Pituitary Disease Resident Tutorial 2017
|
|
|
- Tracy Evans
- 5 years ago
- Views:
Transcription



1 Pituitary Disease Resident Tutorial 2017 Sarat Sunthornyothin MD Division of Endocrinology and Metabolism King Chulalongkorn Memorial Hospital Pituitary Anatomy hypophyseal portal system direct arterial supply from int. carotid a. 1. Sup. hypophyseal a. 2. Inf. hypophyseal a. Pituitary Gland Pituita (latin) = phlegm JAMA Feb 7;317(5):


2 Control of Pituitary Hormones Pituitary Imaging Sellar Masses Pituitary tumor Functioning pituitary adenoma Prolactin, GH, Cushing s, TSH, gonadotroph Non functioning pituitary adenoma Null cell adenoma, gonadotroph Pituitary carcinoma Other mass lesions Rathke s Cyst Craniopharyngioma Metastases Hypophysitis Meningioma 2
3 Pituitary Apoplexy Greek : apoplexia : (ἀποπληξία) to strike Sudden impairment of brain function Pituitary : pituita : phlegm It was believed in the 1500's and 1600's that the pituitary gland channeled mucus to the nose Clinical syndrome consisting of a constellation of signs and symptoms that occur with rapid expansion of the contents of the sella turcica *** CLINICAL DIAGNOSIS *** Pituitary Apoplexy Pituitary apoplexy is a clinical syndrome due to abrupt hemorrhaging and/or infarction of the pituitary gland, generally within a pituitary adenoma. prevalence : 6.2 per 100,000 Incidence: 0.17 per 100,000 per year 2% and 12% of patients with adenoma 45% non functioning adenoma Most common: 5 th 6 th decade male preponderance ( : 1) 26% with precipitating factors Endocrine Reviews, December 2015, 36(6): Pituitary Apoplexy: Precipitating factors Conditions Head trauma Hypotension Medications Anticoagulants Dopamine agonist Procedures Angiography esp. cerebral angiogram Surgery (cardiac and orthopedic surgery) Pituitary dynamic testing TRH / GnRH/ GHRH/ CRH stimulation test Insulin induced hypoglycemia Others History of irradiation History of hypertension intra or postoperative hypotension, cardiopulmonary bypass, anticoagulation and/or microemboli leading to infarction imbalance between the increased metabolic demand induced by the stimulation and the ability of increased blood flow at the level of the pituitary adenoma 3
4 Clinical Manifestations Headache of sudden and severe onset like a thunderclap in a clear sky Dural traction meningeal irritation from extravasation of blood and necrotic material into the subarachnoid space usually retroorbital but can be bifrontal or diffuse Hormonal deficits * Adrenal insufficiency * Chronic Hypothyroid from pre existing pituitary lesions Hormonal excess: pre existing functioning pituitary tumor Endocrine Reviews, December 2015, 36(6): Clinical Manifestations Visual disturbances Visual field defect Ocular palsy Subarachnoid hemorrhage Cerebral ischemia : focal neurological deficits mechanical compression of the carotid artery cerebral vasospasm Pituitary Tumor Apoplexy Prolactin may be an indicator of pituitary function recovery Degree / risk of hypopituitarism related to intrasellar pressure 4
5 Pituitary Apoplexy Score (PAS) Clin Endocrinol (Oxf). 2011;74:9 20 (17) Pathophysiology Pituitary apoplexy is mostly associated with pituitary macroadenoma Pituitary adenoma Less blood supply than normal pituitary Reduced angiogenesis and microvasculature pituitary tumor ischemia / infarction Tumor outgrows blood supply Increased fragility of tumor blood vessels Compression of vessels against the sellar diaphragm by the expanding tumor mass MRI Findings Stage Substance T1 T2 Hyperacute (1 2hr) blood Hypo iso Hyper hypo Acute (>3hr) deoxyhb iso Very hypo Subacute (< 1 wk) methb Hyper Focal or heterogeneous Hypo to hyper Chronic (> 1 wk) protein Hyper Hyper Rarely shows pure hemorrhage; usually mixed infarction/ hemorrhagic infarction Thickening of sphenoid mucosal sinus from venous congestion Related to degree of hypopituitarism J Neurosurg. 2006; 104:
6 Hormonal Deficit Corticotropin deficiency: most common deficit (50% 80%) **** empiric parenteral corticosteroid ***** After serum blood draw for cortisol given to all patients with signs of PA, without waiting for diagnostic confirmation Cortisol < 15 mcg/dl : adrenal insufficiency in critical acute settings Pituitary Apoplexy: Treatment No treatment mortality > 50% Clinical suspicious is very important Blood draw for hormone measurement Supportive hemodynamic treatment Glucocorticoid : stress dose (200 mg of hydrocortisone) Imaging study after initial treatment and hemodynamically stable Conservative or Surgery Conservative therapy can be used in selected patients minimal symptoms improve dramatically after administration of glucocorticoids Factors to choose treatment options Patient s presentation clinical stability initial response to glucocorticoids availability of an experienced neurosurgeon Imaging findings single large hypodense area within the tumor on CT might be associated with better subsequent tumor shrinkage than are several small hypodense areas Simple infarction is less severe than hemorrhagic infarct 6
7 Hormonal Management Glucocorticoid preoperative Thyroid hormone if symptomatic or very low DI : not common (10%) and often transient Re evaluate postoperative 2 4 weeks Glucocorticoid may be tested early postop. Thyroid, sex hormone Outcomes after Apoplexy Ocular palsy resolved 75% 100% of patients without surgery, 31% 57% of patients with surgery Visual field defect resolved 50% normalized, 30% improved after Sx Similar outcome in conservative treatment Worse outcome in severe deficit Better outcome if surgery within first week Hormonal deficit Only 20% does not require hormone replacement after apoplexy Similar outcome for surgical and conservative group UK Guideline Apoplexy Clin Endocrinol (Oxf) Jan;74(1):

8 Pituitary Apoplexy : Summary Clinical diagnosis: high degree of suspicion Hydrocortisone therapy as soon as the diagnosis is suspected Conservative treatment is an option Surgery if Severely reduced VA Severe, persistent, deteriorating VF defect Deteriorating level of consciousness Not improved or worsening with conservative treatment Surgery should be performed within first week Pitfalls of Management Delay in diagnosis Delay in hydrocortisone treatment Need patient education for self adjustment of glucocorticoid dose No testosterone replacement How to prescribe IM, transdermal gel, oral How to follow up Testosterone level, CBC, PSA Consult urology PSA increase > 1.4 in first 12 month PSA > 4 Abn. digital rectal exam Hypothalamic Pituiary Control Neuropeptides are released into the specialized blood supply to the pituitary to regulate its secretion 8
:516 524.")
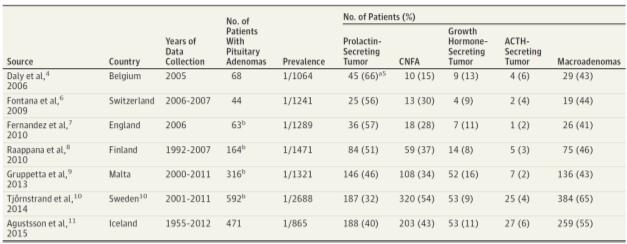
9 Pituitary Adenoma JAMA Feb 7;317(5): Prevalence of Pituitary Adenoma JAMA Feb 7;317(5): Prolactinoma 9

10 Prolactin Regulation Stimulatory TRH, E, EGF Inhibitory Dopamine hypogonadism Prolactin Regulation Predominant effect: Inhibitory Dopaminergic neuron Dopamine D 2 receptor Stimulatory : Prl Releasing Factors Peripheral neural control Hyperprolactinemia inh prolactin Prl inh. Kisspeptin expression Kisspeptin stim GnRH neuron Nat Rev Endocrinol May;11(5):




11 Symptoms of Hyperprolactinemia Female Amenorrhea, Oligomenorrhea infertility Galactorrhea Osteoporosis Male Hypogonadism Gynecomastia Osteoporosis Symptoms from mass effect Visual field defect Apoplexy CN defect CSF rhinorrhea Causes of Hyperprolactinemia Antihistamine Opiate and opiate antagonist Prolactin Measurement Single measurement at any time of the day Avoid excessive venipuncture No need for stimulation test (TRH, L dopa, domperidone) PRL > 500 ng/ml macroprolactinoma PRL > 250 ng/ml usually indicate prolactinoma Some drug induced hyperprl can have PRL > 200 ng/ml Risperidone, metoclopramide Usually drug induced hyperprl; PRL < 100 ng/ml Minimal hyperprolactinemia maybe a prolactinoma, but a non prolactin secreting mass should first be considered 11

12 Prolactin Measurement Nat Clin Pract Endo&Met Mar 2007 Circulating Forms of PRL MACROPROLACTIN Found in 40% of patients with hyperprolactinemia Found in 4% of normal population Galactorrhea 20% oligo/amenorrhea 45% pituitary adenomas 20% 12
 Heterophile Ab Interference Hook Effect")
 Unless using the assay")
13 Heterophile Antibody Interference Heterophile Ab are antibodies induced by external antigens (heterophile Ag) Heterophile Ab Interference Hook Effect Reading can be normal or slightly elevated. Happen in very big tumor (Actual PRL is extremely high) Unless using the assay not affected by this condition: 2 steps method 13
:904 9. Bromocriptine VS Cabergoline N Engl J Med. 1994 Oct 6;331(14):904 9. Presse Med.")
14 Inaccurate Result of Prolactin Falsely high Macroprolactinemia Heterophile antibody Physiologic causes Falsely low Hook effect Heterphile antibody Bromocriptine VS Cabergoline N Engl J Med Oct 6;331(14): Bromocriptine VS Cabergoline N Engl J Med Oct 6;331(14): Presse Med Apr 29;24(16):
, 3 yr (Pituitary Society) Normal serum prolactin No visible tumor remnant on MRI Recurrence")
15 Bromocriptine vs Cabergoline in PRL secreting macroadenoma J Clin Endocrinol Metab Apr;60(4): J Clin Endocrinol Metab Jun;85(6): When to stop DA? Therapy may be tapered and perhaps discontinued treated with dopamine agonists for at least 2 yr (ENDO SOC), 3 yr (Pituitary Society) Normal serum prolactin No visible tumor remnant on MRI Recurrence rate: 26 69% Predicted by initial PRL and tumor size Increase 18% per mm of tumor size Most likely occur in first year Monitor q 3 month during 1 st year then annually Repeat MRI if PRL above UNL Recurrence after DA discontinuation Recurrence is related to PRL level at Dx and before D/C Pituitary dysfunction at Dx Not related to size, DA dose Not related to longer treatment time J Endocrinol Invest May 31 15
16 Women with Asymptomatic Microadenoma YOUNG WOMEN If pregnancy is desired: DA If pregnancy is not desired: DA or OC Microadenoma rarely grows POSTMENOPAUSAL WOMEN DA may be discontinued Monitoring of tumor size increase periodically Drug induced HyperPRL Discontinue medication for 3 days or substitution of an alternative drug, followed by remeasurement of serum prolactin should not be undertaken without consulting the patient s physician. If drug can t be stopped: perform MRI to differentiate drug induced vs. pituitary/hypothalamic lesion if pretreatment PRL is not available Treatment with DA may cause psychosis relapsed! Not common Use estrogen or testosterone in patients with long term hypogonadism (hypogonadal symptoms or low bone mass) 16
Pituitary Tumors and Incidentalomas. Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
 Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Apoplexy. Updated: April 22, 2018 CLINICAL RECOGNITION
 Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Metoclopramide Domperidone. HYPER- PROLACTINAEMIA: the true and the false problems
 Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Hyperprolactinemia: N hidshi i MD. Nahid Shirazian MD. Internist, Endocrinologist
 Diagnosis and Treatment of Hyperprolactinemia: p N hidshi i MD Nahid Shirazian MD. Internist, Endocrinologist An Endocrine Society Clinical Practice Guideline (J Clin Endocrinol Metab 96: 273 288, 2011)
Diagnosis and Treatment of Hyperprolactinemia: p N hidshi i MD Nahid Shirazian MD. Internist, Endocrinologist An Endocrine Society Clinical Practice Guideline (J Clin Endocrinol Metab 96: 273 288, 2011)
Mechanism of hyperprolactinemia
 Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
GLMS CME- Cell Group 5 10 April Greenlane Medical Specialists Pui-Ling Chan Endocrinologist
 GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君
 Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君 Williams text book of endocrinology 11 th e Anterior pituitary hormone 10-20% of pituitary cells, increase to 40% during AP PRL releasing factors: TRH, oxytocin,
Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君 Williams text book of endocrinology 11 th e Anterior pituitary hormone 10-20% of pituitary cells, increase to 40% during AP PRL releasing factors: TRH, oxytocin,
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013
 panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013 PITUITARY GLAND (HYPOPHYSIS CEREBRI) The master of endocrine glands master of endocrine glands It is a small oval
panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013 PITUITARY GLAND (HYPOPHYSIS CEREBRI) The master of endocrine glands master of endocrine glands It is a small oval
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Urgent and Emergent Pituitary Conditions
 Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Sharon maslovitz Lis Maternity Hospital
 Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Medical background Healthy until 24yo
Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Medical background Healthy until 24yo
Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution?
 Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly
 Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly Dr. Peter Igaz MD PhD DSc 2nd Department of Medicine Semmelweis University Fields of Endocrinology Diseases
Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly Dr. Peter Igaz MD PhD DSc 2nd Department of Medicine Semmelweis University Fields of Endocrinology Diseases
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Diseases of pituitary gland
 Diseases of pituitary gland A brief introduction Anterior lobe = adenohypophysis Posterior lobe = neurohypophysis The production of most pituitary hormones is controlled in large part by positively and
Diseases of pituitary gland A brief introduction Anterior lobe = adenohypophysis Posterior lobe = neurohypophysis The production of most pituitary hormones is controlled in large part by positively and
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Imaging pituitary gland tumors
 November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
HYPOTHALAMO PITUITARY GONADAL AXIS
 HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
Imaging The Turkish Saddle. Russell Goodman, HMS III Dr. Gillian Lieberman
 Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Neuroendocrine Disorders in Women
 Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Pituitary Disorders Suranut Charoensri, MD
 Pituitary Disorders Suranut Charoensri, MD Division of Endocrinology and Metabolism Department of Medicine Faculty of Medicine, Khon Kaen University Anatomical Landmarks Nat Rev Endocrinol 2014;10:423-435
Pituitary Disorders Suranut Charoensri, MD Division of Endocrinology and Metabolism Department of Medicine Faculty of Medicine, Khon Kaen University Anatomical Landmarks Nat Rev Endocrinol 2014;10:423-435
Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary Tumor Apoplexy
 Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
Pathology of pituitary gland. By: Shifaa Qa qa
 Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Sharon maslovitz Lis Maternity Hospital
 Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Conditions that may cause episodic headaches:
Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Conditions that may cause episodic headaches:
Pituitary gland diseases
 Pituitary gland diseases Pituitary Gland Weight 600 mg Is located within the sella turcica Anatomically and functionally distinct anterior and posterior lobes Pituitary Development The pituitary originate
Pituitary gland diseases Pituitary Gland Weight 600 mg Is located within the sella turcica Anatomically and functionally distinct anterior and posterior lobes Pituitary Development The pituitary originate
Laurie A. Loevner, MD
 Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Hyperprolactinemia. Justin Moore, MD
 Hyperprolactinemia Justin Moore, MD Biography.com The Miraculous Lactation of St. Bernard Bernard prayed before a statue of the Madonna, asking her, "Show yourself a mother" ("Monstra te esse Matrem").
Hyperprolactinemia Justin Moore, MD Biography.com The Miraculous Lactation of St. Bernard Bernard prayed before a statue of the Madonna, asking her, "Show yourself a mother" ("Monstra te esse Matrem").
Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline
 Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline Shlomo Melmed, Felipe F. Casanueva, Andrew R. Hoffman, David L. Kleinberg, Victor M. Montori, Janet A. Schlechte
Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline Shlomo Melmed, Felipe F. Casanueva, Andrew R. Hoffman, David L. Kleinberg, Victor M. Montori, Janet A. Schlechte
CYSTIC PROLACTINOMA: A SURGICAL DISEASE?
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
X/00/$03.00/0 Vol. 85, No. 5 The Journal of Clinical Endocrinology & Metabolism Copyright 2000 by The Endocrine Society
 0021-972X/00/$03.00/0 Vol. 85, No. 5 The Journal of Clinical Endocrinology & Metabolism Printed in U.S.A. Copyright 2000 by The Endocrine Society The Dominant Role of Increased Intrasellar Pressure in
0021-972X/00/$03.00/0 Vol. 85, No. 5 The Journal of Clinical Endocrinology & Metabolism Printed in U.S.A. Copyright 2000 by The Endocrine Society The Dominant Role of Increased Intrasellar Pressure in
Endocrinological Outcome Among Treated Craniopharyngioma Patients
 Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
THE ANTERIOR PITUITARY. Embryology cont. Embryology of the pituitary BY MISPA ZUH HS09A179. Embryology cont. THE PITUIYARY GLAND Anatomy:
 THE ANTERIOR PITUITARY BY MISPA ZUH HS09A179 Embryology of the pituitary The pituitary is formed early in embryonic life from the fusion of the Rathke s pouch (anterior) and the diencephalon ( posterior)
THE ANTERIOR PITUITARY BY MISPA ZUH HS09A179 Embryology of the pituitary The pituitary is formed early in embryonic life from the fusion of the Rathke s pouch (anterior) and the diencephalon ( posterior)
Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum
 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum") Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum Cell type hormone Clinical syndrome Tumor type Somatotroph Growth
Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum Cell type hormone Clinical syndrome Tumor type Somatotroph Growth
Metastasis. 57 year old with progressive Headache and Right Sided Visual Loss
 Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
No Financial Interest
 Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Visual pathways in the chiasm
 Visual pathways in the chiasm Intracranial relationships of the optic nerve Fixation of the chiasm Chiasmatic pathologies The function of the optic chiasm may be altered by the presence of : 4) Artero
Visual pathways in the chiasm Intracranial relationships of the optic nerve Fixation of the chiasm Chiasmatic pathologies The function of the optic chiasm may be altered by the presence of : 4) Artero
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury
 Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
Pathophysiology of Pituitary Gland Disorders. PHCL 415 Hadeel Alkofide May 2010
 Pathophysiology of Pituitary Gland Disorders PHCL 415 Hadeel Alkofide May 2010 1 Learning Objectives Understand the physiology of pituitary gland Understand acromegaly & describe its clinical features
Pathophysiology of Pituitary Gland Disorders PHCL 415 Hadeel Alkofide May 2010 1 Learning Objectives Understand the physiology of pituitary gland Understand acromegaly & describe its clinical features
High and Low GH: an update of diagnosis and management of GH disorders
 High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
Clinical presentations of endocrine diseases
 Section I Chapter 1 Clinical approaches Clinical presentations of endocrine diseases Karen Gomez-Hernandez and Shereen Ezzat Endocrinology is a fascinating field that covers a wide range of diseases with
Section I Chapter 1 Clinical approaches Clinical presentations of endocrine diseases Karen Gomez-Hernandez and Shereen Ezzat Endocrinology is a fascinating field that covers a wide range of diseases with
Pituitary Disorders. Eiman Ali Basheir Mob: /1/2019
 Pituitary Disorders Eiman Ali Basheir Mob: 0915020385 31/1/2019 Objectives By the end of this lecture the students will be able to: Understand basic Pituitary axis physiology State the common causes of
Pituitary Disorders Eiman Ali Basheir Mob: 0915020385 31/1/2019 Objectives By the end of this lecture the students will be able to: Understand basic Pituitary axis physiology State the common causes of
Evaluation and Management of Pituitary Failure. Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS
, FRCPC Professor of Medicine Dalhousie University, Halifax, NS") Evaluation and Management of Pituitary Failure Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS Conflict of Interest None Objectives Diagnostic approach
Evaluation and Management of Pituitary Failure Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS Conflict of Interest None Objectives Diagnostic approach
Pituitary for the General Practitioner. Marilyn Lee Consultant physician and endocrinologist
 Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea
 Clin Pediatr Endocrinol 1996; 5(2), 61-66 Copyright (C) 1996 by The Japanese Society for Pediatric Endocrinology Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea Toshihisa Okada, Soroku
Clin Pediatr Endocrinol 1996; 5(2), 61-66 Copyright (C) 1996 by The Japanese Society for Pediatric Endocrinology Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea Toshihisa Okada, Soroku
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Challenging Pituitary Cases. Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine
 Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
Where Has My Vision Gone? Evaluation of Sellar Lesions. Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008
 Where Has My Vision Gone? Evaluation of Sellar Lesions Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008 Objectives Present a case highlighting the clinical presentation and evaluation of a sellar
Where Has My Vision Gone? Evaluation of Sellar Lesions Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008 Objectives Present a case highlighting the clinical presentation and evaluation of a sellar
Secondary amenorrhoea Dr.ASMAA AL SANJARY
 Secondary amenorrhoea Dr.ASMAA AL SANJARY The student at the end of this lecture should be able to: Define secondary amenorrhoea. Classify the causes of secondary amenorrhoea. Describe the commonest three
Secondary amenorrhoea Dr.ASMAA AL SANJARY The student at the end of this lecture should be able to: Define secondary amenorrhoea. Classify the causes of secondary amenorrhoea. Describe the commonest three
Case Report. Michael H. Goldman, MD; Alison T. Gruber; Marc A. Herman, MD ABSTRACT
 Case Report CONCURRENT PANHYPOPITUITARISM AND HYPERPROLACTINEMIA DUE TO A GIANT INTERNAL CAROTID ANEURYSM REVEALED BY THYROID HORMONE WITHDRAWAL DURING FOLLOW-UP MANAGEMENT OF THYROID CANCER Michael H.
Case Report CONCURRENT PANHYPOPITUITARISM AND HYPERPROLACTINEMIA DUE TO A GIANT INTERNAL CAROTID ANEURYSM REVEALED BY THYROID HORMONE WITHDRAWAL DURING FOLLOW-UP MANAGEMENT OF THYROID CANCER Michael H.
Hypothalamus & Pituitary Gland
 Hypothalamus & Pituitary Gland Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and
Hypothalamus & Pituitary Gland Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and
Professor Ian Holdaway. Endocrinologist Auckland District Health Board
 Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
Hormonal Replacement in Hypopituitarism in Adults: An Endocrine Society Clinical Practice Guideline
 Hormonal Replacement in Hypopituitarism in Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Maria Fleseriu, MD Ibrahim A. Hashim, PhD Niki Karavitaki, PhD Shlomo Melmed, MD M.
Hormonal Replacement in Hypopituitarism in Adults: An Endocrine Society Clinical Practice Guideline Task Force Members Maria Fleseriu, MD Ibrahim A. Hashim, PhD Niki Karavitaki, PhD Shlomo Melmed, MD M.
Describe the epidemiology and clinical presentations of pituitary tumours:
 Pituitary Tumours: Describe the epidemiology and clinical presentations of pituitary tumours: 10-15% of all primary brain tumours More common in females Unselected autopsy studies 20-25% of population
Pituitary Tumours: Describe the epidemiology and clinical presentations of pituitary tumours: 10-15% of all primary brain tumours More common in females Unselected autopsy studies 20-25% of population
Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC
 10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight. LOCATION Sella turcica A bony cavity. DIVISIONS Anterior lobe Posterior lobe Pars intermedia
 DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight LOCATION Sella turcica A bony cavity DIVISIONS Anterior lobe Posterior lobe Pars intermedia body temperature autonomic nervous system emotional and food
DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight LOCATION Sella turcica A bony cavity DIVISIONS Anterior lobe Posterior lobe Pars intermedia body temperature autonomic nervous system emotional and food
A Case of Pituitary Apoplexy in Third Trimester of Pregnancy
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.16 March. (2018), PP 01-06 www.iosrjournals.org A Case of Pituitary Apoplexy in Third
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 3 Ver.16 March. (2018), PP 01-06 www.iosrjournals.org A Case of Pituitary Apoplexy in Third
Non-Functioning Tumours and Pituitary Hormone Testing. Miguel Debono Consultant in Endocrinology
 Non-Functioning Tumours and Pituitary Hormone Testing Miguel Debono Consultant in Endocrinology Agenda Pituitary masses Non functioning pituitary adenomas Testing pituitary function Pituitary Hormone Replacement
Non-Functioning Tumours and Pituitary Hormone Testing Miguel Debono Consultant in Endocrinology Agenda Pituitary masses Non functioning pituitary adenomas Testing pituitary function Pituitary Hormone Replacement
What we will cover. Evaluation of the Child with Suspected Pituitary Disease. ituitary
 Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Leticia Hernández Dávila, MD May 26, J Clin Endocrinol Metab (2016) 101 (11):
 101 (11):") Leticia Hernández Dávila, MD May 26, 2017 J Clin Endocrinol Metab (2016) 101 (11): 3888-3921. DISCLOSURES None. OBJECTIVES Understanding clinical issues related to hypopituitarism, including: Biochemical
Leticia Hernández Dávila, MD May 26, 2017 J Clin Endocrinol Metab (2016) 101 (11): 3888-3921. DISCLOSURES None. OBJECTIVES Understanding clinical issues related to hypopituitarism, including: Biochemical
A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease
 A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease Z Hussein, MRCP*, B Tress**, P G Cohnan, FRACP***... 'Department of Medicine, Hospital Putrajaya, Putrajaya, Presint 7, 62250
A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease Z Hussein, MRCP*, B Tress**, P G Cohnan, FRACP***... 'Department of Medicine, Hospital Putrajaya, Putrajaya, Presint 7, 62250
Endocrine Glands: Hormone-secreting organs are called endocrine glands
 University of Jordan Department of Physiology and Biochemistry Nursing students, Academic year 2017/2018. ******************************************************************* Ref: Principles of Anatomy
University of Jordan Department of Physiology and Biochemistry Nursing students, Academic year 2017/2018. ******************************************************************* Ref: Principles of Anatomy
Colorectal Cancer Manifesting with Metastasis to Prolactinoma: Report of a Case Involving Symptoms Mimicking Pituitary Apoplexy
 CASE REPORT Colorectal Cancer Manifesting with Metastasis to Prolactinoma: Report of a Case Involving Symptoms Mimicking Pituitary Apoplexy Yotsapon Thewjitcharoen 1, Shanop Shuangshoti 2, Sukalaya Lerdlum
CASE REPORT Colorectal Cancer Manifesting with Metastasis to Prolactinoma: Report of a Case Involving Symptoms Mimicking Pituitary Apoplexy Yotsapon Thewjitcharoen 1, Shanop Shuangshoti 2, Sukalaya Lerdlum
Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports
 CASE REPORT Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports S.H.P.P. Roerink 1 *, E.J. van Lindert 2, A.C. van de Ven 1 Departments of 1 Internal
CASE REPORT Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports S.H.P.P. Roerink 1 *, E.J. van Lindert 2, A.C. van de Ven 1 Departments of 1 Internal
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to
 Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
Table of Contents Section I Pituitary and Hypothalamus 1. Development of the Pituitary Gland 2. Divisions of the Pituitary Gland and Relationship to the Hypothalamus 3. Blood Supply of the Pituitary Gland
TABLES. Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging. Conclusions. Author (Year) Classification Process/Evid ence Class
 Imaging. Conclusions. Author (Year) Classification Process/Evid ence Class") TABLES Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging Author Clark (1986) 9 Reformatted sagittal images in the differential diagnosis meningiomas and adenomas with suprasellar
TABLES Imaging Modalities Evidence Tables Table 1 Computed Tomography (CT) Imaging Author Clark (1986) 9 Reformatted sagittal images in the differential diagnosis meningiomas and adenomas with suprasellar
15 month-old female with a cystic brain lesion. Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014
 + 15 month-old female with a cystic brain lesion Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014 + Chief Complaint 15 month-old female admitted to PICU for concern
+ 15 month-old female with a cystic brain lesion Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014 + Chief Complaint 15 month-old female admitted to PICU for concern
PITUITARY PARASELLAR LESIONS. Kim Learned, MD
 PITUITARY PARASELLAR LESIONS Kim Learned, MD DIFFERENTIALS Pituitary Sella Clivus, Sphenoid Sinus Suprasellar Optic chiasm, Hypothalamus, Circle of Willis Parasellar Cavernous Sinus Case 1 17 YEAR-OLD
PITUITARY PARASELLAR LESIONS Kim Learned, MD DIFFERENTIALS Pituitary Sella Clivus, Sphenoid Sinus Suprasellar Optic chiasm, Hypothalamus, Circle of Willis Parasellar Cavernous Sinus Case 1 17 YEAR-OLD
(3) Pituitary tumours
 Pituitary tumours") Hypopituitarism Diabetes Insipidus Pituitary tumours (2) Dr T Kemp - Endocrinology and Metabolism Unit - Steve Biko Academic Hospital (3) Pituitary tumours Pituitary microadenoma - intrasellar adenoma
Hypopituitarism Diabetes Insipidus Pituitary tumours (2) Dr T Kemp - Endocrinology and Metabolism Unit - Steve Biko Academic Hospital (3) Pituitary tumours Pituitary microadenoma - intrasellar adenoma
Pituitary Tumors: adenoma, craniopharyngioma, rathke cyst
 Pituitary Tumors: adenoma, craniopharyngioma, rathke cyst Overview Tumors that grow from the pituitary gland can affect the whole body by interfering with normal hormone levels. They can also cause headaches
Pituitary Tumors: adenoma, craniopharyngioma, rathke cyst Overview Tumors that grow from the pituitary gland can affect the whole body by interfering with normal hormone levels. They can also cause headaches
Part II - Revising the sellar and parasellar region: differential diagnosis of a sellar region mass
 Part II - Revising the sellar and parasellar region: differential diagnosis of a sellar region mass Poster No.: C-1390 Congress: ECR 2015 Type: Educational Exhibit Authors: I. Candelaria, C. Figueira,
Part II - Revising the sellar and parasellar region: differential diagnosis of a sellar region mass Poster No.: C-1390 Congress: ECR 2015 Type: Educational Exhibit Authors: I. Candelaria, C. Figueira,
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
Living Control Mechanisms
 Living Control Mechanisms Dr Kate Earp MBChB MRCP Specialty Registrar Chemical Pathology & Metabolic Medicine kate.earp@sth.nhs.uk 15/10/2015 Contents Aims & objectives Homeostasis Cell communication Introduction
Living Control Mechanisms Dr Kate Earp MBChB MRCP Specialty Registrar Chemical Pathology & Metabolic Medicine kate.earp@sth.nhs.uk 15/10/2015 Contents Aims & objectives Homeostasis Cell communication Introduction
Pharmacology of Hypothalamic Hormones
 Pharmacology of Hypothalamic Hormones Pharmacology of Hypothalamic Hormones The neuroendocrine system, which is controlled by the pituitary and hypothalamus, coordinates body functions by transmitting
Pharmacology of Hypothalamic Hormones Pharmacology of Hypothalamic Hormones The neuroendocrine system, which is controlled by the pituitary and hypothalamus, coordinates body functions by transmitting
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
Growth Hormone, Somatostatin, and Prolactin 1 & 2 Mohammed Y. Kalimi, Ph.D.
 Growth Hormone, Somatostatin, and Prolactin 1 & 2 Mohammed Y. Kalimi, Ph.D. I. Growth Hormone (somatotropin): Growth hormone (GH) is a 191 amino acid single chain polypeptide (MW 22,000 daltons). Growth
Growth Hormone, Somatostatin, and Prolactin 1 & 2 Mohammed Y. Kalimi, Ph.D. I. Growth Hormone (somatotropin): Growth hormone (GH) is a 191 amino acid single chain polypeptide (MW 22,000 daltons). Growth
Overview of Reproductive Endocrinology
 Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
Overview of Reproductive Endocrinology I have no conflicts of interest to report. Maria Yialamas, MD Female Hypothalamic--Gonadal Axis 15 4 Hormone Secretion in the Normal Menstrual Cycle LH FSH E2, Progesterone,
Subject Index. hypothalamic-pituitary-adrenal axis 158. Atherosclerosis, ghrelin role AVP, see Arginine vasopressin.
 Subject Index Acromegaly, somatostatin analog therapy dopamine agonist combination therapy 132 efficacy 132, 133 overview 130, 131 receptor subtype response 131, 132 SOM30 studies 131, 132 ACTH, see Adrenocorticotropic
Subject Index Acromegaly, somatostatin analog therapy dopamine agonist combination therapy 132 efficacy 132, 133 overview 130, 131 receptor subtype response 131, 132 SOM30 studies 131, 132 ACTH, see Adrenocorticotropic
Case report. Open Access. Abstract
 Open Access Case report Hyperthyroidism unmasked several years after the medical and radiosurgical treatment of an invasive macroprolactinoma inducing hypopituitarism: a case report Luca Foppiani 1 *,
Open Access Case report Hyperthyroidism unmasked several years after the medical and radiosurgical treatment of an invasive macroprolactinoma inducing hypopituitarism: a case report Luca Foppiani 1 *,
Intrasphenoidal Rathke's Cleft Cyst: Case presentation and review of the literature
 Romanian Neurosurgery Volume XXX Number 4 2016 October - December Article Intrasphenoidal Rathke's Cleft Cyst: Case presentation and review of the literature Umit Kocaman, Muhammet Bahadir Yilmaz, Hakan
Romanian Neurosurgery Volume XXX Number 4 2016 October - December Article Intrasphenoidal Rathke's Cleft Cyst: Case presentation and review of the literature Umit Kocaman, Muhammet Bahadir Yilmaz, Hakan
NANOS Patient Brochure
 NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
Pituitary tumors: pathophysiology, clinical manifestations and management
 Pituitary tumors: pathophysiology, clinical manifestations and management B M Arafah and M P Nasrallah Division of Clinical and Molecular Endocrinology, Case Western Reserve University and University Hospitals
Pituitary tumors: pathophysiology, clinical manifestations and management B M Arafah and M P Nasrallah Division of Clinical and Molecular Endocrinology, Case Western Reserve University and University Hospitals
ABNORMAL PITUITARY FUNCTION
 Overview ABNORMAL PITUITARY FUNCTION Specialist Portfolio Seminar Katie Jones Sandwell and West Birmingham Hospitals NHS Trust Anterior pituitary overview Posterior pituitary overview Pituitary dysfunction
Overview ABNORMAL PITUITARY FUNCTION Specialist Portfolio Seminar Katie Jones Sandwell and West Birmingham Hospitals NHS Trust Anterior pituitary overview Posterior pituitary overview Pituitary dysfunction
Prolactin is a pituitary-derived hormone that plays a
 Diagnosis and management of hyperprolactinemia Review Synthèse Omar Serri, Constance L. Chik, Ehud Ur, Shereen Ezzat Abstract PROLACTIN IS A PITUITARY HORMONE that plays a pivotal role in a variety of
Diagnosis and management of hyperprolactinemia Review Synthèse Omar Serri, Constance L. Chik, Ehud Ur, Shereen Ezzat Abstract PROLACTIN IS A PITUITARY HORMONE that plays a pivotal role in a variety of
See the latest estimates for new cases of pituitary tumors in the US and what research is currently being done.
 About Pituitary Tumors Overview and Types If you have been diagnosed with a pituitary tumor or worried about it, you likely have a lot of questions. Learning some basics is a good place to start. What
About Pituitary Tumors Overview and Types If you have been diagnosed with a pituitary tumor or worried about it, you likely have a lot of questions. Learning some basics is a good place to start. What
Autoimmune hypophysitis may eventually become empty sella
 Neuroendocrinology Letters Volume 34 No. 2 2013 Autoimmune hypophysitis may eventually become empty sella Hua Gao*, You-you Gu*, Ming-cai Qiu Department of Endocrinology, Tianjin Medical University General
Neuroendocrinology Letters Volume 34 No. 2 2013 Autoimmune hypophysitis may eventually become empty sella Hua Gao*, You-you Gu*, Ming-cai Qiu Department of Endocrinology, Tianjin Medical University General
Pituitary Interactive Case Presentations Focus on: Hyperprolactinemia
 HYPERPROLACTINEMIA Pituitary Interactive Case Presentations Focus on: Hyperprolactinemia March 6, 2016 Beverly MK Biller, MD Massachusetts General Hospital/Harvard Medical School Hyperprolactinemia is
HYPERPROLACTINEMIA Pituitary Interactive Case Presentations Focus on: Hyperprolactinemia March 6, 2016 Beverly MK Biller, MD Massachusetts General Hospital/Harvard Medical School Hyperprolactinemia is
PATIENT INFORMATION HYPOPITUITARISM YOUR QUESTIONS ANSWERED
 PATIENT INFORMATION HYPOPITUITARISM YOUR QUESTIONS ANSWERED Contents What is hypopituitarism? 1 What causes hypopituitarism? 2 What are the symptoms and signs of hypopituitarism? 4 How is hypopituitarism
PATIENT INFORMATION HYPOPITUITARISM YOUR QUESTIONS ANSWERED Contents What is hypopituitarism? 1 What causes hypopituitarism? 2 What are the symptoms and signs of hypopituitarism? 4 How is hypopituitarism
Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide)
") Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide) INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of
Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide) INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of
Ch 8: Endocrine Physiology
 Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Ch 8: Endocrine Physiology Objectives 1. Review endocrine glands of body. 2. Understand how hypothalamus controls endocrine system & sympathetic epinephrine response. 3. Learn anterior pituitary hormones
Endocrine system overview
 Endocrine system overview Nature of the hormonal system -Major integrator of body function Classification of hormones Endocrine vs paracrine Nature of hormone-receptor systems Role of the hypothalamuspituitary
Endocrine system overview Nature of the hormonal system -Major integrator of body function Classification of hormones Endocrine vs paracrine Nature of hormone-receptor systems Role of the hypothalamuspituitary