The changing face of
|
|
|
- Myles Hunt
- 5 years ago
- Views:
Transcription
1 The changing face of Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser (maternal sepsis) to WHO
2
3 Breast cancer

4

5


6 Cognitive impairment Mild Moderate-severe Before sepsis After sepsis Iwashyna et al: Long-term cognitive impairment & functional disability among survivors of severe sepsis. JAMA, 2010.

7 Basics limit severity
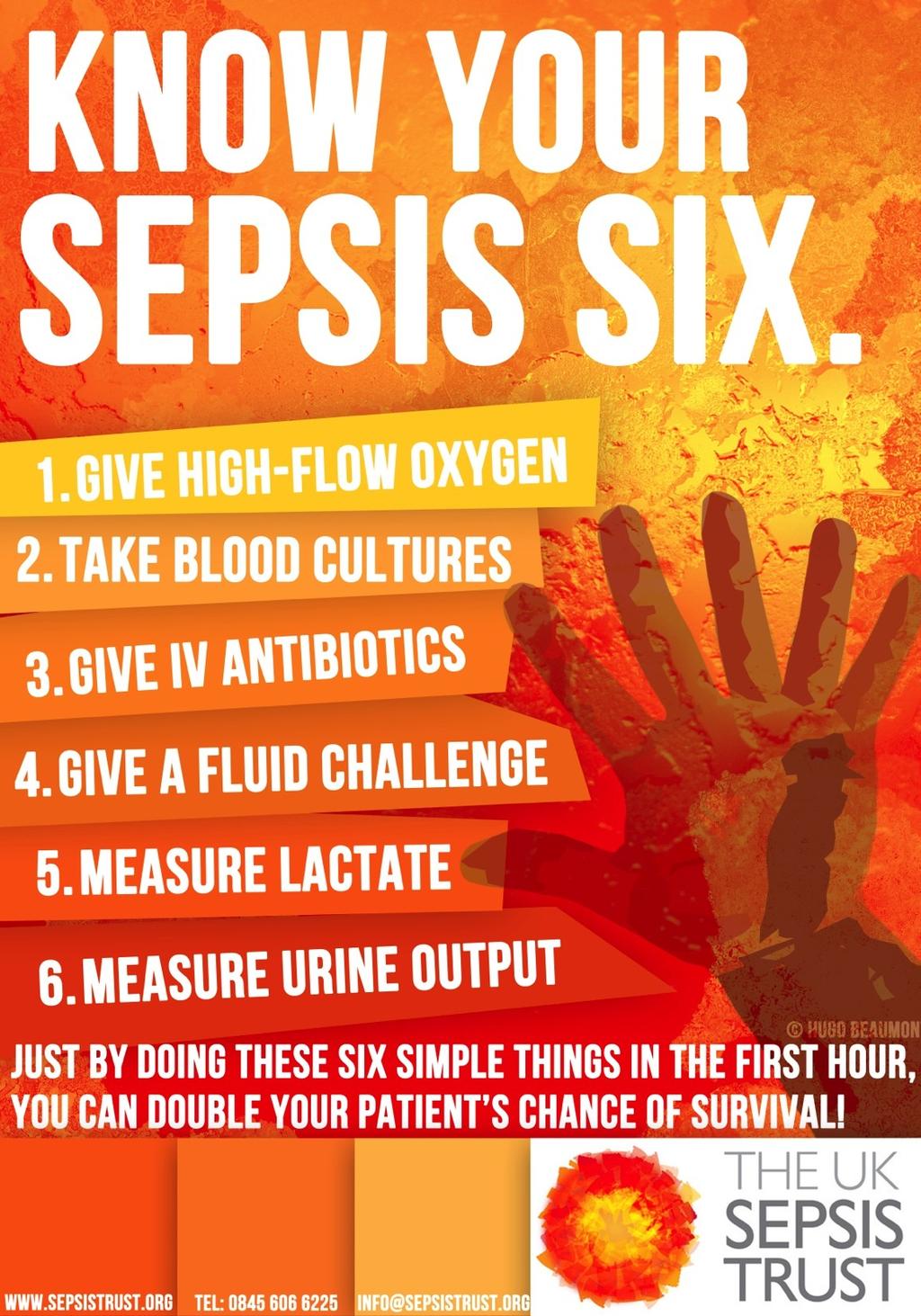
8 The Sepsis Six 1. Give oxygen as needed 94% to target SpO 2 > 2. Take blood cultures control consider source 3. Give IV antibiotics protocol according to local 4. Start IV fluid resuscitation equivalent Hartmann s or 5. Check lactate repeat within 2h 6. Monitor..plus Critical urine Care output support to consider complete EGDT catheterisation
9 @SepsisUK NCEPOD 2015

10 54% of patients had sepsis pre-hospital 80% acquired infection in community
11
12
13 @SepsisUK Recognition 2014
14 Infection Sepsis Severe Sepsis Septic shock Burns Burns Systemic Inflammatory Hypoperfusion Response (SIRS) Organ dysfunction
15 <1% 10% 30% 50% Infection Sepsis Severe Sepsis Septic shock Burns Burns Systemic Inflammatory Hypoperfusion Response (SIRS) Organ dysfunction

16 CVS SBP <90, MAP <70, or SBP decrease >40 SvO 2 70% or ScvO 2 <65% Cardiac index <3.5 Lmin -1 Decreased capillary refill or mottling Lactate >2 mmoll -1 RS PaO 2 /FIO 2 <300 or SpO 2 <90% Renal Urine output <0.5 mlkg -1 hr -1 for 2 hrs Creatinine >177 micromoll -1 Hepatic Bilirubin >4 mgdl-1 or >70mmolL -1 Coagulation INR >1.5 or aptt >60s Platelets <100,000 x 10 6 L -1 GI Ileus
17 Septic shock For each hour s delay in administering antibiotics, mortality increases by 7.6% Funk and Kumar Critical Care Clinics 2011 (in press)

18 Infection Sepsis Severe Sepsis Septic shock Burns Burns
19
20 <1% 10% 35% 50% Severe Infection Sepsis Sepsis Septic shock Burns Burns Systemic Inflammatory Response (SIRS)
21 Recognition
22 Infection Sepsis Badness Burns Burns
23 Infection Sepsis Septic shock Badness Burns Burns
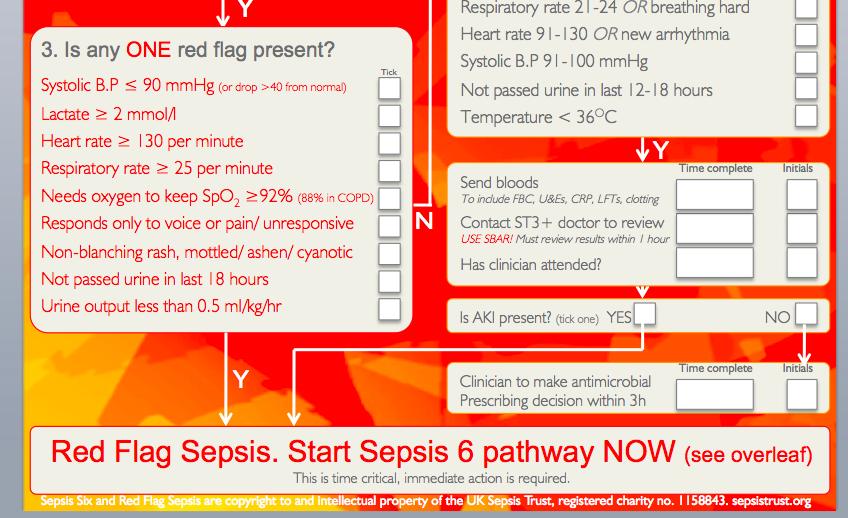
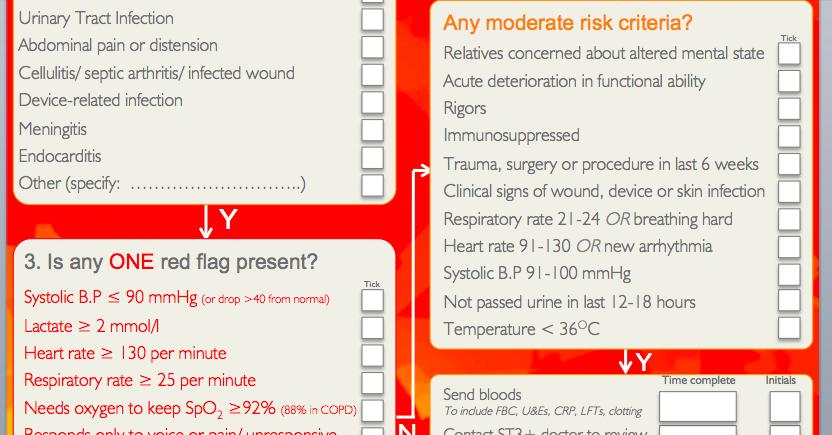
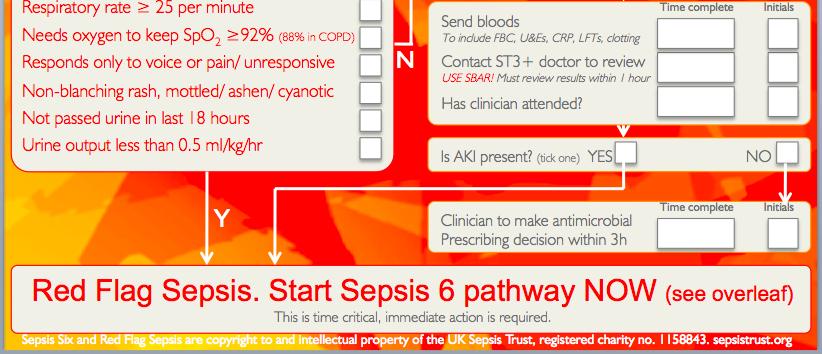
24 3. Is any RED FLAG present? Systolic B.P <90mmHg/ >40mmHg below n. Lactate > 2 mmol/l Heart rate > 130 per minute Respiratory rate > 25 per minute Oxygen saturations < 92% (unless COPD) Responds only to voice or pain/ unresponsive Purpuric rash/ mottled/ ashen/ cyanotic Not passed urine for 18 hours Y Red Flag Sepsis This is a time critical condition, immediate action is required. Assume severe sepsis present. Sepsis Six 1 High-flow oxygen. 2 Blood cultures and consider source control. 3 Intravenous antibiotics. 4 Intravenous fluid resuscitation. 5 Check haemoglobin and serial lactates. 6 Hourly urine output measurement. Record the time each of these actions is completed. All actions should be completed as soon as possible but always within 60 minutes. Communication: Inform senior clinician (e.g. registrar or above). Additional: Bloods should include: FBC, U/E s, LFT s, clotting profile. Observations should be taken every 30 mins Lactate should be repeated within 2 hours. Perform a CXR and Urinalysis Consider source control ( e.g. surgical intervention)
25

26
27 3. Is any red flag present? Systolic B.P <90 mmhg/ MAP <65 mmhg Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Oxygen saturations <91% Responds only to voice or pain/unresponsive Purpuric rash
28 3. Is any red flag present? Systolic B.P <90 mmhg/ MAP <65 mmhg Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Oxygen saturations <91% Responds only to voice or pain/unresponsive Purpuric rash
29 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Oxygen saturations <91% Responds only to voice or pain/unresponsive Purpuric rash
30 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Oxygen saturations <91% Responds only to voice or pain/unresponsive Purpuric rash
31 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Oxygen saturations <91% Responds only to voice or pain/unresponsive Purpuric rash
32 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Oxygen saturations <91% Responds only to voice or pain/unresponsive Purpuric rash
33 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Oxygen saturations <91% Responds only to voice or pain/unresponsive Purpuric rash
34 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Needs oxygen to keep SpO 2 >92% Responds only to voice or pain/unresponsive Purpuric rash
35 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Needs oxygen to keep SpO 2 >92% Responds only to voice or pain/unresponsive Purpuric rash
36 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Needs oxygen to keep SpO 2 >92% Responds only to voice or pain/unresponsive Purpuric rash
37 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Needs oxygen to keep SpO 2 >92% Responds only to voice or pain/unresponsive Purpuric rash/ mottled/ ashen/ cyanotic
38 3. Is any red flag present? Systolic B.P <90 mmhg/ >40mmHg below n. Lactate >2 mmol/l Heart rate >130 per minute Respiratory rate >25 per minute Needs oxygen to keep SpO 2 >92% Responds only to voice or pain/unresponsive Purpuric rash/ mottled/ ashen/ cyanotic Not passed urine for 18 hours
:!...!!!!! Staff member completing form: Date: (DD/MM/YY):! Name (print):! Designation:! Signature:!")
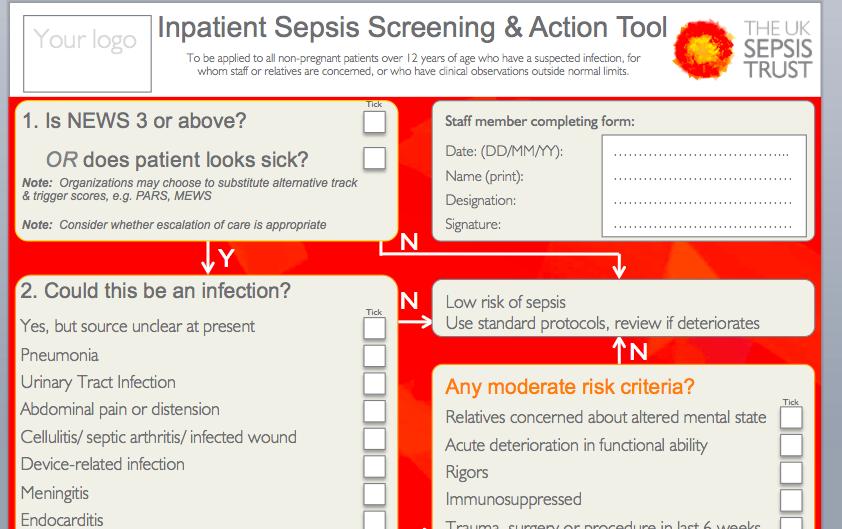
39 !!!!!! Sepsis Screening & Action Tool To be applied to all non-pregnant patients over 16 years who have suspected infection, for whom staff or relatives are concerned, or who have clinical observations outside normal limits.!! Patient details (affix label):!...!!!!! Staff member completing form: Date: (DD/MM/YY):! Name (print):! Designation:! Signature:!...!!!! Important: Is an end of life pathway in place/ is escalation clinically inappropriate? Yes Initials Discontinue pathway! 1. Is NEWS 3 or above? And/or does patient looks sick? Y 2. Could this be due to an infection?! Yes, but source unclear at present! Pneumonia! Urinary Tract Infection! Abdominal pain or distension! Cellulitis/ septic arthritis/ infected wound! Device-related infection! Meningitis! Other (specify:..)! Y 3. Is any ONE red flag present? Systolic BP 90 mmhg (or drop > 40 from normal)! Lactate 2 mmol/l! Red NEWS score for Respiratory Rate (RR)! Red NEWS score for Heart Rate (HR)! Red NEWS score for conscious level! Needs oxygen to keep SpO 2 92% (88% in COPD)! Non-blanching rash, mottled/ ashen/ cyanotic! Oliguria (from history or less than 0.5 ml/kg/hr)! Recent chemotherapy! Y Tick Tick Tick Y N N N!! Low risk of sepsis! Use standard protocols, review if deteriorates! Any moderate risk criteria? Altered mentation/ acute loss of functional ability! Rigors! Immunosuppressed! Trauma, surgery or procedure in last 6 weeks! Clinical signs of wound, device or skin infection! Amber NEWS score for RR or breathing hard! Amber NEWS score for HR or new arrhythmia! Amber NEWS score for Systolic BP! Not passed urine in last hours! Temperature < 36 O C! Red Flag Sepsis. Start Sepsis 6 pathway NOW (see overleaf) This is time critical, immediate action is required.! Sepsis! Six and Red Flag Sepsis are copyright to and intellectual property of the UK Sepsis Trust, registered charity no sepsistrust.org N Y Send bloods! To include FBC, U&Es, CRP, LFTs, clotting!! Contact ST3+ doctor to review! USE SBAR! Must review results within 1 hour!! Has clinician attended?! Time complete Is AKI present? (tick one) YES NO! Clinician to make antimicrobial! Prescribing decision within 3h!! Time complete Tick Initials Initials
40
41
42
43

44 1. Low level awareness alert Temperature recorded/ antibiotic prescribed 2. Medium level awareness alert Temperature recorded/ antibiotic prescribed AND a risk factor
45 1. Yellow flag sepsis alert Moderate risk but no Red Flag criteria


46 1. Yellow flag sepsis alert Moderate risk but no Red Flag criteria 2. Red Flag Sepsis alert Suspected infection and any RFS criterion

47 2. Red Flag Sepsis alert Suspected infection and any RFS criterion
48 @SepsisUK Fixing the system.
49 Systems approach Rivers 2001 RCT Sebat 2005 Before-After Nguyen 2007 Complete or Not Thiel 2009 Before-After Levy 2011 Before-After Goals CVP >8 MAP > 65 ScVO2 >70% HCT >30 MAP > 70 SaO2 > 92 UOP > 30ml/h SvO2 > 60 CI > 2.5 ABX in 4 h CVP > 8, MAP > 65, ScVO2 > 70%, HCT > 30 Check Lactate Steroids Appropriate ABX in 4 h, CVP > 8, MAP > 65, ScVO2 > 70% Early ABX, Blood Cultures, Appropriate ABX, CVP > 8, MAP > 65, SvO2 > 70% Specific Interventions Fluids, Blood, Pressors ABX, Fluids Pressors ABX, Fluids, Blood, Pressors ABX, Fluids, Pressors, Steroids, Xigris, Other Supportive Care ABX, Fluids, Pressors, Steroids, Xigris, Other Supportive Care System Interventions ED-based Sepsis Team Screening, Education, Shock Team, Protocols Education, Inservices, Protocols Education, Inservices, Order Set, Protocols Screening, Education, Order Sets Absolute Change in Mortality -16% -12% -19% -16% -7%
50
51
52
53

54

55 Sepsis is a condition whose time has come The same muscle and effort should be put into sepsis as for meningitis, MRSA and C Diff Now is the time not for words but for practical actions on the ground
56
57

58



59
60 Breast cancer

61 Breast cancer

62 sepsistrust.o
MAKING SENSE OF IT ALL AUGUST 17
 MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
MAKING SENSE OF IT ALL AUGUST 17 @SepsisUK Dr Ron Daniels B.E.M. CEO, UK Sepsis Trust CEO, Global Sepsis Alliance Special Adviser to WHO SCALE AND BURDEN @sepsisuk Dr Ron Daniels B.E.M. CEO, UK Sepsis
The Oxford AHSN Sepsis Pathway
 From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015
 Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
Sepsis! Dr Eric Van Den Bergh Consultant in Emergency Medicine 2015 Annual UK Mortality Sepsis Stroke Heart attack COPD Lung cancer COPD Heart attack Stroke Sepsis Lung cancer 0 10000 20000 30000 40000
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Sepsis. Reliability- can we achieve Dr Ron Daniels
 Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Sepsis. Reliability- can we achieve it? @SepsisUK Dr Ron Daniels Chief Executive, Global Sepsis Alliance Fellow: NHS Improvement Faculty Chief Executive: United Kingdom Sepsis Trust & Chair, UK SSC RRAILS
Management of Severe Sepsis:
 Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Management of Severe Sepsis: Update from the Surviving Sepsis Campaign Barbara Birriel, MSN, ACNP-BC, FCCM The Pennsylvania State University NONE Disclosures Review evidence-based international sepsis
Oxford AHSN Regional pathway
 Sepsis progress & challenges: What are we doing regionally? Andrew Brent Infectious Diseases & Medicine Consultant Sepsis Lead, OUH & Oxford Academic Health Sciences Network 2013 2014 2015 2016 2017 From:
Sepsis progress & challenges: What are we doing regionally? Andrew Brent Infectious Diseases & Medicine Consultant Sepsis Lead, OUH & Oxford Academic Health Sciences Network 2013 2014 2015 2016 2017 From:
Sepsis in primary care. Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells
 Sepsis in primary care Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells sepsisnurses@uhcw.nhs.uk Quiz!! OR Hands on your heads Hands on your hips Definition. The Third International Consensus Definition
Sepsis in primary care Sarah Bailey, Emma Evans, Nicola Shoebridge, Fiona Wells sepsisnurses@uhcw.nhs.uk Quiz!! OR Hands on your heads Hands on your hips Definition. The Third International Consensus Definition
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
The Oxford AHSN Sepsis Pathway
 From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
From confusion to consensus: The Oxford AHSN Sepsis Pathway Andrew Brent Sepsis Clinical Lead, Oxford AHSN & Oxford University Hospitals NHS Foundation Trust 2013 2014 2015 2016 2017 From: The Third International
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway
 Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Reducing the Door to Needle Time for Antibiotics in Suspected Neutropenic Sepsis using a Dedicated Clinical Pathway Dr Alex Williams, Oncology Specialty Doctor. Cheltenham General Hospital Oncology Centre
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the
 Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
Understand the scope of sepsis morbidity and mortality Identify risk factors that predispose a patient to development of sepsis Define and know the differences between sepsis, severe sepsis and septic
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Septic Shock. Rontgene M. Solante, MD, FPCP,FPSMID
 Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Septic Shock Rontgene M. Solante, MD, FPCP,FPSMID Learning Objectives Identify situations wherein high or low BP are hemodynamically significant Recognize complications arising from BP emergencies Manage
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Sepsis in primary care. what is good care?
 Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Sepsis Early Recognition and Management. Therese Hughes, PhD, MPA, RN
 Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis Early Recognition and Management Therese Hughes, PhD, MPA, RN 1 Sepsis a Deadly Progression Affects millions around the world each year, killing one in four Contributes to approximately 50% of all
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
NICE guideline Published: 13 July 2016 nice.org.uk/guidance/ng51
 Sepsis: recognition, diagnosis and early management NICE guideline Published: 13 July 2016 nice.org.uk/guidance/ng51 NICE 2016. All rights reserved. Last updated July 2016 Your responsibility The recommendations
Sepsis: recognition, diagnosis and early management NICE guideline Published: 13 July 2016 nice.org.uk/guidance/ng51 NICE 2016. All rights reserved. Last updated July 2016 Your responsibility The recommendations
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Sepsis. John Parker ICU Consultant & Sepsis Lead
 Sepsis John Parker ICU Consultant & Sepsis Lead 1 A bit about Leicester 2 Aims for today Definition of sepsis risk factors what causes sepsis Why sepsis is important risk to life long-term effects How
Sepsis John Parker ICU Consultant & Sepsis Lead 1 A bit about Leicester 2 Aims for today Definition of sepsis risk factors what causes sepsis Why sepsis is important risk to life long-term effects How
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Sepsis care and the new core measures
 Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis care and the new core measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
9/15/2017. Joyce Turner RN Director of Clinical Program Development
 Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Joyce Turner RN Director of Clinical Program Development A toxic response to an infection that spirals out of control attacking the body s own organs and tissues. The infection can be bacterial, viral
Sepsis Care and the New Core Measures. Daniel S. Hagg, MD January 15, 2016
 Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
Sepsis Care and the New Core Measures Daniel S. Hagg, MD January 15, 2016 Outline What is sepsis? A brief history of sepsis care How should we take care of septic patients now? Core measures What strategies
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Severe Sepsis & Septic Shock
 The College of Emergency Medicine Clinical Audits Severe Sepsis & Septic Shock EXCELLENCE IN EMERGENCY MEDICINE Contents Executive summary 3 Introduction 4 Audit history 4 Format of this report 4 Analysis
The College of Emergency Medicine Clinical Audits Severe Sepsis & Septic Shock EXCELLENCE IN EMERGENCY MEDICINE Contents Executive summary 3 Introduction 4 Audit history 4 Format of this report 4 Analysis
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Update in Sepsis. Conflicts of Interest: None. Bill Janssen, M.D.
 Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Update in Sepsis Bill Janssen, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Conflicts of Interest: None A 62 year-old female presents to the ED with fever,
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Charlson Comorbidities (please TICK all that apply)
") Medical Clerking On Call Consultant: Date: Time: Grade: Specialty: Age: Presenting Complaint: CLINICIAN: GRADE: DATE/TIME: Past Medical History: Charlson Comorbidities (please TICK all that apply) Cancer
Medical Clerking On Call Consultant: Date: Time: Grade: Specialty: Age: Presenting Complaint: CLINICIAN: GRADE: DATE/TIME: Past Medical History: Charlson Comorbidities (please TICK all that apply) Cancer
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Ralph Palumbo, MD, FCCP
 Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Ralph Palumbo, MD, FCCP Septic shock is the leading cause of mortality in patients admitted to the ICU In the United States alone there are over 750,000 cases of severe sepsis and septic shock annually
Sepsis and Septicemia: Clear up Coding and Documentation Confusion october 2009
 Sepsis and Septicemia: Clear Up Coding and Documentation Confusion W h i t e p a p e r Sepsis. Severe sepsis. SIRS. Septicemia. Unfortunately, this isn t a case of tomato, tomahto. Coders and physicians
Sepsis and Septicemia: Clear Up Coding and Documentation Confusion W h i t e p a p e r Sepsis. Severe sepsis. SIRS. Septicemia. Unfortunately, this isn t a case of tomato, tomahto. Coders and physicians
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
trust clinical guideline
 CG19 VERSION 1.2 1/12 Guideline ID CG19 Version 1.2 Title Approved by Sepsis including Meningococcal Septicaemia Clinical Effectiveness Group Date Issued 12/04/2016 Review Date 11/04/2019 Directorate Authorised
CG19 VERSION 1.2 1/12 Guideline ID CG19 Version 1.2 Title Approved by Sepsis including Meningococcal Septicaemia Clinical Effectiveness Group Date Issued 12/04/2016 Review Date 11/04/2019 Directorate Authorised
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Chapter 5: Sepsis Stephen Lo
 Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
Chapter 5: Sepsis Stephen Lo Introduction Sepsis and its consequence are the bread and butter of intensive care medicine and management of it is time critical. This chapter will discuss the definitions,
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines. Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases
 SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases Objectives Context Case Changing definitions Systems for
SIRS, NICE, SOFAs and CQUINs: Challenges of changing definitions and guidelines Dr Sian Coggle Consultant Acute Medicine and Infectious Diseases Objectives Context Case Changing definitions Systems for
4th edition THE SEPSIS MANUAL. Responsible management of sepsis, severe infection and antimicrobial stewardship.
 4th edition 2017-2018 THE SEPSIS MANUAL Responsible management of sepsis, severe infection and antimicrobial stewardship. Published by: United Kingdom Sepsis Trust Level 2, 36 Bennetts Hill Birmingham
4th edition 2017-2018 THE SEPSIS MANUAL Responsible management of sepsis, severe infection and antimicrobial stewardship. Published by: United Kingdom Sepsis Trust Level 2, 36 Bennetts Hill Birmingham
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Date Time PEWS Nurse Initials & NMBI Alert. Airway Behaviour and feeding. Accessory muscle use. Oxygen. Other
 Score Date / Time Minimum Observations 1 4 hourly 2 2-4 hourly Hospital Logo Paediatric Observation Chart 12+ Years Maximum Duration Nurse in Charge Escalation Guide Minimum Alert PEWS does not replace
Score Date / Time Minimum Observations 1 4 hourly 2 2-4 hourly Hospital Logo Paediatric Observation Chart 12+ Years Maximum Duration Nurse in Charge Escalation Guide Minimum Alert PEWS does not replace
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania
 AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
AnnMarie Papa, DNP,RN,CEN,NE-BC,FAEN, FAAN Clinical Director, Emergency, Medical & Observation Nursing Hospital of the University of Pennsylvania Who Am I? Except on few occasions, the patient appears
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Shock - from Diagnostic to Therapeutic Implications
 Shock - from Diagnostic to Therapeutic Implications Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. LEARNING OBJECTIVES Review the markers of tissue
Shock - from Diagnostic to Therapeutic Implications Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. LEARNING OBJECTIVES Review the markers of tissue
Case Scenario 3: Shock and Sepsis
 Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
Name: Molly Boyle 1. Define the term shock (Lewis textbook): Shock is a syndrome characterized by decreased perfusion and impaired metabolism. Shock can have a number of causes that result in damage to
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
4/4/2014. Of patients diagnosed with sepsis 50% will develop severe sepsis 25% will develop shock. SIRS Sepsis Severe Septic Sepsis Shock.
 A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
A summary of pathophysiology, therapeutics, and how the pharmacy TECHNICIAN can help improve OUTCOMES Anthony Nelson 2014 Pharm.D. Candidate Tricia Aggers, Pharm.D. Affiliate Faculty, ISU College of Pharmacy
Acute Kidney Injury (AKI) Undergraduate nurse education
 Undergraduate nurse education") Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
Acute Kidney Injury (AKI) Undergraduate nurse education Year Three Developed Summer 2017 Objectives Understand Acute Kidney Injury and its relevance to patient care. Brief revision of the Anatomy and physiology
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
SHOCK Susanna Hilda Hutajulu, MD, PhD
 SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
SHOCK Susanna Hilda Hutajulu, MD, PhD Div Hematology and Medical Oncology Department of Internal Medicine Universitas Gadjah Mada Yogyakarta Outline Definition Epidemiology Physiology Classes of Shock
Written Guidelines for Laboratory Testing in Intensive Care - Still Effective After 3 Years
 Written Guidelines for Laboratory Testing in Intensive Care - Still Effective After 3 Years S. M. MEHARI, J. H. HAVILL Intensive Care Unit, Waikato Hospital, Hamilton, NEW ZEALAND ABSTRACT Objective: The
Written Guidelines for Laboratory Testing in Intensive Care - Still Effective After 3 Years S. M. MEHARI, J. H. HAVILL Intensive Care Unit, Waikato Hospital, Hamilton, NEW ZEALAND ABSTRACT Objective: The
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
MANAGEMENT OF DENGUE INFECTION IN ADULTS (Revised 2 nd Edition) QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS") 1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
1 KEY MESSAGES Dengue is a dynamic disease and presented in three phases - febrile phase, critical phase and recovery phase. Clinical deterioration often occurs in the critical phase and is marked by plasma
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
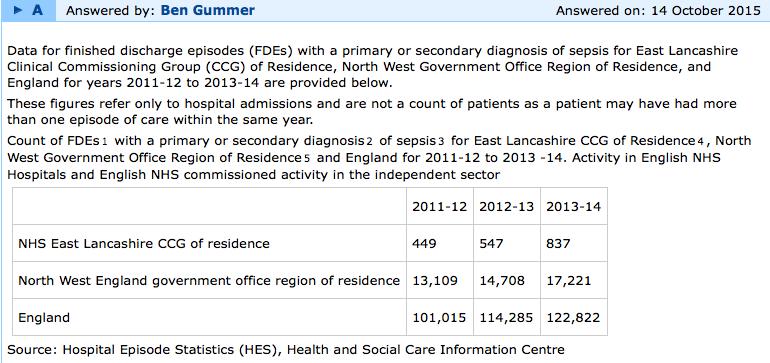
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Sepsis & Beyond Guidelines & Goal-Directed Therapy
 Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST
 ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
ACUTE KIDNEY INJURY FOCUS ON OBSTETRICS DONNA HIGGINS, CLINICAL NURSE EDUCATOR, NORTHERN LINCOLNSHIRE HOSPITALS NHS FOUNDATION TRUST AIMS & OBJECTIVES Review the functions of the kidney Identify renal
Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE
 Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE When are Standard Precautions used? The use of Standard Precautions during patient care is determined by the nature of the anticipated interaction
Communicable Diseases EMT REFRESHER NCCP 2018 JTEMPLE When are Standard Precautions used? The use of Standard Precautions during patient care is determined by the nature of the anticipated interaction
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment
 Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Sepsis new definitions of sepsis and septic shock and Novelities in sepsis treatment What is sepsis? Life-threatening organ dysfunction caused by a dysregulated host response to infection A 1991 consensus
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European