CNS pathology Third year medical students,2019. Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
|
|
|
- Richard Lang
- 5 years ago
- Views:
Transcription
1 CNS pathology Third year medical students,2019 Dr Heyam Awad Lecture 2: Disturbed fluid balance and increased intracranial pressure
2 ILOs Understand causes and symptoms of increased intracranial pressure. Define cerebral edema and know its types and causes. Define hydrocephalus and know its types and causes. Define herniation and know its types and complications Understand auto-regulation of blood flow in the brain List causes of hypoxia and ischemia Understand outcomes of global brain ischemia Apply the above knowledge in clinical scenarios.
3 Topics to be covered in this lecture: - Increased intracranial pressure. - Brain edema - Hydrocephalus - Herniation - Cerebral ischemia

4 The cranium.. The brain is enclosed within the skull, which is a rigid box that protects it. In adults, skull bones cannot expand So if the material within the cranium increases.. Pressure will increase= increased intracranial pressure
5 What's inside the cranium? ROUGHLY: 80% brain tissue ( including intracellular and interstitial fluid which is around 75% of brain weight) 10% blood 10% CSF (cerebrospinal fluid) If any of these components increases, the intracranial pressure increases.
6 Monro- Kellie hypothesis Monro- Kellie hypothesis: intracranial volume= VCNS +VCSF + VBlood + Vlesion V= volume. This hypothesis indicated that any space occupying lesion in the brain will increase the volume inside the cranium and this will result in increased intracranial pressure. Space occupying lesions occur with all major brain diseases ( except degenerative diseases). Examples: brain tumours, trauma, stroke, haemorrhage.
7 OK, so what is intracranial pressure (ICP)??? It is the pressure inside the skull and is measured in millimetres of mercury at rest, it is normally 7 15 mmhg for a supine adult. If pressure in the cranium is higher than this upper limit= increased intracranial pressure (= intracranial hypertension.
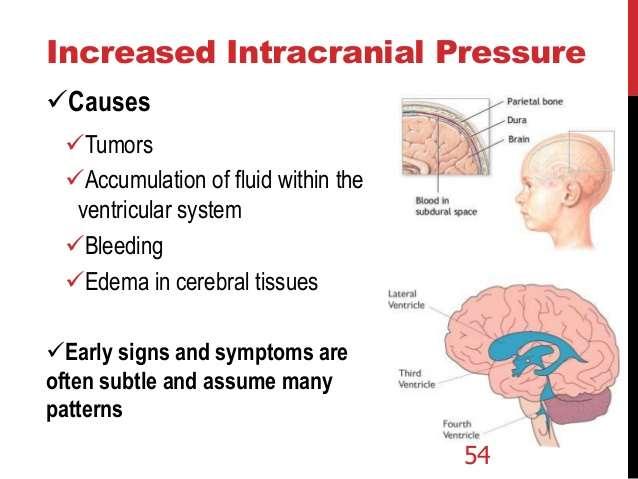
8 Causes of increased intracranial pressure mass effect : brain tumor, hematoma, or abscess. generalized brain swelling :ischemia, hypertension increase in venous pressure : heart failure obstruction to CSF flow and/or absorption or increased CSF production: hydrocephalus. Idiopathic or unknown in this lecture we will discuss two of the causes of increased ICP : ischema and hydrocephalus
9
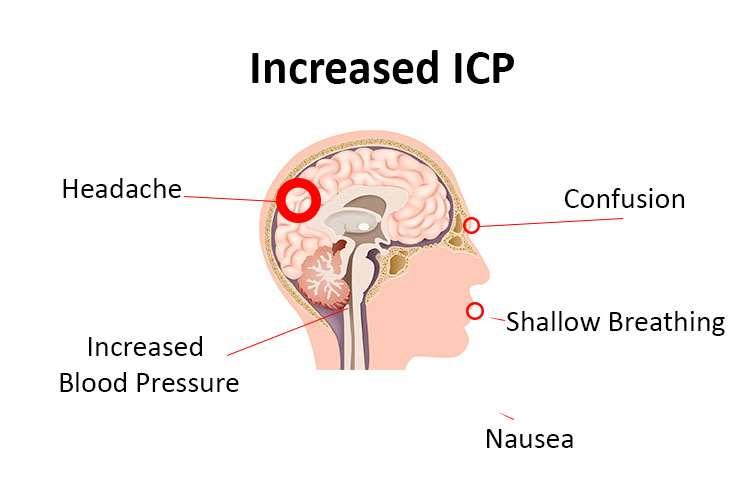
10 clinical presentation of increased intracranial pressure in the early stages patients will have non specific symptoms like headache and vomiting. also in the early stages patients might have Cushing reflex ( Cushing response or Cushing triad) which manifests by: increased blood pressure, bradycardia and irregular breathing. In more advances cases patients have neurological manifestations including disturbed level of consciousness. later complications can occur, mainly herniation and seizures.

11 clinical presentation according to severity:
12
13 Brain edema= cerebral edema = accumulation of excess fluid within the brain parenchyma. Two types: vasogenic and cytotoxic edema.. Usually coexist
14 Vasogenic edema Due to disruption of blood brain barrier. So: shift of fluids from vessels to brain tissue. Lymphatic vessels are rare in the brain.. So there is little or no resorption of excess edema fluid. Can be generalised ( due to hypoxia) or localised ( due to inflammation or tumors)
15 Cytotoxic edema Due to neuronal or glial cell membrane injury. Causes: toxins or hypoxia. Here fluid moves from cells to interstitial tissue.
16 morphology With edema, the brain becomes swollen.. And its weight increases. The normal adult human brain weighs on average about kg,or about 2% of total body weight, although there is substantial individual variation. Edema causes flat gyri and narrow sulci

17 Brain edema: note that the distinction between gyri and sulci is diminished because the sulci are filled with fluid making them narrow and the gyri are widened by the fluid
18 hydrocephalus Increased CSF within ventricles. Caused by overproduction or decreased resorption of CSF. Overproduction: rare, due to choroid plexus tumors. Decreased resorption.. Can be localised or generalised.
19 hydrocephalus Localised: noncommunicating hydrocephalus. Generalised: communicating hydrocephalus.
20 In infancy, before closure of the cranial sutures, the head can enlarge. Note that complete closure of the skull bones occurs between months of age. After closure of the cranial sutures: increased intracranial pressure occurs. Of course there is no increase in head circumference

21 hydrocephalus in children: head circumference increases

22 hydrocephalus: increased CSF within ventricles.
23 Herniation : a complication of brain edema and hydrocephalus Increased volume of tissue inside the skull causes Increased intracranial pressure which causes focal expansion of the brain tissue. Because the cranial vault is subdivided by rigid dural folds (falx and tentorium). The expanded brain tissue is displaced in relation to these folds. Expansion= herniation SO: herniation is a complication of increased intracranial pressure and it occurs in relation to margins of the dural folds.
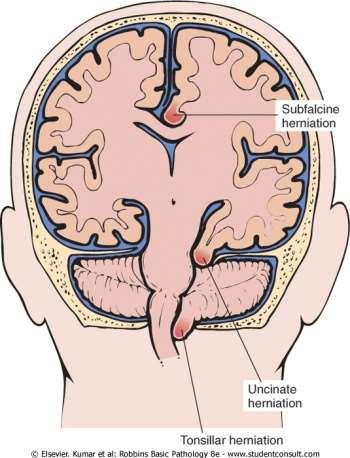
24 herniation: 3 types Subfalcine = cingulate Transtentorial = uncinate Tonsillar.
25 herniation
26 Cingulate herniation -cingulate gyrus displaced under edge of falx -Can cause compression of anterior cerebral artery; so the territory supplied by this artery can suffer ischemic damage and infarction if severe.
27 Transtentorial herniation Medial aspect of temporal lobe compressed against the free margin of the tentorium. so the brain tissue is forced from supra-tentorial to towards the infra-tentorial compartment. Third cranial nerve compressed.. Dilated pupil, impaired ocular movement on the side of the lesion ( ipsilateral side) Posterior cerebral artery can be affected.. Ischemic injury to tissues supplied by it including visual cortex. Transtentorial herniation can cause hemorrhage in the midbrain and pons ( Duret haemorrhage) which is usually fatal.

28 Duret hemorrhage The end result of temporal medial lobe ( transtentorial) herniation is compression of the brainstem (midbrain and pons) and stretching of small arterial branches to cause Duret haemorrhages Duret haemorrhages are small lineal areas of bleeding in the midbrain and upper pons of the brainstem. They are caused by downward displacement of the brainstem. They are named after Henri Duret.
29 Tonsillar herniation Displaced cerebellar tonsils through foramen magnum Brain stem compression respiratory and cardiac centres in medulla compromised. LIFE THREATENING
30 So far we talked about: edema and hydrocephalus as causes of increased intracranial pressure We also discussed herniation as a complication of increased ICP the rest of the lecture will discuss hypoxia and ischemia, which are the main cause of generalised cerebral edema.
31 Hypoxia and ischemia Brain is highly oxygen dependent. Brain weight constitutes 2% of body weight but receives 15% of cardiac output 20% of total body oxygen consumption. Autoregulation of vascular resistance allows stability of cerebral blood flow over a wide range of blood pressures and intracranial pressure. If blood pressure very low (systolic less than 50) hypoxia occurs
32 Auto regulation the brain receives the same amount of blood ( brain blood flow is constant ) if the mean arterial pressure is between mm Hg. If mean arterial pressure is less than 50, the auto regulatory mechanisms fail and the brain blood flow decreases, causing hypoxia.
33
34 Brain hypoxia Functional hypoxia. ischemic hypoxia




35 Functional hypoxia Low partial pressure of oxygen: high altitude Impaired oxygen carrying capacity: anaemia and CO poisoning Decreased oxygen use by tissues: cyanide poisoning
36 Ischemic hypoxia Hypo-perfusion due to hypotension or vascular obstruction Ischemia can be global or focal Focal ischemia causes infarctions ( ischemic stroke)and this will be discussed in another lecture.
37 Global cerebral ischemia Occurs due to severe hypotension, systolic below 50mm Hg: this occurs in situations like: Cardiac arrest Shock Severe hypotension Outcome depends on severity and duration of insult
38 Global ischemia Neurons more susceptible to hypoxic injury than glial cells. Most susceptible neurons are the pyramidal cells of hippocampus and neocortex + Purkinje cells of the cerebellum
39 ischemia If mild: transient confusional state severe : neural death, if survive: severely impaired neurologically Severest forms result in brain death.
40 Morphology of reversible global ischemia= brain edema Swelling Wide gyri Narrow sulci Poor grey white matter demarcation
41 Irreversible global ischemia can cause brain death Diffuse cortical injury with flat EEG ( isoelectric EEG) Brain stem damage: No reflexes and no respiration If on mechanical support: autolysis of brain= respirator brain. /
42 Brain death Brain death is different from coma and vegetative state. the latter two are potentially reversible. Death is irreversible. So diagnosing brain death needs very strict criteria.. when you diagnose brain death you can discontinue artificial breathing, you can remove organs for donation etc The most accepted religious opinion in Islam is that brain death is accepted as a definition of death, and all religious and legal aspects regarding death apply. However, we need very strict criteria to separate brain death from its mimickers.
43 UK guidelines to diagnose brain death 1. Evidence for Irreversible Brain Damage of known Aetiology. 2. Exclusion of Reversible Causes of Coma and Apnoea Examples: hypothermia, drugs and alcohol.. 3. Tests for Absence of Brain-Stem Function. LINK FOR FULL GUIDELINES: 0Neurological%20Criteria%20-%20Full%20Version%20%282014%29.pdf
44 UK guidelines regarding doctors performing the neurological examination for brain death 1. The diagnosis of death by neurological criteria should be made by at least two medical practitioners. Both medical practitioners should have been registered with the General Medical Council (or equivalent Professional Body) for more than five years and be competent in the assessment of a patient who may be deceased following the irreversible cessation of brain-stem function and competent in the conduct and interpretation of the brain-stem examination. At least one of the doctors must be a consultant. 2. Those carrying out the tests must not have, or be perceived to have, any clinical conflict of interest and neither doctor should be a member of the transplant team. 3. Testing should be undertaken by the nominated doctors acting together and must always be performed on two occasions. A complete set of tests should be performed on each occasion, i.e., a total of two sets of tests will be performed. Doctor One may perform the tests while Doctor Two observes; this would constitute the first set. Roles may be reversed for the second set. The tests, in particular the apnoea test, are therefore performed only twice in total.
45 Summary 1/2 The skull protects the brain, but leaves little space to accommodate for any increase of the cranial contents. increased cranial contents cause increased intracranial pressure. This can be due to increased brain tissue ( tumours), fluid ( edema due to hypoxia or inflammation or other causes), CSF (hydrocephalus) or blood ( haemorrhage) increased ICP manifests as headache and projectile vomiting, Cushing triad ( hypertension, bradycardia, irregular slow breathing)) and can progress to coma. Brain edema can be vasogenic or cytotoxic. It manifests as increased brain wight with narrow sulci and flat gyri. Hydrocephalus is increased CSF due to increased production by a choroid plexus tumour ( rare) or more commonly by decreased resorption.it can be localised ( non communicating) or generalised ( communicating)
46 Summary 2/2 increased ICP can be complicated by herniation; which is a displacement of brain tissue from a compartment to another. Subfalcian herniation displaces the cingulate gyrus under edge of falx, it causes compression of anterior cerebral artery Transtentorial herniation displaces the medial aspect of temporal lobe against the free margin of the tentorium. This compresses the third cranial nerve, posterior cerebral artery and can cause Duret haemorrhage in the midbrain which is usually fatal. Tonsillar herniation displaces the cerebellar tonsils through foramen magnum causing brain stem compression, which is usually fatal. Hypoxia and ischemia are the main causes of brain edema. Autoregulation maintains blood flow but below 50 systolic pressure, flow decreases. Pukinji cells and pyramidal cells are the most susceptible to ischemic damage. Irreversible ischemia can cause brain death
47 Question A 54 year old man complained of severe headache and vomiting. imaging studies showed a large subdural hematoma. Two days later he had dilated pupil of the right eye with and his visual acuity decreased. Which of the following is incorrect about his condition? A. Can be complicated by haemorrhage in the pons. B. His eye symptoms could be related to ischemic injury to the visual cortex C.The medial aspect of his temporal lobe is compressed against the free margin of the tentorium D. The dilated pupil indicated damage of the left third cranial nerve E. He might develop fatal brain stem complications.
48 Answer the scenario describes increased ICP due to hematoma. The complications he had indicate herniation, and the symptoms are those of transtentorial herniation. the answer is D: the lesion is related to the ipsilateral nerve ( at the same side of the lesion).. so his right third cranial nerve is compressed. A is correct, it describes Duret hemorrage. Also E is correct, again it describes Duret haemorrhage. C :correct, it simply describes his main complication: transtentorial herniation D is correct, note that the decreased visual acuity is due to effect on the visual cortex ( ischemic damage due to compression on the posterior cerebral artery), however, the dilated pupil and impaired ocular movement are effects of compression on the third cranial nerve.

49
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 5: disturbed fluid balance and increased intracranial pressure ILOs Understand causes and symptoms of increased intracranial pressure.
Characteristic features of CNS pathology. By: Shifaa AlQa qa
 Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Characteristic features of CNS pathology By: Shifaa AlQa qa Normal brain: - The neocortex (gray matter): six layers: outer plexiform, outer granular, outer pyramidal, inner granular, inner pyramidal, polymorphous
Classical CNS Disease Patterns
 Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
Classical CNS Disease Patterns Inflammatory Traumatic In response to the trauma of having his head bashed in GM would have experienced some of these features. NOT TWO LITTLE PEENY WEENY I CM LACERATIONS.
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
features of CNS pathology
 سالي ابو رمان Characteristic features of CNS pathology Important notes : - In this sheet I arranged slides within what the doctor said plus what is written in the book, hopefully it will be helpful and
سالي ابو رمان Characteristic features of CNS pathology Important notes : - In this sheet I arranged slides within what the doctor said plus what is written in the book, hopefully it will be helpful and
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
NEURO IMAGING 2. Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity
 NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
NEURO IMAGING 2 Dr. Said Huwaijah Chairman of radiology Dep, Damascus Univercity I. EPIDURAL HEMATOMA (EDH) LOCATION Seventy to seventy-five percent occur in temporoparietal region. CAUSE Most likely caused
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
What Are We Going to Do? Fourth Year Meds Clinical Neuroanatomy. Hydrocephalus and Effects of Interruption of CSF Flow. Tube Blockage Doctrine
 Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Fourth Year Meds Clinical Neuroanatomy Ventricles, CSF, Brain Swelling etc. David A. Ramsay, Neuropathologist, LHSC What Are We Going to Do? Hydrocephalus and some effects of the interruption of CSF flow
Traumatic Brain Injury TBI Presented by Bill Masten
 1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
1 2 Cerebrum two hemispheres and four lobes. Cerebellum (little brain) coordinates the back and forth ballet of motion. It judges the timing of every movement precisely. Brainstem coordinates the bodies
BRAIN HERNIATION S54 (1) Brain Herniation
 Brain Herniation") BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
BRAIN HERNIATION S54 (1) Brain Herniation Last updated: September 5, 2017 PATHOPHYSIOLOGY... 1 TYPES OF HERNIATION... 2 SUPRATENTORIAL MASSES... 2 Central (s. downward transtentorial) herniation... 2 Uncal
Pathological reaction to disease
 Chapter1 Pathological reaction to disease Normal anatomy Figures 1.1 1.6 2 4 Brain swelling and internal herniation Figures 1.7 1.15 5 9 Epilepsy Figures 1.16 1.18 9 10 Cerebellar atrophy Figures 1.19
Chapter1 Pathological reaction to disease Normal anatomy Figures 1.1 1.6 2 4 Brain swelling and internal herniation Figures 1.7 1.15 5 9 Epilepsy Figures 1.16 1.18 9 10 Cerebellar atrophy Figures 1.19
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD
 Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Head CT Scan Interpretation: A Five-Step Approach to Seeing Inside the Head Lawrence B. Stack, MD Five Step Approach 1. Adequate study 2. Bone windows 3. Ventricles 4. Quadrigeminal cistern 5. Parenchyma
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Meninges and Ventricles
 Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
Meninges and Ventricles Irene Yu, class of 2019 LEARNING OBJECTIVES Describe the meningeal layers, the dural infolds, and the spaces they create. Name the contents of the subarachnoid space. Describe the
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases
 How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
How to interpret an unenhanced CT brain scan. Part 2: Clinical cases Thomas Osborne a, Christine Tang a, Kivraj Sabarwal b and Vineet Prakash c a Radiology Registrar; b Radiology Foundation Year 1 Doctor;
Head Trauma Inservice (October)
") John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
John Tramell - Head Trauma Inservice, October 2005.doc Page 1 Head Trauma Inservice (October) Head trauma is the leading cause of death in trauma patients. Having a basic understanding of the anatomy and
IV. Cerebrovascular diseases
 IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
ICP CSF Spinal Cord Anatomy Cord Transection. Alicia A C Waite March 2nd, 2017
 ICP CSF Spinal Cord Anatomy Cord Transection Alicia A C Waite March 2nd, 2017 Monro-Kellie doctrine Intracranial volume = brain volume (85%) + blood volume (10%) + CSF volume (5%) Brain parenchyma Skull
ICP CSF Spinal Cord Anatomy Cord Transection Alicia A C Waite March 2nd, 2017 Monro-Kellie doctrine Intracranial volume = brain volume (85%) + blood volume (10%) + CSF volume (5%) Brain parenchyma Skull
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia
 Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
Neurophysiology Lecture One : Neurophysiology and Evoked Potentials Lecture Two: Clinical Neuroanesthesia Reza Gorji, MD University Hospital September 2007 Topics Covered Today Intracranial Pressure Intracranial
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
HEAD AND NECK IMAGING. James Chen (MS IV)
") HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
HEAD AND NECK IMAGING James Chen (MS IV) Anatomy Course Johns Hopkins School of Medicine Sept. 27, 2011 OBJECTIVES Introduce cross sectional imaging of head and neck Computed tomography (CT) Review head
secondary effects and sequelae of head trauma.
 Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Neuroimaging of vascular/secondary secondary effects and sequelae of head trauma. Andrès Server Alonso Department of Neuroradiology Division of Radiology Ullevål University Hospital Oslo, Norway. Guidelines
Medical Neuroscience Tutorial Notes
 Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Medical Neuroscience Tutorial Notes Blood Supply to the Brain MAP TO NEUROSCIENCE CORE CONCEPTS 1 NCC1. The brain is the body's most complex organ. LEARNING OBJECTIVES After study of the assigned learning
Brain ميهاربا لض اف دمح ا د The Meninges 1- Dura Mater of the Brain endosteal layer does not extend meningeal layer falx cerebri tentorium cerebelli
 .احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
.احمد د فاضل ابراهيم Lecture 15 Brain The Meninges Three protective membranes or meninges surround the brain in the skull: the dura mater, the arachnoid mater, and the pia mater 1- Dura Mater of the Brain
The central nervous system
 Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
Sectc.qxd 29/06/99 09:42 Page 81 Section C The central nervous system CNS haemorrhage Subarachnoid haemorrhage Cerebral infarction Brain atrophy Ring enhancing lesions MRI of the pituitary Multiple sclerosis
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
CNS pathology Third year medical students. Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage
 CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
CNS pathology Third year medical students Dr Heyam Awad 2018 Lecture 7: Non traumatic brain haemorrhage ILOS To list the causes of intracranial haemorrhage. To understand the pathogenesis of each cause.
NEURORADIOLOGY DIL part 3
 NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
NEURORADIOLOGY DIL part 3 Bleeds and hemorrhages K. Agyem MD, G. Hall MD, D. Palathinkal MD, Alexandre Menard March/April 2015 OVERVIEW Introduction to Neuroimaging - DIL part 1 Basic Brain Anatomy - DIL
PARA210 SUMMARY Hyperglycaemia (DKA & HHS) Brain & Nervous System Anatomy & Physiology Degenerative Neurological Disorders
 Brain & Nervous System Anatomy & Physiology Degenerative Neurological Disorders") PARA210 SUMMARY Page Topic 01-03 Diabetes Mellitus 04-05 Hyperglycaemia (DKA & HHS) 06-13 Toxicology 14-18 12 Lead ECG 19-21 Brain & Nervous System Anatomy & Physiology 22-24 Degenerative Neurological
PARA210 SUMMARY Page Topic 01-03 Diabetes Mellitus 04-05 Hyperglycaemia (DKA & HHS) 06-13 Toxicology 14-18 12 Lead ECG 19-21 Brain & Nervous System Anatomy & Physiology 22-24 Degenerative Neurological
Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY
 Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY Objectives At the end of the lecture, the students should be able to: List the parts of the nervous system. List the function
Organization of The Nervous System PROF. MOUSAED ALFAYEZ & DR. SANAA ALSHAARAWY Objectives At the end of the lecture, the students should be able to: List the parts of the nervous system. List the function
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Traumatic brain injuries are caused by external mechanical forces such as: - Falls - Transport-related accidents - Assault
 PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
PP2231 Brain injury Cerebrum consists of frontal, parietal, occipital and temporal lobes Diencephalon consists of thalamus, hypothalamus Cerbellum Brain stem consists of midbrain, pons, medulla Central
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
CSF. Cerebrospinal Fluid(CSF) System
 System") Cerebrospinal Fluid(CSF) System By the end of the lecture, students must be able to describe Physiological Anatomy of CSF Compartments Composition Formation Circulation Reabsorption CSF Pressure Functions
Cerebrospinal Fluid(CSF) System By the end of the lecture, students must be able to describe Physiological Anatomy of CSF Compartments Composition Formation Circulation Reabsorption CSF Pressure Functions
HYPERTENSIVE ENCEPHALOPATHY
 HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
CSF. Lumbar punction. CSF Cerebrospinal fluid - CSF
 CSF Cerebrospinal fluid - CSF Clear and colorless liquid in ventricles, cisterns and subarachnoidal spaces of brain and spinal cord CSF Production secretion chorioid. plexus in ventricles Resorbtion subarachnoid.
CSF Cerebrospinal fluid - CSF Clear and colorless liquid in ventricles, cisterns and subarachnoidal spaces of brain and spinal cord CSF Production secretion chorioid. plexus in ventricles Resorbtion subarachnoid.
Ventricles, CSF & Meninges. Steven McLoon Department of Neuroscience University of Minnesota
 Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
Ventricles, CSF & Meninges Steven McLoon Department of Neuroscience University of Minnesota 1 Coffee Hour Thursday (Sept 14) 8:30-9:30am Surdyk s Café in Northrop Auditorium Stop by for a minute or an
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
V. CENTRAL NERVOUS SYSTEM TRAUMA
 V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
V. CENTRAL NERVOUS SYSTEM TRAUMA I. Concussion - Is a clinical syndrome of altered consiousness secondary to head injury - Brought by a change in the momentum of the head when a moving head suddenly arrested
DRAFT: Cendoma, M. Sideline Identification of Intracranial Hematoma
 1. Orlando Regional Healthcare, Education and Development. Orlando Regional Health Care. [Online] 2004. [Cited: April 27, 2012.] http://www.orlandoregional.org/pdf%20folder/overview%20adult%20brain%20injury.pd
1. Orlando Regional Healthcare, Education and Development. Orlando Regional Health Care. [Online] 2004. [Cited: April 27, 2012.] http://www.orlandoregional.org/pdf%20folder/overview%20adult%20brain%20injury.pd
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Anesthetic Management of a Patient with Traumatic Brain Injury
 Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
Anesthetic Management of a Patient with Traumatic Brain Injury Arne O. Budde, MD, DEAA Associate Professor of Anesthesiology Director, Division of Neuroanesthesia Department of Anesthesiology Milton S
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
PEDIATRIC BRAIN CARE
 PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
PEDIATRIC BRAIN CARE The brain matters most! OVERVIEW OF NEURO ASSESSMENT 1. Overall responsiveness/activity 2. The eyes 3.? Increased ICP 4. Movements 5.? Seizures 6. Other OVERALL RESPONSIVENESS/ ACTIVITY
TOXIC AND NUTRITIONAL DISORDER MODULE
 TOXIC AND NUTRITIONAL DISORDER MODULE Objectives: For each of the following entities the student should be able to: 1. Describe the etiology/pathogenesis and/or pathophysiology, gross and microscopic morphology
TOXIC AND NUTRITIONAL DISORDER MODULE Objectives: For each of the following entities the student should be able to: 1. Describe the etiology/pathogenesis and/or pathophysiology, gross and microscopic morphology
Brain Injuries. Presented By Dr. Said Said Elshama
 Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Brain Injuries Presented By Dr. Said Said Elshama Types of head injuries 1- Scalp injuries 2- Skull injuries 3- Intra Cranial injuries ( Brain ) Anatomical structure of meninges Intra- Cranial Injuries
Cerebro-vascular stroke
 Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebro-vascular stroke CT Terminology Hypodense lesion = lesion of lower density than the normal brain tissue Hyperdense lesion = lesion of higher density than normal brain tissue Isodense lesion = lesion
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Organic Mental Disorders. Organic Mental Disorders. Axes. Damrongsak Bulyalert Department of Internal Medicine
 Organic Mental Disorders Damrongsak Bulyalert Department of Internal Medicine www.metadon.net 1 Organic Mental Disorders In DSM (Diagnostic and Statistical Manual of Mental Disorders), OMD includes Delirium,
Organic Mental Disorders Damrongsak Bulyalert Department of Internal Medicine www.metadon.net 1 Organic Mental Disorders In DSM (Diagnostic and Statistical Manual of Mental Disorders), OMD includes Delirium,
The Child with Alterations in Cerebral Function
 The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
The Child with Alterations in Cerebral Function Neurologic Assessment VS HR, BP, Respirations, Temperature LOC Orientation Pediatric Glasgow Coma Scale Eyes Pupillary response and movement, extraoccular
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
COMA & INTENSIVE CARE
 COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
COMA & INTENSIVE CARE Jozef Firment, MD. PhD., Judita Capkova, MD. PhD. Department of Anaesthesiology & Intensive Care Medicine Šafárik University Faculty of Medicine, Košice Coma Is a state of unarousable
Chapter 14. The Brain Meninges and Cerebral Spinal Fluid
 Chapter 14 The Brain Meninges and Cerebral Spinal Fluid Meninges of the Brain Skull Brain: Blood vessel Pia mater Gray matter White matter Dura mater: Periosteal layer Meningeal layer Arachnoid villus
Chapter 14 The Brain Meninges and Cerebral Spinal Fluid Meninges of the Brain Skull Brain: Blood vessel Pia mater Gray matter White matter Dura mater: Periosteal layer Meningeal layer Arachnoid villus
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM
 Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
Organization of The Nervous System PROF. SAEED ABUEL MAKAREM Objectives By the end of the lecture, you should be able to: List the parts of the nervous system. List the function of the nervous system.
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
CEREBROVASCULAR DISEASES. By: Shifaa AlQa qa
 CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
CEREBROVASCULAR DISEASES By: Shifaa AlQa qa Cerebrovascular diseases Brain disorders caused by pathologic processes involving blood vessels 3 pathogenic mechanisms (1) thrombotic occlusion, (2) embolic
Principles of Anatomy and Physiology
 Principles of Anatomy and Physiology 14 th Edition CHAPTER 14 The Brain and Cranial Nerves Introduction The purpose of the chapter is to: 1. Understand how the brain is organized, protected, and supplied
Principles of Anatomy and Physiology 14 th Edition CHAPTER 14 The Brain and Cranial Nerves Introduction The purpose of the chapter is to: 1. Understand how the brain is organized, protected, and supplied
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Disorders of the Nervous System. Disorders of the Neurological System. General Endpoints of CNS Disease. General Endpoints of CNS Disease
 HD in Nursing-Pathophysiology Disorders of the Nervous System What are some disorders of the nervous system? Disorders of the Neurological System Dr. C.H. Lai The nervous system is vulnerable to various
HD in Nursing-Pathophysiology Disorders of the Nervous System What are some disorders of the nervous system? Disorders of the Neurological System Dr. C.H. Lai The nervous system is vulnerable to various
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Anatomy & Physiology Central Nervous System Worksheet
 1. What are the two parts of the CNS? 2. What are the four functions of the CNS Anatomy & Physiology Central Nervous System Worksheet 3. What are the four functions of the meninges? (p430) 4. Starting
1. What are the two parts of the CNS? 2. What are the four functions of the CNS Anatomy & Physiology Central Nervous System Worksheet 3. What are the four functions of the meninges? (p430) 4. Starting
b. The groove between the two crests is called 2. The neural folds move toward each other & the fuse to create a
 Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Chapter 13: Brain and Cranial Nerves I. Development of the CNS A. The CNS begins as a flat plate called the B. The process proceeds as: 1. The lateral sides of the become elevated as waves called a. The
Anatomically and functionally the brain is the most complex
 CHAPTER 37 Alterations in Brain Function Brain Injury Mechanisms of Brain Injury Hypoxia and Ischemia Excitatory Amino Acid Injury Cerebral Edema Increased Intracranial Volume and Pressure Brain Herniation
CHAPTER 37 Alterations in Brain Function Brain Injury Mechanisms of Brain Injury Hypoxia and Ischemia Excitatory Amino Acid Injury Cerebral Edema Increased Intracranial Volume and Pressure Brain Herniation
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Vascular Malformations of the Brain. William A. Cox, M.D. Forensic Pathologist/Neuropathologist. September 8, 2014
 Vascular Malformations of the Brain William A. Cox, M.D. Forensic Pathologist/Neuropathologist September 8, 2014 Vascular malformations of the brain are classified into four principal groups: arteriovenous
Vascular Malformations of the Brain William A. Cox, M.D. Forensic Pathologist/Neuropathologist September 8, 2014 Vascular malformations of the brain are classified into four principal groups: arteriovenous
Neurology Clerkship Learning Objectives
 Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Neurology Clerkship Learning Objectives Clinical skills Perform a neurological screening examination of the cranial nerves, motor system, reflexes, and sensory system under the observation and guidance
Somatic Nervous Systems. III. Autonomic Nervous System. Parasympathetic Nervous System. Sympathetic Nervous Systems
 7/21/2014 Outline Nervous System - PNS and CNS I. II. Two Parts of the Nervous System Central Nervous System vs Peripheral Nervous System Peripheral Nervous System A. B. Brain and Spinal Cord III. Autonomic
7/21/2014 Outline Nervous System - PNS and CNS I. II. Two Parts of the Nervous System Central Nervous System vs Peripheral Nervous System Peripheral Nervous System A. B. Brain and Spinal Cord III. Autonomic
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16
 The Brain Chapter 14 and select portions of Chapter 16") Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Anatomy and Physiology (Bio 220) The Brain Chapter 14 and select portions of Chapter 16 I. Introduction A. Appearance 1. physical 2. weight 3. relative weight B. Major parts of the brain 1. cerebrum 2.
Chapter 18: The Brain & Cranial Nerves. Origin of the Brain
 Chapter 18: The Brain & Cranial Nerves BIO 218 Fall 2015 Origin of the Brain The brain originates from a structure called the neural tube, which arises during a developmental stage called neurulation.
Chapter 18: The Brain & Cranial Nerves BIO 218 Fall 2015 Origin of the Brain The brain originates from a structure called the neural tube, which arises during a developmental stage called neurulation.
Central Nervous System (CNS) -> brain and spinal cord. Major Divisions of the nervous system:
 -> brain and spinal cord. Major Divisions of the nervous system:") Central Nervous System (CNS) -> brain and spinal cord Major Divisions of the nervous system: Afferent (sensory input) -> cell bodies outside of the central nervous system (CNS), carry info into the CNS
Central Nervous System (CNS) -> brain and spinal cord Major Divisions of the nervous system: Afferent (sensory input) -> cell bodies outside of the central nervous system (CNS), carry info into the CNS
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Neurology study of the nervous system. nervous & endocrine systems work together to maintain homeostasis
 Nervous System Neurology study of the nervous system nervous & endocrine systems work together to maintain homeostasis Nervous System works very fast Uses electrical signals called nerve impulses Short-lived
Nervous System Neurology study of the nervous system nervous & endocrine systems work together to maintain homeostasis Nervous System works very fast Uses electrical signals called nerve impulses Short-lived
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings. Jonathan A. Micieli, MD Valérie Biousse, MD
 Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
Typical idiopathic intracranial hypertension Optic nerve appearance and brain MRI findings Jonathan A. Micieli, MD Valérie Biousse, MD A 24 year old African American woman is referred for bilateral optic
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
Slide 1. Slide 2. Slide 3. Tomography vs Topography. Computed Tomography (CT): A simplified Topographical review of the Brain. Learning Objective
: A simplified Topographical review of the Brain. Learning Objective") Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
Slide 1 Computed Tomography (CT): A simplified Topographical review of the Brain Jon Wheiler, ACNP-BC Slide 2 Tomography vs Topography Tomography: A technique for displaying a representation of a cross
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Anatomy Lab (1) Theoretical Part. Page (2 A) Page (2B)
 Theoretical Part. Page (2 A) Page (2B)") Anatomy Lab (1) This sheet only includes the extra notes for the lab handout regarding the theoretical part, as for the practical part it includes everything the doctor mentioned. Theoretical Part Page
Anatomy Lab (1) This sheet only includes the extra notes for the lab handout regarding the theoretical part, as for the practical part it includes everything the doctor mentioned. Theoretical Part Page
Elsevier's Encyclopedia of euroscience
 REPRINTED FROM Elsevier's Encyclopedia of euroscience e Edited by George Adelman Barry H. Smith Editorial Manager Jennifer De Pasquale 1999 Elsevier Science B.V. All rights reserved. Visit the Encyclopedia's
REPRINTED FROM Elsevier's Encyclopedia of euroscience e Edited by George Adelman Barry H. Smith Editorial Manager Jennifer De Pasquale 1999 Elsevier Science B.V. All rights reserved. Visit the Encyclopedia's
Chapter 3. Structure and Function of the Nervous System. Copyright (c) Allyn and Bacon 2004
 Allyn and Bacon 2004") Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
Chapter 3 Structure and Function of the Nervous System 1 Basic Features of the Nervous System Neuraxis: An imaginary line drawn through the center of the length of the central nervous system, from the
Experiences as a Donation Support Physician. Dead or not Dead? Are the following statements consistent with neurological
 Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Experiences as a Donation Support Physician Dead or not Dead? Are the following statements consistent with neurological determination of death (dead)? or not (not dead)? With thanks to Drs. Alex Manara,
Department of Cognitive Science UCSD
 Department of Cognitive Science UCSD Verse 1: Neocortex, frontal lobe, Brain stem, brain stem, Hippocampus, neural node, Right hemisphere, Pons and cortex visual, Brain stem, brain stem, Sylvian fissure,
Department of Cognitive Science UCSD Verse 1: Neocortex, frontal lobe, Brain stem, brain stem, Hippocampus, neural node, Right hemisphere, Pons and cortex visual, Brain stem, brain stem, Sylvian fissure,
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ٢ Level of consciousness is depressed Stuporous patients respond only to repeated
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
3/15/17. Outline. Nervous System - PNS and CNS. Two Parts of the Nervous System
 Nervous System - PNS and CNS Bio 105 Outline I. Central Nervous System vs Peripheral Nervous System II. Peripheral Nervous System A. Autonomic Nervous Systems B. Somatic Nervous Systems III. Autonomic
Nervous System - PNS and CNS Bio 105 Outline I. Central Nervous System vs Peripheral Nervous System II. Peripheral Nervous System A. Autonomic Nervous Systems B. Somatic Nervous Systems III. Autonomic
Nervous System - PNS and CNS. Bio 105
 Nervous System - PNS and CNS Bio 105 Outline I. Central Nervous System vs Peripheral Nervous System II. Peripheral Nervous System A. Autonomic Nervous Systems B. Somatic Nervous Systems III. Autonomic
Nervous System - PNS and CNS Bio 105 Outline I. Central Nervous System vs Peripheral Nervous System II. Peripheral Nervous System A. Autonomic Nervous Systems B. Somatic Nervous Systems III. Autonomic