Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses
|
|
|
- Clinton Thomas
- 6 years ago
- Views:
Transcription
1 Diagnosing Heart Failure in Primary Care: Differentiating Zebras from Horses CANP March 2015 Maria Fe White, ACNP-BC Advanced Heart Disease Clinic Comprehensive Transplant Center Cedars-Sinai Medical Center Los Angeles, California

2 Objectives Define Heart Failure Differentiate various etiologies Discuss diagnostic and therapeutic strategies in Primary Care Describe clinical implications for the Primary Care NPs
3 Definition of HF Complex clinical syndrome resulting from structural or functional impairment of ventricular filling or ejection of blood. Result from disorders of the pericardium, myocardium, endocardium, heart valves, great vessels, metabolic, toxic, etc Associated with LV functional abnormalities, systolic or diastolic, preserved or reduced Ejection Fraction (EF). Yancy, et al, 2013 ACCF/AHA Guideline for Management of HF
4 HEART FAILURE Myocardial Injury Fall in LV Performance NEUROHORMONAL ACTIVATION: Renin Angiotensin II-Aldosterone Axis System, Sympathetic Nervous System Endothelin, TNF, Norepinephrine BNP (B-type natriuretic peptide) Myocardial Toxicity Peripheral vasoconstriction Hemodynamic alterations Mortality and Morbidity Remodeling and Progressive worsening of LV function Heart Failure Symptoms: dyspnea, fatigue, edema PATHOPHYSIOLOGY
5 3/30/2015 SBCO0023 Heart Failure An Epidemic 5 Prevalence 5.1 million and rising Incidence >650,000 new cases/yr 1 Mil hospitalizations/year Most Common Medicare DRG Mortality 50% at 5 years Cost : $40 Billion $23,077* per hospitalization 20% Lifetime Risk in Americans >40 years of age AA have highest risk WW have lowest risk 121 per 1,000 Medicare beneficiaries have HF 1 in 9 deaths, HF in Death certificate ACA VBP HF Care accoutability ACC/AHA/AMC. Heart Failure Guidelines Update 2013

6 ETIOLOGY Unknown 34% HTN 14% VHD 7 % CAD 36% Other 4 % A Fib 5 %
7 Definition of Heart Failure Classification I. Heart Failure with Reduced Ejection Fraction (HFrEF) Ejection Description Fraction 40% Also referred to as systolic HF. Randomized clinical trials have mainly enrolled patients with HFrEF and it is only in these patients that efficacious therapies have been demonstrated to date. II. Heart Failure with Preserved Ejection Fraction (HFpEF) 50% Also referred to as diastolic HF. Several different criteria have been used to further define HFpEF. The diagnosis of HFpEF is challenging because it is largely one of excluding other potential nonc-ardiac causes of symptoms suggestive of HF. To date, efficacious therapies have not been identified. a. HFpEF, Borderline 41% to 49% These patients fall into a borderline or intermediate group. Their characteristics, treatment patterns, and outcomes appear similar to those of patient with HFpEF. b. HFpEF, Improved >40% It has been recognized that a subset of patients with HFpEF previously had HFrEF. These patients with improvement or recovery in EF may be clinically distinct from those with persistently preserved or reduced EF. Further research is needed to better characterize these patients.
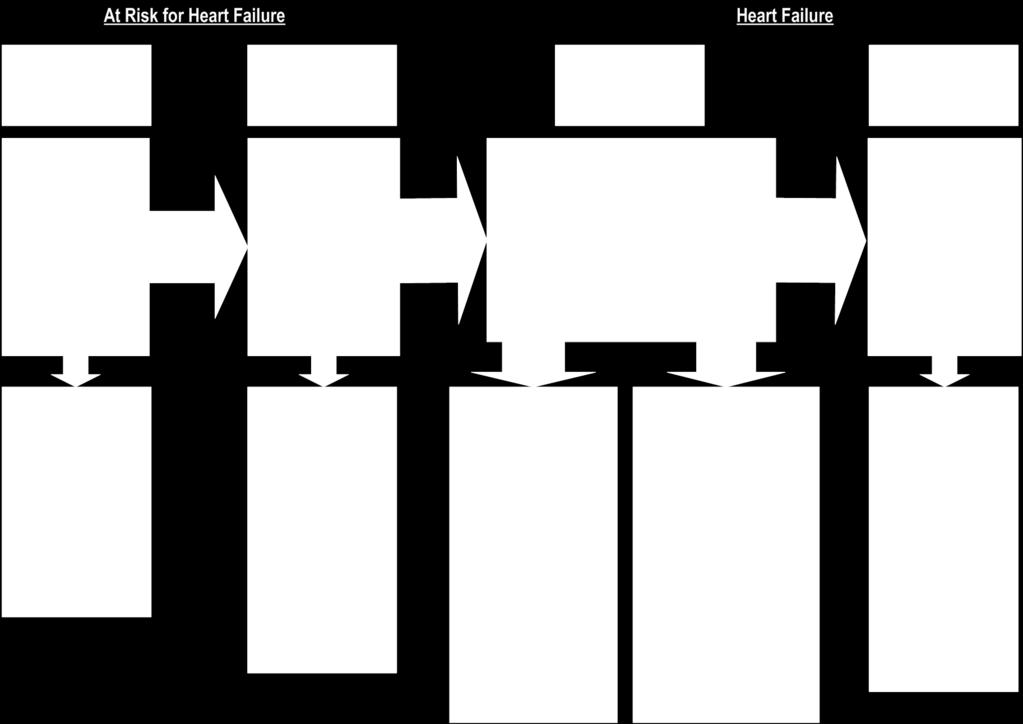
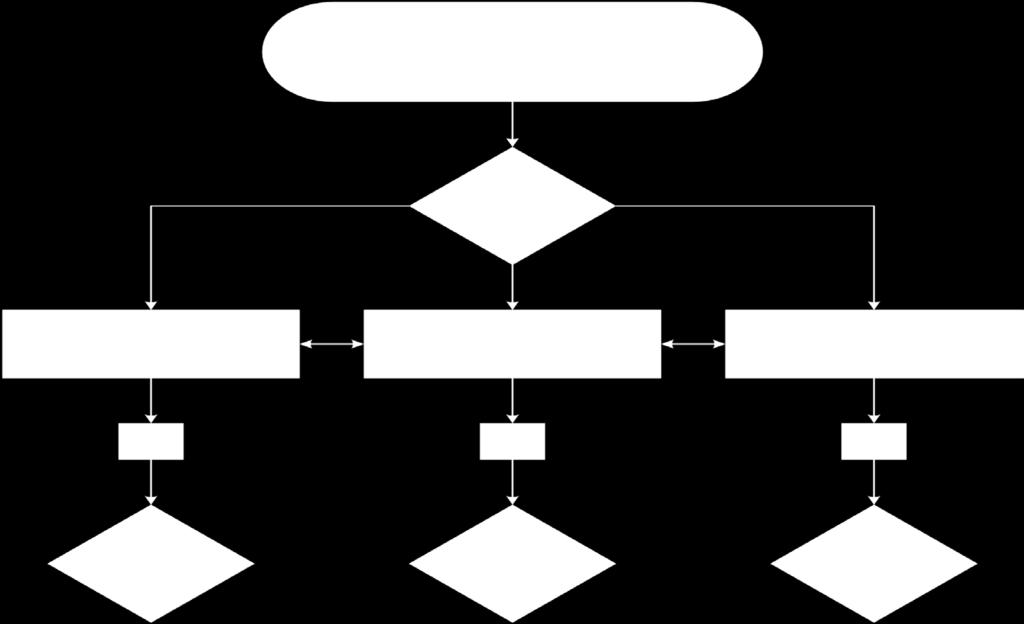
8 Classification of HF A B C D ACCF/AHA Stages of HF At high risk for HF but without structural heart disease or symptoms of HF. Structural heart disease but without signs or symptoms of HF. Structural heart disease with prior or current symptoms of HF. Refractory HF requiring specialized interventions. None I I II III IV NYHA Functional Classification No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF. Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in symptoms of HF. Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF. Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest.
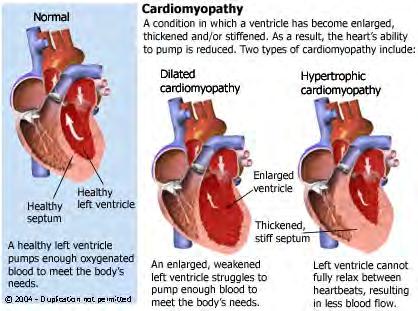
9 Structural Changes
10 Risk Factors for HF Hypertension Diabetes Metabolic Syndrome Atherosclerotic Disease Obesity Genetics Exposure
11 Etiologies of HF Idiopathic Dilated Ischemic Valvular Congenital Familial Endocrine/Metabolic Toxic Tachycardia-Induced Inflammatory/Infectious Connective/Rheumatology Peripartum Iron overload Amyloidosis Sarcoidosis Stress Induced

12 Familial Cardiomyopathy About 20-35% of idiopathic CMY patients have familial CMY Family history: SCD, 2 closely related family Genetic screening have associated cost Genetic Counseling in conjunction with screening
13 Genetic Considerations Condition Family Members Screening Genetic Testing Familial DCM Idiopathic CMY Unaffected first degree relatives should undergo periodic, serial echocardiogram Frequency uncertain but Q 3-5 years reasonable. Patients should inform first degree their diagnosis. Relatives should update their clinicians and discuss if echo screening is needed. Maybe considered in conjunction with genetic counseling. Utility of genetic testing remain uncertain. Higher yield in patients with significant cardiac conduction disease &/or with family history of sudden cardiac death.
14 Initial Evaluation History and Physical Examination
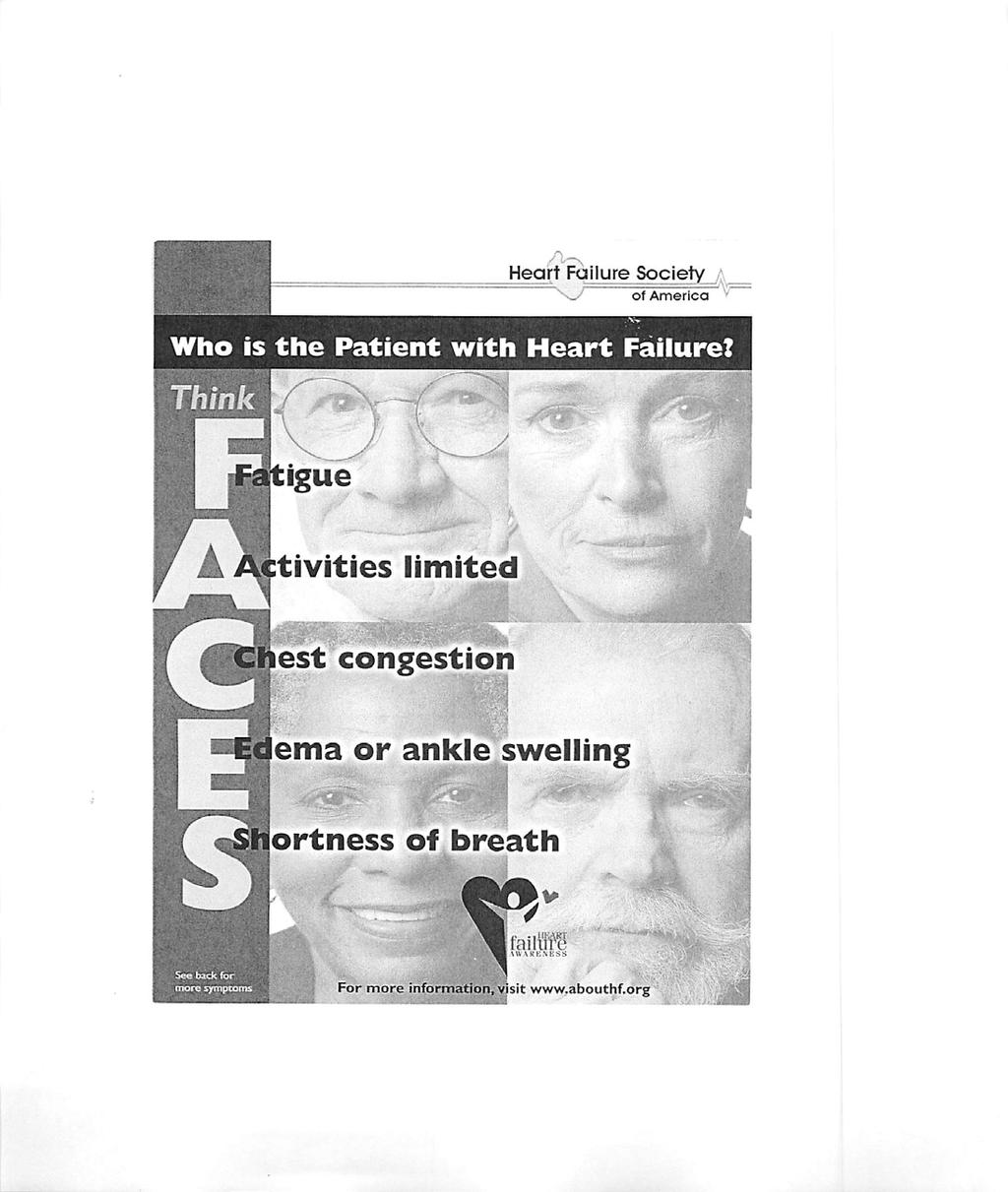
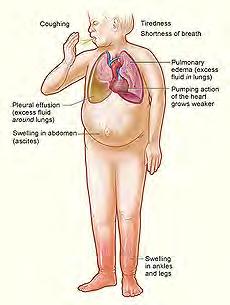
15 Clinical Presentation


16 Classification of Recommendations and Levels of Evidence
17 History & Physical Exam A thorough history and physical examination should be obtained/performed in patients presenting with HF to identify cardiac and noncardiac disorders or behaviors that might cause or accelerate the development or progression of HF. In patients with idiopathic DCM, a 3-generational family History should be obtained to aid in establishing the diagnosis of familial DCM. I IIa IIb III I IIa IIb III Volume status and vital signs should be assessed at each patient encounter. This includes serial assessment of weight, as well as estimates of jugular venous pressure and the presence of peripheral edema or orthopnea. I IIa IIb III
18 Noninvasive Imaging Recommendation COR LOE Patients with suspected, acute, or new-onset HF should undergo a chest x-ray A 2-dimensional echocardiogram with Doppler should be performed for initial evaluation of HF Repeat measurement of EF is useful in patients with HF who have had a significant change in clinical status or received treatment that might affect cardiac function, or for consideration of device therapy Noninvasive imaging to detect myocardial ischemia and viability is reasonable in HF and CAD Viability assessment is reasonable before revascularization in HF patients with CAD Radionuclide ventriculography or MRI can be useful to assess LVEF and volume MRI is reasonable when assessing myocardial infiltration or scar I I I IIa IIa IIa IIa C C C C B C B Routine repeat measurement of LV function assessment should not be performed III: No Benefit B

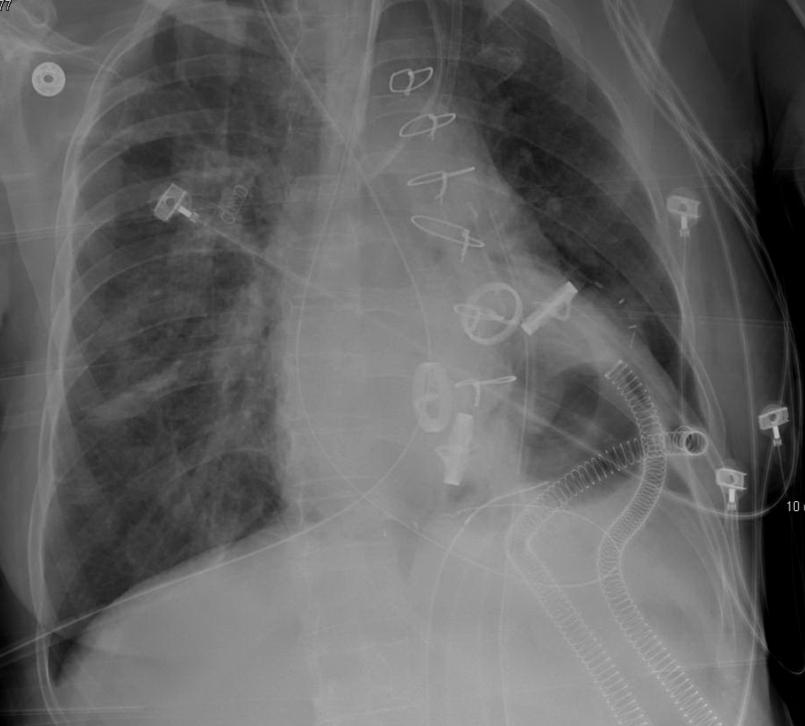
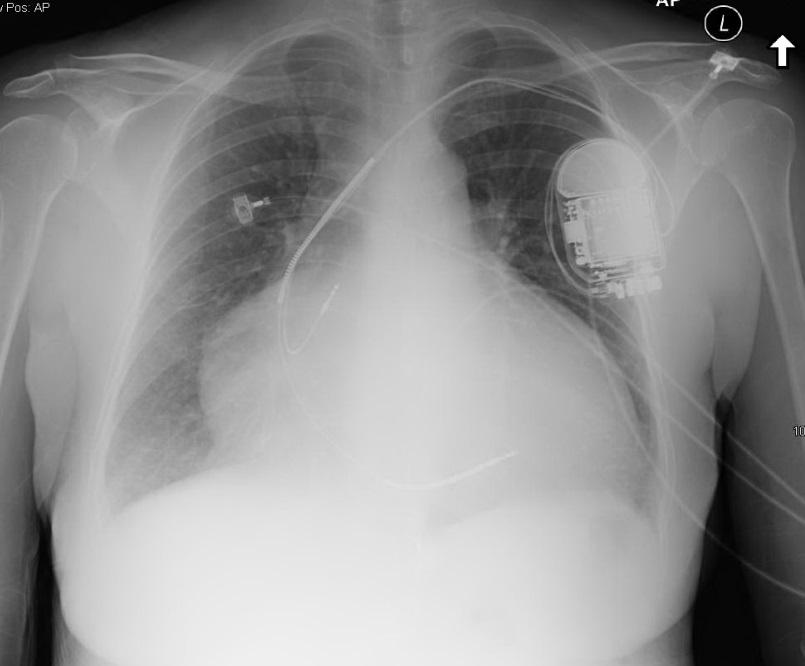
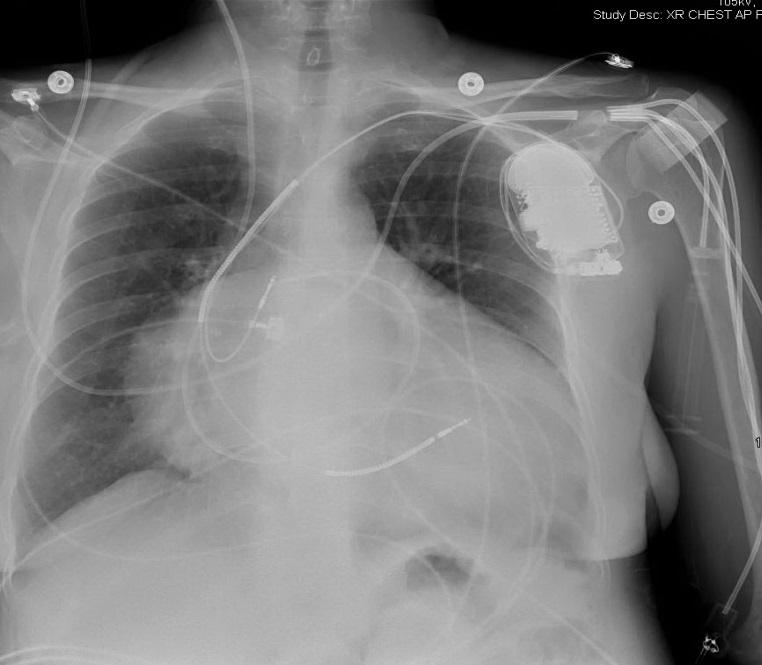
19 Chest Xrays


20 Echocardiogram: TTE/TEE assessment for LV, wall motion, valves, valves, pericardium, pressures TEE show better vegetations thrombus, & valve function TTE highly variable, nonspecific in infectious & inflammatory conditions, limited tissue characterization.
21 Diagnostic Tests Initial laboratory evaluation of patients presenting with HF should include complete blood count, urinalysis, serum electrolytes (including calcium and magnesium), blood urea nitrogen, serum creatinine, glucose, fasting lipid profile, liver function tests, and thyroid-stimulating hormone. Serial monitoring, when indicated, should include serum electrolytes and renal function. I IIa IIb III I IIa IIb III
22 Recommendations for Biomarkers Biomarker, Application Setting COR LOE Natriuretic peptides Diagnosis or exclusion of HF Ambulatory, Acute Prognosis of HF Ambulatory, Acute I A Achieve GDMT Ambulatory IIa B Guidance of acutely decompensated HF therapy Acute IIb C Biomarkers of myocardial injury Additive risk stratification Acute, Ambulatory I A I A Biomarkers of myocardial fibrosis Additive risk stratification Ambulatory Acute IIb IIb B A
23 Causes for Elevated BNP Cardiac Heart failure, including RV syndromes Acute coronary syndrome Heart muscle disease, including LVH Valvular heart disease Pericardial disease Atrial fibrillation Myocarditis Cardiac surgery Cardioversion Noncardiac Advancing age Anemia Renal failure Pulmonary causes: obstructive sleep apnea, severe pneumonia, pulmonary hypertension Critical illness Bacterial sepsis Severe burns Toxic-metabolic insults, including cancer chemotherapy and envenomation
24 Invasive Evaluation Recommendation COR LOE Monitoring with a pulmonary artery catheter should be performed in patients with respiratory distress or impaired systemic perfusion when clinical assessment is inadequate Invasive hemodynamic monitoring can be useful for carefully selected patients with acute HF with persistent symptoms and/or when hemodynamics are uncertain When coronary ischemia may be contributing to HF, coronary arteriography is reasonable Endomyocardial biopsy can be useful in patients with HF when a specific diagnosis is suspected that would influence therapy Routine use of invasive hemodynamic monitoring is not recommended in normotensive patients with acute HF Endomyocardial biopsy should not be performed in the routine evaluation of HF I IIa IIa IIa III: No Benefit III: Harm C C C C B C

25 Treatment of HF by Stages
26 Treatment of HFpEF Recommendations COR LOE Systolic and diastolic blood pressure should be controlled according to clinical practice guidelines Diuretics should be used for relief of symptoms due to volume overload Coronary revascularization for patients with CAD and angina or demonstrable myocardial ischemia. Management of AF according to published clinical practice guidelines for to improve symptomatic HF Use of beta-blocking agents, ACE inhibitors, and ARBs for hypertension in HFpEF ARBs might be considered to decrease hospitalizations in HFpEF Nutritional supplementation is not recommended in HFpEF I I IIa IIa IIa IIb III: No Benefit B C C C C B C
27 Stage A Hypertension and lipid disorders should be controlled in accordance with contemporary guidelines to lower the risk of HF. Other conditions that may lead to or contribute to HF, such as obesity, diabetes mellitus, tobacco use, and known cardiotoxic agents, should be controlled or avoided. I IIa IIb III I IIa IIb III
28 Recommendations for Treatment Stage B, Heart Failure Recommendations COR LOE In patients with a history of MI and reduced EF, ACE inhibitors or ARBs should be used to prevent HF I A In patients with MI and reduced EF, evidence-based beta blockers should be used to prevent HF I B In patients with MI, statins should be used to prevent HF I A Blood pressure should be controlled to prevent symptomatic HF I A ACE inhibitors should be used in all patients with a reduced EF to prevent HF Beta blockers should be used in all patients with a reduced EF to prevent HF An ICD is reasonable in patients with asymptomatic ischemic cardiomyopathy who are at least 40 d post-mi, have an LVEF 30%, and on GDMT Nondihydropyridine calcium channel blockers may be harmful in patients with low LVEF I I IIa III: Harm A C B C
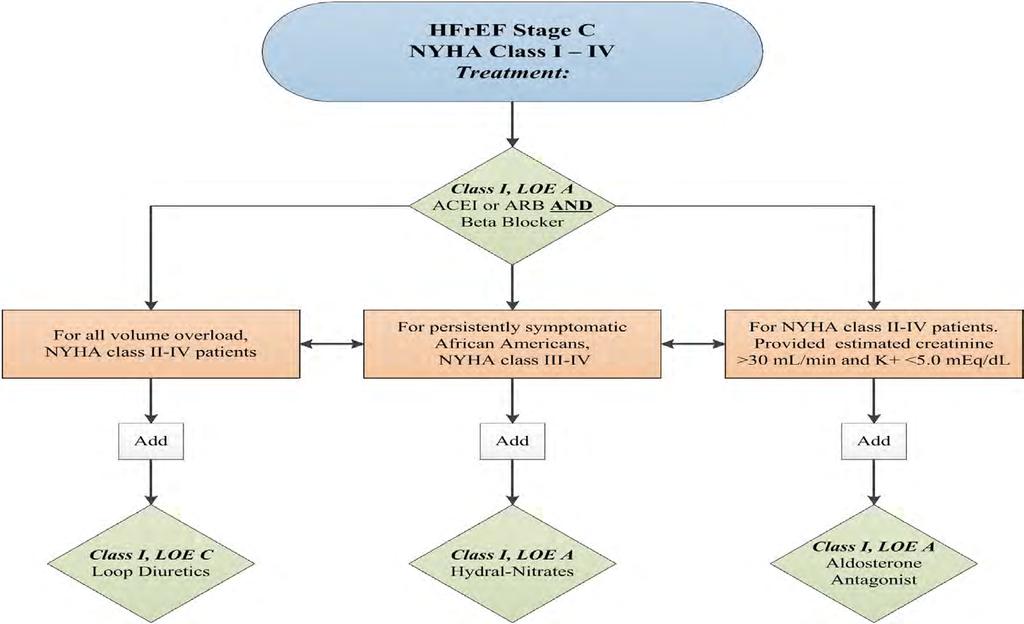
29 Pharmacologic Rx: Stage C HFrEF
30 Drugs Commonly Used in Stage C HFrEF Drug Initial Daily Dose(s) Maximum Doses(s) Mean Doses Achieved in Clinical Trials ACE Inhibitors Captopril 6.25 mg 3 times 50 mg 3 times mg/d (421) Enalapril 2.5 mg twice 10 to 20 mg twice 16.6 mg/d (412) Fosinopril 5 to 10 mg once 40 mg once Lisinopril 2.5 to 5 mg once 20 to 40 mg once 32.5 to 35.0 mg/d (444) Perindopril 2 mg once 8 to 16 mg once Quinapril 5 mg twice 20 mg twice Ramipril 1.25 to 2.5 mg once 10 mg once Trandolapril 1 mg once 4 mg once ARBs Candesartan 4 to 8 mg once 32 mg once 24 mg/d (419) Losartan 25 to 50 mg once 50 to 150 mg once 129 mg/d (420) Valsartan 20 to 40 mg twice 160 mg twice 254 mg/d (109) Aldosterone Antagonists Spironolactone 12.5 to 25 mg once 25 mg once or twice 26 mg/d (424) Eplerenone 25 mg once 50 mg once 42.6 mg/d (445)


31 Pharmacologic Therapy GDMT: Guideline Directed Medical Therapy
32 Drugs Commonly Used in Stage C HFrEF Drug Initial Daily Dose(s) Maximum Doses(s) Mean Doses Achieved in Clinical Trials Beta Blockers Bisoprolol 1.25 mg once 10 mg once 8.6 mg/d (118) Carvedilol mg twice 50 mg twice 37 mg/d (446) Carvedilol CR 10 mg once 80 mg once Metoprolol succinate extended release (metoprolol CR/XL) 12.5 to 25 mg once 200 mg once 159 mg/d (447) Hydralazine & Isosorbide Dinitrate Fixed dose combination (423) 37.5 mg hydralazine/ 20 mg isosorbide dinitrate 3 times daily 75 mg hydralazine/ 40 mg isosorbide dinitrate 3 times daily ~175 mg hydralazine/90 mg isosorbide dinitrate daily Hydralazine and isosorbide dinitrate (448) Hydralazine: 25 to 50 mg, 3 or 4 times daily and isorsorbide dinitrate: 20 to 30 mg 3 or 4 times daily Hydralazine: 300 mg daily in divided doses and isosorbide dinitrate 120 mg daily in divided doses
33 Pharmacological Therapy for Management of Stage C HFrEF Recommendations COR LOE Beta Blockers Use of 1 of the 3 beta blockers proven to reduce mortality is recommended for all stable patients I A Aldosterone Antagonists Aldosterone receptor antagonists are recommended in patients with NYHA class II-IV HF who have LVEF 35% I A Aldosterone receptor antagonists are recommended in patients following an acute MI who have LVEF 40% with symptoms of HF or I B DM Inappropriate use of aldosterone receptor antagonists may be harmful III: Harm B Hydralazine and Isosorbide Dinitrate The combination of hydralazine and isosorbide dinitrate is recommended for African-Americans, with NYHA class III IV HFrEF I A on GDMT A combination of hydralazine and isosorbide dinitrate can be useful in patients with HFrEF who cannot be given ACE inhibitors or ARBs IIa B
34 Pharmacological Therapy for Management of Stage C HFrEF Recommendations COR LOE Diuretics Diuretics are recommended in patients with HFrEF with fluid retention I C ACE Inhibitors ACE inhibitors are recommended for all patients with HFrEF ARBs ARBs are recommended in patients with HFrEF who are ACE inhibitor intolerant ARBs are reasonable as alternatives to ACE inhibitor as first line therapy in HFrEF The addition of an ARB may be considered in persistently symptomatic patients with HFrEF on GDMT IIb A Routine combined use of an ACE inhibitor, ARB, and aldosterone antagonist is potentially harmful III: Harm C I I IIa A A A
35 Pharmacologic Therapy for Management of Stage C HFrEF Recommendations COR LOE Digoxin Digoxin can be beneficial in patients with HFrEF IIa B Anticoagulation Patients with chronic HF with permanent/persistent/paroxysmal AF and an additional risk factor for cardioembolic stroke should receive chronic I A anticoagulant therapy* The selection of an anticoagulant agent should be individualized I C Chronic anticoagulation is reasonable for patients with chronic HF who have permanent/persistent/paroxysmal AF but without an additional risk factor for cardioembolic stroke* IIa B Anticoagulation is not recommended in patients with chronic HFrEF without AF, prior thromboembolic event, or a cardioembolic source Statins Statins are not beneficial as adjunctive therapy when prescribed solely for HF Omega-3 Fatty Acids Omega-3 PUFA supplementation is reasonable to use as adjunctive therapy in HFrEF or HFpEF patients III: No Benefit III: No Benefit IIa B A B
36 Pharmacological Therapy for Management of Stage C HFrEF Recommendations COR LOE Other Drugs Nutritional supplements as treatment for HF are not recommended in HFrEF Hormonal therapies other than to replete deficiencies are not recommended in HFrEF Drugs known to adversely affect the clinical status of patients with HFrEF are potentially harmful and should be avoided or withdrawn Long-term use of an infusion of a positive inotropic drug is not recommended and may be harmful except as palliation Calcium Channel Blockers Calcium channel blocking drugs are not recommended as routine in HFrEF III: No Benefit III: No Benefit III: Harm III: Harm III: No Benefit B C B C A
37 Diuretics Medications Starting Dose Max Duration/Action Loop Diuretics Furosemide mg Daily/BID 600 mg 6 8 hours Bumex mg Daily/BID 10 mg 4 6 hours Torsemide mg Daily 200 mg hours Thiazides Chlorothiazide mg 1000 mg 6-12 hours HCTZ 25 mg Daily/BID 200 mg 6-12 hours Metolazone 2.5 mg once 20 mg hours Indapamide 2.5 mg once 5 mg 36 hours
38 OTHER HF MEDICATIONS Medications Starting Dose Maximum Dose Spironolactone 12.5 mg - 25 mg Daily 25 mg Daily or BID Eplerenone 25 mg Daily 50 mg Daily Isosorbide 10 mg TID 40 mg TID Dinitrate Potassium 8 meq As needed Magnesium Various types As needed Hydralazine 25 mg TID mg TID Digoxin mg Daily mg Daily Sildenafil 20 mg TID 60 mg per Day Warfarin No loading INR goals vary Cholesterol Lowering Various statins, niacin, sequestrants, etc Variable doses for lipid goals
39 Medical Therapy for HFrEF, Stage C: Magnitude of Benefit in RCTs GDMT RR Reduction in Mortality NNT for Mortality Reduction (Standardized to 36 mo) RR HF Hospitalizations ACEi or ARB 17% 26 31% Beta blocker 34% 9 41% Aldosterone antagonist Hydralazine/ nitrate 30% 6 35% 43% 7 33%


40 Cumulative % reduction in odds of death at 24 months with each sequentially applied guideline recommended IMPROVE-HF Fonarow G C et al. J Am Heart Assoc 2012;1:16-26
41 Non-Pharmacologic Rx Salt Restriction Fluid Restriction I IIa IIb III I IIa IIb III Activity, exercise, Rehab Management of Co-morbidities Weight management Blood Pressure control Diabetes management Sleep Apnea I IIa IIb III I IIa IIb III
42 Non-Pharmacologic Rx Patient Education on Self-Management I IIa IIb III Genetic Testing and Counseling Device Therapy Pacemakers Implantable Defibrillators Cardiac Resynchronization
43 Device Therapy for Stage C HFrEF Recommendations COR LOE ICD therapy is recommended for primary prevention of SCD in selected patients with HFrEF at least 40 days post-mi with LVEF 35%, and NYHA class II or III symptoms on chronic GDMT, who are expected to live 1 year* I A CRT is indicated for patients who have LVEF 35%, sinus rhythm, LBBB with a QRS 150 ms ICD therapy is recommended for primary prevention of SCD in selected patients with HFrEF at least 40 days post-mi with LVEF 30%, and NYHA class I symptoms while receiving GDMT, who are expected to live 1 year* CRT can be useful for patients who have LVEF 35%, sinus rhythm, a non- LBBB pattern with a QRS 150 ms, and NYHA class III/ambulatory class IV symptoms on GDMT. CRT can be useful for patients who have LVEF 35%, sinus rhythm, LBBB with a QRS 120 to 149 ms, and NYHA class II, III or ambulatory IV symptoms on GDMT CRT can be useful in patients with AF and LVEF 35% on GDMT if a) the patient requires ventricular pacing or otherwise meets CRT criteria and b) AV nodal ablation or rate control allows near 100% ventricular pacing with CRT I I IIa IIa IIa A (NYHA class III/IV) B (NYHA class II) B A B B

44 Patient Education Teach Back: For Self Management Recommended Websites: American Association of Heart Failure Nurses Heart Failure Society of America





45 Compare Oat Products 0 mg 270 mg Sodium is much higher for many processed oat cereals. 210 mg Old fashioned rolled oats Instant oatmeal Cheerios





46 Provider Resources
47 AHD: When to Refer Repeated ( 2) hospitalizations or ED visits for HF in the past year Progressive deterioration in renal function (e.g., rise in BUN and creatinine) Weight loss without other cause (e.g., cardiac cachexia) Intolerance to ACE inhibitors due to hypotension and/or worsening renal function Intolerance to beta blockers due to worsening HF or hypotension Frequent systolic blood pressure <90 mm Hg Persistent dyspnea with dressing or bathing requiring rest Inability to walk 1 block on the level ground due to dyspnea or fatigue Recent need to escalate diuretics to maintain volume status, often reaching daily furosemide equivalent dose >160 mg/d and/or use of supplemental metolazone therapy Progressive decline in serum sodium, usually to <133 meq/l Frequent ICD shocks Adapted from Russell et al. Congest Heart Fail. 2008;14:
48 Advanced Heart Therapies Evaluation for cardiac transplantation is indicated for carefully selected patients with stage D HF despite GDMT, device, and surgical management. I IIa IIb III Effective systems of care coordination with special attention to care transitions should be deployed for every patient with chronic HF I IIa IIb III Palliative and supportive care is effective for patients with symptomatic advanced HF to improve quality of life. I IIa IIb III
49 Future Directions Novel HF agents Genetics testing Stem Cell regenerative therapy Mechanical Circulatory Support Heart Transplantation
50 Conclusions Primary care provides continue to play an important role in prevention and early diagnosis of HF. Evidence-based guideline directed diagnosis, evaluation and therapy should be the mainstay for patients with HF. Early detection and effective implementation of guidelinedirected care reduces mortality, improves QOL and preserves health care resources. Ongoing research is nee ded to answer the remaining questions on prevention, pharmacologic and nonpharmacological therapy of HF.
51 Q&A Contact information: 127 S San Vicente Blvd Suite A6100 Loa Angeles, CA
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
2016 Update to Heart Failure Clinical Practice Guidelines
 2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
2016 Update to Heart Failure Clinical Practice Guidelines Mitchell T. Saltzberg, MD, FACC, FAHA, FHFSA Medical Director of Advanced Heart Failure Froedtert & Medical College of Wisconsin Stages, Phenotypes
Heart Failure: Guideline-Directed Management and Therapy
 Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Heart Failure: Guideline-Directed Management and Therapy Guideline-Directed Management and Therapy (GDMT) was developed by the American College of Cardiology and American Heart Association to define the
Citation. What is New in the 2013 ACC/AHA HF Guideline. Dimensions in Heart and Vascular Care Penn State Heart and Vascular Institute
 What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
What is New in the 2013 ACC/AHA HF Guideline Dimensions in Heart and Vascular Care Penn State Heart and Vascular nstitute Friday October 18, 2013 Barry S. Clemson, MD Associate Professor of Medicine Penn
Introduction to Heart Failure. Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL
 Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
Introduction to Heart Failure Mauricio Velez, M.D. Transplant Cardiologist APACVS 2018 April 5-7 Miami, FL Disclosures No relevant financial relationships to disclose Objectives and Outline Define heart
The ACC Heart Failure Guidelines
 The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
The ACC Heart Failure Guidelines Fakhr Alayoubi, Msc,R Ph President of SCCP Cardiology Clinical Pharmacist Assistant Professor At King Saud University King Khalid University Hospital Riyadh-KSA 2017 ACC/AHA/HFSA
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
1/4/18. Heart Failure Guideline Review and Update. Disclosure. Pharmacist Objectives. Pharmacy Technician Objectives. What is Heart Failure?
 Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Disclosure Heart Failure Guideline Review and Update I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation. Natalie Beiter,
Heart Failure Management Policy and Procedure Phase 1
 1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
1301 Punchbowl Street, Harkness Suite 225 Honolulu, Hawaii 96813 Phone (808) 691-7220 Fax: (808) 691-4099 www.queenscipn.org Policy and Procedure Phase 1 Policy Number: Effective Date: Revised: Approved
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure
 New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
New Advances in the Diagnosis and Management of Acute and Chronic Heart Failure Deborah Budge, MD Intermountain Healthcare Heart Failure Cardiologist Objectives: State the updates from the ACC 2013 HF
Guideline-Directed Medical Therapy
 Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Guideline-Directed Medical Therapy Cardiovascular Outcomes Assessment of the MitraClip Percutaneous Therapy for Heart Failure Patients with Functional Mitral Regurgitation OPTIMAL THERAPY (As defined in
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
CLINICAL PRACTICE GUIDELINE
 CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
CLINICAL PRACTICE GUIDELINE Procedure: Congestive Heart Failure Guideline Review Cycle: Biennial Reviewed By: Amish Purohit, MD, MHA, CPE, FACHE Review Date: November 2014 Committee Approval Date: 11/12/2014
2 I. Reduced EF (HFrEF)
") HF Classification EF Description 2 I. Reduced EF (HFrEF) 40% 1. Referred to as systolic HF. 2. Randomized trials mainly enrolled patients with HFrEF. 3. Efficacious therapies is shown only in these patients.
HF Classification EF Description 2 I. Reduced EF (HFrEF) 40% 1. Referred to as systolic HF. 2. Randomized trials mainly enrolled patients with HFrEF. 3. Efficacious therapies is shown only in these patients.
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 3/2/2014
 3/2/2014") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center March 2014 Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading
State-of-the-Art Management of Chronic Systolic Heart Failure
 State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
State-of-the-Art Management of Chronic Systolic Heart Failure Michael McCulloch, MD 17 th Annual Cardiovascular Update Intermountain Medical Center December 16, 2017 Disclosures: I have no financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Heart Failure Management. Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist
 Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure Management Waleed AlHabeeb, MD, MHA Assistant Professor of Medicine Consultant Heart Failure Cardiologist Heart failure prevalence is expected to continue to increase¹ 21 MILLION ADULTS WORLDWIDE
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Estimated 5.7 million Americans with HF. 915, 000 new HF cases annually, HF incidence approaches
 Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Heart Failure: Management of a Chronic Disease Jenny Bauerly RN, CHFN, APRN-BC Heart Failure (HF) Definition A complex clinical syndrome that can result from any structural or functional cardiac disorder
Chronic. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Michael G. Shlipak, MD, MPH
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Assessment and Diagnosis of Heart Failure
 Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Assessment and Diagnosis of Heart Failure Heart failure (HF) is a complex clinical syndrome resulting from any structural or functional impairment of ventricular filling or ejection of blood and is characterized
Management Strategies for Advanced Heart Failure
 Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Management Strategies for Advanced Heart Failure Mary Norine Walsh, MD, FACC Medical Director, HF and Cardiac Transplantation St Vincent Heart Indianapolis, IN USA President American College of Cardiology
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Update in Congestive Hear Failure DRAGOS VESBIANU MD
 Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
Update in Congestive Hear Failure DRAGOS VESBIANU MD Case 58 yo AAM c/o shortness of breath for 3 weeks. Used to walk one mile per day and now he has noticed that he gets short of breath after 2 blocks.
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
HFpEF. April 26, 2018
 HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HFpEF April 26, 2018 (J Am Coll Cardiol 2017;70:2476 86) HFpEF 50% or more (40-71%) of patients with CHF have preserved LV systolic function. HFpEF is an increasingly frequent hospital discharge. Outcomes
HEART FAILURE: PHARMACOTHERAPY UPDATE
 HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
HEART FAILURE: PHARMACOTHERAPY UPDATE 3 HEART FAILURE REVIEW 1 5.1 million x1.25 = 6.375 million 40 years old = MICHAEL F. AKERS, PHARM.D. CLINICAL PHARMACIST CENTRACARE HEALTH, ST. CLOUD HOSPITAL HF Diagnosis
Updates in Congestive Heart Failure
 Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
Updates in Congestive Heart Failure GREGORY YOST, DO JOHNSTOWN CARDIOVASCULAR ASSOCIATES 1/28/2018 Disclosures Edwards speaker on Sapien3 valves (TAVR) Stages A-D and NYHA Classes I-IV Stage A: High risk
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 10/5/2015. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center
 10/5/2015. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
Heart Failure. Dr. William Vosik. January, 2012
 Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
Heart Failure Dr. William Vosik January, 2012 Questions for clinicians to ask Is this heart failure? What is the underlying cause? What are the associated disease processes? Which evidence-based treatment
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure
 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure Developed in Collaboration With the American Academy of Family Physicians, American College of Chest
I have no disclosures. Disclosures
 I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
I have no disclosures Disclosures What is Heart Failure? Heart Failure (HF) A complex clinical syndrome where patients present with symptoms (i.e. dyspnea, fatigue, fluid retention) that result from any
Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond
 Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond Steven Sheris, M.D., FACC, FACP Chief of Cardiology Gagnon Cardiovascular Institute at Overlook Medical
Process Improvement in Heart Failure Patient Care: Transitions From Door to Discharge and Beyond Steven Sheris, M.D., FACC, FACP Chief of Cardiology Gagnon Cardiovascular Institute at Overlook Medical
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%
 with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF<40%") Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
Evaluation and Management of Acute Decompensated Heart Failure (HF) with Reduced Ejection Fraction Systolic Heart Failure (HFrEF)(EF
OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE
 OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE GUIDELINE FOR THE MANAGEMENT OF HEART FAILURE Background: Heart failure (HF) is a complex clinical syndrome that results from
OHSU HEALTH SYSTEM OFFICE OF CLINICAL INTEGRATION AND EVIDENCE-BASED PRACTICE GUIDELINE FOR THE MANAGEMENT OF HEART FAILURE Background: Heart failure (HF) is a complex clinical syndrome that results from
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Heart Failure. Disclosures. Objectives: 8/28/2017. This is not a virus. It doesn t go away. none
 Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Heart Failure This is not a virus. It doesn t go away Shelley Wojtaszczyk, FNP-C, CHFN Heart Failure Program Coordinator Mercy Hospital of Buffalo none Disclosures Objectives: Defining and identifying
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Performance and Quality Measures 1. NQF Measure Number. Coronary Artery Disease Measure Set
 Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Unless indicated, the PINNACLE Registry measures are endorsed by the American College of Cardiology Foundation and the American Heart Association and may be used for purposes of health care insurance payer
Heart Failure 101 The Basic Principles of Diagnosis & Management
 Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Heart Failure 101 The Basic Principles of Diagnosis & Management Bill Tran, MD Non Invasive Cardiologist February 24, 2018 What the eye does not see and the mind does not know, does not exist. DH Lawrence
Long-Term Care Updates
 Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
Long-Term Care Updates July 2015 By Amy Friedman Wilson, PharmD Heart failure (HF) is a clinical condition in which ventricular filling or ejection of blood is structurally or functionally impaired. 1
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0.
 New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
New PINNACLE Measures The below measures for PINNACLE will be added as new measures to the outcomes reporting starting with Version 2.0. Measure Steward Measure Name Measure Description Rationale for Adding
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Contemporary Management of Heart Failure. Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium
 Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
Contemporary Management of Heart Failure Keerthy K Narisetty, MD Comprehensive Heart Failure Management Program BHHI Primary Care Symposium Disclosures I have no relevant relationships with commercial
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Definition of Congestive Heart Failure
 Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Heart Failure Definition of Congestive Heart Failure A clinical syndrome of signs & symptoms resulting from the heart s inability to supply adequate tissue perfusion. CHF Epidemiology Affects 4.7 million
Chronic. Outline. Congestive^ Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Chronic Congestive^ Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center
Heart Failure. Cardiac Anatomy. Functions of the Heart. Cardiac Cycle/Hemodynamics. Determinants of Cardiac Output. Cardiac Output
 Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
Cardiac Anatomy Heart Failure Professor Qing ZHANG Department of Cardiology, West China Hospital www.blaufuss.org Cardiac Cycle/Hemodynamics Functions of the Heart Essential functions of the heart to cover
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
HEART FAILURE KEEPING YOUR PATIENT AT HOME
 HEART FAILURE KEEPING YOUR PATIENT AT HOME SUZANNE FRAZIER MS, CRNP, NP-C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY HEART & VASCULAR INSTITUTE IMPACT OF HEART FAILURE In 2010,
HEART FAILURE KEEPING YOUR PATIENT AT HOME SUZANNE FRAZIER MS, CRNP, NP-C, CHFN HEART FAILURE DISEASE MANAGEMENT COORDINATOR PENN STATE HERSHEY HEART & VASCULAR INSTITUTE IMPACT OF HEART FAILURE In 2010,
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
HEART FAILURE. Heart Failure in the US. Heart Failure (HF) 2/20/2017. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center
 2/20/2017. Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center") HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
HEART FAILURE Martina Frost, PA-C Desert Cardiology of Tucson Northwest Medical Center Heart Failure in the US Prevalence - ~5 million 650,000 new cases annually 300,000 deaths annually Leading DRG among
Guideline Management of Chronic Heart Failure
 Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
Guideline Management of Chronic Heart Failure 2013 ACC/AHA Guideline Mgmt HF 2016 ACC/AHA/HFSA Focused Update 2017 ACCAHA/HFSA Focused Update October 17 th, 2017 Dawn Lombardo DO, MSc Professor of Medicine/Clinical
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Cardiovascular Clinical Practice Guideline Pilot Implementation
 Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
Cardiovascular Clinical Practice Guideline Pilot Implementation Pharmacologic Management of Chronic Heart Failure Sept 15, 2004 Angela Allerman, PharmD, BCPS DoD Pharmacoeconomic Center Promoting high
FINANCIAL DISCLOSURE: No relevant financial relationship exists
 The Value of Guideline Directed Medical Therapy in Heart Failure Steve Dentel RN BSN CPHQ National Director, Field Programs and Integration American Heart Association/American Stroke Association FINANCIAL
The Value of Guideline Directed Medical Therapy in Heart Failure Steve Dentel RN BSN CPHQ National Director, Field Programs and Integration American Heart Association/American Stroke Association FINANCIAL
Heart Failure Update John Coyle, M.D.
 Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Heart Failure Update 2011 John Coyle, M.D. Causes of Heart Failure Anderson,B.Am Heart J 1993;126:632-40 It It is now well-established that at least one-half of the patients presenting with symptoms and
Outline. Pathophysiology: Heart Failure. Heart Failure. Heart Failure: Definitions. Etiologies. Etiologies
 Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Outline Pathophysiology: Mat Maurer, MD Irving Assistant Professor of Medicine Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology : Definitions An inability of the
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
Heart Failure Heart Failure Introduction and History AHA 2015 Statistics About 6 million Americans 870,000 new cases each year 1 in 9 deaths related to HF Almost 1 million hospitalizations each year (cost
What s new in the 2017 heart failure guidelines. Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA
 What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
What s new in the 2017 heart failure guidelines Prof.Dr.Mehmet Birhan YILMAZ, FESC, FACC, FHFA Key points to remember 2017 guidelines recommend using natriuretic peptides as biomarkers to screen for heart
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
UPDATES IN MANAGEMENT OF HF
 UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
UPDATES IN MANAGEMENT OF HF Jennifer R Brown MD, MS Heart Failure Specialist Medstar Cardiology Associates DC ACP Meeting Fall 2017 Disclosures: speaker bureau for novartis speaker bureau for actelion
Outline. Chronic Heart Failure: Update on Effective Monitoring and Treatment. Heart Failure Epidemiology. Michael G.
 Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Chronic Heart Failure: Update on Effective Monitoring and Treatment Michael G. Shlipak, MD, MPH Professor of Medicine, UCSF Chief, Division of General Internal Medicine, SFVA Medical Center Scientific
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Heart Failure Medical and Surgical Treatment
 Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Heart Failure Medical and Surgical Treatment Daniel S. Yip, M.D. Medical Director, Heart Failure and Transplantation Mayo Clinic Second Annual Lakeland Regional Health Cardiovascular Symposium February
Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF
 CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
CLASSIFICATION OF HEART FAILURE Nora Goldschlager, M.D. SFGH Division of Cardiology UCSF DISCLOSURES: NONE CLASSIFICATION C OF HEART FAILURE NYHA I IV New paradigm Stage A: Pts at high risk of developing
Pathophysiology: Heart Failure
 Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Pathophysiology: Heart Failure Mat Maurer, MD Irving Assistant Professor of Medicine Outline Definitions and Classifications Epidemiology Muscle and Chamber Function Pathophysiology Heart Failure: Definitions
Innovation therapy in Heart Failure
 Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Innovation therapy in Heart Failure P. Laothavorn September 2015 Topics of discussion Basic Knowledge about heart failure Standard therapy New emerging therapy References: standard Therapy in Heart Failure
Our Readers Have An Attitude Toward Living
 February 2007 America s Wellness Guide Number 43 FREE at Doctor s Offices, Hospitals, Clinics and Kroger Pharmacies in the Midsouth COVER Standard of Care for Heart Failure Management By Arie Szatkowski,
February 2007 America s Wellness Guide Number 43 FREE at Doctor s Offices, Hospitals, Clinics and Kroger Pharmacies in the Midsouth COVER Standard of Care for Heart Failure Management By Arie Szatkowski,
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Improving Transition of Care in Congestive Heart Failure. Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare
 Improving Transition of Care in Congestive Heart Failure Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare Heart Failure Fastest growing clinical cardiac disease in the United
Improving Transition of Care in Congestive Heart Failure Mark J. Gloth, DO, MBA. Vice President, Chief Medical Officer HCR ManorCare Heart Failure Fastest growing clinical cardiac disease in the United
Heart Failure Treatments
 Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
The NEW Heart Failure Guidelines
 The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
The NEW Heart Failure Guidelines Daily Practice HF scenario of the Case Presentations HF as a complex and heterogeneous syndrome Several proposed pathophysiological mechanisms involving the heart and the
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart.org/HFGuidelinesToolkit
 2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
2017 /H/HFS Focused Update of the 2013 F/H 6.3.1 Biomarkers for Prevention: Recommendation OR LOE Recommendation a For patients at risk of developing HF, natriuretic peptide biomarker-based screening followed
Diagnosis & Management of Heart Failure. Abena A. Osei-Wusu, M.D. Medical Fiesta
 Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Diagnosis & Management of Heart Failure Abena A. Osei-Wusu, M.D. Medical Fiesta Learning Objectives: 1) Become familiar with pathogenesis of congestive heart failure. 2) Discuss clinical manifestations
Heart Failure. Subjective SOB (shortness of breath) Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)
 Peripheral edema. Orthopnea (2-3 pillows) PND (paroxysmal nocturnal dyspnea)") Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Pharmacology I. Definitions A. Heart Failure (HF) Heart Failure Ezra Levy, Pharm.D. HF Results when one or both ventricles are unable to pump sufficient blood to meet the body s needs There are 2 types
Congestive Heart Failure 2015
 Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Learn and LiveSM. ACC/AHA Pocket Guideline. Based on the ACC/AHA 2005 Guideline Update. Diagnosis and Management of Chronic Heart Failure in the Adult
 Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2005 Guideline Update Diagnosis and Management of Chronic Heart Failure in the Adult August 2005 I Assessment Characterization Therapy Special
Learn and LiveSM ACC/AHA Pocket Guideline Based on the ACC/AHA 2005 Guideline Update Diagnosis and Management of Chronic Heart Failure in the Adult August 2005 I Assessment Characterization Therapy Special
Gina G. Mentzer, MD Cardiologist, Heart Failure & Transplant Advanced Integrated Medicine & Surgery (AIMS) Program for Heart Failure April 18 th,
 Program for Heart Failure April 18 th,") Gina G. Mentzer, MD Cardiologist, Heart Failure & Transplant Advanced Integrated Medicine & Surgery (AIMS) Program for Heart Failure April 18 th, 2015 Heart Failure (HF) Describe the natural course of
Gina G. Mentzer, MD Cardiologist, Heart Failure & Transplant Advanced Integrated Medicine & Surgery (AIMS) Program for Heart Failure April 18 th, 2015 Heart Failure (HF) Describe the natural course of
DISCLOSURES ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION NONE
 ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
ACHIEVING SUCCESS THROUGH FAILURE: UPDATE ON HEART FAILURE WITH PRESERVED EJECTION FRACTION Lori M. Tam, MD Providence Heart Institute DISCLOSURES NONE 1 OUTLINE Systolic vs. Diastolic Heart Failure New
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary
 Prior Authorization and Quantity Limit Program Summary") Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
Neprilysin Inhibitor (Entresto ) Prior Authorization and Quantity Limit Program Summary FDA APPROVED INDICATIONS DOSAGE 1 Indication Entresto Reduce the risk of cardiovascular (sacubitril/valsartan) death
New CHF Patient in my Office: What Should I Do?
 New CHF Patient in my Office: What Should I Do? Joseph Mishkin MD FACC Advanced Heart Failure, Transplantation and Mechanical Circulatory Support No disclosures Disclosures Clinical Presentation 38 year
New CHF Patient in my Office: What Should I Do? Joseph Mishkin MD FACC Advanced Heart Failure, Transplantation and Mechanical Circulatory Support No disclosures Disclosures Clinical Presentation 38 year
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges
 Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Systolic Dysfunction Clinical/Hemodynamic Guide for Management; New Medical and Interventional Therapeutic Challenges Clyde W. Yancy, MD, MSc, FACC, FAHA, MACP Magerstadt Professor of Medicine Professor,
Heart Failure CTSHP Fall Seminar
 Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure CTSHP Fall Seminar Laurajo Ryan, PharmD, MSc, BCPS, CDE Pharmacist Learning Objectives Outline the pathophysiology of heart failure List triggers for decompensated heart failure Describe
Heart Failure Update. Bibiana Cujec MD May 2015
 Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
Heart Failure Update Bibiana Cujec MD May 2015 Disclosures Participation in clinical trial GUIDE IT (BNP in management of HF) Plan Review of new trials/ccs guidelines Management of heart failure: cases
HEART FAILURE PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
HEART FAILURE PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Understand the effects of heart failure in the body
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials -
 Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Heart Failure Pharmacotherapy An Update
 Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Heart Failure Pharmacotherapy An Update Kenneth Mishler, PharmD, MBA Objectives Review the epidemiology of heart failure (HF) Review evidence based guidelines for the use of mediations used to treat HF
Objectives. Outline 4/3/2014
 Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Jessica Litke PGY1 ISHP Spring Meeting April 12, 2014 Objectives Appreciate the significance of heart failure (HF) to a patient and to the health care system Understand 2013 ACCF/AHA guidelines for the
Heart Failure. Jay Shavadia
 Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
Heart Failure Jay Shavadia Definition Clinical syndrome characterized by: Symptoms: breathlessness at rest or on exercise, fatigue, tiredness or ankle swelling AND Signs: tachycardia, tachypnea, pulmonary
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION
 MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
MEDICAL MANAGEMENT OF PATIENTS WITH HEART FAILURE AND REDUCED EJECTION FRACTION FRANCIS X. CELIS, D.O. OPSO FALL CONFERENCE PORTLAND, OR 16 SEPTEMBER 2017 OVERVIEW What are the ACC/AHA Stages of HF? What
Management of Heart Failure and Cardiomyopathies in Pregnancy
 Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in
Management of Heart Failure and Cardiomyopathies in Pregnancy Professor Sanjay Sharma Disclosures: None Epidemiology of Cardiac Disease In Pregnancy Cardiovascular disease in pregnancy is increasing in