended care 1 50% 46% 40% 30% 36% 35% 32% 20% 10% 0% Diabetes Colorectal cancer Congestive heart failure High blood pressure Coronary artery disease 1 McGlynn et al. N Engl J Med 2003;348:

7
8
9

10 Pathogenesis of Type 2 Diabetes An Evolving Concept Islet b-cell Impaired Insulin Secretion Decreased Incretin Effect Increased Lipolysis Islet a-cell Increased Glucagon Secretion Increased HGP Decreased Glucose Uptake Increased Glucose Reabsorption
11 Considerations for Therapy Selection Baseline HbA1c Efficacy profile Risk for hypoglycemia Risk for fractures Weight effects Adverse event profile Edema GI side effects (nausea, vomiting, diarrhea) Comorbidities Cardiovascular disease Renal impairment Costs and formulary availability
12 Properties of the Ideal Drug Robust HbA1c No hypoglycemia No weight gain Complimentary actions Durability Well tolerated Long-term safety Simple administration Added value e.g., BP, lipids, β cell function, CVD protection, etc.
13
14
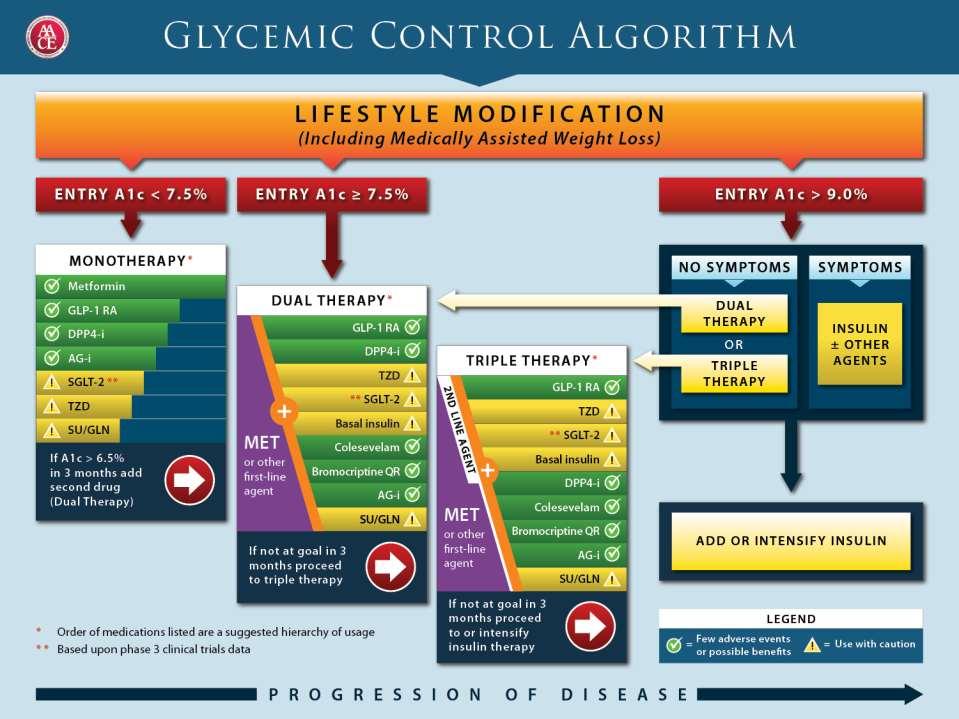
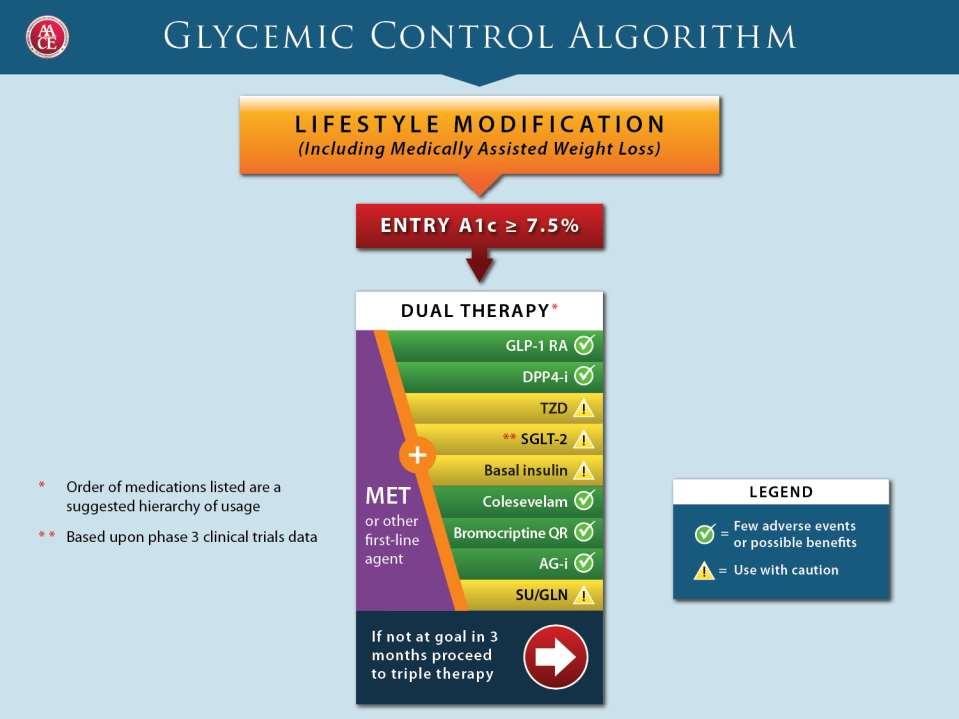
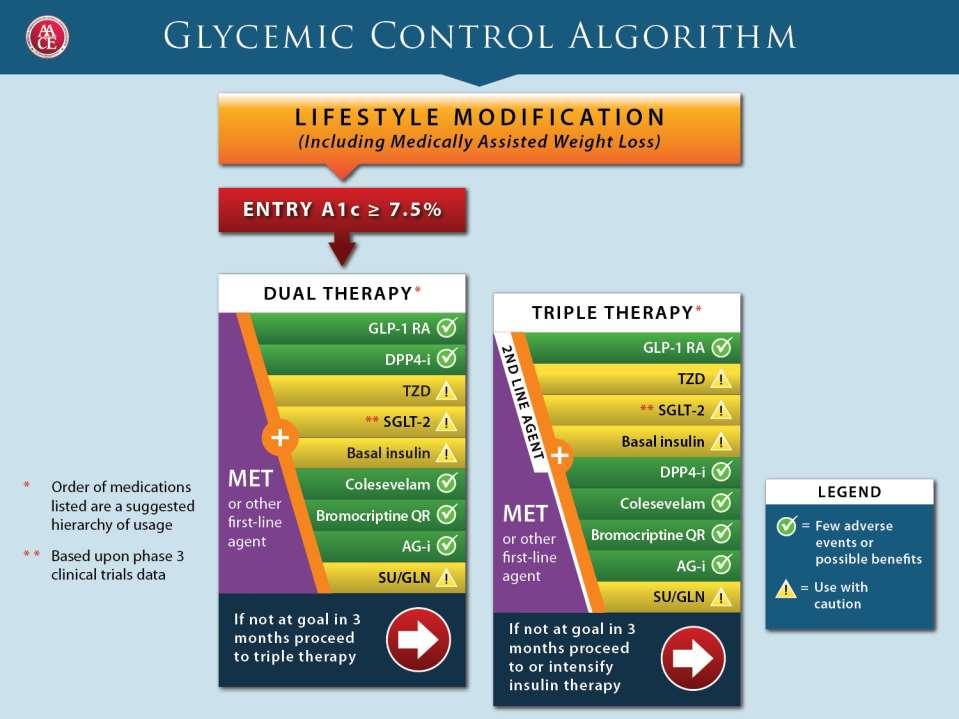
15 Endocrine Practice. 2009;15(6): AACE / ACE Diabetes Algorithm: Principles Prioritize medication choices according to safety, risk of hypoglycemia, efficacy, simplicity, anticipated degree of patient adherence and cost of medications. Stratify treatment choices based on A1C level. Recommend only combinations of medications approved by the FDA that provide complementary mechanisms of action.
16 Endocrine Practice. 2009;15(6): AACE / ACE Diabetes Algorithm: Principles Monitor therapy with A1C and SMBG. Adjust or advance therapy frequently (every 2 to 3 months) if appropriate goal has not been achieved. Provide a flowchart and table summarizing major considerations.

17 ADA? O High
18 AACE / ACE Diabetes Algorithm: Principles (2) Minimize risk of hypoglycemia and weight gain When other agents fail to achieve goal, advance to insulin therapy ± oral agents. Starting insulin with an A1c in the 7% range, AM prandial insulin may be best choice Endocrine Practice. 2009;15(6):
19 AACE / ACE Diabetes Algorithm: Principles (2) Individualize therapy for each patient Major cost of diabetes is due to complications, including hypoglycemia. Minimize total cost of care, not cost of medications per se Endocrine Practice. 2009;15(6):
20 % mortality Association of severe hypoglycaemia and risk of mortality in ACCORD 1 or more severe episodes No severe episodes 4 HR 1.41 HR Intensive group Standard group Bonds DE et al. Br Med J 2010; Gerstein HC et al. N Engl J Med 2008; Patel A et al. N Engl J Med 2008
21 Proportion reporting at least one severe hypo UK Study Group: Proportion experiencing at least 1 episode of severe hypoglycaemia over 9 12 months ns * * * Type 2 treated Type 2 < 2 yrs Type 2 > 5 yrs Type 1 < 5 yrs Type 1 > 15 yrs with sulfonylureas UK Hypoglycaemia Study Group. Diabetologia 2007
22 AACE / ACE Diabetes Algorithm: Principles (3) Lifestyle modification, diabetes education, and dietary consultation are essential, have major benefits, and should be initiated with medical therapy. Delay of pharmacotherapy is inappropriate because lifestyle interventions are usually not sufficient. Endocrine Practice. 2009;15(6):
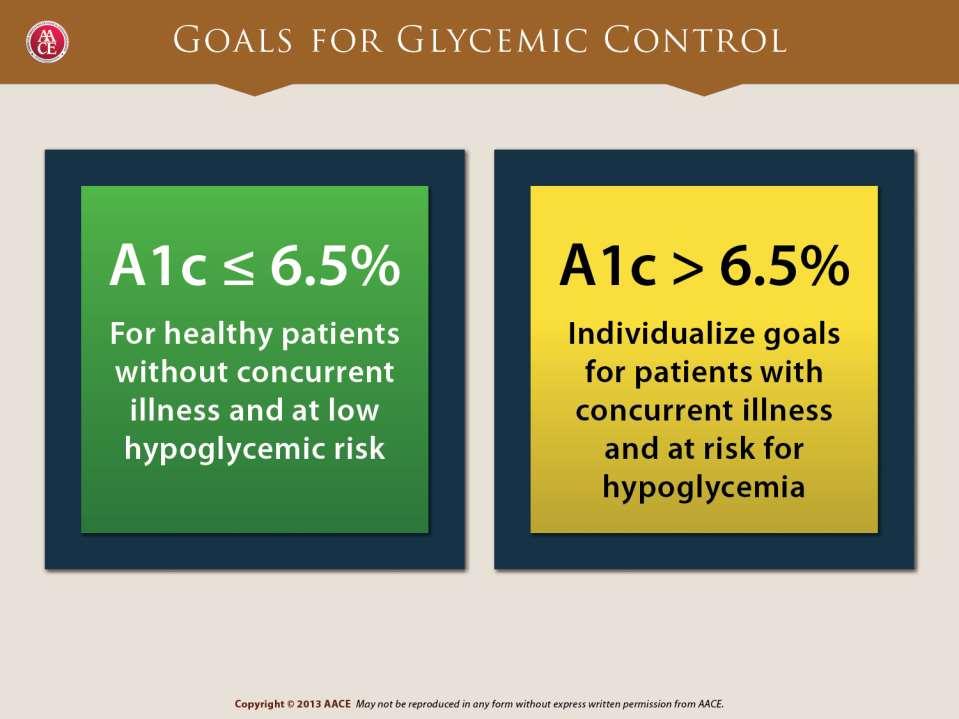
23 AACE / ACE Diabetes Algorithm: Principles (3) An A1C of 6.5% is recommended as the primary goal. This level must be customized for each patient considering: co-morbidities, duration of diabetes, history of hypoglycemia, hypoglycemia unawareness, patient education, motivation, adherence, age, life expectancy and other medications Endocrine Practice. 2009;15(6):
24 AACE / ACE Diabetes Algorithm: Principles (4) Rapid-acting insulin analogues are superior to regular human insulin and provide a better, safer alternative. yield better reproducibility and consistency between patients and within patients reduce risk of hypoglycemia Insulin regimens such as basal, basal-bolus, prandial, pre-mixed and CSII can be combined with a variety of oral agents. Basal analogues preferred Endocrine Practice. 2009;15(6):
25 Insulin Level (mu/ml) Glucose Insulin Rate (mg/min) Rapid Acting Analogues vs Regular Human Insulin Regular human insulin Insulin Lispro Time (hours) Time (hours) 0.05 U/kg (n = 6) 0.1 U/kg (n = 9) 0.2 U/kg (n = 9) 0.3 U/kg (n = 3) Woodworth, et al. Diabetes. 1993;42(suppl 1):54A.

26 Rapid Analogues vs Regular Human Insulin Analogues T max (hours)* Regular human * 0.2 U/kg SC. Diabetes Care. 1996;19:1437.
27 GIR (mg/kg/min) Basal Insulin Variability Same Patient NPH Glargine Detemir Time (hrs) Heise T et al. Diabetes 2004;53:
28 Major Advantages of the AACE Algorithm 1. Includes all major classes of medications 2. Does not relegate important agents to a second tier 3. Incretin analogs and DPP-4 inhibitors are not relegated to a category of too new. SGLT-2 inhibitors are also included 4. Suggested agents based on A1C level and targeted agent activity 5. Attempts to reduce total costs of care including costs related to hypoglycemia and complications 6. Simple graphical layout with emphasis on early intervention and A1c at presentation 7. Simplified table of Benefits and Risks of each medication


29 Early vs Late Intervention in Type 2 Diabetes Trial Intensive Arm HbA 1c Reduction No. Patients/ Trial Duration Disease Severity Goal: <6.0% CVD or 2 risk N=10,251 factors ACCORD Endpoint: 6.4% Early diagnosis and intensive 3.4 yr glucose 10 yr from T2DM 1.4% from BL in 4 months diagnosis control therapy from the start are the key to Goal: <6.5% Vascular disease N=11,140 or 1 risk factor ADVANCE long-term Endpoint: risk 6.5% reduction in diabetes 5.0 yr 8 yr from T2DM 0.6% from BL in 12 months diagnosis VADT UKPDS 80 Goal: 1.5% vs standard Endpoint: 6.9% 2.5% from BL in 3 months Goal: FPG <108 mg/dl Intervention endpoint: 7.0% Follow-up: 7.7% N= yr N= yr 12 yr from T2DM diagnosis Newly diagnosed with T2DM Macrovascular Benefit No Yes BL=baseline; T2DM=type 2 diabetes mellitus. Holman RR, et al. N Engl J Med. 2008;359: ; ACCORD Study Group. N Engl J Med. 2008;358: ; ADVANCE Collaborative Group. N En Med. 2008;358: ; Duckworth W, et al. N Engl J Med. 2009;360:
30 Elevated Mealtime Glucose Is a Concern at All Levels of HbA 1c HbA 1c Mean FPG % Patients With FPG >140 mg/dl Mean 2-h Glucose % Patients With 2-h Glucose >200 mg/dl < > In diagnosed and undiagnosed diabetes only from NHANES III ( ). FPG=fasting plasma glucose.


31 Mean HbA 1c at Last Visit Clinical Inertia: Standard Therapeutic Approaches Lead to Prolonged Hyperglycemia 10% Insulin Combination 9.6% Diet/Exercise Monotherapy Therapy 9% 8.6% 9.0% 8% 7% ACE Goal 6.5% 6% Diagnosis Years At insulin initiation, the average patient had 5 years with HbA 1c >8% 10 years with HbA 1c >7% Brown JB, et al. Diabetes Care. 2004;27:
32 A1C (%) Glucose control : 4 years of data in managed care (N 9376) SU TZD MET (n=2,373) (n=1,590) (n=5,453) Time (months) Riedel AA, et al. Diabetes. 2006;55(suppl 1):A132.
33 First Step- Metformin + Lifestyle Recognizes failure of life-style alone Inhibits hepatic glucose outputpredominantly lowers fasting glycemia Lowers HbA1c by ~1.5% No hypoglycemia Effective in obese and non-obese patients and in preventing diabetes in pre-diabetics (DPP) Glucophage off-patent, very inexpensive
34 Daily glycemic variation (mmol/l) by A1c levels in Breakfast type 2 diabetes 14 Fasting (nocturnal period) Postprandial (daytime period) Morning Period < Diabetes Duration (yrs) L Monnier,C Colette, G Dunseath and D Owens. Diabetes Care. 2007;30:
35 HbA1c (%) Initial Treatment : Insulin plus Metformin in Type 2 Diabetes HbA1c Results Baseline 3-month 5.9 Lingvay et al, J. Investigative Medicine 55: 62, 2007
36 Percent with First Adverse Event Phase 2b/3 Pooled Population Time to Onset of First Primary MACE HR 0.45 (95%CI ) Control n= BL Weeks Patients at Risk Control All SAXA All SAXA (n=3356) (Frederich R, et al. Postgraduate Medicine 2010;122(3). doi: /pgm )
37 Hypoglycemic Events & Change in Weight from Baseline Number (%) of subjects with a hypoglycemic event SAXA + MET (N=428) 13 (3.0%) GLIP + MET (N=430) 156 (36.3%) Difference in proportions vs. glipizide + metformin [95%CI] -33.2% [-38.1%,-28.5%] <0.0001* Adjusted change in weight from baseline, mean (%) Mean difference vs. glipizide + metformin [95%CI] -1.1 kg (0.17%) -2.2 kg [-2.7,-1.7] <0.0001* +1.1 kg (0.17%) * Between group comparison significant after controlling overall alpha of the study B. Goke. Int J Clin Pract Nov;64(12):

38 Liraglutide resulted in weight loss SU resulted in weight gain Japanese study Liraglutide 0.9 mg Glibenclamide 2.5 mg p< to Weeks Liraglutide 0.9 mg Glibenclamide 2.5 mg Analysis population: all subjects with baseline and week 24 measurements (LOCF) Statistical analysis: ANOVA model with treatment group and pre-trial treatment as fixed effects and baseline value as a covariate Trial ID: NN
39 GLP and DPP4 Inhibitors GLP and its Analogues Stimulate insulin secretion Suppress glucagon Slow motility Lower A1c by ~1.0%/1.5% 1-2 injections per day or once weekly Weight loss of ~ 5 lb Associated with nausea, vomiting, diarrhea in ~40% Expensive DPP 4 Inhibitors Inhibit breakdown of endogenous GLP, raising levels by ~2- fold Decrease A1c by ~0.6% Oral medication No weight loss No GI side-effects Expensive
40 Rationale for SGLT2 Inhibitors Inhibit glucose reabsorption in the renal proximal tubule Resultant glucosuria leads to a decline in plasma glucose and reversal of glucotoxicity This therapy is simple and nonspecific Even patients with refractory type 2 diabetes are likely to respond SGLT2=sodium-glucose cotransporter 2.
41 Normal Kidney Glomerulus Proximal Convoluted Tubule Early Distal Glucose reabsorption into systemic circulation Glucose SGLT2 SGLT1 Adapted with permission from Rothenberg PL et al. SGLT = sodium-glucose co-transporter. 1. Kanai Y et al. J Clin Invest. 1994;93(1): You G et al. J Biol Chem. 1995;270(49): Rothenberg PL et al. Presented at: 46th European Association for the Study of Diabetes Annual Meeting; September 20-24, 2010; Stockholm, Sweden. 41
42 Urinary Glucose Excretion (g/d) Type 2 diabetes + SGLT-2 Inhibitor (70-90 mg/dl) RT G Non-diabetic (180 mg/dl) RT G Type 2 diabetes (240 mg/dl) RT G Plasma Glucose (mg/dl) Adapted with permission from Abdul-Ghani MA, DeFronzo RA. RT G = renal threshold for glucose excretion. 1. Cowart SL, Stachura ME. In: Walker HK et al, eds. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston, MA: Butterworths; 1990: Abdul-Ghani MA, DeFronzo RA. Endocr Pract. 2008;14(6): Nair S, Wilding JP. J Clin Endocrinol Metab. 2010;95(1): INVOKANA [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals, Inc.; Rave K et al. Nephrol Dial Transplant. 2006;21(8): Oku A et al. Diabetes. 1999;48(9):

43 Treatment with SGLT-2 Inhibitor Glomerulus Proximal Convoluted Tubule Early Distal Glucose in urine Decreased glucose reabsorption into systemic circulation Glucose SGLT2 SGLT2 inhibitor SGLT1 Adapted with permission from Rothenberg PL et al. SGLT = sodium-glucose co-transporter. 1. Rothenberg PL et al. Poster presented at: 46th European Association for the Study of Diabetes Annual Meeting; September 20-24, 2010; Stockholm, Sweden. 3. Cowart SL, Stachura ME. In: Walker HK et al, eds. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd ed. Boston, MA: Butterworths; 1990: Abdul-Ghani MA, DeFronzo RA. Endocr Pract. 2008;14(6): Oku A et al. Diabetes. 1999;48(9):
44 50 mg qd 100 mg qd 200 mg qd 300 mg qd 300 mg bid Sitagliptin 1 mg qd 5 mg qd 10 mg qd 25 mg qd 50 mg qd Sitagliptin Change in HbA1c in 12-Week Add-on to Metformin Studies of SGLT2 Inhibitors Canagliflozin (placebo adjusted values) 12 wk study (N=451) Empagliflozin (placebo adjusted values) 12 wk study (N=495) Mean change in HbA1c (%) from baseline Mean Baseline HbA1c, % Statistical significance not reported Rosenstock J, et al. Diabetologia 2010;53(Suppl 1):S349; Seman L, et al. Presented at EASD Annual Meeting, Lisbon, September 2011 (abstract #147). Canagliflozin & Empagliflozin not FDA approved
45 Caveats Although the algorithm should apply to most people with type 2 diabetes, it does not apply to all Individualize therapy is a must May select different glycemic goals - Elderly - Persons with projected life span too short to benefit - Persons in whom side-effects outweigh benefits May select different medications based on - Patient acceptance, tolerance - Specific risk factors Don t forget other interventions- lipids, blood pressure, CVD prevention
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
SESSION 4 12:30pm 1:45pm
 SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
GLP-1RA and insulin: friends or foes?
 Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Tresiba Expert Panel Meeting 28/06/2014 GLP-1RA and insulin: friends or foes? Matteo Monami Careggi Teaching Hospital. Florence. Italy Dr Monami has received consultancy and/or speaking fees from: Merck
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011
 New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit?
 Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH
 CHIEF OF MEDICINE, SOUTH WEST HEALTH") Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Insulin Initiation BRIAN MOSES, MD, FRCPC (INTERNAL MEDICINE) CHIEF OF MEDICINE, SOUTH WEST HEALTH Disclosures In the past 12 months, I have received speakers honoraria from AstraZeneca, Boehringer Ingelheim,
Updates in Diabetes Care
 Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Faculty. Timothy S. Reid, MD (Co-Chair, Presenter) Medical Director Mercy Diabetes Center Janesville, WI
 Medical Director Mercy Diabetes Center Janesville, WI") Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Activity Overview In this case-based webcast, meet Jackie, a 62-year-old woman with type 2 diabetes. Her glycated hemoglobin (HbA1C) is 9.2%, and she is taking 2 oral agents and basal insulin; however,
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Combination treatment for T2DM
 Combination treatment for T2DM Date of approval: December 2016 SAGLB.DIA.16.08.0657 Abbreviations ADA: American Diabetes Association CVD: Cardiovascular disease DPP-4: Dipeptidyl Peptidase-4 EASD: European
Combination treatment for T2DM Date of approval: December 2016 SAGLB.DIA.16.08.0657 Abbreviations ADA: American Diabetes Association CVD: Cardiovascular disease DPP-4: Dipeptidyl Peptidase-4 EASD: European
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Galvus the most comprehensively studied DPP-4 inhibitor
 Galvus the most comprehensively studied DPP-4 inhibitor! >7 000 patients enrolled in clinical studies! >4 00 patients exposed to Galvus >1 300 patients exposed 2 weeks >300 patients exposed for 104 weeks!
Galvus the most comprehensively studied DPP-4 inhibitor! >7 000 patients enrolled in clinical studies! >4 00 patients exposed to Galvus >1 300 patients exposed 2 weeks >300 patients exposed for 104 weeks!
Exploring Non-Insulin Therapies in Type 1 Diabetes
 Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Diabetes: Three Core Deficits
 Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
A Clinical Context Report
 Type 2 Diabetes in Practice An Expert Commentary with Silvio E. Inzucchi, MD A Clinical Context Report Clinical Context: Type 2 Diabetes in Practice Expert Commentary Jointly Sponsored by: and Clinical
Type 2 Diabetes in Practice An Expert Commentary with Silvio E. Inzucchi, MD A Clinical Context Report Clinical Context: Type 2 Diabetes in Practice Expert Commentary Jointly Sponsored by: and Clinical
Metabolic Karma. - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D
 2014 ICDM Breakfast Symposium. Oct 18, 2014 Grand Hilton, Seoul Metabolic Karma - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D Department of Endocrinology and Metabolism, Hallym University
2014 ICDM Breakfast Symposium. Oct 18, 2014 Grand Hilton, Seoul Metabolic Karma - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D Department of Endocrinology and Metabolism, Hallym University
Pramlintide & Weight. Diane M Karl MD. The Endocrine Clinic & Oregon Health & Science University Portland, Oregon
 Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Role of incretins in the treatment of type 2 diabetes
 Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Insulin and Post Prandial
 Insulin and Post Prandial Pr Luc Martinez PCDE Meeting Barcelona 2016 Conflicts of interest disclosure Advis consultant f Amgen Inc.; AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Ipsen; Lilly; Mayoly
Insulin and Post Prandial Pr Luc Martinez PCDE Meeting Barcelona 2016 Conflicts of interest disclosure Advis consultant f Amgen Inc.; AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Ipsen; Lilly; Mayoly
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
INSULIN THERAPY. Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital
 INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Basal & GLP-1 Fixed Combination Use
 Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Disclosures of Interest. Publications Diabetologia Key points to emphasize
 Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
Hanyang University Guri Hospital Chang Beom Lee
 Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Taking Translation into the Clinic: Can We Improve the Probability of Success?
 Taking Translation into the Clinic: Can We Improve the Probability of Success? Janssen R&D/Cardiovascular & Metabolism Therapeutic Area Nicholas Di Prospero, MD, PhD Translational Medicine Group Disclaimer:
Taking Translation into the Clinic: Can We Improve the Probability of Success? Janssen R&D/Cardiovascular & Metabolism Therapeutic Area Nicholas Di Prospero, MD, PhD Translational Medicine Group Disclaimer:
Case Report Off-Label Use of Liraglutide in the Management of a Pediatric Patient with Type 2 Diabetes Mellitus
 Case Reports in Pediatrics Volume 2013, Article ID 703925, 4 pages http://dx.doi.org/10.1155/2013/703925 Case Report Off-Label Use of Liraglutide in the Management of a Pediatric Patient with Type 2 Diabetes
Case Reports in Pediatrics Volume 2013, Article ID 703925, 4 pages http://dx.doi.org/10.1155/2013/703925 Case Report Off-Label Use of Liraglutide in the Management of a Pediatric Patient with Type 2 Diabetes
Glycemic control what can be achieved with life-style and when and how to use pharmacological agents?
 Glycemic control what can be achieved with life-style and when and how to use pharmacological agents? Eberhard Standl Munich Diabetes Research Institute At the Munich Helmholtz Center Pathogenetic key
Glycemic control what can be achieved with life-style and when and how to use pharmacological agents? Eberhard Standl Munich Diabetes Research Institute At the Munich Helmholtz Center Pathogenetic key
SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk
 Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale