Peripheral Arterial Disease
|
|
|
- Hannah Morgan
- 5 years ago
- Views:
Transcription

1 Peripheral Arterial Disease Presentation Prevention Treatment Cardiovascular and Stroke Summit 1 June 2018 Mary MacDonald CD MD PhD FRCSC RPVI Vascular Surgeon Thunder Bay Regional Health Sciences Centre Assistant Professor Northern Ontario School of Medicine

2 Faculty/Presenter Disclosure Faculty: Dr. Mary MacDonald Relationships with commercial interests: none
3 Disclosure of Commercial Support Dr. Mary MacDonald, Vascular Surgeon, TBRHSC This program has received no financial or in-kind support Potential for conflict(s) of interest: I have no conflict of interest or affiliations that have influenced this presentation to disclose
4 Objectives 1. Review presentation of peripheral arterial disease 2. Evidence based prevention and risk factor management 3. Treatment options: indications for angiography and surgical bypass
5 Overview Chronic Peripheral Arterial Disease Presentation of PAD Prevention and Management of Risk Factors Guidelines for Treatment of Claudication Guidelines for Treatment of Critical Limb Ischemia Guidelines for Management of Diabetic Foot Ulcer Treatment: Indications for intervention
6 What is Peripheral Arterial Disease? Stenosis or occlusion of the aorta or limb arteries which leads to lack of tissue oxygenation (ischemia) Acute PAD most often caused by embolization Chronic PAD most often by atherosclerosis Either acute or chronic peripheral arterial disease can lead to death of tissues (nerve, muscle, bone) and loss of the limb

7 Peripheral Arterial Disease
8 Population (millions) The Aging Population 17% of the population years of age has PAD Age (years) N=1592 PAD = peripheral arterial disease Fowkes FG, et al. Int J Epidemiol. 1991;20:
9 Independent Risk Factors for PAD* Relative Risk vs the General Population Reduced Increased Diabetes 4.05 Smoking 2.55 Hypertension Total cholesterol (10 mg/dl) * PAD diagnosis based on ABI <0.90. Newman AB, et al. Circulation. 1993;88:

10 Chronic Peripheral Arterial Disease
11 Causes of Chronic Peripheral Arterial Ischemia Popliteal Entrapment Syndrome Popliteal Adventitial Cyst 5% 85% Atherosclerosis 10% Popliteal Aneurysm Thromboangiitis Obliterans (Buerger s disease) Arteritis Fibromuscular Dysplasia

12 Atherosclerosis

13 Atherosclerosis Risk Factors
 Ankle systolic")


14 The Ankle-Brachial Index (ABI) Ankle systolic pressure Brachial systolic pressure Ankle pressure from Posterior Tibial and Dorsalis Pedis use highest
15 Chronic Peripheral Arterial Disease Clinical Ankle Brachial Index Normal ABI is 1.0 intermittent claudication <0.7 rest pain <0.5 tissue loss ulcers, gangrene <0.3
16 Critical Limb Ischemia Peripheral Arterial Disease w/ inadequate tissue oxygenation even at rest Rubor Rest Pain Tissue Loss ulcers, gangrene, infection
17 Chronic Peripheral Arterial Disease -- Natural History Of patients age 50 and older with PAD, only 1-2% will go on to develop critical limb ischemia but in patients who develop critical limb ischemia, after 1 year only 50% will be alive with both lower limbs
18 Case: Belinda B Belinda is a 70 year old who presents with intermittent, reproducible bilateral calf pain at 3 blocks (5-10 minutes). Symptoms have been present for approximately 6 months. She denies pain in her toes or feet at night There has been no tissue loss She has had no prior vascular interventions
19 Case: Belinda B What is your next action? A. Order a CT Angiogram B. Refer for conventional angiogram +/- angioplasty C. Start ASA, statin, and a walking program D. Do an ABI in the office
20 Clinical Presentation of PAD Initial PAD Presentation Asymptomatic PAD 20-50% Symptomatic PAD Atypical Leg Pain 40-50% Intermittent Claudication 10-35% Critical Limb Ischemia 1-2% Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Accessed December 13, 2005.


21 Natural History of Claudication
22 Natural History of PAD: 5-year Outcomes Limb Morbidity Cardiovascular Morbidity and Mortality Stable Claudication70-80% Worsening Claudication10-20% Nonfatal CV Events 15-30% Mortality 15-30% Critical Limb Ischemia 1-2 % CV Causes 75% Non-CV Causes 25%
23 Fate of Patients With Critical Limb Ischemia After Initial Treatment Alive With Amputation 35% Dead 20% Alive Without Amputation 45% Summary of 19 studies on 6-month outcomes 5 year outcomes show increased mortality due to cardiovascular causes Dormandy JA, et al. J Vasc Surg. 2000;31:S1-S296.
24 Chronic Peripheral Arterial Disease Management Medical management: Risk factor modification Antiplatelet Statin Revascularization Open surgery: Endarterectomy Bypass anatomic extraanatomic Endovascular: Angioplasty transluminal subintimal Stent Other (Atherectomy, Cryoplasty)
25 Therapy of Intermittent Claudication: Magnitude of Functional Improvement Pentoxifylline (Trental) Cilostazol * antiplatelet not avail in Canada Supervised Exercise Improvement Over Baseline After 90 to 180 Days (%) Gardner AW, Poehlman ET. JAMA. 1995;274: ; Girolami B, et al. Arch Intern Med. 1999;159: Hiatt WR. N Engl J Med. 2001; 344;
26 Change in Treadmill Walking Distance (%) Effects of Exercise Training on Claudication Meta-analysis of 21 Studies Exercise Training Control Onset of Claudication Pain Gardner AW, Poehlman ET. JAMA. 1995;274: Maximal Claudication Pain
27 Intermittent Claudication: Exercise Therapy Frequency: 3-5 supervised sessions/week Duration: 35 to 50 minutes of exercise/session Type of exercise: treadmill or track walking to near-maximal claudication pain Length: 6 months or more Results: 100%-150% improvement in maximal walking distance Improvement in quality of life Stewart KJ, et al. N Eng J Med. 2002;347:
28 Goals in Treating Patients With PAD Limb Outcomes Outcomes in Cardiovascular Morbidity and Mortality Improve ability to walk Increase walking distance Improvement in QOL Decrease mortality from MI, stroke, and cardiovascular death Decrease nonfatal MI and stroke Prevent progression to critical limb ischemia and amputation
29 2015 SVS Guidelines for the Management of Peripheral Arterial Disease Diagnosis
30 Diagnosis of PAD: The Ankle- Brachial Index Use ABI first to establish lower extremity PAD diagnosis Recommend against routine screening in the absence of symptoms or risk factors Use toe-brachial index in patients with non-compressible vessels Anatomic imaging if revascularization is being considered Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Accessed December 13, 2005.
31 2015 SVS Guidelines for the Management of Peripheral Arterial Disease Risk Factor Management
32 Risk Factor Management: Asymptomatic Patient 1A Comprehensive Smoking Cessation intervention(s) 1C Educate re S&S of PAD progression 1C Recommend against invasive treatment in the absence of symptoms Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Accessed December 13, 2005.
33 Risk Factor Management: Symptomatic Patient 1A Comprehensive Smoking Cessation intervention(s) 1A Statin therapy 1A ASA 81 mg PO OD 1B optimal diabetes control 1B B-blocker use as indicated 1B Plavix if ASA not tolerated
34 Risk Factor Management: Smoking Cessation Patient should discontinue use of cigarettes or other forms of tobacco Offer comprehensive smoking cessation interventions Behavior modification therapy, nicotine replacement therapy, and/or bupropion Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at
35 2015 SVS Guidelines for the Management of Peripheral Arterial Disease Treatment for Claudication
36 Claudication Treatment: Exercise Supervised exercise training should be the initial treatment minute sessions 3 or more times per week At least 12 weeks Value of unsupervised exercise programs is not well established Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Accessed December 13, 2005.
37 Claudication Treatment: Endovascular or Surgical Therapies Indicated only for patients with Vocational or lifestyle-limiting disability; Reasonable likelihood of symptomatic improvement; Prior failure of exercise therapy or pharmacological therapy; and Favorable risk-benefit ratio Not indicated as a prophylactic treatment for asymptomatic patients 1A Optimal Medical Management postintervention (Smoking cessation, ASA, Statin, glycemic and HTN control) Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Accessed December 13, 2005.
38 PAD Indications for Intervention Persistent, lifestyle limiting claudication despite maximal medical therapy Rest pain Nonhealing ulcer Gangrene
39 Case: Belinda B Belinda is a 70 year old who presents with intermittent, reproducible bilateral calf pain at 3 blocks (5-10 minutes). Symptoms have been present for approximately 6 months. She denies pain in her toes or feet at night There has been no tissue loss She has had no prior vascular interventions
40 Case: Belinda B What is your next action? A. Order a CT Angiogram B. Refer for conventional angiogram +/- angioplasty C. Start ASA, statin, and a walking program D. Do an ABI in the office
41 Case: Clive C 78 year old man brought to clinic by his daughters, who describe progressive loss of mobility. At camp last summer, Clive could walk for at least 30 min, but now complains of severe pain in his left calf when walking to the mailbox (100m) and left foot pain that wakes him at night. PMHx: CAD with stents 10 yrs ago, HTN, ex-smoker. Not taking any medication. No prior leg-related complaints. On examination of the left leg he has dependent rubor without tissue loss in the left foot and no palpable pulses in either groin or the distal left leg.

42 Case 3: Clive C
43 Case: Clive C Initial management options: A. Give him a prescription for aspirin and tell him to walk it out -- reassess in a few months B. Start aspirin, a statin and an ACE Inhibitor and arrange an outpatient CT angiogram C. Admit him to hospital and continue the workup as an inpatient D. Start a heparin infusion and take him to the OR

44 Chronic Peripheral Arterial Insufficiency Clinical Ankle Brachial Index Normal ABI is 1.0 intermittent claudication <0.7 rest pain <0.5 tissue loss ulcers, gangrene <0.3


45 Rubor Tissue Loss


46 Major Tissue Loss
47 Selection of Treatment Acute or Chronic? Critical/Limb-threatening? Level, extent and severity of lesion(s)
48 Surgical Revascularization for Peripheral Arterial Disease Endarterectomy Bypass anatomic extra-anatomic autogenous (vein) or nonautogenous graft (Dacron, PTFE)
49 Peripheral Arterial Disease Endovascular Treatment Endovascular: Angioplasty Stent Other transluminal subintimal (Atherectomy, Cryoplasty)
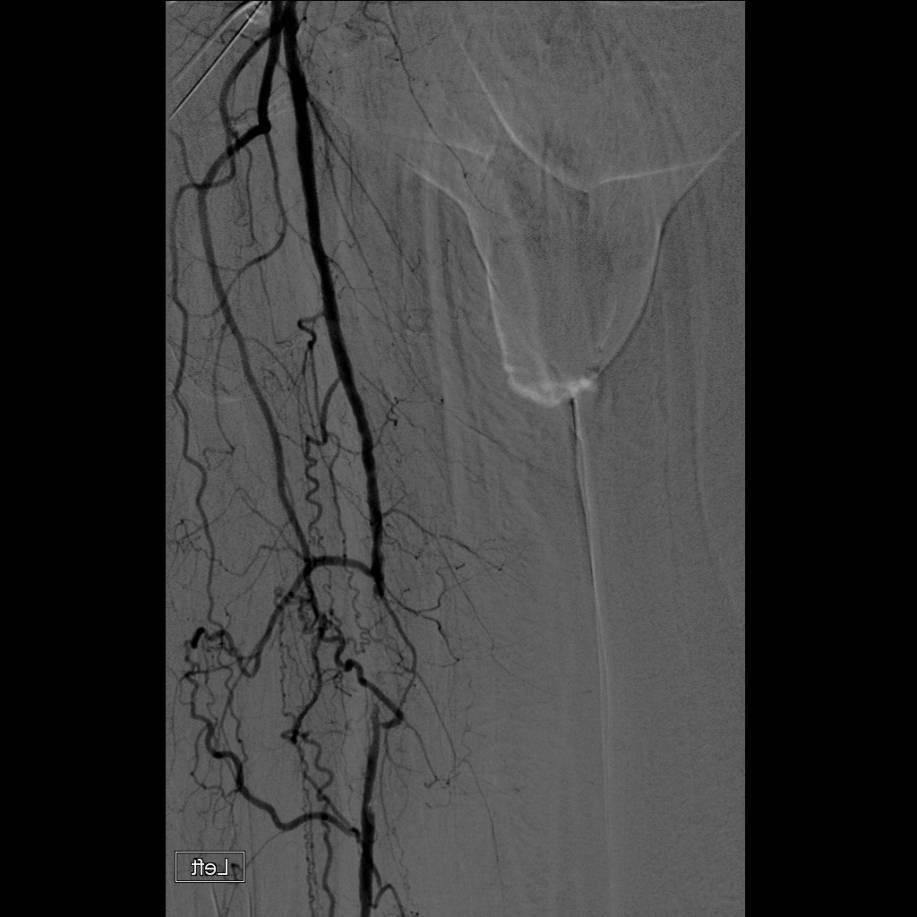
50 Superficial Femoral Artery Occlusion

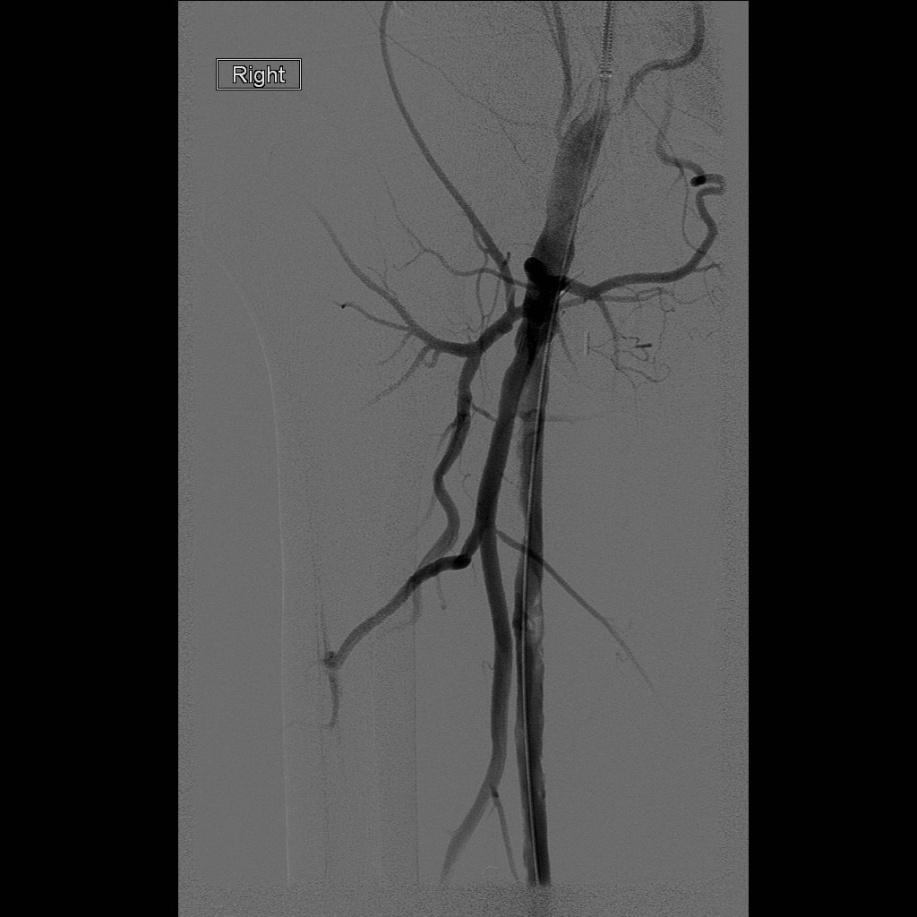
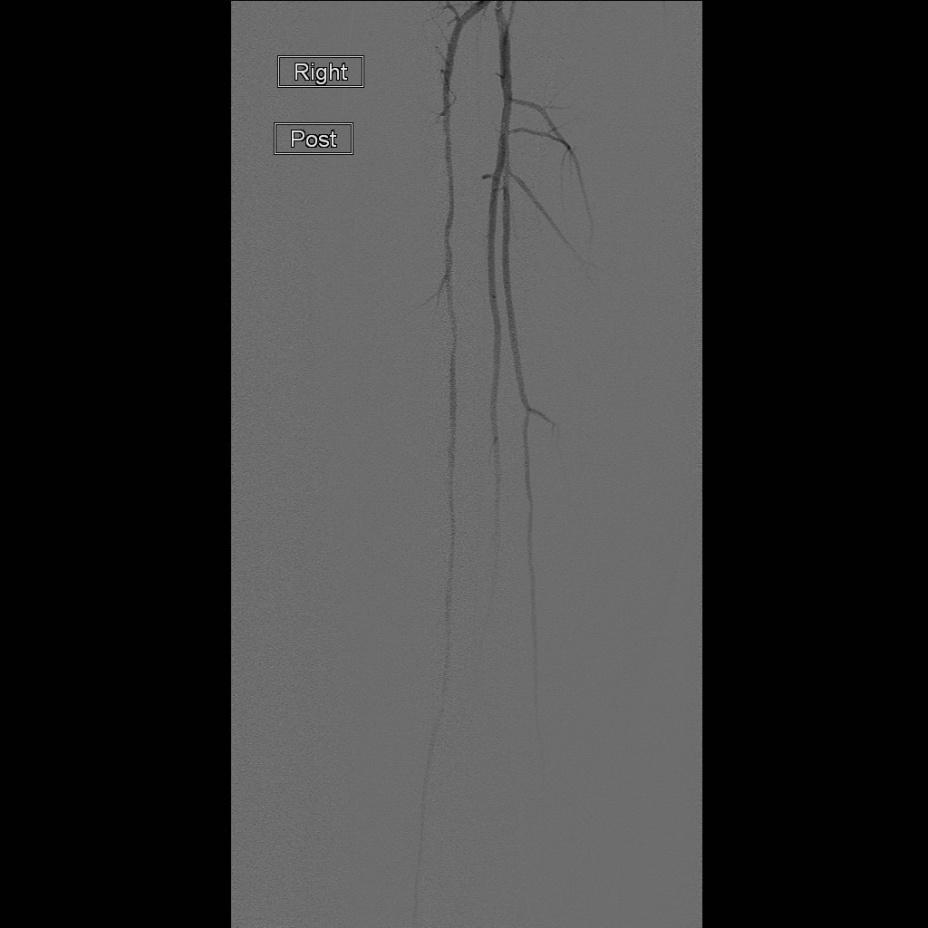
51 Superficial Femoral Artery Angioplasty
52 Stent Deployment :// R7XUnvs

53 Surgical Bypass


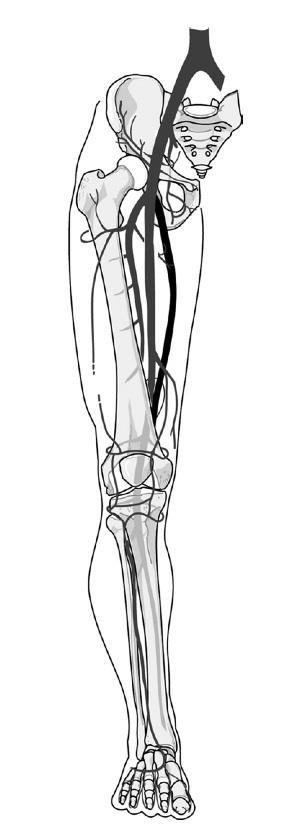
54 Open Anatomic Bypass with Saphenous Vein Graft Popliteal-popliteal bypass with saphenous vein graft
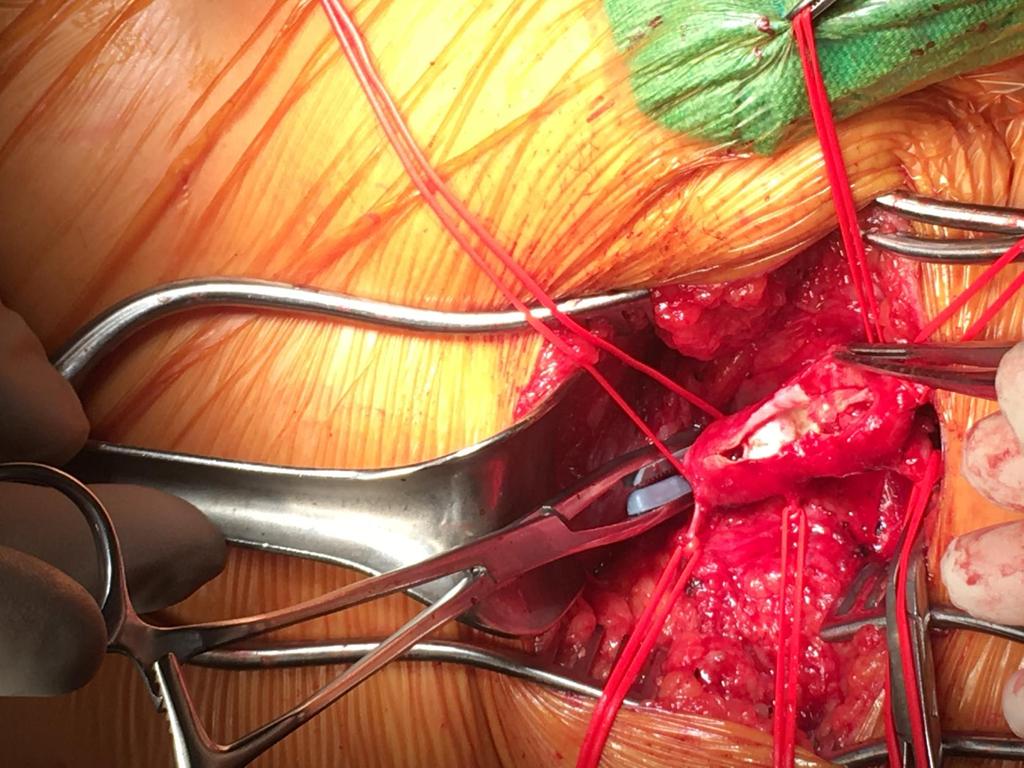
55 Femoral Endarterectomy
56 Postintervention Surveillance 2C Clinical surveillance program to include interval history, ABI, Duplex scanning (for vein grafts), and 1C prophylactic reintervention for graft stenosis to promote long-term bypass patency
57 Case: Clive C 78 year old man with dependent rubor, left foot pain at night and no pulses in the groins or left leg. A. Give him a prescription for aspirin and tell him to walk it out -- reassess in a few months B. Start aspirin, a statin and an ACE Inhibitor and arrange an outpatient CT angiogram C. Admit him to hospital and continue the workup D. Start a heparin infusion and take him to the OR
58 Management of Peripheral Arterial Disease -- Summary Asymptomatic: CV Risk Factor Management Claudication: CV RF Mgt + Walking Program Consider Revascularization if disabling Critical Limb Ischemia: CV Risk Factor Management + Revascularization



59 Wound Healing after Revascularization


60 Ischemia and Diabetes
61 Risk Factor Management: Diabetes Therapies Encourage proper foot care Appropriate footwear, chiropody/podiatric medicine, daily foot inspection, skin cleansing, and topical moisturizing creams Urgently address skin lesions and ulcerations Target Hb A1C <7% to reduce microvascular complications and potentially improve cardiovascular outcomes Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Accessed December 13, 2005.
62 Diabetic Foot Ulcer/Infection NEUROPATHY + ISCHEMIA = INFECTION 20-40% of healthcare resources spent on diabetes are related to diabetic feet 7-10% annual incidence ulcer formation if NO confounders 25-30% annual incidence if PAD, Charcot foot, prior ulcers or amputation
63 Diabetic Foot Ulcer/Infection 5-8% of patients with new ulcers require major amputation within a year Ischemia should be considered as a cause of DFU unless proven absent Neuroischemic and ischemic lesions should be considered together as both may require revascularization
64 Diabetic Foot Ulcer/Infection As intermittent claudication and rest pain are reported far less commonly in diabetics with ischemia compared to non-diabetics; early non-invasive vascular evaluation (ABI) recommended for patients with poor ulcer healing and a high risk for amputation; IWG for the Diabetic Foot recommends vascular studies if the DFU has not healed in 6 weeks even if initial diagnostics suggest only mild disease
65 Diabetic Foot Ulcer/Infection 2B Surgical intervention for moderate or severe infections is likely to decrease the risk of major amputation 2B open, endovascular or hybrid methods should be chosen depending on patient comorbidities, anatomy of the arterial lesion(s) and expertise of the centre 1A Negative-pressure wound therapy appears to be as, or more, effective than other local wound treatments in patients without significant infection
66 Summary: Peripheral Arterial Disease Chronic Limb Ischemia: clinical presentation, risk factors, medical, surgical and endovascular management Guidelines for care of Diabetic Foot Ulcers Acute Limb Ischemia: clinical presentation and treatment
67 Barriers to Practice Change Discussion What is the most prevalent barrier to change that you see in your practice? What can vascular surgery do to mitigate this barrier?
68 Rapid Access to Vascular Evaluation RAVE clinic weekly at TBRHSC we intend to expand clinic frequency, resources Rapid referral and assessment for patients with tissue loss and suspected vascular disease No imaging required we will arrange Fax referrals to (office)
69
70 References Cronenwett and Johnston (2012). Rutherford s Vascular Surgery 7 th ed, Elsevier, Philadelphia PA Dormandy JA, et al. J Vasc Surg. 2000;31:S1-S296. Fowkes FG, et al. Int J Epidemiol. 1991;20: Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Newman AB, et al. Circulation. 1993;88: Norgren et al., (2007). Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). JVS 45:1(S) 1A-65A. Pomposelli et al Society for Vascular Surgery Clinical Guidelines for Management of Peripheral Arterial Insufficiency JVS 66:3(S) Dec 2015 Schneider, PA (2009). Endovascular Skills: Guidewire and catheter skills for endovascular surgery 3 rd ed Informa, New York NY. Zarins and Gewertz (2005). Atlas of Vascular Surgery 2 nd ed, Elsevier, Philadelphia PA
71 Questions?
72


73 Acute limb ischemia
74 Case: Eric E 58 year old man presents to ED with 4 hours of right foot pain which woke him from sleep. The foot is pale, with no palpable pulses or Doppler signal. He now also has motor weakness at the ankle and toes, and numbness from the mid-shin down to the toes. He is a 1 PPD smoker with hypertension. He is otherwise healthy and has had no previous problems with either leg.
75 Case: Eric E Initial management options: A. Give the patient aspirin and get him to walk it out -- reassess in an hour B. Start a heparin infusion and obtain a CT scan C. Start a heparin infusion and obtain an urgent conventional angiogram (diagnostic, possibly therapeutic) D. Start a heparin infusion and take the patient to the Operating Room
76 Causes of Acute Limb Ischemia Acute limb ischemia is usually embolic -- a blood clot forms elsewhere in the body and travels to the limb Most (85%) emboli come from the heart; the remainder originate in proximal arteries (especially if these arteries are aneurysmal) Non embolic causes: thrombosis, dissection, trauma (including iatrogenic)

77 Cardiac Embolization Acute limb ischemia like a stroke, but for your leg
78 Clinical Presentation of Acute Limb Ischemia Acute limb ischemia: pain, progressive loss of motor and sensory function, diminished or absent pulses Clinical examination +/- imaging localize the level of occlusion Acute occlusion of a major artery is not well tolerated as there is little collateral flow, and the tissues will not typically survive longer than 4-6 hours
79 Rutherford Classification Clinical Presentation of Acute Limb Ischemia Sensory Motor Doppler Arterial Venous I Normal Normal Normal Audible IIa Toes only/ Normal Diminished Audible No change IIb Pain/ Weak Poor/no Audible sens loss III Pain/ No/Rigor None None insensate
80 Acute Limb Ischemia -- Treatment 1. Embolectomy 2. Thrombolysis IF the limb is viable, heparin infusion and catheter-directed TPA may be appropriate

81 Femoral Embolectomy for Acute Limb Ischemia Incision and exposure Proximal and distal control Transverse arteriotomy Embolectomy with Fogarty catheter of 1-3 vessels On-table angio if poor result Closure

82 Acute Ischemia: Embolus


83 Pre and Post Embolectomy
84 Case: Eric E 58 year old man presents acutely to ED with a pale, pulseless right foot, with progressive sensory and motor changes A. Give the patient aspirin and get him to walk it out - - reassess in an hour B. Start a heparin infusion and obtain a CT scan C. Start a heparin infusion and obtain an angiogram D. Start a heparin infusion and take the patient to the Operating Room
85
86 Classification of Recommendations Class I: Evidence and/or general agreement that procedure or treatment is beneficial, useful, and effective Class II: Conflicting evidence and/or divergence of opinion about usefulness or efficacy of a procedure or treatment Class IIa: Weight of evidence or opinion favors usefulness or efficacy Class IIb: Usefulness or efficacy is less well established by evidence or opinion Class III: Evidence and/or general agreement that procedure is not useful or effective and in some cases Hirsch AT, Haskal ZJ, may Hertzer NR, be et al. Available harmful at Accessed December 13, 2005.
87 Classification of Recommendations Class I: Evidence and/or general agreement that procedure or treatment is beneficial, useful, and effective Class II: Conflicting evidence and/or divergence of opinion about usefulness or efficacy of a procedure or treatment Class IIa: Weight of evidence or opinion favors usefulness or efficacy Class IIb: Usefulness or efficacy is less well established by evidence or opinion Class III: Evidence and/or general agreement that procedure is not useful or effective and in some cases Hirsch AT, Haskal ZJ, may Hertzer NR, be et al. Available harmful at Accessed December 13, 2005.
88 Peripheral Arterial Disease Aneurysms Rupture, thrombosis, embolization or mass effect Risk of rupture increases with size of aneurysm Treatment involves exclusion of the entire aneurysm sac with preservation of vascular supply to branch vessels and end organs Aneurysm thrombus may embolize distally, causing acute or chronic limb ischemia
89 Endovascular Complications Dissection: intimal tear +/- propagation, arterial occlusion Perforation: 1-3%, tx usually conservative Embolization: 3-5% distal embolization of which approx half is clinically significant. Anticoagulate early and minimize traversal of lesion(s) Access Site: Groin Hematoma Retroperitoneal Hematoma Pseudoaneurysm AV Fistula Axillary/Brachial Nerve Injury Axillary/Brachial Thrombosis Closure Device Complications Ischemic Infectious (EVAR % with 18-50% mortality)
90 Evidence Based Guidelines for Management of PAD ACC/AHA/TASC Guidelines for Treatment -- Class I Evaluate and treat conditions known to increase risk for primary amputation Onset of acute limb symptoms in an at-risk patient should be evaluated by a specialist in vascular disease Specialized wound care for skin breakdown Patients with CLI should be evaluated at least twice yearly by a specialist in vascular disease Evaluate patients with evidence of embolization for aneurysmal disease Hirsch et al 2005 Consensus Guidelines
91 Critical Limb Ischemia -- Evidence Based Guidelines ACC/AHA/TASC Guidelines for Treatment -- Class I Preop cardiac risk stratification prior to open repair Prompt antibiotics in patients with skin ulceration or evidence of limb infection Catheter-based thrombolysis for acute limb ischemia (class I or IIa) of less than 14 days duration Address inflow lesion(s) first in combined disease, then revascularize outflow for persistent symptoms or infection If there is uncertainty regarding inflow disease, measure intraarterial pressures before and after vasodilator administration Hirsch et al 2005 Consensus Guidelines
 stroke, trauma or neurosurgery known intracranial neoplasm uncontrollable coagulopathy or hypertension, known allergic reaction Relative -- moderate risk")
92 Thrombolysis Contraindications Absolute existing,very recent or high risk hemorrhage true allergy ie. active internal bleeding, recent (2 months) stroke, trauma or neurosurgery known intracranial neoplasm uncontrollable coagulopathy or hypertension, known allergic reaction Relative -- moderate risk for bleeding (recent biopsy, obstetric, GI surgery or bleeding, trauma, endocarditis, pancreatitis); severe renal or hepatic failure Peripheral artery thrombolysis led to significant hemorrhage in 5.7% (STILE) to 13% (TOPAS) of patients
93 Thrombolysis Complications Hemorrhagic -- local up to 25%, intracerebral 1-2% Antigenic -less than 0.01% with TPA Catheter-related -- up to 3% Embolic -- distal limb 9 to 13%, of which most (75%+) may be treated by advancing the catheter and continuing the infusion post DVT PE up to 10%, not all clinically significant
94 Thrombolytic Treatment of Critical Limb Ischemia Catheter-based thrombolysis is effective and beneficial for patients with Rutherford category I-IIa acute limb ischemia of less than 14 days duration Mechanical thrombectomy can be used as an adjunctive therapy for acute limb ischemia Catheter-based thrombolysis or thrombectomy may be considered for Rutherford category IIb acute limb ischemia of more than 14 days duration Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Accessed December 13, 2005.
95 Thrombolytic Treatment of Critical Limb Ischemia Catheter-based thrombolysis is effective and beneficial for patients with Rutherford category I-IIa acute limb ischemia of less than 14 days duration Mechanical thrombectomy can be used as an adjunctive therapy for acute limb ischemia Catheter-based thrombolysis or thrombectomy may be considered for Rutherford category IIb acute limb ischemia of more than 14 days duration Hirsch AT, Haskal ZJ, Hertzer NR, et al. Available at Accessed December 13, 2005.
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
John E. Campbell, MD. Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014
 PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
Treatment Strategies For Patients with Peripheral Artery Disease
 Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Peripheral Vascular Disease
 Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Objectives. Abdominal Aortic Aneuryms 11/16/2017. The Vascular Patient: Diagnosis and Conservative Treatment
 The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
Intended Learning Outcomes
 2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
2011 Acute Limb Ischemia Definition, Etiology & Pathophysiology Clinical Evaluation Management Ali SABBOUR Prof. of Vascular Surgery, Ain Shams University Acute Limb Ischemia Intended Learning Outcomes
Introduction to Peripheral Arterial Disease. Stacey Clegg, MD Interventional Cardiology August
 Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Peripheral Arterial Disease Extremity
 Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Guidelines for Management of Peripheral Arterial Disease
 Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
Introduction What Causes Peripheral Vascular Disease? How Do Doctors Treat Peripheral Vascular Disease?... 9
 Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
Patient Information Table of Contents Introduction... 3 What is Peripheral Vascular Disease?... 5 What Are Some of the Symptoms of Peripheral Vascular Disease?... 7 What Causes Peripheral Vascular Disease?...
National Vascular Registry
 National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
Resident Teaching Conference 3/12/2010
 Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
Algorithm for Managing Acute Lower Extremity Ischemia. Peter A. Schneider, MD Honolulu, Hawaii
 Algorithm for Managing Acute Lower Extremity Ischemia Peter A. Schneider, MD Honolulu, Hawaii Disclosure Peter A. Schneider, MD... I have the following potential conflicts of interest to report: Consulting:
Algorithm for Managing Acute Lower Extremity Ischemia Peter A. Schneider, MD Honolulu, Hawaii Disclosure Peter A. Schneider, MD... I have the following potential conflicts of interest to report: Consulting:
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Introduction 3. What is Peripheral Vascular Disease? 5. What Are Some of the Symptoms of Peripheral Vascular Disease? 6
 Patient Information Table of Contents Introduction 3 What is Peripheral Vascular Disease? 5 What Are Some of the Symptoms of Peripheral Vascular Disease? 6 What Causes Peripheral Vascular Disease? 7 How
Patient Information Table of Contents Introduction 3 What is Peripheral Vascular Disease? 5 What Are Some of the Symptoms of Peripheral Vascular Disease? 6 What Causes Peripheral Vascular Disease? 7 How
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
Evidence-Based Optimal Treatment for SFA Disease
 Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease
 Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Limb Salvage in Diabetic Ischemic Foot. Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017
 Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Garland Green, MD Interventional Cardiologist. Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management
 Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment
: Presentation, Diagnosis, and Treatment") Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment Prepared and Presented by Jon Manocchio, Pharm D Blanchard Valley Hospital October 2011 Introduction PAD is a condition that is
Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment Prepared and Presented by Jon Manocchio, Pharm D Blanchard Valley Hospital October 2011 Introduction PAD is a condition that is
Critical Limb Ischemia A Collaborative Approach to Patient Care. Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017
 Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Lower Extremity Arterial Disease
 Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC
 Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA. Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE
 PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital
 Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
SAFETY AND EFFECTIVENESS OF ENDOVASCULAR REVASCULARIZATION FOR PERIPHERAL ARTERIAL OCCLUSIONS
 SAFETY AND EFFECTIVENESS OF ENDOVASCULAR REVASCULARIZATION FOR PERIPHERAL ARTERIAL OCCLUSIONS LIBBY WATCH, MD MIAMI VASCULAR SPECIALISTS MIAMI CARDIAC & VASCULAR INSTITUTE FINANCIAL DISCLOSURES None 2
SAFETY AND EFFECTIVENESS OF ENDOVASCULAR REVASCULARIZATION FOR PERIPHERAL ARTERIAL OCCLUSIONS LIBBY WATCH, MD MIAMI VASCULAR SPECIALISTS MIAMI CARDIAC & VASCULAR INSTITUTE FINANCIAL DISCLOSURES None 2
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Case Discussion. Disclosures. Critical Limb Ischemia: A Selective Approach to Revascularization Works Best 4/28/2012. None. 58 yo M, DM, CAD, HTN
 Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2)
") Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Patient Information. Peripheral Arterial Disease and the Lutonix 035 Balloon. Advancing Lives and the Delivery of Health Care
 Patient Information Peripheral Arterial Disease and the Lutonix 035 Balloon Advancing Lives and the Delivery of Health Care Contents Peripheral Arterial Disease (PAD) Peripheral Arterial Disease (PAD)
Patient Information Peripheral Arterial Disease and the Lutonix 035 Balloon Advancing Lives and the Delivery of Health Care Contents Peripheral Arterial Disease (PAD) Peripheral Arterial Disease (PAD)
Patient Brochure. Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland. PK Rev. 0 05/17
 Patient Brochure Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland PK1411100 Rev. 0 05/17 LIFESTREAM Patient Brochure If you or a member of your family has been diagnosed with
Patient Brochure Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland PK1411100 Rev. 0 05/17 LIFESTREAM Patient Brochure If you or a member of your family has been diagnosed with
How to manage leg ulcers in the elderly
 How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
Social History. Retired internist 2 scotches a day 50 pack-year history, stopped in 2005
 April 17, 2008 HPI 78 year old internist complains of 10 days of tingling and discomfort in left toes Unable to walk or sleep due to severe pain Pain worse with movement Redness in left toes Bilateral
April 17, 2008 HPI 78 year old internist complains of 10 days of tingling and discomfort in left toes Unable to walk or sleep due to severe pain Pain worse with movement Redness in left toes Bilateral
National Clinical Conference 2018 Baltimore, MD
 National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
Peripheral Arterial Disease: Objectives. Disclosure. Definition: Peripheral Arterial Disease (PAD)
") Geriatric Grand Rounds Tuesday, April 21, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 21, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Endovascular Repair o Abdominal. Aortic Aneurysms. Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida
 Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
Endovascular Repair o Abdominal Aortic Aneurysms Cesar E. Mendoza, M.D. Jackson Memorial Hospital Miami, Florida Disclosure Nothing to disclose. 2 Mr. X AAA Mr. X. Is a 70 year old male who presented to
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome
 Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Peripheral Arterial Disease. Westley Smith MD Vascular Fellow
 Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS
 Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
CRITICAL LIMB ISCHEMIA UNITED STATES EPIDEMIOLOGY TABLE OF CONTENTS
 CRITICAL LIMB ISCHEMIA UNITED STATES EPIDEMIOLOGY TABLE OF CONTENTS CRITICAL LIMB ISCHEMIA... 1 CONCLUSION... 9 U.S. CRITICAL LIMB ISCHEMIA PREVALENCE... 9 MARKET OPPORTUNITY ENDOVASCULAR... 9 MARKET OPPORTUNITY
CRITICAL LIMB ISCHEMIA UNITED STATES EPIDEMIOLOGY TABLE OF CONTENTS CRITICAL LIMB ISCHEMIA... 1 CONCLUSION... 9 U.S. CRITICAL LIMB ISCHEMIA PREVALENCE... 9 MARKET OPPORTUNITY ENDOVASCULAR... 9 MARKET OPPORTUNITY
DON T LET LEG PAIN BECOME A REAL THREAT.
 DON T LET LEG PAIN BECOME A REAL THREAT. These three words have the power to change lives. Between 8 to 10 million Americans are estimated to suffer from poor blood flow to the legs and feet potentially
DON T LET LEG PAIN BECOME A REAL THREAT. These three words have the power to change lives. Between 8 to 10 million Americans are estimated to suffer from poor blood flow to the legs and feet potentially
Peripheral arterial disease for primary care Ed Aboian, MD
 Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases
 Original paper Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases Sakir Arslan, Isa Oner Yuksel, Erkan Koklu, Goksel
Original paper Clinical and morphological features of patients who underwent endovascular interventions for lower extremity arterial occlusive diseases Sakir Arslan, Isa Oner Yuksel, Erkan Koklu, Goksel
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia
 Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Peripheral Arterial Disease Management A Practical Guide for Internists. EFIM Vascular Working Group
 2 Peripheral Arterial Disease Management A Practical Guide for Internists EFIM Vascular Working Group 1 Peripheral arterial disease (PAD) is a growing concern among our aging population. More than 27 million
2 Peripheral Arterial Disease Management A Practical Guide for Internists EFIM Vascular Working Group 1 Peripheral arterial disease (PAD) is a growing concern among our aging population. More than 27 million
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
What s New in the Management of Peripheral Arterial Disease
 What s New in the Management of Peripheral Arterial Disease Sibu P. Saha, MD, MBA Professor of Surgery Chairman, Directors Council Gill Heart Institute University of Kentucky Lexington, KY Disclosure My
What s New in the Management of Peripheral Arterial Disease Sibu P. Saha, MD, MBA Professor of Surgery Chairman, Directors Council Gill Heart Institute University of Kentucky Lexington, KY Disclosure My
Boca Raton Regional Hospital Grand Rounds September 13, 2016
 Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
LIMB SALVAGE IN THE DIABETIC PATIENT
 LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
Making the difference with Live Image Guidance
 Live Image Guidance 2D Perfusion Making the difference with Live Image Guidance In Peripheral Arterial Disease Real-time results, instant assessment Severe foot complications the result of hampered blood
Live Image Guidance 2D Perfusion Making the difference with Live Image Guidance In Peripheral Arterial Disease Real-time results, instant assessment Severe foot complications the result of hampered blood
USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential
 USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential MEASURE STEWARD: The US Wound Registry [Note: This measure
USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential MEASURE STEWARD: The US Wound Registry [Note: This measure
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Combat Extremity Vascular Trauma
 Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Due to Perimed s commitment to continuous improvement of our products, all specifications are subject to change without notice.
 A summary Disclaimer The information contained in this document is intended to provide general information only. It is not intended to be, nor does it constitute, medical advice. Under no circumstances
A summary Disclaimer The information contained in this document is intended to provide general information only. It is not intended to be, nor does it constitute, medical advice. Under no circumstances
Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes
 Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes Ashok Handa Reader in Surgery and Consultant Surgeon Nuffield Department of Surgery University of Oxford Introduction Vascular
Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes Ashok Handa Reader in Surgery and Consultant Surgeon Nuffield Department of Surgery University of Oxford Introduction Vascular
Case Study: Chris Arden. Peripheral Arterial Disease
 Case Study: Chris Arden Peripheral Arterial Disease Patient Presentation Diane is a 65-year-old retired school teacher She complains of left calf pain when walking 50 metres; the pain goes away after she
Case Study: Chris Arden Peripheral Arterial Disease Patient Presentation Diane is a 65-year-old retired school teacher She complains of left calf pain when walking 50 metres; the pain goes away after she
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD
 Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD University Hospital of Brooklyn Department of Surgery History 52F c PMHx of HTN, asthma p/w fever, malaise s/p one week of ABx for presumed
Infected Lower Extremity Aneurysms C. Stefan Kénel-Pierre, MD University Hospital of Brooklyn Department of Surgery History 52F c PMHx of HTN, asthma p/w fever, malaise s/p one week of ABx for presumed
2018 ACOI Internal Medicine Board Review. Peripheral Vascular Disease. Robert Bender, DO, FACOI, FACC
 2018 ACOI Internal Medicine Board Review Peripheral Vascular Disease Robert Bender, DO, FACOI, FACC Peripheral Vascular Disease (PVD) Arteriosclerosis Obliterans (ASO) Aneurysmal Disease Acute Arterial
2018 ACOI Internal Medicine Board Review Peripheral Vascular Disease Robert Bender, DO, FACOI, FACC Peripheral Vascular Disease (PVD) Arteriosclerosis Obliterans (ASO) Aneurysmal Disease Acute Arterial
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION
 CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
Aortoiliac occlusive disease
 Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Hypothesis: When compared to conventional balloon angioplasty, cryoplasty post-dilation decreases the risk of SFA nses in-stent restenosis
 Cryoplasty or Conventional Balloon Post-dilation of Nitinol Stents For Revascularization of Peripheral Arterial Segments Background: Diabetes mellitus is associated with increased risk of in-stent restenosis
Cryoplasty or Conventional Balloon Post-dilation of Nitinol Stents For Revascularization of Peripheral Arterial Segments Background: Diabetes mellitus is associated with increased risk of in-stent restenosis
BC Vascular Surgery Day
 BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
V.A. is a 62-year-old male who presents in referral
 , LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
, LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options
 Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
Disclosures. Talking Points. An initial strategy of open bypass is better for some CLI patients, and we can define who they are
 An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
Larry Diaz, MD, FSCAI Mehdi H. Shishehbor, DO, FSCAI
 PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
Case 37 Clinical Presentation
 Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Peripheral Arterial Disease
 UFS Peripheral Arterial Disease A problem of supply and demand Larry Rhoads, Associate Chief Underwriter November 8, 2011 PAD Two categories of these circulation disorders: Functional peripheral vascular
UFS Peripheral Arterial Disease A problem of supply and demand Larry Rhoads, Associate Chief Underwriter November 8, 2011 PAD Two categories of these circulation disorders: Functional peripheral vascular
Cardiovascular Update for Primary Care Providers. Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD
 Cardiovascular Update for Primary Care Providers Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD Agenda Lower Extremity pain Initial evaluation Treatment options of noncritical
Cardiovascular Update for Primary Care Providers Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD Agenda Lower Extremity pain Initial evaluation Treatment options of noncritical
Current Non-Surgical Cardiac Interventions. By Pam Bayles, RN, BSN
 Current Non-Surgical Cardiac Interventions By Pam Bayles, RN, BSN Balloon Angioplasty & DES A balloon-tipped catheter was first used in 1964 to treat a cause of atherosclerotic disease in a patient s leg
Current Non-Surgical Cardiac Interventions By Pam Bayles, RN, BSN Balloon Angioplasty & DES A balloon-tipped catheter was first used in 1964 to treat a cause of atherosclerotic disease in a patient s leg
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI
 Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Disclosures. Objectives. Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach. Christopher D. Owens, MD 4/23/2009
 Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
Chapter 4 Section 9.1
 Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
Surgery Chapter 4 Section 9.1 Issue Date: August 26, 1985 Authority: 32 CFR 199.4(c)(2) and (c)(3) 1.0 CPT 1 PROCEDURE CODES 33010-33130, 33140, 33141, 33200-37186, 37195-37785, 92950-93272, 93303-93581,
SAVE LIMBS SAVE LIVES!
 SAVE LIMBS SAVE LIVES! PAD Awareness: The Key to Limb Preservation By Frank J Tursi, D.P.M., F.A.C.F.A.S. Epidemiology Over 12 million people are afflicted with PAD 11 Million of these-dm 4 Million DFU
SAVE LIMBS SAVE LIVES! PAD Awareness: The Key to Limb Preservation By Frank J Tursi, D.P.M., F.A.C.F.A.S. Epidemiology Over 12 million people are afflicted with PAD 11 Million of these-dm 4 Million DFU
Diagnosis and Management of Femoral Access Site Complications IV: Novel Techniques for Endovascular Rescue
 Diagnosis and Management of Femoral Access Site Complications IV: Novel Techniques for Endovascular Rescue Robert M. Bersin, M.D. Director, Endovascular Services Seattle Cardiology and the Cardiovascular
Diagnosis and Management of Femoral Access Site Complications IV: Novel Techniques for Endovascular Rescue Robert M. Bersin, M.D. Director, Endovascular Services Seattle Cardiology and the Cardiovascular
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Popliteal Artery Aneurysms: Diagnosis and Repair Options
 Deepak N. Deshmukh DO April 27, 2018 Popliteal Artery Aneurysms: Diagnosis and Repair Options No Disclosures Popliteal Artery Aneurysms (PAAs) Male Predominanace Most common peripheral Aneurysm (70%) 30-50%
Deepak N. Deshmukh DO April 27, 2018 Popliteal Artery Aneurysms: Diagnosis and Repair Options No Disclosures Popliteal Artery Aneurysms (PAAs) Male Predominanace Most common peripheral Aneurysm (70%) 30-50%
BTK Case Studies Joseph Cardenas, MD AZ Heart & Vascular, Yuma, AZ
 BTK Case Studies Joseph Cardenas, MD AZ Heart & Vascular, Yuma, AZ 1 Case 1 78 yr. old female Rutherford Class II/III lesion 1 block claudicant 2 Pre Treatment Post Treatment Anterior Tibial Artery Occlusion
BTK Case Studies Joseph Cardenas, MD AZ Heart & Vascular, Yuma, AZ 1 Case 1 78 yr. old female Rutherford Class II/III lesion 1 block claudicant 2 Pre Treatment Post Treatment Anterior Tibial Artery Occlusion
Intermittent Claudication
 Intermittent Claudication Exceptional healthcare, personally delivered Ask 3 Questions Preparation for your Appointments We want you to be active in your healthcare. By telling us what is important to
Intermittent Claudication Exceptional healthcare, personally delivered Ask 3 Questions Preparation for your Appointments We want you to be active in your healthcare. By telling us what is important to
Tom Eisele, Benedikt M. Muenz, and Grigorios Korosoglou. Department of Cardiology & Vascular Medicine, GRN Hospital Weinheim, Weinheim, Germany
 Case Reports in Vascular Medicine Volume 2016, Article ID 7376457, 4 pages http://dx.doi.org/10.1155/2016/7376457 Case Report Successful Endovascular Repair of an Iatrogenic Perforation of the Superficial
Case Reports in Vascular Medicine Volume 2016, Article ID 7376457, 4 pages http://dx.doi.org/10.1155/2016/7376457 Case Report Successful Endovascular Repair of an Iatrogenic Perforation of the Superficial
Perfusion Assessment in Chronic Wounds
 Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Disclosures. TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Purpose of Practice Guidelines
 TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step -
 Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have