Neurologic Recovery and Prognostication
|
|
|
- Randolph Small
- 6 years ago
- Views:
Transcription




1 Neurologic Recovery and Prognostication Sudden Cardiac Arrest Association Jon Rittenberger, MD, MS October 8, 2010 Disclosures Employer: University of Pittsburgh/ UPMC Grants: - National Association of EMS Physicians/Zoll Medical - NIH KL2 Clinical Scholar- University of Pittsburgh Clinical and Translational Science Institute Steering Committee: Zoll Cool Arrest Speaker: Sacramento EMS- conference sponsored by Zoll/Medtronic/Medi-Therm NIRS devices on loan from Somanetics 1
 - Brain Imaging (CT, MRI) - Evoked Potentials - Biomarkers 600-1000 Americans will suffer OOHCA today 300,000 Americans suffer OOHCA yearly 25+ will suffer OOHCA during")
2 Describe new model for early stratification of postcardiac arrest illness Discuss benefits and pitfalls of prognostication during the post-arrest phase: - Clinical Examination - Electroencephalography (EEG) - Brain Imaging (CT, MRI) - Evoked Potentials - Biomarkers Americans will suffer OOHCA today 300,000 Americans suffer OOHCA yearly 25+ will suffer OOHCA during this talk High morbidity and mortality - ~50% never make it to the hospital 2




3 Multiple Ways to Die 100% 80% 60% 40% 20% 0% Out-of-Hospital In-Hospital Location of Cardiac Arrest Survive without Symptoms Survive with Neurological Deficit Neurological Death Cardiovascular Death Multi-System Organ Failure Laver (2004) 3




4 Brain Injury after Cardiac Arrest Brain Dead Severity of Injury Normal If you have acute, severe cerebral edema, no therapy will help Duration of Ischemia Neurological Intensive Care Brain Dead Severity of Injury Normal Proper care can improve outcome for those who are in the salvageable range Duration of Ischemia 4
5 An Integrated Approach Physical / Occupational Therapy Neurology Neurophysiology Cardiology PM&R EMS Emergency Medicine Critical Care Medicine Renal Medicine Surgery Toxicology Internal Medicine Palliative Care Titrating Care - Patients are Different - Not just on Protocol Type 1 Type 2 Type 3 Type 4 5
 Motor response (0-4) Brainstem response (0-4) Respiratory pattern (0-4) Wijdicks Ann Neurol 2005;58:585 Assessment for Shock - Injury Severity Scores")
6 Exam in Coma FOUR score has been proposed as a scale with more resolution for the intubated ICU patient. Incorporates four exams Eye movements (0-4) Motor response (0-4) Brainstem response (0-4) Respiratory pattern (0-4) Wijdicks Ann Neurol 2005;58:585 Assessment for Shock - Injury Severity Scores Serial Organ Function Assessment (SOFA) SOFA Respiratory PaO2 / >400 <400 <300 <200 <100 FIO2 Renal Creat Urine Out < <500 ml/d >5.0 <200 ml/d Hepatic Bili < >12.0 Cardiac MAP < 70 No MAP<70 Dop <5 Dop > 5 Pressors Dobut Epi < 0.1 Dop>15 Epi>0.1 NE>0.1 NE < 0.1 Hematologic Platelet >150 <150 <100 <50 <20 Neurological GCS <6 TOTAL 6
7 Classification of Post-CPR Patients Neurological Injury None Some Lots Complete Shock None Mild Severe Type 1 Type 2 Type 3 Type 4 Shock Neurological Injury Awake or waking up quickly; Combined FOUR Motor-Brainstem Score=8 7
8 Shock Neurological Injury Moderate or deep coma, but with some signs of neurological function; University of Pittsburgh Combined School of FOUR Medicine Motor-Brainstem - Department of Emergency Score Medicine 4-7 Combined SOFA Cardiac and Respiratory Score <4 Shock Neurological Injury Moderate or deep coma, but with some signs of neurological function; University of Pittsburgh Combined School of Medicine FOUR Motor-Brainstem - Department of Emergency Score Medicine 4-7 Combined SOFA Cardiac-Respiratory Score 4 8
9 Shock Neurological Injury Coma with minimal or absent brainstem reflexes University of Pittsburgh Combined School of Medicine FOUR Motor-Brainstem - Department of Emergency Scores Medicine 4 Survival and Good Outcome Good Poor
10 Multiple Organ Failure Rhythm and Category VF/VT PEA Asystole Unknown Category I Category II Category III Category IV



11 Neurologic Prognostication One Potential Model CT scan EEG SSEP* Consider Repeat EEG, SSEP Consider MRI Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Hypothermia Physical / Occupational Therapy; Consider Stimulants Optimize Perfusion and Metabolic Status Discuss long-term support; tracheostomy, feeding tube 11
12 Prognostication Wijdicks (2006) American Academy of Neurology Prognostication Wijdicks (2006) American Academy of Neurology Easter Syndrome At 72 hours, the doctor will tell us if he is going to make it 12
13 Clinical Examination A Cautionary Case Day male arrived in ED after resuscitation from PEA - likely overdose of heroin and xanax - found in arrest by girlfriend who saw him snoring 30 minutes prior - Epi x 3 mg, naloxone x 2 mg, bicarb x 2 amps, amiodarone (300 mg) Surprised we got him back - Sluggish pupils; No gag or cough; Decorticate - Pressure 80/p --> dopamine, norepinephrine - ABG- ph 6.86; pco2 81; po2 373; Lactate = LFT s - ASL 1551; ALT Hypothermia --> 32º for 24 hours 13
 A Cautionary Case Day 1 (24 hrs) - - Sluggish pupils,")
 - Pupils react, no oculocephalic reflex, decorticate,")
14 Early CT/MR Findings Whole brain is tight. Basal ganglia have edema / ischemic changes. (More common with asphyxial / respiratory events) A Cautionary Case Day 1 (24 hrs) - - Sluggish pupils, weak cough, decorticate - Rhabdomyolysis - renal failure - CVVHD Day 2 (48 hrs) - Pupils react, decorticate, some shaking tremor Day 3 (72 hrs) - Pupils react, no oculocephalic reflex, decorticate, shaking all over, eyes closed 14
15 A Cautionary Case Day 1 (24 hrs) - - Sluggish pupils, weak cough, decorticate - Rhabdomyolysis - renal failure - CVVHD Day 2 (48 hrs) - Pupils react, decorticate, some shaking tremor Day 3 (72 hrs) - Pupils react, no oculocephalic reflex, decorticate, shaking all over, eyes closed Day 4 (96 hrs) - Withdrawal of leg from pain Day 5 (120 hrs) - Awake A Cautionary Case Day 17 - Transfer to Rehab (still on dialysis) Day 34 - Home Six-Month Follow-up - Off dialysis; Running 4-5 miles / day; just returned from Caribbean vacation; Continues in drug rehab. 15
16 Local Data: Motor Examination at 72 hours 272 patients treated between cooled, 111 normothermia GCS Motor >3 GCS Motor 3 Odds Ratio (95% CI) 72 hour- Not Cooled (Survival) 33/63 (52%; 95% CI 14, 33%) 4/12 (33%; 95% CI 2, 64%) 2.2 (0.60, 8.06) 72 hour- Cooled (Survival) 44/69 (64%; 95% CI 52, 76%) 4/28 (14%; 95% CI 0, 29%) (3.29, 33.92) Rittenberger et al. Resuscitation 2010;81(9): Local Data: Motor Examination at 72 hours 272 patients treated between cooled, 111 normothermia GCS Motor >3 GCS Motor 3 Odds Ratio (95% CI) 72 hour- Not Cooled (Survival) 33/63 (52%; 95% CI 14, 33%) 4/12 (33%; 95% CI 2, 64%) 2.2 (0.60, 8.06) 72 hour- Cooled (Survival) 44/69 (64%; 95% CI 52, 76%) 4/28 (14%; 95% CI 0, 29%) (3.29, 33.92) Rittenberger et al. Resuscitation 2010;81(9):
17 Local Data: Brainstem Examination at 72 hours 72 hour not cooled (survival) 72 hour cooled (survival) Pupil Present 2/39 (56%; 95% CI 40, 73%) 41/56 (73%; 95% CI %) Pupil Absent 0/1 (0%; 95% CI 0, 50%) 0/16 (0%; 95% CI 0, 3%) 72 hour not cooled (survival) 72 hour cooled (survival) Corneal Present 22/39 (56%; 95% CI 40, 73%) 42/53 (79%; 95% CI 67, 91%) Corneal Absent 0/1 (0%; 95% CI 0, 50%) 0/20 (0%; 95% CI 0, 3%) Local Data: Brainstem Examination at 72 hours 72 hour not cooled (survival) 72 hour cooled (survival) Pupil Present 2/39 (56%; 95% CI 40, 73%) 41/56 (73%; 95% CI %) Pupil Absent 0/1 (0%; 95% CI 0, 50%) 0/16 (0%; 95% CI 0, 3%) 72 hour not cooled (survival) 72 hour cooled (survival) Corneal Present 22/39 (56%; 95% CI 40, 73%) 42/53 (79%; 95% CI 67, 91%) Corneal Absent 0/1 (0%; 95% CI 0, 50%) 0/20 (0%; 95% CI 0, 3%) 17
18 Patience mon Capitan! GCS is most predictive for good outcome at day 4. Sensitivity 84%, PPV 92.5% Schefold, et al. Resuscitation 2009;80(6): CT Imaging Review of 182 CT s obtained within 24 hours of arrest Analyzed results based on initial Glasgow Coma Scale 18
19 CT Imaging by Coma Severity Normal Acute Diffuse Ischemia Acute Focal Ischemia Old Changes Ageindetermi nate changes Acute Bleed Unable to interpret GCS (32%) 33 (32%) 6 (6%) 22 (21%) 2 (2%) 3 (3%) 4 (4%) GCS (59%) 4 (9%) 2 (4%) 8 (17%) 1 (2%) 1 (2%) 3 (7%) Peoples J. Acad Emerg Med 2010 CT Imaging: Survivorship Normal Acute Difuse Ischemia Acute Focal Ischemia Old Changes Ageindetermi nate changes Acute Bleed Unable to interpret Survived 20 (67%) 1 (3%) 3 (10%) 3 (10%) 1 (3%) 0 (0%) 2 (7%) Died 40 (34%) 36 (30%) 5 (4%) 27 (23%) 2 (2%) 4 (3%) 5 (4%) Peoples J. Acad Emerg Med


20 Grey to White Matter Ratio Proposed as an early predictor of survival Associated with survival in pediatric drowning victims Decreasing GWR * * * *p<
21 ROC Curve: Predicting Death Avg GWR is 100% predictive of death Cutoff =1.2 GWR<1.2 GWR>1.2 Surv 0% (0/47) 95% CI 0-1% Surv 58% (76/130) 95% CI 50-67% CT scan EEG SSEP* Consider Repeat EEG, SSEP Consider MRI Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Hypothermia Physical / Occupational Therapy; Consider Stimulants Optimize Perfusion and Metabolic Status Discuss long-term support; tracheostomy, feeding tube 21
22 Comparison to Other Studies Torbey (2000) - 25 adult pts, Ratio < % specificity - Ctrl group GWR (median range) Choi (2008) - 28 adult pts, ratio < % specificity - Ctrl group GWR 1.32 (0.05) Rafaat (2008) peds drowning pts, abnormal CT + GCS=3, 100% specificity EEG 22
 HACA (2002) estimated incidence of 7-8% Abend (2009) noted")

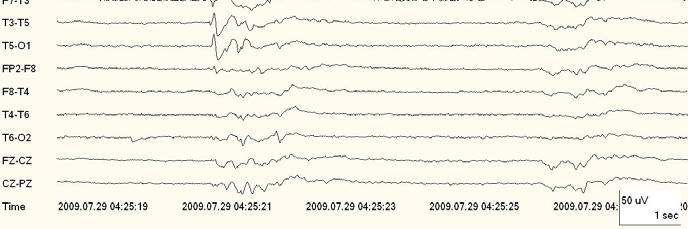
23 Brain Monitoring- EEG Several bad findings possible - Nonconvulsive status epilepticus (NCSE) HACA (2002) estimated incidence of 7-8% Abend (2009) noted incidence of 47% in pediatric CA subjects - Myoclonic status epilepticus - Isoelectric baseline Most literature is pre-hypothermia EEG Post-Arrest: Shivering 23



24 EEG Post-Arrest: Paralyzed, on propofol EEG Post-Arrest: Paralyzed, Off propofol 24



25 Across the hall 25
26 Seizures are Common %: Incidence of electrographic seizure Progression of EEG patterns Epileptiform Discharges: 50% GPED: 22% NCSE: 10% Burst Suppression: 55% MSE: 24% 26
27 Not all patients are at equal risk Electrographic seizure incidence varied by category of arrest (p=0.045) - Category II: 3/31 (10%) - Category III: 4/10 (40%) - Category IV: 10/35 (29%) Electrographic seizure incidence did not vary by rhythm of arrest (p=0.141) or location of arrest (p=0.842) Seizures occur early Time from arrest to ceeg placement is 8 (IQR 6, 11) hours. - Increasing time to diagnosis of nonconvulsive seizures is associated with increased mortality (Young GB, et al. Neurology 1996;47:83-89.) Most (53%) electrographic seizures on ceeg are evident in the first 30 minutes of the recording 27
28 Survival and Good Neurologic Outcomes Same subject Electrographic Seizures GPEDS NCSE Survival Good Outcome 1/17 (6%) 0/17 (0%) 1/17 (6%) 1/8 (13%) 0/17 (0%) 0/8 (0%) Triphasic Waves 0/1 (0%) 0/1 (0%) BS MSE Epileptiform Discharges 5/42 (12%) 0/18 (0%) 3/42 (7%) 0/18 (0%) 5/38 (13%) 1/38 (3%) MRI 28
29 MRI Literature limited to small cohorts Diffusion Weighted Imaging (DWI) may allow quantification of injured brain One study noted that all survivors lacked temporal and parietal lobe injuries - Jarnum. Resuscitation 2009;80:
 Good Outcome 15/47 (32%) MRI median 61 (IQR 34-97) hours Normal 10/47 (21%) Chronic")
30 Bad Brain? Basal Ganglia Infarcts Watershed Infarcts Comatose after day 2 Yes Our Local Experience Survival 28/47 (60%) Good Outcome 15/47 (32%) MRI median 61 (IQR 34-97) hours Normal 10/47 (21%) Chronic Changes 17/47 (36%) Survive 8/10 (80%; 95%CI %) 12/17 (71%; 95%CI %) Good Outcome 6/10 (60%; 95%CI %) 4/17 (24%; 95%CI %) 8/14 (40%; 95%CI %) Acute Changes 14/39 (36%) 5/14 (25%; 95%CI %) 30



31 SSEP SSEP: Median Nerve Electrical Stimulation Picture from Rothstein
32 SEP- Short Latency Cortical Response (N20) Somatosensory Evoked Potential (SSEP) Determines presence of cortical response (N20) to peripheral stimuli Absence of N20 highly predictive of no cortical recovery - Bedside test - Not affected by most drugs (exception is midazolam) - Hypothermia does not abolish N20 until T<~20ºC - However, presence of N20 does not guarantee good recovery 32
 awaken - 95% CI (0-1.")
33 SSEP after Cardiac Arrest Normal N20 Absent N20 Left Right Rothstein 2004 Jorgensen 2006 SSEP and Outcome Absent N20 performed >24 hours post-cpr has strong association with not awakening in literature - 0/249 (0%) awaken - 95% CI (0-1.5%) Present N20 does not necessarily mean good outcome / 438 (32%) awaken - 95% CI (28-37%) All data are prehypothermia Zandbergen 1998; Zanbergen
34 A Case Report 43 year old male, asystolic arrest. Received hypothermia Day 3: intact pupils, no response to pain. Absent N20 response bilaterally Survived and awoke Leithner. Neurology 2010;74: N20 Response Normal Response No Response 34
35 Serum Biomarkers Serum Biomarkers of Injury Serum NSE of >33ug/L at 72 hours predicts poor outcome (pre-hypothermia) - Zandbergen. Neurology 2006;66:62-8. Serum NSE >25ug/L at 48 hours predicts poor outcome (hypothermic and normothermic patients) - Tiainen. Stroke 2003;34: Small sample size 35
36 NSE in a larger group 90 patients receiving hypothermia Increase in NSE of 6.4 ug/l between hours was 100% specific in predicting poor outcome. - Oksanen T. Resuscitation 2009;80: Prediction of outcome following cardiac arrest is difficult Early predictors - CT with G:W ratio of <1.2 appears to be predictive of death - Seizures portend poor outcome Late predictors (72+ hours) - Absent pupil or corneal response - Absent bilateral N20 on SSEP - Increasing NSE (but not an absolute value!) 36


37 Acknowledgements Clif Callaway, MD, PhD Frank Guyette, MD, MPH Ankur Doshi, MD Jestin Carlson, MD Rene Alvarez, MD Samuel Tisherman, MD Richard Brenner, MD Alexandra Popescu, MD Emanuel Kanal, MD Miguel Habeych, MD Margo Holm, PhD Dave Hostler, PhD James Menegazzi, PhD Ron Roth, MD Mark Pinchalk, EMT-P, MS Curt Niel, EMT-P 37
Neurological Prognosis after Cardiac Arrest Guideline
 Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
Neurological Prognosis after Cardiac Arrest Guideline I. Associated Guidelines and Appendices 1. Therapeutic Hypothermia after Cardiac Arrest 2. Hypothermia after Cardiac Arrest Algorithm II. Rationale
ALS 713: Prognostication in Normothermia
 ALS 713: Prognostication in Normothermia TFQO: Clifton Callaway (COI #214) EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35) Taskforce: ALS COI Disclosure (specific to this systematic review)
ALS 713: Prognostication in Normothermia TFQO: Clifton Callaway (COI #214) EVREVs: Claudio Sandroni (COI #134); Tobias Cronberg (COI #35) Taskforce: ALS COI Disclosure (specific to this systematic review)
Post-Cardiac Arrest Syndrome. MICU Lecture Series
 Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Post-Cardiac Arrest Syndrome MICU Lecture Series Case 58 y/o female collapses at home, family attempts CPR, EMS arrives and notes VF, defibrillation x 3 with return of spontaneous circulation, brought
Neuroprognostication after cardiac arrest
 Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Neuroprognostication after cardiac arrest Sam Orde 1st May 2018 Set the scene 55 yo man, found collapsed in park, looks like he d been jogging, no pulse, bystander CPR, ambulance arrives 5 mins later,
Case: 65 year old post-cardiac arrest patient with myoclonus
 Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Case: 65 year old post-cardiac arrest patient with myoclonus David B. Seder MD, FCCP, FCCM, FNCS Associate Professor of Medicine Tufts University School of Medicine Interim Department Chief and Director
Frank Guyette, MD, MS, MPH Jon Rittenberger, MD, MSc Cliff Callaway, MD, PhD University of Pittsburgh Department of Emergency Medicine
 Frank Guyette, MD, MS, MPH Jon Rittenberger, MD, MSc Cliff Callaway, MD, PhD University of Pittsburgh Department of Emergency Medicine Disclosures Philips Healthcare: Faculty Learning Objectives Upon completion
Frank Guyette, MD, MS, MPH Jon Rittenberger, MD, MSc Cliff Callaway, MD, PhD University of Pittsburgh Department of Emergency Medicine Disclosures Philips Healthcare: Faculty Learning Objectives Upon completion
Post-Arrest Care: Beyond Hypothermia
 Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
Post-Arrest Care: Beyond Hypothermia Damon Scales MD PhD Department of Critical Care Medicine Sunnybrook Health Sciences Centre University of Toronto Disclosures CIHR Physicians Services Incorporated Main
UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN (865) LABEL
 LABEL") 1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
1003 UNIVERSITY OF TENNESSEE HOSPITAL 1924 Alcoa Highway * Knoxville, TN 37920 (865) 544-9000 LABEL Knoxville Neurology Clinic Orders and Progress tes : NAME: MED REC#: PHYSICIAN: DATE: DATE PHYSICIAN'S
Controversies in Post Resuscitation After Cardiac Arrest
 Controversies in Post Resuscitation After Cardiac Arrest More News About Gainesville FL.. 124,354 souls 2007 Best place to live and play in USA 2009 UF ranked #1 party school Andrea Gabrielli, MD FCCM
Controversies in Post Resuscitation After Cardiac Arrest More News About Gainesville FL.. 124,354 souls 2007 Best place to live and play in USA 2009 UF ranked #1 party school Andrea Gabrielli, MD FCCM
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center
 Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Neurological Prognostication After Cardiac Arrest Murad Talahma, M.D. Neurocritical Care Ochsner Medical Center Financial Disclosure None 1 Introduction Each year, 356,000 Americans are treated by EMS
Post-anoxic status epilepticus and EEG patterns
 Post-anoxic status epilepticus and EEG patterns Nicolas Gaspard, MD, PhD Université Libre de Bruxelles Hôpital Erasme, Bruxelles, Belgique Yale University School of Medicine, New Haven, CT, USA DISCLOSURES
Post-anoxic status epilepticus and EEG patterns Nicolas Gaspard, MD, PhD Université Libre de Bruxelles Hôpital Erasme, Bruxelles, Belgique Yale University School of Medicine, New Haven, CT, USA DISCLOSURES
In-hospital Care of the Post-Cardiac Arrest Patient. David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine
 In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
In-hospital Care of the Post-Cardiac Arrest Patient David A. Pearson, MD, FACEP, FAAEM Associate Program Director Department of Emergency Medicine Disclosures I have no financial interest, arrangement,
Disclosures. Pediatrician Financial: none Volunteer :
 Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
Therapeutic Hypothermia: 2011 Research Update. Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine
 Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Therapeutic Hypothermia: 2011 Research Update Richard R. Riker MD, FCCM Chest Medicine Associates South Portland, Maine Agenda NMBA, Sedation, and Shivering Seizures Prognostication Early = Staging Late
Med 536 Communicating About Prognosis Workshop. Case 1
 Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Med 536 Communicating About Prognosis Workshop Case 1 ID / CC: 39 year-old woman status-post motor-vehicle collision History of the Presenting Illness Previously healthy 39 year-old woman was found in
Subhairline EEG Part II - Encephalopathy
 Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Subhairline EEG Part II - Encephalopathy Teneille Gofton September 2013 Objectives To review the subhairline EEG changes seen with encephalopathy To discuss specific EEG findings in encephalopathy To outline
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Predicting neurological outcome and survival after cardiac arrest
 Predicting neurological outcome and survival after cardiac arrest Andy Temple MB ChB FRCA FFICM Richard Porter MB ChB FRCA Matrix reference 2C01, 2C04 Key points Accurately predicting neurological outcome
Predicting neurological outcome and survival after cardiac arrest Andy Temple MB ChB FRCA FFICM Richard Porter MB ChB FRCA Matrix reference 2C01, 2C04 Key points Accurately predicting neurological outcome
How to Improve Cardiac Arrest Survival in your Center
 How to Improve Cardiac Arrest Survival in your Center Ankur A. Doshi, MD FACEP Post Cardiac Arrest Service UPMC Presbyterian Department of Emergency Medicine University of Pittsburgh School of Medicine
How to Improve Cardiac Arrest Survival in your Center Ankur A. Doshi, MD FACEP Post Cardiac Arrest Service UPMC Presbyterian Department of Emergency Medicine University of Pittsburgh School of Medicine
1/29/2014. Kimberly Johnson Hatchett, MD PGY-4 11/15/13
 Kimberly Johnson Hatchett, MD PGY-4 11/15/13 History of Present Illness 14 month old previously healthy infant boy presented via EMS after being found by his mother to be breathing loudly and non-responsive.
Kimberly Johnson Hatchett, MD PGY-4 11/15/13 History of Present Illness 14 month old previously healthy infant boy presented via EMS after being found by his mother to be breathing loudly and non-responsive.
Myoclonic status epilepticus in hypoxic ischemic encephalopathy which recurred after somatosensory evoked potential testing
 ANNALS OF CLINICAL NEUROPHYSIOLOGY CASE REPORT Ann Clin Neurophysiol 2017;19(2):136-140 Myoclonic status epilepticus in hypoxic ischemic encephalopathy which recurred after somatosensory evoked potential
ANNALS OF CLINICAL NEUROPHYSIOLOGY CASE REPORT Ann Clin Neurophysiol 2017;19(2):136-140 Myoclonic status epilepticus in hypoxic ischemic encephalopathy which recurred after somatosensory evoked potential
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
4/12/2016. Seizure description Basic EEG ICU monitoring Inpatient Monitoring Elective admission for continuous EEG monitoring Nursing s Role
 Kathleen Rieke, MD Chari Ahrenholz Curt Devos Understand why continuous EEG is being requested in certain patient populations Understand what the EEG can tell us about our patient. Understand nursing role
Kathleen Rieke, MD Chari Ahrenholz Curt Devos Understand why continuous EEG is being requested in certain patient populations Understand what the EEG can tell us about our patient. Understand nursing role
Multimodal monitoring to prognosticate in anoxic brain injury
 Multimodal monitoring to prognosticate in anoxic brain injury Eyal Golan, MD FRCPC PhD(c) Critical Care & Neurosciences Critical Care Medicine Interdepartmental Division of Critical Care and Department
Multimodal monitoring to prognosticate in anoxic brain injury Eyal Golan, MD FRCPC PhD(c) Critical Care & Neurosciences Critical Care Medicine Interdepartmental Division of Critical Care and Department
The Evidence Base. Stephan A. Mayer, MD. Columbia University New York, NY
 Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
Hypothermic for Cardiac Arrest The Evidence Base Stephan A. Mayer, MD Director, Neuro-ICU Columbia University New York, NY Disclosures Columbia University Clinical Trials Pilot Award Radiant Medical, Inc.
5 Key EMS Articles for 2012
 5 Key EMS Articles for 2012 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN 5 Key Topics Cardiac Arrest Trauma
5 Key EMS Articles for 2012 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN 5 Key Topics Cardiac Arrest Trauma
Post-resuscitation care for adults. Jerry Nolan Royal United Hospital Bath
 Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
Post-resuscitation care for adults Jerry Nolan Royal United Hospital Bath Post-resuscitation care for adults Titration of inspired oxygen concentration after ROSC Urgent coronary catheterisation and percutaneous
WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre
 Claudio Sandroni, Giuseppe La Torre") Worksheet No. ALS-PA-041.doc Page 1 of 16 WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre Date Submitted for review: 27
Worksheet No. ALS-PA-041.doc Page 1 of 16 WORKSHEET for Evidence-Based Review of Science for Emergency Cardiac Care Worksheet author(s) Claudio Sandroni, Giuseppe La Torre Date Submitted for review: 27
Resuscitation 82 (2011) Contents lists available at ScienceDirect. Resuscitation
 Contents lists available at ScienceDirect. Resuscitation") Resuscitation 82 (2011) 1399 1404 Contents lists available at ScienceDirect Resuscitation jo u rn al hom epage : www.elsevier.com/locate/resuscitation Clinical paper An early, novel illness severity score
Resuscitation 82 (2011) 1399 1404 Contents lists available at ScienceDirect Resuscitation jo u rn al hom epage : www.elsevier.com/locate/resuscitation Clinical paper An early, novel illness severity score
IN HOSPITAL CARDIAC ARREST AND SEPSIS
 IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
IN HOSPITAL CARDIAC ARREST AND SEPSIS MARGARET DISSELKAMP, MD OVERVIEW Background Epidemiology of in hospital cardiac arrest (IHCA) Use a case scenario to introduce new guidelines Review surviving sepsis
Electroencephalography. Role of EEG in NCSE. Continuous EEG in ICU 25/05/59. EEG pattern in status epilepticus
 EEG: ICU monitoring & 2 interesting cases Electroencephalography Techniques Paper EEG digital video electroencephalography Dr. Pasiri Sithinamsuwan PMK Hospital Routine EEG long term monitoring Continuous
EEG: ICU monitoring & 2 interesting cases Electroencephalography Techniques Paper EEG digital video electroencephalography Dr. Pasiri Sithinamsuwan PMK Hospital Routine EEG long term monitoring Continuous
The Theraputic Role of Hypothermia
 The Theraputic Role of Hypothermia Sharie Bennett R.EEG/EP T 10/2/2014 1 Hypothermia Objectives: Therapeutic benefits of Hypothermia The role of Neurodiagnostics in Hypothermia Monitoring 10/2/2014 2 Hypothermia
The Theraputic Role of Hypothermia Sharie Bennett R.EEG/EP T 10/2/2014 1 Hypothermia Objectives: Therapeutic benefits of Hypothermia The role of Neurodiagnostics in Hypothermia Monitoring 10/2/2014 2 Hypothermia
CHILL OUT! Induced Hypothermia: Challenges & Successes in the
 CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
CHILL OUT! Induced Hypothermia: Challenges & Successes in the ICU Colleen Bell RN, BS, CCRN, Donna Brault RN, BSN, CCRN, Cathy Patnode RN, BSN, CCRN Champlain Valley Physician Hospital November 2012 Objectives
Post-resuscitation Care
 Post-resuscitation Care Kyu-Nam Park Department of Emergency Medicine. St. Mary s Hospital. Catholic University of Korea Dr.James R Jude, Dr. William Kouwenhoven, Dr.G Guy Knickerbocker at Johns Hopkins
Post-resuscitation Care Kyu-Nam Park Department of Emergency Medicine. St. Mary s Hospital. Catholic University of Korea Dr.James R Jude, Dr. William Kouwenhoven, Dr.G Guy Knickerbocker at Johns Hopkins
BRAIN DYSFUNCTION DURING SEPSIS When and how should we monitor the brain in sepsis?
 BRAIN DYSFUNCTION DURING SEPSIS When and how should we monitor the brain in sepsis? andrea.polito@rpc.aphp.fr University of Versailles Raymond Poincaré Teaching Hospital Garches - France SEPTIC PATIENTS
BRAIN DYSFUNCTION DURING SEPSIS When and how should we monitor the brain in sepsis? andrea.polito@rpc.aphp.fr University of Versailles Raymond Poincaré Teaching Hospital Garches - France SEPTIC PATIENTS
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Cardio Pulmonary Cerebral Resuscitation
 Cardio Pulmonary Cerebral Resuscitation Brain Under Pressure October 3, 2017 Canadian Critical Care Forum Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto
Cardio Pulmonary Cerebral Resuscitation Brain Under Pressure October 3, 2017 Canadian Critical Care Forum Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto
Mild therapeutic hypothermia
 Neurologic Critical Care Continuous electroencephalography monitoring for early prediction of neurological outcome in postanoxic patients after cardiac arrest: A prospective cohort study* Marleen C. Cloostermans,
Neurologic Critical Care Continuous electroencephalography monitoring for early prediction of neurological outcome in postanoxic patients after cardiac arrest: A prospective cohort study* Marleen C. Cloostermans,
Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus
 Clinical commentary Epileptic Disord 2012; 14 (3): 340-4 Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus Jemeen Sreedharan
Clinical commentary Epileptic Disord 2012; 14 (3): 340-4 Falsely pessimistic prognosis by EEG in post-anoxic coma after cardiac arrest: the borderland of nonconvulsive status epilepticus Jemeen Sreedharan
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017
 Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
Prehospital Post Arrest Care AHA Strive to Revive 2017 November 3, 2017 Jon Rittenberger, MD, MS Department of University of Pittsburgh Employers: Disclosures - Rittenberger University of Pittsburgh UPMC
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO
 TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
TOO COOL OR NOT TOO COOL- THERAPEUTIC HYPOTHERMIA IN THE ICU SCCM TX 2017 TED WU MD PEDIATRIC CRITICAL CARE UNIVERSITY OF TEXAS HEALTH SAN ANTONIO DISCLOSURE I have no relationships with commercial companies
Med 536 Communicating About Prognosis Workshop. Case 2
 Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Med 536 Communicating About Prognosis Workshop Case 2 ID / CC: 33 year-old man with intracranial hemorrhage History of the Presenting Illness 33 year-old man with a prior history of melanoma of the neck
Generalized seizures, generalized spike-waves and other things. Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke
 Generalized seizures, generalized spike-waves and other things Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke Objectives Give an overview of generalized EEG discharges and seizures
Generalized seizures, generalized spike-waves and other things Charles Deacon MD FRCPC Centre Hospitalier Universitaire de Sherbrooke Objectives Give an overview of generalized EEG discharges and seizures
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
The Role of EEG After Cardiac Arrest and Hypothermia
 Current Literature In Clinical Science The Role of EEG After Cardiac Arrest and Hypothermia Continuous EEG in Therapeutic Hypothermia After Cardiac Arrest: Prognostic and Clinical Value. Crepeau AZ, Rabinstein
Current Literature In Clinical Science The Role of EEG After Cardiac Arrest and Hypothermia Continuous EEG in Therapeutic Hypothermia After Cardiac Arrest: Prognostic and Clinical Value. Crepeau AZ, Rabinstein
Curricullum Vitae. Dr. Isman Firdaus, SpJP (K), FIHA
, FIHA") Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
Curricullum Vitae Dr. Isman Firdaus, SpJP (K), FIHA Email: ismanf@yahoo.com Qualification : o GP 2001 (FKUI) o Cardiologist 2007 (FKUI) o Cardiovascular Intensivist 2010 - present o Cardiovascular Intervensionist
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Enhancing patient care in the ICU with NeuroMonitoring
 Enhancing patient care in the ICU with NeuroMonitoring In the ICU, several patient vital signs are monitored continuously. But what about the brain? Hemodynamics Heart rate Non invasive blood pressure
Enhancing patient care in the ICU with NeuroMonitoring In the ICU, several patient vital signs are monitored continuously. But what about the brain? Hemodynamics Heart rate Non invasive blood pressure
State of the art lecture: 21st Century Post resuscitation management
 State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
State of the art lecture: 21st Century Post resuscitation management ACCA Masterclass 2017 Prof Alain CARIOU Intensive Care Unit - Cochin Hospital (APHP) Paris Descartes University INSERM U970 - France
Scope. EEG patterns in Encephalopathy. Diffuse encephalopathy. EEG in adult patients with. EEG in diffuse encephalopathy
 Scope EEG patterns in Encephalopathy Dr.Pasiri Sithinamsuwan Division of Neurology Department of Medicine Phramongkutklao Hospital Diffuse encephalopathy EEG in specific encephalopathies Encephalitides
Scope EEG patterns in Encephalopathy Dr.Pasiri Sithinamsuwan Division of Neurology Department of Medicine Phramongkutklao Hospital Diffuse encephalopathy EEG in specific encephalopathies Encephalitides
Neurological prognostication after cardiac arrest and targeted temperature management
 Neurological prognostication after cardiac arrest and targeted temperature management Dragancea, Irina Published: 2016-01-01 Document Version Publisher's PDF, also known as Version of record Link to publication
Neurological prognostication after cardiac arrest and targeted temperature management Dragancea, Irina Published: 2016-01-01 Document Version Publisher's PDF, also known as Version of record Link to publication
x = ( A) + (3.296 B) (0.070 C) (1.006 D) + (2.426 E) Receiver Operating Characteristic ROC
 + (3.296 B) (0.070 C) (1.006 D) + (2.426 E) Receiver Operating Characteristic ROC") 7 1... 4. 5. 6. 7. 8. 9. 1. 000 1 01 11 006 01 1 11 6 Glasgow outcome scale GOS GOS 4 n=477 55 A C D 5 ph B E = 1/(1 + e x) x = ( 0.0 A) + (.96 B) (0.070 C) (1.006 D) + (.46 E) 19.489 estimated probability
7 1... 4. 5. 6. 7. 8. 9. 1. 000 1 01 11 006 01 1 11 6 Glasgow outcome scale GOS GOS 4 n=477 55 A C D 5 ph B E = 1/(1 + e x) x = ( 0.0 A) + (.96 B) (0.070 C) (1.006 D) + (.46 E) 19.489 estimated probability
Respiratory Care and Organ Donation
 Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Respiratory Care and Organ Donation Whitni Noyes, RN, OPTC Midwest Transplant Network Midwest Transplant Network CMS requires every accredited hospital to have an agreement with an OPO. MTN is the first
Caring For the ICU Boarder. Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM
 Caring For the ICU Boarder Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM I have no relevant financial relationships with the manufacturer(s) of any commercial product(s)and/or
Caring For the ICU Boarder Kami M. Hu, MD Depts of Emergency & Internal Medicine University of Maryland SOM I have no relevant financial relationships with the manufacturer(s) of any commercial product(s)and/or
Predicting Outcomes in HIE. Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016
 Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Predicting Outcomes in HIE Naaz Merchant Consultant Neonatologist Beds & Herts Meeting 17/03/2016 Interactive please! Case 1 Term, 3.5 kg Antenatal: Breech Labour/Delivery: Em CS failure to progress, mec
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest
 Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Targeted Temperature Management: An Evolving Therapy for Cardiac Arrest By Meagan Dunn, BScN, MSc,, RN, CNE NP Forum April 8, 2016 Objectives To understand: What Therapeutic Temperature Management (TTM)
Brain Death Determination: Outline. Definition. Brain Death Determination. Brain Death Determination. No conflict of interest
 No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
Regionalization of Post-Cardiac Arrest Care
 Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Regionalization of Post-Cardiac Arrest Care David A. Pearson, MD, FACEP, FAAEM Department of Emergency Medicine Disclosures I have no financial interest, arrangement, or affiliations and no commercial
Mild. Moderate. Severe. 32 to to and below
 Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
Mohamud Daya MD, MS Mild 32 to 34 Moderate 28 to 32 Severe 28 and below Jon Rittenberger Shervin Ayati Protocol Development Committee Hypothermia Working Group Lynn Wittwer Jon Jui John Stouffer Scott
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Patient Case. Post cardiac arrest pathophysiology 10/19/2017. Disclosure. Objectives. Patient Case-TM
 Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Disclosure TARGETED TEMPERATURE MANAGEMENT POST CARDIAC ARREST I have nothing to disclose concerning possible financial or personal relationships with commercial entities that may have a direct or indirect
Post Cardiac Arrest Care. From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
 Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
Post Cardiac Arrest Care From : 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Initial Objectives of Post cardiac Arrest Care Optimize cardiopulmonary
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Advanced airway placement (ETT vs SGA)
") Advanced airway placement (ETT vs SGA) Among adults who are in cardiac arrest in any setting (P), does tracheal tube insertion as first advanced airway (I), compared with insertion of a supraglottic airway
Advanced airway placement (ETT vs SGA) Among adults who are in cardiac arrest in any setting (P), does tracheal tube insertion as first advanced airway (I), compared with insertion of a supraglottic airway
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol
 Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Alex Manara Regional Clinical Lead in Organ Donation South West Region Frenchay Hospital, Bristol Diagnosis of Death Masterclass 2. Increased diagnosis of brain stem death 3. Increased donation after cardiac
Common EEG pattern in critical care
 Common EEG pattern in critical care พ.ญ.ส ธ ดา เย นจ นทร Causes Direct neuronal injury Cerebral dysfunction : encephalopathy Psychic problems EEG in critical care 1 October 2009, Pramongkutklao Hospital
Common EEG pattern in critical care พ.ญ.ส ธ ดา เย นจ นทร Causes Direct neuronal injury Cerebral dysfunction : encephalopathy Psychic problems EEG in critical care 1 October 2009, Pramongkutklao Hospital
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest
 ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
ECG Changes in Patients Treated with Mild Hypothermia after Cardio-pulmonary Resuscitation for Out-of-hospital Cardiac Arrest R. Schneider, S. Zimmermann, W.G. Daniel, S. Achenbach Department of Internal
New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto
 New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto COI Declaration Industry and ROC ALS Taskforce ILCOR Author
New ACLS/Post Arrest Guidelines: For Everyone? Laurie Morrison, Li Ka Shing, Knowledge Institute, St Michael s Hospital, University of Toronto COI Declaration Industry and ROC ALS Taskforce ILCOR Author
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
Queen Charlotte Hospital
 Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Queen Charlotte Hospital Neuroprotection for neonatal encephalopathy Neonatal encephalopathy accounts for 1 million deaths worldwide and even greater numbers of disabled survivors In countries with
Author Manuscript Faculty of Biology and Medicine Publication
 Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
Serveur Académique Lausannois SERVAL serval.unil.ch Author Manuscript Faculty of Biology and Medicine Publication This paper has been peer-reviewed but does not include the final publisher proof-corrections
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on Needed to be resuscitated at birth
 No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
No social problems noted No past med hx Mother had spontaneous rupture of fetal membranes SB born on 9-16-2011 Needed to be resuscitated at birth (included assisted vent) Had generalized edema and possible
Hypothermia: The Science and Recommendations (In-hospital and Out)
") Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hypothermia: The Science and Recommendations (In-hospital and Out) L. Kristin Newby, MD, MHS Professor of Medicine Duke University Medical Center Chair, Council on Clinical Cardiology, AHA President, Society
Hospital of the University of Pennsylvania POLICY MANUAL
 Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
Page 1 of 8 KEY WORDS: Brain Death Coma # 1-6-11 Procedures Following Patient Death # 1-6-13 Organ Donation and Anatomical Donation and Pennsylvania s Anatomical Gift Act #1-6-17 Withholding and Withdrawing
한국학술정보. Key Words: Seizures, Prognosis, Out-of-hospital Cardiac Arrest
 Relevance of Seizure with Mortality and Neurologic Prognosis of Out of Hospital Cardiopulmonary Arrest (OHCA) Patients Who had Treated with Therapeutic Hypothermia after Return of Spontaneous Circulation
Relevance of Seizure with Mortality and Neurologic Prognosis of Out of Hospital Cardiopulmonary Arrest (OHCA) Patients Who had Treated with Therapeutic Hypothermia after Return of Spontaneous Circulation
Presenter Disclosure
 Presenter Disclosure Presenter s name: Wanida Nuwisait, Department of Physiology, Faculty of Medicine, University of Toronto I do not have an affiliation (financial or otherwise) with a commercial organization
Presenter Disclosure Presenter s name: Wanida Nuwisait, Department of Physiology, Faculty of Medicine, University of Toronto I do not have an affiliation (financial or otherwise) with a commercial organization
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
PEDIATRIC POST CARDIAC ARREST
 PEDIATRIC POST CARDIAC ARREST ALGORITHM Cardiac arrest with ROSC CPR > 1 min Initial neurologic exam Assess level of consciousness Evaluate for asymmetric neurologic exam (consider early brain CT if exam
PEDIATRIC POST CARDIAC ARREST ALGORITHM Cardiac arrest with ROSC CPR > 1 min Initial neurologic exam Assess level of consciousness Evaluate for asymmetric neurologic exam (consider early brain CT if exam
Jennifer Accardo, 1 Domenico De Lisi, 2 Paola Lazzerini, 3 and Alberto Primavera Introduction. 2. Case Report
 Case Reports in Neurological Medicine Volume 2013, Article ID 872127, 5 pages http://dx.doi.org/10.1155/2013/872127 Case Report Good Functional Outcome after Prolonged Postanoxic Comatose Myoclonic Status
Case Reports in Neurological Medicine Volume 2013, Article ID 872127, 5 pages http://dx.doi.org/10.1155/2013/872127 Case Report Good Functional Outcome after Prolonged Postanoxic Comatose Myoclonic Status
Beyond the Golden Hour: Caring for the ICU Boarder
 Beyond the Golden Hour: Caring for the ICU Boarder Kami M. Hu, MD Dept. of Emergency Medicine Dept. of Pulmonology & Critical Care University of Maryland SOM I have no relevant financial relationships
Beyond the Golden Hour: Caring for the ICU Boarder Kami M. Hu, MD Dept. of Emergency Medicine Dept. of Pulmonology & Critical Care University of Maryland SOM I have no relevant financial relationships
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC
, RN, RNC-NIC") Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
Hypothermia in Neonates with HIE TARA JENDZIO, DNP(C), RN, RNC-NIC Objectives 1. Define Hypoxic-Ischemic Encephalopathy (HIE) 2. Identify the criteria used to determine if an infant qualifies for therapeutic
INDUCED HYPOTHERMIA A Hot Topic. R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences
 INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
INDUCED HYPOTHERMIA A Hot Topic R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Health Sciences Conflicts of Interest Sadly, we have no financial or industrial conflicts of interest
CARES Targeted Temperature Management (TTM) Module
 Module") CARES Targeted Temperature Management (TTM) Module OHCA Data Dictionary June 2014 1 CASE NUMBER This is the number assigned to the patient by the hospital. The case number is the number the hospital assigns
CARES Targeted Temperature Management (TTM) Module OHCA Data Dictionary June 2014 1 CASE NUMBER This is the number assigned to the patient by the hospital. The case number is the number the hospital assigns
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
What Hospitalists Need to Know about ICU Neurology
 What Hospitalists Need to Know about ICU Neurology S. Andrew Josephson, MD Department of Neurology, Neurovascular Service University of California San Francisco September 25, 2009 The speaker has no disclosures
What Hospitalists Need to Know about ICU Neurology S. Andrew Josephson, MD Department of Neurology, Neurovascular Service University of California San Francisco September 25, 2009 The speaker has no disclosures
Cardiac Arrest January 2017 CPR /3/ Day to Survival Propensity Matched
 Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Cardiac Arrest January 217 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN CPR 217 Used data based on protocol that
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
NIH Public Access Author Manuscript Pediatr Neurol. Author manuscript; available in PMC 2014 December 03.
 NIH Public Access Author Manuscript Published in final edited form as: Pediatr Neurol. 2014 November ; 51(5): 663 668.e2. doi:10.1016/j.pediatrneurol.2014.07.026. Neuroprognostication After Pediatric Cardiac
NIH Public Access Author Manuscript Published in final edited form as: Pediatr Neurol. 2014 November ; 51(5): 663 668.e2. doi:10.1016/j.pediatrneurol.2014.07.026. Neuroprognostication After Pediatric Cardiac
Lesson learnt from big trials. Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ.
 Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Drowning is a leading cause of death and loss of years of life with over 90% of cases occurring in lower- and middle-income countries.
 Chapter 145 Drowning Episode Overview: 1) List risk factors for drowning 2) List 5 variables that portend poor outcome 3) Describe the diving reflex 4) Describe the management of a drowning patient with
Chapter 145 Drowning Episode Overview: 1) List risk factors for drowning 2) List 5 variables that portend poor outcome 3) Describe the diving reflex 4) Describe the management of a drowning patient with
Targeted temperature management after post-anoxic brain insult: where do we stand?
 Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Targeted temperature management after post-anoxic brain insult: where do we stand? Alain Cariou Intensive Care Unit Cochin University Hospital Paris Descartes University INSERM U970 (France) COI Disclosure
Altered Mental Status
 Karl Sporer,MD FACEP, FACP Clinical Professor UCSF High Risk Emergency Medicine Patients over 65 25% will have some form of AMS Unknown Economic Impact Wilber ST. Altered mental status in older emergency
Karl Sporer,MD FACEP, FACP Clinical Professor UCSF High Risk Emergency Medicine Patients over 65 25% will have some form of AMS Unknown Economic Impact Wilber ST. Altered mental status in older emergency
Take A Breath: Pulmonary Management of the Organ Donor. Whitni Noyes, RN, CPTC Midwest Transplant Network
 Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
Take A Breath: Pulmonary Management of the Organ Donor Whitni Noyes, RN, CPTC Midwest Transplant Network Objectives Recognize MTN referral criteria. Be familiar with the apnea test for brain death pronouncement.
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM
 ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
0 56 BiPLEDS 3 (L:2, O:1), 9
, 9") Supplementary Table 1. Demographics and clinical characteristics of the patients. CSF Sex/Age Prodrome CSF WBC Protein Patient 1 M/23 Patient 2 M/20 Patient 3 F/27 Patient 4 F/38 3 days headache, 1 day
Supplementary Table 1. Demographics and clinical characteristics of the patients. CSF Sex/Age Prodrome CSF WBC Protein Patient 1 M/23 Patient 2 M/20 Patient 3 F/27 Patient 4 F/38 3 days headache, 1 day
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL
 YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual