Multimodal monitoring to prognosticate in anoxic brain injury
|
|
|
- Berniece Stephens
- 6 years ago
- Views:
Transcription

1 Multimodal monitoring to prognosticate in anoxic brain injury Eyal Golan, MD FRCPC PhD(c) Critical Care & Neurosciences Critical Care Medicine Interdepartmental Division of Critical Care and Department of Medicine University of Toronto
2 Conflicts of interest Financial None (unfortunately) Academic Research program Guideline development (ILCOR, AHA-ECC, CCCTG-CNCS) Evidence reviewer for ILCOR
3 Neuroprognostication things to consider ILCOR review New guidelines

4 Case presentation 65M collapses at home while watching game 6 of the Blue Jays in Kansas - Bystander CPR is performed by his wife - EMS arrives at scene and perform ACLS - Time to ROSC 30min - Patient is brought to ER
5 Family asks what s the prognosis
6 Day 1 Patient is admitted to the ICU and receives TTM intervention (cooling & sedation) On exam, patient is decerebrate (GCS-M = 2) Myoclonic jerks are seen intermittently EEG performed showing encephalopahy CT head at 2hr post-rosc Mild loss of GM/WM differentiation Biomarkers sent Neuron-specific enolase 24hrs = 30
7
8 Day 2 TTM intervention is completed Best motor exam still decerebrate (GCS-M = 2) ceeg is placed no seizures Pupils 3mm and sluggish Biomarkers sent Neuron-specific enolase 48hrs = 40
9
10 Day 3 (72hr after ROSC) No myoclonic jerks ceeg no change Brainstem testing - no change (sluggish pupils & decerebrate) Repeat CT head - slightly worse GM/WM differentiation; edema R>L SSEP absent on R-side TCDs performed suggestive of hyperemia +/- ischemia
11
12 Day 5 (72hr after return to normothermia) No myoclonic jerks EEG no change Brainstem testing bilaterally absent pupillary reflex SSEP bilaterally absent Biomarkers sent Neuron-specific enolase = 80 Optic nerve ultrasound ONSD 6.2 mm bilaterally
13
 Basis of recent guideline recommendations from ILCOR AHA ERC")
14 Family asks what s the prognosis Likely poor neurological outcome with near certainty (FPR near 0% with narrow confidence interval) Basis of recent guideline recommendations from ILCOR AHA ERC CCCTG-CNCS
15 We just performed appropriate multimodal prognostication Continued aggressive management until minimum time from ROSC attained Avoided self-fulfilling prophecies Applied >2 recognized modes Time from ROSC for each mode taken into account Trends in results taken into account (ex. biomarkers & imaging)
16 Prognostication after cardiac arrest Key topic in resuscitation research With the advancement of neurocritical care, studies now examining invasive and non-invasive prognostic tests Newly released guidelines with a focus on an appropriate multimodal approach Callaway CW et al, Circulation Nov 3;132(18 Suppl 2):S Howes DJ et al, Resuscitation Sep 28. pii: S (15) Nolan J et al, Resuscitation Sep 14. pii: S (15)
17 Factors to consider 1. Our predictions are important 2. Self-fulfilling prophecies 3. Dichotomous outcomes 4. Targeted temperature management 5. Selective memory 6. Diagnostic test accuracy
18 Factors to consider 1. Our predictions are important 2. Self-fulfilling prophecies 3. Dichotomous outcomes 4. Targeted temperature management 5. Selective memory 6. Diagnostic test accuracy

19 Termination of life support is the most common way that patients die during ICU Physician prediction of poor outcome is the strongest predictor of termination of life support We re just not very good at it. Clinicians are generally poor at subjectively predicting survival, functional outcome and quality after critical illness Cook et al. N Engl J Med 2003;349: Rocker et al. Crit Care Med 2004; 32: Simchen et al. Crit Care Med 2004; 32:1654 Frick et al. Crit Care Med; 2003, 31:456
20 Factors to consider 1. Our predictions are important 2. Self-fulfilling prophecies 3. Dichotomous outcomes 4. Targeted temperature management 5. Selective memory 6. Diagnostic test accuracy

21

22 Self-fulfilling prophecies Problems clinically Physicians become falsely reassured Problems for research Most studies do not prevent physicians from stopping life support in response to clinical predictors Newer trials aim to prevent early withdrawal Geocadin et al. Neurology 2006; 67:105 Geocadin et al. Curr Op Crit Care 2008; 14:261 Nielsen et al, N Engl J Med Dec 5;369(23):
23 Nielsen et al, N Engl J Med Dec 5;369(23):
24 High rate of protocol violation 37% early WLST 20% death due to early WLST Dragancea I et al, Resuscitation Aug;93:164-70
25 Factors to consider 1. Our predictions are important 2. Self-fulfilling prophecies 3. Dichotomous outcomes 4. Targeted temperature management 5. Selective memory 6. Diagnostic test accuracy

26 GOOD POOR Emphasis is on predicting poor, not good outcomes Patients may still wish to base decisions to withdraw life support on intermediate outcomes Spectrum of outcomes between disability and complete neurological recovery
27 Neuroprognostication after cardiac arrest in Europe Sandroni C et al, Resuscitation 2013;84:
28 Factors to consider 1. Our predictions are important 2. Self-fulfilling prophecies 3. Dichotomous outcomes 4. Targeted temperature management 5. Selective memory 6. Diagnostic test accuracy
29 Bernard et al, NEJM 2002 Holzer et al, NEJM 2002 Nielsen et al, NEJM 2013
30


31
32 The Targeted Temperature Management (TTM) Trial

33 The Targeted Temperature Management (TTM) Trial
34 TTM changes the accuracy of our clinical predictors Confounding due to sedating/paralyzing medications used to induce and maintain hypothermia May change accuracy of predictors used for neuroprognostication by attenuating degree of brain injury Does prognostication change with different levels of cooling?
35 TTM changes the accuracy of our clinical predictors Confounding due to sedating/paralyzing medications used to induce and maintain hypothermia May change accuracy of predictors used for neuroprognostication by attenuating degree of brain injury Does prognostication change with different levels of cooling?
36 Golan E, Resuscitation; 2015 Aug;93:A9-10

37 No difference in diagnostic test accuracies 36 C = 33 C for prognostication Golan E, Resuscitation; 2015 Aug;93:A9-10
38 Factors to consider 1. Our predictions are important 2. Self-fulfilling prophecies 3. Dichotomous outcomes 4. Targeted temperature management 5. Selective memory 6. Diagnostic test accuracy
39 A 55-yr-old man presented with cardiac arrest spontaneous perfusion restored, and therapeutic hypothermia provided Death was pronounced and the family consented to organ donation 24 hrs after brain death, on arrival to the operating room for organ procurement, the patient was found to have regained corneal reflexes, cough reflex, and spontaneous respirations Webb and Samuels, CCM 2011

40 Factors to consider 1. Our predictions are important 2. Self-fulfilling prophecies 3. Dichotomous outcomes 4. Targeted temperature management 5. Selective memory 6. Diagnostic test accuracy
41 The confidence problem No consensus on the PRECISION that should be obtained for predicting poor outcomes How precise is precise enough? How wide should confidence intervals around ZERO be? 0% 95% CI 100 % Golan E, et al; Crit Care Med Aug;42(8): Downar J, You JJ, Bagshaw SM, Golan E, et al; Crit Care Med Feb;43(2):270-81
42 111 cardiac arrests treated with hypothermia Neurological examination HOURS EEG SSEP All measurements during normothermia and off sedation CPC assessed at 3 to 6 months
43
44

45


46

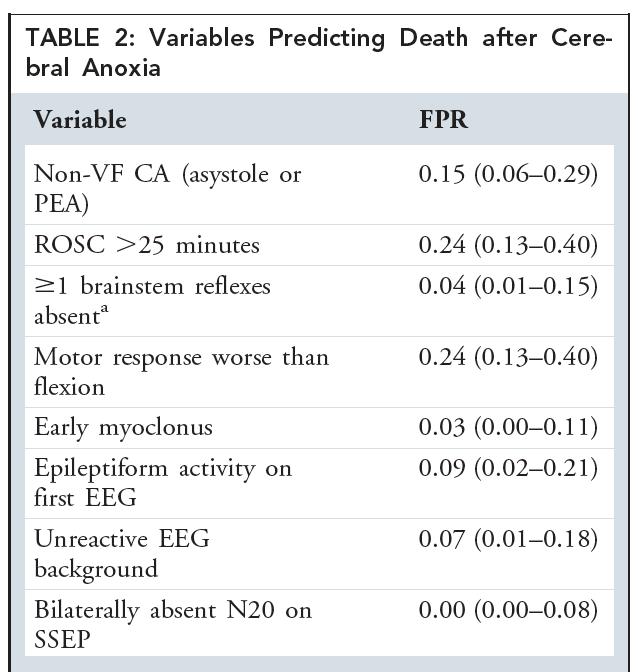
47 2015 ILCOR EVIDENCE EVALUATION RESULTS
48 Achieving Consensus regarding Resuscitation Science The American Heart Association and other member councils of International Liaison Committee on Resuscitation (ILCOR) complete a review of resuscitation science every five years. Australian Resuscitation Council

49 2015 CoSTR DEVELOPMENT Timeline International Consensus February Dallas Evidence Evaluation Reviews ILCOR December Porto ILCOR November Orlando ILCOR April Melbourne ILCOR March Banff PUBLIC COMMENT CoSTR and Guidelines Published Oct 2010 ILCOR November Vienna ILCOR November Chicago CoSTR and Guidelines Published October, 2015

50 International Evidence Evaluation Process 165 scientific evidence reviews February 2015 Consensus Conference 232 professional participants 46% from outside the US 34 countries represented Management of potential COI throughout process
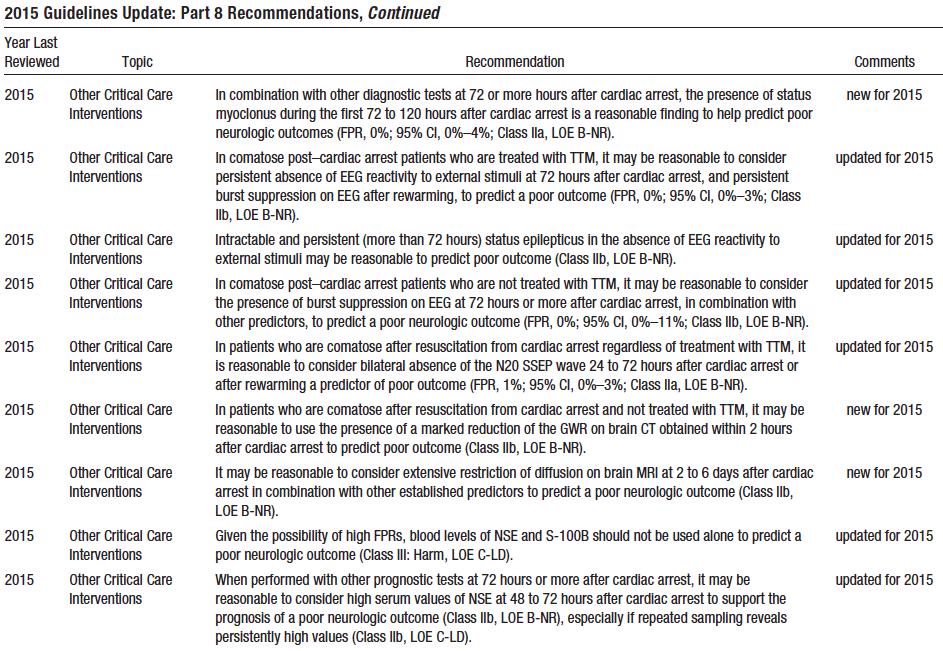
51
52 circ.ahajournals.org
53 Outcomes Outcome dichotomized to good neurological outcome (CPC 1-2) vs poor neurological outcome (CPC 3-5)
54 Clinical Examination timing is crucial Pupillary reflex Corneal reflex GCS-motor response Myoclonus
55 Clinical Examination Bilaterally absent pupillary light reflex at 72 to 108 hours after cardiac arrest predicted poor outcome, with an FPR of 1% (95% CI, 0% 3%) Bilaterally absent corneal reflexes at 72 to 120 hours after cardiac arrest predicted poor outcome, with a 2% FPR (95% CI, 0% 7%) Extensor posturing or no motor response to pain at 36 to 108 hours after cardiac arrest predicted poor outcome, with a 10% FPR (95% CI, 7% 15%)
56 Updated 2015 recommendations In comatose patients who are treated with TTM, the absence of pupillary reflex to light at 72 hours or more after cardiac arrest is useful to predict poor neurologic outcome (FPR, 1%; 95% CI, 0% 3%; Class I, LOE B-NR) Given their unacceptable FPRs, the findings of either absent motor movements or extensor posturing should not be used alone for predicting a poor neurologic outcome (FPR, 10%; 95% CI, 7% 15% to FPR; Class III: Harm, LOE B-NR)
57 Myoclonus and status myoclonus In 2015, new distinction between myoclonus and status myoclonus (continuous, repetitive myoclonic jerks lasting more than 30 minutes) The presence of any myoclonus is not a reliable predictor of poor functional recovery But status myoclonus within 72 to 120 hours after ROSC predicted poor outcome, with a 0% FPR (95% CI, 0% 4%).
58 Myoclonus and status myoclonus In 2015, new distinction between myoclonus and status myoclonus (continuous, repetitive myoclonic jerks lasting more than 30 minutes) The presence of any myoclonus is not a reliable predictor of poor functional recovery But status myoclonus within 72 to 120 hours after ROSC predicted poor outcome, with a 0% FPR (95% CI, 0% 4%).
59 Updated 2015 Recommendations We recommend that the presence of myoclonus, which is distinct from status myoclonus, should not be used to predict poor neurologic outcomes because of the high FPR (FPR, 5%; 95% CI, 3% 8% to FPR, 11%; 95% CI, 3% 26%; Class III: Harm, LOE B-NR). In combination with other diagnostic tests at 72 or more hours after cardiac arrest, the presence of status myoclonus during the first 72 to 120 hours after cardiac arrest is a reasonable finding to help predict poor neurologic outcomes (FPR, 0%; 95% CI, 0% 4%; Class IIa, LOE B-NR).

60 Electrophysiology modalities SSEP considered default gold standard in many studies BUT may artificially inflate the accuracy estimates EEG or ceeg are suggested, with caveat EEG and ceeg are used routinely for prognostication but no standardized terminology Difficult to attain in real time, or sometimes even at a reasonable time

61 Consistently unreliable

62 Consistently unreliable NOT recommended Low voltage EEG Low bispectral index EEG grades
63 Updated 2015 Recommendations Persistent absence of EEG reactivity to external stimuli at 72 hours after cardiac arrest, and persistent burst suppression on EEG after rewarming, predict a poor outcome (FPR, 0%; 95% CI, 0% 3%; Class IIb, LOE B-NR) Intractable and persistent (more than 72 hours) status epilepticus in the absence of EEG reactivity to external stimuli may be reasonable to predict poor outcome (Class IIb, LOE B-NR)


64 ERC-ESICM guidelines (combining unreactivity + BS/SE) Canadian guidelines ( malignant EEG; 1 of 4 definitions)
65 Imaging modalities Attractive modality CT or MRI can define structural brain injury, detect focal injury, and edema Edema can theoretically be quantified CT (quantified as GWR in Hounsfield units; Normal = 1.3, and decreases with edema) MRI (quantified by apparent diffusion coefficient; Normal ADC= Å~ 10 6 mm2/s and decrease with edema)
66 Evidence profile table CT Index Timing from ROSC Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] GWR BG <1.22 < 1 h Serious low [55-100] 0 [0-63] 7 [1-99] Average GWR <1.14 (BG/cerebrum) <1 h No low [4-31] 0 [0-13] 6 [0-113] GWR CN/PIC < h Serious No No Low [12-30] 0 [0-5] 24 [1-396] GWR P/CC < h Serious No No Low [41-64] 0 [0-5] 64 [4-1018] GWR CN/IC 1.18 < 1 h Serious No low [69-90] 8[0-38] 10 [1-64] Global cerebral oedema Median day 1 (1-7) Serious No Serious Low [13-40] 0 [0-5] 29 [2-479] BG = Basal ganglia; CC= Corpus callosum; CN = Caudate nucleus; PIC = Posterior limb of the internal capsule; P = Putamen
67 Evidence profile table MRI Index Timing from ROSC Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] Extensive cortical lesion pattern 80H (IQR ) No low [55-100] 9 [0-41] 10 [2-65] DWI changes in BG 80H (IQR ) No low [44-97] 9 [0-41] 9 [1-58] DWI changes in BS 80H (IQR ) No low [7-65] 0 [0-24] 8 [0-132] Changes in cortex + BG 74h (IQR 61-86) Serious Serious low [33-80] 0 [0-63] 5 [0-63] Changes in cortex + BG < 5 days No low [55-100] 0 [0-63] 7 [1-99] BG = Basal ganglia; BS = Brainstem
68 Evidence profile table MRI Index Timing from ROSC Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] ADC < mm 2 /sec in >10% of brain volume h Serious No low [46-95] 0 [0-28] 15 [1-227] Occipital cortex ADC < mm 2 /sec No low [75-98] 0 [0-24] 21 [1-324] Putamen ADC < mm 2 /sec 45.8 (IQR 36,8-52,4)) No low [60-91] 0 [0-24] 19 [1-281] Thalamus ADC < mm 2 /sec No low [44-79] 0 [0 24] 15 [1-228] ADC = Apparent Diffusion Coefficient
69 But Acquisition and interpretation of imaging studies have not been fully standardized and are subject to interobserver variability In addition, the recommendations are made with the assumption that images are performed in centers with expertise in this area
70 Updated 2015 Recommendations In patients who are comatose after resuscitation, it may be reasonable to use the presence of a marked reduction of the GWR on brain CT obtained within 2 hours after cardiac arrest to predict poor outcome (Class IIb, LOE B-NR) It may be reasonable to consider extensive restriction of diffusion on brain MRI at 2 to 6 days after cardiac arrest in combination with other established predictors to predict a poor neurologic outcome (Class IIb, LOE B-NR)
71 Biomarkers No threshold values that enable prediction of poor outcome with confidence were identified Laboratory standards vary between centers for the two most common markers, NSE and S-100B The kinetics have not been studied, particularly during or after TTM in cardiac arrest patients Importantly, NSE and S-100B are not specific to neuronal damage (can be produced by hemolysis, neuroendocrine tumors, myenteric plexus, muscle, and adipose tissue breakdown) Confirmatory > predictive
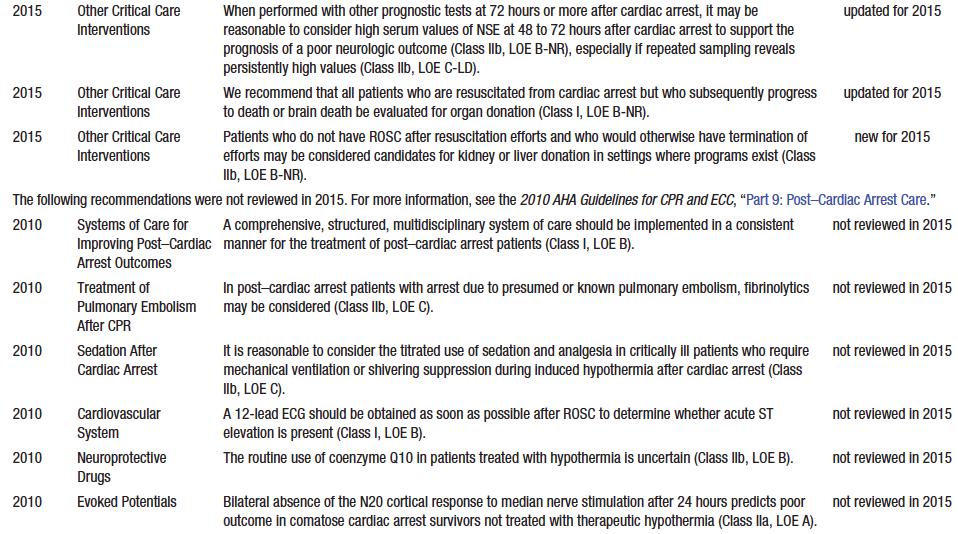
72 Updated 2015 Recommendations Given the possibility of high FPRs, blood levels of NSE and S-100B should not be used alone to predict a poor neurologic outcome (Class III: Harm, LOE C-LD) When performed with other prognostic tests at 72 hours or more after cardiac arrest, it may be reasonable to consider high serum values of NSE at 48 to 72 hours after cardiac arrest to support the prognosis of a poor neurologic outcome (Class IIb, LOE B-NR), especially if repeated sampling reveals persistently high values (Class IIb, LOE C-LD)



73





74 Achieving Consensus regarding Resuscitation Science Australian Resuscitation Council
, and the Canadian Critical Care Trials Group (CCCTG) Howes D, Gray SH, Brooks SC, Boyd JG, Djogovic D, Golan E, Green RS, Jacka MJ, Sinuff T, Chaplin T, Smith OM,")
75 Canadian Guidelines for the use of targeted temperature management (therapeutic hypothermia) after cardiac arrest: A joint statement from the Canadian Critical Care Society (CCCS), Canadian Neurocritical Care Society (CNCCS), and the Canadian Critical Care Trials Group (CCCTG) Howes D, Gray SH, Brooks SC, Boyd JG, Djogovic D, Golan E, Green RS, Jacka MJ, Sinuff T, Chaplin T, Smith OM, Owen J, Szulewski A, Murphy L, Irvine S, Jichici D, Muscedere J
76 Magnetic Resonance Imaging (MRI) EEG - NSE SSEP CT Status Myoclonus Cardiac arrest Days 1-2 Controlled temperature Rewarming Exclude confounders, particularly residual sedation Unconscious patient, M=1-2 at 72h after ROSC Days 3-5 One or both of the following: - No pupillary and corneal reflexes - Bilaterally absent N20 SSEP wave ( 1 ) No Wait at least 24h Yes Poor outcome very likely (FPR <5%, narrow 95%CIs) Two or more of the following: -Status myoclonus 48h after ROSC -High NSE levels ( 2 ) -Unreactive burst-suppression or status epilepticus on EEG -Diffuse anoxic injury on brain CT/MRI ( 2 ) Yes Poor outcome likely No Indeterminate outcome Observe and re-evaluate Use multimodal prognostication whenever possible (1) At 24h after ROSC in patients not treated with targeted temperature (2) See text for details. Sandroni C et al, Resuscitation Dec;85(12):

77 So what s your suggestion
78 So what s your suggestion Apply a protocol based strategy Rule out confounders Wait Use 2 modes
79 So what s your suggestion Apply a protocol based strategy Recognize and avoid self-fulfilling prophecy (aggressiveness and WLST) Family involvement Rule out confounders Wait Use 2 modes
80 So what s your suggestion Apply a protocol based strategy Rule out confounders Wait Use 2 modes
81 So what s your suggestion Apply a protocol based strategy Rule out confounders Rule out confounders to your diagnostic tests Do not attempt neuroprognostication until sedatives, paralytics have worn off, hypotension is treated Wait Use 2 modes
82 So what s your suggestion Apply a protocol based strategy Rule out confounders Wait Use 2 modes
83 So what s your suggestion Apply a protocol based strategy Rule out confounders Wait 72hrs post-nt for clinical examination 72hrs post-arrest for electrophysiology CT/MRI at specific points, in specific centers Use 2 modes
84 So what s your suggestion Apply a protocol based strategy Rule out confounders Wait Use 2 modes

85 Laurie Morrison Damon Scales Cliff Callaway Claudio Sandroni Daniel Howes Jas Soar Jerry Nolan
86 circ.ahajournals.org

87 Questions
88
89 Clinical Examination Evidence profile Predictor (studies) Timing Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] Corneal reflex (4) At h No Serious Serious low [18-32] 2 [0-7] 9 [2-29] Pupillary reflex (5) at h No No No Low [14-25] 1 [0-3] 5 [1-32] GCS Motor 1-2 (6) At h No No very very low [65-74] 10 [7-15] 6 [4-9] Myoclonus (5) At 24-72h No Serious very low [35-44] 5[3-8] 6 [4-10] Status myoclonus (3) 72h No No No Low [11-22] 0 [0-4] 6 [4-10]
90 Evidence profile table Predictor (studies) Absent N20 SSEP (4) Timing Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] During TTM Serious No No No Moderate [22-34] 2 [0-4] 24 [6-98] Absent N20 SSEP (10) After RW No Serious No low [41-50] 1 [0-3] 14 [6-32] Unreactive EEG (3) During TTM No No Serious low [54-72] 2 [1-7] 18 [5-61] Unreactive EEG (3) After RW no no No Low [53-70] 0 [0-3] 33 [7-163] Burstsuppression EEG (4) During TTM no Serious low [40-58] 3 [1-7] 11 [4-30] Burstsuppression EEG (1) After RW Serious no very low [8-34] 0 [0-5] 22 [1-379]
91 Evidence profile table Predictor (studies) Timing Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] EEG seizures, nonreactive During TTM No - low [16-49] 0 [0-10] 18 [1-293] EEG seizures After RW No - low [17-56] 0 [0-22] 9 [1-145] EEG seizures During TTM and RW No - Serious low [8-47] 0 [0-9] 17 [1-292] Status epilepticus During TTM no - no Low [4-27] 0 [0-22] 4 [0,2-60] Status epilepticus After RW no - low [14-79] 0 [0-13] 20 [1-334] Status epilepticus (2) 72h No low [18-32] 6 [1-20] 3 [0-23]
92 Evidence profile table CT Index Timing from ROSC Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] GWR BG <1.22 < 1 h Serious low [55-100] 0 [0-63] 7 [1-99] Average GWR <1.14 (BG/cerebrum) <1 h No low [4-31] 0 [0-13] 6 [0-113] GWR CN/PIC < h Serious No No Low [12-30] 0 [0-5] 24 [1-396] GWR P/CC < h Serious No No Low [41-64] 0 [0-5] 64 [4-1018] GWR CN/IC 1.18 < 1 h Serious No low [69-90] 8[0-38] 10 [1-64] Global cerebral oedema Median day 1 (1-7) Serious No Serious Low [13-40] 0 [0-5] 29 [2-479] BG = Basal ganglia; CC= Corpus callosum; CN = Caudate nucleus; PIC = Posterior limb of the internal capsule; P = Putamen
93 Evidence profile table MRI Index Timing from ROSC Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] Extensive cortical lesion pattern 80H (IQR ) No low [55-100] 9 [0-41] 10 [2-65] DWI changes in BG 80H (IQR ) No low [44-97] 9 [0-41] 9 [1-58] DWI changes in BS 80H (IQR ) No low [7-65] 0 [0-24] 8 [0-132] Changes in cortex + BG 74h (IQR 61-86) Serious Serious low [33-80] 0 [0-63] 5 [0-63] Changes in cortex + BG < 5 days No low [55-100] 0 [0-63] 7 [1-99] BG = Basal ganglia; BS = Brainstem
94 Evidence profile table MRI Index Timing from ROSC Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] ADC < mm 2 /sec in >10% of brain volume h Serious No low [46-95] 0 [0-28] 15 [1-227] Occipital cortex ADC < mm 2 /sec No low [75-98] 0 [0-24] 21 [1-324] Putamen ADC < mm 2 /sec 45.8 (IQR 36,8-52,4)) No low [60-91] 0 [0-24] 19 [1-281] Thalamus ADC < mm 2 /sec No low [44-79] 0 [0 24] 15 [1-228] ADC = Apparent Diffusion Coefficient
95 Biomarkers - Evidence profile Predictor, timing, studies Threshold (mcg L -1 ) Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] 4.97 no - very low [3-56] 4 [0-20] 5 [1-49] 25 no very very low [3-60] 0 [0-12] 13 [1-238] 33 Serious No S Serious low ] 5 [3-10] 9 [5-16] 44.3 no - low [64-97] 0 [0-34] 14 [1-209] NSE 48 h (13) 52.7 no - No Low [48-70] 0 [0-5] 73 [5-1157] 54.5 no low ]0-45] 0 [0-28] 12 [1-176] 58.3 Serious no low [10-35] ][ 4 [2-7] No low [0-45] 0 [0-14] 6 [0-129] 81.8 Serious No Np Moderate [13-25] 0 [0-2] 56 [3-909] Serious No Serious low [15-49] 0 [0-9] 21 [1-343] Serious No Serious low [13-35] 0 [0-7] 19 [1-343]
96 Biomarkers - Evidence profile Predictor, timing Threshold (mcg L -1 ) Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] 33 Serious No - low [53-90] 22 [6-48] 3 [1-8] NSE 72h (4) No - low [26-67] 0 [0-28] 9 [1-142] No - Serious low [58-90] 0 [0-9] 52 [3-813] 78.9 no Serious low [32-63] 0 [0-6] 52 [3-828]
97 Biomarkers - Evidence profile Predictor, timing, studies Threshold (mcg L -1 ) Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] 31.2 no - very very low [3-56] 4 [0-20] 5 [1-49] 41 Serious no - very very low [8-34] 4 [0-14] 4 [1-20] NSE 24 h (6) 49.6 no no very very very low [59-93] 0 [0-29] 15 [1-229] very low [0-45] 0 [0-14] 6 [0,3-129] 80.8 Serious no No Moderate [18-37] 0 0-4][ 33 [2-535] No low [6-24] 0 [0-7] 11 [1-191]

98 A 55-yr-old man presented with cardiac arrest spontaneous perfusion restored, and therapeutic hypothermia provided Death was pronounced and the family consented to organ donation 24 hrs after brain death, on arrival to the operating room for organ procurement, the patient was found to have regained corneal reflexes, cough reflex, and spontaneous respirations Webb and Samuels, CCM 2011.

99
100 The most likely outcome in adult outof-hospital cardiac arrest patients that survive to hospital discharge 1. Minimal disability 2. Moderate disability 3. Severe disability 4. Vegetative state
101 The most likely outcome in adult outof-hospital cardiac arrest patients that survive to hospital discharge 1. Minimal disability 2. Moderate disability 3. Severe disability 4. Vegetative state More than two thirds of patients will have minimal to no disability Kleinman ME et al, Part 5: Adult Basic Life Support and Cardiopulmonary Resuscitation Quality; Circulation. Nov 2015; 3;132(18 Suppl 2):S Aufderheide T et al. NEJM 2011;365:
102 Predicting good neurological outcome in adult cardiac arrest survivors that receive targeted temperature management Golan E, Scales DC, Morrison LM; 2015 (unpublished data)
103 Predicting good neurological outcome in adult cardiac arrest survivors that receive targeted temperature management 78% of patients that survived to hospital discharge experienced a very good neurological outcome as defined by a CPC 1 (431/550 patients) Golan E, Scales DC, Morrison LM; 2015 (unpublished data)


104 The majority (79%) of surviving patients who underwent TH after cardiac arrest in this series had preserved cognitive function and were able to return to work.
105 Diagnostic test Corneal reflex Pupillary reflex Motor score (M1 or M2) Clinical status myoclonus Unfavorable EEG Time post- ROSC, hours Patients tested, n Number of studies, n Sensitivity Specificity FPR Positive LR Simple proportions Continuity correction Simple proportions Continuity correction ( ) 0.98 ( ) 0.97 ( ) 0.02 ( ) 0.03 ( ) 8.4 ( ) > ( ) 1.00 ( ) 0.95 ( ) 0.00 ( ) 0.05 ( ) 4.3 ( ) ( ) 0.99 ( ) 0.98 ( ) 0.01 ( ) 0.02 ( ) 16.5 ( ) > ( ) 1.00 ( ) 0.96 ( ) 0.00 ( ) 0.04 ( ) 4.7 ( ) ( ) 0.90 ( ) 0.90( ) a 0.10 ( ) 0.10( ) a 6.8 ( ) > ( ) 0.96 ( ) 0.95 ( ) 0.04 ( ) 0.05 ( ) 9.5 ( ) ( ) 0.98 ( ) 0.95 ( ) 0.02 ( ) 0.05 ( ) 5.2 ( ) ( ) 0.96 ( ) 0.94 ( ) 0.04 ( ) 0.06 ( ) 8.7 ( ) > ( ) 1.00 ( ) 0.90 ( ) 0.00 ( ) 0.10 ( ) 7.3 ( ) SSEP ( ) 1.00 ( ) 0.98 ( ) 0.01 ( ) 0.02 ( ) 16.1 ( ) > ( ) 1.00 ( ) 0.94 ( ) 0.00 ( ) 0.06 ( ) 7.5 ( ) NSE > ( ) 0.89 ( ) 0.88 ( ) 0.11 ( ) 0.12 ( ) 4.1 ( ) Golan E et al, CCM 2014 Oct;42(10):
106 Evidence profile table Predictor (studies) Timing Risk of bias Indirectness Inconsistency Imprecision Quality of evidence TP FP FN TN Sensitivity [95%CI] FPR [95%CI] LR+ [95%CI] Flat During TTM Serious No - low [38-71] 46 [32-59] Flat or lowvoltage During TTM Serious No - low [19-64] 0 [0-11] Flat After RW Serious No - Serious low [6-31] 5 [1-15] BIS=0 During TTM no - low [31-69] 0 [0-16] 18 [1-284] Lowest mean BIS 5,5 During TTM no - low [69-95] 17 [7-32] 5 [3-10] Lowest BIS=0 During TTM No - low [59-89] 10 [3-23] 8 [3-30]

107 Precision of the diagnostic tests Golan E et al, CCM 2014 Oct;42(10):
108 What about real life data? Consecutive OHCA patients that received TTM and survived to 72hrs postarrest Multicentre (n=34 hospitals) in Southwestern Ontario from N= 982 Golan E et al, Data not yet pubilshed
109 Results Neuroprognostic tests Bilaterally absent corneal reflex at 48 to 72 hours Bilaterally absent pupillary reflex at 48 to 72 hours Bilateral Glasgow coma motor score of 1-2 at 48 to 72 hours Unadjusted OR (95%CI) ( ) ( ) ( ) Unadjusted OR (95%CI) Adjusted OR (95%CI) < ( ) < ( ) < ( ) Adjusted OR (95%CI) <0.001 <0.001 Clinical diagnostic test False positive rate (percentage; 95% CI) Bilaterally absent corneal reflex at 48 to 72 hours 5.1 ( ) Bilaterally absent pupillary reflex at 48 to 72 hours 4.5 ( ) Bilateral Glasgow coma motor score of 1-2 at 48 to ( ) hours Golan E et al, Data not yet pubilshed

110 Do we stop too early?
111




112 The PremaTOR Study (Preventing Premature Termination Of Resuscitation) University of Toronto
ALS 713: Prognostication in Normothermia
 ALS 713: Prognostication in Normothermia TFQO: Clifton Callaway (COI #214) EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35) Taskforce: ALS COI Disclosure (specific to this systematic review)
ALS 713: Prognostication in Normothermia TFQO: Clifton Callaway (COI #214) EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35) Taskforce: ALS COI Disclosure (specific to this systematic review)
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-resuscitation care for adults. Jerry Nolan Royal United Hospital Bath
 Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center
 Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Neuroprognostication after cardiac arrest
 Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
State of the art lecture: 21st Century Post resuscitation management
 State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN (865) LABEL
 LABEL") 1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
Disclosures. Pediatrician Financial: none Volunteer :
 Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto
 New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto COI Declaration Industry and ROC ALS Taskforce ILCOR Author
New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto COI Declaration Industry and ROC ALS Taskforce ILCOR Author
Case: 65 year old post-cardiac arrest patient with myoclonus
 Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Neurological prognostication after cardiac arrest and targeted temperature management
 Neurological prognostication after cardiac arrest and targeted temperature management Dragancea, Irina Published: 2016-01-01 Document Version Publisher's PDF, also known as Version of record Link to publication
Neurological prognostication after cardiac arrest and targeted temperature management Dragancea, Irina Published: 2016-01-01 Document Version Publisher's PDF, also known as Version of record Link to publication
Cardio Pulmonary Cerebral Resuscitation
 Cardio Pulmonary Cerebral Resuscitation Brain Under Pressure October 3, 2017 Canadian Critical Care Forum Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto
Cardio Pulmonary Cerebral Resuscitation Brain Under Pressure October 3, 2017 Canadian Critical Care Forum Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto
Predicting neurological outcome and survival after cardiac arrest
 Predicting neurological outcome and survival after cardiac arrest Andy Temple MB ChB FRCA FFICM Richard Porter MB ChB FRCA Matrix reference 2C01, 2C04 Key points Accurately predicting neurological outcome
Predicting neurological outcome and survival after cardiac arrest Andy Temple MB ChB FRCA FFICM Richard Porter MB ChB FRCA Matrix reference 2C01, 2C04 Key points Accurately predicting neurological outcome
Post-anoxic status epilepticus and EEG patterns
 Post-anoxic status epilepticus and EEG patterns Nicolas Gaspard, MD, PhD Université Libre de Bruxelles Hôpital Erasme, Bruxelles, Belgique Yale University School of Medicine, New Haven, CT, USA DISCLOSURES
Post-anoxic status epilepticus and EEG patterns Nicolas Gaspard, MD, PhD Université Libre de Bruxelles Hôpital Erasme, Bruxelles, Belgique Yale University School of Medicine, New Haven, CT, USA DISCLOSURES
Therapeutic Hypothermia: 2011 Research Update. Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine
 Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre
 Claudio Sandroni, Giuseppe La Torre") Worksheet No. ALS-PA-041.doc Page 1 of 16 WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre Date Submitted for review: 27
Worksheet No. ALS-PA-041.doc Page 1 of 16 WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre Date Submitted for review: 27
Hypothermia: The Science and Recommendations (In-hospital and Out)
") Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Predicting Outcomes in HIE. Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016
 Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Do Prognostic Models Matter in Neurocritical Care?
 Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Do Prognostic Models Matter in Neurocritical Care? Alexis F. Turgeon MD MSc FRCPC Associate Professor and Director of Research Department of Anesthesiology and Critical Care Medicine Division of Critical
Author Manuscript Faculty of Biology and Medicine Publication
 Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
 Emergency Medicine Australasia (2011) 23, 292 296 doi: 10.1111/j.1742-6723.2011.01422_15.x POST-RESUSCITATION THERAPY Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
Emergency Medicine Australasia (2011) 23, 292 296 doi: 10.1111/j.1742-6723.2011.01422_15.x POST-RESUSCITATION THERAPY Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
Enhancing 5 th Chain TTM after Cardiac Arrest
 Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest
 Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care
 Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Controversies in Post Resuscitation After Cardiac Arrest
 Controversies in Post Resuscitation After Cardiac Arrest More News About Gainesville FL.. 124,354 souls 2007 Best place to live and play in USA 2009 UF ranked #1 party school Andrea Gabrielli, MD FCCM
Controversies in Post Resuscitation After Cardiac Arrest More News About Gainesville FL.. 124,354 souls 2007 Best place to live and play in USA 2009 UF ranked #1 party school Andrea Gabrielli, MD FCCM
In the past decade, two large randomized
 Mild therapeutic hypothermia improves outcomes compared with normothermia in cardiac-arrest patients a retrospective chart review* David Hörburger, MD; Christoph Testori, MD; Fritz Sterz, MD; Harald Herkner,
Mild therapeutic hypothermia improves outcomes compared with normothermia in cardiac-arrest patients a retrospective chart review* David Hörburger, MD; Christoph Testori, MD; Fritz Sterz, MD; Harald Herkner,
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Neurologic Recovery and Prognostication
 Neurologic Recovery and Prognostication Sudden Cardiac Arrest Association Jon Rittenberger, MD, MS October 8, 2010 Disclosures Employer: University of Pittsburgh/ UPMC Grants: - National Association of
Neurologic Recovery and Prognostication Sudden Cardiac Arrest Association Jon Rittenberger, MD, MS October 8, 2010 Disclosures Employer: University of Pittsburgh/ UPMC Grants: - National Association of
Curricullum Vitae. Dr. Isman Firdaus, SpJP (K), FIHA
, FIHA") Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
Author Manuscript Faculty of Biology and Medicine Publication
 Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Targeted temperature management after post-anoxic brain insult: where do we stand?
 Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
IN HOSPITAL CARDIAC ARREST AND SEPSIS
 IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
DECLARATION OF CONFLICT OF INTEREST. Research grants: Sanofi-Aventis
 DECLARATION OF CONFLICT OF INTEREST Research grants: Sanofi-Aventis Invasive management after cardiac arrest Nikolaos I Nikolaou FESC, FERC Athens, Greece Survival (%) Survival from Out of Hospital Cardiac
DECLARATION OF CONFLICT OF INTEREST Research grants: Sanofi-Aventis Invasive management after cardiac arrest Nikolaos I Nikolaou FESC, FERC Athens, Greece Survival (%) Survival from Out of Hospital Cardiac
How to Improve Cardiac Arrest Survival in your Center
 How to Improve Cardiac Arrest Survival in your Center Ankur A. Doshi, MD FACEP Post Cardiac Arrest Service UPMC Presbyterian Department of Emergency Medicine University of Pittsburgh School of Medicine
How to Improve Cardiac Arrest Survival in your Center Ankur A. Doshi, MD FACEP Post Cardiac Arrest Service UPMC Presbyterian Department of Emergency Medicine University of Pittsburgh School of Medicine
Post-resuscitation Care
 Post-resuscitation Care Kyu-Nam Park Department of Emergency Medicine. St. Mary s Hospital. Catholic University of Korea Dr.James R Jude, Dr. William Kouwenhoven, Dr.G Guy Knickerbocker at Johns Hopkins
Post-resuscitation Care Kyu-Nam Park Department of Emergency Medicine. St. Mary s Hospital. Catholic University of Korea Dr.James R Jude, Dr. William Kouwenhoven, Dr.G Guy Knickerbocker at Johns Hopkins
Patient Case. Post cardiac arrest pathophysiology 10/19/2017. Disclosure. Objectives. Patient Case-TM
 Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Advanced airway placement (ETT vs SGA)
") Advanced airway placement (ETT vs SGA) Among adults who are in cardiac arrest in any setting (P), does tracheal tube insertion as first advanced airway (I), compared with insertion of a supraglottic airway
Advanced airway placement (ETT vs SGA) Among adults who are in cardiac arrest in any setting (P), does tracheal tube insertion as first advanced airway (I), compared with insertion of a supraglottic airway
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest
 ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
The 2010 evidence-based guidelines: the process, the challenges
 The 2010 evidence-based guidelines: the process, the challenges Jerry Nolan Co-Chair, ILCOR Royal United Hospital Bath, UK European Society of Cardiology Stockholm 30 Aug 2010 The 2010 guidelines: the
The 2010 evidence-based guidelines: the process, the challenges Jerry Nolan Co-Chair, ILCOR Royal United Hospital Bath, UK European Society of Cardiology Stockholm 30 Aug 2010 The 2010 guidelines: the
Post Cardiac Arrest Care. From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
 Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti
 Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti U.O.C Anestesia e Terapia Intensiva Policlinico San Martino - GENOVA Natural Course of Neurological Recovery Following Cardiac Arrest Cardiac
Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti U.O.C Anestesia e Terapia Intensiva Policlinico San Martino - GENOVA Natural Course of Neurological Recovery Following Cardiac Arrest Cardiac
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
Myoclonic status epilepticus in hypoxic ischemic encephalopathy which recurred after somatosensory evoked potential testing
 ANNALS OF CLINICAL NEUROPHYSIOLOGY CASE REPORT Ann Clin Neurophysiol 2017;19(2):136-140 Myoclonic status epilepticus in hypoxic ischemic encephalopathy which recurred after somatosensory evoked potential
ANNALS OF CLINICAL NEUROPHYSIOLOGY CASE REPORT Ann Clin Neurophysiol 2017;19(2):136-140 Myoclonic status epilepticus in hypoxic ischemic encephalopathy which recurred after somatosensory evoked potential
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
The Role of EEG After Cardiac Arrest and Hypothermia
 Current Literature In Clinical Science The Role of EEG After Cardiac Arrest and Hypothermia Continuous EEG in Therapeutic Hypothermia After Cardiac Arrest: Prognostic and Clinical Value. Crepeau AZ, Rabinstein
Current Literature In Clinical Science The Role of EEG After Cardiac Arrest and Hypothermia Continuous EEG in Therapeutic Hypothermia After Cardiac Arrest: Prognostic and Clinical Value. Crepeau AZ, Rabinstein
TCD and cardiac arrest
 TCD and cardiac arrest Background: An effective tissue perfusion has decisive influence on the final prognosis both during cardiopulmonary resuscitation (CPR) and after recovery of spontaneous circulation
TCD and cardiac arrest Background: An effective tissue perfusion has decisive influence on the final prognosis both during cardiopulmonary resuscitation (CPR) and after recovery of spontaneous circulation
Developments in Cardiopulmonary Resuscitation Guidelines
 Developments in Cardiopulmonary Resuscitation Guidelines Bernd W. Böttiger Seite 1 To preserve human life by making high quality resuscitation available to all Outcome after CPR in Germany ROSC ( Return
Developments in Cardiopulmonary Resuscitation Guidelines Bernd W. Böttiger Seite 1 To preserve human life by making high quality resuscitation available to all Outcome after CPR in Germany ROSC ( Return
Kiehl EL, 1,2 Parker AM, 1 Matar RM, 2 Gottbrecht M, 1 Johansen MC, 1 Adams MP, 1 Griffiths LA, 2 Bidwell KL, 1 Menon V, 2 Enfield KB, 1 Gimple LW 1
 C-GRApH: A Validated Scoring System For The Early Risk Stratification Of Neurologic Outcomes After Out-of-hospital Cardiac Arrest Treated With Therapeutic Hypothermia Kiehl EL, 1,2 Parker AM, 1 Matar RM,
C-GRApH: A Validated Scoring System For The Early Risk Stratification Of Neurologic Outcomes After Out-of-hospital Cardiac Arrest Treated With Therapeutic Hypothermia Kiehl EL, 1,2 Parker AM, 1 Matar RM,
Author Manuscript Faculty of Biology and Medicine Publication
 Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Objectives. Trends in Resuscitation POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE?
 POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
The Theraputic Role of Hypothermia
 The Theraputic Role of Hypothermia Sharie Bennett R.EEG/EP T 10/2/2014 1 Hypothermia Objectives: Therapeutic benefits of Hypothermia The role of Neurodiagnostics in Hypothermia Monitoring 10/2/2014 2 Hypothermia
The Theraputic Role of Hypothermia Sharie Bennett R.EEG/EP T 10/2/2014 1 Hypothermia Objectives: Therapeutic benefits of Hypothermia The role of Neurodiagnostics in Hypothermia Monitoring 10/2/2014 2 Hypothermia
Hypothermia After Cardiac Arrest: Where Are We Now?
 Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
The Evidence Base. Stephan A. Mayer, MD. Columbia University New York, NY
 Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Therapeutic Hypothermia after Resuscitated Cardiac Arrest
 Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Subhairline EEG Part II - Encephalopathy
 Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results of Cerebral Perfusion MR Imaging
 pissn 2384-1095 eissn 2384-1109 imri 2018;22:56-60 https://doi.org/10.13104/imri.2018.22.1.56 Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results
pissn 2384-1095 eissn 2384-1109 imri 2018;22:56-60 https://doi.org/10.13104/imri.2018.22.1.56 Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Scope. EEG patterns in Encephalopathy. Diffuse encephalopathy. EEG in adult patients with. EEG in diffuse encephalopathy
 Scope EEG patterns in Encephalopathy Dr.Pasiri Sithinamsuwan Division of Neurology Department of Medicine Phramongkutklao Hospital Diffuse encephalopathy EEG in specific encephalopathies Encephalitides
Scope EEG patterns in Encephalopathy Dr.Pasiri Sithinamsuwan Division of Neurology Department of Medicine Phramongkutklao Hospital Diffuse encephalopathy EEG in specific encephalopathies Encephalitides
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Experiences as a Donation Support Physician. Dead or not Dead? Are the following statements consistent with neurological
 Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
What Hospitalists Need to Know about ICU Neurology
 What Hospitalists Need to Know about ICU Neurology S. Andrew Josephson, MD Department of Neurology, Neurovascular Service University of California San Francisco September 25, 2009 The speaker has no disclosures
What Hospitalists Need to Know about ICU Neurology S. Andrew Josephson, MD Department of Neurology, Neurovascular Service University of California San Francisco September 25, 2009 The speaker has no disclosures
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Early Diffusion MR Imaging Findings and Short-Term Outcome in Comatose Patients with Hypoglycemia
 ORIGINAL RESEARCH K. Johkura Y. Nakae Y. Kudo T.N. Yoshida Y. Kuroiwa Early Diffusion MR Imaging Findings and Short-Term Outcome in Comatose Patients with Hypoglycemia BACKGROUND AND PURPOSE: The relationship
ORIGINAL RESEARCH K. Johkura Y. Nakae Y. Kudo T.N. Yoshida Y. Kuroiwa Early Diffusion MR Imaging Findings and Short-Term Outcome in Comatose Patients with Hypoglycemia BACKGROUND AND PURPOSE: The relationship
Brain Death Determination: Outline. Definition. Brain Death Determination. Brain Death Determination. No conflict of interest
 No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
Case Presentation. Cooling. Case Presentation. New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation
 New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital
 Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
Post-Resuscitation Care. Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena
 Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Resuscitation Guidelines update. Dr. Luis García-Castrillo Riesgo EuSEM Vice president
 Resuscitation Guidelines update Dr. Luis García-Castrillo Riesgo EuSEM Vice president There are no COIs to disclose in this presentation. CPR Mile Stones 1958 -William Kouwenhoven, cardiac massage. 1967
Resuscitation Guidelines update Dr. Luis García-Castrillo Riesgo EuSEM Vice president There are no COIs to disclose in this presentation. CPR Mile Stones 1958 -William Kouwenhoven, cardiac massage. 1967
Prognostication in hypothermia
 Prognostication in hypothermia PICO Among adults with ROSC who are treated with hypothermia, (P), does any clinical variable when normal (e.g. 1. Clinical Exam, 2. EEG, 3. SSEP, 4. Imaging, 5. Other) when
Prognostication in hypothermia PICO Among adults with ROSC who are treated with hypothermia, (P), does any clinical variable when normal (e.g. 1. Clinical Exam, 2. EEG, 3. SSEP, 4. Imaging, 5. Other) when
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Author Manuscript Faculty of Biology and Medicine Publication
 Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Queen Charlotte Hospital
 Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Post Cardiac Arrest Management
 Post Cardiac Arrest Management Romergryko G. Geocadin, MD Neurosciences Critical Care Division Professor Departments of Neurology, Anesthesiology-Critical Care, Neurosurgery and Medicine Baltimore, MD
Post Cardiac Arrest Management Romergryko G. Geocadin, MD Neurosciences Critical Care Division Professor Departments of Neurology, Anesthesiology-Critical Care, Neurosurgery and Medicine Baltimore, MD
The Determination of Brain Death. James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY
 The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
The Determination of Brain Death James Zisfein, M.D. Chief, Division of Neurology Lincoln Medical Center, Bronx, NY James.Zisfein@nychhc.org The early history of brain death Until recently, death was determined
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol
 Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
한국학술정보. Key Words: Seizures, Prognosis, Out-of-hospital Cardiac Arrest
 Relevance of Seizure with Mortality and Neurologic Prognosis of Out of Hospital Cardiopulmonary Arrest (OHCA) Patients Who had Treated with Therapeutic Hypothermia after Return of Spontaneous Circulation
Relevance of Seizure with Mortality and Neurologic Prognosis of Out of Hospital Cardiopulmonary Arrest (OHCA) Patients Who had Treated with Therapeutic Hypothermia after Return of Spontaneous Circulation
Resuscitation Science : Advancing Care for the Sickest Patients
 Resuscitation Science : Advancing Care for the Sickest Patients William Hallinan University of Rochester What is resuscitation science? Simply the science of resuscitation : Pre arrest Arrest care Medical
Resuscitation Science : Advancing Care for the Sickest Patients William Hallinan University of Rochester What is resuscitation science? Simply the science of resuscitation : Pre arrest Arrest care Medical
EXTRACORPOREAL LIFE SUPPORT FOR PROLONGED CARDIAC ARREST
 EXTRACORPOREAL LIFE SUPPORT FOR PROLONGED CARDIAC ARREST Massimo MASSETTI Cardiac Surgery Department University of Sacred Heart, Gemelli Hospital Rome «No financial interest to declare» ESC CONGRESS 2012
EXTRACORPOREAL LIFE SUPPORT FOR PROLONGED CARDIAC ARREST Massimo MASSETTI Cardiac Surgery Department University of Sacred Heart, Gemelli Hospital Rome «No financial interest to declare» ESC CONGRESS 2012
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Out-of-hospital Cardiac Arrest. Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland
 Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
Out-of-hospital Cardiac Arrest Franz R. Eberli MD, FESC, FAHA Cardiology Triemli Hospital Zurich, Switzerland Conflict of Interest I have no conflict of interest to disclose regarding this presentation.
ECPR: An emerging strategy for cardiac arrest
 ECPR: An emerging strategy for cardiac arrest Steven Brooks MD MHSc FRCPC Associate Professor Department of Emergency Medicine, Queen s University November 2016 Conventional CPR is ineffective Conventional
ECPR: An emerging strategy for cardiac arrest Steven Brooks MD MHSc FRCPC Associate Professor Department of Emergency Medicine, Queen s University November 2016 Conventional CPR is ineffective Conventional
The prognostic value of gray-white-matter ratio in cardiac arrest patients treated with hypothermia
 Scheel et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2013, 21:23 ORIGINAL RESEARCH Open Access The prognostic value of gray-white-matter ratio in cardiac arrest patients treated
Scheel et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2013, 21:23 ORIGINAL RESEARCH Open Access The prognostic value of gray-white-matter ratio in cardiac arrest patients treated
Rationale for developing devastating brain injury pathways
 Rationale for developing devastating brain injury pathways Alex Manara Neuro ICU Southmead Hospital North Bristol NHS Trust Regional Clinical Lead in Organ Donation RCEM 2018 RCEM 2018 The Bristol Model
Rationale for developing devastating brain injury pathways Alex Manara Neuro ICU Southmead Hospital North Bristol NHS Trust Regional Clinical Lead in Organ Donation RCEM 2018 RCEM 2018 The Bristol Model
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
The 2015 BLS & ACLS Guideline Updates What Does the Future Hold?
 The 2015 BLS & ACLS Guideline Updates What Does the Future Hold? Greater Kansas City Chapter Of AACN 2016 Visions Critical Care Conference Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Independent CNS/Staff
The 2015 BLS & ACLS Guideline Updates What Does the Future Hold? Greater Kansas City Chapter Of AACN 2016 Visions Critical Care Conference Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Independent CNS/Staff
Serum neutrophil gelatinase-associated lipocalin levels predict the neurological outcomes of out-of-hospital cardiac arrest victims
 Kaneko et al. BMC Cardiovascular Disorders (2017) 17:111 DOI 10.1186/s12872-017-0545-y RESEARCH ARTICLE Open Access Serum neutrophil gelatinase-associated lipocalin levels predict the neurological outcomes
Kaneko et al. BMC Cardiovascular Disorders (2017) 17:111 DOI 10.1186/s12872-017-0545-y RESEARCH ARTICLE Open Access Serum neutrophil gelatinase-associated lipocalin levels predict the neurological outcomes
Regionalization of Post-Cardiac Arrest Care
 Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Any man s death diminishes me, because I am involved in mankind. - John Donne
 Any man s death diminishes me, because I am involved in mankind - John Donne Cardiac Arrest in 2011 Where are we? Or where should we be? Michael W. Dailey, MD FACEP Associate Professor of Emergency Medicine
Any man s death diminishes me, because I am involved in mankind - John Donne Cardiac Arrest in 2011 Where are we? Or where should we be? Michael W. Dailey, MD FACEP Associate Professor of Emergency Medicine
Declaring Brain Death. Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery
 Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Declaring Brain Death Ali Salim, MD Professor of Surgery Chief, Division of Trauma, Burns, Surgical Critical Care, and Emergency General Surgery Disclosures I have nothing to disclose Why should we know
Electroencephalography. Role of EEG in NCSE. Continuous EEG in ICU 25/05/59. EEG pattern in status epilepticus
 EEG: ICU monitoring & 2 interesting cases Electroencephalography Techniques Paper EEG digital video electroencephalography Dr. Pasiri Sithinamsuwan PMK Hospital Routine EEG long term monitoring Continuous
EEG: ICU monitoring & 2 interesting cases Electroencephalography Techniques Paper EEG digital video electroencephalography Dr. Pasiri Sithinamsuwan PMK Hospital Routine EEG long term monitoring Continuous
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Comparison of outcome of etiological factors for non-traumatic coma in geriatric population in India
 Original article: Comparison of outcome of etiological factors for non-traumatic coma in geriatric population in India 1 DrAmit Suresh Bhate, 2 DrSatishNirhale, 3 DrPrajwalRao, 4 DrShubangi A Kanitkar
Original article: Comparison of outcome of etiological factors for non-traumatic coma in geriatric population in India 1 DrAmit Suresh Bhate, 2 DrSatishNirhale, 3 DrPrajwalRao, 4 DrShubangi A Kanitkar
Cardiac Arrest January 2017 CPR /3/ Day to Survival Propensity Matched
 Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that