Headache evaluation and management after concussion. Assistant Professor
|
|
|
- Reynard Green
- 5 years ago
- Views:
Transcription

1 Headache evaluation and management after concussion Juliette Preston, M.D. Assistant Professor OHSU Headache Center
2 OVERVIEW Introduction Definition Acute post-traumatic headache Red flags Persistent post-traumatic headache Recognizing headache types Treatment options
3 INTRODUCTION Headache is one of the most common and persistent symptom following traumatic brain injury. An estimated 2.5 million reported TBIs per year in the USA alone ( Lucas. Curr Pain Headache Rep 2015) 75% of TBI are considered mild (Lucas et al. Cephalgia 2014)

4 Prevalence at 1 year? Prevalence remains high at over 44 % throughout the year after moderate or severe TBI and over 54 % after mild TBI (Lucas et al, Curr Pain Headache Rep, 2015).
5 DEFINITION The diagnostic criteria of ICHD-3 beta for all subtypes require that headache must be reported to have developed within 7 days of trauma or injury. or within 7 days after regaining consciousness and/or the ability to sense and report pain when these have been lost following trauma or injury. The International Classification of Headache Disorders, 3rd edition (beta version), 2013
,")
6 Post traumatic headache attributed to moderate to severe injury to the head The International Classification of Headache Disorders, 3rd edition (beta version), 2013

7 Post traumatic headache attributed to mild injury to the head The International Classification of Headache Disorders, 3rd edition (beta version), 2013
8 DEFINITION During the first 3 months from onset they are considered acute. if they continue beyond that period they are designated persistent.
9 Acute post-traumatic headache Immediately following a head injury Want to identify the injury severity and other associated injuries The sideline or acute medical evaluation should include a systematic examination including how the trauma occurred symptoms following it presence of amnesia, memory problems or loss of consciousness, balance problems, and/or overall behavior change from baseline
10 If there are headaches History of headache prior to trauma Family history of headache Neuroimaging? Concern for skull or spine fracture if red flags are present
 and anticoagulation")
11 RED FLAGS Concern for intracranial process abnormalities or asymmetries on neurologic examination altered mental status worsening headache with Valsalva maneuver underlying risk factors such as hypercoagulable state (genetic or acquired, pregnancy, cancer) and anticoagulation therapy
12 CASE 1 28 yo woman presented to the ED with 5 day gradual persistent headache and scalp tenderness after a whiplash injury. She was rear ended at a stop sign. There was no LOC and she denies any balance difficulty, memory problem or overall behavior changes.
13 CASE 1 On examination she was normotensive and her temperature was also normal. There was no meningeal signs She had no neurological deficit CTH was unremarkable She was reassured and send home

14 CASE 1 The next morning, she noted difficulty in eating. She was able to swallow but found it difficult to move her tongue. She had no hoarseness. On examination her speech was dysarthric, and she had leftward deviation on tongue protrusion. Taste and tongue sensation were normal.

15 TONGUE WEAKNESS CN12 (HYPOGLOSSAL NERVE)

 And")
16 ARTERIAL DISSECTION MRA showed reduction in caliber of L ICA (A) And pseudoaneurysm (B)
17 CASE 1 She was started on ASA Repeat imaging were done at 6 weeks, slight improvement in L ICA was shown. At 3 months in f/u clinic visit, her speech had improved with only occasional dysarthria. She no longer reported headaches.
18 CASE 2 19 yo woman presented with 3 days of mild but constant headache after being hit by soccer ball while playing with her cousin. She complained of difficulty focusing and double vision.
19 CASE 2 Her past medical history is significant for knee surgery 2 months ago, had developed a DVT and was started on anticoagulation 4 weeks ago. On exam, vital signs are normal. BMI >25

20 CASE 2 Pupils were asymmetric Difficulty with adducting R eye CN 3 palsy


21 Normal MRI T1- weighted MRI: hyperintense sellar mass
22 PITUITARY APOPLEXY It s characterized by acute infarction and/or hemorrhage of the pituitary gland. Present with : Headache visual impairment cranial nerve palsies impairment of consciousness pituitary hormone deficiencies. In most cases, apoplexy involves a previously unrecognized pituitary adenoma.

23 Four categories of triggering factors Vascular flux reduction: surgery, specially cardiac surgery, radiotherapy, post spinal anesthesia. Acute increase in blood flow: pregnancy, systemic hypertension. Pituitary stimulation: provocative pituitary tests, specially TRH, GnRH analogues use. Coagulation disturbances: thrombocytopenia, anticoagulation.

24 Take home message.. Acute post traumatic headache with subtle neurological findings should be investigated.
25 PERSISTENT POST TRAUMATIC HEADACHE After 4-11 years, 500 veterans with TBI ( Couch et al, Headache, 2016) TBI - 89% had migraine, 2% probable migraine, 9% had tension, and 0% had no headaches. Control - 36% had migraine, 15% probable migraine, 27% tension, and 22% no headache (P <.0001). Migraine with aura occurred in 38% of TBI and 6% of control (P <.0001). There was no correlation of severity of headache problem with severity of TBI.
26 PERSISTENT POST TRAUMATIC HEADACHE The most common headache type after mtbi are migraine headache and tension-type headache. No randomized clinical trials of medication for posttraumatic headache in either children or adults. Management should be tailored to the type of headache.

27 CASE 3 20 yo man with pmh significant for ADHD, anxiety presented with daily headaches for 6 months. His headaches started after a second snowboard accident. Both event were separated by a few weeks. No LOC, hit his head, felt foggy afterward. Now he still reports difficulty concentrating (attending college, has a W on econ class)
28 CASE 3 His headaches are located in his temples, top of head and back of the head. Intensity varies between 2-4/10. No nausea, light, sound or smell sensitivity Physical activity does not aggravate his headaches.
29 CASE 3 Neurological exam is normal MRI brain done previously was unremarkable He is here with his mom who is very anxious
30 CASE 3 Diagnosis? A. Migraine headache B. Tension-type headache C. Non-classified headache type D. He doesn t have headaches

31 TENSION TYPE HEADACHE Definition: Bilateral location Pressing or tightening (non-pulsating) quality Mild intensity Not aggravated by routine physical activity such as walking or climbing stairs No nausea or vomiting No more than one of photophobia or phonophobia
 Nausea, vomiting, or both Photophobia and phonophobia Last")
32 DEFINITION MIGRAINE HEADACHE Unilateral location Pulsating quality Moderate or severe pain intensity Aggravation by or causing avoidance of routine physical activity (eg, walking or climbing stairs) Nausea, vomiting, or both Photophobia and phonophobia Last >4 hours
33 CASE 3 Diagnosis? A. Migraine headache B. Tension-type headache C. Non-classified headache D. He doesn t have headaches
34 TREATMENT TCA Amitriptyline ( mg qhs) Nortriptyline ( mg qhs ) Protriptyline ( 5-20 mg qam)-activating, weight loss SNRI- Venlafaxine ( mg qam) Muscle relaxant-daily-not proven effective Botulinum toxin injection-not proven effective Trigger point injection-effective
35 CASE 3 Patient did well on 20 mg of Nortriptyline He reported 1-2 headaches per week Ibuprofen 400 mg sufficient to abort his headaches. After 6 months of good control, he didn t want to stop Nortriptyline.
36 CASE 4 18 yo woman with past medical history of migraine headache since age 9, who presented with daily headache for 2 years. She used to play basketball and had a handful of concussions, none with LOC. She had only 1 event associated with LOC, at age 16 she fell off her horse. She felt confused for 15 minutes. Her headaches worsen a few weeks afterwards.
37 CASE 4 Her headaches are located behind the right eye, in the forehead, temple and in the back of the head. The quality of the pain can be throbbing, pressurelike or stabbing. The intensity of the pain varies between 7-10/10. Her headaches are associated with nausea, sensitivity to light, sound, smell, touch, dizziness, fatigue and difficulty concentrating.
38 TRIED MEDICATION/INTERVENTION IN THE PAST 1. Topamax 2. Verapamil 3. Amitriptyline 4. Nortriptyline 5. Lamictal 6. Botox 7. Maxalt 8. Imitrex 9. Zomig NS 10. Toradol IM/IV-helpful 11. Occipital nerve-not effective
39 CASE 4 Currently she is no preventative since nothing ever works for me She only uses Advil or Excedrin to break her headaches.
40 CASE 4 Diagnosis? A. Migraine headache B. Tension-type headache C. Non-classified headache type D. She doesn t have headaches
41 CASE 4 Diagnosis? A. Migraine headache B. Tension-type headache C. Non-classified headache type D. She doesn t have headaches

42 With prompting She admits using 2-3 tablets of either Advil or Excedrin daily. Does that change her diagnosis?
43 No #1 Migraine Headache #2 Medication overuse headache

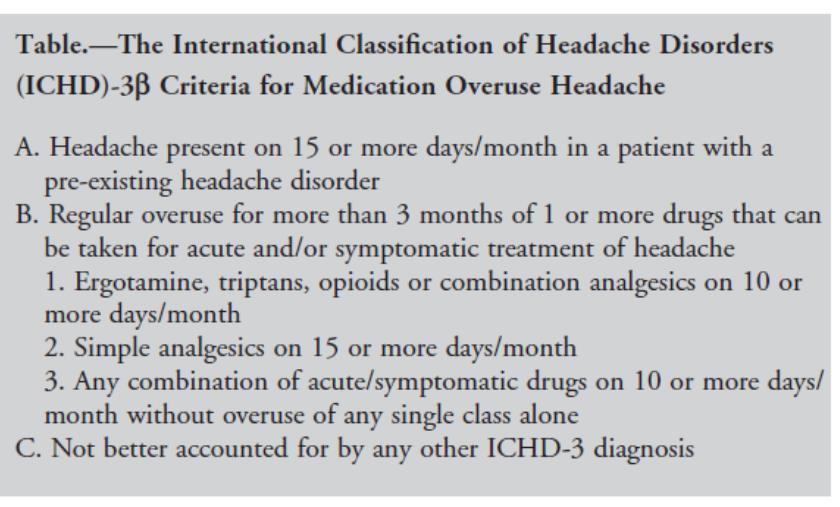
44 MOH Criteria
45 Which drugs? Bigal et al. (2008, Headache) found that barbiturates (butalbital combinations) can cause MOH if used only 5 or more days per month. Opioids if taken 8 days or more per month Triptans if taken 10 or more days per month. Non-steroidal anti-inflammatory drugs (NSAIDs), if if taken 10 or more days per month.
46 CASE 4 Stop daily Advil/Excedrin Bridging therapy (protocol) x 6 weeks long acting NSAIDs ( Naproxen 500 mg bid) + muscle relaxant (Tizanidine 2-16mg qhs) Smith. Headache 2002 Start Venlafaxine 37.5 mg x 2 weeks, then increased to 75 mg qam. Retrial of Rizatriptan ( 10 mg) to break her headaches
.")
47 At 2 months visit She felt like a new person She reports now only 2-4 headaches per month responsive to Rizatriptan ( which did not work in the past). Rizatriptan (10 mg, max 30 mg/24 hrs) was chosen as with Eletriptan ( 40 mg, max 80 mg/24 hrs), they are most potent triptans.
48 When to consider Preventive Treatment? Use acute medications more than 10 days per month No longer responsive to rescue medication Side effects from acute treatment Affect patient daily life-home, work, or school
49 TREATMENT OPTIONS Beta blocker: Propranolol mg daily or bid if short acting, 1-2 mg/kg in children Metoprolol mg daily Nadolol mg daily, fewer side effects than propranolol Atenolol mg daily- fewer side effects than propranolol, more suitable for pts with chronic lung disease/asthma at lower dose
50 Antiepileptic drugs Level A evidence (stablished efficacy) Topiramate: mg qhs ( not effective above 200 mg /day) Valproate/divalproex: mg daily
51 TREATMENT Antidepressant level B evidence (probably effective) Amitriptyline ( 10 mg -75 mg qhs) Venlafaxine ( 37.5 mg- 150 mg qam) Level C evidence ( possibly effective) Lisinopril mg daily Candesartan mg daily Cyproheptadine (12-32 mg bid or qhs)- children/pregnant patient Level U ( inadequate or conflicting data): Acetazolamide, Fluoxetine, Gabapentin, Verapamil
52 Complementary Alternative therapy Physical activity ( 40 min x 3 w) Acupuncture Nutraceuticals Magnesium citrate 400 mg daily Riboflavin 400 mg daily or 200 mg twice a day Coenzyme Q mg qam Biobehavioral treatment CBT Thermal biofeedback with relaxation Relaxation training
53 REVIEW Post traumatic headaches are very common and persistent Treated like a primary headache disorder Mild headache, not aggravated by movement tension-type headache Moderate to severe headache, pt wants to be still migraine headache Headaches with any neurological symptoms Neuroimaging/ED

54 Thank You
Clinical case. Clinical case 3/15/2018 OVERVIEW. Refractory headaches and update on novel treatment. Refractory headache.
 OVERVIEW Refractory headaches and update on novel treatment Definition of refractory headache Treatment approach Medications Neuromodulation In the pipeline Juliette Preston, MD OHSU Headache Center Refractory
OVERVIEW Refractory headaches and update on novel treatment Definition of refractory headache Treatment approach Medications Neuromodulation In the pipeline Juliette Preston, MD OHSU Headache Center Refractory
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation.
 I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
I have no financial relationships to disclose. I will not discuss investigational use of medication in my presentation. In 1962, Bille published landmark epidemiologic survey of headache among 9,000 school
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, II. Management of Refractory Headaches
 October 23, II. Management of Refractory Headaches") Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Headache Master School Japan-Osaka 2016 (HMSJ-Osaka2016) October 23, 2016 II. Management of Refractory Headaches Case presentation 1: A case of intractable daily-persistent headache Keio University School
Strategies in Migraine Care
 Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
Strategies in Migraine Care Julie L. Roth, MD Rhode Island Hospital Assistant Professor, Neurology The Warren Alpert Medical School of Brown University March 28, 2015 Financial Disclosures None. Objectives
A case of a patient with chronic headache. Focus on Migraine. None related to the presentation Grants to conduct clinical trials from: Speaker bureau:
 Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Chronic Daily Headache Bassel F. Shneker, MD, MBA Associate Professor Vice Chair, OSU Neurology The Ohio State University Wexner Medical Center Financial Disclosures None related to the presentation Grants
Headaches in Pregnancy Before, During, and After
 Headaches in Pregnancy Before, During, and After Robert Kaniecki, MD Director, UPMC Headache Center Assistant Professor of Neurology University of Pittsburgh Headaches and Pregnancy Pre-pregnancy counseling
Headaches in Pregnancy Before, During, and After Robert Kaniecki, MD Director, UPMC Headache Center Assistant Professor of Neurology University of Pittsburgh Headaches and Pregnancy Pre-pregnancy counseling
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in
 HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
HMFP Comprehensive Headache Center Department of Anesthesia, Critical Care and Pain Medicine Beth Israel Deaconess Medical Center Instructor in Anesthesia and Neurology Harvard Medical School Limited time
How do we treat migraine? New SIGN Guidelines
 How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
How do we treat migraine? New SIGN Guidelines Managing your migraine Migraine Trust, Edinburgh 2018 Callum Duncan Consultant Neurologist Aberdeen Royal Infirmary Chair SIGN Guideline 155 Premonitory Mood
MIGRAINE UPDATE. Objectives & Disclosures. Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment.
 MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
MIGRAINE UPDATE Karen L. Bremer, MD November 16, 2018 Objectives & Disclosures Learn techniques used to diagnose headaches. Become familiar with medications used for headache treatment. Disclosure: I am
Goals. Primary Headache Syndromes. One-Year Prevalence of Common Headache Disorders
 Goals One-Year Prevalence of Common Headache Disorders Impact of primary headache syndromes Non pharmacologic Rx of migraine individualized to patient triggers Complementary and alternative Rx of migraine
Goals One-Year Prevalence of Common Headache Disorders Impact of primary headache syndromes Non pharmacologic Rx of migraine individualized to patient triggers Complementary and alternative Rx of migraine
Case Presentation. Case Presentation. Case Presentation. Truths about Headaches (2017) Most headaches were muscle-tension headaches
 Most headaches were muscle-tension headaches") Agenda Case presentation Migraine Morphology Primary and Premonitory Phase Secondary Headache Aura Headache Primer on Pain Medication Overuse Headache Case Presentation RT is a 25 year old woman with daily
Agenda Case presentation Migraine Morphology Primary and Premonitory Phase Secondary Headache Aura Headache Primer on Pain Medication Overuse Headache Case Presentation RT is a 25 year old woman with daily
OH, MY ACHING HEAD! I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE MANAGING HEADACHE IN THE OUTPATIENT SETTING SECONDARY HEADACHES
 1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
1 JUSTIN A. OSSMAN, MD CHATTANOOGA FAMILY MEDICINE UPDATE OH, MY ACHING HEAD! MANAGING HEADACHE IN THE OUTPATIENT SETTING 2 I HAVE NO DISCLOSURES OR CONFLICTS OF INTERESTS TO DECLARE OBJECTIVES International
Headache. Headache Case. Migraine Headache. Eric Kraus, MD. Types» Without aura (common)» With aura (classic)
» With aura (classic)") Headache Eric Kraus, MD Headache Case This 23 year-old female has headaches behind the right eye that cause her to lay down in a quiet room. They have a throbbing quality and she may vomit. Migraine Headache
Headache Eric Kraus, MD Headache Case This 23 year-old female has headaches behind the right eye that cause her to lay down in a quiet room. They have a throbbing quality and she may vomit. Migraine Headache
Index. Prim Care Clin Office Pract 31 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Prim Care Clin Office Pract 31 (2004) 441 447 Index Note: Page numbers of article titles are in boldface type. A Abscess, brain, headache in, 388 Acetaminophen for migraine, 406 407 headache from, 369
Faculty Disclosure. Karen L. Bremer, MD. Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest.
 Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Faculty Disclosure Karen L. Bremer, MD Dr. Bremer has listed no financial interest/arrangement that would be considered a conflict of interest. HEADACHE UPDATE Karen L. Bremer, MD November 10, 2017 karen.bremer@creighton.edu
Migraine Management. Jane Melling Headache nurse Mater Misericordiae Hospital
 Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
Migraine Management Jane Melling Headache nurse Mater Misericordiae Hospital Migraine facts Among the most common disorders of the nervous system 3 rd most prevalent medical disorder on the planet (lancet
10/17/2017 CHRONIC MIGRAINES BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES PATIENT CASE EPIDEMIOLOGY EPIDEMIOLOGY
 BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES JENNIFER SHIN, PHARMD PGY2 AMBULATORY CARE PHARMACY RESIDENT COMMUNITYCARE HEALTH CENTERS PHARMACOTHERAPY ROUNDS OCTOBER 20, 2017
BOTOX: TO INJECT OR NOT INJECT? IN CHRONIC MIGRAINE PROPHYLAXIS OBJECTIVES JENNIFER SHIN, PHARMD PGY2 AMBULATORY CARE PHARMACY RESIDENT COMMUNITYCARE HEALTH CENTERS PHARMACOTHERAPY ROUNDS OCTOBER 20, 2017
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy
 HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
Headache and Facial Pain. Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology
 Headache and Facial Pain Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology Introduction It is the most common neurologic complain The diagnosis usually
Headache and Facial Pain Mohammed ALEssa MBBS, FRCSC Assistant Professor Consultant Otolaryngology,Head & Neck Surgical Oncology Introduction It is the most common neurologic complain The diagnosis usually
Treatment of Primary Headache Syndromes
 Presenter Disclosure Information 2:45 3:45pm Treatment of Primary Headache Syndromes SPEAKER Gerald W. Smetana, MD The following relationships exist related to this presentation: Gerald W.Smetana, MD,
Presenter Disclosure Information 2:45 3:45pm Treatment of Primary Headache Syndromes SPEAKER Gerald W. Smetana, MD The following relationships exist related to this presentation: Gerald W.Smetana, MD,
Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital
 Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital Honorarium from Current Pain and Headache Reports; Section Editor Unusual
Jessica Ailani MD FAHS Director, Georgetown Headache Center Associate Professor Neurology Medstar Georgetown University Hospital Honorarium from Current Pain and Headache Reports; Section Editor Unusual
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา
 ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
ปวดศ รษะมา 5 ป ก นยาแก ปวดก ย งไม ข น นพ.พาว ฒ เมฆว ช ย โรงพยาบาลนครราชส มา 1 CONTENT 1 2 3 Chronic Daily Headache Medical Overused Headache Management Headaches are one of the most common symptoms List
HEADACHE. Dr Nick Pendleton. September Headache
 HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
The Pediatric Headache Handbook
 The Pediatric Headache Handbook For the Primary Care Physician Brought to you by the Division of Pediatric Neurology cardinalglennon.com Classification of headache patterns in children Acute onset of worst
The Pediatric Headache Handbook For the Primary Care Physician Brought to you by the Division of Pediatric Neurology cardinalglennon.com Classification of headache patterns in children Acute onset of worst
10/31/2017 PRIMARY CARE AND HEADACHE DISCLOSURES WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Primary Care 67%
 PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
PRIMARY CARE AND HEADACHE Sonja Potrebic MD PhD Regional Headache Specialist Kaiser LAMC 1 WHERE DO THOSE WITH HEADACHE SEEK MEDICAL CARE? Column1 Primary Care 67% Primary Care Headache Specialty Other
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline. Scottish intercollegiate Guidelines Network SIGN
 A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
A synopsis of: Diagnosis and Management of Headaches in Adults: A national clinical guideline Scottish intercollegiate Guidelines Network SIGN November 2008. PETER FRAMPTON MSc MCOptom BAppSc (Optom)(AUS)
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D.
 Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
Prevention and Treatment of Migraines CAITLIN BARNES, PHARM.D. CANDIDATE AMBULATORY CARE JOE CAMMILLERI, PHARM.D. NATOHYA MALLORY, PHARM.D. Objectives Present patient case Review epidemiology/pathophysiology
CHRONIC HEADACHES IN CHILDHOOD
 CHRONIC HEADACHES IN CHILDHOOD EDWIN LIU, MD PEDIATRIC NEUROLOGISTS OF PALM BEACH PEDIATRIC SLEEP CENTERS OF FLORIDA ASSISTANT CLINICAL PROFESSOR FSU ASSISTANT CLINICAL PROFESSOR NOVA SOUTHEASTERN PEDIATRIC
CHRONIC HEADACHES IN CHILDHOOD EDWIN LIU, MD PEDIATRIC NEUROLOGISTS OF PALM BEACH PEDIATRIC SLEEP CENTERS OF FLORIDA ASSISTANT CLINICAL PROFESSOR FSU ASSISTANT CLINICAL PROFESSOR NOVA SOUTHEASTERN PEDIATRIC
25/09/2018 HEADACHE. Dr Nick Pendleton
 HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
Concussion Management. Michael Reardon, M.D. April 24,2016
 Concussion Management Michael Reardon, M.D. April 24,2016 Objectives Understand what a concussion is Know how to recognize it Understand the differential diagnosis Know how to manage and treat symptoms
Concussion Management Michael Reardon, M.D. April 24,2016 Objectives Understand what a concussion is Know how to recognize it Understand the differential diagnosis Know how to manage and treat symptoms
Headache A Practical Approach
 Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
Headache A Practical Approach Integrated Pain Symposium December 1, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache and Pain Development Teams Disclosures:
HEADACHES THE RED FLAGS
 HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
HEADACHES THE RED FLAGS FAYYAZ AHMED CONSULTANT NEUROLOGIST HON. SENIOR LECTURER HULL YORK MEDICAL SCHOOL SECONDARY VS PRIMARY HEADACHES COMMON SECONDARY HEADACHES UNCOMMON BUT SERIOUS SECONDARY HEADACHES
Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert
 Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert Childhood headache: Is it really difficult to manage? It shouldn t be... But it can be...
Ishaq Abu Arafeh Consultant Paediatrician Royal Hospital for Children, Glasgow Forth Valley Royal Hospital, Larbert Childhood headache: Is it really difficult to manage? It shouldn t be... But it can be...
Welcome to the program!
 Calgary Headache Assessment & Management Program (CHAMP) EDUCATION SESSION Welcome to the program! What is the Purpose of this To provide you with: Session? accurate and current headache information the
Calgary Headache Assessment & Management Program (CHAMP) EDUCATION SESSION Welcome to the program! What is the Purpose of this To provide you with: Session? accurate and current headache information the
Headache Mary D. Hughes, MD Neuroscience Associates
 Headache Mary D. Hughes, MD Neuroscience Associates Case 1 22 year old female presents with recurrent headaches. She has had headaches for the past 3 years. They start on the right side of her head and
Headache Mary D. Hughes, MD Neuroscience Associates Case 1 22 year old female presents with recurrent headaches. She has had headaches for the past 3 years. They start on the right side of her head and
Heads Up: Concussion Management. Laurel Short, MSN, FNP-c
 Heads Up: Concussion Management Laurel Short, MSN, FNP-c Diclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in the subject
Heads Up: Concussion Management Laurel Short, MSN, FNP-c Diclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in the subject
Outpatient Headache Care Guideline
 1 Outpatient Care Guideline Inclusion criteria: children > 3 yrs with headaches Is urgent emergency department, neuroimaging, or Neurology consultation indicated? Referral to ED if: New severe headache
1 Outpatient Care Guideline Inclusion criteria: children > 3 yrs with headaches Is urgent emergency department, neuroimaging, or Neurology consultation indicated? Referral to ED if: New severe headache
General Patient Information Dr. David A. Branch, M.D.
 General Patient Information Dr. David A. Branch, M.D. **Please Print** Patient Name: Date of Birth: Social Security # Email Address: Patient Address: _ City: State: Zip Code: Phone : Marital Status: S
General Patient Information Dr. David A. Branch, M.D. **Please Print** Patient Name: Date of Birth: Social Security # Email Address: Patient Address: _ City: State: Zip Code: Phone : Marital Status: S
Headache. Karen Thaxter
 Headache Karen Thaxter An eight year old girl is taken to her paediatrician because she has been complaining of almost daily pain at the back of her head for the past 4 months. She states that each headache
Headache Karen Thaxter An eight year old girl is taken to her paediatrician because she has been complaining of almost daily pain at the back of her head for the past 4 months. She states that each headache
Treatments for migraine
 Treatments for migraine Information for patients and carers Department of Neurology Aberdeen Royal Infirmary Contents Page About this leaflet Abortive medication for migraine Painkillers Antisickness medication
Treatments for migraine Information for patients and carers Department of Neurology Aberdeen Royal Infirmary Contents Page About this leaflet Abortive medication for migraine Painkillers Antisickness medication
Current Migraine Treatment Therapy. Daniel Kassicieh, DO, FAAN
 Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Current Migraine Treatment Therapy Daniel Kassicieh, DO, FAAN Migraine a Disease Process Migraines are a chronic disease process similar to many other chronic medical conditions Migraine has a low mortality
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017
 Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Can I send this headache patient home? Dr Nicola Giffin Consultant Neurologist Bath, Nov 2017 SAH v benign thunderclap headaches Other pathologies not apparent on CT Severe primary headaches: management
Neurological Dilemmas in Primary Care
 Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Neurological Dilemmas in Primary Care David Clark, DO dclark@oregonneurology.com When to test? How to test? Pitfalls in testing? When to treat? How to treat? How long to treat? Neurological Dilemmas Seizure
Headache Questionnaire
 Date: All Headache Patients We would appreciate your cooperation in filling out this form. In our evaluation of headache, your history is typically our most valuable tool for diagnosis and subsequent treatment.
Date: All Headache Patients We would appreciate your cooperation in filling out this form. In our evaluation of headache, your history is typically our most valuable tool for diagnosis and subsequent treatment.
MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache
 MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache Measure Description Percentage of patients age 18 years old and older diagnosed with migraine headache whose migraine frequency is 4 migraine
MEASURE #3: PREVENTIVE MIGRAINE MEDICATION PRESCRIBED Headache Measure Description Percentage of patients age 18 years old and older diagnosed with migraine headache whose migraine frequency is 4 migraine
Headaches in the Pediatric Emergency Dept
 Headaches in Children February 23, 2011 Jinny Tavee, MD Associate Professor Neuromuscular Center Cleveland Clinic Foundation Cleveland, OH 1 Headaches in the Pediatric Emergency Dept Burton Gutierrez Kan
Headaches in Children February 23, 2011 Jinny Tavee, MD Associate Professor Neuromuscular Center Cleveland Clinic Foundation Cleveland, OH 1 Headaches in the Pediatric Emergency Dept Burton Gutierrez Kan
Controlling Migraine Pain
 Migraine Stats Controlling Migraine Pain Alan Zacharias, M.D. Associated Neurologists, Boulder Community Health 303-622-3365 Women 15% Men 5% Usually starts in 2 nd and 3 rd Decade Major Impact on days
Migraine Stats Controlling Migraine Pain Alan Zacharias, M.D. Associated Neurologists, Boulder Community Health 303-622-3365 Women 15% Men 5% Usually starts in 2 nd and 3 rd Decade Major Impact on days
1. On how many days in the last 3 months did you miss work or school because of your headaches?
 The Migraine Disability Assessment Test The MIDAS (Migraine Disability Assessment) questionnaire was put together to help you measure the impact your headaches have on your life. The information on this
The Migraine Disability Assessment Test The MIDAS (Migraine Disability Assessment) questionnaire was put together to help you measure the impact your headaches have on your life. The information on this
Headache. Section 1. Migraine headache. Clinical presentation
 Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Section 1 Headache Migraine headache 1 Clinical presentation It is important to recognize just how significant a problem migraine headache is. It has been estimated that migraine affects 11% of the United
Clinical Learning Days November 10, 2017
 Migraine Clinical Learning Days November 10, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache Disclosures: none Learning Objectives: At the conclusion
Migraine Clinical Learning Days November 10, 2017 Alyssa Lettich. MD Neurosciences Institute/Neurosciences Clinical Program Medical Director Headache Disclosures: none Learning Objectives: At the conclusion
Lynne Kerr, MD May 2014
 Lynne Kerr, MD May 2014 Headache is one of top 5 health problems in children 2 nd most common diagnosis in the peds neurology outpatient clinic 14 year old girl severe headache Headaches 1-2 times/month
Lynne Kerr, MD May 2014 Headache is one of top 5 health problems in children 2 nd most common diagnosis in the peds neurology outpatient clinic 14 year old girl severe headache Headaches 1-2 times/month
This policy addresses only the type B formulation rimabotulinumtoxinb marketed as Myobloc.
 RimabotulinumtoxinB NDC CODE(S) 10454-0710-XX Myobloc 2500 UNIT/0.5ML SOLN (SOLSTICE NEUROSCIENCES) 10454-0711-XX Myobloc 5000 UNIT/ML SOLN (SOLSTICE NEUROSCIENCES) 10454-0712-XX Myobloc 10000 UNIT/2ML
RimabotulinumtoxinB NDC CODE(S) 10454-0710-XX Myobloc 2500 UNIT/0.5ML SOLN (SOLSTICE NEUROSCIENCES) 10454-0711-XX Myobloc 5000 UNIT/ML SOLN (SOLSTICE NEUROSCIENCES) 10454-0712-XX Myobloc 10000 UNIT/2ML
Paediatric headaches. Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services. Brevity, levity, repetition
 Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
Paediatric headaches Dr Jaycen Cruickshank Director of Clinical Training Ballarat Health Services Brevity, levity, repetition Paediatric)headache?)! Headache!in!children!is!not!that!common.!The!question!is!which!headaches!do!I!
COLUMBIA UNIVERSITY HEADACHE CENTER: NEW PATIENT QUESTIONNAIRE
 COLUMBIA UNIVERSITY HEADACHE CENTER: NEW PATIENT QUESTIONNAIRE HEADACHE CHARACTERISTICS Frequency and Severity 1. At what AGE did you get your first headache, of ANY kind? 2. At what AGE did your headaches
COLUMBIA UNIVERSITY HEADACHE CENTER: NEW PATIENT QUESTIONNAIRE HEADACHE CHARACTERISTICS Frequency and Severity 1. At what AGE did you get your first headache, of ANY kind? 2. At what AGE did your headaches
ADVANCES IN MIGRAINE MANAGEMENT
 ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
ADVANCES IN MIGRAINE MANAGEMENT Joanna Girard Katzman, M.D.MSPH Assistant Professor, Dept. of Neurology Project ECHO, Chronic Pain Program University of New Mexico Outline Migraine throughout the decades
Adult with headache. Problem-specific video guides to diagnosing patients and helping them with management and prevention
 Adult with headache Problem-specific video guides to diagnosing patients and helping them with management and prevention London Strategic Clinical Networks London Neuroscience Strategic Clinical Network
Adult with headache Problem-specific video guides to diagnosing patients and helping them with management and prevention London Strategic Clinical Networks London Neuroscience Strategic Clinical Network
Disclosures. Triptans for Kids 5/16/13
 5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
5/16/13 Disclosures Triptans for Kids Amy A. Gelfand, MD GelfandA@neuropeds.ucsf.edu Departments of Neurology and Pediatrics UCSF Child Neurology and Headache Center I receive grant funding from: NIH/NINDS
10/13/17. Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD
 Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD } Depomed Consultant 2014 to present } Avanir Consultant 2014 to present } Amgen
Christy M. Jackson, MD Director, Dalessio Headache Center Scripps Clinic, La Jolla Clinical Professor, Neurosciences UCSD } Depomed Consultant 2014 to present } Avanir Consultant 2014 to present } Amgen
Proposed Project Scope. OPTIMAL USE OnabotulinumtoxinA for the Prevention of Chronic Migraine Clinical Evidence, Policies and Practice
 Proposed Project Scope OPTIMAL USE OnabotulinumtoxinA for the Prevention of Chronic Migraine Clinical Evidence, Policies and Practice May 2018 1. BACKGROUND AND RATIONALE Migraine is a common, debilitating
Proposed Project Scope OPTIMAL USE OnabotulinumtoxinA for the Prevention of Chronic Migraine Clinical Evidence, Policies and Practice May 2018 1. BACKGROUND AND RATIONALE Migraine is a common, debilitating
IT S ALL IN YOUR HEAD!
 IT S ALL IN YOUR HEAD! CARING FOR CONCUSSIONS IN YOUR COMMUNITY Stephen K Stacey, DO CPT, MC, USA OUTLINE Definition Epidemiology Diagnosis Evaluation Recovery Sequelae Prevention Resources for providers
IT S ALL IN YOUR HEAD! CARING FOR CONCUSSIONS IN YOUR COMMUNITY Stephen K Stacey, DO CPT, MC, USA OUTLINE Definition Epidemiology Diagnosis Evaluation Recovery Sequelae Prevention Resources for providers
Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE
 Headache in children and adolescents Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE Dept. of Psychiatry of Childhood and Adolescence Medical University of Vienna, Vienna, Austria Impact
Headache in children and adolescents Çiçek Wöber-Bingöl HEADACHE UNIT FOR CHILDREN AND ADOLESCENCE Dept. of Psychiatry of Childhood and Adolescence Medical University of Vienna, Vienna, Austria Impact
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Migraine in Children. Germano Falcao, MD Pediatric Neurology 03/07/2014
 Migraine in Children Germano Falcao, MD Pediatric Neurology 03/07/2014 Headaches in Children One of the most common concerns reported by children 3% for children age 3-7 years 4-11% for children age 7-11
Migraine in Children Germano Falcao, MD Pediatric Neurology 03/07/2014 Headaches in Children One of the most common concerns reported by children 3% for children age 3-7 years 4-11% for children age 7-11
Headache Assessment In Primary Eye Care
 Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
Headache Assessment In Primary Eye Care Spencer Johnson, O.D., F.A.A.O. Northeastern State University Oklahoma College of Optometry johns137@nsuok.edu Course Objectives Review headache classification Understand
What You Should Know About Your HEADACHE. Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself
 What You Should Know About Your HEADACHE Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself Introduction The purpose of this brochure is to give you a
What You Should Know About Your HEADACHE Learn more about headache types, triggers, and treatments, when to get help, and how to help yourself Introduction The purpose of this brochure is to give you a
CONCUSSIONS. Recognition, Assessment, Management, and Return to Play
 CONCUSSIONS Recognition, Assessment, Management, and Return to Play What is a concussion? A concussion is a traumatic injury to the soft tissue of the brain as a result of a violent blow. The brain tissue
CONCUSSIONS Recognition, Assessment, Management, and Return to Play What is a concussion? A concussion is a traumatic injury to the soft tissue of the brain as a result of a violent blow. The brain tissue
Understanding Migraines
 Understanding Migraines Migraine is a severe headache syndrome that recurs. Migraine headaches are usually throbbing, but may also be described as exploding, shooting, or squeezing. Migraine headaches
Understanding Migraines Migraine is a severe headache syndrome that recurs. Migraine headaches are usually throbbing, but may also be described as exploding, shooting, or squeezing. Migraine headaches
6/4/2018. Headache. Headaches. Headache. Migraine Headaches. Headache. Red Flag signs and symptoms. Imaging CT without contrast.
 Presented by M.D. Shepherd, M.D. OH MY ACHING HEAD! Estimated that one half of the adult population is affected by a headache disorder International Society Classification Primary : Tension s 40% of the
Presented by M.D. Shepherd, M.D. OH MY ACHING HEAD! Estimated that one half of the adult population is affected by a headache disorder International Society Classification Primary : Tension s 40% of the
How could I be having migraine when I don't have a headache?
 Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Migraine, Tension, and Cluster Headache: Primary Care for Primary Headaches. Jonathon M. Firnhaber, MD, FAAFP
 Migraine, Tension, and Cluster Headache: Primary Care for Primary Headaches Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Utilize evidence-based strategies to diagnose patients presenting with
Migraine, Tension, and Cluster Headache: Primary Care for Primary Headaches Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Utilize evidence-based strategies to diagnose patients presenting with
July 2012 Target Population. Adult patients 18 years or older in primary care settings.
 Guideline for Primary Care Management of Headache in Adults July 2012 Target Population Adult patients 18 years or older in primary care settings. Exclusions: This guideline does not provide recommendations
Guideline for Primary Care Management of Headache in Adults July 2012 Target Population Adult patients 18 years or older in primary care settings. Exclusions: This guideline does not provide recommendations
Concussion Update and Case Presentations
 Concussion Update and Case Presentations Cayce Onks, DO, MS, ATC Associate Professor Primary Care Sports Medicine Penn State Concussion Program Departments of Family Medicine and Orthopaedics I have no
Concussion Update and Case Presentations Cayce Onks, DO, MS, ATC Associate Professor Primary Care Sports Medicine Penn State Concussion Program Departments of Family Medicine and Orthopaedics I have no
Management of headache
 Management of headache TJ Steiner Imperial College London Based on European principles of management of common headache disorders TJ Steiner, K Paemeleire, R Jensen, D Valade, L Savi, MJA Lainez, H-C Diener,
Management of headache TJ Steiner Imperial College London Based on European principles of management of common headache disorders TJ Steiner, K Paemeleire, R Jensen, D Valade, L Savi, MJA Lainez, H-C Diener,
Craig Davidson, MD University Health Center Team Physician Department of Athletic Medicine University of Oregon
 Craig Davidson, MD University Health Center Team Physician Department of Athletic Medicine University of Oregon In the news Definition Pathophysiology Signs and symptoms Review current clinical guidelines
Craig Davidson, MD University Health Center Team Physician Department of Athletic Medicine University of Oregon In the news Definition Pathophysiology Signs and symptoms Review current clinical guidelines
June National Migraine and Headache Awareness Month
 June 2018- National Migraine and Headache Awareness Month A note from the author Hello NCP friends! This month, I wanted to feature a topic that has been much discussed amongst several of my friends and
June 2018- National Migraine and Headache Awareness Month A note from the author Hello NCP friends! This month, I wanted to feature a topic that has been much discussed amongst several of my friends and
Discussion Questions WHAT ARE SOME POSSIBLE CAUSES OF HER PAIN? WHAT ELSE WOULD YOU LIKE TO KNOW
 CLINICAL CASES Case: Ms. FM Case: Ms. FM Ms. FM is a 37-year-old school teacher Under your care for 10 years Unremarkable past history Was in minor car accident 4 months ago Has had progressive generalized
CLINICAL CASES Case: Ms. FM Case: Ms. FM Ms. FM is a 37-year-old school teacher Under your care for 10 years Unremarkable past history Was in minor car accident 4 months ago Has had progressive generalized
PAEDIATRIC ACUTE CARE GUIDELINE. Headache. This document should be read in conjunction with this DISCLAIMER
 Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children PAEDIATRIC ACUTE CARE GUIDELINE Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Dubai Standards of Care (Migraine)
") Dubai Standards of Care 2018 (Migraine) Preface Migraine is one of the most common problem dealt with in daily practice. In Dubai, the management of migraine is done through various different strategies.
Dubai Standards of Care 2018 (Migraine) Preface Migraine is one of the most common problem dealt with in daily practice. In Dubai, the management of migraine is done through various different strategies.
MIGRAINE A MYSTERY HEADACHE
 MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
Chronic Daily Headaches
 Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Chronic Daily Headaches ANWARUL HAQ, MD, MRCP(UK), FAHS DIRECTOR BAYLOR HEADACHE CENTER, DALLAS, TEXAS DISCLOSURES: None OBJECTIVES AT THE CONCLUSION OF THIS ACTIVITY, PARTICIPANTS WILL BE ABLE TO: define
Refractory Headache Challenges and Strategies. David W. Dodick, M.D. Department of Neurology Mayo Clinic Phoenix Arizona USA
 Refractory Headache Challenges and Strategies David W. Dodick, M.D. Department of Neurology Mayo Clinic Phoenix Arizona USA Headache Masters School, Tokyo 2013 Definition of refractory/intractability depends
Refractory Headache Challenges and Strategies David W. Dodick, M.D. Department of Neurology Mayo Clinic Phoenix Arizona USA Headache Masters School, Tokyo 2013 Definition of refractory/intractability depends
Disclosures. Objectives 6/2/2017
 Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Classification: Migraine and Trigeminal Autonomic Cephalalgias Lauren Doyle Strauss, DO, FAHS Assistant Professor, Child Neurology Assistant Director, Child Neurology Residency @StraussHeadache No disclosures
Common Headaches. Types and Natural Treatments
 Common Headaches Types and Natural Treatments by Heidi Fritz, MA, ND Bolton Naturopathic Clinic 64 King St W, Bolton, Ontario, L7E1C7 www.boltonnaturopathic.ca Three Common Types of Headaches Headaches
Common Headaches Types and Natural Treatments by Heidi Fritz, MA, ND Bolton Naturopathic Clinic 64 King St W, Bolton, Ontario, L7E1C7 www.boltonnaturopathic.ca Three Common Types of Headaches Headaches
Triptan Quantity Limit
 *- Florida Healthy Kids Triptan Quantity Limit Override(s) Quantity Limit Approval Duration 1 year Oral Tablets Axert (almotriptan) tablets Relpax (eletriptan) tablets 6 tablets (6.25 mg) 12 tablets (12.5
*- Florida Healthy Kids Triptan Quantity Limit Override(s) Quantity Limit Approval Duration 1 year Oral Tablets Axert (almotriptan) tablets Relpax (eletriptan) tablets 6 tablets (6.25 mg) 12 tablets (12.5
VA/DoD Clinical Practice Guideline for the Management of Concussion/mTBI
 VA/DoD Clinical Practice Guideline for the Management of Concussion/mTBI Chief, Evidence-Based Practice US Army Medical Command Clinical Program Specialist Office of Performance and Quality Improvement
VA/DoD Clinical Practice Guideline for the Management of Concussion/mTBI Chief, Evidence-Based Practice US Army Medical Command Clinical Program Specialist Office of Performance and Quality Improvement
Lost in Translation: Making Sense of Clinical Treatment Guidelines
 Lost in Translation: Making Sense of Clinical Treatment Guidelines Charles E. Argoff, MD, CPE Disclosures: Charles Argoff Financial Disclosure: Consultant: Teva, Daiichi Sakyo, Pfizer, Nektar, Purdue,
Lost in Translation: Making Sense of Clinical Treatment Guidelines Charles E. Argoff, MD, CPE Disclosures: Charles Argoff Financial Disclosure: Consultant: Teva, Daiichi Sakyo, Pfizer, Nektar, Purdue,
Primary Care Adult Headache Management Pathway (formerly North West Headache Management Guideline for Adults) Version 1.0
 Version 1.0") Primary Care Adult Headache Management Pathway (formerly rth West Headache Management Guideline for Adults) Version 1.0 1 VERSION CONTROL Version Date Amendments made Version 1.0 October 2018 Reformatted
Primary Care Adult Headache Management Pathway (formerly rth West Headache Management Guideline for Adults) Version 1.0 1 VERSION CONTROL Version Date Amendments made Version 1.0 October 2018 Reformatted
PHARMACY COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 5/18/17 SECTION: DRUGS LAST REVIEW DATE: 5/17/18 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 ALLZITAL (butalbital and acetaminophen) 25 mg/325 mg oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
ALLZITAL (butalbital and acetaminophen) 25 mg/325 mg oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
Migraine Treatment What you need to know
 Migraine Treatment What you need to know DR NICOLE LIMBERG ST ANDREWS PLACE SPRING HILL www.migrainespecialist.com.au Migraine what is it? Primary neurobiological condition Waves of reduced brain activity
Migraine Treatment What you need to know DR NICOLE LIMBERG ST ANDREWS PLACE SPRING HILL www.migrainespecialist.com.au Migraine what is it? Primary neurobiological condition Waves of reduced brain activity
2008 Migraine Update Migraine Update Migraine Update. Epidemiology. Yousef Mohammad MD., MSc. Epidemiology
 2008 Migraine Update Yousef Mohammad MD., MSc Assistant Professor of Neurology Ohio State University Medical Center 2008 Migraine Update Epidemiology 2008 Migraine Update Epidemiology Abortive Treatment
2008 Migraine Update Yousef Mohammad MD., MSc Assistant Professor of Neurology Ohio State University Medical Center 2008 Migraine Update Epidemiology 2008 Migraine Update Epidemiology Abortive Treatment
Disclosures. Objectives 6/20/2018. No disclosures. Tools & Tips for Headache Management in Special Populations: The Young & Old, Pregnant & Lactating
 Tools & Tips for Headache Management in Special Populations: The Young & Old, Pregnant & Lactating Lauren Doyle Strauss, DO, FAHS Child Neurology Residency Director @StraussHeadache No disclosures Disclosures
Tools & Tips for Headache Management in Special Populations: The Young & Old, Pregnant & Lactating Lauren Doyle Strauss, DO, FAHS Child Neurology Residency Director @StraussHeadache No disclosures Disclosures
Reflections on NICE Headache Guideline. Dr Kay Kennis GPwSI in Headache, Bradford
 Reflections on NICE Headache Guideline Dr Kay Kennis GPwSI in Headache, Bradford Overview The process of guideline development illustrated with the headache guideline Reflections on the process Key recommendations
Reflections on NICE Headache Guideline Dr Kay Kennis GPwSI in Headache, Bradford Overview The process of guideline development illustrated with the headache guideline Reflections on the process Key recommendations
Treatment of Headache in the ED
 Treatment of Headache in the ED Benjamin W. Friedman, MD, MS, FAAEM Associate professor of Emergency Medicine Albert Einstein College of Medicine Montefiore Medical Center Disclosure Topics of Discussion
Treatment of Headache in the ED Benjamin W. Friedman, MD, MS, FAAEM Associate professor of Emergency Medicine Albert Einstein College of Medicine Montefiore Medical Center Disclosure Topics of Discussion
Subject: CGRP Inhibitors
 ARCHIVED (NOT ACTIVE RETIRED) Archived: 08/01/18 09-J2000-98 Original Effective Date: 06/15/18 Reviewed: 05/09/18 Revised: 08/01/18 Next Review: ARCHIVED (NOT ACTIVE RETIRED) Subject: CGRP Inhibitors THIS
ARCHIVED (NOT ACTIVE RETIRED) Archived: 08/01/18 09-J2000-98 Original Effective Date: 06/15/18 Reviewed: 05/09/18 Revised: 08/01/18 Next Review: ARCHIVED (NOT ACTIVE RETIRED) Subject: CGRP Inhibitors THIS
Headaches. Mini Medical School. November 10, A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology)
 Assistant Professor Department of Medicine (Neurology)") Headaches. Mini Medical School. November 10, 2016 A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology) Artist Agnes Cecile Disclosures I have received an honorarium from
Headaches. Mini Medical School. November 10, 2016 A. Laine Green MSc, MD FRCP(C) Assistant Professor Department of Medicine (Neurology) Artist Agnes Cecile Disclosures I have received an honorarium from
Chronic Migraine in Primary Care. December 11 th, 2017 Werner J. Becker University of Calgary
 Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
Chronic Migraine in Primary Care December 11 th, 2017 Werner J. Becker University of Calgary Disclosures Faculty: Werner J. Becker Relationships with commercial interests: Grants/Research Support: Clinical
SPRINGFIELD CLINIC S
 SPRINGFIELD CLINIC S HEAD INJURY MANAGEMENT GUIDE FOR PARENTS Given the complexities of concussion management, Springfield Clinic recognizes the importance of managing concussions on an individualized
SPRINGFIELD CLINIC S HEAD INJURY MANAGEMENT GUIDE FOR PARENTS Given the complexities of concussion management, Springfield Clinic recognizes the importance of managing concussions on an individualized
Kristin s Head Trauma Board Questions 11/07/14
 Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Kristin s Head Trauma Board Questions { 11/07/14 A healthy 15 y/o boy was playing football at a park near his home with a group of friends when he tripped over a friend s leg while trying to catch a pass.
Short Clinical Guidelines: Headache, Key Points for Diagnosis and Treatment
 Clinical Highlights 1. Headache is diagnosed by history and physical examination with limited need for imaging or laboratory tests. 2. Warning signs of possible disorder other than primary headache are:
Clinical Highlights 1. Headache is diagnosed by history and physical examination with limited need for imaging or laboratory tests. 2. Warning signs of possible disorder other than primary headache are: