in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
|
|
|
- Clifford Barnett
- 6 years ago
- Views:
Transcription
1 Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
2 None Conflict of Interest
3 Topics to be Covered Adrenal Incidentaloma Pituitary incidentaloma and hypopituitarism Male hypogonadism Osteoporosis
4 Adrenal Incidentaloma Generally, do not evaluate any adenoma < 1 cm unless there is an obvious hormonal syndrome associated with it (hyperaldosteronism (Conn s syndrome), pheochromocytoma, or Cushing s syndrome). Radiologic evaluation should distinguish benign from tumors of concern several options All tumors 1 cm or larger should have hormonal evaluation Consider removal of tumors over 4-6 cm even if benign characteristics unless myelolipoma.
5 Radiologic Evaluation Non-contrast CT benign if Hounsfield unit measurement is 10 Contrast enhanced CT benign if rapid washout of contrast by minutes. Relative washout > 40% and absolute washout > 60% suggests benign MRI compares in phase to out of phase imaging to distinguish benign from concerning lesions FDG-PET can also differentiate benign lesions from those of concern
6 Normal Adrenals on CT



7 Adrenal Adenoma on CT
8 Radiologic Evaluation Lesion found incidentally on an initial study Repeat as adrenal protocol CT or MRI depends a bit on your institution. If benign appearing, repeat non-contrast CT for size after 6-12 months to be sure not growing. If of concern and not having surgery, repeat study in 3-12 months. Some recommend one more study one year later for benign appearing lesions but others do not DO NOT DO BIOPSY UNLESS PHEOCHROMOCYTOMA RULED OUT BIOPSY ONLY HELPFUL IN DIAGNOSING METASTATIC DISEASE BENIGN AND MALIGNANT ADRENAL LESIONS CANNOT BE RELIABLY DISTINGUISHED ON BIOPSY.
9 Radiologic Evaluation Consider surgery for nodules > 4-6 cm unless consistent with myelolipoma li (Hounsfield < -20). Consider surgery for high density lesions smaller than 4 cm once pheochromocytoma excluded. PET can be helpful here at times.
10 Hormonal Evaluation of all Incidentally Found Adrenal Nodules 1 cm 1 mg overnight dexamethasone suppression test Normal < 1.8 mcg/dl Cortisol excess > 5 mcg/dl DHEA-S can help usually low if cortisol secreting adrenal adenoma ACTH can help usually low normal or low-normal if cortisol secreting adrenal adenoma Aldosterone/renin ratio If > 20, confirm with another test. Beta blockers can cause falsely elevated ratio by suppressing renin (if spontaneous hypokalemia, undetectable t renin, aldosterone > 20 ng/dl can go right to sampling). Plasma free metanephrine vs 24 hour urine catecholamines Pheochromocytoma is frequently high density on CT
11 Hormonal Evaluation of all Incidentally Found Adrenal Nodules 1 cm Assuming benign imaging characteristics and initial benign hormonal evaluation, repeat dexamethasone suppression test t after 1-2 years different organizations have given different recommendations on this. Certainly if suppression > 1.8, repeat and also obtain other measurement of cortisol excess 24 hour urine free cortisol or midnight salivary cortisol. Consider endocrine consultation.


12 From: Approach to the Patient with an Adrenal Incidentaloma. 2010;95(9): doi: /jc Figure Legend: Suggested evaluation of an incidentally found adrenal mass. *, Surgery for large masses without a cause that requires resection, e.g. tuberculosis. LN, Late-night; Aldo, aldosterone; Dex, dexamethasone; F/U, follow-up; eval, evaluation; mo, months. Date of download: 2/19/2017 Copyright 2010 by The Endocrine Society
13 Pituitary Incidentaloma Hypopituitarism Pituitary incidentaloma all should undergo hormonal evaluation and if initial study a brain MRI or CT, get dedicated pituitary MRI with and without contrast. Repeat MRI scan of the pituitary 6 months after the initial scan if the incidentaloma is a macro-incidentaloma ( 1 cm) and 1 year after the initial scan if it is a microincidentaloma (< 1 cm). In patients whose incidentaloma does not change in size, suggest repeating the MRI every year for macro and every 1 2 yr in micro for the following 3 yr, and gradually less frequently thereafter Visual fields if near chiasm
14 MRI Pituitary

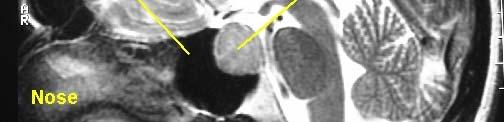

15 MRI Pituitary Adenoma
16 Pituitary Incidentaloma Indications for Surgery A Visual Field deficit due to the lesion. Other visual abnormalities, such as ophthalmoplegia or neurological compromise due to nerve compression by the lesion. Lesion abutting or compressing the optic nerves or chiasm on MRI. Pituitary apoplexy with visual disturbance. Hypersecreting tumors other than prolactinomas
17 Pituitary Incidentaloma Screen for Hormonal Excess Prolactin ideally get with dilution to avoid issues with hook effect (falsely low measurement due to overwhelming of antibodies by very high prolactin). Growth hormone screen with IGF-1 Thyroid hormone screen with TSH and Free T4 Cortisol late night salivary cortisol x 2 or 24 hour urine free cortisol +/- ACTH Most non-functional adenomas are gonadotroph adenoma but non-secretory
18 Pituitary Incidentaloma Screen for Hypopituitarism Most important in macro-incidentaloma Adrenal AM cortisol (ACTH not helpful) < 3 indicative of adrenal insufficiency > 15 normal 3-15 do ACTH stimulation test Thyroid Free T4 (TSH not helpful and can confuse) Gonadal (be sure prolactin not elevated) Men - LH, FSH testosterone t t (early AM) +/- SHBG Women LH, FSH, Estradiol Growth hormone Can do IGF-1 as screen or if concern do GH stimulation testing random GH not helpful
19 Pituitary Incidentaloma Screen for Hypopituitarism No need to repeat testing in micro-incidentaloma If macro, repeat testing at 6 months and then yearly or use growth on scanning as indication usually no progression to hypopituitarism if lesion not growing
20 From: Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline. 2016;96(4): doi: /jc [Modified from Molitch ME: J Clin Endocrinol Metab 80:3 6, 1995 (49).] Date of download: 2/19/2017 Copyright 2011 by The Endocrine SocietyThis article is published under the terms of the Creative Commons Attribution-Non Commercial-No Derivatives License (CC-BY-NC-ND;
21 Male Hypogonadism More specific signs and symptoms Incomplete or delayed sexual development, eunuchoidism Reduced sexual desire (libido) and activity Decreased spontaneous (early AM) erections Breast discomfort, gynecomastia Loss of body (axillary and pubic) hair, reduced shaving Very small (especially <5 ml) or shrinking testes Inability to father children, low or zero sperm count Height loss, low trauma fracture, low bone mineral density Hot flushes, sweats
22 Male Hypogonadism Less specific signs and symptoms Decreased energy, motivation, initiative, and self-confidence Feeling sad or blue, depressed d mood, dysthymia Poor concentration and memory Sleep disturbance, increased sleepiness Mild anemia (normochromic, normocytic, in the female range) Reduced muscle bulk and strength Increased body fat, body mass index Diminished physical or work performance
23 Male Hypogonadism Measure testosterone before 10 AM Never treat based on a single measurement Consider measuring SHBG unless you know your lab does accurate testing for free or bioavailable il bl testosterone Evaluation of androgen deficiency should not be done during an acute or subacute illness.
24 Male Hypogonadism If testosterone low, repeat with prolactin, LH and FSH If primary hypogonadism and no obvious cause, get genetic testing for Klinefelter s DEXA scan in men with marked hypogonadism If secondary, get MRI if testosterone level < 150 ng/dl or if there is suggestion of hypopituitarism, mass effect, hyperprolactinemia, visual field defect. Screen iron studies and at least one other pituitary hormone level (e.g. Free T4 and TSH)
25 Potential Benefits of Androgen Therapy
26 Monitoring of therapy Male Hypogonadism Hematocrit stop it 54% until level comes down DEXA 2 years after initiating therapy (use T score age > 50, Z score if younger Age > 40, repeat prostate exam and PSA at 3-6 month follow up visit Get urology evaluation if PSA rises by 1.4 ng/ml in a one year period, gy y g y p abnormal prostate exam or bladder outlet symptoms
27 Hematocrit > 50 Male Hypogonadism Contraindications to Therapy Untreated severe obstructive sleep apnea Severe lower urinary tract symptoms Uncontrolled or poorly controlled heart failure Those desiring fertility Prostate cancer, nodule or induration PSA 4 or 3 if high risk of prostate cancer
28 Male Hypogonadism Topical preferred therapy gel vs patch Can use injectable but may have higher h risks due to peaks and valleys. Re-evaluate evaluate after 3-6 months and then every 6-12 months (Testosterone is controlled so should check state database and new prescription needed every 6 months) Aim for mid normal range for age If using IM, aim for level of ng/dl one week after injection




29 Male Hypogonadism Journal of Clinical Endocrinology & Metabolism, June 2010, Vol. 95(6):
30 Side effects of testosterone therapy Lowering of sperm count Gynecomastia Possible increased risk of prostate cancer (or growth of undiagnosed cancers) Increase in prostate size with hbladder outlet symptoms Polycythemia Worsening of CHF Worsening of obstructive sleep apnea Phlebitis Possible increased cardiovascular risk, especially in high h risk individuals id
31 Male Hypogonadism Do not treat all older men with low testosterone evaluate on case by case basis Alternatives to testosterone therapy not as well studied Clomiphene citrate t most common dose 25 mg daily benefits are it is a pill, not controlled, and does not lower sperm count HCG therapy helpful if previous testosterone therapy with desire for fertility can take 18 months or more for spermatogenesis to return spontaneously. Aromatase inhibitors (anastrozoleand letrozole) l least well studied d
32 Male Hypogonadism World J Nephrol May 6; 4(2):
33 Post-Menopausal Osteoporosis Who to screen with DEXA? Age 65 History of fragility fracture Starting or taking glucocorticoids long-term ( 3 months) Radiologic osteopenia Clinical risk factors low body weight, smoker, family history of spine or hip fracture esp at younger age, early menopause, secondary osteoporosis, excessive alcohol When to do vertebral fracture assessment (VFA) Concern that treatment needed but FRAX under recommended threshold
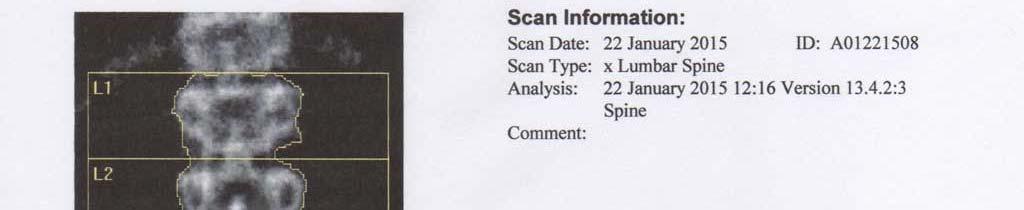
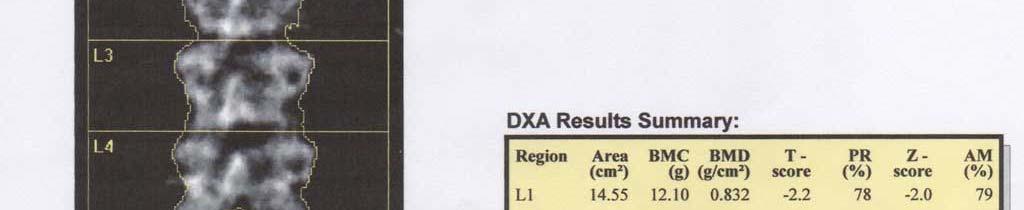
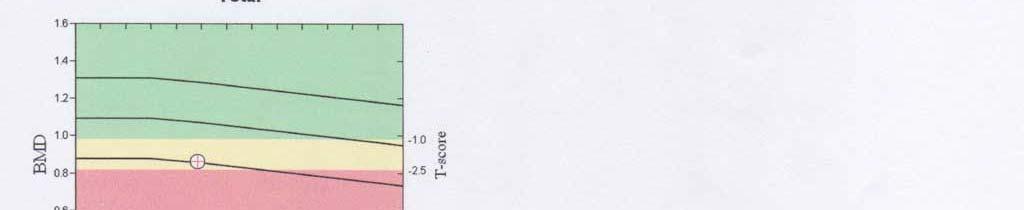
34 DEXA
35 Post-Menopausal Osteoporosis When and how to screen for secondary osteoporosis When if Z score -2 or lower or signs/symptoms of other disease How celiac disease (e.g.ttg), Vitamin i D level, l PTH level, l SPEP, TSH, 24 hour urine calcium/creat
36 Who to treat? Post-Menopausal Osteoporosis FRAX > 3% risk of hip fracture or > 20% risk of major osteoporotic fracture in next 10 years Fragility fracture either clinical or radiologic (VFA vertebral fracture assessment) To be on long term (> 3 month) steroids and T score < -1.0 To be on anastrazole therapy for breast cancer and T score < -1.0
37 How to treat Post-Menopausal Osteoporosis Limit i alcohol, l smoke cessation, encourage exercise, try to prevent falls Vitamin D units daily (max 4000 units) Ensure sufficient calcium intake mg by diet and/or supplement Bisphosphonate esp alendronate, risedronate, or zoledronic acid Denosumab Teriparatide/abaloparatide Raloxiphene
38 How long to treat Post-Menopausal Osteoporosis If mild to moderate osteoporosis, treat t for 3 years with IV bisphosphonate or 5 years with oral and then can stop and evaluate over time via DEXA If severe, keep on therapy +/- drug holiday Teriparatide/abaloparatide treat for 18 months to 2 years and then switch to antiresorptive only therapy that is anabolic Denosumab need to keep on long term possible rebound loss when stopped Raloxifene no documented benefit on hip
39 Questions?
Testosterone Therapy in Men with Hypogonadism
 Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Testosterone Therapy in Men with Hypogonadism (Endocrine Society 2018 Guideline) Ngwe Yin, MD Assistant Clinical Professor of Medicine, UCSF Fresno Medical Education Program Disclosures None Objective
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Testosterone Treatment: Myths Vs Reality. Fadi Al-Khayer, M.D, F.A.C.E
 Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Testosterone Treatment: Myths Vs Reality Fadi Al-Khayer, M.D, F.A.C.E The Biological Functions of Testosterone in Men Testosterone is essential to the musculoskeletal and metabolic systems throughout a
Pituitary Tumors and Incidentalomas. Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
 Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients
 Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
Evaluation and Treatment of Primary Androgen Deficiency Syndrome in Male Patients Jeff Unger, MD Director Chino Medical Group Diabetes and Headache Intervention Center Chino, California January 16, 2008
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Hypogonadism 4/27/2018. Male Hypogonadism -- Definition. Epidemiology. Objectives HYPOGONADISM. Men with Hypogonadism. 95% untreated.
 Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Male Hypogonadism -- Definition - Low T, Low Testosterone Hypogonadism -...a clinical syndrome that results from failure of the testes to produce physiological concentrations of testosterone due to pathology
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Androgen deficiency. Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital
 Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Androgen deficiency Dr Rakesh Iyer Staff Specialist in Endocrinology Calvary hospital Outline Pathological androgen deficiency - Background, causes, interpretation - Indications for treatment Androgen
Aromatase Inhibitors & Osteoporosis
 Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
Aromatase Inhibitors & Osteoporosis Miss Sarah Horn Consultant Oncoplastic Breast Surgeon April 2018 Aims Role of Aromatase Inhibitors (AI) in breast cancer treatment AI s effects on bone health Bone health
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
GUIDELINES ON. Introduction. G.R. Dohle, S. Arver, C. Bettocchi, S. Kliesch, M. Punab, W. de Ronde
 GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
GUIDELINES ON Male Hypogonadism G.R. Dohle, S. Arver,. Bettocchi, S. Kliesch, M. Punab, W. de Ronde Introduction Male hypogonadism is a clinical syndrome caused by androgen deficiency. It may adversely
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel AXIRON transdermal solution FORTESTA transdermal gel NATESTO nasal gel STRIANT buccal mucoadhesive
GA KS KY LA MD NJ NV NY TN TX WA Applicable X X N/A N/A X N/A X X X X X X N/A N/A NA *FHK- Florida Healthy Kids. Androgens
 Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Generic Androgel 1% (2.5 g) packet 2 packets per day (testosterone
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System
 PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
6/14/2010. GnRH=Gonadotropin-Releasing Hormone.
 Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Male Androgen Replacement Mitchell Sorsby, MD June 19, 2010. QUESTION # 1 Which of the following is not a symptom associated with low T levels? a) decreased libido b) erectile dysfunction c) depression
Male Hypogonadism. Types and causes of hypogonadism. What is male hypogonadism? Symptoms. Testosterone production. Patient Information.
 Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Patient Information English 31 Male Hypogonadism The underlined terms are listed in the glossary. What is male hypogonadism? Male hypogonadism means the testicles do not produce enough of the male sex
Diagnosis and Treatment of Osteoporosis. Department of Endocrinology and Metabolism Ajou University School of Medicine.
 Diagnosis and Treatment of Osteoporosis Department of Endocrinology and Metabolism Ajou University School of Medicine Yoon-Sok CHUNG WCIM, COEX, Seoul, 27Oct2014 Case 1 71-year old woman Back pain Emergency
Diagnosis and Treatment of Osteoporosis Department of Endocrinology and Metabolism Ajou University School of Medicine Yoon-Sok CHUNG WCIM, COEX, Seoul, 27Oct2014 Case 1 71-year old woman Back pain Emergency
Hormone Balance - Female Report SAMPLE. result graph based on Luteal Phase. result graph based on Luteal Phase
 Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Patient Name: Patient DOB: Gender: Physician: Test Hormone Balance - Female Report SAMPLE Grote, Mary Jane Batch Number: B6437 2/16/1954 Accession Number: N52281 F Date Received: 2/3/2015 Any Lab Test
Basics of Male Libido: Dysfunction & Treatment. Ripu Hundal MD FACE First State Endocrinology Newark, DE
 Basics of Male Libido: Dysfunction & Treatment Ripu Hundal MD FACE First State Endocrinology Newark, DE Sexual Hormones Steroid hormones Commonly referred to as male sex hormones and female sex hormones,
Basics of Male Libido: Dysfunction & Treatment Ripu Hundal MD FACE First State Endocrinology Newark, DE Sexual Hormones Steroid hormones Commonly referred to as male sex hormones and female sex hormones,
Late onset hypogonadism
 Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Late onset hypogonadism Farrukh Javid Male Menopause Clinical AND biochemical syndrome Testosterone levels decline by 0.4-3% per year after the age of 30, as opposed to the more rapid decline that occurs
Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male
: female / male") 1. Patient personal details Institute code: Physician code: Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male 2. Changes in acromegaly-specific medical
1. Patient personal details Institute code: Physician code: Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male 2. Changes in acromegaly-specific medical
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY)
") HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
HYPOGONADISM DEFINITION: PRODUCTION OF SEX HORMONES AND GERM CELLS IS INADEQUATE (ENDOCRINE SOCIETY) DEFECT OF THE REPRODUCTIVE SYSTEM THAT RESULTS IN LACK OF FUNCTION OF THE GONADS (Wikipedia) REDUCTION
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
TESTOSTERONE DEFINITION
 DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
DEFINITION A hormone that is a hydroxyl steroid ketone (C19H28O2) produced especially by the testes or made synthetically and that is responsible for inducing and maintaining male secondary sex characteristics.
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Osteoporosis Clinical Guideline. Rheumatology January 2017
 Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Osteoporosis Clinical Guideline Rheumatology January 2017 Introduction Osteoporosis is a condition of low bone mass leading to an increased risk of low trauma fractures. The prevalence of osteoporosis
Point-Counterpoint: Late Onset Hypogonadism (LOH)
") Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Point-Counterpoint: Late Onset Hypogonadism (LOH) We are Under-diagnosing and Treating Men with LOH LOH is a Non-existent Disease ~ Robert E. Donohue, MD Late Onset Hypogonadism LOH: underdx. & undertx
Androgens. Medication Strengths Quantity Limit Comments Androderm (testosterone patch) 1% pump 2 pump bottles per Non-Preferred
 1% pump 2 pump bottles per Non-Preferred") Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Market DC Androgens Override(s) Prior Authorization Quantity Limit Approval Duration Varies upon diagnosis Medication Strengths Quantity Limit Comments Androderm (testosterone patch) AndroGel (testosterone
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
How to treat: TRT modalities and formulations
 How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
How to treat: TRT modalities and formulations Paul PIETTE, PharmD Senior Research Fellow Clinique Antoine Depage - Belgium ppiette@besins-healthcare.com Bruges 2014, May 15 th Testosterone-replacement
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Pharmacy Coverage Guidelines are subject to change as new information becomes available.
 TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
TESTOSTERONE REPLACEMENT THERAPY: ANDRODERM transdermal patch ANDROGEL pump transdermal gel and transdermal gel ANDROID (methyltestosterone) oral capsule ANDROXY (fluoxymesterone) oral tablet AXIRON transdermal
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency
 Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Corporate Medical Policy Testosterone Pellet Implantation for Androgen Deficiency File Name: Origination: Last CAP Review: Next CAP Review: Last Review: testosterone_pellet_implantation_for_androgen_deficiency
Mechanism of hyperprolactinemia
 Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Consent for Testosterone Therapy-Men Revised 4/10/18
 Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
Consent for Testosterone Therapy in Men You have been diagnosed with or have an increased risk of having a hormone deficiency and your provider has recommended treatment with bio-identical hormone replacement
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
EAU GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
BMD: A Continuum of Risk WHO Bone Density Criteria
 Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
Pathogenesis of Osteoporosis Osteoporosis Diagnosis: BMD, FRAX and Assessment of Secondary Osteoporosis AGING MENOPAUSE OTHER RISK FACTORS RESORPTION > FORMATION Bone Loss LOW PEAK BONE MASS Steven T Harris
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
GUIDELINES ON MALE HYPOGONADISM
 GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
GUIDELINES ON MALE HYPOGONADISM (Text update March 2015) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch, M. Punab Introduction Male hypogonadism is a clinical syndrome caused by androgen
Imaging pituitary gland tumors
 November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
HYPOTHALAMO PITUITARY GONADAL AXIS
 HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
ANDROGEN DEFICIENCY/MALE HYPOGONADISM 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of testosterone (androgen deficiency)
TEST REPORT # SB. Patient Name: Comprehensive Male Profile I Patient Phone Number: TEST NAME RESULTS 08/12/18 RANGE
 TEST REPORT Ordering Provider: David Getuwell, MD 8605 SW Creekside Place Beaverton, OR 97008 Phone: 503-466-2445 Fax: 503-466-1636 Samples Received 08/15/2018 Report Date 08/20/2018 Samples Collected
TEST REPORT Ordering Provider: David Getuwell, MD 8605 SW Creekside Place Beaverton, OR 97008 Phone: 503-466-2445 Fax: 503-466-1636 Samples Received 08/15/2018 Report Date 08/20/2018 Samples Collected
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology
 Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
One Day Hormone Check
 One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
One Day Hormone Check DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Salivary Hormone Results Estradiol pmol/l >3330.0 Testosterone pmol/l
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
ANDROGEN DEFICIENCY/MALE HYPOGONADISM
 Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Medical Information to Support the Decisions of TUE Committees 1. Medical Condition Hypogonadism in men is a clinical syndrome that results from failure of the testes to produce physiological levels of
Beyond the Break. After Breast Cancer: Osteoporosis in Survivorship. Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO
 FCFP Regional Primary Care Lead CCO") Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
Beyond the Break After Breast Cancer: Osteoporosis in Survivorship Dr Alexandra Ginty CCFP(EM) FCFP Regional Primary Care Lead CCO Disclosures No disclosures Osteoporosis in Breast Cancer Survivorship
EAU GUIDELINES ON MALE HYPOGONADISM
 EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
EAU GUIDELINES ON MALE HYPOGONADISM (Limited text update March 2017) G.R. Dohle (Chair), S. Arver, C. Bettocchi, T.H. Jones, S. Kliesch Introduction Male hypogonadism is a clinical syndrome caused by androgen
Lab Guide Endocrine Section Lab Guide
 Lab Guide - 2019 Endocrine Section Lab Guide Estradiol Estradiol, Cerner Name: Estradiol Competitive test principle using a polyclonal antibody specifically directed against 17βestradiol in Roche Cobas
Lab Guide - 2019 Endocrine Section Lab Guide Estradiol Estradiol, Cerner Name: Estradiol Competitive test principle using a polyclonal antibody specifically directed against 17βestradiol in Roche Cobas
New Developments in Osteoporosis: Screening, Prevention and Treatment
 Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
Osteoporosis: Overview New Developments in Osteoporosis: Screening, Prevention and Treatment Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF Definitions Risk factors
What we will cover. Evaluation of the Child with Suspected Pituitary Disease. ituitary
 Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Late onset Hypogonadism. Dr KhooSay Chuan Department of Urology Penang General Hospital
 Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Late onset Hypogonadism Dr KhooSay Chuan Department of Urology Penang General Hospital Late onset hypogonadism(loh) Definition LOH age associated testoteronedeficiency syndrome (TDS) Male menopause, andropause,
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Men and Osteoporosis So you think that it can t happen to you
 Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Therapeutic Cohort Results
 Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
Patient: PAGE LOVE DOB: January 11, 1983 Sex: F MRN: 1232704193 Order Number: J9020008 Completed: July 08, 2016 Received: July 02, 2016 Collected: July 01, 2016 Aum Healing Center Sarika Arora MD 332 Newbury
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
[If no, skip to question 10.] Y N. 2. Does the member have a diagnosis of Paget s disease of bone? Y N. [If no, skip to question 4.
![[If no, skip to question 10.] Y N. 2. Does the member have a diagnosis of Paget s disease of bone? Y N. [If no, skip to question 4.](/thumbs/86/94943423.jpg "[If no, skip to question 10.] Y N. 2. Does the member have a diagnosis of Paget s disease of bone? Y N. [If no, skip to question 4.") Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Zoledronic Acid (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Zoledronic Acid (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules. Celeste Thomas November 1, 2012
 57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
3. Has bone specific alkaline phosphatase level increased OR does the member have symptoms related to active Paget s?
 Pharmacy Prior Authorization AETA BETTER HEALTH VIRGIIA CCC PLUS and MEDALLIO/FAMIS 4.0 Zoledronic Acid (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH VIRGIIA CCC PLUS and MEDALLIO/FAMIS 4.0 Zoledronic Acid (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Trust Guideline for the Investigation of Incidental Adrenal Masses in Adults
 A clinical guideline recommended for use For Use in: A&E, Medical Assessment Unit, ITU/HDU Medical and Surgical wards By: Medical, Clinical investigation unit and Surgical staff For: Investigation of incidental
A clinical guideline recommended for use For Use in: A&E, Medical Assessment Unit, ITU/HDU Medical and Surgical wards By: Medical, Clinical investigation unit and Surgical staff For: Investigation of incidental
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
OVERVIEW OF PRESENTATION
 Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations
Thanh D. Hoang, DO, FACP, FACE Division of Endocrinology Department of Internal Medicine WRNMMC 13 Aug 2018 OVERVIEW OF PRESENTATION Take Home Points Definition of Hypogonadism Clinical Manifestations
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Hormonal Control of Human Reproduction
 Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
Hormonal Control of Human Reproduction Bởi: OpenStaxCollege The human male and female reproductive cycles are controlled by the interaction of hormones from the hypothalamus and anterior pituitary with
4.04 Understand the Functions and Disorders of the ENDOCRINE SYSTEM Understand the functions and disorders of the endocrine system
 4.04 Understand the Functions and Disorders of the 4.04 Understand the Functions and Disorders of the What are the functions of the endocrine system? What are some disorders of the endocrine system? How
4.04 Understand the Functions and Disorders of the 4.04 Understand the Functions and Disorders of the What are the functions of the endocrine system? What are some disorders of the endocrine system? How
REFERRAL GUIDELINES ENDOCRINOLOGY
 REFERRAL GUIDELINES ENDOCRINOLOGY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
REFERRAL GUIDELINES ENDOCRINOLOGY Referral Form: The GP Referral Template is the preferred referral tool (previously known as the Victorian Statewide Referral Form) GP Referral Template This tool is housed
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018
 Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
Polycystic Ovary Syndrome HEATHER BURKS, MD OU PHYSICIANS REPRODUCTIVE MEDICINE SEPTEMBER 21, 2018 Learning Objectives At the conclusion of this lecture, learners should: 1) Know the various diagnostic
06-Mar-17. Premature menopause. Menopause. Premature menopause. Menstrual cycle oestradiol. Premature menopause. Prevalence ~1% Higher incidence:
 Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Menopause Dr Sonia Davison MBBS FRACP PhD Endocrinologist and Clinical Fellow, Jean Hailes for Women s Health Women s Health Research Program, Monash University = the last natural menstrual period depletion
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Hormone Replacement Therapy For Men Consultation Information
 Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Hormone Replacement Therapy For Men Consultation Information www.urologyaustin.com Biological Aging and Hormones As we age, a natural degeneration and aging of organs causes the levels of our hormones
Growth and DMD Endocrine aspects of care
 Growth and DMD Endocrine aspects of care Meilan Rutter, MB,BCh, FRACP Division of Endocrinology Cincinnati Children s Hospital Medical Center July 2007 Where are we now? Inactive Reactive Proactive CCHMC
Growth and DMD Endocrine aspects of care Meilan Rutter, MB,BCh, FRACP Division of Endocrinology Cincinnati Children s Hospital Medical Center July 2007 Where are we now? Inactive Reactive Proactive CCHMC
Overview. Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases. People Centred Positive Compassion Excellence
 Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Overview Osteoporosis and Metabolic Bone Disease Dr Chandini Rao Consultant Rheumatologist Bone Biology Osteoporosis Osteomalacia Paget s Disease Cases Bone Biology Osteoporosis Increased bone remodelling
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas: