Thursday School 2010 Management of Inpatient Diabetes and Hyperglycemia and Quality Improvement Efforts
|
|
|
- Raymond Patrick
- 5 years ago
- Views:
Transcription
1 Thursday School 2010 Management of Inpatient Diabetes and Hyperglycemia and Quality Improvement Efforts Kendall Rogers, MD

2 Using subcutaneous insulin to reliably achieve desired glycemic outcomes in non-critically ill hospitalized patients
3 Objectives For This Lecture Appreciate the obstacles to achieving good glycemic control in hospital patients Understand and apply the best practice of inpatient hyperglycemia/diabetes management using subcutaneous insulin, including the use of anticipatory, physiologic insulin dosing in a variety of clinical situations Understand the common deviations from the best practices of insulin management in the hospital Learn how to prevent and manage hyperglycemia and hypoglycemia
4 Case 1 56 year old woman with DM2 admitted with a diabetes-related foot infection which may require surgical debridement in the near future, eating regular meals. - Weight: 100 kg - Home medical regimen: Glipizide 10 mg po qd, Metformin 1000 mg po bid, and 20 units of NPH q HS - Control: A recent HbA1c is 10%, POC glucose in ED 240 mg/dl What are your initial orders?
5 You put the patient on the Insulin Order Set with the reg diet checked, moderate dose scale check marked, and 10 units of glargine written for Write down: When will the CBGs be checked? Exactly what insulin is scheduled and at what times? If the patient is hypoglycemic, what will happen?
6 Managing Diabetes in the Hospital Presents Different Challenges than Managing Diabetes in the Outpatient Arena! The hospital is associated with: - Nutritional and clinical instability - The need for changes from the home diabetes medical regimen - Acute illness, stress-related hyperglycemia - Use of medications that impact glycemic control
7 Why Should We Care? Hyperglycemia occurs frequently in hospital patients, and is associated with poor outcomes Hypoglycemia occurs frequently in hospital patients, and is unpleasant and dangerous Adequate metabolic control is an attainable goal for hospital patients
8 What is the Appropriate Glycemic Control Target for Inpatients? Controversial! ICU Non-ICU, Preprandial Non-ICU, Maximum ACCE/ACE 110 mg/dl 110 mg/dl 180 mg/dl ADA 110 mg/dl mg/dl 180 mg/dl
9 NICE SUGAR March 26, 2009 NEJM Vol 360 (13) Open Label RCT, Multinational 6104 critically ill patients Intensive infusion ( mg/dl) vs Conventional control ( mg/dl) 90 day survival primary end point
10 The NICE-SUGAR Study Blood Glucose Level, According to Treatment Group Probability of Survival RR= 1.14 IIT goal: mg/dl (mean BG 118 mg/dl) CIT goal: <180 mg/dl (mean BG 145 mg/dl) Nice Sugar, NEJM 360; march 26, day mortality: IIT: 829 patients (27.5%), CIT: 751 (24.9%) Absolute mortality difference: 2.6% (95% CI, 0.4 to 4.8); Odds ratio for death with IIT was 1.14 (95% CI, 1.02 to 1.28; P = 0.02).
11 NICE-SUGAR Study Outcomes Outcome Measure Intensive Group Conventional Group Morning BG (mg/dl) Hypoglycemia 206/ /3014 ( 40mg/dL) 28 Day Mortality (p=0.17) 90 Day Mortality (p=0.02) (6.8%) (0.5%) 22.3% 20.8% 27.5% 24.9% 97% infusion 69% infusion The NICE-SUGAR Study Investigators. N Engl J Med. 360: , 2009.
12 RABBIT 2- Surgical ADA Abstract- Umpierrez et al RCT - Gla / Glu basal bolus vs SSI 211 adult (mean age 58) inpatients Hyperglycemic (mean 190, mg/dl) Diabetes 2 diagnosis for 3 months or more Composite outcome hospital complications including postoperative wound infection, pneumonia, respiratory failure, acute renal failure, and bacteremia Mortality Glycemic Control and Hypoglycemia
13 RABBIT 2 SURGICAL Gla / Glu N = 104 SSI N = 107 P value Daily mean glucose <.01 Severe hypoglycemia 3.8% 0%.057 Mortality 1% 1% NS Wound infection 2.9% 10.3%.05 Pneumonia 0 2.8%.24 ARF 3.8% 10.3%.10 ICU transfer 12.5% 19.9%.16 ICU LOS 1.2 days 3.2 days.003 Composite 8.6% 24.3% <.003



14 ? New AACE / ADA Guidelines? BAD GOOD BAD Hypoglycemia Somewhere in the Middle Hyperglycemia < >200
15 How Can Diabetes and Hyperglycemia be Controlled in the Hospital? Oral agents = often inappropriate for hospital patients IV insulin = most often used in the intensive care unit setting (or in other defined populations) Subcutaneous insulin = the drug of choice for controlling hyperglycemia in the majority of non-critically ill patients
16 Recommendations for Managing Patients With Diabetes in the Hospital Setting Antihyperglycemic Therapy Insulin Recommended OADs Not Generally Recommended IV Insulin Critically ill patients in the ICU SC Insulin Non-critically ill patients 1. ACE/ADA Task Force on Inpatient Diabetes. Diabetes Care & Diabetes Care. 2009;31(suppl 1):S1-S110.
17 Oral Agents in the Hospital Oral agents can be continued in stable patients with normal nutritional intake, normal blood glucose levels, and stable renal and cardiac function. However, otherwise not recommended in inpatient setting. Disadvantages of most oral agents: Slow-acting/difficult to titrate Sulfonyureas are a major cause of severe hypoglycemia Metformin is contraindicated in settings of decrease renal blood flow, eg. Use of contrast dye, CHF, dehydration Thiazolidinediones are associated with edema and CHF
18 Diabetes and Hyperglycemia Require Proactive Management Diabetes requires proactive management in all hospital patients. There are no autopilot insulin regimens Insulin is a high alert medication that is frequently associated with medication errors in the hospital, and JCAHO considers insulin to be one of the highest risk medications in the hospital (JCAHO Website, 2006)
19 Current Practice Best Practice Dependence on non-physiologic insulin prescribing (as opposed to insulin that mimics physiologic insulin secretion) Dependence on reactive strategies (e.g. sliding-scale insulin) Overemphasis on simplicity (particularly simplicity from the perspective of the ordering physician) Overemphasis on avoidance of hypoglycemia Lack of standardization of insulin use in the hospital
20 Issues- It is not just about glycemic target Choice of initial regimen in the hospital. Poor glycemic control ignored/accepted. Reliance on sliding scale insulin. Inappropriate follow up of hypoglycemia. Stacking of insulin dosing. Communication between services. Inconsistent approach to insulin ordering Nurse to physician communication.
21 It is not just about glycemic target Hypoglycemia rates high Poor management of hypoglycemia Failure to prevent hypoglycemia Uneven training amongst staff Poor coordination of tray delivery, monitoring, and insulin Inconsistent transitions Patients often confused or angry Obesity and Diabetes increasingly common!
22 What is the Best Practice for Managing Diabetes and Hyperglycemia in the Hospital? The answer is anticipatory, physiologic insulin dosing, prescribed as a basal/bolus insulin regimen This means giving the right type of insulin, in the right amount, at the right time, to meet the insulin needs of the patient Not Sliding Scale Insulin
23 Indications for IV Insulin Therapy Prolonged fasting (>12 h) in type 1 DM Critical illness Before major surgical procedures After organ transplantation DKA Labor and delivery Acute MI Other illnesses requiring prompt glucose control ACE Position statement on inpatient diabetes 2004
24 The Components of a Physiologic Insulin Regimen Basal insulin Nutritional insulin Correctional insulin
25 Glucose (mg/dl) Insulin (µu/ml) Physiologic Insulin Secretion: Basal/Bolus Concept Nutritional (Prandial) Insulin Basal Insulin Breakfast Lunch Supper Nutritional Glucose Basal Glucose A.M. P.M. Time of Day Suppresses Glucose Production Between Meals & Overnight The 50/50 Rule
26 The Components of a Physiologic Insulin Regimen Basal insulin - long-acting insulin required in all Type 1 (and most Type 2) patients to maintain euglycemia by preventing gluconeogenesis Nutritional insulin - scheduled short-acting insulin given just before a meal, in anticipation of the glycemic spike that occurs due to carbohydrate ingestion (this dose is given even when the blood sugar is in the normal range). Correctional insulin - short-acting insulin that is given in addition to scheduled nutritional insulin (or given at other times of the day) as a response to preexisting high blood glucose levels
27 Providing Exogenous Basal Insulin Long-acting, non-peaking insulin is preferred as it provides continuous insulin action, even when the patient is fasting Required in ALL patients with type 1 diabetes Many patients with type 2 diabetes will require basal insulin in the hospital Can be estimated to be about 1/2 of the total daily dose of insulin (TDD)
28 Insulin Effect Which Insulins are Best for Basal Coverage? NPH Detemir (Levemir) Glargine (Lantus) Regular Lispro (Humalog) Aspart (Novolog) Glulisine (Apidra) Inhaled insulin Time (hours)
29 Providing Exogenous Nutritional Insulin Usually given as rapid-acting analogue (preferred in most cases) or regular insulin, for those patients who are eating meals Must be matched to the patient s nutrition Should not be given to patients who are not receiving nutrition (e.g. NPO) Can be estimated to be about ½ of the total daily dose of insulin (TDD)
30 Insulin Effect Which Insulins are Best for Basal Coverage? NPH Detemir (Levemir) Glargine (Lantus) Regular Lispro (Humalog) Aspart (Novolog) Glulisine (Apidra) Inhaled insulin Time (hours)
31 Providing Exogenous Correctional Insulin Correctional insulin is extra insulin that is given to correct preexisting hyperglycemia Usually rapid-acting or regular insulin (usually the same as the nutritional insulin) Often written in a stepped format that is used in addition to basal and nutritional insulin Customized to the patient using an estimate of the patient s insulin sensitivity If correctional insulin is required consistently, or in high doses, it suggests a need to modify the basal and/or nutritional insulin doses
32 Using Exogenous Insulin to Imitate Physiologic Insulin Secretion: Summary Basal insulin: Use non-peaking, longer acting insulins Glargine or detemir are preferred NPH also possible Nutritional insulin: Depends on the type of nutrition Rapid-acting insulin is preferred when patients are eating meals Regular insulin also possible Correctional insulin: Use rapid-acting (or regular) insulin Usually the same as the nutritional insulin
33 Which Patients Should be Treated with a Physiologic Insulin Regimen? During hospitalization Any patient with blood glucose levels consistently above the target range Immediately at the time of admission All patients with type 1 diabetes Patients with type 2 diabetes if They are known to be insulin-requiring They are known to be poorly controlled despite treatment with significant doses of oral agents They are known to require high doses of oral agents that will be held in the hospital
34 A Stepwise Approach to Physiologic Insulin Dosing in the Hospital 1. Decide if patient is appropriate for the guideline and discontinue oral antidiabetic agents 2. Calculate the estimated total daily dose (TDD) of insulin 3. Determine the distribution of the TDD calculated above based on nutrition regimen. 4. Re-evaluate & adjust the TDD daily based on the glycemic control of the previous 24h
35
36

37
38 STEP 2: Estimate the Amount of Insulin the Patient Would Need Over One Day, If Getting Adequate Nutrition = Total Daily Dose (TDD) Insulin drip-based estimate For patients already treated with insulin, consider the patient s preadmission subcutaneous regimen and glycemic control on that regimen Weight-based estimate: TDD = 0.4 units x Wt in Kg Adjust down to 0.3 units x Wt in Kg for those with hypoglycemia risk factors, including kidney failure, type 1 diabetes (especially if lean), frail/low body weight/ malnourished elderly, or insulin naïve patients Adjust up to units (or more) x Wt in Kg for those with hyperglycemia risk factors, including obesity and high-dose glucocorticoid treatment
39
40 STEP 3: Decide Which Components of Insulin the Patient Will Require, and Which Percentage of the TDD Each Should Represent Basal insulin can generally be estimated to be 1/2 of the TDD Nutritional insulin makes up the remaining 1/2 of the TDD
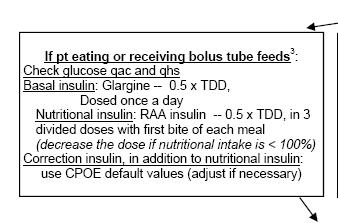
41 STEP 3: Assess the Patient s Nutritional Situation Eating meals or receiving bolus tube feeds Eating meals but with unpredictable intake Getting continuous tube feeds Getting tube feeds for only part of the day Getting parenteral nutrition NPO
42 STEP 3: Decide Which Components of Insulin the Patient Will Require, and Which Percentage of the TDD Each Should Represent In most cases, basal insulin should be provided In most cases, well-designed corrective insulin regimens should be provided When a patient is not receiving nutrition, nutritional insulin should not be given Nutritional insulin needs must be matched to the actual nutritional intake

43
44 STEP 4: Assess Blood Glucoses at Least Daily, Adjusting Insulin Doses as Appropriate Blood glucose targets can only be achieved via continuous management of the insulin program There is no autopilot insulin regimen for a hospitalized patient!
45 Glycemic Control Points Above 180 twice is uncontrolled DM and a change needs to be made in insulin management Use of correction scale is sign of a treatment failure Uncontrolled DM should be on all 3 insulins Avoid clinical inertia, make changes to insulin Check MAR and administration times Use admission HgA1c in transition to home decisions
46 UNM Glycemic Control
47
48 Components of a Glycemic Control Program Administrative support Multidisciplinary steering committee to promote the development of initiatives Assessment of current processes, quality of care, and barriers to change Development and implementation of interventions Standardized order sets, protocols, policies. Educational programs, Special teams Metrics for evaluation Inpatient Diabetes and Glycemic Control: A Call to Action Conference. Position Statement. AACE, February Available at: IDGC0207.pdf. Accessed October 24, Garber et al. Endocr Pract. 2006;12(suppl 3):3-13.
49 Primary Improvement Areas IV Insulin (Critical Care) Subcutaneous Insulin (Non-Critical Care) Transition from IV to Subcutaneous Insulin Transition to Home
50 Our current champions: Quality Dept Sharon Perrilliat and Paul Nelson Floor Nursing - Annabelle Baca and Susan Grohman Inpatient Diabetic Educator - Rosa Matonti Outpt DM Ed - Linda Reineke and Barbara McMillan Pharmacy - Nick Crozier IT - Mary Rivera Tricore Lab - Michelle Neal Unit Director - Donna Kindley Finance - Paula Williams Food and Nutrition - Chester "Chet" Kubic
51 History of Project Phase I started in Completed. Development, testing, and implementation of a basal bolus subcutaneous insulin order set and nursing insulin MAR Focus on elimination of sliding scale insulin and insulin myths Extensive education house-wide of nurses and physicians Grassroots and front-line staff leadership and champions Phase II started in Ongoing. Structured quality improvement project currently ongoing with quality department leadership and a multidisciplinary team Focus on identifying and resolving nursing, tech, pharmacy, dietary, and physician practice and process issues About to enter implementation phase of interventions
52 Measures Process Measures MD Process Measures Nursing Process Measures Outcomes Measures Glucose Measurements Patient Sample Means Patient Day Weighted Means Patient Stay Weighted Means
53 Glucose Control Measurement What unit of analysis? Glucose reading Pros: easy to calculate, most statistical power Cons: least clinically relevant, skewed data Patient Stay Pros: most clinically relevant Cons: skewed data by LOS, uneven testing Patient-Day Pros: least biased, good balance of other two Cons: slightly more difficult to calculate and interpret 53
54 Patient Safety Percent patient-days with any value < 40 mg/dl (extreme hypoglycemia) < 70 mg/dl (hypoglycemia) > 300 mg/dl (extreme hyperglycemia) 54



55 55% Reduction 36% Reduction
56 Glycemic Control Outcomes Medicine SAC Floor Patient Day Averages July 2008 July 2009 CBG Median CBG Mean >10% Improvement Percent CBG < Percent CBG > ~50% Reductions
57
58 RALS Annual Report 2009 University Hospital

59

60 Mean Blood Glucose All Measurements
61 Mean Blood Glucose Non-ICU Measurements
62 Process Measures Insulin Process Measures Excel Sheet
63 Order Set Utilization 100% 90% 80% 70% 60% 50% 40% 86% 74% 71% 72% 73% 70% 50% 86% 67% 95% 58% 76% 79% 54% 87% 60% 75% 72% 74% 69% 70% 72% 67% 63% 82% 89% 90% 60% 74% 71% 88% 65% 83% 74% 72% 55% 100% 91% 89% 86% 91% 58% 57% 53% 82% 57% 80% 63% 90% 88% 85% 83% 61% 63% Order Set Used Insulin Change Made 30% 20% 10% 0% Weeks
64 100% Insulin Type Utilization 90% 80% 70% 60% 50% 40% 71% 57% 67% 63% 44% 57% 57% 58% 57% 54% 53% 38% 38% 43% 42% 67% 52% 50% 48% 45% 44% 42% 72% 74% 70% 59% 56% 62% 60% 58% 55% 53% 48% 44% 42% 39% 70% 65% 64% 64% 62% 60% 59% 53% 48% 53% 55% 50% 40% 35% 61% 58% SS Insulin Only Basal 30% 20% 10% 7% 7% 11% 9% 24% 26% 19% 25% 13% 11% 19% 13% 13% 11% 7% 5% 21% 29% 31% 30% 21% 16% 14% 13% 30% 27% 11% 21% Nutrition 0% Weeks
65 Control of Hyper- and Hypo-glycemia 100% 90% 90% 80% 70% 60% 50% 71% 70% 72% 73% 67% 58% 76% 54% 60% 75% 69% 70% 72% 67% 60% 71% 65% 55% 72% 58% 57% 53% 82% 57% 63% 61% 63% Controlled 40% 30% Hypo Event 20% 10% 0% 23% 22% 16% 17% 10% 13% 14% 11% 13% 13% 11% 10% 9% 7% 6% 7% 7% 6% 5% 3% 4% 7% 3% 0% 0% 0% 0% 0% Weeks
66 30% Treatment Failure Rate 25% 25% 24% 23% 23% 20% 19% 15% 14% 15% 12% 16% 13% 13% 15% 14% 17% 17% 17% Treatment Failure Linear (Treatment Failure) 11% 11% 10% 8% 8% 10% 7% 10% 9% 10% 5% 5% 5% 3% 0%
67 Processes of Care: Other Measures Glucose measured w/in 8h of admission Hgb A1c available w/in 30 days POC glucose testing for all patients w/ diabetes or hyperglycemia Use of diabetes order sets Use of oral diabetic agents (esp. if contraindicated) Coordination of POC glucose testing, insulin administration, and food delivery Patient, physician, and nurse attitudes, education, and satisfaction Reporting of hypoglycemic events, RCA 67
68 Current Initiatives CPOE Insulin Order Set Process Mapped Nursing Processes Insulin Pens Resident MD Education Multi-Disciplinary GC Walk Rounds
69 Primary Issues - Subcutaneous Not recognizing poor control MD Processes Incorrect use of order set on admission Not changing orders when uncontrolled Nursing Processes Delay in insulin administration from CBG timing Incorrect administration Other Processes DM Meal Delivery
70 New Areas Transition to Home Guidelines Transition from IV Insulin Needed order set IV Insulin Coordination with ICU efforts
71 Average glucose mg/dl Run Chart: Outcome Measures Glycemic control 48 hrs post transition with and without protocol. Glucose averages before and after transition from infusion insulin 250 Transition Time Protocol Not Used Insulin Per Protocol No Insulin Per Protocol Insulin Infusion 6HR 5HR 4HR 3HR 2HR 1HR 1-6 HR Day 1 Day HR HR HR HR HR HR HR
72 Step by Step Stable enough for transition? Need SC insulin with transition? Calculate the Total Daily Dose (TDD) Give 40-50% of TDD as basal glargine BEFORE you stop the insulin infusion
73 Transitioning to the Outpatient Arena Deciding on a home regimen HbA1c Anticipating clinical improvement Patient factors: Financial, social, abilities, wishes Patient education Changes made in the hospital Diabetes/insulin survival skills Communication with outpatient physicians
74 Next Steps Continue MultiDisciplinary Rounds Start real time monitoring and interventions Reconvene the full Glycemic Control Team Begin using data to effect process improvement Engage more physician champions

75 Kendall Rogers, MD Pejvak Salehi, MD
76 Case 1 56 year old woman with DM2 admitted with a diabetes-related foot infection which may require surgical debridement in the near future, eating regular meals. - Weight: 100 kg - Home medical regimen: Glipizide 10 mg po qd, Metformin 1000 mg po bid, and 20 units of NPH q HS - Control: A recent HbA1c is 10%, POC glucose in ED 240 mg/dl What are your initial orders?
77 Case 1: Solution Bedside glucose testing AC and HS Discontinue oral agents Total daily dose 100 kg x 0.6 units/kg/day = 60 Basal: Glargine 30 units q HS Nutritional: Rapid-acting analogue 10 units q ac at the first bite of each meal Correction: Rapid-acting analogue per scale q ac and HS (Note: Use correctional insulin with caution at HS, reduce the daytime correction by up to 50% to avoid nocturnal hypoglycemia) How would you alter this if the patient had renal failure?
78 8 AM Noon Supper Bedtime Prior Day Glucose Insulin Total Lispro 18 u 18 u 16 u 8 u 60 u Glargine 30 u 30 u TDD 90 u
79 What is your next step? A. Continue the current regimen B. Increase the Basal insulin by 20 units C. Increase the Nutritional Insulin by 5 units/meal D. Increase the Basal by 15 units and the Nutritional by 15 units (5 with each meal) E. Increase the Basal by 10 units and the Nutritional by 6 units (2 with each meal)
80 8 AM Noon Supper Bedtime Prior Day Glucose Insulin Lispro Mealtime Total 10 u 10 u 10 u 30 u Lispro 8 u 8 u 6 u 8 u 30 u Correctional Glargine 30 u 30 u TDD 90
81 Case 1 Continued The patient is made NPO after midnight for a bone biopsy, but is expected to be able to resume her diet at lunch or dinner the next day. What changes would you make to her management program regarding glucose monitoring and her insulin program?
82 Case 1 continued: Solution Change bedside glucose checks to q 4 hours, as the patient will not be eating meals Continue basal insulin: If using glargine, continue as is. If using NPH, continue in equal twice daily doses with a dose reduction of 1/3-1/2 while NPO. Hold nutritional insulin while NPO Continue appropriate correctional insulin for hyperglycemia
83 Case 2 58 yo M admitted to Vascular surgery team for amputation of RLE for dry gangrene. Medicine consulted on POD #3 for diabetic management. At home he is on max doses of metformin and glyburide and glargine 15 units at bedtime. His HgA1c this admission is 9.2 and there is a question about his compliance in PCP notes. He is on regular SSI and glargine 15 units at bedtime
84 Case 2 Continued POD 1: POD 2 AM CBG: 85 Noon CBG: 248 Dinner CBG: 166 Bedtime CBG: 287 AM CBG: 182 Noon CBG: 255 Dinner CBG: 72 Dinner CBG: 207 SSI given 12 units SSI given 12 units
85 Case 2 Continued What would you do next? A) Divide total daily dose into 50/50 basal and bolus B) Yell at Vascular surgery for using SSI C) Gather more information on meal intake, time of CBG measurements and insulin administration D) Continue with current regimen one more day to gather more data
86 Case 2 Explanation Answer is C Gather more information on meal intake, time of CBG measurements and insulin administration Patient with labile CBGs, but good response to insulin. With history of non-compliance he maybe not eating or snacking in between meals. CBG time and insulin administration may also play an effect. Before dividing CBG 50/50 you need to gather more data. You can make changes to insulin regime after you gather more data.
87 Case 2 Continued His CBGs in POD #1 and 2 are the following POD 1: AM CBG: 85, no insulin given, day prior glargine was given Noon CBG: 248, 4 units Dinner CBG: 166, 2 units Bedtime CBG: 287, 6 units given, glargine held POD 2 AM CBG: 182, 2 units given Noon CBG: 255, 6 units given Dinner CBG: 72, no insulin given Dinner CBG: 207, 4 units insulin and 15 units glargine given
88 Case 3 56 year old woman with type 1 diabetes admitted with a diabetesrelated foot infection. The wound is an infected ulcer on the fifth digit with necrosis. The plan is for amputation first thing in the morning, so the patient will be NPO after midnight. However, she is expected to resume a regular diet at lunch the following day after surgery. - Weight: 70 kg - Home medical regimen: 70/30 insulin 14 units BID - Control: A recent HbA1c is 9%, POC glucose in ED is 240 mg/dl It is now dinner time, and the patient took her last dose of insulin before breakfast. What insulin would you give her now (before dinner) and how would you modify her regimen given the plan for NPO after midnight?
89 Case 3: Solution Bedside glucose testing AC and HS while eating, and q 4 hours when NPO TDD by weight = 70 kg x 0.4 units/kg/day = 28 units Her home TDD is 28, but patient has very poor control on this regimen, so increase (arbitrarily) by 20% = 34 units IV dextrose infusion while NPO (e.g. D5 at cc/hr) Basal: Glargine 17 units q HS Nutritional: Rapid-acting insulin 6 units q ac at the first bite of each meal Correction: Rapid-acting insulin per scale q ac and HS
90 Case 4 77 yo 100kg M with COPD and T2DM is admitted for syncopal episode and pyelonephritis. He reports being clammy and shaky prior to passing. Per EMS CBG was 50. He is from Alabama and uses 70/30 80 units in am and 20 units at bedtime. He takes his meds as prescribed, but has had poor appetite during the past several days. Does not remember his HgA1C. What insulin regimen would you place him on?
91 Case 4 A) Continue home dose of insulin B) Calculate TDD based on weight and place patient on glargine and short acting insulin C) Place on SSI and monitor CBGs for 24 hours D) Call Kendall or Pejvak E) None of the above
92 Case 4 Explanation Answer: none of the above First correct hypoglycemia Once normalized, consider 20u of basal with correction scale, no nutritional until eating well. Then you can place on nutritional and correctional insulin. Basal glargine insulin has much lower incidence of hypoglycemia than NPH
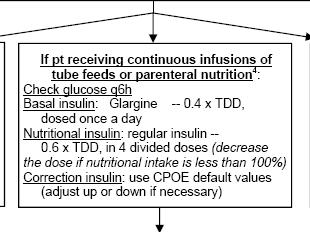
93 Case 5 You are consulted by the neurology service for diabetes management on a 79 y/o M who suffered a large stroke, leaving him with severe dysphagia. He has type 2 diabetes, on maximum doses of metformin, glipizide, and rosiglitazone at home. A PEG was placed and he is up to his goal of 60 cc/hr on continuous tube feeds, but is now hyperglycemic (see next slide). - Weight: 100 kg (BMI 35) - Current medical regimen: High sliding-scale (orals all held) - Control: Glucoses consistently in the mid to high 200 s, a recent HbA1c is 9.6% What insulin regimen will you choose? Does the distinction between basal and nutritional insulin still make sense with continuous feeding?
94 Case 5: Solution TDD = 100 x 0.6 units/kg/day = 60 units Provide this TDD to meet basal and continuous nutritional insulin requirements There is no scientific evidence suggesting one way is better than another Examples: Glargine 60 units daily Glargine 24 units daily (basal) + rapid-acting insulin 6 units q4 hrs (nutritional) Glargine 24 units daily (basal) + regular 9 units q6 hrs (nutritional) 70/30 20 units q8 hrs Regular insulin 15 units q6 hrs Rapid-acting insulin 10 units q 4 hrs Other combinations
95 How would you manipulate this patient s insulin as you initiate tube feeds? Bolus feeds TID Nocturnal Tube Feeds
96 Case 6 62 yo M with COPD is admitted with increased cough, sputum production and green/thick sputum. CXR consistent with pneumonia. He is started on ceftraixone, doxy, duonebs and prednisone 60mg/day. He does not have diabetes, but he reports that during prior hospitalizations and with steroid use he has needed insulin injections. What would you do next?
97 Case 6 Answers A) Calculate TDD insulin and place on Glargine and Aspart B) Place on SSI and monitor CBGs for 24 hours and change to basal/bolus after 24 hours C) Given infection and taper of steroids, monitor CBGs and put on correction insulin D) Do nothing
98 Case 6 Explanation Answer C then maybe B Patient has an acute infection and is on steroids. This combination leads to increased CBGs. However, as infection is treated and steroids tapered, his insulin requirement will decrease. This could lead to unpredictable CBGs and increased risk of hypoglycemia on basal/bolus protocol. Treating increased CBGs shortens hospital stay. If 2 CBGs are above 180 daily, consider using basal/bolus protocol
99 Case 6 Part 2 Patient did well and after 3 days of treatment is ready to be discharged on 14 day taper of steroids. Currently he is on 40mg prednisone and required 4 units of insulin yesterday. Would you discharge this patient in insulin? A) Yes B) No
100 Case 6 Part 2 Explanation Answer is B) NO Patient is not used to using injectable insulin and there is no indication to start him on oral glycemic meds as he has not have a diagnosis of DM. In addition, as mentioned previously, as prednisone is tapers his CBGs will decrease to more normal range and he is at increased risk for hypoglycemia.
101 Case 7 52 yo male, no previous history of dm, admitted for CAP with an O2 requirement, his admission cbg is 210 Wt 60kg What orders would you write? What if the patient had known DM was on 1 oral agent with relatively good control?
102 Case 8 53 yo M with DM, HTN and CAD is admitted for unstable angina to the VAMC. At home he takes NPH 30 units QAM and 30 units QPM, in addition to sliding scale regular insulin. He reports good CBG control at home and uses 7-10units of insulin prior to meals. His last HgA1c is 6.8. He is NPO for possible cardiac cath in the morning. What regimen would you place him on?
103 Case 8 Answers A) Calculate TDD and place on 50/50 basal bolus insulin and correctional insulin B) Decrease NPH by 50% and place on correctional insulin while NPO C) Continue home NPH and correctional insulin D) Convert total home insulin use to glargine and aspart insulin premeal and correctional insulin
104 Case 8 Explanation Answer is B Patient has good control with NPH at home with HgA1c at goal. Due to increased ease of transition from inpatient to outpatient diabetes management, NPH should be continued. However, NPH has increased risk of hypoglycemia if patient is NPO. Dose should be decreased by 1/3 to 1/2 if patient is NPO. Since patient is not eating, his CBGs can be monitored per protocol and treated with correctional insulin while NPO. Once patient is eating, he can be placed on home NPH dose, premeal and correctional insulin
105 Case 9 42 yo on 160 u with HgA1c of 14.3 admitted with pneumonia and current CBG is 260. What are your admit insulin orders?
106 Case yo F with obesity, DM and HTN is admitted to the VAMC with hypertensive urgency. She takes metformin and glyburide with last HGA1c 8.3. He weight is 120kg and BMI 33. She is able to eat. What regime would you place her on at the VA and at the UH respectively.
107 Insulin Order Sets UNM Order Set VA Order Set
108 Summary Understanding these basic principles of physiologic, anticipatory insulin will allow clinicians to formulate rational insulin regimens in virtually any clinical situation!
109 Key Review Articles Inzucchi. Management of Hyperglycemia in the Hospital Setting. N Engl J Med 2006;355: Clement and colleagues. Diabetes Care 2004; 27: American College of Endocrinology Position Statement on Inpatient Diabetes and Metabolic Control. Endocrine Practice 2004; 10: American College of Endocrinology and American Diabetes Association Consensus Statement on Inpatient Diabetes and Glycemic Control. Diabetes Care 2006; 29:
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin
 Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin David Newman, MD University of North Dakota School of Medicine Sanford Health Big Sky Conference 2017 Dr. David Newman, Personal/Professional
Inpatient Diabetes Management: The Slippery Slope of Sliding Scale Insulin David Newman, MD University of North Dakota School of Medicine Sanford Health Big Sky Conference 2017 Dr. David Newman, Personal/Professional
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Glycemic Control Insulin In The Hospital Setting
 Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Glycemic Control Insulin In The Hospital Setting Glycemic Control The Evidence For Insulin s s Benefit The Mechanism of Insulin s s Benefit The Achievement of Insulin s s Benefit A Few Cases Hyperglycemia
Special Situations 1
 Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς
 Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, :30 a.m. 11:15 a.m.
 Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, 2018 10:30 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US.
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, 2018 10:30 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US.
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
HAP PA-HEN Achieving More Together
 HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 10, :30 a.m. 11:15 a.m.
 Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 1, 218 1:3 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US. About
Inpatient Management of Hyperglycemia Guillermo Umpierrez, MD, CDE Saturday, February 1, 218 1:3 a.m. 11:15 a.m. There are over 7.5 million hospital admissions for patients with diabetes in the US. About
Insulin Regimens: Hitting Glycemia Targets
 Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting
 Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Managing Diabetes and Hyperglycemia Safely in the Complex Hospital Setting Greg Maynard MD, MSc Clinical Professor of Medicine and CQO, UC Davis Medical Center Sacramento, CA Greg Maynard Disclosure SHM
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action
 Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action Learning Objectives Identify patient situations where specific attention to glycemic control is warranted Determine
Optimizing Care of the Inpatient with Hyperglycemia and Diabetes: Case Studies in Action Learning Objectives Identify patient situations where specific attention to glycemic control is warranted Determine
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Glucose Management in the ICU: The Role of the Pharmacist
 Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Objectives Glucose Management in the ICU: The Role of the Pharmacist James Gilmore PharmD, BCPS Senior Pharmacist- Surgical Intensive Care Unit Brigham and Women s Hospital Boston, MA Evaluate primary
Disclosure. Disclosure. Disclosure. Course Outline. Objectives. A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings 7/25/2013
 47 th Annual Meeting August 2-4, 2013 Orlando, FL A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings Kevin Forbush, Pharm. D Central Maine Medical Center Lewiston, Maine Disclosure I do
47 th Annual Meeting August 2-4, 2013 Orlando, FL A Touch of Sugar : Controlling Hyperglycemia in Acute Care Settings Kevin Forbush, Pharm. D Central Maine Medical Center Lewiston, Maine Disclosure I do
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine
 The Approach to Inpatient Hyperglycemia Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine Great Lakes Hospital Medical Symposium May 7th 2010 Further Increases in the Prevalence of Diabetes
The Approach to Inpatient Hyperglycemia Martin J Stevens MD, FRCP, Endocrinologist and Professor of Medicine Great Lakes Hospital Medical Symposium May 7th 2010 Further Increases in the Prevalence of Diabetes
Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Insulin Basics. Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology
 Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Insulin Basics Bryan Primary Care Conference May 21, 2016 Shannon Wakeley MD Complete Endocrinology Disclosures Speakers Bureau for Sanofi, Astra Zeneca, Janssen, Boehringer-Ingelheim Objectives Discuss
Nph insulin conversion to lantus
 Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Deepika Reddy MD Department of Endocrinology
 Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN. Kacy Aderhold, MSN, APRN-CNS, CMSRN
 HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
HYPERGLYCEMIA MANAGEMENT PROTOCOL A BASAL/BOLUS REGIMEN Kacy Aderhold, MSN, APRN-CNS, CMSRN Hyperglycemia Management Protocol Mimics the body s normal pancreas function, releasing a slow steady amount
NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING
 Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Sharp HealthCare s 2016 Diabetes Conference November 11, 2016 NOT-SO-SWEET! THE STRAIGHT SCOOP ON DIABETES IN THE HOSPITAL SETTING Tamara Swigert, MSN, RN, CDE Speaker Disclosure Tammy Swigert has no conflicts
Evidence for Basal Bolus Insulin Versus Slide Scale Insulin
 Curr Emerg Hosp Med Rep (2014) 2:26 34 DOI 10.1007/s40138-013-0032-4 DIABETES AND METABOLIC DISEASE (W FORD, SECTION EDITOR) Evidence for Basal Bolus Insulin Versus Slide Scale Insulin Sameer Badlani William
Curr Emerg Hosp Med Rep (2014) 2:26 34 DOI 10.1007/s40138-013-0032-4 DIABETES AND METABOLIC DISEASE (W FORD, SECTION EDITOR) Evidence for Basal Bolus Insulin Versus Slide Scale Insulin Sameer Badlani William
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
4/10/2015. Foundations to Managing Inpatient Hyperglycemia. Learning Objectives
 Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
LIBERTYHEALTH. Jersey City Medical Center Department of Patient Care Services. Approved by Policy Committee:
 LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
9/16/2013. No Conflict of Interest to Disclose
 Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
nocturnal hypoglycemia percentage of Hispanics in the insulin glargine than NPH during forced patients who previously This study excluded
 Clinical Trial Design/ Primary Objective Insulin glargine Treat-to-Target Trial, Riddle et al., 2003 (23) AT.LANTUS trial, Davies et al., 2005 (24) INSIGHT trial, Gerstein et al., 2006 (25) multicenter,
Clinical Trial Design/ Primary Objective Insulin glargine Treat-to-Target Trial, Riddle et al., 2003 (23) AT.LANTUS trial, Davies et al., 2005 (24) INSIGHT trial, Gerstein et al., 2006 (25) multicenter,
ANNUAL MEETING 2 #FSHP2017
 FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
Learning Objectives. Perioperative SWEET Success
 Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
In - Hospital Diabetes Care. A review and personal experience
 In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
Diabetes: Inpatient Glucose control
 Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Glycemic Control Hitting the Sweet Spot During Inpatient Care
 Glycemic Control Hitting the Sweet Spot During Inpatient Care Tim R. Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Family Medicine Cleveland Clinic Akron General Professor, Northeast
Glycemic Control Hitting the Sweet Spot During Inpatient Care Tim R. Brown, PharmD, BCACP, FASHP Director of Clinical Pharmacotherapy, Family Medicine Cleveland Clinic Akron General Professor, Northeast
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
How to BBIT An Educational Resource for Prescribers AHS Adult Subcutaneous Basal Bolus Insulin Therapy (BBIT)
") How to BBIT An Educational Resource for Prescribers AHS Adult Subcutaneous Basal Bolus Insulin Therapy (BBIT) The Basics, New Concepts and Practical Pearls for Basal Bolus Insulin Therapy February 2018
How to BBIT An Educational Resource for Prescribers AHS Adult Subcutaneous Basal Bolus Insulin Therapy (BBIT) The Basics, New Concepts and Practical Pearls for Basal Bolus Insulin Therapy February 2018
123 Are You Providing Evidence-Based Diabetes Care? - Martin
 Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Donna Martin, DNP, RN, CDE, CMSRN Lewis University Learner will be able to: Identify current inpatient standards of care for patients with diabetes Describe causes of hyperglycemia / hypoglycemia in the
Disclosures. Glycemic Control in the Intensive Care Unit. Objectives. Hyperglycemia. Hyperglycemia. History. No disclosures
 Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
Disclosures Glycemic Control in the Intensive Care Unit No disclosures Jorie Frasiolas, Pharm.D., BCPS Clinical Pharmacy Manager, CTICU NewYork-Presbyterian Hospital Columbia University Medical Center
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies
 Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies Leigh Briscoe-Dwyer, PharmD, BCPS, FASHP Chief Pharmacy and Medication Safety Officer North Shore Long Island Jewish Health
Improving Inpatient Diabetes Care: Focus on Safe Use of Anti-diabetic Therapies Leigh Briscoe-Dwyer, PharmD, BCPS, FASHP Chief Pharmacy and Medication Safety Officer North Shore Long Island Jewish Health
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical
 Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
Diabetes Technology Continuous Subcutaneous Insulin Infusion Therapy And Continuous Glucose Monitoring In Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Anne Peters, MD (Chair)
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk
 Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk Harvard/Joslin Primary Care Congress for Cardiometabolic Health 2013 Richard S. Beaser, MD Medical Executive
Evolving insulin therapy: Insulin replacement methods and the impact on cardiometabolic risk Harvard/Joslin Primary Care Congress for Cardiometabolic Health 2013 Richard S. Beaser, MD Medical Executive
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Pharmacy Plan Guidance
 Pharmacy Plan Guidance The pharmacy plan is a tool used during the site readiness process to develop and document the site-specific procedures for study drug ordering, labeling and dispensing for the SHINE
Pharmacy Plan Guidance The pharmacy plan is a tool used during the site readiness process to develop and document the site-specific procedures for study drug ordering, labeling and dispensing for the SHINE
Welcome Everyone. Monitoring, Sick Days, Inpatient Management - Objectives. Mrs. Jones has new diabetes. She asks you: Page 1
 Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Welcome Everyone Sign-In Enjoy Breakfast Meet someone new Enter Raffle Pick a team name Please silence phones We start at 8:00am Monitoring, Sick Days, Inpatient Management - Objectives Objectives: Strategies
Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting:
 T h e E n d o c r i n e S o c i e t y s Clinical Guidelines Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline Authors:
T h e E n d o c r i n e S o c i e t y s Clinical Guidelines Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline Authors:
LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA
 LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018 Objectives 1. Identify common preventable causes of hypoglycemia
LOW SUGAR: CAUSES, COMPLICATIONS AND MANAGEMENT OF HYPOGLYCEMIA Anne Leake, PhD, APRN-Rx, BC-ADM ECHO Diabetes Learning Group 3/28/2018 Objectives 1. Identify common preventable causes of hypoglycemia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Peripartum and Postpartum Management of Diabetes
 Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
Peripartum and Postpartum Management of Diabetes General Principles Glucose goal ~ 100 mg/dl (70-110 mg/dl) Labor is EXERCISE with increased metabolic demands. Insulin requirements decrease however the
ClinicalTrials.gov Identifier: sanofi-aventis. Sponsor/company:
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinicalTrials.gov
Diabetic Ketoacidosis (DKA) Critical Care Guideline Two Bag System
 Critical Care Guideline Two Bag System") Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Glucose Management in Noncritical Hospitalized Patients
 Glucose Management in Noncritical Hospitalized Patients October 17, 2015 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill
Glucose Management in Noncritical Hospitalized Patients October 17, 2015 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill
Hypoglycemia Reduction STARTER PACK WEBINAR #1
 Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Hypoglycemia Reduction STARTER PACK WEBINAR #1 Why is it important to reduce hypoglycemia? Why Hypoglycemia Reduction? Key Statistics Overall 29% reduction in ADEs since 2010 Hypoglycemia still occurs
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Glucose Management in NON-ICU Hospitalized Patients
 Glucose Management in NON-ICU Hospitalized Patients October 15, 2016 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill Cornell
Glucose Management in NON-ICU Hospitalized Patients October 15, 2016 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill Cornell
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Poll Question 2. Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services.
 Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Poll Question 1 Mary takes 6 units lispro (Humalog) before dinner. Which BG result reflects
Special Boot Camp Workshop Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Poll Question 1 Mary takes 6 units lispro (Humalog) before dinner. Which BG result reflects
9/23/09. What are the key components of preoperative, intraoperative, & postoperative care of diabetes management? Rebecca L. Sturges, M.D.
 RMHS Perioperative Summit: Perioperative Diabetes Management Rebecca L. Sturges, M.D. Oct 6, 2009 Mrs. B was referred by her orthopedic surgeon to your preoperative clinic to discuss medical management
RMHS Perioperative Summit: Perioperative Diabetes Management Rebecca L. Sturges, M.D. Oct 6, 2009 Mrs. B was referred by her orthopedic surgeon to your preoperative clinic to discuss medical management
5/15/2018 DISCLOSURE OBJECTIVES. FLORIDA HOSPITAL ORLANDO Not for profit organization Acute care medical center 1,368 licensed beds BACKGROUND
 DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
In-hospital management of diabetes
 Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Dr. Tom Elliott MBBS, FRCPC Medical Director 400-210 W Broadway phone: 604.683.3734 Vancouver, BC fax: 604.628.3821 V5Y 3W2 Canada email: moa@bcdiabetes.ca In-hospital management of diabetes General Management
Individualising Insulin Regimens: Premixed or basal plus/bolus?
 Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Individualising Insulin Regimens: Premixed or basal plus/bolus? Dr. Ted Wu Director, Diabetes Centre, Hospital Sydney, Australia Turkey, April 2015 Centre of Health Professional Education Optimising insulin
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Improving Glycemic Control in the Critical Care
 Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions
 Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Implementing Glucose Control in 2009 and Beyond: Changes in Patterns and Perceptions Charles C. Reed MSN, RN, CNRN Patient Care Coordinator Surgical Trauma ICU University Hospital San Antonio, Texas Relationships
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins. Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP
 These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
This certificate-level program is non-sponsored.
 Program Name: Diabetes Education : A Comprehensive Review Module 5 Intensive Insulin Therapy Planning Committee: Michael Boivin, B. Pharm. Johanne Fortier, BSc.Sc, BPh.LPh, CDE Carlene Oleksyn, B.S.P.
Program Name: Diabetes Education : A Comprehensive Review Module 5 Intensive Insulin Therapy Planning Committee: Michael Boivin, B. Pharm. Johanne Fortier, BSc.Sc, BPh.LPh, CDE Carlene Oleksyn, B.S.P.
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It
 The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary
 Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
The principles of insulin adjustment guidance
 The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
The principles of insulin adjustment guidance Tips for insulin titration Blood glucose (BG) monitoring is needed to help identify the efficacy of treatment in diabetes. Monitor blood glucose according
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Inpatient Diabetes and Hyperglycaemia. Philip Dyer Heart of England NHS Foundation Trust Birmingham
 Inpatient Diabetes and Hyperglycaemia Philip Dyer Heart of England NHS Foundation Trust Birmingham Outline of the Talk Definitions and the burden The impact and the cost A case The effects of hyperglycaemia
Inpatient Diabetes and Hyperglycaemia Philip Dyer Heart of England NHS Foundation Trust Birmingham Outline of the Talk Definitions and the burden The impact and the cost A case The effects of hyperglycaemia
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Inpatient Glycemic Management 2016
 2016 Jim Chamberlain MD Medical Director for Diabetes Services St. Mark s Hospital and St. Mark s Diabetes Center Salt Lake City, Utah Disclosures Speakers Bureaus Merck & Co. Janssen Pharmaceutical Companies
2016 Jim Chamberlain MD Medical Director for Diabetes Services St. Mark s Hospital and St. Mark s Diabetes Center Salt Lake City, Utah Disclosures Speakers Bureaus Merck & Co. Janssen Pharmaceutical Companies
Important Stuff. Basal Bolus What Adjustments? Pt weighs 80kg
 Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
Diabetes Boot Camp Class 4 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Special Insulin and Pattern Management Diabetes Education Services 1998-2015. All rights
How to manage type 2 diabetes in medical and surgical patients in the hospital
 MEDICAL GRAND ROUNDS CME CREDIT EDUCATIONAL OBJECTIVE: Readers will learn the relationship between glycemic control and clinical outcomes in hospitalized medical and surgical patients who are not in an
MEDICAL GRAND ROUNDS CME CREDIT EDUCATIONAL OBJECTIVE: Readers will learn the relationship between glycemic control and clinical outcomes in hospitalized medical and surgical patients who are not in an
Management of Inpatient Hyperglycemia: 2011 Endocrine Society Meeting Hyperglycemia in Critically ill patients in ICU Settings.
 Management of Inpatient Hyperglycemia: 2011 Endocrine Society Meeting Guillermo E. Umpierrez, MD, Emory University School of Medicine and Jack Leahy, MD, University of Connecticut Hyperglycemia in Critically
Management of Inpatient Hyperglycemia: 2011 Endocrine Society Meeting Guillermo E. Umpierrez, MD, Emory University School of Medicine and Jack Leahy, MD, University of Connecticut Hyperglycemia in Critically
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia
 CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia Javier Carrasco, MD, PhD Juan Ramón Jiménez Hospital University of Huelva, Spain Case Study: Medical and Social History A 60 years old female
CHALLENGING CASE PRESENTATION Steroid Induced Hyperglycemia Javier Carrasco, MD, PhD Juan Ramón Jiménez Hospital University of Huelva, Spain Case Study: Medical and Social History A 60 years old female
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches