Post-resuscitation Care
|
|
|
- Colin Horn
- 5 years ago
- Views:
Transcription
1 Post-resuscitation Care Kyu-Nam Park Department of Emergency Medicine. St. Mary s Hospital. Catholic University of Korea


2 Dr.James R Jude, Dr. William Kouwenhoven, Dr.G Guy Knickerbocker at Johns Hopkins Hospital, 1961




3 소방 119 구급대 대한응급의학회 대한순환기학회 대한심폐소생협회 BLS, ACLS Courses
 Good outcome:13 %(6 M) By BRCT")
4 Postresuscitation Coma ROSC : 25-50% of Attempted CPR 80% of ROSC pts : initially Coma Survival rate:18 % (6 M) Good outcome:13 %(6 M) By BRCT II
5 I/R Injury mechanism Treatment Outcome evaluation
6 Reperfusion injury Fever Hypotension Hypoxia Seizure Glucose(hypo, Hyper) Acid-base Electrolytes Most neurons tolerate up to ~15 min of normothermic ischemia in vivo
7 -Key Points - Identify and treat precipitating causes of the arrest (6H s and 5T s factors) Support care (Critical Care) V/S, electrolyte, acid-base, seizure, glucose etc, at least 24hrs Therapeutic Hypothermia Outcome evaluation SEP, N/Ex
8 M/34 고 O 주 C A S E 1 Near drowning, Arrest T:25min, Asystole, initial BT: 28 C CPR T:15min, bystander CPR(-), 119 no CPR Brain stem reflex( CR: 6hr) 1D:GCS=3 3D:GCS=5 12D:GCS=15, Posthypoxic Myoclonus(Lance Adams) SEP,MRS,Echo=O.K
9 MRS : lactate(-) at 1.3ppm, At 2D after ROSC SSEP : N20 (+), At 30hrs after ROSC

10 의식회복후상태 Lance-Adams syndrome(posthypoxic myoclonus)
11 Temperature Regulation
12 Hyperthermia 40 pts,prs (Resuscitation 2001;49:273) Peak axillary Temp. Above 39 C within initial 72hrs all 20pts : dead( vs 3 of 20 pts, less than 39 C ) Either frequent use of antipyretics or controlled normothermia with cooling techniques Monitor the patient s temperature after resuscitation and avoid hyperthermia
. With non-vf arrest out of hospital or for in-hospital arrest (Class IIb).")
13 Induced Hypothermia Unconscious adult patients with ROSC after OHCA should be cooled to 32 C to 34 C for 12 to 24 hours when the initial rhythm was VF (Class IIa). With non-vf arrest out of hospital or for in-hospital arrest (Class IIb). Bernard SA, NEJM 2002; 346: HACA Study Group, NEJM 2002; 346:549-56
14 Australian Study (Bernard SA) Good outcome Hypo- vs Normothermia (21/43 vs 9/34, 49% vs 26%, p=0.046). Mortality rate Hypo- vs Normothermia (22/43 vs 23/34, 51% vs 68%, p=0.145) Primary causes of death -Cardiac failure -Brain death -Severe neurologic injury -Withdrawal of all active therapy
15 European Study( HACA Study Group)





16 Resuscitative hypothermia, ST.Mary s Hosp
17 Results (1) Patient Age Arrest ACLS Initial Causes of Underlying CPC (n=12) (yr) Time(min Time(min Rhythm cardiac arrest Disease PEA R (Drug overdose) Depression Asystole R (Drug overdose) Depression VF C (AMI) Asystole R (Unknown) HBP PEA R (Hanging) Depression Asystole C (Dysrhythmia) VF C (AMI) HBP,DM Asystole C (CHF) HBP,DM Asystole C (dysrhythmia) Asystole R (Asphyxia) HBP Asystole R (Asphyxia) DM,CAD Asystole C (AMI) CAD 5 SUM VF (n=2) C (cardiac,n=6) Good AVR ± S.D 48 ±17 20 ± ± 8 PEA (n=2) Asystole (n=8) R (respiratory,n=6) (n=4) Poor (n=8) 2002, ACEP, oral presentation, Seatle, WA
 36.2±0.3(36-36.7) 36.6±0.6 (35.8-37.")
18 Results (2) Resuscitative Outcome Hypothermia All Patients (n=12) Good (n=4) Poor (n=8) Initiation Temperature ( ) 36.5±0.5( ) 36.2±0.3( ) 36.6±0.6 ( ) Initiation Time (min) 129±113 (40-420) 188±159 (60-750) 99±78 (40-250) Induction Time (min) 160±79 (80-330) 171±107 ( ) Rewarming Time (min) 605±190 ( ) 603±284 ( ) Induction Rewarming 154±69 (80-300) 606±106 ( ) Maintenance

19 European Study
 Ref.: Vanden hoek,tl,md. CCM.")
 CoolGard")
20 Internal cooling techniques (cold saline techniques) Ref.: Vanden hoek,tl,md. CCM. volume 32(9) supplement Sep 2004;pps425 (Endovascular cooling catheter) CoolGard 3000; Alsius


21 J Neurosurg 100:272, 2004
22 Regulated hypothermia
23 Forced hypothermia Regulated hypothermia Physiological responses to maintain normothermia - Vigorous heat gain and conserving response (thermoregulatory system) - Blunt or delay achieving the hypothermic therapeutic target temp. - Create undue physiological and psychological stress ( shivering, increased catecholamine & cortisol) Reduced body temp via a reduction in the set-point of thermoregulation - The theoretical advantage of mild hypothermia more quickly - Less stress ( shivering, increased catecholamine & cortisol) - Reduce the benefits of the hypothermic therapy.

24 Hibernation in Animals



25 Bats normal heart beat : 400 /min during hibernation : /min saves 99.3 % of their energy. Bears survive six months without eating, drinking, urinating or defecating The largest and most dramatic hibernators during hibernation their body temperature does not drop despite slowing their breathing and heart rates. so bears put on large fat reserves
26 Hibernation induction trigger, an 88 kd peptide : -in the serum of hibernating groud squirrels -increase survival time in a multiorgan preparation model with dogs (J thorac Cadiovascular Surg 1991; 102:224) D-Ala2, D-Leu5-enkephalin (DADLE) : extends hypothermic preservation time of the lung (J thorac Cadiovascular Surg 1996; 111:259) Neurotensin 77 : induce hibernation for several hrs in rats (CCM 2004;32:806) H 2 S : reversible hibernation in mice by the way of inhibition oxidative phosphorylation (Science 2005;308:518)
27 Neurotensin An endogeneous tridecapeptide Elevation during hibernation (Comp biochem physiol C 1983) Induces hypothermia by activation of neurotensin receptors in the brain Normally degraded rapidly by circulating peptidases found in the blood
28 Figure 1. Brain temperature was measured telemetrically and recorded during surgical preparation and for 24 hrs after reperfusion from asphyxial cardiac arrest Neurotensin-induced hypothermia improves neurologic outcome after hypoxic-ischemia Critical Care Medicine. 32(3): , March 2004
29 Figure 3. Performance (latency time) in the Morris maze days after reperfusion from asphyxial cardiac arrest in rats Neurotensin-induced hypothermia improves neurologic outcome after hypoxic-ischemia Critical Care Medicine. 32(3): , March 2004
30 Support - Cardiovascular System Transient myocardial stunning& dysfunction - lasts 48-72hrs, high level of cathecholamine - low cardiac output, followed vasodilation Tx.: Fluid, vasoactive, inotropics, inodilator (JACC 2002;40:2110) Hemodynamic instability: Echo & cardiac evaluation within the first 24 hrs after arrest Early corticosteroid supplementation (adrenal insufficiency)? Prophylactic of antiarrhythmics: insufficiency of evidence Continue infusion of antiarrhythmics associated with ROSC (Class Indeterminate) β-blocker with ischemic heart disease if there are no CIx.
31 Support - Ventilatory Parameters Hyperventilation hypocapnea (PCO2 ) cbr. vasoconstriction CBF cerebral ischemia and ischemic injury Hyperventilation 기도압 auto PEEP CVP & ICP CBF cerebral ischemic injury Routine hyperventilation is detrimental (Class III)
32
33 Support - CNS Optimize cerebral perfusion pressure Treat hyperthermia + therapeutic hypothermia Seizures control by anticonvulsant therapy initiated (Class IIa) Routine seizure prophylaxis (Class Indeterminate)
34 Thrombolytic agents during CPR 90 OHCA, Heparin & rt-pa (Lancet 2001;357:1583) A prospective pilot intervention trial in pts undergoing CPR ROSC ( 68% vs 48%) Alive at 24 hrs after CA (35% vs 25%) Hospital discharge ( 15% vs 8%) No bleeding complication 108 pts, rt-pa (Resuscitation 2001;50:71) A retrospective case control study Large European multicenter trial (TROICA trial)-large scale, randomized, controlled clinical trial, over 1000 pts, over 40 centers Intravascular fibrin formation & microthrombosis; distributed throughout the entire microcirculation after CA
35 Outcome Prediction of Postresuscitation Coma







36 Happy Faces ^^* Unhappy Faces ^^* CPC 3 CPC 4 CPC 5 CPC 1, 2
37 Aggressive early management? Withdrawal of Critical Care Support? COMA
38 가장효과적인 예후예측인자는???


39 St.Mary s Hosp Case 96.05
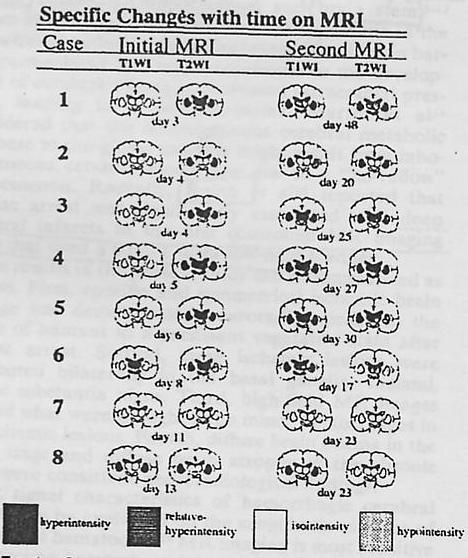
40 Stroke 1994:25; 박 0 0 MRI findings


41 St.Mary s Hosp Case : 박
42 1. Neurologic examination 2. Electrophysiologic Studies (SEP,EEG) 3. Imaging ( CT, MRI, MRS, Diffusion Imaging) 4. Biochemical markers (NSE, S-100, CK-BB) 5. Inflammatory markers ( IL-6, IL-8 ) 6. Combination of predictive markers
43 1. Neurologic Examination
44 Is This Patient Dead, Vegetative, or Severely Neurologically Impaired? Assessing Outcome for Comatose Survivors of Cardiac Arrest 1914pts (11 studies) Booth, et. Al. JAMA,, 2004

45 Booth, et. Al. JAMA, 2004

46 Booth, et. Al. JAMA, 2004
47 2005. AHA. Recommendation Predictors of poor neurologic outcome (1) absent corneal reflex at 24 hrs (2) absent pupillary response at 24 hrs (3) absent withdrawal to pain at 24 hrs (4) no motor response at 24 hrs (5) no motor response at 72 hrs
48 Advantage and Limitation of Advantage - Universal availability - Ease of performance - First line of information Neurologic Exam Limitation - Many resuscitated pts : still under analgesia and sedation : thus not fully assessable by neurologic exam - Not objective - Relative wide C.I
49 2. Electrophysiologic Studies (SEP)
50 Somatosensory Evoked Potential (SEP) Electrode 1) Erb point(n9 peak) 2) 7 th cervical level(c7 : N13 peak) 3) Sensory Cortical level (C3, C5 : N20 peak)


51 Somatosensory Evoked Potential
52 Review of the use somatosensory evoked potentials in the prediction of outcome after severe brain injury Bradley G. et al., Crit Care Med Vol.29,No pts, reviewed 44 studies Bradley G, Crit Care Med, 2001
53 PLR (95% C.I) PPV Sensitive Normal SEP (favorable outcome) 4.04( ) 71.2% (394/553) 59% (394/668) Bilat. Abs SEP (unfavorable outcome) 11.41( ) 98.5% (765/777) 46.2% (765/1657) PLR : Positive liklihood ratio, PPV : Positive predictive value, SEP : Somatosensery evoked potential 95% C.I (Confidence Interval) Bradley G, Crit Care Med, 2001
54 Bradley G, Crit Care Med, 2001
55 Bradley G, Crit Care Med, 2001
56 The time dependency of SSEPs in comatose CA survivors. 25 pts - Within 24hr after ROSC there was a significant improvement in SEP Therefore we recommend allowing a period of at least 24hr after ROSC Gendo A, Vienna, Austria, Intensive Care Med, 2001
57 2005. AHA. Recommendation Prediction of poor neurologic outcome Bilateral median nerve SEP (N20) at least 72 hrs with hypoxic-anoxic coma
58 Proton Magnetic Resonance Spectroscopy(MRS)









")
59 Figure.1 Case 5, Spectra from PO region at 48 hours after ROSC showed no evidence of any lactate signal. He recovered consciousness at 12 days after ROSC and has shown mild memory impairment. Figure.2 Case 9, Spectra from PO region at 72 hours after ROSC showed elevated lactate peak at 1.3 ppm. He presented with persistent vegetative state. 27 pts, Lac(+) Sensitivity : 78.9%, Specificity : 100% LR(+) : 13.9, LR(-) : 0.2 St. Mary Hosp., Ann Emerg Med 2001:38(4); S39
60 Summery of MRS Advantage Greater advantage than clinical evaluation Not influenced by sedating drugs or other medical treatment Objective parameter Limitation Expensive Availability Need intensive care monitoring during test
61 CPC(1-2) CPC(1-2) CPC(3-5) CPC(3-5) CPC(1-2) CPC(1-2) CPC(3-5) CPC(3-5) pg/ml pg/ml pg/ml pg/ml m 4h 24h 48h 20m 4h 24h 48h time time 20m 4h 24h 48h 20m 4h 24h 48h time time Figure1. The comparison of the time course between the course between the CPC(1-2) and CPC(3-5)in CSF IL-1 concentration Figure2. The comparison of the time course between the course between the CPC(1-2) and CPC(3-5)in CSF IL-6 concentration St. Mary s Hosp., Ann Emerg Med 2001:38(4); S39
62 300 IL-6 concentration(pg/ml) * * * CPC(1-2) CPC(3-5) 20min 2h 4h 12h 24h 48h 72h Time Patterns of evolution of serum IL-6 after successful CPR. Data are expressed as mean ± SEM, * p < 0.05 St.Mary s Hosp., Ann Emerg Med 2000:36(4); S91
63 Combination of Predictive factors
64 Sensitivity, specificity, positive and negative likelihood ratio of numerous tests and results in predicting poor outcome after coma Indicator of poor prognosis Outcome Poor * Good * Sensitivity (%) Specificity (%) LR+ LRp SEP, bilateral absent N20 (n=35) 13/24 0/ SEP, uni-/bilateral absent N20 (n=35) 15/24 1/ MRS, lactate(+) (n=27) 15/19 0/ SEP, bilateral absent N20 when MRS also examed (n=26) 11/18 0/ MRS, lactate(+), SEP, bilateral absent N20, or both (n=26) 17/18 0/ St.Mary s Hosp. Unpubulished data,
65 Sensitivity(%) BL abs N20 BL abs N20 when MRS UL/BL abs N20 Lac (+) Lac(+) or BL abs N20 Figure 1. Sensitivity of various criteria for predicting poor outcome. Specificity of all criteria except 'UL/BL abs N20' is 100% in the population tested. UL = unilateral; BL = bilateral; Lac = lactate; abs = absent. St.Mary s Hosp., Unpubulished data,
66 Good outcome Poor outcome Lac(+) Lac(-) Other Bilateral N20(-) Figure 2. MRS lactate, SEP N20, and outcome in 26 coma patients with cardiac arrest. BL = bilateral; Lac = lactate; abs = absent. St.Mary s Hosp., Unpubulished data,
67
68
69

70 Thanks for your attention!!
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Enhancing 5 th Chain TTM after Cardiac Arrest
 Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Patient Case. Post cardiac arrest pathophysiology 10/19/2017. Disclosure. Objectives. Patient Case-TM
 Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Post Cardiac Arrest Care. From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
 Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
Hypothermia: The Science and Recommendations (In-hospital and Out)
") Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Objectives. Trends in Resuscitation POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE?
 POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
POST-CARDIAC ARREST CARE: WHAT S THE EVIDENCE? Nicole Kupchik RN, MN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest Care Discuss oxygenation & hemodynamic taregts
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center
 Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Post-resuscitation care for adults. Jerry Nolan Royal United Hospital Bath
 Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Neuroprognostication after cardiac arrest
 Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Curricullum Vitae. Dr. Isman Firdaus, SpJP (K), FIHA
, FIHA") Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
The Evidence Base. Stephan A. Mayer, MD. Columbia University New York, NY
 Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Induced Hypothermia for Cardiac Arrest. Heather Hand RN,CCRN,CNRN,ATCN,LNC
 Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
Induced Hypothermia for Cardiac Arrest Heather Hand RN,CCRN,CNRN,ATCN,LNC Cardiac Arrest Epidemiology 400,000 arrests / year in U.S.A 3 / 4 Out-of-hospital 1 / 4 In-hospital survival to hospital 1-5% discharge
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
INDUCED HYPOTHERMIA. F. Ben Housel, M.D.
 INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
INDUCED HYPOTHERMIA F. Ben Housel, M.D. Historical Use of Induced Hypothermia 1950 s - Moderate hypothermia (30-32º C) in open heart surgery to protect brain against global ischemia 1960-1980 s - Use of
RACE CARS: Hospital Response. David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012
 L MODULE 9 RACE CARS: Hospital Response David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012 2 Objectives: Post-cardiac arrest syndrome Therapeutic hypothermia
L MODULE 9 RACE CARS: Hospital Response David A. Pearson, MD Department of Emergency Medicine Carolinas Medical Center February 23, 2012 2 Objectives: Post-cardiac arrest syndrome Therapeutic hypothermia
Case Presentation. Cooling. Case Presentation. New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation
 New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
New Developments in Cardiopulmonary Arrest: Therapeutic Hypothermia in Resuscitation Michael Sayre, MD Emergency Medicine and LeRoy Essig, MD Pulmonary/Critical Care Medicine Case Presentation 3:40 (+
POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association
 POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association - 2016 Nicole Kupchik MN, RN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest
POST-CARDIAC ARREST CARE: WHAT HAPPENS AFTER ROSC MATTERS! Emergency Nurses Association - 2016 Nicole Kupchik MN, RN, CCNS, CCRN, PCCN, CMC Objectives Discuss the 2015 AHA Guideline Updates for Post- Arrest
Samphant Ponvilawan Bumrungrad International
 Samphant Ponvilawan Bumrungrad International Definitions Artificial circulation using VA ECMO as an alternative to ventilation and external cardiac massage Indications Out-of-Hospital Cardiac Arrest (OHCA)
Samphant Ponvilawan Bumrungrad International Definitions Artificial circulation using VA ECMO as an alternative to ventilation and external cardiac massage Indications Out-of-Hospital Cardiac Arrest (OHCA)
State of the art lecture: 21st Century Post resuscitation management
 State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest
 ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
Disclosures. Pediatrician Financial: none Volunteer :
 Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
IN HOSPITAL CARDIAC ARREST AND SEPSIS
 IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
ALS 713: Prognostication in Normothermia
 ALS 713: Prognostication in Normothermia TFQO: Clifton Callaway (COI #214) EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35) Taskforce: ALS COI Disclosure (specific to this systematic review)
ALS 713: Prognostication in Normothermia TFQO: Clifton Callaway (COI #214) EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35) Taskforce: ALS COI Disclosure (specific to this systematic review)
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest
 Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Regionalization of Post-Cardiac Arrest Care
 Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Therapeutic Hypothermia after Resuscitated Cardiac Arrest
 Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
Therapeutic Hypothermia after Resuscitated Cardiac Arrest The purpose of this protocol is to improve the neurologic outcomes of patients who have experienced cardiac arrest and have been successfully resuscitated.
CRS Center for Resuscitation Science
 Therapeutic hypothermia after cardiac arrest and in critical care Speaker disclosures Research Funding: NIH NHLBI Philips Healthcare Doris Duke Foundation American Heart Association CRS Center for Resuscitation
Therapeutic hypothermia after cardiac arrest and in critical care Speaker disclosures Research Funding: NIH NHLBI Philips Healthcare Doris Duke Foundation American Heart Association CRS Center for Resuscitation
In the past decade, two large randomized
 Mild therapeutic hypothermia improves outcomes compared with normothermia in cardiac-arrest patients a retrospective chart review* David Hörburger, MD; Christoph Testori, MD; Fritz Sterz, MD; Harald Herkner,
Mild therapeutic hypothermia improves outcomes compared with normothermia in cardiac-arrest patients a retrospective chart review* David Hörburger, MD; Christoph Testori, MD; Fritz Sterz, MD; Harald Herkner,
Cardio Pulmonary Cerebral Resuscitation
 Cardio Pulmonary Cerebral Resuscitation Brain Under Pressure October 3, 2017 Canadian Critical Care Forum Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto
Cardio Pulmonary Cerebral Resuscitation Brain Under Pressure October 3, 2017 Canadian Critical Care Forum Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto
Hypothermia Post Cardiac Arrest: An Update
 Hypothermia Post Cardiac Arrest: An Update Justin Lundbye, M.D., FACC Hospital of Central Connecticut Justin.Lundbye@HHCHealth.org Outline Background Whom to Cool How to Cool Post Cardiac Arrest Care Other
Hypothermia Post Cardiac Arrest: An Update Justin Lundbye, M.D., FACC Hospital of Central Connecticut Justin.Lundbye@HHCHealth.org Outline Background Whom to Cool How to Cool Post Cardiac Arrest Care Other
Mild. Moderate. Severe. 32 to to and below
 Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Therapeutic Hypothermia
 Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Objectives Overview Therapeutic Hypothermia Nerissa U. Ko, MD, MAS UCSF Department of Neurology Critical Care Medicine and Trauma June 4, 2011 Hypothermia as a neuroprotectant Proven indications: Adult
Hypothermia After Cardiac Arrest: Where Are We Now?
 Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
Hypothermia After Cardiac Arrest: Where Are We Now? David A. Pearson, MD, MS Associate Professor Director of Cardiac Arrest Resuscitation Carolinas HealthCare System Disclosures I have no financial interest,
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN (865) LABEL
 LABEL") 1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
Update on Sudden Cardiac Death and Resuscitation
 Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Update on Sudden Cardiac Death and Resuscitation Ashish R. Panchal, MD, PhD Medical Director Center for Emergency Medical Services Assistant Professor Clinical Department of Emergency Medicine The Ohio
Today s Outline WA--ACEP Journal Club ACEP Journal Club Background on WA Background on WA--ACEP ACEP Journal Club Strategic Goals for JC
 Today s Outline WA-ACEP ACEP Journal Club Value of Therapeutic Hypothermia as a Treatment Modality (May 18, 2011) Review History and Objectives of JC Summary of November JC Therapeutic Hypothermia Current
Today s Outline WA-ACEP ACEP Journal Club Value of Therapeutic Hypothermia as a Treatment Modality (May 18, 2011) Review History and Objectives of JC Summary of November JC Therapeutic Hypothermia Current
Post-Resuscitation Care. Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena
 Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Post-Resuscitation Care Prof. Wilhelm Behringer Center of Emergency Medicine University of Jena Conflict of interest Emcools Shareholder and founder, honoraria Zoll: honoraria Bard: honoraria, nephew works
Controversies in Post Resuscitation After Cardiac Arrest
 Controversies in Post Resuscitation After Cardiac Arrest More News About Gainesville FL.. 124,354 souls 2007 Best place to live and play in USA 2009 UF ranked #1 party school Andrea Gabrielli, MD FCCM
Controversies in Post Resuscitation After Cardiac Arrest More News About Gainesville FL.. 124,354 souls 2007 Best place to live and play in USA 2009 UF ranked #1 party school Andrea Gabrielli, MD FCCM
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest. Objectives: U.S. stats
 Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
Post-Resuscitation Care: Optimizing & Improving Outcomes after Cardiac Arrest Nicole L. Kupchik RN, MN, CCNS CCRN-CMC Clinical Nurse Specialist Harborview Medical Center Seattle, WA Objectives: At the
2015 AHA Guidelines: Pediatric Updates
 2015 AHA Guidelines: Pediatric Updates Advances in Pediatric Emergency Medicine December 9, 2016 Karen O Connell, MD, MEd Associate Professor of Pediatrics and Emergency Medicine Emergency Medicine and
2015 AHA Guidelines: Pediatric Updates Advances in Pediatric Emergency Medicine December 9, 2016 Karen O Connell, MD, MEd Associate Professor of Pediatrics and Emergency Medicine Emergency Medicine and
Cardiac Arrest January 2017 CPR /3/ Day to Survival Propensity Matched
 Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
 Emergency Medicine Australasia (2011) 23, 292 296 doi: 10.1111/j.1742-6723.2011.01422_15.x POST-RESUSCITATION THERAPY Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
Emergency Medicine Australasia (2011) 23, 292 296 doi: 10.1111/j.1742-6723.2011.01422_15.x POST-RESUSCITATION THERAPY Post-resuscitation Therapy in Adult Advanced Life Support. ARC and NZRC Guideline 2010
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
CrackCast Episode 8 Brain Resuscitation
 CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
CrackCast Episode 8 Brain Resuscitation Episode Overview: 1) Describe 6 therapeutic interventions for the post-arrest brain 2) List 5 techniques for initiating therapeutic hypothermia 3) List 4 mechanisms
Lesson learnt from big trials. Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ.
 Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Therapeutic Hypothermia ANZCA 2013
 Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
Therapeutic Hypothermia ANZCA 2013 Stephen Bernard MD Therapeutic Hypothermia-Indications Anoxic brain injury (cardiac arrest) Severe traumatic brain injury Spinal cord injury Why not Therapeutic Hypothermia?
Hypothermia Induction Methods
 Hypothermia Induction Methods Advantages and Disadvantages Xia Luo, M.D. Vice President, Clinical Education ZOLL Corporation Targeted Temperature Management (TTM) Temperature is one of the four vital signs
Hypothermia Induction Methods Advantages and Disadvantages Xia Luo, M.D. Vice President, Clinical Education ZOLL Corporation Targeted Temperature Management (TTM) Temperature is one of the four vital signs
3/6/2017. Endovascular Selective Cerebral Hypothermia First-in-Human Experience
 Endovascular Selective Cerebral Hypothermia First-in-Human Experience Ronald Jay Solar, Ph.D. San Diego, CA 32 nd Annual Snowmass Symposium March 5-10, 2017 Introduction Major limitations in acute ischemic
Endovascular Selective Cerebral Hypothermia First-in-Human Experience Ronald Jay Solar, Ph.D. San Diego, CA 32 nd Annual Snowmass Symposium March 5-10, 2017 Introduction Major limitations in acute ischemic
Current status of temperature management in the neuro-icu
 Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
Current status of temperature management in the neuro-icu Gregor Brössner, MD Neurologic Intensiv Care Unit Innsbruck, Austria Disclosures: Gregor Brössner has recieved an unrestricted Grant by Alsius
WORKSHEET for Evidence-Based Review of Science for Veterinary CPCR
 RECOVER 2011 1 of 12 WORKSHEET for Evidence-Based Review of Science for Veterinary CPCR 1. Basic Demographics Worksheet author(s) Jane Quandt Mailing address: 501 DW Brooks Drive Small Animal Medicine
RECOVER 2011 1 of 12 WORKSHEET for Evidence-Based Review of Science for Veterinary CPCR 1. Basic Demographics Worksheet author(s) Jane Quandt Mailing address: 501 DW Brooks Drive Small Animal Medicine
Targeted temperature management after post-anoxic brain insult: where do we stand?
 Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results of Cerebral Perfusion MR Imaging
 pissn 2384-1095 eissn 2384-1109 imri 2018;22:56-60 https://doi.org/10.13104/imri.2018.22.1.56 Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results
pissn 2384-1095 eissn 2384-1109 imri 2018;22:56-60 https://doi.org/10.13104/imri.2018.22.1.56 Complete Recovery of Perfusion Abnormalities in a Cardiac Arrest Patient Treated with Hypothermia: Results
THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST
 THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST Heather Harrington RN, BScN, CNCC(c) Clinical Nurse Educator Sunnybrook Health Sciences Centre Objectives Define Therapeutic Hypothermia (TH) Describe current
THERAPEUTIC HYPOTHERMIA POST CARDIAC ARREST Heather Harrington RN, BScN, CNCC(c) Clinical Nurse Educator Sunnybrook Health Sciences Centre Objectives Define Therapeutic Hypothermia (TH) Describe current
Post Resuscitation Care
 Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Princess Margaret Hospital f Children PAEDIATRIC ACUTE CARE GUIDELINE Post Resuscitation Care Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should
Cardiac Critical Care Lance Cohen, MD MBBCh FCCP
 Cardiac Critical Care 2011 Lance Cohen, MD MBBCh FCCP Open Heart Surgery Program Lance Cohen, MD MBBCh FCCP Medical Director - HSU Open Heart Surgery Program Team Cardiac Surgeons Richard Perryman, MD
Cardiac Critical Care 2011 Lance Cohen, MD MBBCh FCCP Open Heart Surgery Program Lance Cohen, MD MBBCh FCCP Medical Director - HSU Open Heart Surgery Program Team Cardiac Surgeons Richard Perryman, MD
Developments in Cardiopulmonary Resuscitation Guidelines
 Developments in Cardiopulmonary Resuscitation Guidelines Bernd W. Böttiger Seite 1 To preserve human life by making high quality resuscitation available to all Outcome after CPR in Germany ROSC ( Return
Developments in Cardiopulmonary Resuscitation Guidelines Bernd W. Böttiger Seite 1 To preserve human life by making high quality resuscitation available to all Outcome after CPR in Germany ROSC ( Return
Therapeutic Hypothermia. Jonas Cooper, MD MPH
 Therapeutic Hypothermia Jonas Cooper, MD MPH Hypothermia in Cardiology Early cardiac surgery included cooling to 15 C and stopping all blood flow for one hour while surgery proceeded Belsey RH et al. Profound
Therapeutic Hypothermia Jonas Cooper, MD MPH Hypothermia in Cardiology Early cardiac surgery included cooling to 15 C and stopping all blood flow for one hour while surgery proceeded Belsey RH et al. Profound
Controversies in Chest Compressions & Airway Management During CPR. Bob Berg
 Controversies in Chest Compressions & Airway Management During CPR Bob Berg No Financial Conflicts of Interest Employment: University of Pennsylvania AHA Volunteer AHA GWTG-R & Systems of Care committees
Controversies in Chest Compressions & Airway Management During CPR Bob Berg No Financial Conflicts of Interest Employment: University of Pennsylvania AHA Volunteer AHA GWTG-R & Systems of Care committees
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care
 Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
Pathophysiology and Cardiac Insights for Targeted Temperature Management in Emergency Medicine and Critical Care LINDSAY LEWIS BSN, RN, CCCC Faculty Disclosure I AM CURRENTLY EMPLOYED AS A CLINICAL MANAGER
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
New Therapeutic Hypothermia Techniques
 New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
New Therapeutic Hypothermia Techniques Joseph P. Ornato, MD, FACP, FACC, FACEP Professor & Chairman, Emergency Medicine Virginia Commonwealth University Health System Richmond, VA Medical Director Richmond
EXTRACORPOREAL LIFE SUPPORT FOR PROLONGED CARDIAC ARREST
 EXTRACORPOREAL LIFE SUPPORT FOR PROLONGED CARDIAC ARREST Massimo MASSETTI Cardiac Surgery Department University of Sacred Heart, Gemelli Hospital Rome «No financial interest to declare» ESC CONGRESS 2012
EXTRACORPOREAL LIFE SUPPORT FOR PROLONGED CARDIAC ARREST Massimo MASSETTI Cardiac Surgery Department University of Sacred Heart, Gemelli Hospital Rome «No financial interest to declare» ESC CONGRESS 2012
Therapeutic Hypothermia After Cardiac Arrest: Best Practices 2014
 Therapeutic Hypothermia After Cardiac Arrest: Best Practices 2014 Deborah Klein, RN, MSN, ACNS-BC, CCRN, CHFN, FAHA Clinical Nurse Specialist Coronary ICU, Heart Failure ICU, and Cardiac Short Stay/PACU/CARU
Therapeutic Hypothermia After Cardiac Arrest: Best Practices 2014 Deborah Klein, RN, MSN, ACNS-BC, CCRN, CHFN, FAHA Clinical Nurse Specialist Coronary ICU, Heart Failure ICU, and Cardiac Short Stay/PACU/CARU
Emergency Cardiac Care Guidelines 2015
 Emergency Cardiac Care Guidelines 2015 VACEP 2016 William Brady, MD University of Virginia Guidelines 2015 Basic Life Support & Advanced Cardiac Life Support Acute Coronary Syndrome Pediatric Advanced
Emergency Cardiac Care Guidelines 2015 VACEP 2016 William Brady, MD University of Virginia Guidelines 2015 Basic Life Support & Advanced Cardiac Life Support Acute Coronary Syndrome Pediatric Advanced
Neurotrauma: The Place for Cooling
 Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Neurotrauma: The Place for Cooling Cooling: to achieve hypothermia History, evidence, open questions Cooling: to achieve normothermia Evidence, open questions Cooling: Practical Aspects Hypothermia: History
Therapeutic Hypothermia: 2011 Research Update. Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine
 Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Accidental Hypothermia
 Accidental Hypothermia Gordon G. Giesbrecht, Ph.D., Professor Health Leisure and Human Performance Research Institute University of Manitoba, Winnipeg, Manitoba, Canada, R3T 2N2 Learning Objectives: 1)
Accidental Hypothermia Gordon G. Giesbrecht, Ph.D., Professor Health Leisure and Human Performance Research Institute University of Manitoba, Winnipeg, Manitoba, Canada, R3T 2N2 Learning Objectives: 1)
Identifying Best Practice for Out-of-Hospital Cardiac Arrest (OHCA) in the Hospital Setting
 in the Hospital Setting") Identifying Best Practice for Out-of-Hospital Cardiac Arrest (OHCA) in the Hospital Setting Mary Ann Peberdy, MD, FACC, FAHA C. Kenneth Wright Professor of Cardiology & Professor of Emergency Medicine
Identifying Best Practice for Out-of-Hospital Cardiac Arrest (OHCA) in the Hospital Setting Mary Ann Peberdy, MD, FACC, FAHA C. Kenneth Wright Professor of Cardiology & Professor of Emergency Medicine
Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti
 Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti U.O.C Anestesia e Terapia Intensiva Policlinico San Martino - GENOVA Natural Course of Neurological Recovery Following Cardiac Arrest Cardiac
Ipotermia terapeutica controversie e TTM 2 Trial Iole Brunetti U.O.C Anestesia e Terapia Intensiva Policlinico San Martino - GENOVA Natural Course of Neurological Recovery Following Cardiac Arrest Cardiac
Disclosures. Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 ECG. Case. Case. Case Summary 4/22/2016
 Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 Nothing to disclose. Disclosures Ivan J Chavez MD Case ECG History 60 y/o male No prior history of CAD In
Extra-Corporeal Membrane Oxygenation During Cardio- Pulmonary Resuscitation ECPR April 22, 2016 Nothing to disclose. Disclosures Ivan J Chavez MD Case ECG History 60 y/o male No prior history of CAD In
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Epinephrine Cardiovascular Emergencies Symposium 2018
 Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Multimodal monitoring to prognosticate in anoxic brain injury
 Multimodal monitoring to prognosticate in anoxic brain injury Eyal Golan, MD FRCPC PhD(c) Critical Care & Neurosciences Critical Care Medicine Interdepartmental Division of Critical Care and Department
Multimodal monitoring to prognosticate in anoxic brain injury Eyal Golan, MD FRCPC PhD(c) Critical Care & Neurosciences Critical Care Medicine Interdepartmental Division of Critical Care and Department
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital
 Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
Tina Yoo, PharmD Clinical Pharmacist Alameda Health System Highland Hospital 1 Review changes in the 2015 AHA ACLS guidelines with emphasis on changes in therapeutic hypothermia Provide overview of ACLS
WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre
 Claudio Sandroni, Giuseppe La Torre") Worksheet No. ALS-PA-041.doc Page 1 of 16 WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre Date Submitted for review: 27
Worksheet No. ALS-PA-041.doc Page 1 of 16 WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre Date Submitted for review: 27
Therapeutic hypothermia following cardiac arrest
 TITLE: Therapeutic hypothermia following cardiac arrest AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
TITLE: Therapeutic hypothermia following cardiac arrest AUTHOR: Jeffrey A. Tice, MD Assistant Professor of Medicine Division of General Internal Medicine Department of Medicine University of California
Case: 65 year old post-cardiac arrest patient with myoclonus
 Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Any man s death diminishes me, because I am involved in mankind. - John Donne
 Any man s death diminishes me, because I am involved in mankind - John Donne Cardiac Arrest in 2011 Where are we? Or where should we be? Michael W. Dailey, MD FACEP Associate Professor of Emergency Medicine
Any man s death diminishes me, because I am involved in mankind - John Donne Cardiac Arrest in 2011 Where are we? Or where should we be? Michael W. Dailey, MD FACEP Associate Professor of Emergency Medicine
Drowning is a leading cause of death and loss of years of life with over 90% of cases occurring in lower- and middle-income countries.
 Chapter 145 Drowning Episode Overview: 1) List risk factors for drowning 2) List 5 variables that portend poor outcome 3) Describe the diving reflex 4) Describe the management of a drowning patient with
Chapter 145 Drowning Episode Overview: 1) List risk factors for drowning 2) List 5 variables that portend poor outcome 3) Describe the diving reflex 4) Describe the management of a drowning patient with
Predicting neurological outcome and survival after cardiac arrest
 Predicting neurological outcome and survival after cardiac arrest Andy Temple MB ChB FRCA FFICM Richard Porter MB ChB FRCA Matrix reference 2C01, 2C04 Key points Accurately predicting neurological outcome
Predicting neurological outcome and survival after cardiac arrest Andy Temple MB ChB FRCA FFICM Richard Porter MB ChB FRCA Matrix reference 2C01, 2C04 Key points Accurately predicting neurological outcome
Emergency Preservation and Resuscitation
 Emergency Preservation and Resuscitation Samuel A. Tisherman, MD, FACS, FCCM Director, Center for Critical Care and Trauma Education Director, SICU RA Cowley Shock Trauma Center Disclosures Co-author of
Emergency Preservation and Resuscitation Samuel A. Tisherman, MD, FACS, FCCM Director, Center for Critical Care and Trauma Education Director, SICU RA Cowley Shock Trauma Center Disclosures Co-author of
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on Needed to be resuscitated at birth
 No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Ipotermia terapeutica nel bambino: manca l evidenza?
 Ipotermia terapeutica nel bambino: manca l evidenza? Andrea Moscatelli UOSD Terapia Intensiva Neonatale e Pediatrica Dipartimento Integrato di Alta Intensita` di Cura e Chirurgia Istituto Giannina Gaslini
Ipotermia terapeutica nel bambino: manca l evidenza? Andrea Moscatelli UOSD Terapia Intensiva Neonatale e Pediatrica Dipartimento Integrato di Alta Intensita` di Cura e Chirurgia Istituto Giannina Gaslini
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation
 The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
Objectives. Birth Depression Management. Birth Depression Terms
 Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Objectives Birth Depression Management Regional Perinatal Outreach Program 2016 Understand the terms and the clinical characteristics of birth depression. Be familiar with the evidence behind therapeutic
Disclosures. Overview. Cardiopulmonary Arrest: Quality Measures 5/29/2014. In-Hospital Cardiac Arrest: Measuring Effectiveness and Improving Outcomes
 Disclosures In-Hospital Cardiac Arrest: Measuring Effectiveness and Improving Outcomes Research support from UCOP CHQI award J. Matthew Aldrich, MD Anesthesia & Critical Care UCSF Overview Epidemiology
Disclosures In-Hospital Cardiac Arrest: Measuring Effectiveness and Improving Outcomes Research support from UCOP CHQI award J. Matthew Aldrich, MD Anesthesia & Critical Care UCSF Overview Epidemiology
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
Neurologic Recovery and Prognostication
 Neurologic Recovery and Prognostication Sudden Cardiac Arrest Association Jon Rittenberger, MD, MS October 8, 2010 Disclosures Employer: University of Pittsburgh/ UPMC Grants: - National Association of
Neurologic Recovery and Prognostication Sudden Cardiac Arrest Association Jon Rittenberger, MD, MS October 8, 2010 Disclosures Employer: University of Pittsburgh/ UPMC Grants: - National Association of
What Hospitalists Need to Know about ICU Neurology
 What Hospitalists Need to Know about ICU Neurology S. Andrew Josephson, MD Department of Neurology, Neurovascular Service University of California San Francisco September 25, 2009 The speaker has no disclosures
What Hospitalists Need to Know about ICU Neurology S. Andrew Josephson, MD Department of Neurology, Neurovascular Service University of California San Francisco September 25, 2009 The speaker has no disclosures
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017
 Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC