Arboviral infections of the CNS: Japanese Encephalitis, West Nile, Dengue, Zika and co
|
|
|
- Abel Shaw
- 6 years ago
- Views:
Transcription

1 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Teaching Course 15 Neurological infections in travellers and immigrants - Level 3 Arboviral infections of the CNS: Japanese Encephalitis, West Nile, Dengue, Zika and co Tom Solomon Liverpool, United Kingdom tsolomon@liv.ac.uk
2 Conflict of interest: The author has no conflict of interest in relation to this manuscript Returning travellers and migrants from tropical areas present particular challenges in terms of neurological infections. On the one hand, they may be infected with a range of rare and exotic pathogens, on the other hand, the common and important causes must not be overlooked. Neurological infections are more common in the tropics than in the developed industrial world. A complex mixture of socioeconomic and environmental factors contribute to the increased incidence. Reasons for increased incidence of neurological disorders in the tropics Infectious neurological diseases the climate supports transmission of insect-borne pathogens (malaria, trypanosomiasis, arthropod-borne viruses). Environmental factors include the close proximity of homes to zoonotic infections. Vaccine-preventable diseases are more common (e.g. measles, tetanus, diphtheria, polio). There is also unregulated use of over-the-counter antibiotics, leading to the partial pretreatment of central nervous system (CNS) infections, which hampers diagnosis and therapy, and promotes the development of antibiotic resistance. 1
3 Poverty, overcrowding, poor sanitation and lack of education about disease risk factors and prevention are important. These may lead, for example, to cysticercosis and typhoid. Immunosuppression, particularly as a result of HIV, allows many other infections such as cryptococcal and tuberculous meningitis. Non-infectious neurological disorders trauma is more common in the tropics, especially road traffic accidents. Patterns of vascular disease are catching up with those in the developed world, but the usage of drugs to control them lags behind. Neurological syndromes Neurological diseases particularly infections can present with a range of syndromes. Encephalopathy a reduced level of consciousness from any cause (infectious, metabolic, vascular, traumatic). Meningism clinical signs of meningeal irritation (headache, neck stiffness, Kernig s sign; see below). Paralysis weakness of one or more limb, respiratory or bulbar muscles, which may be a result of damaged upper motor neurones, lower motor neurones, peripheral nerves, or muscles. Chronic neurological presentations insidious presentation over weeks or months, often with changes in personality, behaviour or other psychiatric illness. Fever may not be prominent, even with an infectious cause (Table 3.2). 2

4 Headache may be the only symptom (e.g. in cryptococcal meningitis). Other focal neurological signs including hemispheric signs, brainstem signs, seizures and movement disorders. Table 3.2 Causes of chronic neurological presentations in the tropics. Pathological processes These neurological syndromes are explained by a range of pathological processes. Encephalitis inflammation of the brain substance, usually in response to viral infection, but also in response to other pathogens. Meningitis inflammation of the meningeal membranes covering the brain, in response to bacterial, viral or fungal infection. Myelitis inflammation of the spinal cord. This may occur across the whole cord (causing transverse myelitis, which is often postinfectious) or be confined to the anterior horn cells. Neuropathy damage to peripheral nerves (e.g. Guillain Barré syndrome, diphtheria, leprosy, rabies, vitamin deficiencies). 3
 these cause pathology in the brain or spinal cord directly (by interrupting neuronal pathways), and indirectly (by causing localized swelling, raised intracranial pressure and brainstem herniation")
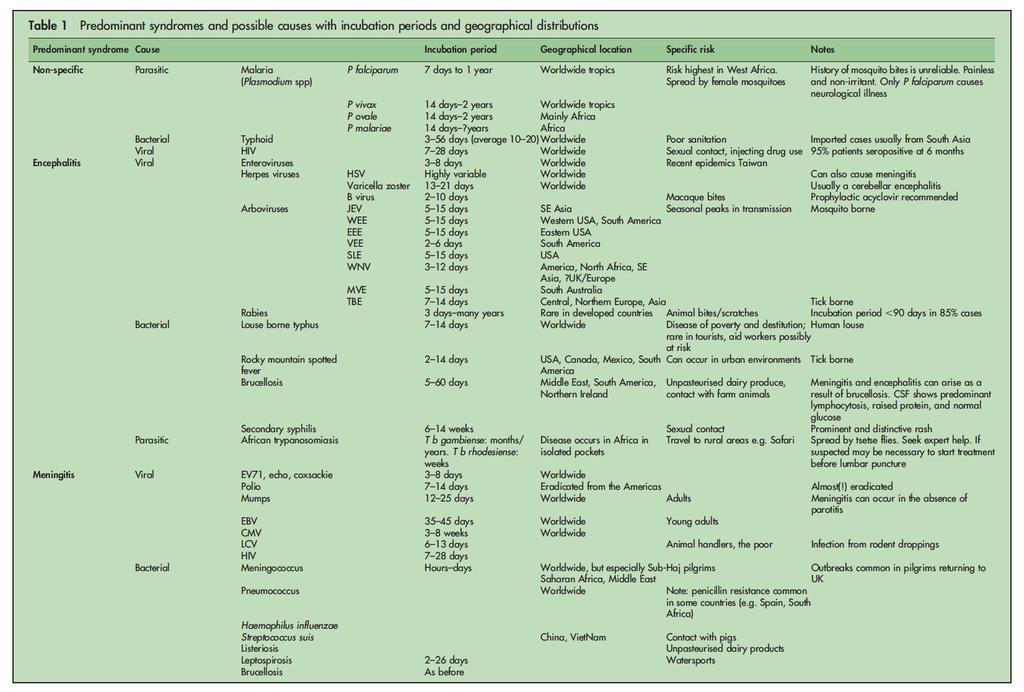
5 Space-occupying lesions (Table 3.3) these cause pathology in the brain or spinal cord directly (by interrupting neuronal pathways), and indirectly (by causing localized swelling, raised intracranial pressure and brainstem herniation syndromes). Typically, they present with focal signs or a chronic insidious deterioration. The neurological syndromes are caused by a wide range of bacterial, viral, parasitic and fungal pathogens (Table 1) 4
6 5

7 6 From J N Day and D G Lalloo. Neurological Syndromes and the Returning Traveller: An Approach to Differential Diagnosis J. Neurol. Neurosurg. Psychiatry 2004;75;i2-i9
8 Rapid assessment of patient with coma returning from the tropics 1 Stabilize the patient, and treat any immediately life-threatening conditions. Airways. Breathing give oxygen; intubate if breathing is inadequate or gag reflex impaired. Circulation establish venous access. Obtain blood for immediate bedside blood glucose test (hypoglycaemia?). Malaria film (look for parasites and pigment of partially treated malaria). FBC, U&E, blood cultures, arterial blood gases. Disability. Give intravenous (i.v.) glucose (e.g. 10% glucose 50 ml in adults, 5 ml/kg in children), irrespective of blood glucose. Give adults 100 mg thiamine i.v., especially if alcohol abuse is suspected. Immobilize cervical spinal cord if neck trauma is suspected. Rapidly assess AVPU scale (alert, responds to voice, to pain, or unresponsive). If patient responds to pain or is unresponsive, examine the pupils, eye movements, respiratory pattern, tone and posture for signs of cerebral herniation (see below). If herniation is suspected start treatment for this. If purpuric rash is present give penicillin or chloramphenicol (or third generation cephalosporin) for presumed meningococcal meningitis (after taking blood cultures). 7
9 Look for and treat generalized seizures, focal seizures and subtle motor seizures (mouth or finger twitching, or tonic eye deviation). 2 Take a history, while preliminary assessment and resuscitation proceeds. This is the single most useful tool in determining the cause of coma. In particular: Duration of onset of coma. Rapid onset (minutes hours) suggests a vascular cause, especially brainstem cerebrovascular accidents or subarachnoid haemorrhage. If preceded by hemispheric signs, then consider intracerebral haemorrhage. Coma caused by some infections (e.g. malaria, encephalitis) can also develop rapidly, especially when precipitated by convulsions. Intermediate onset (hours days) suggests diffuse encephalopathy (metabolic or, if febrile, infectious). Prolonged onset (days weeks) suggests tumours, abscess or chronic subdural haematoma (see Table 3.2). Any drugs? Any trauma? Important past medical history (e.g. hypertension)? Family history (e.g. tuberculosis)? Known epidemic area (e.g. viral encephalitis)? 8
10 3 Perform a rapid general medical examination, and in particular: Check pockets for drugs. Note temperature (febrile or hypothermia) and blood pressure (hypo- or hypertensive). Examine for signs of trauma (check ears and nose for blood or cerebrospinal fluid (CSF) leak). Smell the breath for alcohol or ketones (diabetes?). Examine the skin for: rash (meningococcal rash, dengue or other haemorrhagic fever, typhus, relapsing fever); needle marks of drug abuse; recent tick bite or eschar (tick-borne encephalitis, tick paralysis, tickborne typhus or relapsing fever); chancre, with or without circinate rash (trypanosomiasis, especially Trypanosoma rhodesiense); healed dog bite (rabies); or snake bite. Examine for lymphadenopathy (e.g. Winterbottom s sign of posterior cervical lymphadenopathy in African trypanosomiasis). Examine the fundi for papilloedema (long-standing raised intracranial pressure) or signs of hypertension. 9


11 4 Determine the coma score to allow subsequent changes to be accurately monitored. The scale in Box 3.1 is for adults and children over 5 years of age and in Box 3.2 for young children. 5 Neurological examination. A detailed description of the neurological examination is beyond the scope of this chapter. For most practical purposes the ability to recognize the following four clinical patterns (and combinations of them) will allow appropriate classification and subsequent investigation and treatment. Meningism with or without encephalopathy. Diffuse encephalopathies usually metabolic or infectious. Supratentorial focal damage (above the cerebellar tentorium) usually manifests as hemispheric signs. 10
12 Damage in the diencephalon or brainstem (midbrain, pons or medulla) may indicate a syndrome of cerebral herniation through the tentorial hiatus or the foramen magnum (Fig. 3.1). The importance of these syndromes is being increasingly recognized in non-traumatic coma (particularly that caused by infections). Although the level of brainstem damage is given in brackets below (and in Fig. 3.1), recognizing the presence or absence of brainstem signs, and in particular early signs of reversible damage, is usually more important than determining their exact localization. Assessment of the following five points allows most patients to be classified. 1 Check for neck stiffness (if no trauma), and Kernig s sign (extension of knee when hip is already flexed causes pain). 2 Examine pupil reaction to light (Fig. 3.1). A normal reaction (constriction) is seen in a diffuse encephalopathy. A unilateral large pupil is seen in herniation of the uncus of the temporal lobe. The pupils are reactive (small or mid-sized) in the diencephalic syndrome. Unreactive pupils occur in brainstem lesions (mid-sized in midbrain or pontine lesions; large in medullary lesions). Pinpoint pupils occur following opiate or organophosphate overdose, or in isolated pontine lesion. Other drugs can cause large unreactive pupils. 3 Assess eye movements (holding eyelids open if necessary). Spontaneous eye movements eyes spontaneously roving or eyes following indicates the brainstem is intact (a diencephalic syndrome or a diffuse encephalopathy). 11
13 Oculocephalic (doll s eye) reflex when rotating the head, the eyes normally deviate away from the direction of rotation. A normal response indicates that the brainstem is intact (diffuse encephalopathy). Reduced or absent responses occur in uncal herniation, brainstem damage or, rarely, deep metabolic coma. Oculovestibular reflex caloric response to water should be tested if the result of the oculocephalic reflex is unclear. Check that the eardrum is not perforated, then irrigate by injecting 20 ml ice-cold water. Nystagmus is the normal response and indicates psychogenic coma. Both eyes deviate towards the irrigated ear in coma with the brainstem intact. A reduced or absent response indicates an uncal syndrome or a damaged brainstem. 4 Assess breathing pattern. A normal pattern occurs in diffuse encephalopathy. Cheyne Stokes breathing and hyperventilation occur in reversible herniation syndromes. Shallow, ataxic or apnoeic respiration occurs in more severe syndromes (Fig. 3.1). Hyperventilation also occurs in acidosis or may be caused by aspiration pneumonia, which is common in coma. 5 Assess response to pain by applying painful stimulus to the supraorbital ridge and nail bed of each limb. Hemiparesis most often indicates supratentorial hemispheric focal pathology (other signs include asymmetry of tone and focal seizures), but also occurs in uncal herniation. 12
14 Decorticate posturing flexion of arms with extension of legs, indicating damage in the diencephalon, and decerebrate posturing (extension of arms and legs caused by midbrain/upper pontine damage) may both be reversible. No response, or leg flexion only, are more severe. Symmetrical posturing (decorticate or decerebrate) and hemiparetic focal signs are also occasionally seen in metabolic encephalopathies (e.g. hypoglycaemia; hepatic, uraemic or hypoxic coma; sedative drugs), cerebal malaria, and intra- or postictally. Other pointers to metabolic disease include asterixis, tremor and myoclonus preceding the onset of coma. Classification and further investigation of patients with coma At this stage, if the history, general examination and preliminary investigation have not made one diagnosis extremely likely, most comatose patients will fall into one of three categories, based on the presence or absence of meningism, supratentorial and brainstem signs. 1 Coma only (no hemispheric signs, brainstem signs or meningism sleeping beauties ). If patient is febrile (or has a history of fever), suspect CNS infection (especially cerebral malaria) or metabolic coma plus secondary aspiration pneumonia. If afebrile, coma is likely to be metabolic (hypoglycaemia, drugs, alcohol, diabetic ketoacidosis, toxins), psychogenic (test caloric response to water causes nystagmus), or, occasionally, resulting from subarachnoid haemorrhage or other cerebrovascular accident. 13
15 2 Coma with meningism, but no focal signs. If febrile, CNS infection (especially bacterial meningitis) is likely. If afebrile, subarachnoid haemorrhage is likely. 3 Coma with focal signs (with or without meningism). Decide if the signs are hemispheric signs, brainstem signs, or both. Hemispheric signs only. If febrile, consider CNS infection (especially encephalitis, bacterial meningitis, abscess, etc.). If afebrile, consider space-occupying lesion (Table 3.3), cerebrovascular accident or trauma. Brainstem signs only may be caused by either focal pathology within the brainstem (e.g. encephalitis) especially if markedly asymmetrical signs, or by herniation of the brainstem (through the foramen magnum) secondary to a diffuse process (e.g. diabetic ketoacidosis, or late bacterial meningitis) causing raised intracranial pressure. Hemispheric and brainstem signs may be a result of either a supratentorial lesion causing hemispheric signs and sufficient swelling to precipitate brainstem herniation (e.g. cerebral bleed, abscess) or patchy focal pathology in the hemispheres and brainstem (e.g. toxoplasmosis, viral encephalitis). Indications and contraindications for lumbar puncture in suspected CNS infections (Table 3.4) For many years lumbar puncture was performed in all patients with suspected CNS infections, in both the tropics and western industrialized nations. It has gone out of fashion in the latter, following concerns that it was being performed on patients with contraindications, and may have precipitated herniation. 14

16 In patients with a contraindication, treatment should be started and then a lumbar puncture reconsidered later. In many tropical settings in Africa and Asia, where CNS infections are very common, lumbar puncture is still considered an essential investigation. Here the benefits of accurate diagnosis and appropriate treatment may outweigh the theoretical risk of herniation, and even patients with relative contraindications often receive lumbar punctures with no apparent harm. Cerebrospinal fluid findings in CNS infections Although most patients with CNS infections will have findings that are straightforward to interpret, there may be considerable overlap (Table 3.5). Ideally, the decision about starting antibiotics should await the result of the lumbar puncture (if it is available quickly). However, antibiotics should be started immediately for patients with a typical meningococcal rash, because of the speed with which meningococcal 15

17 septicaemia can become fatal. In such patients, if it is certain that the rash is meningococcal it has been argued that the lumbar puncture is not necessary, because the diagnosis is already made, though others advocate always doing a lumbar puncture. Table 3.5 Cerebrospinal fluid (CSF) findings in central nervous system infections. 16
18 Further reading Kirkham FJ. Non-traumatic coma in children. Arch Dis Child 2001; 85: [An excellent review of pathophysiology and management.] Kneen R, Solomon T, Appleton RA. The role of lumbar punctures in CNS infections. Arch Dis Child 2001; 87: [Detailed discussion of the use of lumbar puncture.] J N Day and D G Lalloo. Neurological Syndromes and the Returning Traveller: An Approach to Differential Diagnosis J. Neurol. Neurosurg. Psychiatry 2004;75;i2-i9 17
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
CHAPTER 3. Neurological Presentations
 GBL3 11/27/03 3:43 PM Page 17 CHAPTER 3 Neurological Presentations Rapid assessment of patient with coma in the tropics, 19 Classification and further investigation of patients with coma, 23 Indications
GBL3 11/27/03 3:43 PM Page 17 CHAPTER 3 Neurological Presentations Rapid assessment of patient with coma in the tropics, 19 Classification and further investigation of patients with coma, 23 Indications
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
COMA & INTENSIVE CARE
 COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
CNS Infections. Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London. Hammersmith Acute Medicine 2011
 CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
CNS Infections Philip Gothard Consultant in Infectious Diseases Hospital for Tropical Diseases, London Hammersmith Acute Medicine 2011 Case 1 HISTORY 27y man Unwell 3 days Fever Headache Photophobia Previously
Aurora Health Care South Region EMS st Quarter CE Packet
 Name: Dept: Date: Aurora Health Care South Region EMS 2010 1 st Quarter CE Packet Meningitis Meningitis is an inflammatory disease of the leptomeninges. Leptomeninges refer to the pia matter and the arachnoid
Name: Dept: Date: Aurora Health Care South Region EMS 2010 1 st Quarter CE Packet Meningitis Meningitis is an inflammatory disease of the leptomeninges. Leptomeninges refer to the pia matter and the arachnoid
PAEDIATRIC ACUTE CARE GUIDELINE. Resuscitation Coma
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Resuscitation Coma Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Resuscitation Coma Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be
Advanced Concept of Nursing- II
 In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI) Advanced Concept of Nursing- II UNIT- VIII Advance Nursing Management Of neurovascular Diseases. Shahzad Bashir RN, BScN, DCHN,MScN
In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI) Advanced Concept of Nursing- II UNIT- VIII Advance Nursing Management Of neurovascular Diseases. Shahzad Bashir RN, BScN, DCHN,MScN
CHILD IN NON - TRAUMATIC COMA
 May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
May / 2018 PELC / SLCP 1 CHILD IN NON - TRAUMATIC COMA PELS May / 2018 PELC / SLCP 2 Objectives Recognize depressed mental status Know the causes of depressed mental status in children Assessment and workup
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
COPYRIGHT 2012 THE TRANSVERSE MYELITIS ASSOCIATION. ALL RIGHTS RESERVED
 The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
The Transverse Myelitis Association...advocating for those with acute disseminated encephalomyelitis, neuromyelitis optica, optic neuritis and transverse myelitis ACUTE DISSEMINATED ENCEPHALOMYELITIS (ADEM)
EVALUATION OF COMATOSE PATIENT. Prof. G. Zuliani
 EVALUATION OF COMATOSE PATIENT Prof. G. Zuliani Consciousness Two components of conscious behavior: Vigilance (arousal): appearance of wakefulness Awareness (content): the sum of cognitive and affective
EVALUATION OF COMATOSE PATIENT Prof. G. Zuliani Consciousness Two components of conscious behavior: Vigilance (arousal): appearance of wakefulness Awareness (content): the sum of cognitive and affective
Organic Mental Disorders. Organic Mental Disorders. Axes. Damrongsak Bulyalert Department of Internal Medicine
 Organic Mental Disorders Damrongsak Bulyalert Department of Internal Medicine www.metadon.net 1 Organic Mental Disorders In DSM (Diagnostic and Statistical Manual of Mental Disorders), OMD includes Delirium,
Organic Mental Disorders Damrongsak Bulyalert Department of Internal Medicine www.metadon.net 1 Organic Mental Disorders In DSM (Diagnostic and Statistical Manual of Mental Disorders), OMD includes Delirium,
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL
 YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
YALE-NEW HAVEN HOSPITAL CLINICAL ADMINISTRATIVE POLICY & PROCEDURE MANUAL Administrative Policy Title: Brain Death, Guidelines Determination of Death by Neurological Criteria in the Pediatric Patient Manual
The Neurologic Examination. John W. Engstrom, M.D. University of California San Francisco School of Medicine
 The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
COMA. DIAH MUSTIKA HW,SpS,KIC INTENSIVE CARE UNIT of EMERGENCY DEPARTMENT
 COMA DIAH MUSTIKA HW,SpS,KIC INTENSIVE CARE UNIT of EMERGENCY DEPARTMENT NAVAL HOSPITAL dr RAMELAN, SURABAYA DEFINITIONS Coma State of unresponsiveness to external or internal stimuli in which a patient
COMA DIAH MUSTIKA HW,SpS,KIC INTENSIVE CARE UNIT of EMERGENCY DEPARTMENT NAVAL HOSPITAL dr RAMELAN, SURABAYA DEFINITIONS Coma State of unresponsiveness to external or internal stimuli in which a patient
Central nervous system
 Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Central nervous system By Dr. Mohsen Dashti Clinical Medicine & Pathology 316 7 th Lecture Lecture outline Review of structure & function. Symptoms, signs & tests. Specific diseases. Review of structure
Dr Paul Holmes Guy s and St Thomas NHS Foundation Trust, London
 Dr Paul Holmes Guy s and St Thomas NHS Foundation Trust, London HIV and Lumbar punctures in 2018 Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals I have no competing interests Summary of
Dr Paul Holmes Guy s and St Thomas NHS Foundation Trust, London HIV and Lumbar punctures in 2018 Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals I have no competing interests Summary of
SHASTA COUNTY Health and Human Services Agency
 FROM: 530 229 8447 TO: 15302293984 08/06/14 12:30 Pg 1 of 5 especially SHASTA COUNTY Health and Human Services Agency Public Health 2650RreslauerWay Redding, CA 96001-4297 (530) 229-8484 FAX (530) 225-3743
FROM: 530 229 8447 TO: 15302293984 08/06/14 12:30 Pg 1 of 5 especially SHASTA COUNTY Health and Human Services Agency Public Health 2650RreslauerWay Redding, CA 96001-4297 (530) 229-8484 FAX (530) 225-3743
Clinical Information on West Nile Virus (WNV) Infection
 Infection") Clinical Information on West Nile Virus (WNV) Infection Introduction In 1999, West Nile Virus (WNV), an Old World flavivirus, producing a spectrum of disease including severe meningoencephalitis, appeared
Clinical Information on West Nile Virus (WNV) Infection Introduction In 1999, West Nile Virus (WNV), an Old World flavivirus, producing a spectrum of disease including severe meningoencephalitis, appeared
Altered Mental Status Basic Emergency Care Course
 Altered Mental Status Basic Emergency Care Course Objectives Recognize key history findings suggestive of different causes of altered mental status Recognize key physical findings suggestive of different
Altered Mental Status Basic Emergency Care Course Objectives Recognize key history findings suggestive of different causes of altered mental status Recognize key physical findings suggestive of different
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Below you will find information about diseases, the risk of contagion, and preventive vaccinations.
 Vaccinations Below you will find information about diseases, the risk of contagion, and preventive vaccinations. DTP - Diphtheria Tetanus Polio Yellow fever Hepatitis A Typhoid fever Cerebrospinal meningitis
Vaccinations Below you will find information about diseases, the risk of contagion, and preventive vaccinations. DTP - Diphtheria Tetanus Polio Yellow fever Hepatitis A Typhoid fever Cerebrospinal meningitis
Appendix 2 (as supplied by the authors): ICD codes to identify high-risk children
: ICD codes to identify high-risk children") Appendix 2 (as supplied by the authors): ICD codes to identify high-risk children ICD-9 codes to identify high risk children in physician claims database Category of condition Condition ICD-9 code Bacterial
Appendix 2 (as supplied by the authors): ICD codes to identify high-risk children ICD-9 codes to identify high risk children in physician claims database Category of condition Condition ICD-9 code Bacterial
Acute neurological syndromes
 Acute neurological syndromes Assoc.Prof. Murat Sayan Kocaeli Üniversitesi, Rutin PCR Lab. Sorumlu Öğt.Üyesi Yakın Doğu Üniversitesi, DESAM Kurucu Öğrt. Üyesi sayanmurat@hotmail.com 0533 6479020 Medical
Acute neurological syndromes Assoc.Prof. Murat Sayan Kocaeli Üniversitesi, Rutin PCR Lab. Sorumlu Öğt.Üyesi Yakın Doğu Üniversitesi, DESAM Kurucu Öğrt. Üyesi sayanmurat@hotmail.com 0533 6479020 Medical
Council of State and Territorial Epidemiologists Position Statement
 04-ID-01 Committee: Title: Infectious Disease Revision of the National Surveillance Case Definition of Diseases Caused by Neurotropic Domestic Arboviruses, Including the Addition to the NNDSS of Non-Neuroinvasive
04-ID-01 Committee: Title: Infectious Disease Revision of the National Surveillance Case Definition of Diseases Caused by Neurotropic Domestic Arboviruses, Including the Addition to the NNDSS of Non-Neuroinvasive
BRAIN HERNIATION S54 (1) Brain Herniation
 Brain Herniation") BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Neurologic Examination
 John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Class 9 th Why do we fall ill?
 Class 9 th Why do we fall ill? Health: health is a state of physical, mental and social well being. The health of all individuals is dependent on their physical environment, social environment, and their
Class 9 th Why do we fall ill? Health: health is a state of physical, mental and social well being. The health of all individuals is dependent on their physical environment, social environment, and their
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Dilemmas in the Management of Meningitis & Encephalitis HEADACHE AND FEVER. What is the best initial approach for fever, headache, meningisums?
 Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Dilemmas in the Management of Meningitis & Encephalitis Paul D. Holtom, MD Professor of Medicine and Orthopaedics USC Keck School of Medicine HEADACHE AND FEVER What is the best initial approach for fever,
Neurological Determination of Death Adult
 Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
Approved by: Vice President and Chief Medical Officer Neurological Determination of Death Adult Corporate Policy & Procedures Manual Number: VII-B-400 Date Approved June 9, 2015 Next Review (3 years from
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
APPROACH TO THE COMATOSE CHILD
 APPROACH TO THE COMATOSE CHILD Jimmy S. Lee 1. Background... 1 a) Definitions... 1 b) Background Physiology... 1 2. Questions to ask... 2 a) Timing... 2 b) Associated symptoms... 2 3. Differential diagnosis...
APPROACH TO THE COMATOSE CHILD Jimmy S. Lee 1. Background... 1 a) Definitions... 1 b) Background Physiology... 1 2. Questions to ask... 2 a) Timing... 2 b) Associated symptoms... 2 3. Differential diagnosis...
Paraparesis. Differential Diagnosis. Ran brauner, Tel Aviv university
 Paraparesis Differential Diagnosis Ran brauner, Tel Aviv university Definition Loss of motor power to both legs Paraparesis (paraplegia) refers to partial (- paresis) or complete (-plegia) loss of voluntary
Paraparesis Differential Diagnosis Ran brauner, Tel Aviv university Definition Loss of motor power to both legs Paraparesis (paraplegia) refers to partial (- paresis) or complete (-plegia) loss of voluntary
Post Travel Fever. Dr. Eyal Leshem. Center for Geographic Medicine Sheba Medical Center Tel Hashomer, Israel
 Post Travel Fever Dr. Eyal Leshem Center for Geographic Medicine Sheba Medical Center Tel Hashomer, Israel Introduction Fever in returned traveler: Trivial vs. life threatening infections Tropical and
Post Travel Fever Dr. Eyal Leshem Center for Geographic Medicine Sheba Medical Center Tel Hashomer, Israel Introduction Fever in returned traveler: Trivial vs. life threatening infections Tropical and
VISUAL REFLEXES. B. The oculomotor nucleus, Edinger-Westphal nucleus, and oculomotor nerve at level of the superior colliculus.
 Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
Introduction. Infections acquired by travellers
 Introduction The number of Australians who travel overseas has increased steadily over recent years and now between 3.5 and 4.5 million exits are made annually. Although many of these trips are to countries
Introduction The number of Australians who travel overseas has increased steadily over recent years and now between 3.5 and 4.5 million exits are made annually. Although many of these trips are to countries
Activity 1: Person s story
 Epilepsy Session outline Introduction to epilepsy. Assessment of epilepsy. Management of epilepsy. Follow-up of a person with epilepsy. Review or materials and skills. Activity 1: Person s story Present
Epilepsy Session outline Introduction to epilepsy. Assessment of epilepsy. Management of epilepsy. Follow-up of a person with epilepsy. Review or materials and skills. Activity 1: Person s story Present
DISORDERS OF THE NERVOUS SYSTEM
 DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
DISORDERS OF THE NERVOUS SYSTEM Bell Work What s your reaction time? Go to this website and check it out: https://www.justpark.com/creative/reaction-timetest/ Read the following brief article and summarize
Professor Michael Kossove
 Professor Michael Kossove Is this a new disease? No, but doctors only began noticing it in 2014. That s when dozens of children began showing up in hospitals unable to move their arms or legs. Ultimately,
Professor Michael Kossove Is this a new disease? No, but doctors only began noticing it in 2014. That s when dozens of children began showing up in hospitals unable to move their arms or legs. Ultimately,
Nervous System. Unit 6.6 (6 th Edition) Chapter 7.6 (7 th Edition)
 Chapter 7.6 (7 th Edition)") Nervous System Unit 6.6 (6 th Edition) Chapter 7.6 (7 th Edition) 1 Learning Objectives Identify the main parts (anatomy) of a neuron. Identify the 2 divisions of nervous system. Classify the major types
Nervous System Unit 6.6 (6 th Edition) Chapter 7.6 (7 th Edition) 1 Learning Objectives Identify the main parts (anatomy) of a neuron. Identify the 2 divisions of nervous system. Classify the major types
Case Classification West Nile Virus Neurological Syndrome (WNNS)
") WEST NILE VIRUS Case definition Case Classification West Nile Virus Neurological Syndrome (WNNS) CONFIRMED CASE West Nile Virus Neurological Syndrome (WNNS) Clinical criteria AND at least one of the confirmed
WEST NILE VIRUS Case definition Case Classification West Nile Virus Neurological Syndrome (WNNS) CONFIRMED CASE West Nile Virus Neurological Syndrome (WNNS) Clinical criteria AND at least one of the confirmed
Brain Death Determination: Outline. Definition. Brain Death Determination. Brain Death Determination. No conflict of interest
 No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
No conflict of interest : Outline Definition Definition Confounding factors Clinical examination Apnea test Confirmatory testing Communicating the diagnosis Ethical issues Brain death remains the preferred
D is for Disability Altered Mental Status in Children
 D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
D is for Disability Altered Mental Status in Children Joshua Ross, MD, FAAP Pediatric Emergency Medicine Emergency Care and Trauma Symposium June 22, 2015 Objectives Describe a basic approach to evaluating
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
IMAGING OF INTRACRANIAL INFECTIONS
 IMAGING OF INTRACRANIAL INFECTIONS Dr Carolina Kachramanoglou LYSHOLM DEPARTMENT OF NEURORADIOLOGY NATIONAL HOSPITAL FOR NEUROLOGY AND NEUROSURGERY Plan Introduce MR sequences that are useful in the diagnosis
IMAGING OF INTRACRANIAL INFECTIONS Dr Carolina Kachramanoglou LYSHOLM DEPARTMENT OF NEURORADIOLOGY NATIONAL HOSPITAL FOR NEUROLOGY AND NEUROSURGERY Plan Introduce MR sequences that are useful in the diagnosis
NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY
 & COOLING THERAPY") Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Background NEONATAL HYPOXIC-ISCHAEMIC ENCEPHALOPATHY (HIE) & COOLING THERAPY A perinatal hypoxic-ischaemic insult may present with varying degrees of neonatal encephalopathy, neurological disorder and
Encephalitis following Purified Chick-Embryo Cell Anti-Rabies Vaccination
 CASE REPORT JIACM 2003; 4(3): 251-9 Encephalitis following Purified Chick-Embryo Cell Anti-Rabies Vaccination NS Neki*, Ashok Khurana**, Ashok Duggal*** Abstract A case of encephalitis following purified
CASE REPORT JIACM 2003; 4(3): 251-9 Encephalitis following Purified Chick-Embryo Cell Anti-Rabies Vaccination NS Neki*, Ashok Khurana**, Ashok Duggal*** Abstract A case of encephalitis following purified
European Resuscitation Council
 European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
European Resuscitation Council Incidence of Trauma in Childhood Leading cause of death and disability in children older than one year all over the world Structured approach Primary survey and resuscitation
Chapter 16 - Depressed consciousness and coma
 Chapter 16 - Depressed consciousness and coma Episode overview: 1) List a broad differential diagnosis for coma 2) List GCS / Pediatric GCS 3) Describe the oculocephalic and oculovestibular reflex Wise
Chapter 16 - Depressed consciousness and coma Episode overview: 1) List a broad differential diagnosis for coma 2) List GCS / Pediatric GCS 3) Describe the oculocephalic and oculovestibular reflex Wise
Failure to wake. Robin S. Howard
 Failure to wake Robin S. Howard National Hospital for Neurology and Neurosurgery, Queen Square St. Thomas Hospital, Guys & St. Thomas NHS (Foundation) Trust Royal College of Physicians - November 2017
Failure to wake Robin S. Howard National Hospital for Neurology and Neurosurgery, Queen Square St. Thomas Hospital, Guys & St. Thomas NHS (Foundation) Trust Royal College of Physicians - November 2017
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function
 Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function") 1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
Unsupervised activity is a major risk factor for traumatic coma and its age-specific
 The assessment of patients in coma is a medical emergency. The cause should be identified and, where possible, corrected and the brain provided with appropriate protection to reduce further damage. It
The assessment of patients in coma is a medical emergency. The cause should be identified and, where possible, corrected and the brain provided with appropriate protection to reduce further damage. It
Appendix I (a) Human Surveillance Case Definition (Revised July 4, 2005)
 Human Surveillance Case Definition (Revised July 4, 2005)") Section A: Case Definitions Appendix I (a) Human Surveillance Case Definition (Revised July 4, 2005) The current Case Definitions were drafted with available information at the time of writing. Case Definitions
Section A: Case Definitions Appendix I (a) Human Surveillance Case Definition (Revised July 4, 2005) The current Case Definitions were drafted with available information at the time of writing. Case Definitions
Emergency Neurological Life Support Meningitis and Encephalitis
 Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
Emergency Neurological Life Support Meningitis and Encephalitis Version: 2.0 Last Updated: 19-Mar-2016 Checklist & Communication Meningitis and Encephalitis Table of Contents Emergency Neurological Life
The management of children and young people with an acute decrease in conscious level. Summary of Recommendations
 The management of children and young people with an acute decrease in conscious level Summary of Recommendations 3.1 Assessment of airway and airway protection in children with a decreased conscious level
The management of children and young people with an acute decrease in conscious level Summary of Recommendations 3.1 Assessment of airway and airway protection in children with a decreased conscious level
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS
 ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
ANTIBIOTIC GUIDELINES FOR THE MANAGEMENT OF COMMUNITY-ACQUIRED MENINGITIS AND ENCEPHALITIS IN ADULTS Version 4.0 Date ratified February 2009 Review date February 2011 Ratified by Authors Consultation Evidence
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University
 Dr Mubarak Abdelrahman Assistant Professor Jazan University") Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Pediatric emergencies (SHOCK & COMA) Dr Mubarak Abdelrahman Assistant Professor Jazan University SHOCK Definition: Shock is a syndrome = inability to provide sufficient oxygenated blood to tissues. Oxygen
Status Epilepticus in Children
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Status Epilepticus in Children. These podcasts are designed to give medical students an overview of key topics in pediatrics.
coma problems of consciousness
 coma problems of consciousness in children Kees Braun UMC Utrecht definitions consciousness state of full awareness of the self and one s relationship to the environment consiousness responsiveness level
coma problems of consciousness in children Kees Braun UMC Utrecht definitions consciousness state of full awareness of the self and one s relationship to the environment consiousness responsiveness level
Title: Revision to the Standardized Surveillance and Case Definition for Acute Flaccid Myelitis
 17-ID-01 Committee: Infectious Disease Title: Revision to the Standardized Surveillance and Case Definition for Acute Flaccid Myelitis I. Statement of the Problem Acute flaccid myelitis (AFM) is a syndrome
17-ID-01 Committee: Infectious Disease Title: Revision to the Standardized Surveillance and Case Definition for Acute Flaccid Myelitis I. Statement of the Problem Acute flaccid myelitis (AFM) is a syndrome
General information. El Salvador. Provided by NaTHNaC https://travelhealthpro.org.uk 07 Jul 2018
 El Salvador Capital City : "San Salvador" Official Language: "Spanish" Monetary Unit: "dollar (U.S.$)" General information The information on these pages should be used to research health risks and to
El Salvador Capital City : "San Salvador" Official Language: "Spanish" Monetary Unit: "dollar (U.S.$)" General information The information on these pages should be used to research health risks and to
10/6/2017. Notice. Traumatic Brain Injury & Head Trauma
 Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
Notice All EMS Live@Nite presentations will be recorded (both audio and video) and available for public viewing online. By participating in EMS Live@Nite, you consent to audio and video recording and its/their
PARA210 SUMMARY Hyperglycaemia (DKA & HHS) Brain & Nervous System Anatomy & Physiology Degenerative Neurological Disorders
 Brain & Nervous System Anatomy & Physiology Degenerative Neurological Disorders") PARA210 SUMMARY Page Topic 01-03 Diabetes Mellitus 04-05 Hyperglycaemia (DKA & HHS) 06-13 Toxicology 14-18 12 Lead ECG 19-21 Brain & Nervous System Anatomy & Physiology 22-24 Degenerative Neurological
PARA210 SUMMARY Page Topic 01-03 Diabetes Mellitus 04-05 Hyperglycaemia (DKA & HHS) 06-13 Toxicology 14-18 12 Lead ECG 19-21 Brain & Nervous System Anatomy & Physiology 22-24 Degenerative Neurological
Injuries to the head and spine
 Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Injuries to the head and spine Aaron J. Katz, AEMT-P, CIC www.es26medic.net 2013 Nervous System Two sub-systems Central Nervous System ( CNS ) Brain and spinal cord Peripheral Nervous System 12 cranial
Review. 1. How does a child s anatomy differ from an adult s anatomy?
 Chapter 32 Review Review 1. How does a child s anatomy differ from an adult s anatomy? A. The child s trachea is more rigid B. The tongue is proportionately smaller C. The epiglottis is less floppy in
Chapter 32 Review Review 1. How does a child s anatomy differ from an adult s anatomy? A. The child s trachea is more rigid B. The tongue is proportionately smaller C. The epiglottis is less floppy in
Delirium & Dementia. Nicholas J. Silvestri, MD
 Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
Delirium & Dementia Nicholas J. Silvestri, MD Outline Delirium vs. Dementia Neural pathways relating to consciousness Encephalopathy Stupor Coma Dementia Delirium vs. Dementia Delirium Abrupt onset Lasts
301 W. Alder, Missoula, MT or
 301 W. Alder, Missoula, MT 59802 406-258-4745 or 406-258-3363 Routine Immunizations are available on a walk-in basis: Mondays, Tuesdays, Thursdays, and Fridays from 9:00am to 4:30pm Wednesdays, 10:00am-4:30pm
301 W. Alder, Missoula, MT 59802 406-258-4745 or 406-258-3363 Routine Immunizations are available on a walk-in basis: Mondays, Tuesdays, Thursdays, and Fridays from 9:00am to 4:30pm Wednesdays, 10:00am-4:30pm
Moath Darweesh. Zaid Emad. Anas Abu -Humaidan
 3 Moath Darweesh Zaid Emad Anas Abu -Humaidan Introduction: First two lectures we talked about acute and chronic meningitis, which is considered an emergency situation. If you remember, CSF examination
3 Moath Darweesh Zaid Emad Anas Abu -Humaidan Introduction: First two lectures we talked about acute and chronic meningitis, which is considered an emergency situation. If you remember, CSF examination
Local Public Health Department. Communicable diseases Environmental health Chronic diseases Emergency preparedness Special programs
 Susan I. Gerber, MD Local Public Health Department Communicable diseases Environmental health Chronic diseases Emergency preparedness Special programs Public Health Reporting Ground Zero Local government
Susan I. Gerber, MD Local Public Health Department Communicable diseases Environmental health Chronic diseases Emergency preparedness Special programs Public Health Reporting Ground Zero Local government
4/24/2013. Haemophilus influenzae Meningitis. Neisseria Meningitis. Streptococcus pneumoniae Meningitis
 1 2 3 4 5 6 7 Chapter 22 Microbial Diseases of the Nervous System The Human Nervous System Meninges protect brain and spinal cord Dura mater: Outermost layer Arachnoid mater: Middle layer Subarachnoid
1 2 3 4 5 6 7 Chapter 22 Microbial Diseases of the Nervous System The Human Nervous System Meninges protect brain and spinal cord Dura mater: Outermost layer Arachnoid mater: Middle layer Subarachnoid
Myelitis= inflammation of the spinal cord
 Polio infection 1 Illustrate the epidemiology of the disease 2 Demonstrate the clinical features of polio infection 3 Enumerate the complications 4 Prevent and treat polio infection MUMPS 1 Identify the
Polio infection 1 Illustrate the epidemiology of the disease 2 Demonstrate the clinical features of polio infection 3 Enumerate the complications 4 Prevent and treat polio infection MUMPS 1 Identify the
Mosquitoborne Viral Diseases
 Mosquitoborne Viral Diseases Originally prepared by Tom J. Sidwa, D.V.M, M.P.H State Public Health Veterinarian Zoonosis Control Branch Manager Texas Department of State Health Services 1 AGENT Viruses
Mosquitoborne Viral Diseases Originally prepared by Tom J. Sidwa, D.V.M, M.P.H State Public Health Veterinarian Zoonosis Control Branch Manager Texas Department of State Health Services 1 AGENT Viruses
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Chapter Fifteen. Neurological Disorders
 Chapter Fifteen Neurological Disorders Causes of Neurological Disorders Head Injuries Tumors Seizures Drugs (primary effects, side effects, and withdrawal) Circulation Issues Circulation Issues STROKES!
Chapter Fifteen Neurological Disorders Causes of Neurological Disorders Head Injuries Tumors Seizures Drugs (primary effects, side effects, and withdrawal) Circulation Issues Circulation Issues STROKES!
Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases
 Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases are caused by bacteria. Pneumococcal bacteria (Streptococcus pneumoniae) are the
Pneumococcal Meningitis Meningitis is an inflammation of the lining around the brain and spinal cord. Most severe cases are caused by bacteria. Pneumococcal bacteria (Streptococcus pneumoniae) are the
Immunizations Offered
 Immunizations Offered Most vaccines commercially available in the United States are available at the health clinic. A partial list of available vaccines follows. For more information about specific vaccines
Immunizations Offered Most vaccines commercially available in the United States are available at the health clinic. A partial list of available vaccines follows. For more information about specific vaccines
The Child with Alterations in Cerebral Function
 The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS)
 Stroke (2 of 2) Seizures Altered Mental Status (AMS)") 1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
NICE guideline Draft for consultation, October 2009
 Bacterial meningitis and meningococcal septicaemia: management of bacterial meningitis and meningococcal septicaemia in children and young people younger than 16 years in primary and secondary care NICE
Bacterial meningitis and meningococcal septicaemia: management of bacterial meningitis and meningococcal septicaemia in children and young people younger than 16 years in primary and secondary care NICE
BBS2711 Virology. Central Nervous System (CNS) Viruses. Dr Paul Young, Department of Microbiology & Parasitology.
 Viruses. Dr Paul Young, Department of Microbiology & Parasitology.") BBS2711 Virology Central Nervous System (CNS) Viruses Dr Paul Young, Department of Microbiology & Parasitology. p.young@mailbox.uq.edu.au Viruses of the CNS Many human pathogenic viruses are capable of
BBS2711 Virology Central Nervous System (CNS) Viruses Dr Paul Young, Department of Microbiology & Parasitology. p.young@mailbox.uq.edu.au Viruses of the CNS Many human pathogenic viruses are capable of
Child Neurology Elective PL1 Rotation
 PL1 Rotation The neurology elective is available to first year residents in either a 2 or 4 week block rotation. The experience will include performing inpatient consultations, attending outpatient clinics
PL1 Rotation The neurology elective is available to first year residents in either a 2 or 4 week block rotation. The experience will include performing inpatient consultations, attending outpatient clinics
Class time required: Four forty minute class periods. Parts 1 and 4 could be assigned as homework but Parts 2 and 3 should be completed in class.
 Disease Detectives Core Concepts: Symptoms and laboratory tests can be used to diagnose diseases. Meningitis is a serious infection that can lead to permanent brain damage or death. A vaccine can prevent
Disease Detectives Core Concepts: Symptoms and laboratory tests can be used to diagnose diseases. Meningitis is a serious infection that can lead to permanent brain damage or death. A vaccine can prevent
Role of MRI in acute disseminated encephalomyelitis
 Original Research Article Role of MRI in acute disseminated encephalomyelitis Shashvat Modiya 1*, Jayesh Shah 2, C. Raychaudhuri 3 1 1 st year resident, 2 Associate Professor, 3 HOD and Professor Department
Original Research Article Role of MRI in acute disseminated encephalomyelitis Shashvat Modiya 1*, Jayesh Shah 2, C. Raychaudhuri 3 1 1 st year resident, 2 Associate Professor, 3 HOD and Professor Department
Cerebral malaria in children
 Cerebral malaria in children M. Chiara Stefanini Catholic University - Rome Malaria: epidemiology Global distribution of malaria transmission risk,, 2003 World malaria report, WHO, 2005 Estimated incidence
Cerebral malaria in children M. Chiara Stefanini Catholic University - Rome Malaria: epidemiology Global distribution of malaria transmission risk,, 2003 World malaria report, WHO, 2005 Estimated incidence
General information. Costa Rica. Resources. Provided by NaTHNaC https://travelhealthpro.org.uk
 Costa Rica Capital City : "San José" Official Language: "Spanish" Monetary Unit: "Costa Rican colón ( )" General information The information on these pages should be used to research health risks and to
Costa Rica Capital City : "San José" Official Language: "Spanish" Monetary Unit: "Costa Rican colón ( )" General information The information on these pages should be used to research health risks and to
A list of useful resources including advice on how to reduce the risk of certain health problems is available below.
 Honduras Capital City : "Tegucigalpa" Official Language: "Spanish" Monetary Unit: "lempira (L)" General Information The information on these pages should be used to research health risks and to inform
Honduras Capital City : "Tegucigalpa" Official Language: "Spanish" Monetary Unit: "lempira (L)" General Information The information on these pages should be used to research health risks and to inform