Paediatric Renal Disease
|
|
|
- Abraham Webb
- 5 years ago
- Views:
Transcription
1 Pharmacy Department Paediatric Renal Disease NUH Pharmacy
2 At the end of the session you should be able to: Determine the level/type of renal dysfunction in a child and what the implications might be for drug dosing. Identify common drug causes of Acute Kidney Injury and ways in which damage can be minimised or avoided. Describe the key features of Nephrotic Syndrome and outline the management of this condition.

3 Quiz NUH Pharmacy

4 What is normal?
5 Renal Dose Adjustments Calculate egfr using the Schwartz equation Child over 1 year: Estimated GFR (ml/min/1.73 m 2 )= 40 height (cm) serum creatinine (micromol/l) Neonate: Estimated GFR (ml/min/1.73 m 2 )= 30 height (cm) serum creatinine (micromol/l)
6 (Unless you are in Nottingham.)
7 Paediatric Renal Dosing BNFC Renal Drug Handbook Others.?
8 BNFC Cefuroxime Gentamicin
9 Others Drug Prescribing in Renal Failure, 5th Edition- Aronoff Micromedex Lexicomp / Up to Date
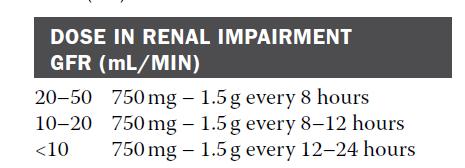
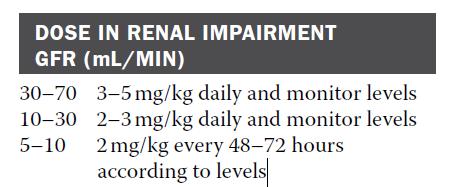
10 Renal Drug Handbook/Database Cefuroxime: Gentamicin:
11 Acute Kidney Injury
12 Case 1

13 Grading of AKI
14 Causes of AKI Pre-renal Sepsis Dehydration Shock Medication Post-renal Medication Obstruction Intra-renal Endotoxin Immune mediated Medication
15 Drug-Induced Pre-renal AKI Hypovolaemia: Excessive renal fluid loss: inappropriate use of diuretics. Systemic Hypotension: Usually due to cardiogenic shock/sepsis, but can arise due to pharmacological vasodilatation Renal Hypoperfusion: Afferent Arteriolar Constriction: NSAIDs, amphotericin, ciclosporin, adrenaline, noradrenaline Efferent Arteriolar Dilatation: ACE Inhibitors (ACEIs), Angiotensin II Inhibitors (ARBs)
16 ACEIs, ARBs and the Kidney Contraindicated in bilateral renal artery stenosis. Creatinine usually rises on starting/dose increase: NICE CCF Guideline: If egfr change is >25% or plasma creatinine >30% AND no other causes of deterioration is found stop ACEI/ARB or reduce dose to previously tolerated dose. Reno-protective in diabetic and non-diabetic microalbuminuria / proteinuria, irrespective of whether BP raised or not
17 Drug-induced Intra-renal AKI Drug Statins Contrast Media Aminoglycosides Effect on kidney Induce rhabdomyolysis Renal vasoconstriction & free radical production Direct toxic effect on tubular cells
18 Drug-Induced Post-Renal AKI Drug causes rare- due to obstruction of urine flow: Retroperitoneal haemorrhage due to overanticoagulation: bleeding creates external pressure on the ureters Retroperitoneal fibrosis: methotrexate, beta-blockers Crystallisation of urate and stone formation within the ureter: Tumour lysis syndrome Other drugs include: aciclovir, acetazolamide, cisplatin and naftidofuryl, topiramate, mirtazepine, risedronate
19 Medication Review in AKI Avoid and/or stop known nephrotoxins- where possible Avoid drugs which raise serum potassium. Stop/review antihypertensives (including diuretics). Adjust doses of drugs which are to continue in light of reduced renal clearance. Start with low doses and titrate slowly. Consider if alternative drug may be more suitable. Monitor levels whenever you can.
20 Not all cases are quite so obvious 9 year old girl Abdominal pain, joint pain and fever-? Cause Treated with cefuroxime No improvement Day 3: Trough level 5mg/L Dose increased by 20% Day 5: Trough level 8mg/L Serum creatinine 60 micromol/l Increased to 6-hourly Vancomycin added 15mg/kg 8-hourly Day 8: Trough level 25mg/L Serum creatinine 135 micromol/l
21 Not all cases are quite so obvious What are the possible learning points from this case? What information is missing? NUH Pharmacy
22 Not all cases are quite so obvious Learning points: Rapid increase in dose and frequency. Initial creatinine 25 micromol/l- increase not identified Concomitant use of NSAID not identified, Poor communication of plan to stop vanc
23 Prevention Avoid Nephrotoxic preparations / combinations. If unavoidable, monitor patients very closely. Remember that 25-50% of kidney function may have been lost before any rise in creatinine seen. Sick day rules for patients on ACE Inhibitors / ARBs. Be alert to the risk factors.

24 Sick Day Rules for ACE Inhibitors/ARBs NUH Pharmacy
25 Risk Factors for AKI Pre-renal: Limited access to fluids. Hypovolaemia and / or hypotension Sepsis Deteriorating PEWS Others: Heart Failure Liver Disease Haematological maligancy Nephrotoxic drugs Intra-renal: Chronic Kidney Disease History of AKI or oliguria Severe diarrhoea, particularly bloody diarrhoea. Signs or symptoms of nephritis Urinary obstruction. Renal Transplant
26 Nephrotic Sydrome
27 What is it?
28 What is it? Characterised by: Heavy proteinuria (protein:creatinine ratio > 250mg/mmol). Hypoalbuminaemia (serum albumin <25g/l). Oedema. Relapsing/Remitting Condition. Annual incidence in the UK of 2 per 100,000 children. More common in children from South Asia with an incidence up to 16 per children.
29 Initial Treatment Aim is to induce remission with steroids and therefore promote diuresis. Most patients respond within 7-14 days. Prednisolone 60mg/m 2 (max 80mg) once daily for 28 days, then 40 mg/m 2 on alternate days for the next 28 days and then stop. Intensified Regimen: Weeks 1-4: 60 mg/m 2 /day Weeks 5 8: 40 mg/m 2 on alternate days Weeks 9 12: 25 mg/m 2 on alternate days Weeks mg/m 2 then stop. PREDNOS Study Children who do not respond to prednisolone within 28 days need a renal biopsy.
30 Preventing Complications Hypovolaemia Increases the risk of thrombosis. Tachycardia, hypertension, cool peripheries and delayed capillary refill time. If severe consider albumin and thromboprophylaxis. Give albumin if symptomatic hypovolaemia or severe diuretic resistant oedema. Shock: 4.5% albumin 20 ml/kg over mins repeated if necessary. Mild hypovolaemia + oedema = 20% albumin 5 ml/kg (1g/kg) over 4 hrs. Preventing Thrombosis: Avoid hypovolaemia Prevent sepsis Encourage mobilisation and avoid bedrest Consider TEDS and LMWH.
31 Preventing Complications Oedema and Ascites: Fluid restriction and low salt diet. Diuretics if severe/worsening oedema/ascites in the absence of hypovolaemia. Usually furosemide and spironolactone. Can add metolazone. Infection: Oral Penicillin V given to oedematous/ascitic patients to protect against pneumococcal infection. 125 mg twice daily if 0-5yrs 250 mg twice daily 5-12 yrs 500mg twice daily if > 12 years. Give Pneumovax II pneumococcal vaccine if not already given.
32 Classification Steroid Sensitive (SSNS). Steroid Resistant (SRNS). Frequently Replapsing (FRNS). Steroid Dependant (SDNS).
33 Steroid Sensitive NS Most cases will respond completely to steroids. Some will fail to come off steroids completely. 80% will have a relapse: May be frequent
34 Relapses Often triggered by viral infection. Treated with high dose steroids to induce remission. May be possible to prevent relapses by giving a low dose of daily steroids for 5 days at the time of an URTI without waiting for proteinuria to develop. Potential to have a large impact on long-term steroid burden. Subject of a national multicentre trial, PREDNOS2.
35 Steroid Dependant / Frequently Relapsing NS
36 Levamisole Increased likelihood of remission when given for 16 weeks May be best suited in frequent relapsers who are not steroid dependent. Takes several months to become effective. Usually started alongside slow steroid wean. Dose: 2.5 mg/kg (max 150 mg) on alternate days. Can crush tablets. Side-effects: leucopenia, gastro-intestinal effects and vasculitis. Monitor FBC and cunsel parents to seek medical attention if unusual or severe infection. Usually continued for at least 1-2 years.
37 Cyclophosphamide Significantly reduces risk of relapse in FRNS. Dose 2-3mg/kg orally once daily for 8 weeks. Alternate day dosing with tablets. Liquid special. Generally well tolerated: Weekly FBC during treatment. May lead to hair thinning Minimal effect on fertility. Preferred second-line agent in pre-pubertal children where there is steroid dependence. In peri- and post-pubertal children consider tacrolimus instead due to a theoretical increased risk of gonadal toxicity at this age. IV alternative to oral if concern about concordance 500 mg/m 2 monthly for 6 months.
38 Tacrolimus Effective at reducing frequency of relapses. Usually 3 rd line agent. Starting dose 0.15 mg (max 5mg) twice daily. Target trough level 4-8 nanograms/ml. Prescribe/dispense by brand: Prograf, Adoport, Modigraf, Adoport. If relapse free after 2 years on tacrolimus, it should be stopped. If early relapse, restart after induction of remission with prednisolone. If taking for >2 years, renal biopsy needed. If significant nephrotoxicity, switched to rituximab or mycophenolate. Dose related side-effects: headache, tremor, abdo pain, visual disturbance and hyperglycaemia.
39 Rituximab Indications: Frequent relapses on tacrolimus SRNS unresponsive to 3 months of tacrolimus FRNS/SDNS if poor concordance tacrolimus or levamisole Life-threatening nephrotic complications In FRNS/SDNS, usually consolidates remission for at least 6 months Dose: 375 mg/m 2 : Increasing rate, pre-med. Hepatitis B status must be determined before starting. Repeat dose on relapse / B-cell repopulation. Long-term effects not known. On current evidence, give maximum 4 prophyactic doses before waiting to see if in long-term remission.
40 Mycophenolate Effective as add-on agent when already on tacrolimus: Some evidence as a sole prophylactic agent less effective than ciclosporin or tacrolimus. If used with tacrolimus, dose is 300 mg/m 2 bd but due to GI side effects often started at lower dose initially. Dose if used without tacrolimus is 600 mg/m 2 bd, but again start at low dose. Prescribe by brand.
41 Steroid Resistant NS If unresponsive after 4 weeks of prednisolone give methylprednisolone (300 mg/m 2 ) for 3 days. If no response renal biopsy indicated. Tacrolimus then usually commenced. Followed if needed by rituximab. Focal and segmental sclerosis (FSGS) More steroid-resistant disease with a poorer prognosis Other drugs to consider for persistent nephrotic states: ACE inhibitors and ARBs; statins; and anticoagulants or antiplatelets.


42 Any questions?
43 NUH Pharmacy
Childhood nephrotic syndrome practice guidelines
 Childhood nephrotic syndrome practice guidelines Dr Shuman Haq Consultant Paediatric Nephrologist Southampton Children s Hospital Definitions Nephrotic syndrome Proteinuria Urine protein : creatinine >200
Childhood nephrotic syndrome practice guidelines Dr Shuman Haq Consultant Paediatric Nephrologist Southampton Children s Hospital Definitions Nephrotic syndrome Proteinuria Urine protein : creatinine >200
Management of Nephrotic Syndrome
 Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Guidelines for the management of Nephrotic syndrome in children
 Guidelines for the management of Nephrotic syndrome in children Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the author(s)
Guidelines for the management of Nephrotic syndrome in children Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the author(s)
This guideline describes the assessment and management of children and young people with nephrotic syndrome Key Words
 Nephrotic Syndrome Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline for the assessment and management of nephrotic
Nephrotic Syndrome Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Guideline for the assessment and management of nephrotic
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Clinical trials in childhood steroid sensitive nephrotic syndrome: the PREDNOS studies
 Clinical Research Facility Central Manchester University Hospitals NHS Foundation Trust Clinical trials in childhood steroid sensitive nephrotic syndrome: the PREDNOS studies Professor Nick Webb DM FRCP
Clinical Research Facility Central Manchester University Hospitals NHS Foundation Trust Clinical trials in childhood steroid sensitive nephrotic syndrome: the PREDNOS studies Professor Nick Webb DM FRCP
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
CKD IN THE CLINIC. Session Content. Recommendations for commonly used medications in CKD. CKD screening and referral
 CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome
 P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
Acute Renal Failure. Dr Kawa Ahmad
 62 Acute Renal Failure Dr Kawa Ahmad Acute Renal Failure It is characterised by an abrupt reduction (usually within a 48- h period) in kidney function. This results in an accumulation of nitrogenous waste
62 Acute Renal Failure Dr Kawa Ahmad Acute Renal Failure It is characterised by an abrupt reduction (usually within a 48- h period) in kidney function. This results in an accumulation of nitrogenous waste
Cisplatin / Capecitabine (+ Trastuzumab) in Gastric Cancer
 in Gastric Cancer") Cisplatin / Capecitabine (+ Trastuzumab) in Gastric Cancer Page 1 of 5 Indication: Confirmed HER2-positive (3+ or FISH+) metastatic adenocarcinoma of the stomach or gastrooesophageal junction. Patient
Cisplatin / Capecitabine (+ Trastuzumab) in Gastric Cancer Page 1 of 5 Indication: Confirmed HER2-positive (3+ or FISH+) metastatic adenocarcinoma of the stomach or gastrooesophageal junction. Patient
Southern Derbyshire Shared Care Pathology Guidelines. AKI guidelines for primary care
 Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: Flow Diagram: Recommended response time to AKI warning stage test results for adults in primary care 2 Table
Southern Derbyshire Shared Care Pathology Guidelines AKI guidelines for primary care Contents: Flow Diagram: Recommended response time to AKI warning stage test results for adults in primary care 2 Table
Nephrotic syndrome in children. Bashir Admani KPA Nephrology Precongress 24/4/2018
 Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Doncaster & Bassetlaw. AKI guidelines for primary care
 Doncaster & Bassetlaw AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE... 2 FLOW DIAGRAM: MANAGEMENT OF HYPERKALAEMIA.... 3 FLOW DIAGRAM:
Doncaster & Bassetlaw AKI guidelines for primary care Contents: FLOW DIAGRAM: MANAGEMENT OF PATIENTS WITH AKI DETECTED IN PRIMARY CARE... 2 FLOW DIAGRAM: MANAGEMENT OF HYPERKALAEMIA.... 3 FLOW DIAGRAM:
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Bulletin Independent prescribing information for NHS Wales
 Bulletin Independent prescribing information for NHS Wales October 2017 Chronic kidney disease Chronic kidney disease (CKD) is a long-term irreversible deterioration in the function of the kidneys, often
Bulletin Independent prescribing information for NHS Wales October 2017 Chronic kidney disease Chronic kidney disease (CKD) is a long-term irreversible deterioration in the function of the kidneys, often
Renal Transporters- pathophysiology of drug - induced renal disorders. Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November
 Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Renal Transporters- pathophysiology of drug - induced renal disorders Lisa Harris, Pharmacist, John Hunter Hospital, Newcastle, 2015 November Renal Failure Up to 25% of acute renal failure is drug induced
Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org & 2012 KDIGO Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, 172 176; doi:10.1038/kisup.2012.17 INTRODUCTION This
http://www.kidney-international.org & 2012 KDIGO Chapter 4: Steroid-resistant nephrotic syndrome in children Kidney International Supplements (2012) 2, 172 176; doi:10.1038/kisup.2012.17 INTRODUCTION This
Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck
 Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck Indication: 1) Concomitant chemo-radiotherapy for locally advanced squamous cell carcinoma head and neck 2) Post-operative
Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck Indication: 1) Concomitant chemo-radiotherapy for locally advanced squamous cell carcinoma head and neck 2) Post-operative
Patient details GP details Specialist details Name GP Name Dr Specialist Name Dr R. Horton
 Rationale for Initiation, Continuation and Discontinuation (RICaD) Sacubitril/Valsartan (Entresto) For the treatment of symptomatic heart failure with reduced ejection fraction (NICE TA388) This document
Rationale for Initiation, Continuation and Discontinuation (RICaD) Sacubitril/Valsartan (Entresto) For the treatment of symptomatic heart failure with reduced ejection fraction (NICE TA388) This document
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus
 Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Swindon Diabetes Guidelines: Management of Chronic Kidney Disease Associated with Diabetes Mellitus 1 Contents Executive Summary... 3 How to Screen for Diabetic Nephropathy... 4 What to Measure... 4 Frequency
Shared Care Guideline Metolazone for fluid management in CKD (Adults)
") Shared Care Guideline Metolazone for fluid management in CKD (Adults) It is vital for safe and appropriate patient care that there is a clear understanding of where clinical and prescribing responsibility
Shared Care Guideline Metolazone for fluid management in CKD (Adults) It is vital for safe and appropriate patient care that there is a clear understanding of where clinical and prescribing responsibility
0BCore Safety Profile. Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg SE/H/PSUR/0024/003 Date of FAR:
/strength: Film-coated tablet 40, 80, 160, 320 mg SE/H/PSUR/0024/003 Date of FAR:") 0BCore Safety Profile Active substance: Valsartan Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg P-RMS: SE/H/PSUR/0024/003 Date of FAR: 28.02.2013 4.2 Posology and method of administration
0BCore Safety Profile Active substance: Valsartan Pharmaceutical form(s)/strength: Film-coated tablet 40, 80, 160, 320 mg P-RMS: SE/H/PSUR/0024/003 Date of FAR: 28.02.2013 4.2 Posology and method of administration
Mycophenolate Mofetil (MMF)
") SCG: For Transplant patients The following guidelines are designed to provide information relating to mycophenolate mofetil and to outline the responsibilities of the primary and secondary care teams in
SCG: For Transplant patients The following guidelines are designed to provide information relating to mycophenolate mofetil and to outline the responsibilities of the primary and secondary care teams in
Obinutuzumab+Bendamustine followed by Obinutuzumab Maintenance Burton in-patient Derby in-patient Burton day-case Derby day-case
 Obinutuzumab+Bendamustine followed by Obinutuzumab Maintenance Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby out-patient Available
Obinutuzumab+Bendamustine followed by Obinutuzumab Maintenance Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby out-patient Available
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update)
") Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Acute Kidney Injury in The Acute Oncology Patient
 Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
Acute Kidney Injury in The Acute Oncology Patient Dr Andrew Lewington BSc MEd MD FRCP Consultant Renal Physician/Honorary Senior Lecturer Leeds Teaching Hospitals Definition Definitions and terminology
WEEK. MPharm Programme. Acute Kidney Injury. Alan M. Green MPHM13: Acute Kidney Injury. Slide 1 of 47
 MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
MPharm Programme Acute Kidney Injury Alan M. Green 2017 Slide 1 of 47 Overview Renal Function What is it? Why does it matter? What causes it? Who is at risk? What can we (Pharmacists) do? How do you recognise
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree
 and egfr: Decision and Dilemma. Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree") Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
Chronic Kidney Disease (CKD) and egfr: Decision and Dilemma Dr Bhavna K Pandya Consultant Nephrologist University Hospital Aintree Topics CKD background egfr background Patient with egfr Referral Guidelines
A patient guide to membranous nephropathy
 A patient guide to membranous nephropathy Queen Elizabeth Hospital Kidney Care Department UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
A patient guide to membranous nephropathy Queen Elizabeth Hospital Kidney Care Department UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
A guide to the treatment and management of Childhood Nephrotic Syndrome
 A guide to the treatment and management of Childhood Nephrotic Syndrome CONTENTS Introduction What is Nephrotic Syndrome? What is the cause of Nephrotic Syndrome? What is the treatment? Side-effects of
A guide to the treatment and management of Childhood Nephrotic Syndrome CONTENTS Introduction What is Nephrotic Syndrome? What is the cause of Nephrotic Syndrome? What is the treatment? Side-effects of
Tacrolimus (Adoport, Prograf, Modigraf or Advagraf )
") Shared Care Guideline DRUG: Tacrolimus (Adoport, Prograf, Modigraf or Advagraf ) for Renal Transplant (Adults) Introduction: Indication: Prophylaxis of transplant rejection in kidney recipients Tacrolimus
Shared Care Guideline DRUG: Tacrolimus (Adoport, Prograf, Modigraf or Advagraf ) for Renal Transplant (Adults) Introduction: Indication: Prophylaxis of transplant rejection in kidney recipients Tacrolimus
Family Medicine Counseling (Additional topics)
") Family Medicine Counseling (Additional topics) Doa'a Samarah Al Zoubi Hope/2010 batch 1. ACEI 2. Diabetic with microalbuminuria 3. Osteoporosis 4. Anti-thyroid drugs and ablation. 1. ACEI counseling: -
Family Medicine Counseling (Additional topics) Doa'a Samarah Al Zoubi Hope/2010 batch 1. ACEI 2. Diabetic with microalbuminuria 3. Osteoporosis 4. Anti-thyroid drugs and ablation. 1. ACEI counseling: -
Burkitt s Lymphoma or DLBCL with adverse features PATIENTS WITH GOOD PERFORMANCE STATUS
 Regimen R-CODOX M Indication Burkitt s Lymphoma or DLBCL with adverse features Therapeutic Intent Radical/Curative PATIENTS WITH GOOD PERFORMANCE STATUS Day Medication Dose Route Administration Details
Regimen R-CODOX M Indication Burkitt s Lymphoma or DLBCL with adverse features Therapeutic Intent Radical/Curative PATIENTS WITH GOOD PERFORMANCE STATUS Day Medication Dose Route Administration Details
Introduction The Role of the Kidneys Drugs used in Renal Disease Drugs and Dialysis Renal Pharmacy Team
 Introduction The Role of the Kidneys Drugs used in Renal Disease Drugs and Dialysis Renal Pharmacy Team Drugs play a major role in both treating and causing renal disease Doses of some drugs need to be
Introduction The Role of the Kidneys Drugs used in Renal Disease Drugs and Dialysis Renal Pharmacy Team Drugs play a major role in both treating and causing renal disease Doses of some drugs need to be
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Managing a child with nephrotic syndrome
 Current practice Managing a child with nephrotic syndrome R S Thalgahagoda 1, S Abeyagunawardena 2, U I Karunadasa 1, *A S Abeyagunawardena 1 Sri Lanka Journal of Child Health, 2017; 46(3): 267-272 DOI:
Current practice Managing a child with nephrotic syndrome R S Thalgahagoda 1, S Abeyagunawardena 2, U I Karunadasa 1, *A S Abeyagunawardena 1 Sri Lanka Journal of Child Health, 2017; 46(3): 267-272 DOI:
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
THE CLATTERBRIDGE CANCER CENTRE NHS FOUNDATION TRUST. Systemic Anti Cancer Treatment Protocol. EDP + mitotane
 Systemic Anti Cancer Treatment Protocol EDP + mitotane PROCEDURE REF: MPHAHANEDP (Version No: 1.0) Approved for use in: Symptomatic treatment for advanced (unresectable, metastatic or relapsed) adrenocortical
Systemic Anti Cancer Treatment Protocol EDP + mitotane PROCEDURE REF: MPHAHANEDP (Version No: 1.0) Approved for use in: Symptomatic treatment for advanced (unresectable, metastatic or relapsed) adrenocortical
Acute Kidney Injury shared guidance
 Acute Kidney Injury shared guidance Acute Kidney Injury (AKI) Fluid balance assessment (NICE CG 169) Assess the patient s likely fluid and electrolyte needs 1.History previous limited intake, thirst, abnormal
Acute Kidney Injury shared guidance Acute Kidney Injury (AKI) Fluid balance assessment (NICE CG 169) Assess the patient s likely fluid and electrolyte needs 1.History previous limited intake, thirst, abnormal
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
CHRONIC KIDNEY DISEASE DIAGNOSIS
 CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
CHRONIC KIDNEY DISEASE DIAGSIS GFR categories, description and range WHO SHOULD BE TESTED FOR CKD CLASSIFICATION OF CKD USING egfr AND ACR CATEGORIES Offer testing for CKD using egfr, creatinine and ACR
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Cisplatin / 5-Fluorouracil (+ Trastuzumab) in Gastric Cancer
 in Gastric Cancer") Cisplatin / 5-Fluorouracil (+ Trastuzumab) in Gastric Cancer Indication: Confirmed HER2-positive (3+ or FISH+) metastatic adenocarcinoma of the stomach or gastro-oesophageal junction. For Trastuzumab doses
Cisplatin / 5-Fluorouracil (+ Trastuzumab) in Gastric Cancer Indication: Confirmed HER2-positive (3+ or FISH+) metastatic adenocarcinoma of the stomach or gastro-oesophageal junction. For Trastuzumab doses
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
P-RMS: FR/H/PSUR/0056/001
 Core Safety Profile Active substance: Piretanide Pharmaceutical form(s)/strength: Tablets, 3mg, 6mg Capsules, 6mg Ampoules, 6mg, 12mg, 60mg P-RMS: FR/H/PSUR/0056/001 Date of FAR: 21.12.2009 4.2 Posology
Core Safety Profile Active substance: Piretanide Pharmaceutical form(s)/strength: Tablets, 3mg, 6mg Capsules, 6mg Ampoules, 6mg, 12mg, 60mg P-RMS: FR/H/PSUR/0056/001 Date of FAR: 21.12.2009 4.2 Posology
BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine
 BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine Protocol Code Tumour Group Contact Physician UGOOVBEVV Gynecologic Oncology Dr.
BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine Protocol Code Tumour Group Contact Physician UGOOVBEVV Gynecologic Oncology Dr.
The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions. Jonathan Evans Paediatric Nephrologist
 The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions Jonathan Evans Paediatric Nephrologist CKD in adults Often unrecognised Preventable Major cardiovascular
The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions Jonathan Evans Paediatric Nephrologist CKD in adults Often unrecognised Preventable Major cardiovascular
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: AZATHIOPRINE Protocol number: CV 04
 UHB Corporate Medicines Management Group (c MMG) SHARED CARE. Drug: AZATHIOPRINE Protocol number: CV 04") Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: AZATHIOPRINE Protocol number: CV 04 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION LIVER
Cardiff & Vale (C&V) UHB Corporate Medicines Management Group (c MMG) SHARED CARE Drug: AZATHIOPRINE Protocol number: CV 04 Indication: RENAL, PANCREAS OR COMBINED RENAL PANCREAS TRANSPLANTATION LIVER
Additional file 2: Details of cohort studies and randomised trials
 Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Over- and underfill: not all nephrotic states are equal. Detlef Bockenhauer
 Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Over- and underfill: not all nephrotic states are equal Detlef Bockenhauer Objectives Review pathophysiology of oedema: undervs overfill Treatment options The clinical setting: case 1 A6-y old girl with
Professor Suetonia Palmer
 Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST
 ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI)
") Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI) Renal function Kidney has many roles: 1. Excretory function 2. Osmolality regulation 3. Acid base balance 4. BP regulation through salt and water balance
Medicine Dr. Dana Lecture 1 Acute Kidney Injury (AKI) Renal function Kidney has many roles: 1. Excretory function 2. Osmolality regulation 3. Acid base balance 4. BP regulation through salt and water balance
High Dose Cytarabine plus high dose Methotrexate for CNS Lymphoma
 High Dose Cytarabine plus high dose Methotrexate for CNS Lymphoma Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton
High Dose Cytarabine plus high dose Methotrexate for CNS Lymphoma Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton
Minimal change nephropathy: an update (for adults) Dr. CC Szeto Department of Medicine & Therapeutics The Chinese University of Hong Kong
 Dr. CC Szeto Department of Medicine & Therapeutics The Chinese University of Hong Kong") Minimal change nephropathy: an update (for adults) Dr. CC Szeto Department of Medicine & Therapeutics The Chinese University of Hong Kong First, it is not uncommon Cameron JS. Am J Kidney Dis 10: 157 171,
Minimal change nephropathy: an update (for adults) Dr. CC Szeto Department of Medicine & Therapeutics The Chinese University of Hong Kong First, it is not uncommon Cameron JS. Am J Kidney Dis 10: 157 171,
DERBY-BURTON CANCER NETWORK CONTROLLED DOC NO:
 OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
OBINUTUZUMAB+CHLORAMBUCIL Regimen RDH; Day 1 and 2 Dose to be given on Ward Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community
ECX. Anti-emetics: Day 1: highly emetogenic Days 2 21: mildly emetogenic
 Page 1 of 5 As an alternative to ECF: For locally advanced (inoperable) or metastatic oesophageal or gastric cancer; peri-operative use in oesophageal or gastric cancer; adenocarcinoma of unknown primary
Page 1 of 5 As an alternative to ECF: For locally advanced (inoperable) or metastatic oesophageal or gastric cancer; peri-operative use in oesophageal or gastric cancer; adenocarcinoma of unknown primary
Axitinib (renal) Note: in some patients it may be appropriate to increase the dose to 6mg BD before increasing to 7mg BD.
 Note: in some patients it may be appropriate to increase the dose to 6mg BD before increasing to 7mg BD.") Axitinib (renal) Indication Treatment of advanced renal cell carcinoma after failure of treatment with a first-line tyrosine kinase inhibitor (UK licensed indication states sunitinib) or a cytokine. (NICE
Axitinib (renal) Indication Treatment of advanced renal cell carcinoma after failure of treatment with a first-line tyrosine kinase inhibitor (UK licensed indication states sunitinib) or a cytokine. (NICE
Trust Guideline. for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis. (*ie aged 16 years and over)
") Trust Guideline for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis (*ie aged 16 years and over) abc A guideline recommended for use In: Gastroenterology/Medical
Trust Guideline for Ciclosporin Treatment & Monitoring for Adult* Patients with Acute, Severe Ulcerative Colitis (*ie aged 16 years and over) abc A guideline recommended for use In: Gastroenterology/Medical
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
ALL MAINTENANCE (25-60 years)
") ALL MAINTENANCE (25-60 years) INDICATION Adult Acute Lymphoblastic Leukaemia (ALL) in remission not eligible for allogeneic transplantation This protocol is suitable for patients aged 25-60 years. It may
ALL MAINTENANCE (25-60 years) INDICATION Adult Acute Lymphoblastic Leukaemia (ALL) in remission not eligible for allogeneic transplantation This protocol is suitable for patients aged 25-60 years. It may
Summary of Recommendation Statements Kidney International Supplements (2013) 3, 5 14; doi: /kisup
 3, 5 14; doi: /kisup") http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
http://www.kidney-international.org & 2013 DIGO Summary of Recommendation Statements idney International Supplements (2013) 3, 5 14; doi:10.1038/kisup.2012.77 Chapter 1: Definition and classification of
Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
http://www.kidney-international.org chapter 6 & 2012 KDIGO Chapter 6: Idiopathic focal segmental glomerulosclerosis in adults Kidney International Supplements (2012) 2, 181 185; doi:10.1038/kisup.2012.19
Learning Objectives. How big is the problem? ACUTE KIDNEY INJURY
 ACUTE KIDNEY INJURY Karen Innocent, DNP, RN, CRNP, ANP-BC, CMSRN Executive Director, Continuing Education Wolters Kluwer Health, Inc May 2016 Orlando FL Learning Objectives Identify the risk factors and
ACUTE KIDNEY INJURY Karen Innocent, DNP, RN, CRNP, ANP-BC, CMSRN Executive Director, Continuing Education Wolters Kluwer Health, Inc May 2016 Orlando FL Learning Objectives Identify the risk factors and
Bortezomib, Thalidomide and Dexamethasone (VTD) 28 day
 28 day") Bortezomib, Thalidomide and Dexamethasone (VTD) 28 day Indication First line treatment of multiple myeloma in patients who are eligible for stem cell transplantation. (NICE TA311) ICD-10 codes Codes with
Bortezomib, Thalidomide and Dexamethasone (VTD) 28 day Indication First line treatment of multiple myeloma in patients who are eligible for stem cell transplantation. (NICE TA311) ICD-10 codes Codes with
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC)
") Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in advanced/metastatic
Lung Pathway Group Cisplatin & IV Vinorelbine in Non- Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in advanced/metastatic
M0BCore Safety Profile
 M0BCore Safety Profile Active substance: Aciclovir Pharmaceutical form(s)/strength: Tablets 200, 400 or 800 mg Dispersible tablets 200, 400 or 800 mg Oral suspensions 200 mg or 400 mg per 5 ml. Freeze
M0BCore Safety Profile Active substance: Aciclovir Pharmaceutical form(s)/strength: Tablets 200, 400 or 800 mg Dispersible tablets 200, 400 or 800 mg Oral suspensions 200 mg or 400 mg per 5 ml. Freeze
R-GDP: Rituximab, Gemcitabine, Dexamethasone &Cisplatin
 : Rituximab, Gemcitabine, Dexamethasone &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma or high grade T cell non-hodgkin
: Rituximab, Gemcitabine, Dexamethasone &Cisplatin INDICATION Relapsed or refractory Hodgkin and non-hodgkin lymphoma. Omit Rituximab for patients with Hodgkin Lymphoma or high grade T cell non-hodgkin
ALL Phase 2 Induction (25-60 years)
") ALL Phase 2 (25-60 years) INDICATION of remission in Adult Acute Lymphoblastic Leukaemia (ALL) patients This protocol is suitable for patients aged 25-60 years. It may sometimes be used in older patients
ALL Phase 2 (25-60 years) INDICATION of remission in Adult Acute Lymphoblastic Leukaemia (ALL) patients This protocol is suitable for patients aged 25-60 years. It may sometimes be used in older patients
Gemcitabine + Cisplatin Regimen
 Gemcitabine + Cisplatin Regimen Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby out-patient Indication
Gemcitabine + Cisplatin Regimen Available for Routine Use in Burton in-patient Derby in-patient Burton day-case Derby day-case Burton community Derby community Burton out-patient Derby out-patient Indication
Chronic Kidney Disease. Paul Cockwell Queen Elizabeth Hospital Birmingham
 Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
PRESCRIBING GUIDANCE TACROLIMUS for the treatment of INFLAMATORY BOWEL DISEASE (IBD)
") PRESCRIBING GUIDANCE TACROLIMUS for the treatment of INFLAMATORY BOWEL DISEASE (IBD) For the latest information on interactions and adverse effects, always consult the latest version of the Summary of
PRESCRIBING GUIDANCE TACROLIMUS for the treatment of INFLAMATORY BOWEL DISEASE (IBD) For the latest information on interactions and adverse effects, always consult the latest version of the Summary of
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Factsheet Sacubitril valsartan (Entresto ) for chronic heart failure with reduced ejection fraction
 for chronic heart failure with reduced ejection fraction") North Central London Joint Formulary Committee Factsheet Sacubitril valsartan (Entresto ) for chronic heart failure with reduced ejection fraction Start date: July 2016 Review date: July 2019 Document
North Central London Joint Formulary Committee Factsheet Sacubitril valsartan (Entresto ) for chronic heart failure with reduced ejection fraction Start date: July 2016 Review date: July 2019 Document
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE
 Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care
 Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care Paula D Souza Senior CKD Nurse Specialist Royal Devon and Exeter Healthcare Trust Introduction Background What
Nice CKD Clinical Guidelines 2014 The challenges and benefits they may bring toprimary care Paula D Souza Senior CKD Nurse Specialist Royal Devon and Exeter Healthcare Trust Introduction Background What
Bevacizumab + Paclitaxel + Cisplatin
 Bevacizumab + Paclitaxel + Cisplatin Available for Routine Use in Not routinely commissioned, each case requires prior documented approval before offering & commencing therapy from the Cancer Drugs Fund
Bevacizumab + Paclitaxel + Cisplatin Available for Routine Use in Not routinely commissioned, each case requires prior documented approval before offering & commencing therapy from the Cancer Drugs Fund
Cisplatin Vinorelbine (Oral) therapy +/- radiotherapy
 therapy +/- radiotherapy") 1 REGIMEN TITLE: Cisplatin Vinorelbine (Oral) therapy +/- radiotherapy Page 1 of 5 Indication: First line in Radical/ Induction, Adjuvant and Advanced & Palliative treatment of Non-small cell lung cancer
1 REGIMEN TITLE: Cisplatin Vinorelbine (Oral) therapy +/- radiotherapy Page 1 of 5 Indication: First line in Radical/ Induction, Adjuvant and Advanced & Palliative treatment of Non-small cell lung cancer
Carboplatin, Paclitaxel and Bevacizumab (gynae)
") Carboplatin, Paclitaxel and Bevacizumab (gynae) Indication First line treatment of recurrent or metastatic cervical cancer. WHO performance status 0 or 1. First line treatment of advanced epithelial ovarian,
Carboplatin, Paclitaxel and Bevacizumab (gynae) Indication First line treatment of recurrent or metastatic cervical cancer. WHO performance status 0 or 1. First line treatment of advanced epithelial ovarian,
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel
 BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
Use ideal body weight (IBW) unless actual body weight is less. Use the following equation to calculate IBW:
 unless actual body weight is less. Use the following equation to calculate IBW:") Amikacin is a partially restricted (amber) antibiotic for the treatment of infections due to gentamicin resistant Gram negative bacilli or as advised by microbiology. As with other aminoglycosides, therapeutic
Amikacin is a partially restricted (amber) antibiotic for the treatment of infections due to gentamicin resistant Gram negative bacilli or as advised by microbiology. As with other aminoglycosides, therapeutic
Essential Shared Care Agreement: Lithium
 Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
Ref No. E042 Essential Shared Care Agreement: Lithium Please complete the following details: Patient s name, address, date of birth Treatment (indication, dose regimen, brand name) Monitoring (proposed
TIP: Paclitaxel / Ifosfamide / Cisplatin in Relapsed Germ Cell Tumour
 TIP: Paclitaxel / Ifosfamide / Cisplatin in Relapsed Germ Cell Tumour Indication: Second line therapy in Relapsed Germ Cell Tumours Regimen details: Paclitaxel 175mg/m 2 IV Cisplatin 20mg/m 2 IV - D5 Ifosfamide
TIP: Paclitaxel / Ifosfamide / Cisplatin in Relapsed Germ Cell Tumour Indication: Second line therapy in Relapsed Germ Cell Tumours Regimen details: Paclitaxel 175mg/m 2 IV Cisplatin 20mg/m 2 IV - D5 Ifosfamide
Please complete all sections 1. Name of Drug, Brand Name, Form and Strength
 GMMMG Interface Prescribing Subgroup Shared Care Template Shared Care Guideline Ciclosporin for use in childhood nephrotic syndrome Reference Number Replaces: n/a Issue date: 15/10/2015 Author(s)/Originator(s):
GMMMG Interface Prescribing Subgroup Shared Care Template Shared Care Guideline Ciclosporin for use in childhood nephrotic syndrome Reference Number Replaces: n/a Issue date: 15/10/2015 Author(s)/Originator(s):
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 9 March 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 March 2011 TAREG 3 mg/ml oral solution B/1 160 ml (CIP code: 491 474-8) Applicant: NOVARTIS PHARMA SAS valsartan
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 9 March 2011 TAREG 3 mg/ml oral solution B/1 160 ml (CIP code: 491 474-8) Applicant: NOVARTIS PHARMA SAS valsartan
Acute Kidney Injury (AKI)
") (Last Updated: 08/22/2018) Created by: Socco, Samantha Acute Kidney Injury (AKI) Thambi, M. (2017). Acute Kidney Injury. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. AKI This
(Last Updated: 08/22/2018) Created by: Socco, Samantha Acute Kidney Injury (AKI) Thambi, M. (2017). Acute Kidney Injury. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. AKI This
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Use of mycophenolate mofetil in steroid-dependent and -resistant nephrotic syndrome
 Pediatr Nephrol (2003) 18:833 837 DOI 10.1007/s00467-003-1175-4 BRIEF REPORT Gina-Marie Barletta William E. Smoyer Timothy E. Bunchman Joseph T. Flynn David B. Kershaw Use of mycophenolate mofetil in steroid-dependent
Pediatr Nephrol (2003) 18:833 837 DOI 10.1007/s00467-003-1175-4 BRIEF REPORT Gina-Marie Barletta William E. Smoyer Timothy E. Bunchman Joseph T. Flynn David B. Kershaw Use of mycophenolate mofetil in steroid-dependent
Gemcitabine, Carboplatin and Bevacizumab (gynae)
") Gemcitabine, Carboplatin and Bevacizumab (gynae) Indication Second line advanced epithelial ovarian, fallopian tube or primary peritoneal cancer. WHO performance status 0 or 1. (Funding via the CDF) ICD-10
Gemcitabine, Carboplatin and Bevacizumab (gynae) Indication Second line advanced epithelial ovarian, fallopian tube or primary peritoneal cancer. WHO performance status 0 or 1. (Funding via the CDF) ICD-10