FINANCIAL DISCLOSURE: No relevant financial relationship exists
|
|
|
- George Johns
- 5 years ago
- Views:
Transcription
1 The Value of Guideline Directed Medical Therapy in Heart Failure Steve Dentel RN BSN CPHQ National Director, Field Programs and Integration American Heart Association/American Stroke Association FINANCIAL DISCLOSURE: No relevant financial relationship exists 12/7/ , American Heart Association 2 1
2 The Need 5.7 million Americans are currently living with heart failure, and 670,000 new cases are diagnosed each year- up significantly from 500,000 cases annually just a few years ago. As our population ages, this epidemic of heart failure will only continue to grow. The cost of providing heart failure ranks among the leading U.S. healthcare expenditures. Additionally, the toll of heart failure on life, both in quality and longevity, is sobering. 12/7/ , American Heart Association 3 Estimated Direct and Indirect Costs of HF in US Hospitalization $ % Total Cost $39.2 billion 14% Nursing Home $4.7 8% Lost Productivity/ Mortality* $4.1 Home Healthcare $3.8 8% 10% 7% Physicians/Other Professionals $2.5 Drugs/Other Medical Durables $3.2 Circ Heart Fail If one assumes all costs of cardiac care for HF patients are attributable to HF (no cost attribution to comorbid conditions), the 2030 projected cost estimates of treating patients with HF will be $160 billion in direct costs. 2

3 The Challenges that We Face Nearly one in four patients hospitalized with HF are rehospitalized within 30 days of discharge 30 day rates of rehospitalizations in HF have risen over the past 2 decades Rehospitalizations for HF vary widely by hospital, even after adjusting for case mix and other factors HF rehospitalizations may be preventable, but effective strategies to prevent rehospitalizations have been traditionally underutilized due to lack of incentives Most of the cost associated with the care of HF patients is attributable to these rehospitalizations 5 HF Readmission in 30 Days ; N=1,330, ,308 rehospitalization; 24.8% Dharmarajan K et al. JAMA 2013:309:
4 Complexity of HF Care Albert NM, et al. Circ Heart Fail. 2015;8: ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest Physicians, Heart Rhythm Society, and International Society for Heart and Lung Transplantation Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation American College of Cardiology Foundation and American Heart Association, Inc. 4
5 Stages, Phenotypes and Treatment of HF GDMT Guideline-Directed Medical Therapy GDMT, which stands for guideline-directed medical therapy. We used to say optimal medical therapy, but this is driven by guidelines. Why is this so important? 5
6 Maintenance of GDMT During Hospitalization I IIa IIb III In patients with HFrEF experiencing a symptomatic exacerbation of HF requiring hospitalization during chronic maintenance treatment with GDMT, it is recommended that GDMT be continued in the absence of hemodynamic instability or contraindications. I IIa IIb III Initiation of beta-blocker therapy is recommended after optimization of volume status and successful discontinuation of intravenous diuretics, vasodilators, and inotropic agents. Beta-blocker therapy should be initiated at a low dose and only in stable patients. Caution should be used when initiating beta blockers in patients who have required inotropes during their hospital course ACCF/AHA Heart Failure Guidelines Pharmacologic Treatment for Stage C HFrEF Yancy C et al. Circulation,
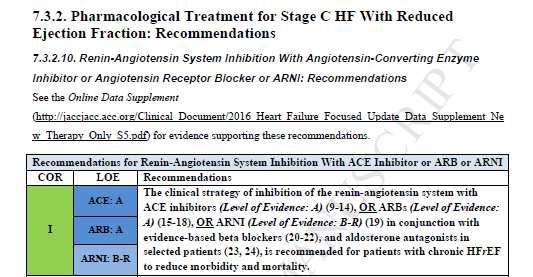
7 Pharmacological Therapy for Management of Stage C HFrEF Recommendations COR LOE Diuretics Diuretics are recommended in patients with HFrEF with fluid retention I C ACE Inhibitors ACE inhibitors are recommended for all patients with HFrEF I A ARBs ARBs are recommended in patients with HFrEF who are ACE inhibitor intolerant ARBs are reasonable as alternatives to ACE inhibitor as first line therapy in HFrEF The addition of an ARB may be considered in persistently symptomatic patients with HFrEF on GDMT Routine combined use of an ACE inhibitor, ARB, and aldosterone antagonist is potentially harmful I IIa IIb III: Harm A A A C Pharmacological Therapy for Management of Stage C HFrEF (cont.) Recommendations COR LOE Beta Blockers Use of 1 of the 3 beta blockers proven to reduce mortality is recommended for all stable patients Aldosterone Antagonists Aldosterone receptor antagonists are recommended in patients with NYHA class II-IV HF who have LVEF 35% Aldosterone receptor antagonists are recommended in patients following an acute MI who have LVEF 40% with symptoms of HF or DM Inappropriate use of aldosterone receptor antagonists may be harmful Hydralazine and Isosorbide Dinitrate The combination of hydralazine and isosorbide dinitrate is recommended for African-Americans, with NYHA class III IV HFrEF on GDMT A combination of hydralazine and isosorbide dinitrate can be useful in patients with HFrEF who cannot be given ACE inhibitors or ARBs I I I III: Harm I IIa A A B B A B 7
8 Pharmacologic Therapy for Management of Stage C HFrEF (cont.) Recommendations COR LOE Digoxin Digoxin can be beneficial in patients with HFrEF IIa B Anticoagulation Patients with chronic HF with permanent/persistent/paroxysmal AF and an additional risk factor for cardioembolic stroke should receive chronic anticoagulant therapy* The selection of an anticoagulant agent should be individualized I C Chronic anticoagulation is reasonable for patients with chronic HF who have permanent/persistent/paroxysmal AF but without an additional risk factor for cardioembolic stroke* IIa B Anticoagulation is not recommended in patients with chronic HFrEF without AF, prior thromboembolic event, or a cardioembolic source Statins Statins are not beneficial as adjunctive therapy when prescribed solely for HF I III: No Benefit III: No Benefit A B A Omega-3 Fatty Acids Omega-3 PUFA supplementation is reasonable to use as adjunctive therapy in HFrEF or HFpEF patients IIa B Pharmacological Therapy for Management of Stage C HFrEF (cont.) Recommendations COR LOE Other Drugs Nutritional supplements as treatment for HF are not recommended III: No in HFrEF Benefit B Hormonal therapies other than to replete deficiencies are not III: No recommended in HFrEF Benefit C Drugs known to adversely affect the clinical status of patients with HFrEF are potentially harmful and should be avoided or III: Harm B withdrawn Long-term use of an infusion of a positive inotropic drug is not recommended and may be harmful except as palliation III: Harm C Calcium Channel Blockers Calcium channel blocking drugs are not recommended as routine III: No in HFrEF Benefit A 8

9 New Guidelines Have Emerged Pharmacologic Treatment for Stage C HFrEF Strategies: Disease Management Genetic Counseling Frailty Assessments Palliative Care Co-morbidities Anemia Sleep disordered breathing Hypertension Atrial Fibrillation Devices Remote PA monitoring Wearable Vests Quality Improvement Process Improvement Patient Education Valsartan/Sacubutril Ivabradine 9

10 RAAS inhibition Ivabradine

 RR Reduction in HF Hospitalizations ACE inhibitor or ARB 17% 26 31% Beta")
11 Evidence-based medical therapy. Mitchell A. Psotka, and John R. Teerlink Circulation. 2016;133: Copyright American Heart Association, Inc. All rights reserved. Medical Therapy for Stage C HFrEF: Magnitude of Benefit Demonstrated in RCTs GDMT RR Reduction in Mortality NNT for Mortality Reduction (Standardized to 36 mo) RR Reduction in HF Hospitalizations ACE inhibitor or ARB 17% 26 31% Beta blocker 34% 9 41% Aldosterone antagonist 30% 6 35% Hydralazine/nitrate 43% 7 33% 11
12 Evidence-Based, Guideline-Recommended Heart Failure Therapies Guideline Recommended Relative Risk Reduction Number Needed to Treat NNT for Mortality Relative Risk Reduction in Therapy in Mortality for Mortality (standardized to 36 HF Hospitalizations months) ACEI/ARB 17% 22 over 42 months 26 31% ARNI 16% 36 over 27 months 27 21% Beta-blocker 34% 28 over 12 months 9 41% Aldosterone Antagonist 30% 9 over 24 months 6 35% Hydralazine/Nitrate 43% 25 over 10 months 7 33% Ivabradine 10% 100 over 23 months 64 26% CRT 36% 12 over 24 months 8 52% ICD 23% 14 over 60 months 23 NA Updated from Fonarow GC, et al. Am Heart J 2011;161: Potential Impact of Optimal Implementation of Evidence-Based HFrEF Therapies on Mortality Guideline Recommended Therapy HF Patient Population Eligible for Treatment, n* Current HF Population Eligible and Untreated, n (%) Potential Lives Saved per Year Potential Lives Saved per Year (Sensitivity Range*) ACEI/ARB 2,459, ,767 (20.4) 6516 ( ,260) Beta-blocker 2,512, ,809 (14.4) 12,922 ( ,329) Aldosterone Antagonist 603, ,326 (63.9) 21,407 (10,960-36,991) Hydralazine/Nitrate 150, ,749 (92.7) 6655 ( ,500) CRT 326, ,604 (61.2) 8317 ( ,372) ICD 1,725, ,512 (49.4) 12,179 ( ,045) Total ,996 (34, ,497) ARNI (replacing ACEI/ARB) 2,287,296 2,287,296 (100) 28,484 (18,230-41,017) Updated from Fonarow GC, et al. Am Heart J 2011;161: and JAMA Cardiology
13 Affordable Care Act Up to 3% cut to all DRGs for readmissions over the expected % Up to 1% in fiscal year 2013, 2% in fiscal year 2014, and 3% in fiscal year 2015 and beyond Initially AMI, heart failure, and pneumonia Expanded to COPD and hip/knee replacements in year decrease in reimbursement to hospitals $7.1 billion The proposed prospective payment systems began October 2012 (beginning of fiscal year 2013) Affordable Care Act In FY 2016, Medicare is penalizing 2592 hospitals Hospitals receive lower payments for every Medicare patient that stays in the hospital readmitted or not Total penalties FY 2016 are $420 million Average payment reduction is 0.61% Maximum penalty of 3% for 38 hospitals A total of 506 hospitals will lose 1% or more of their Medicare payments 13
14 Value of Care as Reported by Medicare in Hospital Compare Looking at payment measures together with quality-of-care measures (such as death rates) allows you to assess the value of care in hospitals. The payment measures add up the payments for care starting the day the patient enters the hospital and continuing for the next 30 days. For example, this can include payments to the hospital, doctor s office, skilled nursing facility, hospice, as well as patient co-pays made during this time. Death rate for heart failure patients Payment for heart failure patients No different than the National Rate Greater than the National Average Payment The National Death Rate for HF patients this reporting period was 11.6%. The National Average Payment for HF patients this reporting period was $15,223. Measuring and Improving the Quality of HF Care Heart failure remains a major public health problem resulting in substantial morbidity and mortality. A number of evidence-based, guideline-recommended therapies are available to treat patients with heart failure. However, study after study shows the large gaps, variations, and disparities in the use of these evidence based therapies in eligible patients


15 Bridging the Gap Between Knowledge and Routine Clinical Practice ACC/AHA/H FSA Guidelines Systems Clinical Practice I IIa IIb III Clinical trial evidence National guidelines Implement evidence-based care Improve communications Ensure compliance Adapted from the American Heart Association. Get With The Guidelines; Improve quality of care Improve outcomes 20 Evidence Based Interventions to Reduce 30 Day Rehospitalization in HF Pre-discharge use of certain GDMT Pre-discharge HF education by trained educators Discharge medication programs Comprehensive discharge planning Early post-discharge physician follow-up Home visits by RNs and/or physicians Comprehensive HF disease management programs Implantable hemodynamic sensors 15

16 31 Most Comprehensive Measure Set Available Achievement Measures Quality Measures Reporting Measures ACEI/ARBs or ARNi at Aldosterone Antagonist at Blood Pressure Control at Discharge Discharge Discharge Evidence-Based Specific Anticoagulation for Atrial Beta Blocker at Discharge Beta Blockers Fibrillation and Atrial Flutter Beta Blocker Medication at Measure LV Function Hydralazine Nitrate at Discharge Post-Discharge Appointment Discharge Lipid-Lowering Medications for Heart Failure Patients DVT Prophylaxis at Discharge CRT-D or CRT-P Placed or Omega-3 Fatty Acid Prescribed at Discharge Supplement Use at ICD Counseling Provided or Discharge Prescribed or Placed at Diabetes Treatment Discharge Diabetes Teaching Influenza Vaccination During Smoking Cessation Flu Season Discharge Instructions Pneumococcal Vaccination ICD Placed or Prescribed at Follow-Up Visit Scheduled Discharge Within 7 Days or Less Advanced Care Plan ARNi at Discharge QRS Duration Documented Heart Failure Disease Management Program Referral Follow-Up Visit or Contact Within 48 Hours of Discharge Scheduled 12/7/ , American Heart Association 32 16
17 Most Comprehensive Measure Set Available Reporting Measures (Continued) Descriptive Measures Mortality & Readmission Measures Follow Up Visit or Contact Within 72 Hours of Discharge Scheduled 60 Minutes of Heart Failure Education Referral to AHA Heart Failure Interactive Workbook Referral to HF Disease Management, 60 Minutes Patient Education, Or HF Interactive Workbook Heart Failure Activity Level Heart Failure Diet Heart Failure Follow-Up Heart Failure Weight Heart Failure Symptoms Worsen Length of Stay Care Transition Record Transmitted Advance Directive Executed Discharge Disposition Ivabradine Prescribed Age Diagnosis Gender Race HF Composite Measure HF Defect-Free Measure JC/CMS HF Defect Free Measure Target: HF Defect Free Measure In-Hospital Mortality Risk Adjusted Mortality Ratio Readmission Frequency & Rate 30, 60 & 90 Day Readmissions & Rate Not equivalent to the CMS 30-Day Risk-Standardized Readmission Measure. It is not risk-adjusted, does not represent all cause readmission, and does not capture readmissions from other hospitals. 12/7/ , American Heart Association 33 17

18 35 Get With The Guidelines - Heart Failure Get With The Guidelines - Heart Failure launched in 2005 There are currently 4 Achievement Measures and 10 Quality Measures for participating hospitals to collect and report measuring how well their hospitals follow the AHA guidelines for HF Hospitals enrolled have several opportunities to be recognized for their efforts and are recognized at National events as mentioned above. As of November 2016, there are greater than 80 Get With The Guidelines manuscripts focused on Heart Failure. Please review them at
19 The American Heart Association is supported by 7 affiliates throughout the United States and make it possible to have our expert quality improvement field staff covering all 50 states plus Puerto Rico. With this structure, all hospitals throughout the nation are supported by at least one person who has significant experience in hospital/system/region/statewide quality improvement initiatives. Not only will this affiliate field staff review your hospital level data but they will also provide you with realworld recommendations that may help you improve the care your patients receive. Additionally, field staff will keep you updated on what is occurring within your city, state, and the nation in relation to quality improvement in cardiovascular services. Focus on Quality Suite of Programs are Supported by our Expert Field Staff Each affiliate staff person is supported by a Quality Improvement Vice President. With these two people, your hospital is well-supported and represented at the affiliate level and AHA National Center. 37 The Patient Management Tool The Get With The Guidelines Patient Management Tool (PMT) through Quintiles provides applications as easy-to-use web-based tools. o o The tools are online, interactive assessment and reporting systems that aid in Get With The Guidelines program implementation. The tools provide patient-specific American College of Cardiology/American Heart Association guideline information and enable each institution to track its adherence to the guidelines individually and against the AHA s national benchmarks over time. The PMT application is an important part of implementing Get With The Guidelines Heart Failure, Stroke, Resuscitation and AFIB programs because it helps hospital care teams manage each patient to the guidelines and reduces missed cases. These tools have demonstrated effectiveness in improving hospital compliance rates with guidelines. These programs also include technical support from the Quintiles help desk and one-onone support from the American Heart Association field staff
20 Recognition from the American Heart Association Our goal is help hospitals improve care processes to therefore help us reach our Mission of Building Healthier Lives Free of Cardiovascular Disease and Stroke. Because our hospitals join us in this mission and see measurable results, we want to congratulate them for a job well done. Hospitals that meet eligibility criteria may apply for the Get With The Guidelines Performance Achievement Awards and will be recognized in USNWR advertisement, Circulation advertisement and the International Stroke Conference and Scientific Sessions Get With The Guidelines Achievement Awards 85% compliance for module specific Achievement Measures Bronze: 90 consecutive days Silver: 12 consecutive months Gold: 24 consecutive months Get With The Guidelines Plus Awards Must have current Silver or Gold Award for Get With The Guidelines Hospital may self select group of Quality Measures and demonstrate 75% compliance for same time period as Silver or Gold Award 39 GWTG-HF: Data Submission Number of records July
21 GWTG-HF: Achievement Measures Com pliance Evidence-Based Post Discharge Composite LV Function ACEI or ARB at Beta Blocker at Discharge 100% Compliance Beta Blocker at Appointment for Performance Measurement D/C for LVSD Discharge Instructions Measure* D/C for LVSD HF patients Measure* Baseline 90.1% 81.2% 61.0% 87.3% 39.3% 69.7% 80.3% 62.1% Current 98.7% 92.8% 92.6% 98.2% 74.9% 95.7% 96.8% 93.0% Achievement Measure * Modified to include Beta Blocker at Discharge and Discharge Instructions rather than Evidence-Based Beta Blocker at D/C and Post Discharge Appointment Baseline = Admissions Jan2005 Dec2005 July 2016 Current = Overall GWTG-HF: Quality Measures (1) Compliance ICD Counseling or ICD placed or Warfarin at d/c Aldosterone antagonist at d/c for LVSD Hydralazine/Isosorbide at d/c for AA prescribed at D/C Baseline 57.3% 19.9% 10.8% 31.3% Current 84.7% 38.9% 29.8% 53.1% Quality Measure Baseline = Admissions Jan2005 Dec2005 July 2016 Current = Overall 21
22 GWTG-HF: Quality Measures (2) Compliance Pnemococcal Vaccine Influenza Vaccine Follow-up visit within 7 days or less DVT Management CRT placed or prescribed at discharge Baseline 22.9% 17.7% 61.9% 25.4% 39.9% Current 67.8% 76.9% 78.8% 84.1% 51.7% Quality Measure Baseline = Admissions Jan2009 Dec2009 July 2016 Current = Overall Conclusions Significant opportunities exist to improve the quality of care, care transitions, and outcomes for patients hospitalized with HF Improving care, including GDMT, and reducing preventable hospitalizations in HF is a national focus but very challenging Some programs and strategies have been successful in reducing (re)hospitalizations 22
23 Questions? 12/7/ , American Heart Association 45 23
HF QUALITY MEASURES. Hydralazine/nitrate at discharge: Percent of black heart
 Get With The Guidelines - Heart Failure is the American Heart Association s collaborative quality improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized
Get With The Guidelines - Heart Failure is the American Heart Association s collaborative quality improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized
HEART FAILURE QUALITY IMPROVEMENT. American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement
 HEART FAILURE QUALITY IMPROVEMENT American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement 1 DISCLOSURES NONE 2 3 WHY IS THIS IMPORTANT? WHY? Heart Failure Currently, an
HEART FAILURE QUALITY IMPROVEMENT American Heart Association Shawni Smith Regional Director, Quality & Systems Improvement 1 DISCLOSURES NONE 2 3 WHY IS THIS IMPORTANT? WHY? Heart Failure Currently, an
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
9/10/ , American Heart Association 2
 Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Clyde W. Yancy, MD, MSc, MACC, FAHA, MACP Vice Dean, Diversity & Inclusion Magerstadt Professor of Medicine Professor of Medical Social Sciences Chief, Division of Cardiology Northwestern University, Feinberg
Improving Outcomes After Hospital Discharge: How To Do It and What is the Evidence That it Works?
 UCSD Heart Failure Symposium Improving Outcomes After Hospital Discharge: How To Do It and What is the Evidence That it Works? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA The Eliot Corday Professor of Cardiovascular
UCSD Heart Failure Symposium Improving Outcomes After Hospital Discharge: How To Do It and What is the Evidence That it Works? Gregg C. Fonarow, MD, FACC, FAHA, FHFSA The Eliot Corday Professor of Cardiovascular
Get With The Guidelines: Lessons for National Healthcare Improvement Programs
 Get With The Guidelines: Lessons for National Healthcare Improvement Programs Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of Cardiovascular Medicine and Science UCLA Division of Cardiology
Get With The Guidelines: Lessons for National Healthcare Improvement Programs Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Eliot Corday Professor of Cardiovascular Medicine and Science UCLA Division of Cardiology
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
To download handouts for today s presentation, click the three paper icon at the top right of your screen.
 To download handouts for today s presentation, click the three paper icon at the top right of your screen. Get With The Guidelines Heart Failure PMT Spring Update September 9, 2013 Clyde W. Yancy, MD,
To download handouts for today s presentation, click the three paper icon at the top right of your screen. Get With The Guidelines Heart Failure PMT Spring Update September 9, 2013 Clyde W. Yancy, MD,
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Heart Failure. Disclosures. Objectives: 8/28/2017. This is not a virus. It doesn t go away. none
 Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes?
 Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
Keynote Address II Managing Acute Heart Failure: What Can We Do to Improve Outcomes? 24 th Annual San Diego Heart Failure Symposium June 1-2, 2018 La Jolla, CA Barry Greenberg, MD Distinguished Professor
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
The Role of Information Technology in Disease Management: A Case for Heart Failure
 The Role of Information Technology in Disease Management: A Case for Heart Failure Teresa De Peralta, MSN, APN-C Heart Failure Product Workflow Consultant Medtronic Population Management Level 3: As patient
The Role of Information Technology in Disease Management: A Case for Heart Failure Teresa De Peralta, MSN, APN-C Heart Failure Product Workflow Consultant Medtronic Population Management Level 3: As patient
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management
 Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management
Cardiovascular Guideline-Driven Pharmacotherapies: Optimizing Management David Parra, Pharm.D., FCCP, BCPS Clinical Pharmacy Program Manager in Cardiology/Anticoagulation VISN 8 Pharmacy Benefits Management
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
What s new in the 2017 heart failure guidelines. Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA
 What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
Heart Failure Therapies State of the Art 2017
 Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Heart Failure Therapies State of the Art 2017 Andrew J. Sauer, MD Assistant Professor Director, Center for Heart Failure Medical Director, Heart Transplantation UNOS Primary Transplant Physician asauer@kumc.edu
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
Reducing 30-day Rehospitalization for Heart Failure: An Attainable Goal?
 Reducing 30-day Rehospitalization for Heart Failure: An Attainable Goal? Ileana L. Piña, MD, MPH Professor of Medicine, Epi/Biostats Case Western Reserve University Graduate VA Quality Scholar Cleveland
Reducing 30-day Rehospitalization for Heart Failure: An Attainable Goal? Ileana L. Piña, MD, MPH Professor of Medicine, Epi/Biostats Case Western Reserve University Graduate VA Quality Scholar Cleveland
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
GET WITH THE GUIDELINES- PAST AND FUTURE
 GET WITH THE GUIDELINES- PAST AND FUTURE Amy Graham, RN, BS, CEN, NREMT-P Director, Quality & Systems Improvement Kentucky and Southwest Ohio American Heart Association 1 DISCLOSURE SLIDE I AM THE QUALITY
GET WITH THE GUIDELINES- PAST AND FUTURE Amy Graham, RN, BS, CEN, NREMT-P Director, Quality & Systems Improvement Kentucky and Southwest Ohio American Heart Association 1 DISCLOSURE SLIDE I AM THE QUALITY
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Update in Congestive Hear Failure DRAGOS VESBIANU MD
 Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Guideline Management of Chronic Heart Failure
 Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Heart Failure Management: Continuum of Care
 Healthy Kingsport Conference Heart Failure Management: Continuum of Care Robin Harris PhD, ANP-BC, ACNS-BC Clinical Assistant Professor University of Tennessee College of Nursing Important Info I, Robin
Healthy Kingsport Conference Heart Failure Management: Continuum of Care Robin Harris PhD, ANP-BC, ACNS-BC Clinical Assistant Professor University of Tennessee College of Nursing Important Info I, Robin
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Tuesday October 18, :00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc
 Tuesday October 18, 2016 1:00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc Amgen Cardiovascular proudly sponsors Heart Science Amplified: An Online Speaker Series and Get With The Guidelines -Heart
Tuesday October 18, 2016 1:00pm 2:00pm Central Presenter: Clyde W. Yancy, MD, MSc Amgen Cardiovascular proudly sponsors Heart Science Amplified: An Online Speaker Series and Get With The Guidelines -Heart
*NOTE: When submitting CPT code and 99239, it is recommended the measure be submitted each time the code is submitted for hospital discharge.
 Quality ID #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) National Quality
Quality ID #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) National Quality
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
All Roads Lead to HF. Presenter Disclosure Information. After a Decade of (Almost) Nothing Multiple New Therapies for Heart Failure CAD.
 Nothing Multiple New Therapies for Heart Failure CAD.") After a Decade of (Almost) Nothing Multiple New Therapies for Heart Failure Larry A. Allen, MD, MHS Director for Advanced Heart Failure October 18, 2016 Presenter Disclosure Information I will not discuss
After a Decade of (Almost) Nothing Multiple New Therapies for Heart Failure Larry A. Allen, MD, MHS Director for Advanced Heart Failure October 18, 2016 Presenter Disclosure Information I will not discuss
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
CRT Vs RV Pacing Benefits
 CRT-P & CRT-D Indications According to Guidelines are Guidelines Fully Adopted? Salama H. Omar M.D. Prof. Critical Care Medicine, Cairo University CRT Vs RV Pacing Benefits 1 Benefit of Upgrade CTR-P &
CRT-P & CRT-D Indications According to Guidelines are Guidelines Fully Adopted? Salama H. Omar M.D. Prof. Critical Care Medicine, Cairo University CRT Vs RV Pacing Benefits 1 Benefit of Upgrade CTR-P &
2/3/2017. Objectives. Effective Heart Failure Management through Evidence Based Practice and Innovation
 Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
Effective Heart Failure Management through Evidence Based Practice and Innovation Jennifer Bauerly RN, CHFN, APRN-BC CentraCare Heart and Vascular Center Objectives Describe the scope and impact of heart
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE
 OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE GUIDELINE FOR THE MANAGEMENT OF HEART FAILURE Background: Heart failure (HF) is a complex clinical syndrome that results from
OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE GUIDELINE FOR THE MANAGEMENT OF HEART FAILURE Background: Heart failure (HF) is a complex clinical syndrome that results from
Heart Failure with Reduced EF. Dino Recchia, MD, FACC, FHFSA
 Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Heart Failure with Reduced EF Dino Recchia, MD, FACC, FHFSA Heart Failure HF is the end phenotype of almost all CV disorders Complex clinical syndrome resulting from any structural or functional impairment
Disclosures. Preventing Heart Failure Re-admissions in Deaths Due to Cardiovascular Disease (United States: ) Heart Failure
 Heart Failure") 29 th Annual Cardiology for Clinicians Spring Symposium Workshop #3 Alumni Hallway, Northeastern Conference Room, 1-9525 Thursday, May 5, 2016 Preventing Heart Failure Re-admissions in 2016 Leway Chen,
29 th Annual Cardiology for Clinicians Spring Symposium Workshop #3 Alumni Hallway, Northeastern Conference Room, 1-9525 Thursday, May 5, 2016 Preventing Heart Failure Re-admissions in 2016 Leway Chen,
Implementing the CardioMEMS HF System into the Management of Heart Failure Patients
 Implementing the CardioMEMS HF System into the Management of Heart Failure Patients Robert W. Hull MD FACC Associate Professor of Medicine WVU Heart Institute Co-director, Arrhythmia Service Director,
Implementing the CardioMEMS HF System into the Management of Heart Failure Patients Robert W. Hull MD FACC Associate Professor of Medicine WVU Heart Institute Co-director, Arrhythmia Service Director,
I have no disclosures. Disclosures
 I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
Initiating New Medications in the Management of Heart Failure
 Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Initiating New Medications in the Management of Heart Failure Sandra Oliver-McNeil DNP, MSN, ACNP-BC, CHFN Associate Professor (Clinical) Wayne State University College of Nursing Objectives The participant
Background: Patient Adherence Challenges/Barriers
 This Nurse Tip Sheet was developed by AAHFN as resource in facilitating patient education. It provides additional information so that the Nurse can supplement patient teaching with the corresponding Patient
This Nurse Tip Sheet was developed by AAHFN as resource in facilitating patient education. It provides additional information so that the Nurse can supplement patient teaching with the corresponding Patient
Known Actions of Digoxin
 Known Actions of Digoxin Hemodynamic effects in heart failure Increases cardiac output, no effect on blood pressure Decreases PCWP Increases LVEF (
Known Actions of Digoxin Hemodynamic effects in heart failure Increases cardiac output, no effect on blood pressure Decreases PCWP Increases LVEF (
GWG Heart Failure Progress to Date. Lorraine Montoya BSN, MAdEd
 GWG Heart Failure Progress to Date Lorraine Montoya BSN, MAdEd Our Partners Friday, May 6, 2011 The Heart Failure GAP Project Background HF is steadily increasing as a result of success in treating heart
GWG Heart Failure Progress to Date Lorraine Montoya BSN, MAdEd Our Partners Friday, May 6, 2011 The Heart Failure GAP Project Background HF is steadily increasing as a result of success in treating heart
HEART FAILURE KEEPING YOUR PATIENT AT HOME
 HEART FAILURE KEEPING YOUR PATIENT AT HOME SUZANNE FRAZIER MS, CRNP, NP-C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY HEART & VASCULAR INSTITUTE IMPACT OF HEART FAILURE In 2010,
HEART FAILURE KEEPING YOUR PATIENT AT HOME SUZANNE FRAZIER MS, CRNP, NP-C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY HEART & VASCULAR INSTITUTE IMPACT OF HEART FAILURE In 2010,
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update)
") Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges
 Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
ESC Guidelines. ESC Guidelines Update For internal training purpose. European Heart Journal, doi: /eurheart/ehn309
 ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
ESC Guidelines Update 2008 ESC Guidelines Heart failure update 2008 For internal training purpose. 0 Agenda Introduction Classes of recommendations Level of evidence Treatment algorithm Changes to ESC
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
2 I. Reduced EF (HFrEF)
") HF Classification EF Description 2 I. Reduced EF (HFrEF) 40% 1. Referred to as systolic HF. 2. Randomized trials mainly enrolled patients with HFrEF. 3. Efficacious therapies is shown only in these patients.
HF Classification EF Description 2 I. Reduced EF (HFrEF) 40% 1. Referred to as systolic HF. 2. Randomized trials mainly enrolled patients with HFrEF. 3. Efficacious therapies is shown only in these patients.
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare?
 1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare? Dr Nerys Davies, GPST Ms B. Davies, Specialist Nurse (Heart Failure) Dr J. Taylor, Consultant Cardiologist
1000 Lives Key Components of Reliable, Evidence-Based Chronic Heart Failure Care how do we compare? Dr Nerys Davies, GPST Ms B. Davies, Specialist Nurse (Heart Failure) Dr J. Taylor, Consultant Cardiologist
Heart Failure Guidelines For your Daily Practice
 Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Heart Failure Guidelines For your Daily Practice Juan M. Aranda, Jr., MD, FACC, FHFSA Professor of Medicine Director of Heart Failure and Cardiac Transplantation University of Florida College of Medicine
Citation. What is New in the 2013 ACC/AHA HF Guideline. Dimensions in Heart and Vascular Care Penn State Heart and Vascular Institute
 What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
Session 9: Key Strategies to Keep Heart Failure Patients Out of the Hospital Learning Objectives
 Session 9: Key Strategies to Keep Heart Failure Patients Out of the Hospital Learning Objectives 1. Evaluate the risk factors and clinical interventions for heart failure. 2. Identify the importance of
Session 9: Key Strategies to Keep Heart Failure Patients Out of the Hospital Learning Objectives 1. Evaluate the risk factors and clinical interventions for heart failure. 2. Identify the importance of
Positive Impact of Recent Metrics
 Seeing Faces on Readmissions and Unmet Metrics Who is getting readmitted after heart failure hospitalizations? Who with HFrEF is discharged without guideline-based medications? Positive Impact of Recent
Seeing Faces on Readmissions and Unmet Metrics Who is getting readmitted after heart failure hospitalizations? Who with HFrEF is discharged without guideline-based medications? Positive Impact of Recent
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
*NOTE: When submitting CPT code and 99239, it is recommended the measure be submitted each time the code is submitted for hospital discharge.
 Quality ID #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) National Quality
Quality ID #5 (NQF 0081): Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) National Quality
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA
 Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Management of chronic heart failure: pharmacology. Giuseppe M.C. Rosano, MD, PhD, FHFA Declaration of potential conflict of interests Type of job or financial support Salary Ordinary funds Position in
Long-Term Management Of the ACS Patient: State-of-the-Art. Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA
 Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
What s at the Heart of the Matter?
 What s at the Heart of the Matter? Inpatient Pharmacy Services for Heart Failure Patients Jason Williamson, PharmD, BCPS Clinical Pharmacy Manager, PGY1 Pharmacy Residency Director Genesys Regional Medical
What s at the Heart of the Matter? Inpatient Pharmacy Services for Heart Failure Patients Jason Williamson, PharmD, BCPS Clinical Pharmacy Manager, PGY1 Pharmacy Residency Director Genesys Regional Medical
Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond
 Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond Steven Sheris, M.D., FACC, FACP Chief of Cardiology Gagnon Cardiovascular Institute at Overlook Medical
Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond Steven Sheris, M.D., FACC, FACP Chief of Cardiology Gagnon Cardiovascular Institute at Overlook Medical
Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses
 Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center
Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
A Global perspective on Heart Failure: What needs to change? Martin R Cowie London, United Kingdom
 A Global perspective on Heart Failure: What needs to change? Martin R Cowie London, United Kingdom Global perspective on heart failure: what needs to change? Martin R Cowie Professor of Cardiology National
A Global perspective on Heart Failure: What needs to change? Martin R Cowie London, United Kingdom Global perspective on heart failure: what needs to change? Martin R Cowie Professor of Cardiology National
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
Optimal Implementation of Heart Failure Guidelines and Standards Gregg C. Fonarow, MD, FACC, FAHA
 Optimal Implementation of Heart Failure Guidelines and Standards Gregg C. Fonarow, MD, FACC, FAHA Eliot Corday Professor of Cardiovascular Medicine and Science UCLA Division of Cardiology Director, Ahmanson-UCLA
Optimal Implementation of Heart Failure Guidelines and Standards Gregg C. Fonarow, MD, FACC, FAHA Eliot Corday Professor of Cardiovascular Medicine and Science UCLA Division of Cardiology Director, Ahmanson-UCLA
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
2012 Core Measures. Acute Myocardial Infarction (AMI)
") 2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
2012 Core Measures Acute Myocardial Infarction (AMI) Aspirin at Arrival Aspirin Prescribed at Discharge Angiotensin converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB) for left ventricular
Practice-Level Executive Summary Report
 PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
The CCS Heart Failure Companion: Bridging Guidelines to your Practice
 The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
The CCS Heart Failure Companion: Bridging Guidelines to your Practice Looking for practical answers concerning optimal heart failure care? The CCS Heart Failure Guidelines Companion can help. The Canadian
Saudi Heart Failure Guidelines. Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group
 Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
Saudi Heart Failure Guidelines Waleed AlHabeeb, MD, MHA Consultant Heart Failure Cardiologist President of the Saudi Heart Failure Group Heart Failure Expert committee The Heart Failure Expert Committee,
Objectives. Outline 4/3/2014
 Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Enhancing the Quality of Heart Failure Care
 Enhancing the Quality of Heart Failure Care 2 Enhancing the quality of Heart Failure care Kent Surrey Sussex Academic Health Science Network 3 Contents 2 Heart failure care in the UK: Case for change 3
Enhancing the Quality of Heart Failure Care 2 Enhancing the quality of Heart Failure care Kent Surrey Sussex Academic Health Science Network 3 Contents 2 Heart failure care in the UK: Case for change 3
Treating Heart Failure in Biodiverse Patient Populations: Best Practices and Unveiling Disparities in Blacks
 Treating Heart Failure in Biodiverse Patient Populations: Best Practices and Unveiling Disparities in Blacks 12th Annual Leadership Summit on Health Disparities & Congressional Black Caucus Spring Health
Treating Heart Failure in Biodiverse Patient Populations: Best Practices and Unveiling Disparities in Blacks 12th Annual Leadership Summit on Health Disparities & Congressional Black Caucus Spring Health
The Future of Cardiac Care: Managing Our Patients Together
 The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
The Future of Cardiac Care: Managing Our Patients Together Charles R. Caldwell, MD, FACC Disclosures: iheartdoc,inc. Telemedicine 1 MACRA Medicare Access and CHIP Reauthorization Act of 2015 Repealed the
Reducing Hospital Readmissions and Increasing Time to Hospital Readmission in Blacks with Heart Failure
 10th Annual National Summit on Health Disparities CBC Health Braintrust Meeting April 22 April 23, 2013, Washington, DC Reducing Hospital Readmissions and Increasing Time to Hospital Readmission in Blacks
10th Annual National Summit on Health Disparities CBC Health Braintrust Meeting April 22 April 23, 2013, Washington, DC Reducing Hospital Readmissions and Increasing Time to Hospital Readmission in Blacks
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
Gerasimos Filippatos MD, FESC, FCCP, FACC
 Gerasimos Filippatos MD, FESC, FCCP, FACC Head of HF Unit at Athens University Hospital, Greece President (2014-2016) of the HF Association of the European Society of Cardiology (ESC) Served as Chair of
Gerasimos Filippatos MD, FESC, FCCP, FACC Head of HF Unit at Athens University Hospital, Greece President (2014-2016) of the HF Association of the European Society of Cardiology (ESC) Served as Chair of
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior
Neprilysin Inhibitor (Entresto ) Page 1 of 6 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Neprilysin Inhibitor (Entresto ) Prime Therapeutics will review Prior