Welcome to Fall CE Event 2015
|
|
|
- Stephanie Sims
- 5 years ago
- Views:
Transcription

1 Welcome to Fall CE Event 2015
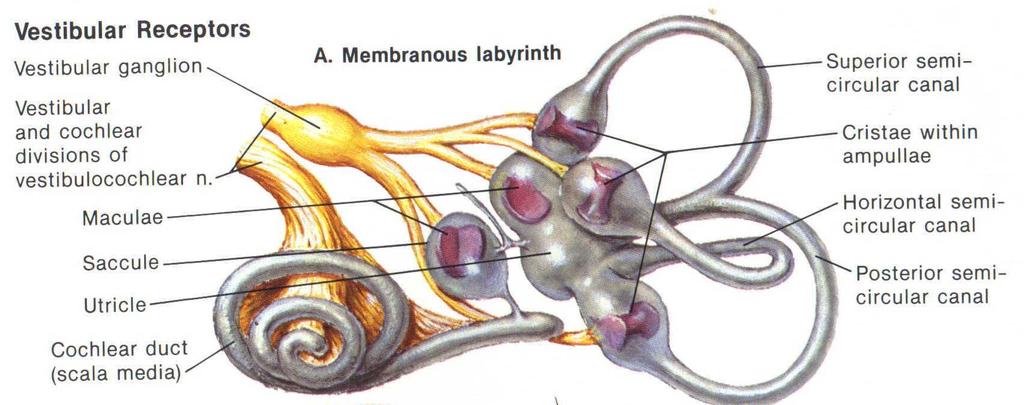
2 Basic Vestibular Function, Examination Procedures, Diagnosis, and Intervention Mark Amos, BA, DC, DACNB, FABVR
3 What s It About? Fall prevention 6 million people/ year Balance disorders and dizziness in top 3 complaints among elderly Falls leading cause of death and disability in elderly 85% of falls are vestibular
4 Who Falls? Over 55 years old Someone who has fallen and develops fear of falling History of head or neck trauma Should be evaluated
5 Anatomy and Physiology of Vertigo and Balance Humans have a very complex system to maintain balance and eye position The system relies on vestibular, visual, and proprioceptive input This input is translated into neurological signals
6 Things to Remember Intensity of movement determines intensity of signal Vestibular system is capable of self regulation of sensitivity
7 Localization Vertigo (feeling of motion) is cortical disruption in interpreting spatial orientation Nystagmus results from direction specific imbalance of VOR Postural imbalance results from inappropriate activation of vestibulospinal pathways
8 Localization Autonomic symptoms (nausea, vomiting, anxiety) results from activation of the vestibulo-autonomic pathways
9 Visual System What needs to be said? Get new glasses Get checked for cataracts Get checked for glaucoma
10 Proprioceptive System Moving joints it s what we do Decreased motion = decreased input Restored motion = increased input More later with cervicogenic vertigo
11 Vestibular System Works with the other two Weakness in one will lead to compensation by the others
12 Example A diabetic patient with peripheral neuropathy Cannot feel his legs or feet Decreased proprioception Walks by looking at his feet Turn off the lights and see what happens
13 Vestibular Rehabilitation Certain exercises and maneuvers can correct or mitigate vestibular disturbance That s what we will explore today
14 2 Vestibular Sensations Otolithic System Linear acceleration Static head position Canal System Rotational acceleration
15 Why Review Anatomy? Understanding anatomy leads to understanding of pathology Understanding pathology leads to understanding of treatment The why s and how s

16

17

18
19
20 How It Works The hair cells stick straight up The hairs are ion channels In the upright position they are closed Note the channels are connected
21 How It Works The hairs deflect with motion of the macula or cupula The connections open the ion channels Ions rush into the channels and depolarize the cell
22 How It Works The hair cells stick straight up The hairs are ion channels In the upright position they are closed Note the channels are connected
23 How It Works When the kinocilium bends the opposite direction it makes it harder to open the channel and depolarize the cell Inhibition
24 Otolithic System Utricle- horizontal acceleration Saccule- vertical acceleration Utilize otoliths
25 Otolith System Macula Calcium Carbonate Otoliths Vestibular Nerve
26 Otolith System Head Motion! (+) Vestibular Nerve
27 Otolith System!Head Motion (-) Vestibular Nerve

28 Bear 1996

29 Purves 2001.
30 Canals 3 canals- angular acceleration 90º orientation Ampulla Cupula

31
32 Semicircular Canal Ampulla Cupula Hair Crista Amullaris Vestibular Nerve
33 Semicircular Canal Ampulla Cupula Endolymph Flow! (+) Crista Amullaris Vestibular Nerve
34 Semicircular Canal Ampulla Cupula (-) Endolymph! Flow Crista Amullaris Vestibular Nerve

35

36
37 Top View Anterior Canal Horizontal Canal Posterior Canal
38 Anterior and Posterior Canals Anterior canal activates when the head moves FORWARD and lateral Posterior canal activates when the head moves BACK and lateral
39 Lesions
40 Cervicogenic Vertigo Whiplash or cervical trauma Affects COR cervico-ocular reflexes Affects CSR cervicospinal reflexes Involves muscle spasm May be confused with BPPV Subluxation indicators apply Upper cervical Horizontal canal orientation Cervical mechanoreceptors develop before vestibular
41 3 Basic Types Bilateral peripheral loss- patient has feeling of up and down head movement while walking, gait instability, increased difficulty with darkness and uneven ground Acute/subacute unilateral loss- causes imbalance in tone, vertigo, body positioning, nystagmus, autonomic symptoms
42 3 Basic Types Paroxysmal stimulation- short attacks of vertigo
43 Two Locations Peripheral vestibular lesion Central vestibular lesion
44 Peripheral vs. Central Peripheral Intermittent Motion provoked Cause nausea Consistent nystagmus Central Constant (usually) Not motion dependent Only fluctuates in intensity Variable nystagmus
45 Peripheral Lesions BPPV Neuritis Labyrinthitis Meniere disease Fistula-dehiscience Nerve compression Bilateral vestibular loss
46 BPPV Benign paroxysmal positional vertigo Results from head/neck trauma Medication use Dislodges otolithis from the utricle and saccule into the semicircular canals
47 BPPV 2 models Canalolithiasis Cupulolithiasis Otolithic debris causes extreme vertigo, nausea with head position
48 Normal Canal Function Head Motion Endolymph!
49 Canalithisiasis Canaliths
50 Canalolithiasis Responds well to repositioning maneuvers Purpose is to move the crystals out of the canal
51 Normal Canal Function Head Motion Endolymph!
52 Cupulolithiasis Cupulolithiasis
53 Cupulolithiasis Does not respond to canalith repositioning Responds well to a liberatory maneuver to break it free
54 BPPV 3 canals 3 forms 90%, 9%, 1% Posterior, horizontal, anterior
55 Vestibular Neuritis Acute unilateral viral infection Usually superior portion of vestibular nerve (anterior and lateral canals) Associated with GI or upper respiratory infection Lasts hours
56 Labyrinthitis Infection of the membranous labyrinth Often with upper respiratory infection Dizziness with hearing loss Gradual return to function (months)
57 Meniere Disease Endolymphatic hydrops Overproduction of endolymph Feeling of fullness in the ear Ringing + vertigo Newer information shows correlation with autoimmune disorders and migraine
58 Meniere Disease Does not respond well to vestibular rehabilitation Intermittent Episodes may last minutes to hours Standard treatment is salt restriction and /or surgery
59 Meniere Disease Patient will experience fullness of the ear and ringing The there is a sudden change as the membranes rupture Tumarkin otolithic crisis

60 Meniere Disease
61 Fistula/Dehiscience Head or neck trauma Tears an opening in the membranous labyrinth results in new window and decreased pressure Changing pressure or loud noise causes vertigo

62 Fistula/Dehiscience

63 Nerve Compression Will often involve hearing loss Often affects facial nerve and trigeminal nerve All three emerge at the cerebellopontine angle

64 Acoustic Neuroma
65 Bilateral Vestibular Loss Often medicinal/toxic (mycin drugs) May be autoimmune May be infectious May be longstanding Meniere May or may not involve hearing Often has oscillopsia and gait ataxia
66 Central Lesions Stroke/degeneration/scarring Constant Ischemia Hyperventilation Low cardiac output Possible low blood sugar
67 Medulla Lesion Habituation is the key System will decrease sensitivity Chiropractic is a piece of this puzzle Increase input Normalize function Cawthorn Cooksey exercises
68 Hyperventilation The exception to the constant rule May be intermittent Often with fear of falling leading to anxiety attack Anxiety attack leads to hyperventilation which leads to fall
69 How? Capillaries have chemoreceptors for carbon dioxide More carbon dioxide in the blood means more capillary dilation Less carbon dioxide in blood means less capillary dilation and ischemia
70 How? Decreased CO2 means heart and brainstem ischemia Brainstem ischemia leads to dizziness and anxiety and panic and hyperventilation
71 How? Decreased CO2 means heart and brainstem ischemia Heart ischemia leads to angina and therefore panic attack over heart attack and hyperventilation

72 Hyperventilation
73 History Considerations
74 BPPV Vestibular Neuritis Labyrinthitis Meniere's Disease Fistula Dehiscience Nerve Compression Bilateral Loss Vertigo Yes Yes Yes Yes Yes Yes No Nystagmus Yes Yes Yes Yes Yes Yes No Duration 30 sec- 2 min hours Months 30 min- 24 hours Seconds Seconds to minutes Periodic Nausea Yes Yes Yes Yes No Yes No Specificity Onset with position Acute onset w/ viral inf Acute onset w/ viral inf Fullness and tinnitis Tullio or pressure Frequent tinnitis Severe gait ataxia Hearing Loss No No Yes Yes No Yes Possible Precipitating Action Postural change None None None Valsalva Increased ICP Facial weakness Drugs
75 Evaluation
76 CTSIB Clinical Test of Sensory Organization in Balance Foam Dome Test 6 conditions Help reveal which has failed: vision, proprioception, vestibular

77 Sensory Organization Test Condition 1 Stable platform Eyes open Utilizes all 3 sensory modalities

78 Sensory Organization Test Condition 2 Stable platform Eyes closed Relies on somatosensory and vestibular

79 Sensory Organization Test Condition 3 Stable platform Eyes open Environment movesprovides false sense of motion Patient MUST suppress vision and rely on somatosensory input and vestibular input

80 Sensory Organization Test Condition 4 Unstable platform Eyes open Patient must rely on vestibular and visual input

81 Sensory Organization Test Condition 5 Unstable platform Eyes closed Patient must rely solely on vestibular input
82 Sensory Organization Test Condition 6 Unstable platform Moving environment Patient must rely entirely on vestibular input
83 Positional Head in extension + rotation Vertebral artery Cervicogenic Posterior canal
84 Cervicogenic Test Patient seated in a spinning stool Stabilize patient s head Rotate patient with head horizontal Dizziness = Cervical problem Do what we do best
85 Vertebrobasilar Artery Test Have patient seated leaning forward Neck is in extension Have patient rotate head to one side then hold 30 seconds Repeat to other side and hold Hautant test
86 Eye Movement Testing Observe nystagmus while stationary Pursuit Saccade Vestibulo-ocular reflex VOR


87 Pursuit!!!Cardinal fields of gaze!! H pattern + convergence!!patient should follow smoothly to all positions


88 !!Hold fingers 14 apart!!1-2 in front of patient!!patient goes to one side on command!!back to neutral!!go to side on command Saccade!


89 Vestibulo-ocular Reflex!!!Ask the patient to fixate on doctor!!doctor slowly turns head side to side!!patient should maintain fixation on doctor!!head Thrust Test!!Test VOR a little faster
90 Dizziness Simulation Battery Designed to reproduce dizziness The portion of the test reproducing dizziness is the cause and then may be addressed Helps aid the patient in understanding the cause
91 Dizziness Simulation Battery Seating vs. standing blood pressure Carotid sinus reflex Valsalva test or Tullio Hyperventilation provocative test Hallpike Dix maneuver Lateral canal maneuver Anterior canal test

92 Hallpike Dix Maneuver Patient s head is turned 45º This sets the posterior canal parallel to the table

93 Hallpike Dix Maneuver Patient is quickly lowered back to a head off the table position This view shows testing the right posterior canal Nystagmus indicates BPPV




94 Hallpike Dix Movie!
95 Top View Anterior Canal Horizontal Canal Posterior Canal
96 Hallpike Dix Position Anterior Canal Posterior Canal
97 Hallpike Dix Maneuver The test focuses on the posterior canal by putting it in a gravity dependent position Patient complains of dizziness or develops nystagmus to make the test (+)


98 Hallpike Dix (+)!!!Patient is leaned back in the right posterior canal position!!eyes will beat upward and right
99 Nystagmus Will point toward the affected ear Hallpike Dix will give the plane of the problem Observation of nystagmus will reveal whether it is the posterior canal or the OPPOSITE anterior canal
100 Horizontal Canal Testing Lay patient supine Flex head 30º Turn head side to side Nystagmus toward the affected ear will reveal which horizontal canal is involved
101 Horizontal Canal Movie!!!The video shows a purely horizontal nystagmus!!the position places the horizontal canal in a purely vertical orientation
102 Treatment
103 Based Upon Cause Cervicogenic = adjustment Orthostatic = send patient back to MD Fistula = rest in bed for several days until it heals, possible surgery VBAI = light force adjustment, doppler unltrsound, MRA Infection- re-evaluate and VRT as needed
104 Hyperventilation Breathing exercises Lots available on line 10 breaths/ minute in 2, hold 2, out 2 Andrew Weil 4, 7, 8 Work to six breaths per minute Start 5 minutes work up to 1/2 hour
105 BPPV Cupulolithiasis = liberatory maneuvers (Semont) Canalolithiasis = repositioning maneuvers Epley, Lempert????? = Brandt Daroff
106 Semont Maneuver To liberate the stuck on cupulolithiasis Preloads endolymph Then slams the head opposite Washes the crystals off the cupula

107 Semont s Maneuver


108 Posterior Canal Semont!!!Starts like Hallpike!!Turning head lines up the posterior canal with direction of motion!!fall and wait 2-3 minutes!!flip and wait 5 minutes!!important to slam patient into table repetitively



109 Horizontal Semont!!!Clears the horizontal canal by liberating crystals off the cupula
110 Epley s Maneuver Specific to posterior canal Also will clear opposite anterior canal Starts with Hallpike-Dix position Moves free floating otoliths through the canal to drop out into the vestibule Hold each position 30 seconds or until dizziness/nystagmus stops

111 Epley s Maneuver

112 Epley Video!




113 Vertigone Movie!

114 DizzyFix
115 Bar-B-Que Roll Lempert maneuver Clears horizontal canal Put the patient on a spit
116 Lempert s Maneuver
117 Bar-B-Que Roll Movie!!!Starts with affected ear down!!then is a 450º roll to the opposite side


118 Anterior Canal!!!This is the rarest form!!patients often have confusing contradictory symptoms
119 Brandt Daroff Maneuver This is the WTF maneuver If all else fails maneuver Promotes habituation Fall and stay there until the dizziness stops Then go the other way

120 Brandt Daroff Maneuver



121 Brandt Daroff Movie!!!This is used also in conjunction with other maneuvers to promote habituation.
122 Central Lesion Cawthorn Cooksey Exercise Starts with eyes Then head moves Then seated Then standing
123 Cawthorn Cooksey Exercise In Bed Supine Eye movements done slow then quick Gazing up and down Gazing side to side Accommodation 3 feet to 1 foot Head movements done slow, then quick, eyes open, then closed Flexion extension Rotation
124 Cawthorn Cooksey Exercise Sitting Bed exercises 1-5 Shoulder shrugging and circles Bend forward to pick up objects from the ground
125 Cawthorn Cooksey Exercise Standing Bed exercises 1-5 Sitting exercise 6 Sitting to standing eyes open and closed Doing same with a turn Throwing ball hand to hand above eye level Throwing a ball hand to hand below the knees
126 Cawthorn Cooksey Exercise While moving Circle round a person while playing catch Walking with eyes open and closed Walking up and down a slope eyes open and closed Walk up and down steps eyes open then closed Performing stooping, stretching and aiming motions
127 Vestibular Rehabilitative Therapy (VRT) Main types Gaze stabilization Adaptation exercises Substitution exercises
128 Gaze Stabilization Just as it says Do pursuit exercises Track moving target side to side, up and down Do Saccade exercises Look from side to side, up and down Do VOR exercises Look at stationary target move head side to side and up and down


129 Gaze Stabilization!!!Combine the above!!x2 viewing- move target and head in opposite directions!!okn plus
130 Adaptation Exercises For unilateral vestibular loss Main goal is to restore VOR Use Gaze stabilization exercises Use head moving exercises Walking with head turns Walking on foam
131 Substitution Exercises For bilateral vestibular lesion No restoration of of VOR (no V) These train patients to use vision and mechanoreception in place of VOR Exercises include 1 leg stand, sit to stand, balance beam, foam walk Patients also need balance hygiene
132 Documentation WHO is gearing more toward quality of life Describes how a balance disorder may turn into a handicap This underscores the importance of rehabilitation
133 Documentation The patient perception of the problem is the handicap or disability Even the patient who has been rehabilitated with no symptoms may be disabled by fear of falling or recurrence Documentation = patient education? Documentation = psychological recovery?
134 Documentation Activities-Specific Balance Confidence Scale Dizziness handicap inventory Vertigo score card
135 Activities-Specific Balance Confidence Scale Powers and Myers, Patients are asked to fill in one of the following percentages for each individual question. Even if the patient does not perform the activity now, the patient should consider the activity and assign a confidence rating. A rating of 100% indicates certainty that unsteadiness or loss of balance will not result from that activity. If an aid is usually used to perform the activity, rate the activity as though performing with the aid. 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% No Confidence Complete Confidence 1. Walking around the house. 2. Walking up and down stairs inside the home. 3. Picking up a slipper or something from the floor 4. Reaching at eye level. 5. Reaching overhead while standing on toes. 6. Reaching overhead while standing on a chair. 7. Sweeping the floor. 8. Walking outside to a nearby car. 9. Getting in and out of a car or other transportation. 10. Walking across a parking lot. 11. Walking up and down a ramp. 12. Walking in a crowded area where people walk rapidly past you. 13. Being bumped while walking in a crowd. 14. Using an escalator while holding the railing. 15. Using an escalator while holding packages without holding the railing. 16. Walking on slippery floors or icy sidewalks. Total Average Score (< 68% = low mobility, increased fear)
136 Dizziness Handicap Inventory Patient Name: Date: The purpose of this scale is to identify difficulties that you may be experiencing because of your dizziness or unsteadiness. Please answer "Yes," "No," or "Sometimes" to each question by writing the corresponding letter in the blanks to the right of the questions. Answer each question as it pertains to your dizziness or unsteadiness only. Y = Yes S = Sometimes N = No Physical 1. Does looking up increase your problem? Emotional 2. Because of your problem do you feel frustrated? Functional 3. Because of your problem, do you restrict your travel for business or recreation? Physical 4. Does walking down the aisle of a supermarket increase your problem? Functional 5. Because of your problem, do you have difficulty getting into, or out of bed? 6. Does your problem significantly restrict your participation in social activities such Functional as going out to dinner, going to movies, dancing, or to parties? Functional 7. Because of your problem, do you have trouble reading? 8. Does performing ambitious activities like sports, dancing, household chores such Physical as sweeping or putting dishes away increase your problem? 9. Because of your problem are you afraid to leave your home, without having Emotional someone to accompany you? Emotional 10. Because of your problem, have you been embarrassed in front of others? Physical 11. Do quick movements of your head increase your problem? Functional 12. Because of your problem, do you avoid heights? Physical 13. Does turning over in bed increase your problem? 14. Because of your problem, is it difficult for you to do strenuous housework or yard Functional work? Emotional 15. Because of your problem, are you afraid people may think you are intoxicated? Functional 16. Because of your problem, is it difficult for you to go for a walk by yourself? Physical 17. Does walking down a sidewalk increase your problem? Emotional 18. Because of your problem, is it difficult for you to concentrate? 19. Because of your problem, is it difficult for you to walk around your house in the Functional dark? Emotional 20. Because of your problem, do you feel handicapped? Emotional 21. Because of your problem, are you afraid to stay home alone? Emotional 22. Has your problem placed strain on you relationships with family and friends? Emotional 23. Because of your problem, are you depressed? Functional 24. Does your problem interfere with your job or household responsibilities? Physical 25. Does bending over increase your problem? FOR OFFICE USE ONLY: Initial Visit Follow-up Visit Functional (36) Emotional (36) Physical (28) Scoring: Yes = 4; Sometimes = 2; No = 0 Jacobson and Newman 1990.
137 Vertigo Score Card Developed by Savundra 1993 Position Changing Stimuli Do You Get Dizzy.. No Yes 1. Bending down to pick up something from the floor? 2. Looking up? 3. On first laying in bed? 4. Upon turning left or right? 5. When walking in the dark? Subtotal No = 1 Yes = 0 Visual Stimuli Do You Get Dizzy.. No Yes 1. Walking between shelves in a store? 2. Sitting in a moving vehicle? 3. Ironing striped material? 4. Walking up or down stairs? 5. Walking up an escalator? Subtotal Total
Benign Paroxysmal Positional Vertigo
 Benign Paroxysmal Positional Vertigo Information for patients and families Read this booklet to learn about: What Benign Paroxysmal Positional Vertigo (BPPV) is Symptoms How your doctor will diagnose it
Benign Paroxysmal Positional Vertigo Information for patients and families Read this booklet to learn about: What Benign Paroxysmal Positional Vertigo (BPPV) is Symptoms How your doctor will diagnose it
Sasan Dabiri, MD, Assistant Professor
 Sasan Dabiri, MD, Assistant Professor Department of Otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medical Sciences October 2015 Outlines Anatomy of Vestibular System
Sasan Dabiri, MD, Assistant Professor Department of Otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medical Sciences October 2015 Outlines Anatomy of Vestibular System
Cross Country Education Leading the Way in Continuing Education and Professional Development.
 To comply with professional boards/associations standards: I declare that I or my family do not have any financial relationship in any amount, occurring in the last 12 months with a commercial interest
To comply with professional boards/associations standards: I declare that I or my family do not have any financial relationship in any amount, occurring in the last 12 months with a commercial interest
Control of eye movement
 Control of eye movement Third Nerve Palsy Eye down and out Trochlear Nerve Palsy Note: Right eye Instead of intorsion and depression action of superior oblique See extorsion and elevation Observe how
Control of eye movement Third Nerve Palsy Eye down and out Trochlear Nerve Palsy Note: Right eye Instead of intorsion and depression action of superior oblique See extorsion and elevation Observe how
OBJECTIVES BALANCE EVALUATION COMMON CAUSES OF BALANCE DEFICITS POST TBI BRAIN INJURY BALANCE RELATIONSHIP
 OBJECTIVES Understand variables that contribute to balance deficits Understand the relationship between a brain injury and balance Become familiar with the components of a vestibular/balance assessment
OBJECTIVES Understand variables that contribute to balance deficits Understand the relationship between a brain injury and balance Become familiar with the components of a vestibular/balance assessment
Vestibular physiology
 Vestibular physiology 2017 Utricle A flat epithelium: horizontal in the upright head Utricle Hair cells: no axons hair cells Utricle Hair cells synapse onto 8th nerve afferents. 8th nerve afferents Hair
Vestibular physiology 2017 Utricle A flat epithelium: horizontal in the upright head Utricle Hair cells: no axons hair cells Utricle Hair cells synapse onto 8th nerve afferents. 8th nerve afferents Hair
Vestibular Differential Diagnosis
 Vestibular Differential Diagnosis P R E S E N T E D B Y : S H A R I K I C K E R, P T, M P T C E R T I F I C A T E I N V E S T I B U L A R R E H A B I L I T A T I O N 2 0 1 7 L A C E Y H A L E, P T, D P
Vestibular Differential Diagnosis P R E S E N T E D B Y : S H A R I K I C K E R, P T, M P T C E R T I F I C A T E I N V E S T I B U L A R R E H A B I L I T A T I O N 2 0 1 7 L A C E Y H A L E, P T, D P
VESTIBULAR SYSTEM. Deficits cause: Vertigo. Falling Tilting Nystagmus Nausea, vomiting
 VESTIBULAR SYSTEM Objectives: Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? Describe the vestibular apparatus, the 2
VESTIBULAR SYSTEM Objectives: Understand the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? Describe the vestibular apparatus, the 2
BPPV and Pitfalls in its Management. Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist
 BPPV and Pitfalls in its Management Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist Objectives 1-The best methods of diagnosis of BPV 2-How to differentiate between
BPPV and Pitfalls in its Management Reza Golrokhian Sani MD, Otolaryngologist- Head & Neck Surgeon Otologist & Neurotologist Objectives 1-The best methods of diagnosis of BPV 2-How to differentiate between
CITY & HACKNEY PATHFINDER CLINICAL COMMISSIONING GROUP. Vertigo. (1) Vertigo. (4) Provisional Diagnosis. (5) Investigations. lasting days or weeks
 Vertigo. (4) Provisional Diagnosis. (5) Investigations. lasting days or weeks") Authors: Dr Lucy O'Rouke and Mr N Eynon-Lewis Review date: January 2017 Vertigo (1) Vertigo (2) History (3) Examination (4) Provisional Diagnosis (5) Investigations (6) Medical Cause (7) Psychiatric Cause
Authors: Dr Lucy O'Rouke and Mr N Eynon-Lewis Review date: January 2017 Vertigo (1) Vertigo (2) History (3) Examination (4) Provisional Diagnosis (5) Investigations (6) Medical Cause (7) Psychiatric Cause
Name: Date of Birth: Age:
 VESTIBULAR HISTORY Name: Date of Birth: Age: Today's Date: Phone number Referring MD Next MD Appt: Briefly describe your problem: Describe: Date of onset: Time of day: What were you doing when it began?
VESTIBULAR HISTORY Name: Date of Birth: Age: Today's Date: Phone number Referring MD Next MD Appt: Briefly describe your problem: Describe: Date of onset: Time of day: What were you doing when it began?
Vertigo: A practical approach to diagnosis and treatment. John Waterston
 Vertigo: A practical approach to diagnosis and treatment John Waterston Background. Vertigo is a symptom that has diverse causes. The diagnosis may remain elusive even after exhaustive clinical enquiry
Vertigo: A practical approach to diagnosis and treatment John Waterston Background. Vertigo is a symptom that has diverse causes. The diagnosis may remain elusive even after exhaustive clinical enquiry
Vestibular System. Dian Yu, class of 2016
 Vestibular System Dian Yu, class of 2016 Objectives 1. Describe the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? 2. Describe the vestibular
Vestibular System Dian Yu, class of 2016 Objectives 1. Describe the functions of the vestibular system: What is it? How do you stimulate it? What are the consequences of stimulation? 2. Describe the vestibular
BALANCE EXERCISES FACTSHEET
 London Road Reading RG1 5AN BALANCE EXERCISES FACTSHEET If you need balance exercises (vestibular rehabilitation) your audiologist will devise a tailored package of exercises to meet your specific needs.
London Road Reading RG1 5AN BALANCE EXERCISES FACTSHEET If you need balance exercises (vestibular rehabilitation) your audiologist will devise a tailored package of exercises to meet your specific needs.
Quick Guides Vestibular Diagnosis and Treatment:
 VNG - Balance Testing Quick Guides Vestibular Diagnosis and Treatment: A Physical Therapy Approach Dix-Hallpike Test for Diagnosis of BPPV Epley Canalith Repositioning Procedure (CRP) Semont Maneuver for
VNG - Balance Testing Quick Guides Vestibular Diagnosis and Treatment: A Physical Therapy Approach Dix-Hallpike Test for Diagnosis of BPPV Epley Canalith Repositioning Procedure (CRP) Semont Maneuver for
Predictors of Protracted Recovery
 CONCUSSION MANAGEMENT SPECIALIST ON LINE CURRICULUM Protracted Recovery and Clinical Rehabilitation All rights reserved. Sports Medicine Concepts Concussion Management Specialist Program 1 Predictors of
CONCUSSION MANAGEMENT SPECIALIST ON LINE CURRICULUM Protracted Recovery and Clinical Rehabilitation All rights reserved. Sports Medicine Concepts Concussion Management Specialist Program 1 Predictors of
Because dizziness is an imprecise term, a major role of the clinician is to sort patients out into categories
 Dizziness and Imbalance Timothy C. Hain, MD Clinical Professor of Neurology, Otolaryngology, Physical Therapy Chicago Dizziness and Hearing 645 N. Michigan, Suite 410 312-274-0197 Lecture Goals 1. What
Dizziness and Imbalance Timothy C. Hain, MD Clinical Professor of Neurology, Otolaryngology, Physical Therapy Chicago Dizziness and Hearing 645 N. Michigan, Suite 410 312-274-0197 Lecture Goals 1. What
Vestibular Evaluation
 Chris Carpino, MPT Vestibular Evaluation 1. History Most important aspect of evaluation (see DHI) 2. Vital Signs Check blood pressure in supine and sitting 3. Eye Exam 4. Positional Testing 5. Balance
Chris Carpino, MPT Vestibular Evaluation 1. History Most important aspect of evaluation (see DHI) 2. Vital Signs Check blood pressure in supine and sitting 3. Eye Exam 4. Positional Testing 5. Balance
Acute Vestibular Syndrome (AVS) 12/5/2017
 12/5/2017") Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Sharon Hartman Polensek, MD, PhD Dept of Neurology, Emory University Atlanta VA Medical Center DIAGNOSTIC GROUPS FOR PATIENTS PRESENTING WITH DIZZINESS TO EMERGENCY DEPARTMENTS Infectious 2.9% Genitourinary
Dizziness: Natural Treatment for Vertigo and BPPV
 Wellness and WBV Studio Home» Bodywork» Massage» CranioSacral Therapy» Dizziness: Natural Treatment for Vertigo and BPPV CRANIOSACRAL THERAPY HOLISTIC HEALING Dizziness: Natural Treatment for Vertigo and
Wellness and WBV Studio Home» Bodywork» Massage» CranioSacral Therapy» Dizziness: Natural Treatment for Vertigo and BPPV CRANIOSACRAL THERAPY HOLISTIC HEALING Dizziness: Natural Treatment for Vertigo and
Building Better Balance
 Building Better Balance The Effects of MS on Balance Individuals with MS experience a decline in their balance due to various MS related impairments. Some of these impairments can be improved with exercise
Building Better Balance The Effects of MS on Balance Individuals with MS experience a decline in their balance due to various MS related impairments. Some of these impairments can be improved with exercise
Acoustic neuroma s/p removal BPPV (Crystals)- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness
- 50% of people over 65 y/ o with dizziness will have this as main reason for dizziness") Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Dizziness and the Heart Mended Hearts Inservice Karen Hansen, PT, DPT, Cert Vestibular Rehab, CEAS Tennessee Therapy & Balance Center, LLC July 21, 2016 Balance We maintain balance with input from our
Balance (Vestibular) Rehabilitation
 Rehabilitation") Balance (Vestibular) Rehabilitation When there is a problem in the balance (or vestibular) system either in the ears or in the brain, the symptoms can range from mild to very severe. The symptoms can range
Balance (Vestibular) Rehabilitation When there is a problem in the balance (or vestibular) system either in the ears or in the brain, the symptoms can range from mild to very severe. The symptoms can range
Vestibular Physiology Richard M. Costanzo, Ph.D.
 Vestibular Physiology Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be able to: 1. Describe the structure and function of the vestibular organs.
Vestibular Physiology Richard M. Costanzo, Ph.D. OBJECTIVES After studying the material of this lecture, the student should be able to: 1. Describe the structure and function of the vestibular organs.
What is the effect on the hair cell if the stereocilia are bent away from the kinocilium?
 CASE 44 A 53-year-old man presents to his primary care physician with complaints of feeling like the room is spinning, dizziness, decreased hearing, ringing in the ears, and fullness in both ears. He states
CASE 44 A 53-year-old man presents to his primary care physician with complaints of feeling like the room is spinning, dizziness, decreased hearing, ringing in the ears, and fullness in both ears. He states
VESTIBULAR SYSTEM ANATOMY AND PHYSIOLOGY. Professor.Dr. M.K.Rajasekar MS., DLO.,
 VESTIBULAR SYSTEM ANATOMY AND PHYSIOLOGY Professor.Dr. M.K.Rajasekar MS., DLO., Life is hard for those who don t have a VOR During a walk I found too much motion in my visual picture of the surroundings
VESTIBULAR SYSTEM ANATOMY AND PHYSIOLOGY Professor.Dr. M.K.Rajasekar MS., DLO., Life is hard for those who don t have a VOR During a walk I found too much motion in my visual picture of the surroundings
Saccades. Assess volitional horizontal saccades with special attention to. Dysfunction indicative of central involvement (pons or cerebellum)
") Saccades Assess volitional horizontal saccades with special attention to Amplitude? Duration? Synchrony? Dysfunction indicative of central involvement (pons or cerebellum) Dynamic Visual Acuity Compare
Saccades Assess volitional horizontal saccades with special attention to Amplitude? Duration? Synchrony? Dysfunction indicative of central involvement (pons or cerebellum) Dynamic Visual Acuity Compare
Differential Diagnosis: Vestibular Pathology. Causes of Dizziness. Benign Paroxysmal Positional Vertigo
 Differential Diagnosis: Vestibular Learning objective: The participant will identify the pathologies associated with complaints of imbalance and dizziness Anne K Galgon PT, PhD, NCS Vestibular and Related
Differential Diagnosis: Vestibular Learning objective: The participant will identify the pathologies associated with complaints of imbalance and dizziness Anne K Galgon PT, PhD, NCS Vestibular and Related
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: vestibular_function_testing 5/2017 N/A 10/2017 5/2017 Description of Procedure or Service Dizziness, vertigo,
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: vestibular_function_testing 5/2017 N/A 10/2017 5/2017 Description of Procedure or Service Dizziness, vertigo,
Computerized Dynamic Posturography (CDP) & Videonystagmography (VNG) Packet
 & Videonystagmography (VNG) Packet") Computerized Dynamic Posturography (CDP) & Videonystagmography (VNG) Packet Name: Audiologist: Nicole Smith, Au.D Trista Williams, Au.D DOB: Location: DOS: Balance Clinic Information At the DeFatta ENT
Computerized Dynamic Posturography (CDP) & Videonystagmography (VNG) Packet Name: Audiologist: Nicole Smith, Au.D Trista Williams, Au.D DOB: Location: DOS: Balance Clinic Information At the DeFatta ENT
Vertigo. Definition. Causes. (Dizziness) Benign Paroxysmal Positional Vertigo (BPPV) Labyrinthitis. by Karen Schroeder, MS, RD
 Benign Paroxysmal Positional Vertigo (BPPV) Labyrinthitis. by Karen Schroeder, MS, RD") Vertigo (Dizziness) by Karen Schroeder, MS, RD En Español (Spanish Version) Definition Vertigo is a feeling of spinning or whirling when you are not moving. It can also be an exaggerated feeling of motion
Vertigo (Dizziness) by Karen Schroeder, MS, RD En Español (Spanish Version) Definition Vertigo is a feeling of spinning or whirling when you are not moving. It can also be an exaggerated feeling of motion
Dear Patient: Sincerely. Julie A. Honaker, Ph.D. Director, Dizziness and Balance Disorder Laboratory
 , DEPARTMENT OF SPECIAL EDUCATION AND COMMUNICATION DISORDERS Dizziness and Balance Disorder Lab (402) 472-8790 dizzinesslab@unlnotes.unl.edu Dear Patient: Enclosed is a questionnaire used to assist in
, DEPARTMENT OF SPECIAL EDUCATION AND COMMUNICATION DISORDERS Dizziness and Balance Disorder Lab (402) 472-8790 dizzinesslab@unlnotes.unl.edu Dear Patient: Enclosed is a questionnaire used to assist in
Paediatric Balance Assessment
 BAA regional meeting 11 th March 2016 Paediatric Balance Assessment Samantha Lear, Lead Clinical Scientist, Hearing Services, SCH overview The balance system Vestibular disorders referrals Vestibular assessment
BAA regional meeting 11 th March 2016 Paediatric Balance Assessment Samantha Lear, Lead Clinical Scientist, Hearing Services, SCH overview The balance system Vestibular disorders referrals Vestibular assessment
BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV)
") 5018 NE 15 TH AVE PORTLAND, OR 97211 FAX: (503) 229-8064 (800) 837-8428 INFO@VESTIBULAR.ORG VESTIBULAR.ORG BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV) By Sheelah Woodhouse, BScPT WHAT IS BPPV? Benign Paroxysmal
5018 NE 15 TH AVE PORTLAND, OR 97211 FAX: (503) 229-8064 (800) 837-8428 INFO@VESTIBULAR.ORG VESTIBULAR.ORG BENIGN PAROXYSMAL POSITIONAL VERTIGO (BPPV) By Sheelah Woodhouse, BScPT WHAT IS BPPV? Benign Paroxysmal
The Physiology of the Senses Lecture 10 - Balance
 The Physiology of the Senses Lecture 10 - Balance www.tutis.ca/senses/ Contents Objectives... 1 The sense of balance originates from the labyrinth... 2 The auditory and vestibular systems have a common
The Physiology of the Senses Lecture 10 - Balance www.tutis.ca/senses/ Contents Objectives... 1 The sense of balance originates from the labyrinth... 2 The auditory and vestibular systems have a common
Inner Ear Disorders. Information for patients and families
 Inner Ear Disorders Information for patients and families Read this booklet to learn about: What are inner ear disorders Symptoms Tests you may need Treatment options Please visit the UHN Patient Education
Inner Ear Disorders Information for patients and families Read this booklet to learn about: What are inner ear disorders Symptoms Tests you may need Treatment options Please visit the UHN Patient Education
Otologic (Ear) Dizziness Fistula SCD Bilateral. Other. Neuritis BPPV. Menieres
 Dizziness Fistula SCD Bilateral. Other. Neuritis BPPV. Menieres") Otologic Dizziness (Dizziness from Ear) Ear Structures of importance Timothy C. Hain, MD Northwestern University, Chicago t-hain@northwestern.edu The ear is an inertial navigation device Semicircular Canals
Otologic Dizziness (Dizziness from Ear) Ear Structures of importance Timothy C. Hain, MD Northwestern University, Chicago t-hain@northwestern.edu The ear is an inertial navigation device Semicircular Canals
Benign Paroxysmal Positional Vertigo (BPPV) Structures of importance. The ear is an inertial navigation device. Vestibular Reflexes
 Structures of importance. The ear is an inertial navigation device. Vestibular Reflexes") Otologic Dizziness (Dizziness from Ear) Structures of importance Timothy C. Hain, MD Northwestern University, Chicago t-hain@northwestern.edu The ear is an inertial navigation device Semicircular Canals
Otologic Dizziness (Dizziness from Ear) Structures of importance Timothy C. Hain, MD Northwestern University, Chicago t-hain@northwestern.edu The ear is an inertial navigation device Semicircular Canals
Course: PG- Pathshala Paper number: 13 Physiological Biophysics Module number M23: Posture and Movement Regulation by Ear.
 Course: PG- Pathshala Paper number: 13 Physiological Biophysics Module number M23: Posture and Movement Regulation by Ear Principal Investigator: Co-Principal Investigator: Paper Coordinator: Content Writer:
Course: PG- Pathshala Paper number: 13 Physiological Biophysics Module number M23: Posture and Movement Regulation by Ear Principal Investigator: Co-Principal Investigator: Paper Coordinator: Content Writer:
met het oog op evenwicht
 met het oog op evenwicht Herman Kingma, Department of ORL, Maastricht University Medical Centre Faculty of Biomedical Technology, Technical University Eindhoven problems in patients with dizziness and
met het oog op evenwicht Herman Kingma, Department of ORL, Maastricht University Medical Centre Faculty of Biomedical Technology, Technical University Eindhoven problems in patients with dizziness and
The Big 3 of Vertigo
 They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
They feel it, you see it, few know it: Common vertigo conditions seen, but rarely diagnosed Peter Johns MD, FRCPC University of Ottawa pjohns@toh.ca Twitter @peterjohns84 The Big 3 of Vertigo BPPV Vestibular
Vertigo. Tunde Magyar MD, PhD
 Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
Vertigo Tunde Magyar MD, PhD What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea
What could be reffered to as dizziness by the patient?
 What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
What could be reffered to as dizziness by the patient? Rotational vertigo Sense of instability Ataxia of gait Disturbance of vision Loss of contact with surroundings Nausea Loss of memory Loss of confidence
Dominic J Mort 23/03/17 Spire Bushey Hospital
 Dominic J Mort 23/03/17 Spire Bushey Hospital Dizziness Good grief! Hx: Pre-syncope Dizziness As if you might faint? Vertigo Mostly about this As if on a merry-go-round? Non-rotational commoner than spinning
Dominic J Mort 23/03/17 Spire Bushey Hospital Dizziness Good grief! Hx: Pre-syncope Dizziness As if you might faint? Vertigo Mostly about this As if on a merry-go-round? Non-rotational commoner than spinning
I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General
 I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General Dizziness and Balance is a broad area encompassing multiple fields: primary care (internal medicine, pediatrics),
I m dizzy-what can I expect at my doctor visit? Dennis M. Moore, M.D. Lutheral General Dizziness and Balance is a broad area encompassing multiple fields: primary care (internal medicine, pediatrics),
Particle Liberation Maneuvers for Benign Paroxysmal Positional Vertigo
 Particle Liberation Maneuvers for Benign Paroxysmal Positional Vertigo Ahmed A. El Degwi, MD* and Ayman E. El Sharabasy, MD** ENT Department * and Audiology Unit** Mansoura Faculty of Medicine Abstract
Particle Liberation Maneuvers for Benign Paroxysmal Positional Vertigo Ahmed A. El Degwi, MD* and Ayman E. El Sharabasy, MD** ENT Department * and Audiology Unit** Mansoura Faculty of Medicine Abstract
Vertigo. Definition Important history questions Examination Common vertigo cases and management Summary
 Vertigo Vertigo Definition Important history questions Examination Common vertigo cases and management Summary Cases 1) 46 year old man presents two weeks after knocking his head with recurrent episodes
Vertigo Vertigo Definition Important history questions Examination Common vertigo cases and management Summary Cases 1) 46 year old man presents two weeks after knocking his head with recurrent episodes
exercise HOW TO DO IT: PRACTICAL NEUROLOGY
 36 PRACTICAL NEUROLOGY HOW TO DO IT: exercise Pract Neurol: first published as 10.1046/j.1474-7766.2001.00406.x on 1 October 2001. Downloaded from http://pn.bmj.com/ on 14 October 2018 by guest. Protected
36 PRACTICAL NEUROLOGY HOW TO DO IT: exercise Pract Neurol: first published as 10.1046/j.1474-7766.2001.00406.x on 1 October 2001. Downloaded from http://pn.bmj.com/ on 14 October 2018 by guest. Protected
Instructions for BPPV Testing
 Instructions for BPPV Testing You are scheduled for a balance workup on With: Paige Pierozynski, AuD Bernice A. McKenzie, AuD Please report to: The Hearing & Dizziness Clinic 35 Victoria Ave, Essex ON
Instructions for BPPV Testing You are scheduled for a balance workup on With: Paige Pierozynski, AuD Bernice A. McKenzie, AuD Please report to: The Hearing & Dizziness Clinic 35 Victoria Ave, Essex ON
Current Concepts in the Management of Patients With Vestibular Dysfunction
 Current Concepts in the Management of Patients With Vestibular Dysfunction Kathleen M Gill-Body, PT, MS, NCS Objectives After reading this continuing education (CE) article, you should be able to: Describe
Current Concepts in the Management of Patients With Vestibular Dysfunction Kathleen M Gill-Body, PT, MS, NCS Objectives After reading this continuing education (CE) article, you should be able to: Describe
Vertigo. David Clark, DO Oregon Neurology Associates Springfield, OR
 Vertigo David Clark, DO Oregon Neurology Associates Springfield, OR 44F vertigo, nausea & vomiting Unidirectional Nystagmus 44F vertigo, nausea & vomiting Impaired VOR Gain to the right Vertigo History
Vertigo David Clark, DO Oregon Neurology Associates Springfield, OR 44F vertigo, nausea & vomiting Unidirectional Nystagmus 44F vertigo, nausea & vomiting Impaired VOR Gain to the right Vertigo History
The Physiology of the Senses Lecture 10 - Balance
 The Physiology of the Senses Lecture 10 - Balance www.tutis.ca/senses/ Contents Objectives... 1 The sense of balance originates in the labyrinth.... 2 The vestibular system has two parts.... 3 The Anatomy
The Physiology of the Senses Lecture 10 - Balance www.tutis.ca/senses/ Contents Objectives... 1 The sense of balance originates in the labyrinth.... 2 The vestibular system has two parts.... 3 The Anatomy
Dizziness is a Health Concern. Vestibular Disorders and Rehabilitation. ReZlexes. ReZlex (cont.) Functions of Vestibular System. Dysfunction 2/24/13
 Functions of Vestibular System. Dysfunction 2/24/13") Vestibular Disorders and Rehabilitation Week 8: Dr. E Dizziness is a Health Concern From 2001-2004, 35.4% of US adults age 40 y/o and > had vestibular dysfunction. People with a measured vestibular dysfunction
Vestibular Disorders and Rehabilitation Week 8: Dr. E Dizziness is a Health Concern From 2001-2004, 35.4% of US adults age 40 y/o and > had vestibular dysfunction. People with a measured vestibular dysfunction
An Introduction to Dizziness and Vertigo
 An Introduction to Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base Surgery McGill University
An Introduction to Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base Surgery McGill University
A&P 1. Ear, Hearing & Equilibrium Lab. Basic Concepts. Pre-lab Exercises
 A&P 1 Ear, Hearing & Equilibrium Lab Basic Concepts Pre-lab Exercises In this "Lab Exercise Guide", we will be looking at the basics of hearing and equilibrium. NOTE: these notes do not follow the order
A&P 1 Ear, Hearing & Equilibrium Lab Basic Concepts Pre-lab Exercises In this "Lab Exercise Guide", we will be looking at the basics of hearing and equilibrium. NOTE: these notes do not follow the order
ORIGINAL ARTICLE. A New Physical Maneuver for the Treatment of Benign Paroxysmal Positional Vertigo
 ORIGINAL ARTICLE Victor Vital, MD; Athanasia Printza, MD; Joseph Vital, MD; Stefanos Triaridis, MD; Miltiadis Tsalighopoulos, MD From the Department of Otolaryngology, Aristotle University of Thessaloniki,
ORIGINAL ARTICLE Victor Vital, MD; Athanasia Printza, MD; Joseph Vital, MD; Stefanos Triaridis, MD; Miltiadis Tsalighopoulos, MD From the Department of Otolaryngology, Aristotle University of Thessaloniki,
Evaluation & Management of Vestibular Disorders
 Evaluation & Management of Vestibular Disorders Richard A. Roberts, Ph.D., FAAA Alabama Hearing & Balance Associates, Inc. Disclosure and Copyright Statements Richard Roberts has no financial or nonfinancial
Evaluation & Management of Vestibular Disorders Richard A. Roberts, Ph.D., FAAA Alabama Hearing & Balance Associates, Inc. Disclosure and Copyright Statements Richard Roberts has no financial or nonfinancial
VESTIBULAR FUNCTION TESTING
 VESTIBULAR FUNCTION TESTING Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
VESTIBULAR FUNCTION TESTING Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
THE STATS KEEPING YOUR BALANCE THE PROFESSIONALS 2/23/2018 THE STATS QUALITY OF LIFE QUALITY OF LIFE - FALLS
 KEEPING YOUR BALANCE EVAL & MANAGEMENT OF INNER EAR BALANCE DISORDERS Dr. Lily V. Hughes, Audiologist Fairbanks Hearing & Balance Center at the ENT Clinic THE STATS THE STATS QUALITY OF LIFE Vestibular
KEEPING YOUR BALANCE EVAL & MANAGEMENT OF INNER EAR BALANCE DISORDERS Dr. Lily V. Hughes, Audiologist Fairbanks Hearing & Balance Center at the ENT Clinic THE STATS THE STATS QUALITY OF LIFE Vestibular
Labyrinthitis and Vestibular Neuritis
 Labyrinthitis and Vestibular Neuritis http://www.patient.co.uk/health/labyrinthitis-and-vestibular-neuritis.htm Labyrinthitis and vestibular neuritis are most commonly caused by a viral infection that
Labyrinthitis and Vestibular Neuritis http://www.patient.co.uk/health/labyrinthitis-and-vestibular-neuritis.htm Labyrinthitis and vestibular neuritis are most commonly caused by a viral infection that
International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal)
") ORIGINAL ARTICLE International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal) PHYSICAL THERAPY MANAGEMENT IN PATIENTS WITH CERVICOGENIC DIZZINESS-A CASE
ORIGINAL ARTICLE International Journal of Medical and Exercise Science (Multidisciplinary, Peer Reviewed and Indexed Journal) PHYSICAL THERAPY MANAGEMENT IN PATIENTS WITH CERVICOGENIC DIZZINESS-A CASE
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium!
 Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! Chapter 17 Part 2 Special Senses! The Special Senses! Hearing and Equilibrium!
 Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
Chapter 17, Part 2! The Special Senses! Hearing and Equilibrium! SECTION 17-5! Equilibrium sensations originate within the inner ear, while hearing involves the detection and interpretation of sound waves!
COGS 107B Week 2. Hyun Ji Friday 4:00-4:50pm
 COGS 107B Week 2 Hyun Ji Friday 4:00-4:50pm Lecture 3: Proprioception Principles: The Neuron Doctrine and The Law of Dynamic Polarization Proprioception Joint-protecting reflexes (ex. Knee jerk reflex)
COGS 107B Week 2 Hyun Ji Friday 4:00-4:50pm Lecture 3: Proprioception Principles: The Neuron Doctrine and The Law of Dynamic Polarization Proprioception Joint-protecting reflexes (ex. Knee jerk reflex)
Instructions for Vestibular Testing
 Instructions for Vestibular Testing You are scheduled for a balance workup on With: Paige Pierozynski, AuD Bernice A. McKenzie, AuD Please report to: The Hearing & Dizziness Clinic 35 Victoria Ave, Essex
Instructions for Vestibular Testing You are scheduled for a balance workup on With: Paige Pierozynski, AuD Bernice A. McKenzie, AuD Please report to: The Hearing & Dizziness Clinic 35 Victoria Ave, Essex
Vestibular Symptoms in Concussion: Medical/Surgical Perspective. Jacob R. Brodsky, MD Boston Children s Hospital
 Vestibular Symptoms in Concussion: Medical/Surgical Perspective Jacob R. Brodsky, MD Boston Children s Hospital jacob.brodsky@childrens.harvard.edu On Field Symptoms Headache Dizziness Confusion Fatigue
Vestibular Symptoms in Concussion: Medical/Surgical Perspective Jacob R. Brodsky, MD Boston Children s Hospital jacob.brodsky@childrens.harvard.edu On Field Symptoms Headache Dizziness Confusion Fatigue
Workshop: The Assessment of Patients with Dizziness and Vertigo
 Workshop: The Assessment of Patients with Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base
Workshop: The Assessment of Patients with Dizziness and Vertigo Tamara Mijovic MD CM FRCSC Clinical Assistant Professor Department of Otolaryngology Head and Neck Surgery Otology, Neurotology & Skull Base
Balance disorders What is a balance disorder? How does the vestibular system work?
 Balance disorders What is a balance disorder? A balance disorder is a condition that makes you feel unsteady or dizzy, as if you are moving, spinning, or floating, even though you are standing still or
Balance disorders What is a balance disorder? A balance disorder is a condition that makes you feel unsteady or dizzy, as if you are moving, spinning, or floating, even though you are standing still or
Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, :00 AM-10:00 AM
 Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, 2017 8:00 AM-10:00 AM Kerry Lammers, PT, DPT Gabrielle Steinhorn, PT, DPT, NCS Vestibular dysfunction
Defining Dizziness: An Acute Approach to Vestibular Dysfunction in the Hospital Setting Friday, February 17, 2017 8:00 AM-10:00 AM Kerry Lammers, PT, DPT Gabrielle Steinhorn, PT, DPT, NCS Vestibular dysfunction
Body Mechanics--Posture, Alignment & Core
 Body Mechanics--Posture, Alignment & Core Proper Alignment Proper body alignment allows you to safely perform different tasks throughout the day, and to do so in a way that does not require you to exert
Body Mechanics--Posture, Alignment & Core Proper Alignment Proper body alignment allows you to safely perform different tasks throughout the day, and to do so in a way that does not require you to exert
UNDERSTANDING VERTIGO
 Backgrounder UNDERSTANDING VERTIGO Vertigo is a false sensation of movement, either of one s self or one s surroundings. It may exist as an isolated symptom or it may be associated with other conditions
Backgrounder UNDERSTANDING VERTIGO Vertigo is a false sensation of movement, either of one s self or one s surroundings. It may exist as an isolated symptom or it may be associated with other conditions
VERTIGO. Tuesday 20 th February 2018 Dr Rukhsana Hussain. Disclaimers apply:
 VERTIGO Tuesday 20 th February 2018 Dr Rukhsana Hussain WHAT IS VERTIGO? 4 Vertigo is defined as an illusory sensation of motion of either the self or the surroundings in the absence of true motion. Explaining
VERTIGO Tuesday 20 th February 2018 Dr Rukhsana Hussain WHAT IS VERTIGO? 4 Vertigo is defined as an illusory sensation of motion of either the self or the surroundings in the absence of true motion. Explaining
INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE
 INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE David Domoracki Ph.D. Cleveland VAMC Audiology Service Jennifer
INCIDENCE OF SUSPECTED OTOLITHIC ABNORMALITIES IN MILD TRAUMATIC BRAIN INJURED VETERANS OBSERVATIONS FROM A LARGE VA POLYTRAUMA NETWORK SITE David Domoracki Ph.D. Cleveland VAMC Audiology Service Jennifer
Window to an Unusual Vestibular Disorder By Mark Parker
 WELCOME BACK to an ongoing series that challenges the audiologist to identify a diagnosis for a case study based on a listing and explanation of the nonaudiology and audiology test battery. It is important
WELCOME BACK to an ongoing series that challenges the audiologist to identify a diagnosis for a case study based on a listing and explanation of the nonaudiology and audiology test battery. It is important
Peripheral vestibular disorders will affect 1 of 13 people in their lifetime
 Peripheral vestibular disorders will affect 1 of 13 people in their lifetime 80% of affected persons seek medical consultation Unclear how many of these are for peripheral vs central disorders Generally:
Peripheral vestibular disorders will affect 1 of 13 people in their lifetime 80% of affected persons seek medical consultation Unclear how many of these are for peripheral vs central disorders Generally:
The Dizziness Handicap Inventory and Its Relationship with Vestibular Diseases
 Int. Adv. Otol. 2012; 8:(1) 69-77 ORIGINAL ARTICLE The Dizziness Handicap Inventory and Its Relationship with Vestibular Diseases Mi Joo Kim, Kyu-Sung Kim, Yeon Hee Joo, Soo Young Park, Gyu Cheol Han Department
Int. Adv. Otol. 2012; 8:(1) 69-77 ORIGINAL ARTICLE The Dizziness Handicap Inventory and Its Relationship with Vestibular Diseases Mi Joo Kim, Kyu-Sung Kim, Yeon Hee Joo, Soo Young Park, Gyu Cheol Han Department
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Comparison of Effectiveness of Epley s Maneuver and Half-Somersault Exercise with Brandt-Daroff
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Original Research Article Comparison of Effectiveness of Epley s Maneuver and Half-Somersault Exercise with Brandt-Daroff
Balance Assessment and Rehabilitation in Audiology. Andy Phillips Director of Therapies and Health Science ABMU Health Board
 Balance Assessment and Rehabilitation in Audiology Andy Phillips Director of Therapies and Health Science ABMU Health Board Balance Mechanism This has 3 components -Sensory Input -Central Processing -Motor
Balance Assessment and Rehabilitation in Audiology Andy Phillips Director of Therapies and Health Science ABMU Health Board Balance Mechanism This has 3 components -Sensory Input -Central Processing -Motor
Disclosures. Goals. Canalith Repositioning Basics to Advanced. John Li, M.D. We have no conflicts of interest to disclose.
 Canalith Repositioning Basics to Advanced John Li, M.D. Disclosures We have no conflicts of interest to disclose. Goals Beginner to Epert 2 hrs into 1 Definition, History, Physical, Diagnosis, Treatment
Canalith Repositioning Basics to Advanced John Li, M.D. Disclosures We have no conflicts of interest to disclose. Goals Beginner to Epert 2 hrs into 1 Definition, History, Physical, Diagnosis, Treatment
Subject: Vestibular Rehabilitation
 01-92502-14 Original Effective Date: 06/15/05 Reviewed: 09/27/18 Revised: 10/15/18 Subject: Vestibular Rehabilitation THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
01-92502-14 Original Effective Date: 06/15/05 Reviewed: 09/27/18 Revised: 10/15/18 Subject: Vestibular Rehabilitation THIS MEDICAL COVERAGE GUIDELINE IS NOT AN AUTHORIZATION, CERTIFICATION, EXPLANATION
BPPV: pathophysiology, subtypes and therapy Marco Mandalà
 BPPV: pathophysiology, subtypes and therapy Marco Mandalà ENT Department, University of Siena, Italy BPPV Most frequent vestibular disease Most common cause of vertigo in humans Lifetime prevalence: 2.4%
BPPV: pathophysiology, subtypes and therapy Marco Mandalà ENT Department, University of Siena, Italy BPPV Most frequent vestibular disease Most common cause of vertigo in humans Lifetime prevalence: 2.4%
Vertigo. Done by : Njoud Alrasheed. Reviewed by :Hadeel B. Alsulami. Correction File
 Vertigo Objectives: To know anatomy of balance organs Physiology of balance Relevant history in dizzy patients Classification of vertigo Common peripheral causes of vertigo, clinical features, investigation
Vertigo Objectives: To know anatomy of balance organs Physiology of balance Relevant history in dizzy patients Classification of vertigo Common peripheral causes of vertigo, clinical features, investigation
Romberg Balance. Stand with feet together, up tall. Hold balance for seconds
 VOR Horizontal - Sit with arm fully extended and thumb out in front - Tip head down 30 degrees - Move head side to side in rapid small movements like shaking head no - Go as quickly as possible while keeping
VOR Horizontal - Sit with arm fully extended and thumb out in front - Tip head down 30 degrees - Move head side to side in rapid small movements like shaking head no - Go as quickly as possible while keeping
2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard
 2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard 1 2/8/2017 MY GOAL TODAY. 1. Provide a quick overview on falls 2. How our balance systems work 3. What treatments
2/8/2017 WHERE ARE WE? East Amherst East Aurora Hamburg West Seneca Williamsville Boulevard 1 2/8/2017 MY GOAL TODAY. 1. Provide a quick overview on falls 2. How our balance systems work 3. What treatments
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination
 Three-step H.I.N.T.S. eye examination") Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
9/6/2017. Physical Therapist Role in Management of Concussions. Areas where Physical Therapy Can Help. What is the Vestibular System?
 Physical Therapist Role in Management of Concussions The APTA recognizes that physical therapists are part of the multidisciplinary team of licensed healthcare providers that assist in concussion management,
Physical Therapist Role in Management of Concussions The APTA recognizes that physical therapists are part of the multidisciplinary team of licensed healthcare providers that assist in concussion management,
Ear. Utricle & saccule in the vestibule Connected to each other and to the endolymphatic sac by a utriculosaccular duct
 Rahaf Jreisat *You don t have to go back to the slides. Ear Inner Ear Membranous Labyrinth It is a reflection of bony labyrinth but inside. Membranous labyrinth = set of membranous tubes containing sensory
Rahaf Jreisat *You don t have to go back to the slides. Ear Inner Ear Membranous Labyrinth It is a reflection of bony labyrinth but inside. Membranous labyrinth = set of membranous tubes containing sensory
Evaluation of the Dizzy Patient
 Evaluation of the Dizzy Patient S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 1, 2007 Who Sees Dizzy Patients? ED physicians Internists Neurologists ENT
Evaluation of the Dizzy Patient S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 1, 2007 Who Sees Dizzy Patients? ED physicians Internists Neurologists ENT
NIDCD Fact Sheet. Balance Disorders
 NIDCD Fact Sheet Balance Disorders hearing balance U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES NATIONAL INSTITUTES OF HEALTH NATIONAL INSTITUTE ON DEAFNESS AND OTHER COMMUNICATION DISORDERS What is a balance
NIDCD Fact Sheet Balance Disorders hearing balance U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES NATIONAL INSTITUTES OF HEALTH NATIONAL INSTITUTE ON DEAFNESS AND OTHER COMMUNICATION DISORDERS What is a balance
Vestibular testing: what patients can expect
 American Hearing Research Foundation Symposium on Dizziness & Balance Disorders April 6, 2013 Vestibular testing: what patients can expect Marcello Cherchi, MD PhD Assistant Professor of Neurology Northwestern
American Hearing Research Foundation Symposium on Dizziness & Balance Disorders April 6, 2013 Vestibular testing: what patients can expect Marcello Cherchi, MD PhD Assistant Professor of Neurology Northwestern
Update '08: Vestibular and Balance Rehabilitation Therapy
 Update '08: Vestibular and Balance Rehabilitation Therapy In Context with Surgery Medicine & Diet Symptoms of Dizziness Dizziness non-specific term; encompasses any and all of the specific symptoms: Vertigo
Update '08: Vestibular and Balance Rehabilitation Therapy In Context with Surgery Medicine & Diet Symptoms of Dizziness Dizziness non-specific term; encompasses any and all of the specific symptoms: Vertigo
Vestibular service (balance)
") The vestibular service at Addenbrooke s Hospital works closely with the Ear Nose and Throat (ENT), Neurology consultants and physiotherapists to help manage patients with dizziness/balance problems. The
The vestibular service at Addenbrooke s Hospital works closely with the Ear Nose and Throat (ENT), Neurology consultants and physiotherapists to help manage patients with dizziness/balance problems. The
Assessing the Deaf & the Dizzy. Phil Bird Senior Lecturer University of Otago, Christchurch Consultant Otolaryngologist CPH & Private
 Assessing the Deaf & the Dizzy Phil Bird Senior Lecturer University of Otago, Christchurch Consultant Otolaryngologist CPH & Private Overview Severe & profoundly deaf children & adults Neonatal screening
Assessing the Deaf & the Dizzy Phil Bird Senior Lecturer University of Otago, Christchurch Consultant Otolaryngologist CPH & Private Overview Severe & profoundly deaf children & adults Neonatal screening
A review of the otological aspects of whiplash injury. Journal of Forensic and Legal Medicine Volume 16, Issue 2, February 2009, Pages 53-55
 A review of the otological aspects of whiplash injury 1 Journal of Forensic and Legal Medicine Volume 16, Issue 2, February 2009, Pages 53-55 R.M.D. Tranter and J.R. Graham FROM ABSTRACT Approximately
A review of the otological aspects of whiplash injury 1 Journal of Forensic and Legal Medicine Volume 16, Issue 2, February 2009, Pages 53-55 R.M.D. Tranter and J.R. Graham FROM ABSTRACT Approximately
Sky Ridge Medical Center, Aspen Building Ridgegate Pkwy., Suite 309 Lone Tree, Colorado Office: Fax:
 ANKLE SPRAIN What is the ATFL? The ankle joint is made up of the tibia, fibula (bones in the lower leg) and the talus (bone below the tibia and fibula). Ligaments in the ankle connect bone to bone and
ANKLE SPRAIN What is the ATFL? The ankle joint is made up of the tibia, fibula (bones in the lower leg) and the talus (bone below the tibia and fibula). Ligaments in the ankle connect bone to bone and
VIDEONYSTAGMOGRAPHY (VNG) TUTORIAL
 TUTORIAL") VIDEONYSTAGMOGRAPHY (VNG) TUTORIAL Expected Outcomes Site of lesion localization: Determine which sensory input, motor output, and/or neural pathways may be responsible for the patient s reported symptoms
VIDEONYSTAGMOGRAPHY (VNG) TUTORIAL Expected Outcomes Site of lesion localization: Determine which sensory input, motor output, and/or neural pathways may be responsible for the patient s reported symptoms
Snow Angels on Foam Roll
 Thoracic Mobilization on Foam Roll Lie on your back with a foam roller positioned horizontally across your mid back, and arms crossed in front of your body. Bend your knees so your feet are resting flat
Thoracic Mobilization on Foam Roll Lie on your back with a foam roller positioned horizontally across your mid back, and arms crossed in front of your body. Bend your knees so your feet are resting flat
The Vestibular System
 The Vestibular System Vestibular and Auditory Sensory Organs Bill Yates, Ph.D. Depts. Otolaryngology & Neuroscience University of Pittsburgh Organization of Sensory Epithelium Displacement of Stereocilia
The Vestibular System Vestibular and Auditory Sensory Organs Bill Yates, Ph.D. Depts. Otolaryngology & Neuroscience University of Pittsburgh Organization of Sensory Epithelium Displacement of Stereocilia
Chapter 19 Dizziness and Vertigo
 Chapter 19 Dizziness and Vertigo Episode overview: 1) Compare characteristics of peripheral and central vertigo 2) What are risk factors for central causes of vertigo? 3) List 4 vestibulotoxic drugs. 4)
Chapter 19 Dizziness and Vertigo Episode overview: 1) Compare characteristics of peripheral and central vertigo 2) What are risk factors for central causes of vertigo? 3) List 4 vestibulotoxic drugs. 4)
Phase 1 Initiating Normal Spinal Motion. Activities to Avoid or Minimize. Good choices to make
 Phase 1 Initiating Normal Spinal Motion Activities to Avoid or Minimize 1. Sitting 2. Standing with weight on one foot 3. Reading on back with head flexed forward 4. One sided sports (always practice both
Phase 1 Initiating Normal Spinal Motion Activities to Avoid or Minimize 1. Sitting 2. Standing with weight on one foot 3. Reading on back with head flexed forward 4. One sided sports (always practice both