Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
|
|
|
- Charla Crystal Casey
- 5 years ago
- Views:
Transcription

1 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies available Kaberi Dasgupta, Associate Professor of Medicine, McGill University
2 Canadian Society of Internal Medicine Annual Meeting 2016 The following presentation represents the views of the speaker at the time of the presentation. This information is meant for educational purposes, and should not replace other sources of information or your medical judgment. K Dasgupta: Choosing the right agent for your diabetes patient 28 October 2016
3 Canadian Society of Internal Medicine Annual Meeting 2016 Conflict Disclosures I sit on the CDA 2018 pharmacotherapy in type 2 diabetes chapter. I have held and hold research grants from the CIHR, FRQS, Heart and Stroke Foundation, Canadian Diabetes Association, Lawson Foundation, Medavie Foundation, and Diabete Quebec. None of these place me in conflict. I study health behaviour change in type 2 diabetes, gestational diabetes, and hypertension. Some of the drugs, devices, or treatment modalities mentioned in this presentation are: All current classes of antihyperglycemic medications
4 1. Identify therapeutic options for patients on maximal doses of / intolerant to biguanides, sulfonylureas, and insulin 1. Compare and contrast the effects of the expanding options for anti-diabetic agents in diabetic patients, considering the risks of hypoglycaemia, body weight and other their side effects. 2. Interpret the evidence for cardiovascular outcomes for various hypoglycaemic agents 3. Recognize the impact of egfr on prescribing medications for type 2 diabetes.
5 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemia Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost -glucosidase inhibitor (acarbose) Rare neutral to Improved postprandial control, GI sideeffects $$ Incretin agents: DPP-4 Inhibitors GLP-1R agonists to Rare Rare Neutral to Superior (Lira, ) Neutral (alo, saxa, sita) Neutral (lixi) Caution with saxagliptin in heart failure GI side-effects $$$ $$$$ Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $- $$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare Superiority (empa in T2DM patients with clinical CVD) Genital infections, UTI, hypotension, dose-related changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$ Thiazolidinediones Rare Neutral CHF, edema, fractures, rare bladder cancer (pioglitazone), cardiovascular controversy (rosiglitazone), 6-12 weeks required for maximal effect $$ Weight loss agent None GI side effects $$$ (orlistat) guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 alo=alogliptin; Canadian Diabetes glar=glargine; Association saxa=saxagliptin; sita=sitagliptin; lixi=lixisenatide; empa=empagliflozin 201
6 The ominous octet (3) depicting the mechanism and site of action of antidiabetes medications based upon the pathophysiologic disturbances present in T2DM. View at: Ralph A. DeFronzo et al. Dia Care 2013;36:S127-S by American Diabetes Association
7 67 year old woman with type 2 diabetes diagnosed 15 years ago and hypertension for the past 10 years. Her A1C is 8.7%, blood pressure is 140/90 mm Hg in your office, and her LDL is 2.2 mmol/l. Her GFR is 45. Her BMI is 34 kg/m2, her waist circumference is 93 cm, and she walks her dog 20 minutes each day. Her current medications include a statin, ASA, perindoprilindapamide combination, metformin, and maximal doses of gliclazide MR. She had an MI 1 year ago. How would you manage this patient?

8 Glucose filtered, glucose resorbed (proximal tubule) Glucosuria if maximal transporter capacity exceeded SGLT2 inhibitors block reabsorption at higher glucose levels Glucose Glucose
9 Both sodium and glucose are excreted when SGLT2 is blocked View at: Chao EC, Henry RR. SGLT2 inhibition: A novel strategy for diabetes treatment. Nat Rev Drug Discov.2010;9:551 9
10 Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes, Zinman and colleagues, Nov 2015 Population- High risk CVD Adults BMI < 45 kg/m2 GFR > 30 established CVD (MI, stroke, amputation, multivessel coronary artery disease, or CABG) Intervention/comparison Empagliflozin 10 mg vs. placebo Empagliflozin 20 mg vs. placebo Outcomes: CVD morbidity and mortality
11 Antihyperglycemics Metformin 74% Insulin 48% Sulfonylureas 43% DPP-4 inhibitor 11% TZD 4% GLP 1 agonist 3% Other cardioprotective ACE I/ARB 81% Beta blocker 65% Diuretic 44% Statin 77% ASA 83% Plavix 11%
12 Some A1C lowering View at: (fig 3) Zinman B et al. N Engl J Med 2015;373:
13 Blood pressure lowering View here: Fig 1 Ilkka Tikkanen et al. Dia Care 2015;38: by American Diabetes Association

14 Primary and Secondary Cardiovascular Outcomes. Zinman B et al. N Engl J Med 2015;373:

15 Genital infections Vulvovaginal infections Balanitis Candida Adverse Events. Zinman B et al. N Engl J Med 2015;373:
16
 In Europe")

17 Canagliflozin (Invokana) Dapagliflozin (Forxiga) In Europe these and empagliflozin are available in combination with metformin From CDA website, 2016:
18 Rare but life threatening cases have occurred in type 2 diabetes patient taking SGLT2 inhibitors Glucose levels may not be as high as expected for DKA Context Low insulin production or increased need Symptoms Nausea and vomiting Abdominal pain Thirst Tachypnea Confusion Medscape, Internal Medicine European Medicines Agency, 2016
19 A. In whom should we use empagliflozin? All patients with type 2 diabetes? Those with established CVD? Those with creatinine clearance above 30? All patients with renal injury? What other antihyperglycemic agents should be used first? A. Is this a class effect?
20 Secreted by intestinal mucosa (ileum, distal colon) Half-life under two minutes enzyme dipeptidyl peptidase-iv (DPP-IV) Stimulates insulin secretion Slows gastric emptying Short half-life in circulation Liraglutide 97% structurally similar to GLP-1 Longer half life because of a fatty chain for binding with proteins
21 Manning and colleagues, Physiology, Published 5 January 2015 Vol. 30 no. 1, View here: Fig 2
22 Type 2 diabetes 18 years BMI < 45 kg/m2 GFR > 30 established CVD with 1 or more of: MI Stroke Amputation Multivessel coronary artery disease CABG EMPAreg eligibility A1C 7% 50 years with 1 Coronary heart disease Cerebrovascular disease Peripheral vascular disease Chronic kidney disease stage 3 or greater 60 years with 1 Microalbuminuria/Proteinuria Hypertension with LVH LV systolic or diastolic dysfunction Chronic kidney disease stage 3 or greater Ankle-brachial index < 0.9 LEADER eligibility
23 Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes, Marso and colleagues, Aug 2016 Intervention/comparison 1.8 mg liraglutide injection once daily vs. placebo following run-in period Stratified randomization by GFR (< 30 ) Outcomes Composite Death from cardiovascular causes Nonfatal MI Nonfatal stroke Coronary revascularization Hospitalization for unstable angina Hospitalization for heart failure
24 Primary Composite Outcomes in Various Demographic and Clinical Subgroups. View here Table 1 Marso SP et al. N Engl J Med 2016;375: View here Fig 2 Marso SP et al. N Engl J Med 2016;375: View here Table 2 Marso SP et al. N Engl J Med 2016;375:
25
26 Exenatide Lixisenatide Dulaglutide Albiglutide Semaglutide

27 Once/week GLP-1 agonis
28 In whom would you use a GLP-1 agonist? Which one? Why?

29 DPP 4 saxagliptin and heart failure
30 Population Type 2 diabetes 35 to 75 years of age with A1C > 6.5% MI, stroke, PTCA, CABG, PVD, Intervention vs. Control Pioglitazone vs. placebo
31
32
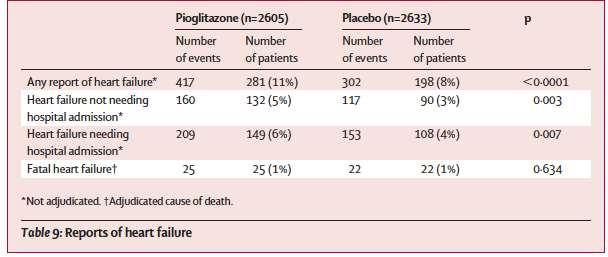
33

34 Population No type 2 diabetes HOMA-IR > 3 Ischemic stroke or TIA Intervention vs Control Pioglitazone vs. Placebo Outcome Fatal or nonfatal stroke or MI
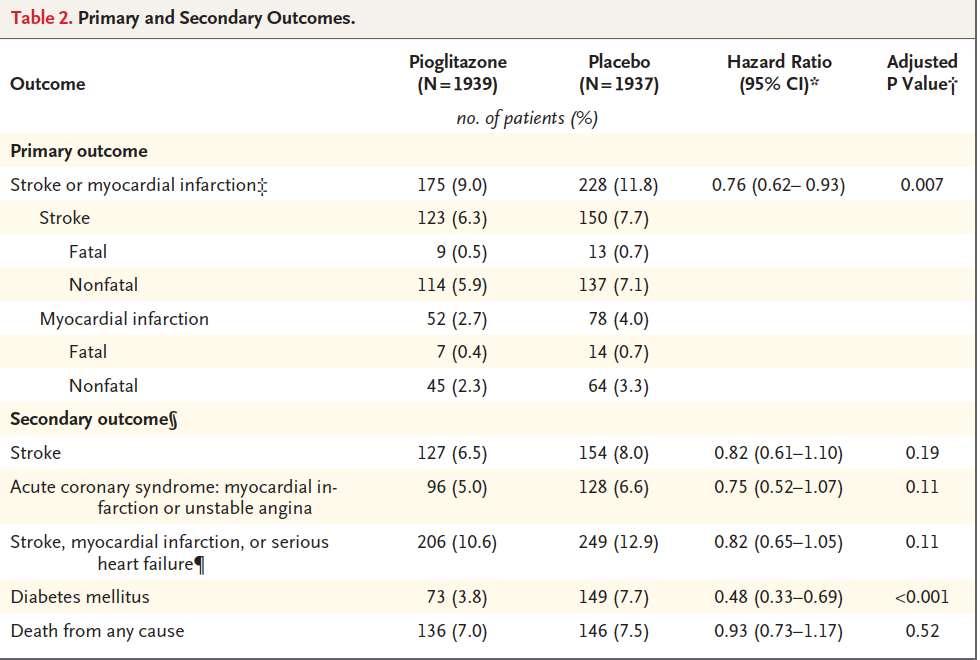
35
36 Many agents lower A1C to similar extent DeFronzo provides evidence that durability of glycemic control differs across agents Studying the impact of combo therapy
37 The effect of sulfonylurea (glibenclamide = glyburide) and metformin therapy on the plasma HbA1c concentration in newly diagnosed T2DM subjects in UKPDS. Conventionally treated diabetic subjects received diet plus exercise therapy (113,114). View here: Fig 3 Ralph A. DeFronzo et al. Dia Care 2013;36:S127-S by American Diabetes Association
38 Durability of glycemic control with sulfonylureas. View here: Fig 4 Ralph A. DeFronzo et al. Dia Care 2013;36:S127-S by American Diabetes Association
39 Durability of glycemic control with TZDs. Summary of studies examining the effect of TZDs versus placebo or versus active comparator on HbA1c in T2DM subjects. View here: Fig 5 Ralph A. DeFronzo et al. Dia Care 2013;36:S127-S by American Diabetes Association
40 Population Newly diagnosed type 2 diabetes patients Intervention Combination: Pioglitazone, metformin, exenatide Comparison Sequential: metformin, then sulfonylurea, then insulin Outcome A1C 134 patients (preliminary): 2.7% vs. 2.2% reduction at 2 years with 1.5 vs 4 kg loss and less hypos
41 The ominous octet (3) depicting the mechanism and site of action of antidiabetes medications based upon the pathophysiologic disturbances present in T2DM. View at: Ralph A. DeFronzo et al. Dia Care 2013;36:S127-S by American Diabetes Association
 Rare neutral to Improved postprandial control, GI sideeffects $$ Incretin agents: DPP-4 Inhibitors GLP-1R agonists to Rare Rare")
42 Add another class of agent best suited to the individual (agents listed in alphabetical order): Class Relative A1C Lowering Hypoglycemia Weight Effect in Cardiovascular Outcome Trial Other therapeutic considerations Cost -glucosidase inhibitor (acarbose) Rare neutral to Improved postprandial control, GI sideeffects $$ Incretin agents: DPP-4 Inhibitors GLP-1R agonists to Rare Rare Neutral to Superior (Lira, ) Neutral (alo, saxa, sita) Neutral (lixi) Caution with saxagliptin in heart failure GI side-effects $$$ $$$$ Insulin Yes Neutral (glar) No dose ceiling, flexible regimens $- $$$$ Insulin secretagogue: Meglitinide Sulfonylurea Yes Yes Less hypoglycemia in context of missed meals but usually requires TID to QID dosing Gliclazide and glimepiride associated with less hypoglycemia than glyburide $$ $ SGLT2 inhibitors to Rare Superiority (empa in T2DM patients with clinical CVD) Genital infections, UTI, hypotension, dose-related changes in LDL-C, caution with renal dysfunction and loop diuretics, dapagliflozin not to be used if bladder cancer, rare diabetic ketoacidosis (may occur with no hyperglycemia) $$$ Thiazolidinediones Rare Neutral CHF, edema, fractures, rare bladder cancer (pioglitazone), cardiovascular controversy (rosiglitazone), 6-12 weeks required for maximal effect $$ Weight loss agent None GI side effects $$$ (orlistat) guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 alo=alogliptin; Canadian Diabetes glar=glargine; Association saxa=saxagliptin; sita=sitagliptin; lixi=lixisenatide; empa=empagliflozin 201
43 If you were diagnosed with type 2 diabetes, what would you do?
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
CASES DR TINA KADER MCGILL JGH; LMC CVPH CDE
 CASES DR TINA KADER MCGILL JGH; LMC CVPH CDE Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria:
CASES DR TINA KADER MCGILL JGH; LMC CVPH CDE Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria:
Faculty/Presenter Disclosure
 DIABETES UPATE 2016 Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria: eli lilly sanofi;
DIABETES UPATE 2016 Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria: eli lilly sanofi;
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC
 MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
In-Hospital Management of Diabetes. Dr Benjamin Schiff Assistant Professor McGill University
 In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
In-Hospital Management of Diabetes Dr Benjamin Schiff Assistant Professor McGill University No conflict of interest to declare CLINICAL SCENARIO 62 y/o male with hx of DM 2, COPD, and HT is admitted with
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Canadian Diabetes Association 2013 Clinical Practice Guidelines
 Canadian Diabetes Association 2013 Clinical Practice Guidelines The Essentials (Updated d November 2016) 2016 1 Faculty/Presenter Disclosure Faculty: Alan Bell MD CCFP Relationships with commercial and
Canadian Diabetes Association 2013 Clinical Practice Guidelines The Essentials (Updated d November 2016) 2016 1 Faculty/Presenter Disclosure Faculty: Alan Bell MD CCFP Relationships with commercial and
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Canadian Diabetes Association 2013
 Spring 2014 Canadian Diabetes Association 2013 clinical practice guidelines - Do claims data align to the guidelines? Canadian Diabetes Association 2013 clinical practice guidelines - Do claims data align
Spring 2014 Canadian Diabetes Association 2013 clinical practice guidelines - Do claims data align to the guidelines? Canadian Diabetes Association 2013 clinical practice guidelines - Do claims data align
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Vascular complications
 Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Michael Mansfield Consultant Leeds Teaching Hospitals
 Easing, fixing and avoiding diabetic hyperglycaemia: new drugs, new approaches Michael Mansfield Consultant Leeds Teaching Hospitals Declaration: no significant gifts, fees, funding from pharma Topics:
Easing, fixing and avoiding diabetic hyperglycaemia: new drugs, new approaches Michael Mansfield Consultant Leeds Teaching Hospitals Declaration: no significant gifts, fees, funding from pharma Topics:
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Canadian Journal of Diabetes
 Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
DIABETES UPDATE 2018
 DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Content Development Committee
 1 Content Development Committee Cardiologists: Family Physicians: Shaun Goodman, MD, MSc, FRCPC, FACC, FESC, FAHA, FCCS (Chair) Associate Head, Division of Cardiology, St. Michael s Hospital Professor,
1 Content Development Committee Cardiologists: Family Physicians: Shaun Goodman, MD, MSc, FRCPC, FACC, FESC, FAHA, FCCS (Chair) Associate Head, Division of Cardiology, St. Michael s Hospital Professor,
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital
 Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Disclosures. Type 2 Diabetes. The New Epidemic: How Did We Get Here and What's to Come? Summary:
 Type 2. The New Epidemic: How Did We Get Here and What's to Come? Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco None Disclosures robert.rushakoff@ucsf.edu Type 2.
Type 2. The New Epidemic: How Did We Get Here and What's to Come? Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco None Disclosures robert.rushakoff@ucsf.edu Type 2.
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Making Sense of New DM Therapies and Technologies
 Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
What to add after metformin: primary care conference 2016
 objectives What to add after metformin: primary care conference 216 Dr. Tsang Man Wo Specialist in Endocrinology, Diabetes & Metabolism Medical Director, United Medical Practice. Consultant (P), M+G department,
objectives What to add after metformin: primary care conference 216 Dr. Tsang Man Wo Specialist in Endocrinology, Diabetes & Metabolism Medical Director, United Medical Practice. Consultant (P), M+G department,
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.