Jock Murray Constance LeBlanc Jennie Leverman Caitlin Wolfe
|
|
|
- Scott Henderson
- 6 years ago
- Views:
Transcription
1
2 Jock Murray Constance LeBlanc Jennie Leverman Caitlin Wolfe
3 Disclosures
4 ARTICLE #1
5 Background Physicians are reluctant to use IV contrast for CT scans in patients with impaired renal function We feel that we can not order the optimal test in an emergent situation due to the risk of kidney injury This study helps determine if this concern is justified
6 Methods Objective: To determine if IV contrast administration for CT Scans is independently associated with acute kidney injury
7 Methods Design: The Largest study on this topic. Single- Centre retrospective cohort analysis over 5 years. Serum creatinine levels were recorded within 8 hours before and hours after CT scanning There was propensity matching with patients who had a CT without contrast or no CT at all.
8 Funding and Conflicts Funding: John Hopkins University Conflicts: None Reported

9 Results
10 Results The risk of Acute Kidney Injury as 7.5 % in all three groups
11 Limits Retrospective Study Single centre study Ideally a DBRTC study would be performed but this is unlikely to be approved by any Research Ethics Board. Creatinine range from Some critics (who do their work in the dark) suggest that a study focusing on patient with borderline renal function is needed
12 Discussion This is likely the best done and largest study we will every get addressing the association between kidney Injury and intravenous contrast There was no difference in kidney Injury between groups
13 Discussion If you need a Contrast study to answer an important question then get it. Work with your Radiologist for a more permissive approach to CT Scanning with contrast in patients with impaired renal function.
14 References Risk of Acute Kidney Injury After Intravenous Contrast Media Administration. Hinson, J. S., et. al., Annals of Emergency Medicine. Vol. 69, no. 05. page

15 Contrast: NO PROBLEM
16 ARTICLE #2
17 Background Early Goal Directed Therapy (EDGT) as described by Manny Rivers has been promoted as the standard of care for treatment of sepsis This approach was promoted in the Surviving Sepsis campaign. This approach was eventually recognized to be inappropriate for most Emergency Departments. Which Components of EDGT matter?
18 Methods Objective: To determine if Early Goal Directed Therapy (EDGT) is superior to standard care. Design: A Preplanned Patient Level Meta-Analysis of Three large prospective Double Blind trials patients at 138 hospitals in seven countries. (ProCess, ARISE, and ProMISe)
19 Funding and Conflicts Funding: Funding by Multiple large National and International funding organizations in Australia, the UK and North America Conflicts: Several investigators have financial ties to Drug companies. None had ties to device makers

20 Results

21 Results


22 Results

23 Results
24 Results Mortality at 90 days- EDGT 24.9% vs. 25.4% (P=0.68) EDGT was associated with greater mean use of Intensive care ( vs. 4.9+/-7.0 days ) (P=0.04) Inotrope use (1.9+/-3.7 vs. 1.6+/- 2.9 days) (P=0.01)
25 Results Cost Effectiveness No difference in Quality Adjusted Life Years 4 times as likely that Usual Care is more cost effective than EDGT
26 Discussion EDGT provides no mortality benefit at increased cost
27 Conclusion Physicians should not feel that they need to follow a complicated protocol for patients with sepsis Standard care with early early antibiotics and aggressive fluid is equivalent to a much more complicated protocol Central lines, special catheters and complicated inotrope management are not valuable and can be left to the ICU

28 Just Do It!!!

29 Mensour ARTICLE #3
30 No need to intubate peds patients with IHCA P: Inclusions - IHCA age <18 yrs Exclusions - had invasive airway or being ventilated at the time of starting chest compressions I: Endotracheal intubation C: Those not tracheal intubated O: Survival to hospital discharge (primary) ROSC & favorable neurologic outcome at D/C (secondary)
31 Peds intubation IHCA n = 2294, 57% were male, age~7 months (21 days- 4 yrs) 1555 were intubated during the cardiac arrest Propensity score matched cohort 2270 Survival was lower in those intubated 36% vs 41%
32 What do I do? Put in an LMA to ventilate and measure the quality of CPR using ETCO 2 Although the study design does not eliminate the potential for confounding, findings do not support the current emphasis on early tracheal intubation for peds in-hospital cardiac arrest JAMA. 2016;316(17): doi: /jama

33
34 ARTICLE #4
35 Introduction Asthma accounts for more than 2.1 million unscheduled emergency department (ED) visits annually, with a prevalence that includes 8.4% of the population
36 OBJECTIVE Oral dexamethasone demonstrates bioavailability similar to that of oral prednisone with a longer half-life Evaluate whether a single dose of oral dexamethasone plus 4 days of placebo is not inferior to 5 days of oral prednisone in treatment Adults with mild to moderate asthma exacerbations to prevent relapse


37 Non-Inferiority Prednisone x 5 Dex + placebo x 4
38 Methods Adult ED patients (18 to 55 years) Randomized to receive either single dose of 12 mg of oral dexamethasone with 4 days of placebo 5-day course of oral prednisone 60 mg a day Follow-up phone interview at 2 weeks
39 Results Dexamethasone 173 completed Relapse rates within 14 days 12.1% Hospitalization for relapse dexamethasone 3.4% Prednisone 203 completed Relapse rates within 14 days 9.8% Relapse rates within 14 days 2.9% Adverse effect rates were the same in the 2 groups
40 Conclusion One dose of oral dexamethasone did not demonstrate non-inferiority to prednisone for 5 days by a very small margin for treatment of adults with mild to moderate asthma exacerbations Enhanced compliance and convenience may support the use of dexamethasone regardless
41 Discussion Technically a negative trial These data support, rather than refute, the use of a single dose of dexamethasone in the treatment of asthma with acute exacerbation Statistically, this non-inferiority trials results mean there simply weren t enough patients enrolled to meet their predefined criteria Choice of single-dose dexamethasone is likely as safe as the typical prednisone burst
42 Take Home! Single oral doses of longer-acting corticosteroids might be just as effective as multi-day short courses of prednisone A single dose of oral dexamethasone 12 mg is either similar to or slightly inferior to a 5-day course of prednisone 60 mg for asthma


43 Steroids

44 ARTICLE #5
45 Why bother? ED visits for skin infections have increased with the emergence of MRSA In cellulitis without purulent drainage, β- hemolytic streptococci are presumed to be the predominant pathogens Do antimicrobial regimens possessing in vitro MRSA activity improve outcomes compared with treatments lacking MRSA activity
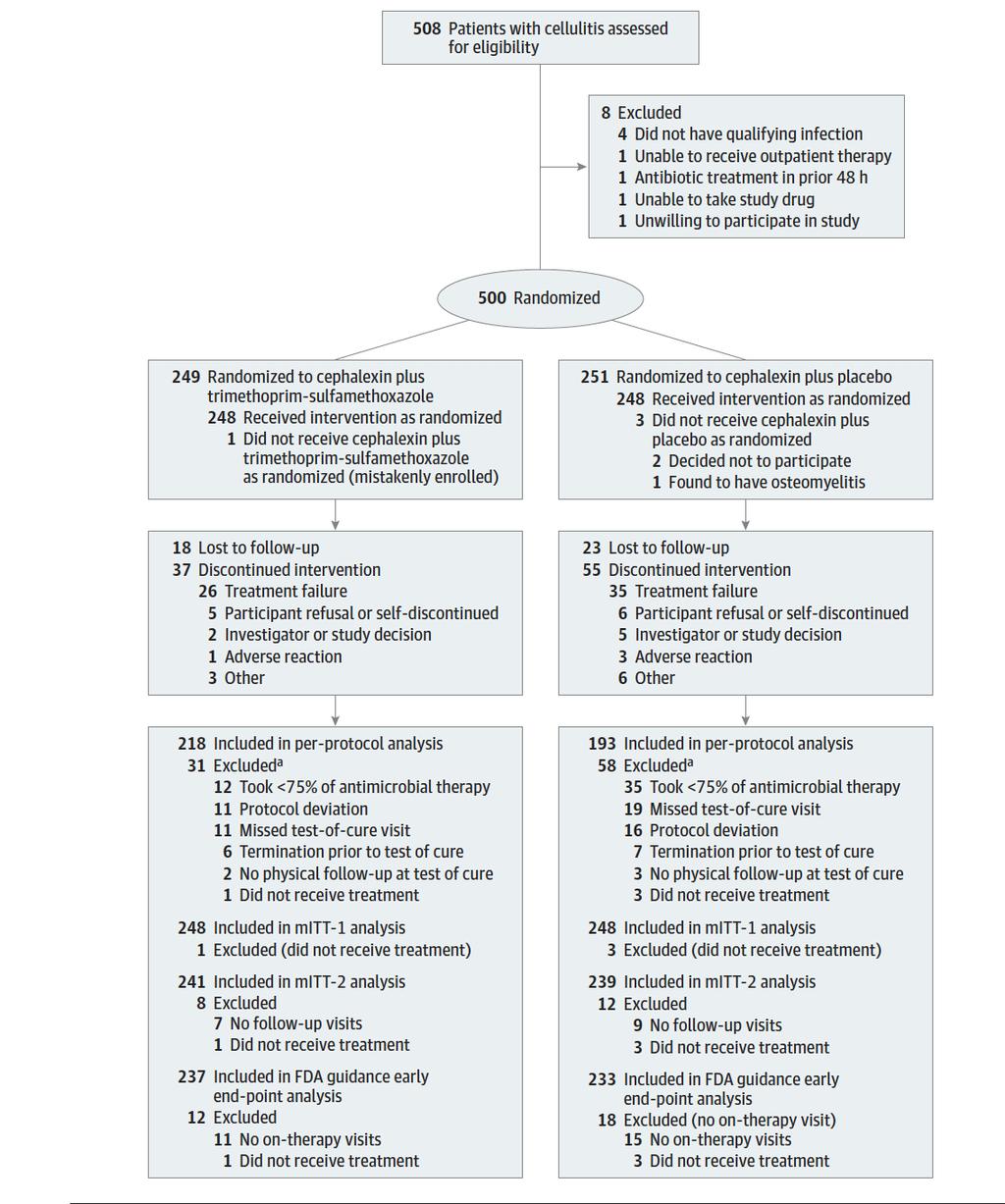
46 Question Does cephalexin + TMP-SMX yield a higher clinical cure rate of uncomplicated cellulitis than cephalexin alone
47 Methods Multicenter, double-blind, RTC superiority 5 US EDs among outpatients Over 12 years of age Cellulitis and no wound, purulent drainage, or abscess April 2009 to June 2012 All had soft tissue US Follow-up August 2012
48 Groups Cephalexin + TMP-SMX Cephalexin + placebo 7 days 7 days (n = 248) (n = 248)
49 Outcomes Primary outcome determined a priori as clinical cure Absence of clinical failure criteria Fever increase in erythema (>25%) swelling, or tenderness (days 3-4) no decrease in erythema, swelling tenderness (days 8-10) More than minimal erythema, swelling, or tenderness (days 14-21) A clinically significant difference was >10%
50

51
52 Limitations US use Rechecked frequently Generalizable?
53 Conclusions For uncomplicated cellulitis Cephalexin plus trimethoprimsulfamethoxazole compared to cephalexin alone did not result in higher rates of clinical resolution

54 No Pus = No MRSA
55 ARTICLE #6
56 Problem Patients want/ need this Sometime take it Toxic to cornea Put out an APB?
57 Methods Outcomes were compared between patients who did or did not received tetracaine
58 Retrospective study Simple corneal abrasions Allow EPs to prescribe topical 1% tetracaine drops q 30 minutes prn for 24
59 Groups 1,576 initial ED presentations 532 simple abrasions 1,044 non-simple corneal abrasions Tetracaine was dispensed at the initial visit 303 simple abrasions (57%) 141 non-simple corneal abrasions (14%)
60
61 Results No serious complications or uncommon adverse events attributed to tetracaine in either group (0/459; upper 95% confidence interval [CI] 0.80%) Relative risks of ED recheck and fluorescein staining were increased overall among patients who received tetracaine (RR 1.67, 95% CI 1.25 to 2.23; and RR 1.65, 95% CI 1.07 to 2.53) Relative risks for only SIMPLE ABRASIONS receiving tetracaine was 1.16 (95% CI 0.69 to 1.93) and 0.77 (95% CI 0.37 to 1.62)
62 Results Referrals to ophthalmology were significantly decreased for all patients dispensed tetracaine (relative risk 0.33; 95% CI 0.19 to 0.59) The number of complications was too small to permit modeling
63 Limitations Not blinded Retrospective No harm found Large review
64 Conclusions There was no evidence that up to 24- hour topical tetracaine for the treatment of pain caused by SIMPLE CORNEAL ABRASIONS was unsafe CIs were wide Increased risks in NOT SIMPLE

65 Tetracaine OK

66 ARTICLE #7
67 Why is it Important? Ketorolac is a NSAID analgesic that is widely used in the ED It is one of few (? the only) medication(s) that has a higher parenteral dose than the oral form Why is that? Is it necessary? Do the benefits outweigh the harms?
68 Methods Single centre randomized double blind study of 240 subjects Compared 3 doses (10mg, 15mg, 30mg) of IV Ketorolac in the treatment of moderate to severe pain (NRS 5) Convenience sample, presenting to ED with predominantly flank, abdominal pain or headache M-F 9-5 enrolled by research team
69 Methods Recorded pain scores at 15, 30, 60, 90 and 120 minute mark Rescue analgesia morphine if still requesting analgesia 30 minutes after study dose
70 Outcome Measures Primary: Reduction in NRS pain scale at 30 minutes from medication administration Secondary: 1. Rates and numbers of patients experiencing adverse effects 2. Numbers of patients requiring rescue analgesia
71 Results at 30 Min. 10 mg Ketorolac NRS mg Ketorolac NRS mg Ketorolac NRS NO SIGNIFICANT DIFFERENCE between the groups with all having a significant reduction in pain
72 Results by Time No significant difference in pain scores across the time points All pts who reported complete resolution of pain DID NOT receive morphine There was no difference in the number of patients requesting rescue morphine across the doses

73 Results by Time
74 Adverse Effects No patients developed unstable vitals Nausea, dizziness and headache were main adverse effects Again no differences between the groups Not powered to look at safety
75 Limitations Small study, one centre No follow up to assess delayed AE such as GI bleeding Not long enough to assess if higher doses give lasting analgesia beyond 120 minutes
76 Conclusions There appears to be little to no benefit of higher parenteral doses of ketorolac A new standard of 10 mg dosing will provide equivalent analgesia and may decrease adverse events


77 Ketorolac

78 ARTICLE #8
79 Why is it Important Uncontrolled atrial fibrillation/flutter is a relatively common condition in the ED Although similar mortality for rate versus rhythm control in long term management acute management is left to clinical judgment, with little evidence to guide either way
80 Questions For patients presenting with acute Afib/ flutter, if choosing a rhythm control strategy, what are the outcomes after ED discharge? Are there certain patients who are higher risk for negative outcomes with this approach?
81 Methods Prospective cohort study Identified all pts (except 29) presenting with acute Afib/flutter at 6 academic EDs in Canada over 2 years Looked at ED management then followed pts for 30 days post discharge Afib/flutter was primary issue (i.e.: excluded ACS, sepsis, PE, pneumonia etc.)
82 Methods Composite outcome: death, stroke, ACS, CHF, subsequent Afib/flutter related hospitalization or subsequent ED cardioversion Logistic regression to look at independent risk factors associated with the composite outcome
83 Results Patients were most likely (72.8%) to be treated with electrical or chemical cardioversion (procainamide most common chemical choice) Only 9% were admitted Eighty percent were in sinus at d/c Only 4.8% were rx d anticoagulant from ED
84 Results MD follow up was recommended but only 50.7% had seen MD by 30 days Only 9.6% of those who did follow up were on some form of anticoagulation
85 Results Overall 10.5% had an adverse event 6.5% required repeat cardioversion 3.2% required admit for Afib/flutter NO DEATHS related to AFib/flutter One ischemic stroke (in anti-coagulated patient)
86 Results Patients leaving ED in sinus rhythm were less likely to have adverse outcome Independent predictors of adverse outcome: Longer duration of Afib/flutter (OR 1.03/hr) Hx stroke/ TIA (OR 2.09) Pulmonary congestion on CXR (OR 7.37) Patients who were chemically cardioverted had lowest risk (OR 0.23) for adverse events
87 Results
88 Conclusions Cardioversion of acute Afib/flutter is associated with few adverse events at 30-day follow up Pts with CHF, Stroke hx and longer duration before ED presentation are higher risk for adverse events Rates of ED and follow up anticoagulation are low Need head to head trial of rate vs. rhythm to assess for superiority

89 Atrial Fibrillation

90 Mensour ARTICLE #9
91 Why does it matter? Drive to continue improving outcomes in cardiac arrest Training and dogma around need for definitive airway Vs many other tasks that need to occur in early ACLS How should we prioritize our time?
92 Methods Retrospective analysis Get-with-the-Guidelines- Resuscitation registry Multicenter Sponsored by AHA All in-hospital cardiac arrests Jan 1, Dec 31, 2004
93 Methods Inclusion: adult, in-hospital, CPR given, no DNR Exclusion: invasive airway at the time, data missing Definitions Tracheal intubation if successful Unsuccessful attempts not counted Time to ROSC or ending CPR without ROSC
94 Methods Outcomes Survival to hospital discharge ROSC Favourable functional outcome Cerebral performance category 1-2 Statistics Matched patients being intubated with non-intubated (yet?) for each time score
95 Results 108,079 total patients 69.9% intubated at some point 94.8% of intubations in first 15 mins Median time of 5 mins
96 Results 22.4% overall survived to discharge Intubated patients had lower survival 17% vs 33.2% (RR 0.58, 95% CI , p< 0.001) 3% absolute reduction in survival 16% relative
97 Results 62.5% of patients attained ROSC Intubated patients less likely to get ROSC 59.2% vs 69% (RR 0.75, 95% CI , p<0.001) 2% absolute reduction Similar results for functional outcome but some data missing
98 Subgroups etc. Effect of tracheal intubation lowering survival: most pronounced if initially had shockable rhythm 32% relative decrease vs 9% Not present if presented with respiratory insufficiency!
99 Limitations Matched cases to others within data set who were potentially intubated later Indication for intubation, cause of arrest, and skill level not specifically recorded in registry Unsuccessful attempts not logged But would have biased to null
100 Conclusions In adults with in-hospital cardiac arrest. Initiation of tracheal intubation at any point in first 15mins was associated with worse scores on all outcomes vs not intubating Probably we shouldn t be doing this early/as a matter of priority Congruent with current guidelines
101 Conclusions In adults who arrest in hospital 70% got intubated within 15mins ¼ survived to hospital discharge 1/6 had good neurological status

102

103 ARTICLE #10 Academic Emergency Medicine 2017;24:
104 Why does it matter? Traumatic intracranial bleeding is the feared complication of head injury How can we apply decision rules to our patients? Are anti-platelets as scary as anticoagulants? full dose antiplatelet vs small?
105
106 Methods Consecutive patients at trauma center Prospective, observational, cohort Inclusion Adult patients (>18) Ground-level fall (or lesser mechanism) On ASA, clopidogrel, warfarin, LMWH, DOACs, other antiplatelets Exclusion Injury >24 hours Patients transferred with known injury
107 Methods Treating clinician noted ground level fall + antiplatelet or anticoagulant All received CT scan on first visit Outcomes Primary: traumatic bleed Subdural, epidural, subarachnoid, intraparenchymal Secondary: clinical characteristics, intervention, disposition
108 Results 939 patients enrolled 78% were on ASA 71% alone 24% on Warfarin 3.3% on DOAC Some on multiple agents Mean age: 78 (+/-11.9 years)
109 Results 33 intracranial hemorrhages 3.5% of all cases reviewed 99% were awake and alert, only 30% had LOC Antiplatelets: rate of 4.3% (3-6.2% CI) And 82% of those who bled on ASA were on 81mg alone Anticoagulants: 1.7% ( %) Mean INR on warfarin 3.3
110 Results Medical interventions in several Vit K, FFP, platelets 0.4% rate of surgery or death 2 craniotomies 4 deaths 3 on ASA alone
111 Limitations Fair approximation of patient population, although all low risk First presentation, well at triage Needed CT head for age alone Numbers in the non-asa groups were small, less reliable No control group Can t confirm if were taking Rx Could bleeds have preceded fall?
112 Conclusions No statistical difference between tich rate on anti-platelet or anti-coagulants Including low dose ASA! Because platelets are important earlier in clotting cascade? Because strength of inhibition not measureable? Beware both yourself and patients being falsely reassured about risk

113


114
Anticoagulants and Head Injuries. Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar
 Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Anticoagulants and Head Injuries Asaad Shujaa,MD,FRCPC,FAAEM Assistant Professor,weill Corneal Medicne Senior Consultant,HMC Qatar Common Anticoagulants and Indications Coumadin (warfarin) indicated for
Atrial Fibrillation is Common. The (S)Low-down on Rapid Afib Resuscitation Step ED Dx - Rx 4/4/2017. There Are 5 Causes of Atrial Fibrillation
Low-down on Rapid Afib Resuscitation Step ED Dx - Rx 4/4/2017. There Are 5 Causes of Atrial Fibrillation") The (S)Low-down on Rapid Afib Resuscitation 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial Fibrillation
The (S)Low-down on Rapid Afib Resuscitation 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial Fibrillation
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Enhancing 5 th Chain TTM after Cardiac Arrest
 Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
Enhancing 5 th Chain TTM after Cardiac Arrest Seoul St. Mary s Hospital Department of Emergency Medicine Chun Song Youn Agenda Past Current Future First study, 1958 2002, Two landmark paper HACA Trial
VanderbiltEM.com. Atrial Fibrillation Update Don t Miss a Beat ACEP Atrial Fibrillation is Common
 Atrial Fibrillation Update Don t Miss a Beat ACEP 2016 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Atrial Fibrillation Update Don t Miss a Beat ACEP 2016 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Supplementary Online Content
 Supplementary Online Content Hasegawa K, Hiraide A, Chang Y, Brown DFM. Association of prehospital advancied airway management with neurologic outcome and survival in patients with out-of-hospital cardiac
Supplementary Online Content Hasegawa K, Hiraide A, Chang Y, Brown DFM. Association of prehospital advancied airway management with neurologic outcome and survival in patients with out-of-hospital cardiac
Dental Management Considerations for Patients on Antithrombotic Therapy
 Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Dental Management Considerations for Patients on Antithrombotic Therapy Warfarin and Antiplatelet Joel J. Napeñas DDS FDSRCS(Ed) Program Director General Practice Residency Program Department of Oral Medicine
Emergency Medicine Research: Creating Evidence to Improve Safety and Effectiveness of ED Patient Care
 Emergency Medicine Research: Creating Evidence to Improve Safety and Effectiveness of ED Patient Care Dr Eric Clark MD, FRCPC Department of Emergency Medicine University of Ottawa Canada No Conflicts of
Emergency Medicine Research: Creating Evidence to Improve Safety and Effectiveness of ED Patient Care Dr Eric Clark MD, FRCPC Department of Emergency Medicine University of Ottawa Canada No Conflicts of
CPR What Works, What Doesn t
 Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
Resuscitation 2017 ECMO and ECLS April 1, 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Circulation 2013;128:417-35
What A Headache! Theresa Biesiada March 8, 2012
 What A Headache! Theresa Biesiada March 8, 2012 Objectives Describe the EM relevance of headaches and migraines Discuss the rationale for steroid therapy Review the evidence Conclusions My inspiration
What A Headache! Theresa Biesiada March 8, 2012 Objectives Describe the EM relevance of headaches and migraines Discuss the rationale for steroid therapy Review the evidence Conclusions My inspiration
Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD
: What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD") Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting
Myocardial Injury after Noncardiac Surgery (MINS): What is it and what can we do to help patients suffering this event? PJ Devereaux, MD, PhD Disclosure Member of research group with policy of not accepting
Updates in Stroke Management. Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy
 Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
Updates in Stroke Management Jessica A Starr, PharmD, FCCP, BCPS Associate Clinical Professor Auburn University Harrison School of Pharmacy Disclosure I have no actual or potential conflict of interest
2016 Top Papers in Critical Care
 2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience
2016 Top Papers in Critical Care Briana Witherspoon DNP, APRN, ACNP-BC Assistant Director of Advanced Practice, Neuroscience Assistant in Division of Critical Care, Department of Anesthesiology Neuroscience
Lesson learnt from big trials. Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ.
 Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
Lesson learnt from big trials Sung Phil Chung, MD Gangnam Severance Hospital, Yonsei Univ. Trend of cardiac arrest research 1400 1200 1000 800 600 400 200 0 2008 2009 2010 2011 2012 2013 2014 2015 2016
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine
 Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Joshua D. Lenchus, DO, RPh, FACP, SFHM Associate Professor of Medicine and Anesthesiology University of Miami Miller School of Medicine Antithrombotics Antiplatelets Aspirin Ticlopidine Prasugrel Dipyridamole
Hit head, on blood thinner-wife wants CT. Will Davies June 2014
 Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Hit head, on blood thinner-wife wants CT Will Davies June 2014 Selection of Adults with Head Injury for CT Scan Early management of head injury: summary of updated NICE guidance. Hodgkinson S, Pollit V,
Outcomes of Therapeutic Hypothermia in Cardiac Arrest. Saad Mohammed Shariff, MBBS Aravind Herle, MD, FACC
 Outcomes of Therapeutic Hypothermia in Cardiac Arrest Saad Mohammed Shariff, MBBS Aravind Herle, MD, FACC https://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/@scon/documents/downloadable/ucm_427331.pdf
Outcomes of Therapeutic Hypothermia in Cardiac Arrest Saad Mohammed Shariff, MBBS Aravind Herle, MD, FACC https://my.americanheart.org/idc/groups/ahamah-public/@wcm/@sop/@scon/documents/downloadable/ucm_427331.pdf
Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion. Greg Francisco, MD, FACC
 Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion Greg Francisco, MD, FACC DISCLOSURES None to declare Estimated 33.5million have AF worldwide (6-7million in
Primary Care Atrial Fibrillation Update: Anticoagulation and Left Atrial Appendage Occlusion Greg Francisco, MD, FACC DISCLOSURES None to declare Estimated 33.5million have AF worldwide (6-7million in
How did I decide on the topics?
 Disclosures None How did I decide on the topics? Important papers within 1 year vs topics of importance or innovation/aha moments Sepsis Atrial Fibrillation Pneumonia Procalcitonin Objectives By the end
Disclosures None How did I decide on the topics? Important papers within 1 year vs topics of importance or innovation/aha moments Sepsis Atrial Fibrillation Pneumonia Procalcitonin Objectives By the end
CLOSE. Closure of Patent Foramen Ovale, Oral anticoagulants or Antiplatelet Therapy to Prevent Stroke Recurrence
 CLOSE Closure of Patent Foramen Ovale, Oral anticoagulants or Antiplatelet Therapy to Prevent Stroke Recurrence Guillaume TURC, MD, PhD Paris Descartes University Sainte-Anne hospital Paris, France On
CLOSE Closure of Patent Foramen Ovale, Oral anticoagulants or Antiplatelet Therapy to Prevent Stroke Recurrence Guillaume TURC, MD, PhD Paris Descartes University Sainte-Anne hospital Paris, France On
High Risk + Challenging Trauma Cases. Hawaii. Topics 1/27/2014. David Thompson, MD, MPH. Head injury in the anticoagulated patient.
 High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
High Risk + Challenging Trauma Cases David Thompson, MD, MPH Hawaii Topics Head injury in the anticoagulated patient Shock recognition Case 1: Head injury HPI: 57 yo male w/ PMH atrial fibrillation, on
Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion
 Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion John Rickard MD, MPH Staff Electrophysiologist Cleveland Clinic Agenda NOACs: Update on Real World Data NOAC reversal:
Role of NOACs in AF Management. From Evidence to Real World Data Focus on Cardioversion John Rickard MD, MPH Staff Electrophysiologist Cleveland Clinic Agenda NOACs: Update on Real World Data NOAC reversal:
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Geriatric Grand Rounds
 Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 13, 21 12: noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS
 EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
EXTENDING VTE PROPHYLAXIS IN ACUTELY ILL MEDICAL PATIENTS Samuel Z. Goldhaber, MD Director, VTE Research Group Cardiovascular Division Brigham and Women s Hospital Professor of Medicine Harvard Medical
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials
 Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Using DOACs in CAD Patients in Sinus Ryhthm Results of the ATLAS ACS 2, COMPASS and COMMANDER-HF Trials 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La
Newer Anti-Anginal Agents and Anticoagulants
 Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
Newer Anti-Anginal Agents and Anticoagulants Satish Gadi, MD FACC FSCAI Interventional Cardiologist, Cardiovascular Institute of the South (CIS) Baton Rouge Clinical Assistant Professor, Tulane University
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC
 MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
MODULE 1: Stroke Prevention in Atrial Fibrillation Benjamin Bell, MD, FRCPC Specialty: General Internal Medicine Lecturer, Department of Medicine University of Toronto Staff Physician, General Internal
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases?
 Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Atrial Fibrillaiton and Heart Failure: Anticoagulation therapy in all cases? Nicolas Lellouche Fédération de Cardiologie Hôpital Henri Mondor Créteil Disclosure Statement of Financial Interest I currently
Mohammad Zubaid, MB, ChB, FRCPC, FACC
 Management and one year outcome of atrial fibrillation in Middle Eastern cohort enrolled in the observational Gulf Survey of Atrial Fibrillation Events (Gulf SAFE) Mohammad Zubaid, MB, ChB, FRCPC, FACC
Management and one year outcome of atrial fibrillation in Middle Eastern cohort enrolled in the observational Gulf Survey of Atrial Fibrillation Events (Gulf SAFE) Mohammad Zubaid, MB, ChB, FRCPC, FACC
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
AF stroke prevention in the Canadian context
 AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
AF stroke prevention in the Canadian context 5 th Annual State of the Heart Toronto, May 31, 2014 Andrew C.T. Ha, MD, MSc, FRCPC Cardiac Electrophysiology Toronto General Hospital, University Health Network
Antithrombotics in Stroke management
 Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Antithrombotics in Stroke management Faculty: Robert Beveridge Relationships with commercial interests: Grants/Research Support: N/A Speakers Bureau/Honoraria: Astra Zeneca, Bayer, Boerhinger Ingelheim,
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Prostate Biopsy Alerts
 Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
Prostate Biopsy Alerts Saskatchewan Prostate Assessment Pathway Guidelines for the Primary Care Provider for Patient Preparation and the Management of Medications and Complications September 2016 Table
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Kiehl EL, 1,2 Parker AM, 1 Matar RM, 2 Gottbrecht M, 1 Johansen MC, 1 Adams MP, 1 Griffiths LA, 2 Bidwell KL, 1 Menon V, 2 Enfield KB, 1 Gimple LW 1
 C-GRApH: A Validated Scoring System For The Early Risk Stratification Of Neurologic Outcomes After Out-of-hospital Cardiac Arrest Treated With Therapeutic Hypothermia Kiehl EL, 1,2 Parker AM, 1 Matar RM,
C-GRApH: A Validated Scoring System For The Early Risk Stratification Of Neurologic Outcomes After Out-of-hospital Cardiac Arrest Treated With Therapeutic Hypothermia Kiehl EL, 1,2 Parker AM, 1 Matar RM,
Epinephrine Cardiovascular Emergencies Symposium 2018
 Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Epinephrine Cardiovascular Emergencies Symposium 218 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN High Quality
Atrial Fibrillation is Common. ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat. Incidence of Atrial Fibrillation by Age
 ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial
ACEP 2017 Atrial Fibrillation Update 2017 Don t Miss a Beat Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Atrial
Atrial Fibrillation. Epidemiology. Goals 11/12/2012. Faithful marker for age and underlying cardiopulmonary disease
 Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
Atrial Fibrillation Goals the emerging epidemic Rate Control Thromboembolism and anticoagulation Cardioversion: When, How, and Why 1st time AF < 48hr 1st time AF > 48hr PAF < 48 hr. PAF > 48 hr. Eric R.
VanderbiltEM.com. Atrial Fibrillation Update Don t Miss a Beat ACEP AFib. 20 Facts on Atrial Fibrillation in 20 minutes
 Atrial Fibrillation Update Don t Miss a Beat ACEP 2015 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Atrial Fibrillation Update Don t Miss a Beat ACEP 2015 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Lumbar puncture. Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: ml Replenished: 4-6 h Routine LP (3-5 ml): <1h
: <1h") Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Lumbar puncture Lumbar puncture Invasive procedure: diagnostic or therapeutic. The subarachnoid space 4-13 ys: 65-150ml Replenished: 4-6 h Routine LP (3-5 ml):
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre
 Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
Dr Julia Hopyan Stroke Neurologist Sunnybrook Health Sciences Centre Objectives To learn what s new in stroke care 2010-11 1) Acute stroke management Carotid artery stenting versus surgery for symptomatic
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital
 New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
New options in Stroke Prevention in AF Paul Dorian University of Toronto St Michael s Hospital Disclosures: Honoraria, research support, and consulting f Sanofi, Boehringer-Ingleheim, Portola, BMS, Bayer,
Afib, Stroke, and DOAC. Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS
 Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Afib, Stroke, and DOAC Albert Luo, MD. Cardiology Lindsey Frischmann, DO. Neurology Xiao Cai, MD. HBS Disclosure of Relevant Financial Relationships I have no relevant financial relationships with commercial
Atrial Fibrillation and Heart Failure: A Cause or a Consequence
 Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
Atrial Fibrillation and Heart Failure: A Cause or a Consequence Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology, Electrophysiology Section University of Pennsylvania November
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin?
 MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
MMS/Mass Coalition Program, Nov. 4, 2008 Patients with AF: Who Should be on Warfarin? Daniel E. Singer, MD Massachusetts General Hospital Harvard Medical School 1 Speaker Disclosure Information DISCLOSURE
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #326 (NQF 1525): Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY
Quality ID #326 (NQF 1525): Atrial Fibrillation and Atrial Flutter: Chronic Anticoagulation Therapy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY
Anticoagulation Therapy in LTC
 Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
Anticoagulation Therapy in LTC By: Cynthia Leung, RPh, BScPhm, PharmD. Clinical Consultant Pharmacist MediSystem Pharmacy Jun 11, 2013 Agenda Stroke and Bleeding Risk Assessment Review of Oral Anticoagulation
VanderbiltEM.com. Prehospital STEMIs. EMS Today 2018 Research That Should Be On Your Radar Screen 3/1/2018
 EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
EMS Today 2018 Research That Should Be On Your Radar Screen Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN VanderbiltEM.com
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
The changing face of
 The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
The changing face of sepsis. @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO Breast cancer Cognitive impairment Mild 3.8 7.1
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Major Points. The ED-ICU Interface. Chain of Survival. It usually starts here
 Major Points The ED-ICU Interface Robert M. Rodriguez, MD FAAEM Most ICU patients start in ED Chain of critical care starting in field and ED Collaborate, develop protocols (define roles), communicate
Major Points The ED-ICU Interface Robert M. Rodriguez, MD FAAEM Most ICU patients start in ED Chain of critical care starting in field and ED Collaborate, develop protocols (define roles), communicate
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Palliative Sedation An ICU Perspective. William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC
 Department of Critical Care Thunder Bay Regional HSC") Palliative Sedation An ICU Perspective William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC Conflict Disclosure Information: Presenter: Dr. Will Anderson I have no financial
Palliative Sedation An ICU Perspective William Anderson; B.Sc. MD FRCP(C) Department of Critical Care Thunder Bay Regional HSC Conflict Disclosure Information: Presenter: Dr. Will Anderson I have no financial
Goals. Geriatric Trauma. What s the impact Erlanger Trauma Symposium
 Geriatric Trauma William S. Havron III MD Assistant Professor of Surgery University of Oklahoma Goals Realize the impact of injuries in the ageing population Identify the pitfalls associated with geriatric
Geriatric Trauma William S. Havron III MD Assistant Professor of Surgery University of Oklahoma Goals Realize the impact of injuries in the ageing population Identify the pitfalls associated with geriatric
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Show Me the Outcomes!
 Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Show Me the Outcomes! Real-World Safety Data on Oral Anticoagulants in Nonvalvular Atrial Fibrillation Gabby Anderson, PharmD PGY1 Pharmacy Resident anderson.gabrielle@mayo.edu Pharmacy Grand Rounds October
Left Atrial Appendage Occlusion
 Left Atrial Appendage Occlusion A new strategy to prevent stroke in atrial fibrillation Ashok Talreja MD and Arijit Chanda MD VHVI symposium 24th February 2018 Outline of presentation 1. Risk of stroke
Left Atrial Appendage Occlusion A new strategy to prevent stroke in atrial fibrillation Ashok Talreja MD and Arijit Chanda MD VHVI symposium 24th February 2018 Outline of presentation 1. Risk of stroke
In this article, discussing the (almost**) latest addition to PE/Dimer studies:
 latest addition to PE/Dimer studies:") Summary RAP 24: GI/Pulm/Skin Is the Road to Hell Paved with D-Dimers? Reviewed by: Caitlin Ward General topic : Recent studies utilizing D-dimer in detection of pulmonary embolism. Begins by mentioning
Summary RAP 24: GI/Pulm/Skin Is the Road to Hell Paved with D-Dimers? Reviewed by: Caitlin Ward General topic : Recent studies utilizing D-dimer in detection of pulmonary embolism. Begins by mentioning
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni. Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna
 NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
NUOVI ANTICOAGULANTI NELL ANZIANO: indicazioni e controindicazioni Mario Cavazza Medicina d Urgenza Pronto Soccorso AOU di Bologna Two major concerns Atrial Fibrillation: Epidemiology The No. 1 preventable
On behalf of the RE-CIRCUIT Investigators. March 19, :45 am 10:55 am. Johns Hopkins Medical Institutions, Baltimore, MD, USA.
 Safety and Efficacy of Uninterrupted Anticoagulation with Dabigatran Etexilate versus in Patients Undergoing Catheter Ablation of Atrial Fibrillation: The RE-CIRCUIT Study Hugh Calkins, M.D., 1 Stephan
Safety and Efficacy of Uninterrupted Anticoagulation with Dabigatran Etexilate versus in Patients Undergoing Catheter Ablation of Atrial Fibrillation: The RE-CIRCUIT Study Hugh Calkins, M.D., 1 Stephan
4. Which survey program does your facility use to get your program designated by the state?
 TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
TRAUMA SURVEY Please complete one survey for each TCD designation you have in your facility. There would be a maximum of three surveys completed if your facility was designated as a trauma, stroke and
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Multidisciplinary Geriatric Trauma Care Guideline
 Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Multidisciplinary Geriatric Trauma Care Background Traumatic injury in the geriatric population is increasing in prevalence and is associated with higher mortality and complication rates comparted to younger
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Dual Antiplatelet Therapy Made Practical
 Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Dual Antiplatelet Therapy Made Practical David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management Clinical Associate Professor
Resuscitation Articles 2017
 Resuscitation Articles 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Annal Emerg Med 2017;Epub ahead of print
Resuscitation Articles 2017 Corey M. Slovis, M.D. Vanderbilt University Medical Center Metro Nashville Fire Department Nashville International Airport Nashville, TN Annal Emerg Med 2017;Epub ahead of print
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis
 Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Apixaban for Atrial Fibrillation in Patients with End-Stage Renal Disease on Dialysis Caitlin Reedholm, PharmD PGY1 Pharmacy Resident St. David s South Austin Medical Center November 2, 2018 Abbreviations
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm
 Overall Algorithm") Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
Family Centered Pediatric Emergency Department Sickle Cell Assessment of Needs and Strengths (FC-Peds-ED-SCANS) Overall Algorithm Decision 1: Triage Decision 2: Analgesic Management Decision 3: Diagnostic
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION
 ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
ANTI-THROMBOTIC THERAPY in NON-VALVULAR ATRIAL FIBRILLATION Colin Edwards Auckland Heart Group Waitemata Health June 2015 PFIZER Lecture series Disclosures EPIDEMIOLOGY Atrial fibrillation is the most
Therapeutic hypothermia
 INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
INDUCED HYPOTHERMIA Dr. Attilla Kiss M.D. Acting Medical Director Emergency Services EMS Medical Director St. John Medical Center OBJECTIVES Define and explain Induced Hypothermia Discuss both pre-hospital
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Rate or Rhythm Control? Epidemiology. Relevant Advances in Atrial Fibrillation 6/20/2011. Stroke Prophylaxis
 Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Relevant Advances in Atrial Fibrillation Stroke Prophylaxis Managing Atrial Fibrillation: Tips for the Generalist Antiarrhythmic Drug Therapy Ablation Gregory M Marcus, MD, MAS Assistant Professor of Medicine
Role and safety of epidural analgesia
 Anaesthesia for Liver Resection Surgery The Association of Anaesthetists Seminars 21 Portland Place, London Thursday 15 th December 2005 Role and safety of epidural analgesia Lennart Christiansson MD,
Anaesthesia for Liver Resection Surgery The Association of Anaesthetists Seminars 21 Portland Place, London Thursday 15 th December 2005 Role and safety of epidural analgesia Lennart Christiansson MD,
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation
 The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
Scenario Development Template
 Scenario Development Template Scenario Title: Inf STEMI, ICH, PEA Arrest Author: E. Merrick Last edit: April 12, 2018 Set up: Confederates: Duration: Scenario 20 min Debriefing 30 min Learning Objectives:
Scenario Development Template Scenario Title: Inf STEMI, ICH, PEA Arrest Author: E. Merrick Last edit: April 12, 2018 Set up: Confederates: Duration: Scenario 20 min Debriefing 30 min Learning Objectives:
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
New Antithrombotic Agents DISCLOSURE
 New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
New Antithrombotic Agents DISCLOSURE Relevant Financial Relationship(s) Speaker Bureau None Research Alexion (PNH) delought@ohsu.edu Tom DeLoughery, MD FACP FAWM Oregon Health and Sciences University What
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
GSK Medicine: Study Number: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Disclosures. Pediatrician Financial: none Volunteer :
 Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
Brain Resuscitation Neurocritical Care Monitoring & Therapies CCCF November 2, 2016 Anne-Marie Guerguerian Critical Care Medicine, The Hospital for Sick Children University of Toronto Disclosures Pediatrician
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Warfarin and the risk of major bleeding events in patients with atrial fibrillation: a population-based study Laurent Azoulay PhD 1,2, Sophie Dell Aniello MSc 1, Teresa
DECLARATION OF CONFLICT OF INTEREST Warfarin and the risk of major bleeding events in patients with atrial fibrillation: a population-based study Laurent Azoulay PhD 1,2, Sophie Dell Aniello MSc 1, Teresa
Rapid Response Teams and End-of-Life Care. James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto
 Rapid Response Teams and End-of-Life Care James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto Conflicts of Interest To place your ad here, please call
Rapid Response Teams and End-of-Life Care James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto Conflicts of Interest To place your ad here, please call
Manuel Castella MD PhD Hospital Clínic, University of
 Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Manuel Castella MD PhD Hospital Clínic, University of Barcelona mcaste@clinic.ub.es @mcastellamd www.escardio.org/guidelines European Heart Journal - doi:10.1093/eurheartj/ehw210 Providing integrated care
Challenges in Anticoagulation Bridging and Emerging Therapies. Disclosures and Relationships. Objectives. Dr. Cumbler has no conflicts of interest
 Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Challenges in Anticoagulation Bridging and Emerging Therapies Ethan Cumbler MD FACP Associate Professor of Medicine Hospitalist Medicine Section University of Colorado Denver 2011 Disclosures and Relationships
Saudi Heart Association February 22, 2011
 Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Pharmacological Therapy of Atrial Fibrillation: Recent Advances Dr Martin Green Professor of Medicine (Cardiology) University of Ottawa Saudi Heart Association February 22, 2011 Atrial Fibrillation Drugs
Data Collection Tool. Standard Study Questions: Admission Date: Admission Time: Age: Gender:
 Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Kenneth W. Mahaffey, MD and Keith AA Fox, MB ChB
 Once-daily oral direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation Kenneth W. Mahaffey, MD and Keith AA Fox, MB ChB on behalf
Once-daily oral direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation Kenneth W. Mahaffey, MD and Keith AA Fox, MB ChB on behalf
8.0 Parenteral Nutrition vs. Standard care May 2015
 8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition