BRAIN HERNIATION S54 (1) Brain Herniation
|
|
|
- Austen Maxwell
- 6 years ago
- Views:
Transcription
 herniation... 2 Cingulate (s. Subfalcine) herniation... 7 INFRATENTORIAL MASSES... 8 Cerebellar Tonsillar herniation... 8 Upward Transtentorial herniation.")
 falx (cerebri) 2) tentorium (cerebelli).")
1 BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal (s. Lateral Mass) herniation... 2 Cingulate (s. Subfalcine) herniation... 7 INFRATENTORIAL MASSES... 8 Cerebellar Tonsillar herniation... 8 Upward Transtentorial herniation... 9 HERNIATION AFTER LUMBAR PUNCTURE... 9 INVESTIGATIONS... 9 TREATMENT PATHOPHYSIOLOGY cranial cavity is divided into compartments by semirigid, densely fibrous folds of dura mater: 1) falx (cerebri) 2) tentorium (cerebelli). herniation occurs when brain is subjected to PRESSURE GRADIENTS that cause portions of it to flow from one compartment to another. pressure gradients are created by mass lesions (often surrounded by extensive edema). injudicious use of hyposmolar 5% dextrose IV often is sufficient to produce abrupt increase in brain edema and herniation. arteries and veins are relatively fixed in space - moving brain portions lose blood supply. in lateral herniation, hernia itself may compress or distort vessels. herniation produces dysfunction in white matter pathways (via geometrical distortion of pathways distension or compression); extracerebral structures (esp. CN3) are also susceptible to distortion. brain tissue is injured along free edges of dural reflections across which it is squeezed. (1) CINGULATE (SUBFALCINE) HERNIATION under falx cerebri. (2) CENTRAL (DOWNWARD TRANSTENTORIAL) HERNIATION through tentorial notch. (3) UNCAL (LATERAL MASS) HERNIATION over edge of tentorium.
2 BRAIN HERNIATION S54 (2) (4) CEREBELLAR TONSILLAR HERNIATION through foramen magnum. (5) TRANSCALVARIAL HERNIATION - swollen brain herniates through any defect in dura & skull. (2) (4) types may cause death through brainstem compression. Cushing's triad is response to diminished brain stem perfusion, regardless of etiology. TYPES OF HERNIATION All types may have nonspecific symptoms of increased ICP (headache, vomiting, hypertension, bradycardia, papilledema, CN6 palsy, transient visual obscurations, alterations in consciousness). N.B. syndromes can develop over hours or minutes! SUPRATENTORIAL MASSES CENTRAL (s. DOWNWARD TRANSTENTORIAL) herniation - DIENCEPHALON symmetrically moves caudally through tentorial notch whole brainstem is compressed toward foramen magnum stretch on paramedian branches of basilar artery. ETIOLOGY - diffuse brain swelling, centrally located supratentorial mass (or multiple bilateral masses). CLINICAL FEATURES - ROSTROCAUDAL neurologic deterioration: 1. RF dysfunction - progressive alteration of consciousness - earliest warning! 2. Diencephalic stage (still reversible!): 1) pinpoint reactive pupils (loss of sympathetic output from hypothalamus), roving eye movements. 2) many individuals have hemiparesis before herniation; as diencephalic stage evolves, contralateral hemiplegia worsens with homolateral limbs developing paratonic resistance to movement bilateral hyperreflexia and Babinski responses decorticate posturing. 3) frequent yawns and sighs Cheyne-Stokes respiration. 3. Midbrain stage (reflects infarction rather than reversible ischemia and compression prognosis poor): 1) pupils enlarge to midposition and become fixed, disconjugate gaze with failure to adduct (internuclear ophthalmoplegia). 2) decerebrate posturing. 3) central neurogenic hyperventilation. 4. Pontine stage impairment of oculocephalic and oculovestibular reflexes, rapid shallow respirations, flaccid extremities with bilateral Babinski responses. 5. Medullary stage flaccidity, Cushing's triad pupils dilate, hypotension, slow irregular respirations apnea, death. N.B. coma may develop before eye signs appear! UNCAL (s. LATERAL MASS) herniation - impaction of ANTERIOR MEDIAL TEMPORAL GYRUS into anterior portion of tentorial opening (into ambient cistern surrounding midbrain). ETIOLOGY - expanding unilateral, supratentorial mass.
3 CLINICAL FEATURES BRAIN HERNIATION S54 (3) 1) CN3 palsy: a) 80-85% - ipsilateral (CN3 is compressed against tentorial notch by inferomedial temporal lobe). N.B. pupillary fibers are located most peripherally in nerve, and are primarily damaged - prominent early sign is FIXED LARGE PUPIL! (level of consciousness may still not be altered!); later complete CN3 paralysis develops (ptosis and lateral eye deviation). b) 15% - contralateral or bilateral (may relate to midbrain ischemia as brainstem moves away from basilar artery). Mydriasis is most reliable sign for determining side of hematoma (correct in 85% cases) CN3 palsy often takes many months to resolve once pressure is relieved. 2) PCA may be compressed against tentorium, producing homonymous hemianopia. 3) as diencephalon begins to shift laterally away from mass, consciousness begins to diminish; midbrain compression causes coma. N.B. early depression of consciousness correlates more with lateral brain displacement than with transtentorial herniation DIASCHISIS - function inhibition produced by acute focal disturbance in brain portion at distance from original injury, but anatomically connected with it through fiber tracts (e.g. sudden large unilateral lesion functionally disrupts contralateral hemisphere coma). 4) ipsilateral hemiplegia (contralateral corticospinal tract in cerebral peduncle is compressed against tentorium edge - KERNOHAN notch* phenomenon) false localization of primary lesion! *notch - deep indentation of crus cerebri by free edge of tentorium described in Kernohan and Woltman's 1929 article N.B. hemiparesis in 50% cases is contralateral! Hemiplegia is not as accurate localizing sign as is mydriasis (50% vs %) 5) eventually (if uncal syndrome is allowed to progress), brainstem dysfunction: bilaterally fixed pupils, ophthalmoplegia, loss of brainstem reflexes. breathing (normal hyperventilation ataxic). bilateral decerebrate posturing (decorticate posturing is not usually seen), progressive unresponsiveness. circulating collapse and death. NEUROIMAGING Best diagnosed by evaluating CSF spaces around midbrain (MESENCEPHALIC CISTERNS) - absence or occlusion of mesencephalic cisterns usually indicates dislocation of supratentorial structures below tentorial notch! early only enlargement of ipsilateral perimesencephalic cistern (opposite perimesencephalic cistern is compressed from lateral movement of brainstem); later transtentorial movement of temporal lobe (both perimesencephalic cisterns are compressed); uncus and hippocampus are most medial portions of temporal lobe, they are first structures to cross tentorial edge. movement of more posterior aspects of medial temporal lobe may compress posterior cerebral artery ischemia in medial temporal lobe and sometimes in occipital lobe (hemianopsia).

: herniation displaces")
4 BRAIN HERNIATION S54 (4) N.B. consciousness occurs with moderate lateral shifts at level of diencephalon (when there is only minimal vertical displacement of structures near tentorial opening, i.e. well before downward herniation is evident on neuroimaging). 3-5 mm horizontal displacement of pineal body from midline corresponds to drowsiness; 5-8 mm corresponds to stupor; > 8 mm corresponds to coma. aqueductal obstruction may raise supratentorial pressure further. progression of transtentorial herniation is often accompanied by DURET hemorrhages (linear or flame-shaped hemorrhages in midline and paramedian regions of midbrain and pons): herniation displaces brainstem downward, stretching medial perforating branches of basilar artery (as artery is tethered to circle of Willis)

 >> Source of picture: Klatt, MD)")
5 BRAIN HERNIATION S54 (5) Source of picture: WebPath - The Internet Pathology Laboratory for Medical Education (by Edward C. Klatt, MD) >> Source of picture: WebPath - The Internet Pathology Laboratory for Medical Education (by Edward C. Klatt, MD) >> Arrow shows strangulation groove:

 >>")
6 BRAIN HERNIATION S54 (6) Source of picture: WebPath - The Internet Pathology Laboratory for Medical Education (by Edward C. Klatt, MD) >> Arrow shows strangulation groove: Source of picture: WebPath - The Internet Pathology Laboratory for Medical Education (by Edward C. Klatt, MD) >>
 herniation - MEDIAL FRONTAL STRUCTURES (e.g.")


7 BRAIN HERNIATION S54 (7) CINGULATE (s. SUBFALCINE) herniation - MEDIAL FRONTAL STRUCTURES (e.g. cingulate gyrus) herniate beneath falx compression on internal cerebral veins, ipsilateral anterior cerebral artery. ETIOLOGY - frontal lobe masses. CLINICAL FEATURES 1) signs related to mass itself 2) signs related to ICP 3) rarely, ischemia in ipsilateral anterior cerebral artery (loss of function in opposite leg, loss of bladder control). does not affect consciousness!
. CEREBELLAR TONSILLAR herniation - CEREBELLAR TONSILS pushed through foramen magnum. ETIOLOGY - posterior fossa (infratentorial) masses.")
8 BRAIN HERNIATION S54 (8) INFRATENTORIAL MASSES infratentorial compartment is much smaller than 2 supratentorial compartments - compensatory mechanisms are exhausted much more quickly (tolerated volume increases are much smaller). CEREBELLAR TONSILLAR herniation - CEREBELLAR TONSILS pushed through foramen magnum. ETIOLOGY - posterior fossa (infratentorial) masses. CLINICAL FEATURES - medulla compression: 1) stiff neck (due to tension of dura mater around cerebellar pressure cone). 2) flaccid quadriplegia (bilateral compression of corticospinal tracts) 3) apnea and circulatory collapse (as medulla is impinged) secondary coma (medullary RF has little direct role in arousal!). mass itself may compress-destroy brainstem ( pinpoint pupils, disconjugate eye movements, etc). mortality 70% Note cone shape of tonsils around medulla:
 >> UPWARD TRANSTENTORIAL herniation - CONTENTS OF POSTERIOR FOSSA herniate through tentorial opening into diencephalic region.")
9 BRAIN HERNIATION S54 (9) Source of picture: WebPath - The Internet Pathology Laboratory for Medical Education (by Edward C. Klatt, MD) >> UPWARD TRANSTENTORIAL herniation - CONTENTS OF POSTERIOR FOSSA herniate through tentorial opening into diencephalic region. ETIOLOGY - posterior fossa (infratentorial) masses + ventriculostomy. posterior fossa masses usually herniate caudally because obstructive hydrocephalus they produce prevents pressure gradient across tentorial opening. N.B. obstructive hydrocephalus is particularly common complication of posterior fossa mass! ventriculostomy allows pressure gradient to quickly build up. neurosurgeons prepare patient for emergent posterior fossa decompression just before performing ventriculostomy in case this problem occurs. CLINICAL FEATURES - midbrain compression: 1) rapid decline in level of consciousness 2) upward gaze paresis; other oculomotor signs. superior cerebellar artery ischemia ataxia. HERNIATION after LUMBAR PUNCTURE CSF removal lowers lumbar spinal canal pressure increased gradient between cranial and lumbar compartments ROSTROCAUDAL HERNIATION: a) TRANSTENTORIAL b) CEREBELLAR TONSILLAR. 50% patients lose consciousness immediately after LP. in 50% cases opening lumbar pressure is normal; 2/3 patients have no papilledema. general risk of herniation after lumbar puncture is 1.2-3%. preventive measures: see Op3 p.! 1) careful neurologic examination & CT before LP. 2) small-caliber spinal needles. 3) aggressive concurrent use of ICP-lowering agents. INVESTIGATIONS
10 BRAIN HERNIATION S54 (10) CT findings that suggest unequal pressure between intracranial compartments: 1) lateral shift of midline structures 2) loss of suprachiasmatic, circum-mesencephalic, superior cerebellar and quadrigeminal plate cisterns with sparing of ambient cisterns. 3) shift or obliteration of 4 th ventricle 4) posterior fossa mass (strong contraindication to lumbar puncture!). CT may miss cerebellar tonsillar herniation due to beam hardening artifact at level of foramen magnum. Angiographic signs: subfalcine herniation displacement of ACA or internal cerebral veins across midline; transtentorial herniation medial displacement of anterior choroidal artery; tonsillar herniation displacement of PICA branches below foramen magnum. TREATMENT Herniation must be recognized and treated immediately (to prevent irreversible brain damage)! 1. Temporary measures to lower ICP: see S50 p. 1) hyperventilation. 2) MANNITOL. 3) DEXAMETHASONE. 2. Neurosurgical intervention (evacuation of mass). BIBLIOGRAPHY see p. S50 Viktor s Notes for the Neurosurgery Resident Please visit website at
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
The dura is sensitive to stretching, which produces the sensation of headache.
 Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
Dural Nerve Supply Branches of the trigeminal, vagus, and first three cervical nerves and branches from the sympathetic system pass to the dura. Numerous sensory endings are in the dura. The dura is sensitive
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
Pathological reaction to disease
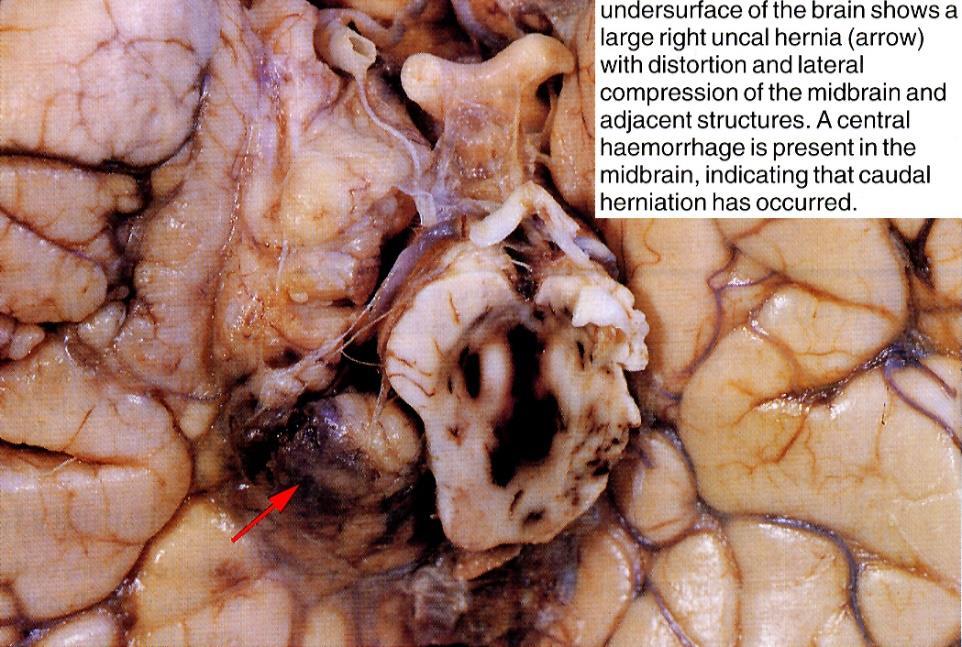
 Chapter1 Pathological reaction to disease Normal anatomy Figures 1.1 1.6 2 4 Brain swelling and internal herniation Figures 1.7 1.15 5 9 Epilepsy Figures 1.16 1.18 9 10 Cerebellar atrophy Figures 1.19
Chapter1 Pathological reaction to disease Normal anatomy Figures 1.1 1.6 2 4 Brain swelling and internal herniation Figures 1.7 1.15 5 9 Epilepsy Figures 1.16 1.18 9 10 Cerebellar atrophy Figures 1.19
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
VISUAL REFLEXES. B. The oculomotor nucleus, Edinger-Westphal nucleus, and oculomotor nerve at level of the superior colliculus.
 Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Brain ميهاربا لض اف دمح ا د The Meninges 1- Dura Mater of the Brain endosteal layer does not extend meningeal layer falx cerebri tentorium cerebelli
 .احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
.احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
The Skull, the Brain, the Meninges, and the Blood Supply of the Brain Relative to Trauma and Intracranial 14Hemorrhage
 The Nervous System The Skull, the Brain, the Meninges, and the Blood Supply of the Brain Relative to Trauma and Intracranial 14Hemorrhage Chapter Outline The Skull 213 The Thinnest Part of the Lateral
The Nervous System The Skull, the Brain, the Meninges, and the Blood Supply of the Brain Relative to Trauma and Intracranial 14Hemorrhage Chapter Outline The Skull 213 The Thinnest Part of the Lateral
CSF. Lumbar punction. CSF Cerebrospinal fluid - CSF
 CSF Cerebrospinal fluid - CSF Clear and colorless liquid in ventricles, cisterns and subarachnoidal spaces of brain and spinal cord CSF Production secretion chorioid. plexus in ventricles Resorbtion subarachnoid.
CSF Cerebrospinal fluid - CSF Clear and colorless liquid in ventricles, cisterns and subarachnoidal spaces of brain and spinal cord CSF Production secretion chorioid. plexus in ventricles Resorbtion subarachnoid.
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Lecture 4 The BRAINSTEM Medulla Oblongata
 Lecture 4 The BRAINSTEM Medulla Oblongata Introduction to brainstem 1- Medulla oblongata 2- Pons 3- Midbrain - - - occupies the posterior cranial fossa of the skull. connects the narrow spinal cord
Lecture 4 The BRAINSTEM Medulla Oblongata Introduction to brainstem 1- Medulla oblongata 2- Pons 3- Midbrain - - - occupies the posterior cranial fossa of the skull. connects the narrow spinal cord
b. The groove between the two crests is called 2. The neural folds move toward each other & the fuse to create a
 Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Head & Brain Trauma. Presented By: Steven Jones, NREMT-P
 Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Head & Brain Trauma Presented By: Steven Jones, NREMT-P Head & Brain Trauma ~ 4 million head injuries in US per year ~ 450,000 require hospitalization Most are minor injuries Major head injury most common
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
features of CNS pathology
 سالي ابو رمان Characteristic features of CNS pathology Important notes : - In this sheet I arranged slides within what the doctor said plus what is written in the book, hopefully it will be helpful and
سالي ابو رمان Characteristic features of CNS pathology Important notes : - In this sheet I arranged slides within what the doctor said plus what is written in the book, hopefully it will be helpful and
Slide 1. Slide 2. Slide 3. Tomography vs Topography. Computed Tomography (CT): A simplified Topographical review of the Brain. Learning Objective
: A simplified Topographical review of the Brain. Learning Objective") Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Multiple cranial nerve signs from supratentorial tumors
 Multiple cranial nerve signs from supratentorial tumors CHARLES W. NEEDHAM, M.D., (~ILLES BERTRAND, M.D., AND S. TERENCE MYLES, M.D. Department o/neurology and Neurosurgery, McGill University, and the
Multiple cranial nerve signs from supratentorial tumors CHARLES W. NEEDHAM, M.D., (~ILLES BERTRAND, M.D., AND S. TERENCE MYLES, M.D. Department o/neurology and Neurosurgery, McGill University, and the
M555 Medical Neuroscience Lab 1: Gross Anatomy of Brain, Crainal Nerves and Cerebral Blood Vessels
 M555 Medical Neuroscience Lab 1: Gross Anatomy of Brain, Crainal Nerves and Cerebral Blood Vessels Anatomical Directions Terms like dorsal, ventral, and posterior provide a means of locating structures
M555 Medical Neuroscience Lab 1: Gross Anatomy of Brain, Crainal Nerves and Cerebral Blood Vessels Anatomical Directions Terms like dorsal, ventral, and posterior provide a means of locating structures
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Medical Neuroscience Tutorial Notes
 Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Department of Cognitive Science UCSD
 Department of Cognitive Science UCSD Verse 1: Neocortex, frontal lobe, Brain stem, brain stem, Hippocampus, neural node, Right hemisphere, Pons and cortex visual, Brain stem, brain stem, Sylvian fissure,
Department of Cognitive Science UCSD Verse 1: Neocortex, frontal lobe, Brain stem, brain stem, Hippocampus, neural node, Right hemisphere, Pons and cortex visual, Brain stem, brain stem, Sylvian fissure,
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Ventricles, CSF & Meninges. Steven McLoon Department of Neuroscience University of Minnesota
 Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
Chapter 3. Structure and Function of the Nervous System. Copyright (c) Allyn and Bacon 2004
 Allyn and Bacon 2004") Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
Cerebral hemisphere. Parietal Frontal Occipital Temporal
 Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
Cerebral hemisphere Sulcus / Fissure Central Precental gyrus Postcentral gyrus Lateral (cerebral) Parieto-occipital Cerebral cortex Frontal lobe Parietal lobe Temporal lobe Insula Amygdala Hippocampus
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
coma in children Kees Braun UMC Utrecht
 a diagnostic approach to coma in children Kees Braun UMC Utrecht free pdf: Google search Plum and Posner s diagnosis of stupor and coma pdf first hit definitions consciousness state of full awareness
a diagnostic approach to coma in children Kees Braun UMC Utrecht free pdf: Google search Plum and Posner s diagnosis of stupor and coma pdf first hit definitions consciousness state of full awareness
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM
 Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST
 BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST Steven L. Galetta, MD NYU Langone Medical Center New York, NY I. Anatomical Considerations The brain stem is about the size of a fat forefinger and
BRAINSTEM SYNDROMES OF NEURO-OPHTHALMOLOGICAL INTEREST Steven L. Galetta, MD NYU Langone Medical Center New York, NY I. Anatomical Considerations The brain stem is about the size of a fat forefinger and
coma problems of consciousness
 coma problems of consciousness in children Kees Braun UMC Utrecht definitions consciousness state of full awareness of the self and one s relationship to the environment consiousness responsiveness level
coma problems of consciousness in children Kees Braun UMC Utrecht definitions consciousness state of full awareness of the self and one s relationship to the environment consiousness responsiveness level
Brain Meninges, Ventricles and CSF
 Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Brain Meninges, Ventricles and CSF Lecture Objectives Describe the arrangement of the meninges and their relationship to brain and spinal cord. Explain the occurrence of epidural, subdural and subarachnoid
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
For Emergency Doctors. Dr Suzanne Smallbane November 2011
 For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
For Emergency Doctors Dr Suzanne Smallbane November 2011 A: Orbit B: Sphenoid Sinus C: Temporal Lobe D: EAC E: Mastoid air cells F: Cerebellar hemisphere A: Frontal lobe B: Frontal bone C: Dorsum sellae
A GLANCE ON NEUROLOGICAL EMERGENCIES. Baystate Medical Center
 A GLANCE ON NEUROLOGICAL EMERGENCIES Baystate Medical Center Anthony Shamoun, MSN, RN, ACNP-BC, CCNS Clinical Nurse Specialist/Nurse Educator anthony.shamoun@bhs.org Outline I. Neurological Examination
A GLANCE ON NEUROLOGICAL EMERGENCIES Baystate Medical Center Anthony Shamoun, MSN, RN, ACNP-BC, CCNS Clinical Nurse Specialist/Nurse Educator anthony.shamoun@bhs.org Outline I. Neurological Examination
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018
 Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Blood Supply of Brain and Spinal Cord Arterial Supply of Brain The brain receives blood
Neuroanatomy Dr. Maha ELBeltagy Assistant Professor of Anatomy Faculty of Medicine The University of Jordan 2018 Blood Supply of Brain and Spinal Cord Arterial Supply of Brain The brain receives blood
BRAIN STEM AND CEREBELLUM..
 Lecture Title: BRAIN STEM AND CEREBELLUM.. (CNS Block, Radiology) Dr. Hamdy Hassan Ass.Prof. Consultant Radiology Department KKHU King Saud University Lecture Objectives.. Students at the end of the lecture
Lecture Title: BRAIN STEM AND CEREBELLUM.. (CNS Block, Radiology) Dr. Hamdy Hassan Ass.Prof. Consultant Radiology Department KKHU King Saud University Lecture Objectives.. Students at the end of the lecture
Nervous System The Brain and Spinal Cord Unit 7b
 Nervous System The Brain and Spinal Cord Unit 7b Chetek High School Mrs. Michaelsen 9.12 Meninges A. Meninges 1. The organs of the CNS are covered by membranes a. The meninges are divided into 3 layers:
Nervous System The Brain and Spinal Cord Unit 7b Chetek High School Mrs. Michaelsen 9.12 Meninges A. Meninges 1. The organs of the CNS are covered by membranes a. The meninges are divided into 3 layers:
OBJECTIVES. At the end of the lecture, students should be able to: List the cerebral arteries.
 DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
DR JAMILA EL MEDANY OBJECTIVES At the end of the lecture, students should be able to: List the cerebral arteries. Describe the cerebral arterial supply regarding the origin, distribution and branches.
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
Primary pontine haemorrhage: clinical and computed tomographic correlations
 Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:346-352 Primary pontine haemorrhage: clinical and computed tomographic correlations LEON A WESBERG From the Department of Neurology and Psychiatry
Journal of Neurology, Neurosurgery, and Psychiatry 1986;49:346-352 Primary pontine haemorrhage: clinical and computed tomographic correlations LEON A WESBERG From the Department of Neurology and Psychiatry
DEVELOPMENT OF BRAIN
 Ahmed Fathalla OBJECTIVES At the end of the lecture, students should: List the components of brain stem. Describe the site of brain stem. Describe the relations between components of brain stem & their
Ahmed Fathalla OBJECTIVES At the end of the lecture, students should: List the components of brain stem. Describe the site of brain stem. Describe the relations between components of brain stem & their
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16
 The Brain Chapter 14 and select portions of Chapter 16") Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Brain and Cranial Nerves (Ch. 15) Human Anatomy lecture. caudal = toward the spinal cord)
 Human Anatomy lecture. caudal = toward the spinal cord)") Insight: Some cranial nerve disorders Brain and Cranial Nerves (Ch. 15) Human Anatomy lecture I. Overview (Directional terms: rostral = toward the forehead caudal = toward the spinal cord) A. 3 Major parts
Insight: Some cranial nerve disorders Brain and Cranial Nerves (Ch. 15) Human Anatomy lecture I. Overview (Directional terms: rostral = toward the forehead caudal = toward the spinal cord) A. 3 Major parts
Upward spinal coning: impaction of occult spinal tumours following relief of hydrocephalus
 Journal of Neurology, Neurosurgery, and Psychiatry 1984;47: 386-390 Upward spinal coning: impaction of occult spinal tumours following relief of hydrocephalus RASHID JOOMA, RICHARD D HAYWARD From the Departments
Journal of Neurology, Neurosurgery, and Psychiatry 1984;47: 386-390 Upward spinal coning: impaction of occult spinal tumours following relief of hydrocephalus RASHID JOOMA, RICHARD D HAYWARD From the Departments
Anatomically and functionally the brain is the most complex
 CHAPTER 37 Alterations in Brain Function Brain Injury Mechanisms of Brain Injury Hypoxia and Ischemia Excitatory Amino Acid Injury Cerebral Edema Increased Intracranial Volume and Pressure Brain Herniation
CHAPTER 37 Alterations in Brain Function Brain Injury Mechanisms of Brain Injury Hypoxia and Ischemia Excitatory Amino Acid Injury Cerebral Edema Increased Intracranial Volume and Pressure Brain Herniation
Dissection of the Sheep Brain
 Dissection of the Sheep Brain Laboratory Objectives After completing this lab, you should be able to: 1. Identify the main structures in the sheep brain and to compare them with those of the human brain.
Dissection of the Sheep Brain Laboratory Objectives After completing this lab, you should be able to: 1. Identify the main structures in the sheep brain and to compare them with those of the human brain.
Chiari Malformations. Google. Objectives Seventh Annual NKY TBI Conference 3/22/13. Kerry R. Crone, M.D.
 Chiari Malformations Kerry R. Crone, M.D. Professor of Neurosurgery and Pediatrics University of Cincinnati College of Medicine University of Cincinnati Medical Center Cincinnati Children s Hospital Medical
Chiari Malformations Kerry R. Crone, M.D. Professor of Neurosurgery and Pediatrics University of Cincinnati College of Medicine University of Cincinnati Medical Center Cincinnati Children s Hospital Medical
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Unit 18: Cranial Cavity and Contents
 Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Unit 18: Cranial Cavity and Contents Dissection Instructions: The calvaria is to be removed without damage to the dura mater which is attached to the inner surface of the calvaria. Cut through the outer
Spontaneous Intracranial Hypotension Diagnosis and Treatment
 Spontaneous Intracranial Hypotension Diagnosis and Treatment John W. Engstrom MD, Philip R. Weinstein MD, and William P. Dillon M.D. University of California, San Francisco Spontaneous Intracranial Hypotension
Spontaneous Intracranial Hypotension Diagnosis and Treatment John W. Engstrom MD, Philip R. Weinstein MD, and William P. Dillon M.D. University of California, San Francisco Spontaneous Intracranial Hypotension
Biological Bases of Behavior. 3: Structure of the Nervous System
 Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
Biological Bases of Behavior 3: Structure of the Nervous System Neuroanatomy Terms The neuraxis is an imaginary line drawn through the spinal cord up to the front of the brain Anatomical directions are
Lecturer. Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014
 Lecturer Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014 Dorsal root: The dorsal root carries both myelinated and unmyelinated afferent fibers to the spinal cord. Posterior gray column: Long
Lecturer Prof. Dr. Ali K. Al-Shalchy MBChB/ FIBMS/ MRCS/ FRCS 2014 Dorsal root: The dorsal root carries both myelinated and unmyelinated afferent fibers to the spinal cord. Posterior gray column: Long
Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY
 Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY Objectives At the end of the lecture, the students should be able to: List the parts of the nervous system. List the function
Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY Objectives At the end of the lecture, the students should be able to: List the parts of the nervous system. List the function
CENTRAL NERVOUS SYSTEM
 Student Name CHAPTER 13 CENTRAL NERVOUS SYSTEM Approximately one hundred billion neurons make up the brain. Everything we are and everything we hope to become are centered in this structure, which is about
Student Name CHAPTER 13 CENTRAL NERVOUS SYSTEM Approximately one hundred billion neurons make up the brain. Everything we are and everything we hope to become are centered in this structure, which is about
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
Chapter 18: The Brain & Cranial Nerves. Origin of the Brain
 Chapter 18: The Brain & Cranial Nerves BIO 218 Fall 2015 Origin of the Brain The brain originates from a structure called the neural tube, which arises during a developmental stage called neurulation.
Chapter 18: The Brain & Cranial Nerves BIO 218 Fall 2015 Origin of the Brain The brain originates from a structure called the neural tube, which arises during a developmental stage called neurulation.
TRANSVERSE SECTION PLANE Scalp 2. Cranium. 13. Superior sagittal sinus
 TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
TRANSVERSE SECTION PLANE 1 1. Scalp 2. Cranium 3. Superior sagittal sinus 4. Dura mater 5. Falx cerebri 6. Frontal lobes of the cerebrum 7. Middle meningeal artery 8. Cortex, grey matter 9. Cerebral vessels
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings. Jonathan A. Micieli, MD Valérie Biousse, MD
 Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
DIRECT SURGERY FOR INTRA-AXIAL
 Kitakanto Med. J. (S1) : 23 `28, 1998 23 DIRECT SURGERY FOR INTRA-AXIAL BRAINSTEM LESIONS Kazuhiko Kyoshima, Susumu Oikawa, Shigeaki Kobayashi Department of Neurosurgery, Shinshu University School of Medicine,
Kitakanto Med. J. (S1) : 23 `28, 1998 23 DIRECT SURGERY FOR INTRA-AXIAL BRAINSTEM LESIONS Kazuhiko Kyoshima, Susumu Oikawa, Shigeaki Kobayashi Department of Neurosurgery, Shinshu University School of Medicine,
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Sheep Brain Dissection
 Sheep Brain Dissection Mammalian brains have many features in common. Human brains may not be available, so sheep brains often are dissected as an aid to understanding the mammalian brain since he general
Sheep Brain Dissection Mammalian brains have many features in common. Human brains may not be available, so sheep brains often are dissected as an aid to understanding the mammalian brain since he general
Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage
 Int J Clin Exp Med 2016;9(8):15921-15927 www.ijcem.com /ISSN:1940-5901/IJCEM0022273 Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage Xielin Tang
Int J Clin Exp Med 2016;9(8):15921-15927 www.ijcem.com /ISSN:1940-5901/IJCEM0022273 Original Article CT grouping and microsurgical treatment strategies of hypertensive cerebellar hemorrhage Xielin Tang
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
PHYSIOLOHY OF BRAIN STEM
 PHYSIOLOHY OF BRAIN STEM Learning Objectives The brain stem is the lower part of the brain. It is adjoining and structurally continuous with the spinal cord. 1 Mid Brain 2 Pons 3 Medulla Oblongata The
PHYSIOLOHY OF BRAIN STEM Learning Objectives The brain stem is the lower part of the brain. It is adjoining and structurally continuous with the spinal cord. 1 Mid Brain 2 Pons 3 Medulla Oblongata The
Blood Supply of the CNS
 Blood Supply of the CNS Lecture Objectives Describe the four arteries supplying the CNS. Follow up each artery to its destination. Describe the circle of Willis and its branches. Discuss the principle
Blood Supply of the CNS Lecture Objectives Describe the four arteries supplying the CNS. Follow up each artery to its destination. Describe the circle of Willis and its branches. Discuss the principle
EVALUATION OF COMATOSE PATIENT. Prof. G. Zuliani
 EVALUATION OF COMATOSE PATIENT Prof. G. Zuliani Consciousness Two components of conscious behavior: Vigilance (arousal): appearance of wakefulness Awareness (content): the sum of cognitive and affective
EVALUATION OF COMATOSE PATIENT Prof. G. Zuliani Consciousness Two components of conscious behavior: Vigilance (arousal): appearance of wakefulness Awareness (content): the sum of cognitive and affective
Concepts of Neurologic Dysfunction
 Concepts of Neurologic Dysfunction Chapter 14 Alterations in Arousal Coma is produced by either: Ø Bilateral hemisphere damage or suppression Ø Brain stem lesions or metabolic derangement that damages
Concepts of Neurologic Dysfunction Chapter 14 Alterations in Arousal Coma is produced by either: Ø Bilateral hemisphere damage or suppression Ø Brain stem lesions or metabolic derangement that damages
Central Nervous System (CNS) -> brain and spinal cord. Major Divisions of the nervous system:
 -> brain and spinal cord. Major Divisions of the nervous system:") Central Nervous System (CNS) -> brain and spinal cord Major Divisions of the nervous system: Afferent (sensory input) -> cell bodies outside of the central nervous system (CNS), carry info into the CNS
Central Nervous System (CNS) -> brain and spinal cord Major Divisions of the nervous system: Afferent (sensory input) -> cell bodies outside of the central nervous system (CNS), carry info into the CNS
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
The orbit-1. Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology
 The orbit-1 Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Orbital plate of frontal bone Orbital plate of ethmoid bone Lesser wing of sphenoid Greater wing of sphenoid Lacrimal bone Orbital
The orbit-1 Dr. Heba Kalbouneh Assistant Professor of Anatomy and Histology Orbital plate of frontal bone Orbital plate of ethmoid bone Lesser wing of sphenoid Greater wing of sphenoid Lacrimal bone Orbital
Brainstem. By Dr. Bhushan R. Kavimandan
 Brainstem By Dr. Bhushan R. Kavimandan Development Ventricles in brainstem Mesencephalon cerebral aqueduct Metencephalon 4 th ventricle Mylencephalon 4 th ventricle Corpus callosum Posterior commissure
Brainstem By Dr. Bhushan R. Kavimandan Development Ventricles in brainstem Mesencephalon cerebral aqueduct Metencephalon 4 th ventricle Mylencephalon 4 th ventricle Corpus callosum Posterior commissure
CSF. Cerebrospinal Fluid(CSF) System
 System") Cerebrospinal Fluid(CSF) System By the end of the lecture, students must be able to describe Physiological Anatomy of CSF Compartments Composition Formation Circulation Reabsorption CSF Pressure Functions
Cerebrospinal Fluid(CSF) System By the end of the lecture, students must be able to describe Physiological Anatomy of CSF Compartments Composition Formation Circulation Reabsorption CSF Pressure Functions
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7. Some PGY1
 Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
Divine Intervention Episode 58 Neurology Clerkship Shelf Review Part 7 Some PGY1 1 Discussion of the pathway/information carried by the 3 HY spinal cord tracts (DCMLS, STT, CST). Description of the Romberg
COMA & INTENSIVE CARE
 COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al.
 ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al. visualization of the posterior inferior cerebellar artery. The patient, now 11 months post-operative, has shown further neurological improvement since
ANASTAMOSIS FOR BRAIN STEM ISCHEMIA/Khodadad et al. visualization of the posterior inferior cerebellar artery. The patient, now 11 months post-operative, has shown further neurological improvement since
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE
 Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE") Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL
Superior View of the Skull (Norma Verticalis) Anteriorly the frontal bone articulates with the two parietal bones AT THE CORONAL SUTURE 1 The two parietal bones articulate in the midline AT THE SAGITTAL